")
Back to Journals » International Journal of General Medicine » Volume 15
Association of Smoking with the Blood Concentration of 25-Hydroxy Vitamin D and Testosterone at High and Low Altitudes
Authors Zaman GS , Alshahrani SASAS, Laskar NB, Hadadi I , Alelyani M , Adam M , Babiker M, Musa MJ, Barua P, Mohammed MEA
Received 4 November 2021
Accepted for publication 24 January 2022
Published 7 February 2022 Volume 2022:15 Pages 1213—1223
DOI https://doi.org/10.2147/IJGM.S344904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gaffar Sarwar Zaman,1 Safar Abadi Saeed Al-Saleem Alshahrani,2 Nasrin Banu Laskar,3 Ibrahim Hadadi,4 Magbool Alelyani,4 Mohamed Adam,4 Mohammed Babiker,5 Mustafa Jafar Musa,6 Pranab Barua,7 Mohammed Elimam Ahamed Mohammed8
1Department of Clinical Laboratory Sciences, College of Applied Medical Sciences, King Khalid University, Abha, Saudi Arabia; 2Family & Community Department, College of Medicine, King Khalid University, Abha, Saudi Arabia; 3Department of Community Medicine, Sikkim Manipal Institute of Medical Sciences, Sikkim, India; 4Department of Radiological Sciences, College of Applied Medical Sciences, King Khalid University, Abha, Saudi Arabia; 5Department of Clinical Biochemistry, College of Medicine, King Khalid University, Abha, Saudi Arabia; 6Department of Radiology, College of Applied Medical Sciences, Jeddah University, Jeddah, Saudi Arabia; 7Department of Statistics, J.B. College, Jorhat, Assam, India; 8Department of Chemistry, Faculty of Science, King Khalid University, Abha, Saudi Arabia
Correspondence: Gaffar Sarwar Zaman
Department of Clinical Laboratory Sciences, College of Applied,Medical Sciences, King Khalid University, P.O. Box: 960, Abha, 61421, Saudi Arabia
, Tel +966 509228143
, Email [email protected]
Purpose: This research examined the association of cigarette smoking and altitude with the blood levels of 25-hydroxy vitamin D, testosterone and carotid artery thickness.
Patients and methods: This comparative cross-sectional study involved 37 non-smokers and 24 smokers from a high-altitude area (≥ 2245 m above sea level) and 40 smokers and 40 non-smokers from a low-altitude area (39– 283 m above sea level). The blood testosterone level was determined spectrophotometrically, and the 25-hydroxy vitamin D concentration was measured by ELISA. The IMT of the right and left carotid arteries was determined using ultrasound imaging.
Results: Smoking notably elevated the thickness of the intima media of the right and left carotid arteries at both high and low altitudes (p ≤ 0.001). Smoking at high altitude was associated with a significant increase in the concentration of 25-hydroxy vitamin D and testosterone, while at low altitude it was associated with a significant decrease in both parameters (p ≤ 0.046).
Conclusion: These contrasting results suggest that future studies should focus on finding out if other biochemical parameters show any significant differences in smokers or/and non-smokers when they are tested at elevated height and sea-level. This indicates that dose modifications of medicines (related to alterations in vitamin D and testosterone levels) should be kept in mind while treating smokers and non-smokers at elevated height above sea level.
Keywords: altitude, smoking, aging, body mass index, intima media thickness
Introduction
Several studies have reported a positive relationship between smoking and the intima media thickness (IMT) of the carotid arteries,1 while other studies have found a strong association with carotid artery plaque and alterations in carotid hemodynamics, but absence of stenosis of the carotid arteries, in some cases of smokers.2 One study noted that the effect of smoking on the IMT depends on the gene polymorphism of the NADPH oxidase.3 With respect to the relationship of smoking with the blood level of 25-hydroxy vitamin D (25-HVD), it has been reported that smoking is associated with a lower blood level of vitamin D.4,5 The circulating amount of 25-HVD is considered as an individual’s vitamin D status. A study using an electrochemiluminescence immunoassay (ECLIA) reported an increased concentration of 25-HVD in the blood of smokers by unknown mechanisms.6 Many conflicting reports have been reported regarding the level of 25-HVD in smokers and non-smokers.6 With reference to the association of smoking with the blood level of testosterone, different results have been reported, ranging from insignificant, negative, to positive effects.7–9 Previous studies showed that living at high altitude is associated with both an increase and decrease in the IMT of the carotid arteries compared to living at low altitudes.1,10 People living at high altitude are reported to have either low or high blood levels of vitamin D.11–13 It has also been reported that living at high altitude is associated with increased blood concentration of testosterone and erythrocytosis.14 Another study concluded that adaptation to high altitude is associated with a decreased blood concentration of testosterone.15 Aging is associated with the thickening of the IMT, as reported by many studies.16,17 Many studies have remarked that low concentration of blood 25-HVD and testosterone is characteristic of aging.18,19 Increased BMI is associated with increased thickening of the intima media of the carotid arteries20 and also low blood concentration of 25-HVD and testosterone.21,22 All these led us to formulate this study, to find out what difference we can practically expect for smokers and non-smokers, for the above-mentioned parameters, at an elevated height and at sea level. The current study investigated the relationship of altitude, smoking, aging, and body mass index with the IMT and the blood concentration of 25-HVD and testosterone. The parameters we have studied, at an elevated height with almost zero humidity, are unique study, considering the fact that they were compared with sea-level where humidity was present.
Materials and Methods
Study Design
This comparative cross-sectional study, conducted among people of same ethnic groups, was carried out among smokers (male) and healthy male participants living at high and low altitudes of ≥2245 metre above sea level and 39–283 m above sea level, respectively.
Study Community
The study subjects in the high-altitude group were 37 non-smoking and 24 smoking males aged 20 to 49 years. The low altitude participants were 40 non-smoking and 40 smoking males with age range of 40 to 60 years. Smoking status of the smokers was self-reported. To be considered smokers, the amount of daily smoked cigarettes was taken as minimum 3 cigarettes per day for the last 7 years; however, level of cigarette dependence and exact duration of smoking were not available. Medication history was taken to exclude any participant who was taking vitamin D or testosterone supplement in last 3 months.
Ethical Clearance
This study was carried out after obtaining an ethical license certificate from governmental ethical committee of King Khalid University, with the code number (REC#2018-06-36). Our study complies with the Declaration of Helsinki. The study subjects participated in this study only after signing a written informed consent.
Blood Sampling
Blood sampling was carried out from 08:00 to 11:00 AM. The sample quantity was 5 mL of intravenous blood in an EDTA tube. Then, centrifugation of the blood samples was done, and the separated plasma was stored at −20 ͦ C.
Measurement of Vitamin D and Testosterone
Vitamin D was analyzed using an ELISA kit of CTK Biotech Company, 13855 Stowe Dr, Poway, CA 92064, United States (REF E8010) and the testosterone level was measured with a HUMAN diagnostics ELISA kit (Reference number 55010).
Ultrasound Test of Carotid Intima Media Thickness
To ascertain the carotid intima media thickness (CIMT), an ultrasonography device (South Korean MEDISON) supported by a linear probe of 7.5 MHz probe was utilized. Measurement of CIMT was carried out by B-mode sonography with an electrical sensor on both extra-cranial and carotid arteries. The study subjects were told to face the left side and lie comfortably for the investigation involving the central sternocleidomastoid lying under thyroid cartilage. We analyzed the common carotid arterial forms at a point 1 cm near the carotid split bulb area using images along the length of the carotid artery. The highest IMT was calculated at the bifurcation region, bulb region, and both the near and far sides of the carotid. CIMT was assessed in mm units using the correct software.
Statistical Assessment
The results of this study were statistically analyzed utilizing the analysis of variance test (ANOVA) with the least significance post-hoc test and the independent samples t-test of the Statistical Package for Social Sciences (IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp. IBM Corp. Released 2012). The statistical significance level was set at p ≤ 0.05.
Results
Effect of Smoking on the Studied Parameters
Smoking at high and low altitudes was associated with a significantly increased carotid artery IMT. Smoking at high altitude was associated with increased blood level of 25-HVD and testosterone, while smoking at a low altitude was significantly associated with decreased concentration of 25-HVD and testosterone (Table 1).
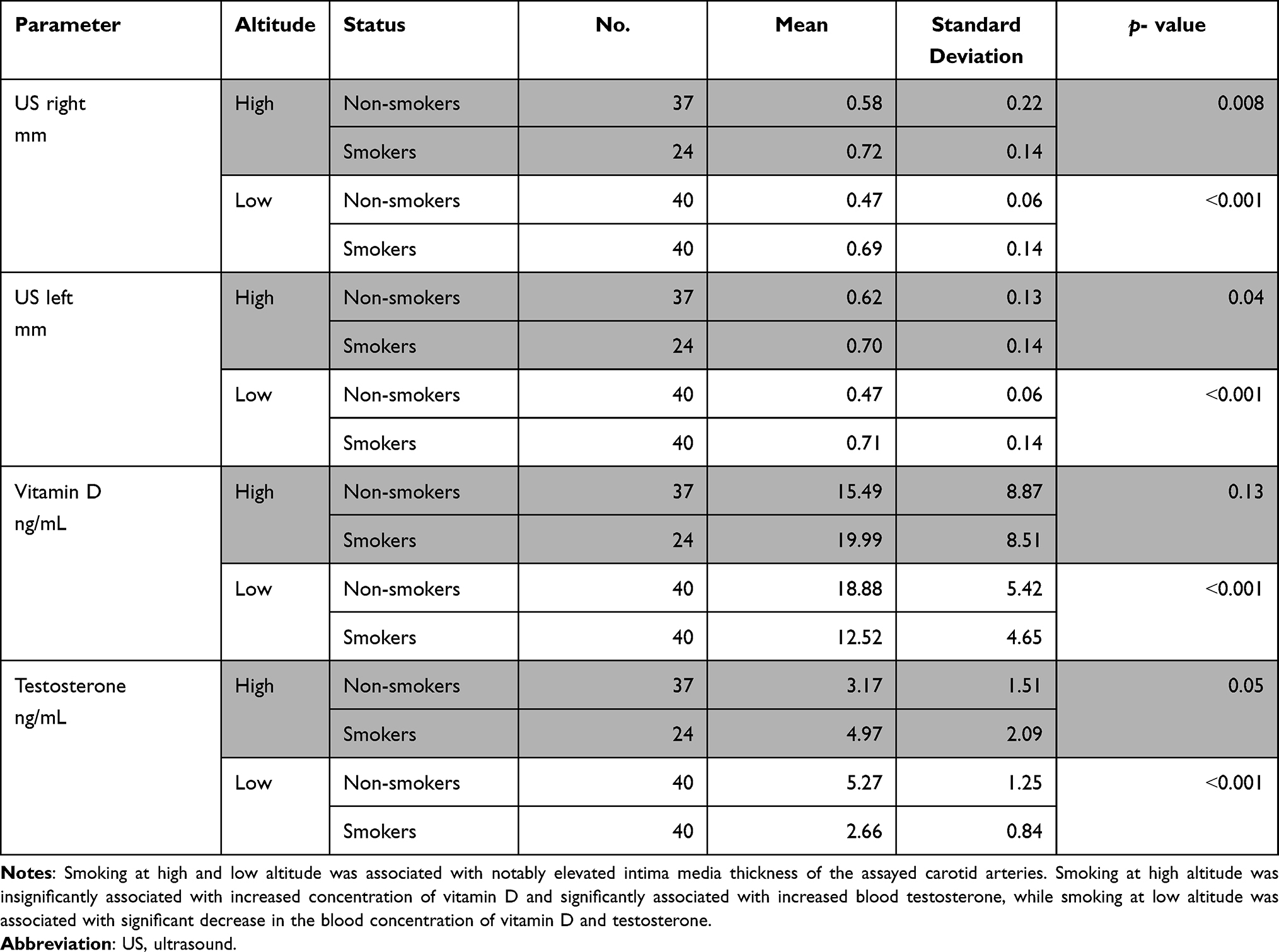 |
Table 1 Association of Smoking with the Studied Parameters |
Effect of Altitude on the Results
Altitude was significantly associated with all the studied parameters except the IMT of the carotid arteries of the smokers (Table 2). However, altitude was associated with a significant increase in the IMT of carotid arteries of the non-smokers and in the mean blood level of 25-HVD and testosterone of the smokers. Moreover, altitude was associated with significantly decreased mean blood concentration of 25-HVD and testosterone in the non-smokers (Table 2).
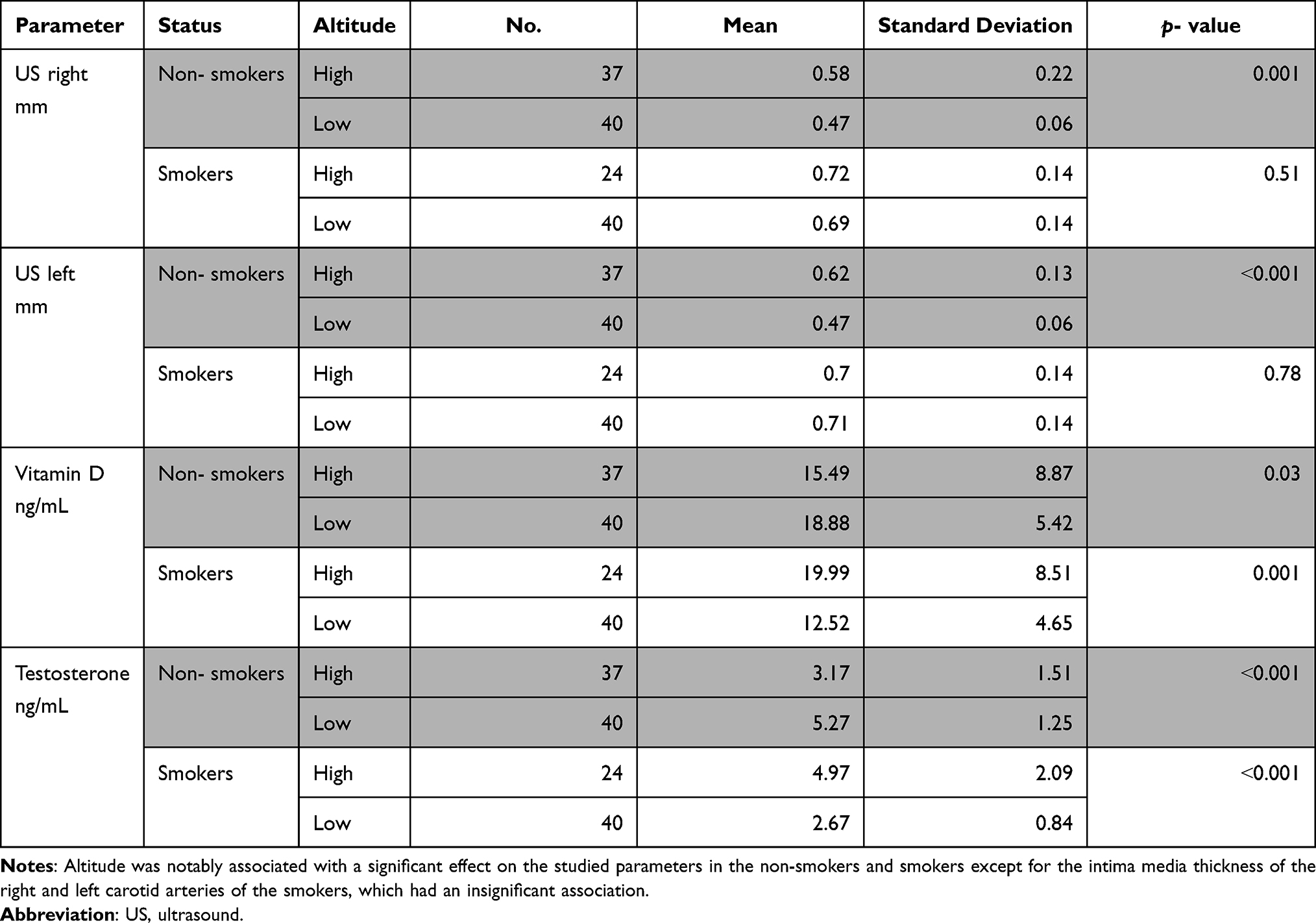 |
Table 2 Association of Altitude with the Studied Parameters |
Age Effects
At high altitude, in the non-smokers the IMT of the carotid arteries and the mean blood concentration of 25-HVD were significantly increased with age but there was an insignificant effect on the mean blood concentration of testosterone. The age of the smokers at high altitude was associated with insignificant effects on the studied parameters (Table 3). At low altitude, age had no significant association with the studied parameters in the non-smokers and smokers (Table 4).
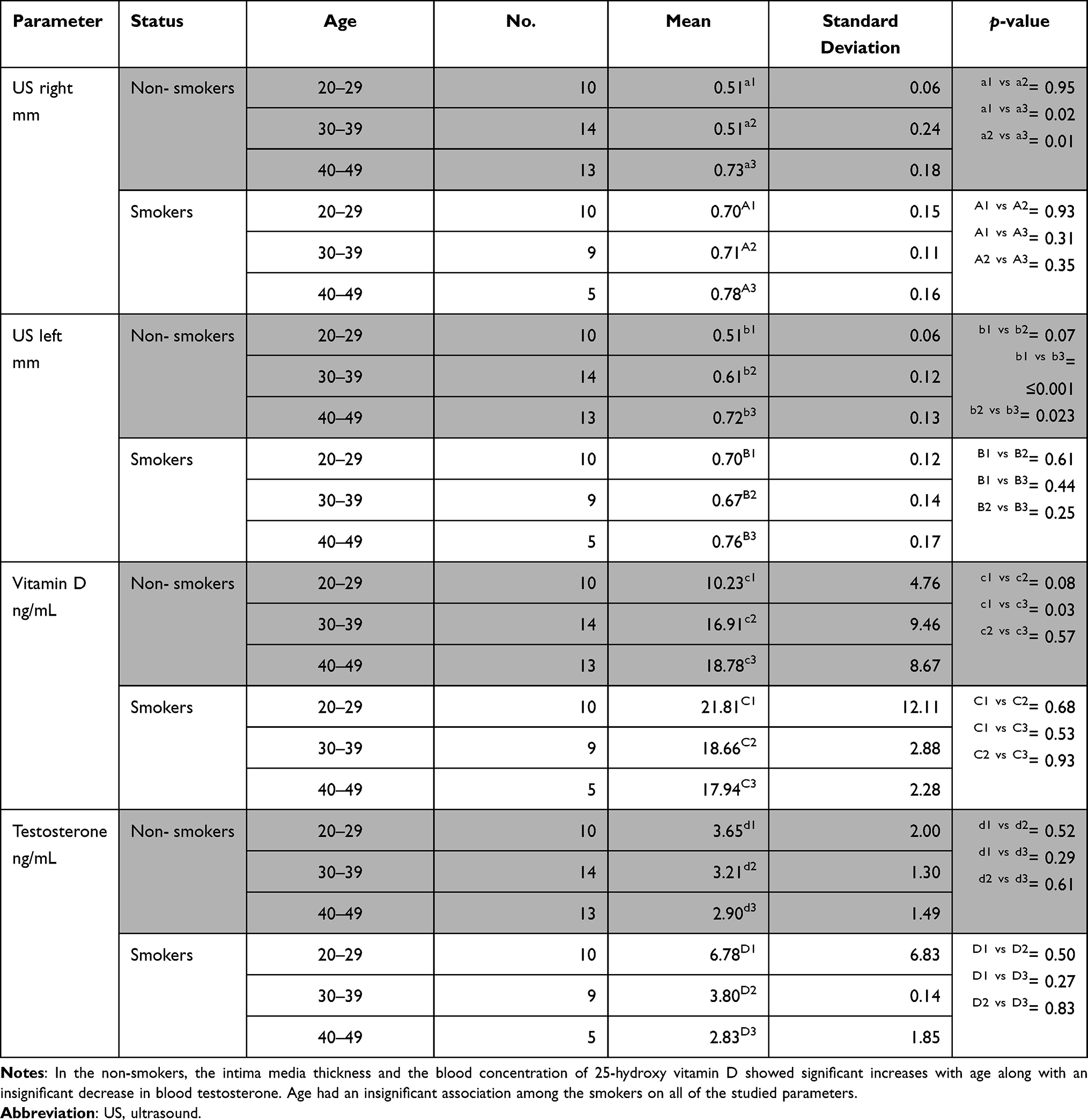 |
Table 3 Association of Age with the Studied Parameters at High Altitude |
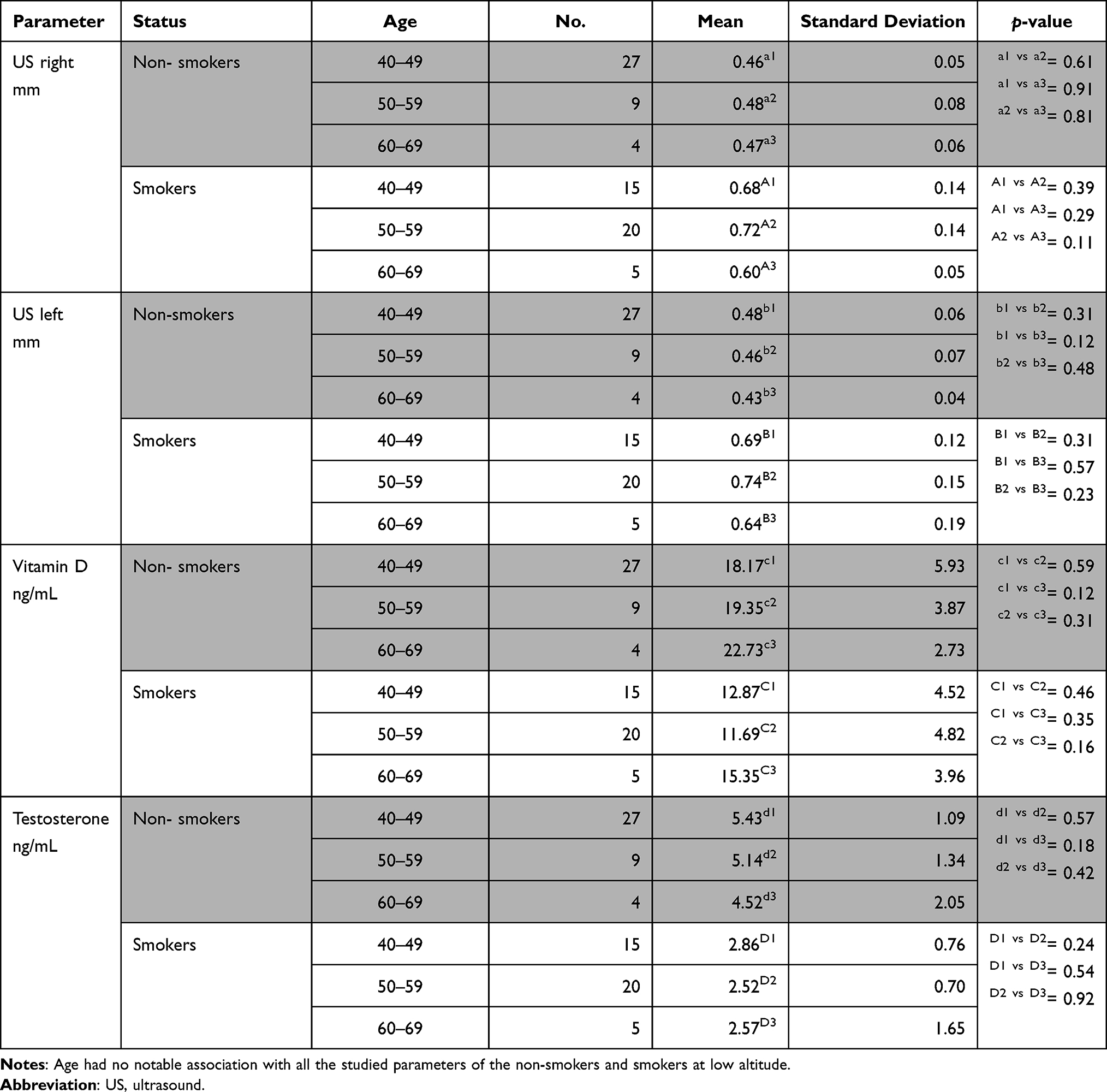 |
Table 4 Association of Age with the Studied Parameters at Low Altitude |
Effect of BMI
The BMI of the non-smokers living at high altitude was associated with a significant decrease in the blood concentration of testosterone, and it was insignificantly associated with the other parameters (Table 5). The BMI of the smokers at high altitude was significantly associated with increased IMT of the carotid arteries (Table 5).
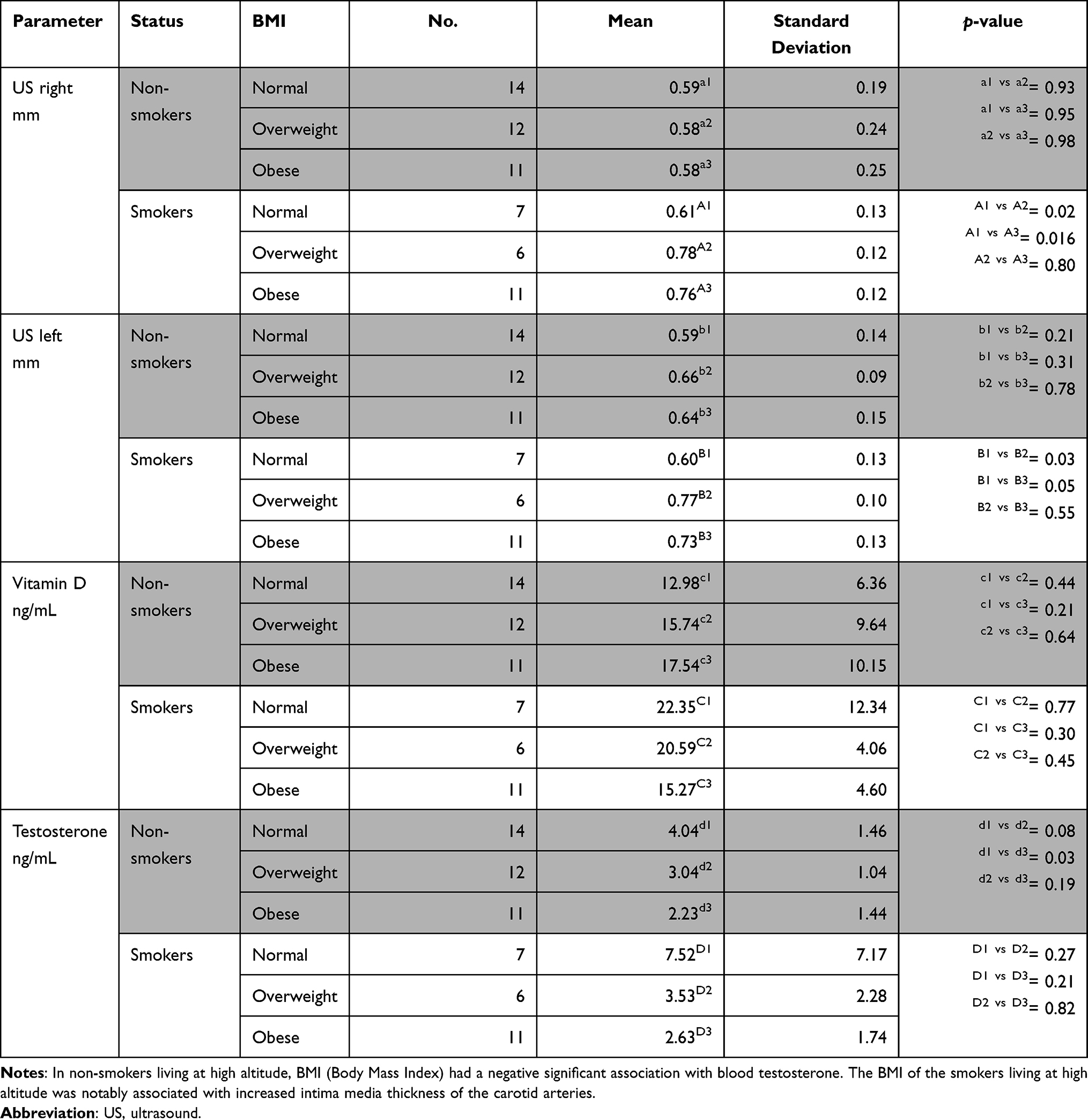 |
Table 5 Association of BMI with the Studied Parameters at High Altitude |
The association of BMI and the studied parameters in the non-smokers and smokers living at low altitude was insignificant except that the testosterone of the non-smokers was significantly increased in the obese participants compared to the overweight ones (Table 6).
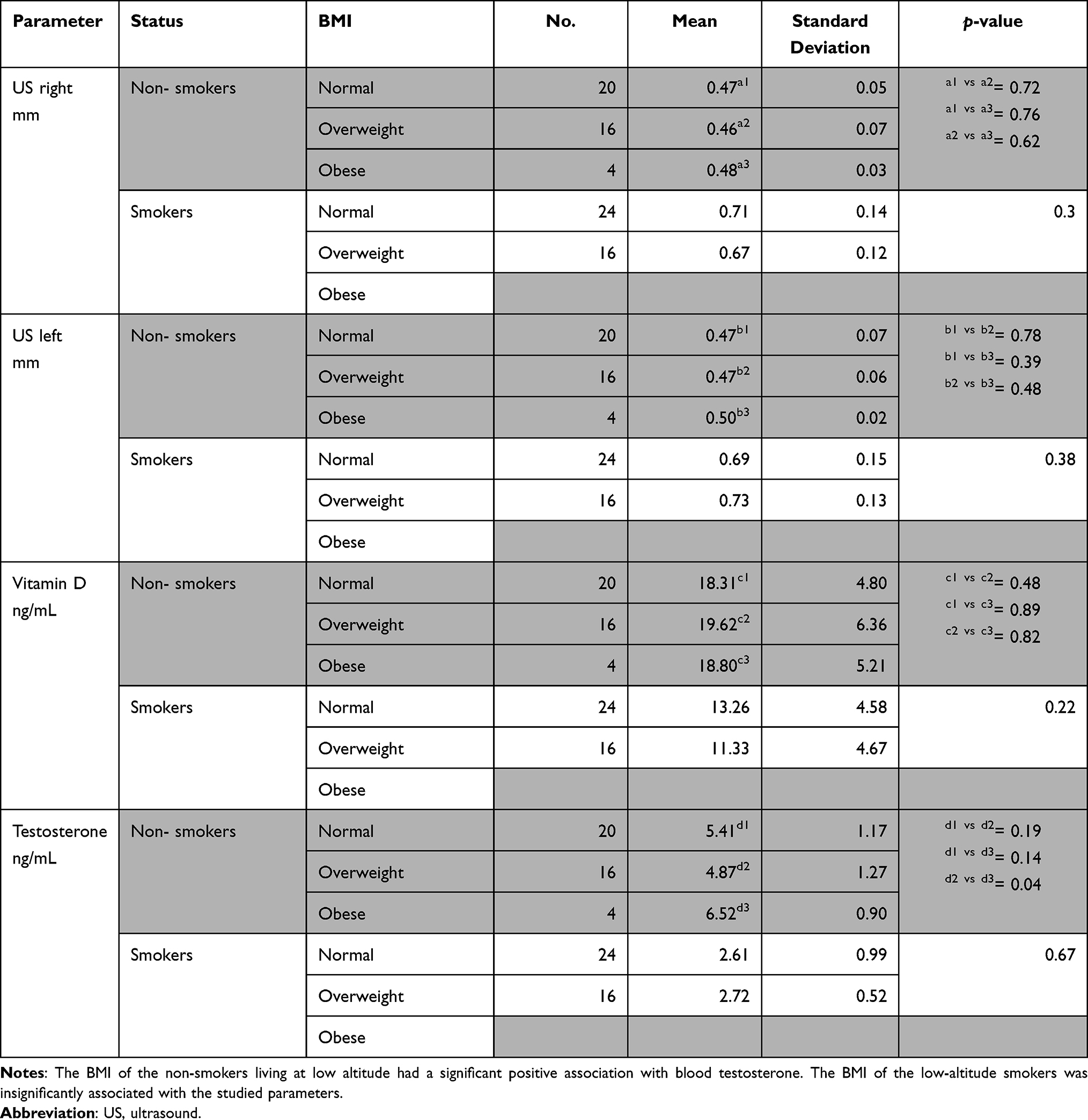 |
Table 6 Association of BMI with the Studied Parameters at Low Altitude |
Discussion
Similar to most previous studies,1,23 this study showed that smoking is associated with significantly increased IMT of the carotid arteries, possibly as a result of speeding the atherosclerotic process. However, Babiker et al noted that there is a strong association between tobacco smoking and the formation of carotid artery plaques, but he reported that the majority of the smokers did not develop narrowing and thickening of the carotid arteries.2 Similar to Grimnes et al,6 we have reported that smoking at high altitude had an insignificant association with increased blood concentration of vitamin D. Moreover, this study found that smoking at a low altitude was associated with a significant decrease in the blood level of 25-HVD, similar to the findings of Ren et al.,4 Jiang et al,5 and Lange et al.24 This may be due to the fact that cigarette smoke may affect expression levels of the vitamin D receptor.25 This may also be due to decline in production of the active form of vitamin D (1,25-dihydroxyvitamin D) in lung epithelial cells,26 which was absent or delayed due to some unknown reasons at height, the reason for which is beyond the scope of this study. Also, reduced barometric pressures and excessive erythrocytosis encountered at higher altitudes might be also the reason for this increment of blood Vitamin D at high altitude due to some unknown mechanisms. Our results showed that altitude was associated with a significantly decreased level of 25-HVD in the blood of non-smokers while it was associated with a significantly increased concentration of the vitamin in the blood of the smokers. Orces11 and Calvo12 stated that women living at high altitude in Ecuador and Colombia were suffering from low concentration of 25-HDV. Kapil et al28 reported that children living in an Indian high-altitude area (Shimla, Himachal Pradesh) suffer from vitamin D deficiency. Other studies found that living at high altitudes is associated directly and significantly with blood concentration of 25-HVD.13
In this study, smoking was also associated with a significant increase in blood testosterone at high altitude and a significant decrease in blood testosterone at low altitude. Elevated blood testosterone at high altitude could be due to proliferation of Leydig cells and subsequent enhanced testosterone release due to hypoxia. Testosterone production results in the Leydig cells with 17α-hydroxyprogesterone being one of its precursors. Since 17α-hydroxyprogesterone is elevated at high altitude with respect to sea level, this could be another reason for this.14 However, previous studies reported an insignificant difference in the increase and decrease in the blood testosterone of smokers. Haik et al7 reported an insignificant variation in the blood testosterone (total and free) between waterpipe smokers and non-smokers.7 Svartberg and Jorde8 reported that smokers were characterized by 15% excess total testosterone and 13% excess free testosterone compared to non-smokers. In a letter to the editor, James9 wrote that some studies found that smoking is associated with decreased blood testosterone. Regarding the effect of altitude on the blood concentration of testosterone, this study found that altitude was associated with a significantly decreased level of testosterone in the blood of the non-smokers while it was associated with a significantly increased concentration of the hormone in the blood of the smokers. Gonzales et al14 and Gonzales29 reported that high altitude acclimatization is associated with high blood testosterone. Sawhney et al15 reported that living at high altitude (3500 m above sea level) is associated with low concentration of luteinizing hormone (LH) and testosterone. Regarding association of age with testosterone, many literatures have reported that there is a gradual decline in serum total testosterone level, which begins from 30 years of age and thereby proceeds at a level of approximately 1.6% every year.30,31 Also, it has been cited in previous literature that BMI is always inversely proportional to the concentration of serum testosterone.32 It is assumed that 25-HVD requirements vary with age, but age-related serum 25-HVD is not constant.33 Recent literatures have stated that regardless of the BMI of the participant, 25-HVD were found to be higher in those participants who practice daily physical activity.34
This study found that altitude was associated with a significantly increased IMT of the carotid arteries in the non-smokers and was associated with an insignificant effect on the IMT of the carotid arteries of the smokers.27 Two previous studies showed that altitude is associated with significant increase in the IMT of the carotid arteries.1,28 Sukun et al10 found that people living at high altitude had a lower rate of carotid artery stenosis and lower value of carotid artery IMT.
We have shown that at high altitude, the IMT of the carotid arteries and the blood concentration of vitamin D increased significantly with aging, along with an insignificant decrease in the blood testosterone. The age of the high-altitude smokers was associated with insignificant effects on the studied parameters. The age of the low-altitude non-smokers and smokers was not associated with the studied parameters. Previous studies showed that the aging and thickening of the carotid arteries are significantly associated.16,17,35 Aging was mostly associated with decreased blood concentration of 25-HVD and 1, 25-dihydroxy vitamin D mostly because of the decreased synthesis of cholesterol in the skin.18,20 Moreover, aging is known to decrease the blood levels of testosterone.19,36,37
This study showed that in non-smokers at high altitudes, BMI was significantly associated with decreased blood testosterone but not other parameters. The BMI of the high-altitude smokers was associated with significantly increased IMT of the carotid arteries. At low altitude, BMI was associated with significantly increased blood testosterone in the non-smokers. Previous studies showed that BMI is one of the factors associated with increased IMT of the carotid arteries.20,38 Increased BMI is associated with decreased blood concentration of vitamin D.21,39 Previously published articles found that obesity was associated with low levels of total and free blood testosterone.22,40,41
Because this is a comparative cross-sectional study, it is limited by the small number of the participants and subgroups. Also, we did not go too deep into the socioeconomic status, lifestyles, medical history of both groups. However, it opens the door for future research on the effect of smoking and altitude on the blood levels of vitamin D, testosterone and other biochemical parameters and their physiological consequences.
Conclusion
The results of this study showed that 1) smoking at high altitude was associated with a significantly increased blood concentration of testosterone—while smoking at low altitude was associated with a significant decrease of both of vitamin D and testosterone; 2) living at high altitude was associated with a significant increase in the blood concentration of 25-HVD and testosterone of the smokers, and significant decrease in the blood concentration of 25-HVD and testosterone in non-smokers; 3) aging at high altitude was associated with a significantly increased IMT of the carotid arteries and blood 25-HVD in the non-smokers; and 4) BMI was associated with a significantly decreased blood testosterone level in the non-smokers at high altitude while BMI of the non-smokers at low altitude was associated with a significantly increased blood testosterone level. The findings that smoking resulted in differences in blood levels of testosterone and vitamin D with respect to height and sea level indicate that dose modifications of medicines (related to alterations in vitamin D and testosterone levels) should be kept in mind while treating smokers and non-smokers at elevated height above sea level. Also, future studies can add to the justifications given for these differences. Future studies should focus on finding out if other biochemical parameters show any significant differences in smokers or/and non-smokers, when they are tested at elevated height and sea-level.
Acknowledgment
The authors are grateful to the Deanship of Scientific Research, King Khalid University, for funding this research under grant number R.G.P1.\92\40.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alelyani M, Al-Saleem Alshahrani SAS, Zaman GS, et al. Stenosis of carotid arteries and concentration of some blood lipid parameters amongst tobacco smokers in Abha: a case–control study. Appl Sci. 2021;11:2001. doi:10.3390/app11052001
2. Babiker MS. The effects of smoking on carotid artery hemodynamics. J Diagn Med Sonog. 2016;32:149–152. doi:10.1177/8756479316646062
3. Fan M, Raitakari OT, Kähönen M, et al. The association between cigarette smoking and carotid intima–media thickness is influenced by the −930A/GCYBA gene polymorphism: the cardiovascular risk in young Finns. Am J Hypertens. 2009;22:281–287. doi:10.1038/ajh.2008.349
4. Ren W, Gu Y, Zhu L, et al. The effect of cigarette smoking on vitamin D level and depression in male patients with acute ischemic stroke. Compr Psychiatry. 2016;65:9–14. doi:10.1016/j.comppsych.2015.09.006
5. Jiang CQ, Chan YH, Xu L, et al. Smoking and serum vitamin D in older Chinese people: cross-sectional analysis based on the Guangzhou Biobank Cohort Study. BMJ Open. 2016;6:e010946. doi:10.1136/bmjopen-2015-010946
6. Grimnes G, Almaas B, Eggen AE, et al. Effect of smoking on the serum levels of 25-hydroxy vitamin D depends on the assay employed. Eur J Endocrinol. 2010;163:339–348. doi:10.1530/EJE-10-0150
7. Haik MY, Ashour AA, Alahmad YFM, et al. Water-pipe smoking and serum testosterone levels in adult males in Qatar. Tob Induc Dis. 2019;17:19. doi:10.18332/tid/99572
8. Svartberg J, Jorde R. Endogenous testosterone levels and smoking in men. The fifth Tromsø study. Int J Androl. 2007;30:137–143. doi:10.1111/j.1365-2605.2006.00720.x
9. James WH. Smoking, sperm quality and testosterone level. Human Reprod. 2002;17:3275–3276. doi:10.1093/humrep/17.12.3275
10. Sukun A, Onal C, Tufanoğlu FH. The effect of living at high altitude on carotid intima-media thickness in the elderly: a comparative study. Acta Radiol. 2021. doi:10.1177/02841851211022503
11. Orces CH. Vitamin D status among older adults residing in the littoral and Andes mountains in Ecuador.. Sci World J. 2015;545297. doi:10.1155/2015/545297
12. Calvo MS. High-altitude living and vitamin D: factors associated with viral risk? Am J Clin Nutrit. 2020;112:915–916. doi:10.1093/ajcn/nqaa250
13. Hirschler V, Molinari C, Maccallini G, Intersimone P, Gonzalez CD. Vitamin D levels and cardiometabolic markers in indigenous Argentinean children living at different altitudes. Glob Pediatr Health. 2019. doi:10.1177/2333794X18821942
14. Gonzales GF, Gasco M, Tapia V, Gonzales-Castañeda C. High serum testosterone levels are associated with excessive erythrocytosis of chronic mountain sickness in men. Am J Physiol Endocrinol Metab. 2009;296:e1319–E1325. doi:10.1152/ajpendo.90940.2008
15. Sawhney R, Chhabra P, Malhotra A, Singh T, Riar S, Rai R. Hormone profiles at high altitude in man. Andrologia. 1985;17:178–184. doi:10.1111/j.1439-0272.1985.tb00983.x
16. Ishizu T, Ishimitsu T, Yanagi H, et al. Effect of age on carotid arterial intima-media thickness in childhood. Heart Vessels. 2004;19:189–195. doi:10.1007/s00380-004-0766-8
17. van den Munckhof ICL, Jones H, Hopman MTE, et al. Relation between age and carotid artery intima-medial thickness: a systematic review. Clin Cardiol. 2018;41:698–704. doi:10.1002/clc.22934
18. Gallagher JC. Vitamin D and aging. Endocrinol Metab Clin North Am. 2013;42:319–332. doi:10.1016/j.ecl.2013.02.004
19. Lopes R, Neves K, Carneiro F, Tostes R. Testosterone and vascular function in aging. Front Physiol. 2012;3:89. doi:10.3389/fphys.2012.00089
20. Jin Y, Kim D, Cho J, Lee I, Choi K, Kang H. Association between obesity and carotid intima-media thickness in Korean office workers: the mediating effect of physical activity. BioMed Res Int. 2018;Article ID 4285038. doi:10.1155/2018/4285038
21. Orces C. The association between body mass index and vitamin D supplement use among adults in the United States. Cureus. 2019;11:e5721. doi:10.7759/cureus.5721
22. Diaz-Arjonilla M, Schwarcz M, Swerdloff RS, Wang C. Obesity, low testosterone levels and erectile dysfunction. Int J Impotence Res. 2009;21:89–98.
23. Hansen K, Östling G, Persson M, et al. The effect of smoking on carotid intima-media thickness progression rate and rate of lumen diameter reduction. Eur J Intern Med. 2016;28:74–79. doi:10.1016/j.ejim.2015.10.018
24. Lange NE, Sparrow D, Vokonas P, Litonjua AA. Vitamin D deficiency, smoking, and lung function in the Normative Aging Study. Am J Respir Crit Care Med. 2012;186:616–621. doi:10.1164/rccm.201110-1868OC
25. Okrit F, Chantranuwatana P, Werawatganon D, Chayanupatkul M, Sanguanrungsirikul S. Changes of vitamin D receptors (VDR) and MAPK activation in cytoplasmic and nuclear fractions following exposure to cigarette smoke with or without filter in rats. Heliyon. 2021;7(1):e05927. doi:10.1016/j.heliyon.2021.e05927
26. Lange NE, Sparrow D, Vokonas P, Litonjua AA. Vitamin D deficiency, smoking, and lung function in the Normative Aging Study. Am J Respir Crit Care Med. 2012;186(7):616–621. doi:10.1164/rccm.201110-1868OC
27. Qin C, Zhang L, Ye Z, Xie M. Application of quality intima-media thickness test in assessing carotid vascular function in obese people at high altitudes and risk of coronary heart disease. Int J Clin Exp Med. 2018;11:6136–6140.
28. Kapil U, Pandey RM, Goswami R, et al. Prevalence of Vitamin D deficiency and associated risk factors among children residing at high altitude in Shimla district, Himachal Pradesh, India. Indian J Endocrinol Metab. 2017;21:178–183. doi:10.4103/2230-8210.196031
29. Gonzales GF. Hemoglobina y testosterona: importancia en la aclimatación y adaptación a la altura [Hemoglobin and testosterone: importance on high altitude acclimatization and adaptation]. Rev Peru Med Exp Salud Publica. 2011;28:92–100. doi:10.1590/s1726-46342011000100015
30. Tajar A, Forti G, O’Neill TW; EMAS Group, et al. Characteristics of secondary, primary, and compensated hypogonadism in aging men: evidence from the European Male Ageing Study. J Clin Endocrinol Metab. 2010;95:1810–1818. doi:10.1210/jc.2009-1796
31. Qaseem A, Horwitch CA, Vijan S, Etxeandia-Ikobaltzeta I, Kansagara D. Testosterone treatment in adult men with age-related low testosterone: a clinical guideline from the American college of physicians. Ann Intern Med. 2020;172(2):126–133. doi:10.7326/M19-0882
32. Diaz-Arjonilla M, Schwarcz M, Swerdloff R, et al., Obesity, low testosterone levels and erectile dysfunction. Int J Impot Res. 2009;21:89–98.
33. Vieth R, Ladak Y, Walfish PG. Age-related changes in the 25-hydroxyvitamin D versus parathyroid hormone relationship suggest a different reason why older adults require more vitamin D. J Clin Endocrinol Metab. 2003;88(1):185–191. doi:10.1210/jc.2002-021064
34. Valentini A, Perrone MA, Cianfarani MA, et al. Obesity, vitamin D status and physical activity: 1,25(OH)2D as a potential marker of vitamin D deficiency in obese subjects. Panminerva Med. 2020;62(2):83–92. doi:10.23736/S0031-0808.20.03770-2
35. Buljan K, Soldo SB, Janculjak D, et al. Relationship between age and thickness of carotid arteries in a population without risk factors for atherosclerosis. Coll Antropol. 2015;39:779–784.
36. Elizondo-Montemayor L, Castillo EC, Rodríguez-López C, et al. Seasonal variation in vitamin D in association with age, inflammatory cytokines, anthropometric parameters, and lifestyle factors in older adults. Mediators Inflamm. 2017;Article ID 5719461. doi:10.1155/2017/5719461
37. Handelsman DJ. Testosterone and male aging: faltering hope for rejuvenation. JAMA. 2017;317:699–701. doi:10.1001/jama.2017.0129
38. Qu B, Qu T. Causes of changes in carotid intima-media thickness: a literature review. Cardiovasc Ultrasound. 2015;13:46. doi:10.1186/s12947-015-0041-4
39. Lagunova Z, Porojnicu AC, Lindberg F, Hexeberg S, Moan J. The dependency of vitamin D status on body mass index, gender, age and season. Anticancer Res. 2009;29:3713–3720.
40. Kelly DM, Jones TH. Testosterone and obesity. Obes Rev. 2015;16:581–606. doi:10.1111/obr.12282
41. Shamim MO, Ali Khan FM, Arshad R. Association between serum total testosterone and Body Mass Index in middle aged healthy men. Pak J Med Sci. 2015;31:355–359. doi:10.12669/pjms.312.6130
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.