")
Back to Journals » Clinical Epidemiology » Volume 14
Association of Sleep Duration, Midday Napping with Atrial Fibrillation in Patients with Hypertension
Authors Xiong Y, Yu Y, Cheng J, Zhou W, Bao H, Cheng X
Received 3 December 2021
Accepted for publication 9 March 2022
Published 22 March 2022 Volume 2022:14 Pages 385—393
DOI https://doi.org/10.2147/CLEP.S351045
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Vera Ehrenstein
Yurong Xiong,1,2,* Yun Yu,1,2,* Jianduan Cheng,3 Wei Zhou,2,4 Huihui Bao,1,2,4 Xiaoshu Cheng1,2,4
1Department of Cardiovascular Medicine, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China; 2Jiangxi Provincial Cardiovascular Disease Clinical Medical Research Center, Nanchang, Jiangxi, People’s Republic of China; 3Wuyuan Chinese Medicine Hospital, Shangrao, Jiangxi, People’s Republic of China; 4Center for Prevention and Treatment of Cardiovascular Diseases, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huihui Bao; Xiaoshu Cheng, Department of Cardiovascular Medicine, The Second Affiliated Hospital of Nanchang University, No. 1 Minde Road, Nanchang, Jiangxi, 330006, People’s Republic of China, Tel +8613870092915 ; +8613607089128, Fax +86-0791-86262262, Email [email protected]; [email protected]
Objective: This study aimed to assess the associations of sleep duration, midday napping and the risk of atrial fibrillation (AF) in patients with hypertension.
Methods: We conducted a cross-sectional study enrolling 11,524 hypertensive participates from the Chinese Hypertension Registry Study. Information on sleep duration and midday napping were obtained by a self-administered questionnaire. Multivariate logistic regression analyses were performed to estimate odds ratio (OR) and 95% confidence intervals (CIs) for the risk of AF.
Results: Compared with sleeping 6 to ≤ 8 hours/night, those reporting shorter sleep duration (≤ 5 hours/night) had a greater risk of AF (OR 1.95; 95% CI 1.28– 2.95) in the fully adjusted model, while longer sleep (≥ 9 hours/night) was not significantly associated with the risk of AF. Compared with nonhabitual nappers, nappers had a higher risk of AF (OR 1.28; 95% CI 1.03– 1.60) in the fully adjusted model. Moreover, we observed significant joint effects of sleeping ≤ 5 hours/night and nap (OR 2.13; 95% CI 1.09– 4.14) on the risk of AF after adjusting for confounding factors.
Conclusion: Short sleep duration and midday napping were independently and jointly associated with higher risks of AF in patients with hypertension.
Keywords: sleep medicine, midday napping, atrial fibrillation, hypertension
Introduction
Atrial fibrillation (AF) is the most common sustained heart arrhythmia in adults and affects an estimated 43.6 million individuals worldwide.1 In China, the prevalence of AF increased 20-fold over 11 years, and the currently estimated prevalence of AF is 0.2% in individuals aged ≥ 20 years.2 AF is a major societal health problem related to the risk of stroke,3 heart failure,4 coronary artery disease,5 and chronic kidney disease,6 as well as morbidity and mortality.7 Identifying all the risk factors for AF is important for creating population-based strategies to reduce the risk of AF-related morbidity.8 However, currently known risk factors for AF explain only about one-half of the population attributable risk, emphasizing the need to identify the novel risk factors for AF, especially modifiable risk factors.9–11
Up to now, the relationship between sleep duration and AF remains in dispute. Several studies have indicated that longer sleep duration was associated with incident AF.12,13 However, recent data from Pittsburgh Medical Center sleep laboratories showed that short sleep duration is an independent risk factor for incident AF.14 Moreover, a Mendelian randomization (MR) study has demonstrated that too little sleep may be associated with the risk of AF.15 Evidence from prior studies indicated that both short and long sleep duration as the risk factors for various health problems including metabolic syndrome,16 diabetes,17 obesity,18 hypertension,19 dyslipidemia20 and myocardial infarction.21 Moreover, all these diseases were related with AF. In addition, most of the studies have assessed the relationship of sleep duration with incident AF regardless of midday napping, which is common throughout China. In the meantime, little is known, about the effect of sleep duration on the incident AF among hypertensive patients. Hypertension as a risk factor that leads to AF,22 a better understanding of the sleep duration in hypertensive patients may reduce the huge burden of AF. Therefore, we designed this study to explore the association between sleep duration, midday napping and incident AF in patients with hypertension.
Methods
Participants and Study Design
The patients in this study came from China H-type Hypertension Registry Study that was reported previously.23,24 Briefly, this is a real-world, multicenter, observational registry study. From March 2018 to August 2018, a total of 14,234 hypertensive subjects were enrolled in this study in Wuyuan, Jiangxi province of China. Eligible participants were adults aged 18 years and older who had hypertension. Hypertension was determined as seated, resting systolic blood pressure (SBP) ≥140 mmHg or diastolic blood pressure (DBP) ≥90 mmHg at the screening, self-report history of hypertension, or the use of antihypertensive drug(s). The exclusion criteria included neurological abnormalities, inability to follow up according to the study protocol, or plans to relocate shortly, and the patients, who were not suitable for inclusion or for long-term follow-up assessed by study physicians. All participants provided written informed consent. The protocol was approved by the Ethics Committee of Institute of BioMedicine, Anhui Medical University (Registration number: ChiCTR1800017274).
2710 patients were excluded for missing data on sleep duration or midday napping. Thus, a final sample of 11,524 subjects was included in the analyses (Figure S1).
Assessment of Covariates
The information on demographic characteristics (age and gender), lifestyle factors (smoking, drinking, and physical activity, sleep quality), and medical history (diabetes mellitus, coronary heart disease (CHD), hyperlipidemia, stroke, duration of hypertension, and use of medications) were collected by trained researchers. The body mass index (BMI) was calculated as weight (kg)/height (m2). Blood pressure (BP) was measured by the automated electronic device (Omron; Dalian, China). After 10 minutes of rest, we calculated SBP and DBP as the average of the three BP measurements.
Fasting venous blood samples were obtained from all study patients. Next, the blood samples would be frozen and analyzed Biaojia Biotechnology Laboratory, Shenzhen, China. Fasting plasma glucose (FPG) and fasting lipids (total cholesterol, high-density lipoprotein-cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglycerides) were determined using automatic clinical analyzers (Beckman Coulter). The formula for estimated glomerular filtration rate (eGFR) was used for the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.
Assessment of Sleep Behavior
Sleep duration and midday napping were assessed by a self-administered questionnaire. Sleep duration was assessed by the question: “How many hours on average do you sleep per night?” Mean sleep duration was categorized into 3 groups: ≤5, 6 ≥ ≤ 8 and ≥9 hours, based on previous studies.25,26 Midday napping was assessed by asking “Did you have midday napping habit?” with the following responses: yes, no. Sleep quality was ascertained by the question: “How was your sleep quality at night?” with the following responses: good, fair, poor. Snoring status was obtained by asking “Do you snore when you sleep?” with the following responses: “no,” “sometimes,” and “frequently.”
Assessment of Atrial Fibrillation
AF was defined as AF or atrial flutter captured on standard 12-lead electrocardiogram. Subjects who were not found to have AF according to the ECG test, but had previous medical records or any prior ECG record for AF episode were also defined as having AF. The diagnosis of AF based on the ECG was first conducted by a physician and then verified by the senior physician.8
Statistical Analyses
Continuous variables were presented as mean ± standard deviation (SD) or median (interquartile range (IQR)) and compared using the t-test. Categorical variables were summarized as count (%) and analyzed by chi-square tests. Multivariate logistic regression analysis was used to evaluate the risk of AF by calculating the odds ratio (OR) and 95% confidence interval (CI) with adjustment for major covariates in four models. Model 1: crude model; Model 2: adjusted for age, gender, BMI, physical activity, smoking, drinking; Model 3: added SBP, DBP, duration of hypertension, diabetes mellitus, hyperlipidemia, CHD, antihypertensive agents, antidiabetes agents, lipid-lowering agents, FPG, triglyceride, HDL-C, LDL-C, and eGFR to model 2. Model 4: added snoring status, sleep quality, sleep duration and midday napping to model 3. In addition, possible modifications on the associations between sleep duration, midday napping and AF were also evaluated by stratified analyses and interaction testing. Moreover, we estimated the joint effects of sleep duration and midday napping on the risk of AF, and using the moderate sleep duration (6–8 hours) and nonhabitual nap as the reference group.
All data analyzed were using the statistical package R (http://www.r-project.org) and Empower (R) (www.empowerstats.com; X&Y Solutions, Inc., Boston, MA). A 2-tailed P < 0.05 was considered to be statistically significant.
Results
Characteristics of the Subjects
A total of 11,524 participants with hypertension were included in the final analysis (5542 men and 5982 women, aged 64.1 ± 9.8 years). The prevalence of AF was 3.4% (388/11,524). Baseline characteristics are shown in Table 1. Of the 11,524 subjects, 4.3%, 51.0% and 44.7% reported they sleep ≤5, 6–8 and ≥9 hours/night, respectively and 53.1% reported midday napping (Table 1). Compare with participants reporting 6 to ≤8 hours/night, those reporting sleep duration ≤5 hours/night had higher values of age, stroke, hyperlipidemia, CHD, lower values of male, physical activity, smoking, drinking and eGFR. In addition, compare with nonhabitual nappers, nappers had higher values of male, age, smoking, drinking, stroke, hyperlipidemia, diabetes mellitus, hyperlipidemia and antidiabetes agents.
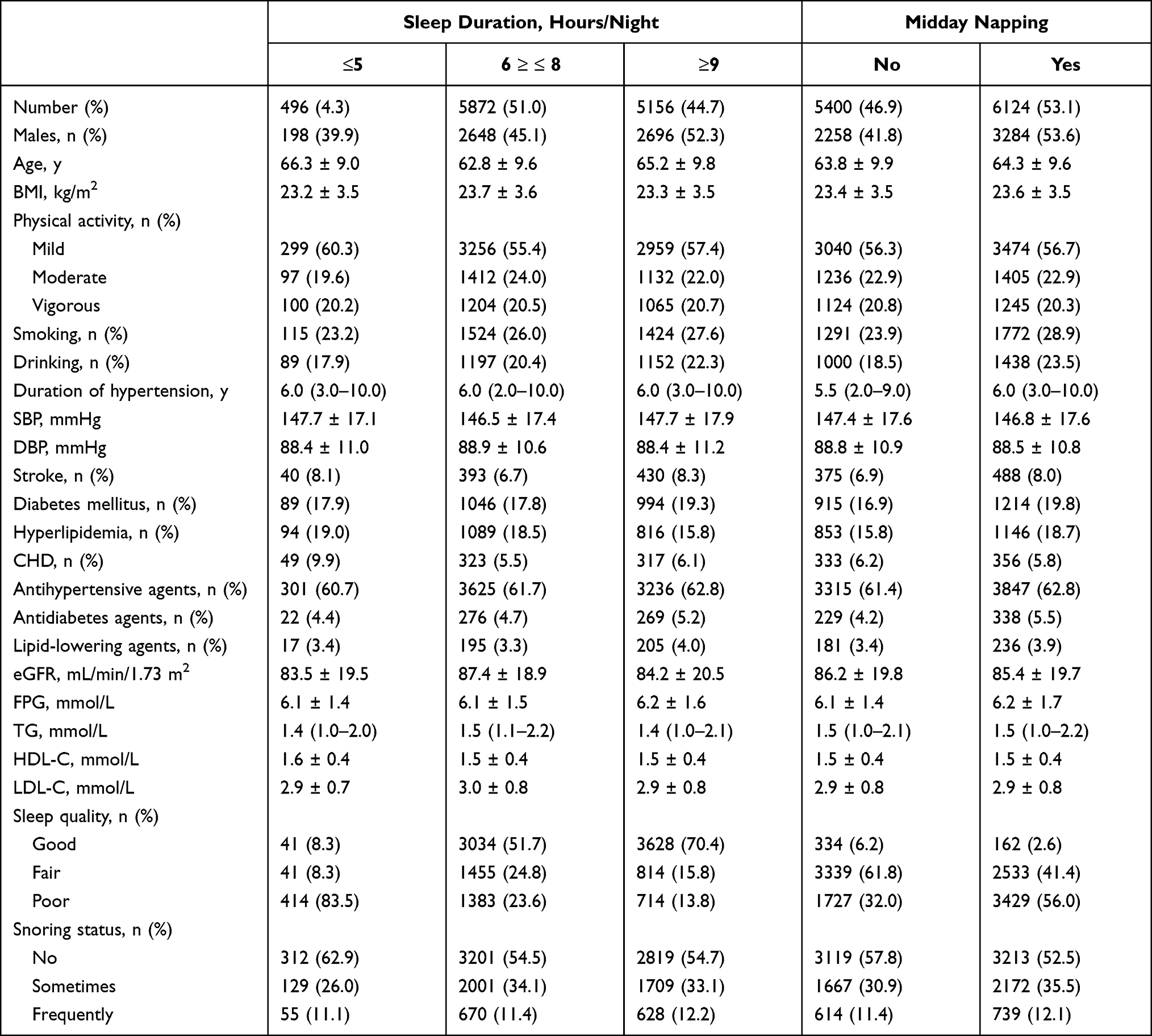 |
Table 1 Baseline Characteristics of the Study Participants According to Sleep Duration and Midday Napping |
Association Between Sleep Duration, Midday Napping and AF
Table 2 shows the associations of sleep duration and midday napping with AF. Compared with sleeping 6 to ≤8 hours/night, those reporting shorter sleep duration (≤5 hours/night) had a greater risk of AF (aOR 1.95; 95% CI 1.28, 2.95) in the fully adjusted model, while longer sleep (≥9 hours/night) had no significant associated on the risk of AF (aOR 0.89; 95% CI 0.71, 1.12). We further investigated the association between midday napping with incident AF. Compare with nonhabitual nappers, nappers had a higher risk of AF (aOR 1.28; 95% CI 1.03, 1.60). Moreover, we explored the joint effects of sleep duration and midday napping on the risks of AF. Compared with those reporting moderate sleep duration (6 to ≤8 hours) and no napping, subjects who short sleep duration ≤5 hours combined with midday napping showed a significantly increased risk of AF (aOR 2.16, 95% CI 1.11–4.23), whereas no significant joint effect of sleeping ≥9 hours and no napping on AF was observed (Figure 1).
 |
Table 2 Association of Sleep Duration and Midday Napping with Atrial Fibrillation |
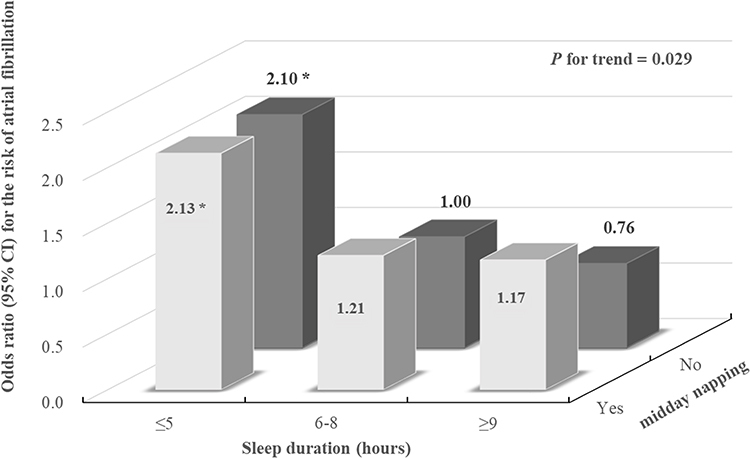 |
Figure 1 Joint effects of sleep duration and midday napping on incident AF risk. Each subgroup analysis adjusted, if not stratified, for age, sex, BMI, physical activity, smoking, drinking, SBP, DBP, duration of hypertension, diabetes mellitus, hyperlipidemia, CHD, antihypertensive agents, antidiabetes agents, lipid-lowering agents, FPG, TG, HDL-C, LDL-C, eGFR, snoring status and sleep quality (*P <0.05). |
Subgroup Analysis
A predefined subgroup analysis on the associations between sleep duration, midday napping and the risk of AF was done in the following variables: sex, age, BMI, smoking, drinking, CHD, hyperlipidemia, and diabetes mellitus. The association of the risk of AF and short sleep duration was consistent in all subgroups except for CHD (P for interaction = 0.02) (Figure 2). Moreover, the risk of AF and midday napping was consistent in all stratification subgroups (all P for interaction >0.05) (Figure 3).
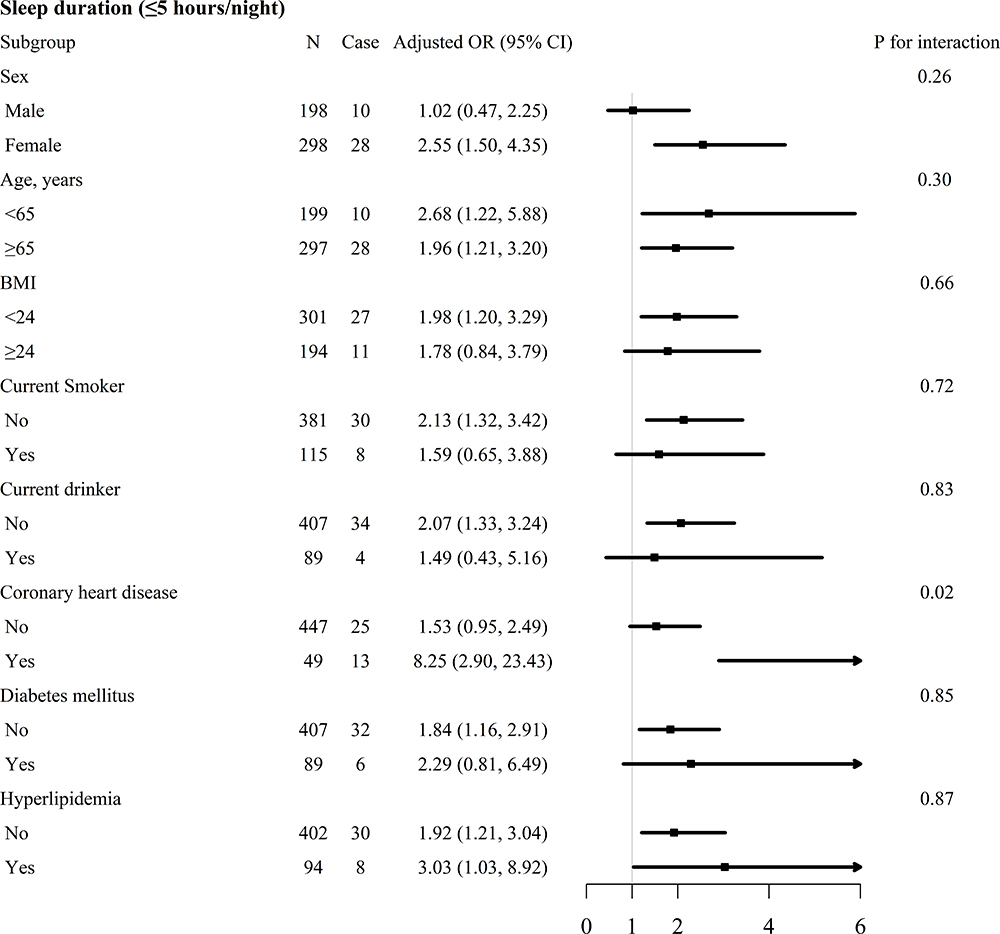 |
Figure 2 Subgroup analyses of the effect of sleep duration on incident AF risk. Each subgroup analysis adjusted, if not stratified, for age, sex, BMI, physical activity, smoking, drinking, SBP, DBP, duration of hypertension, diabetes mellitus, hyperlipidemia, CHD, antihypertensive agents, antidiabetes agents, lipid-lowering agents, FPG, TG, HDL-C, LDL-C, eGFR, snoring status, sleep quality and midday napping. |
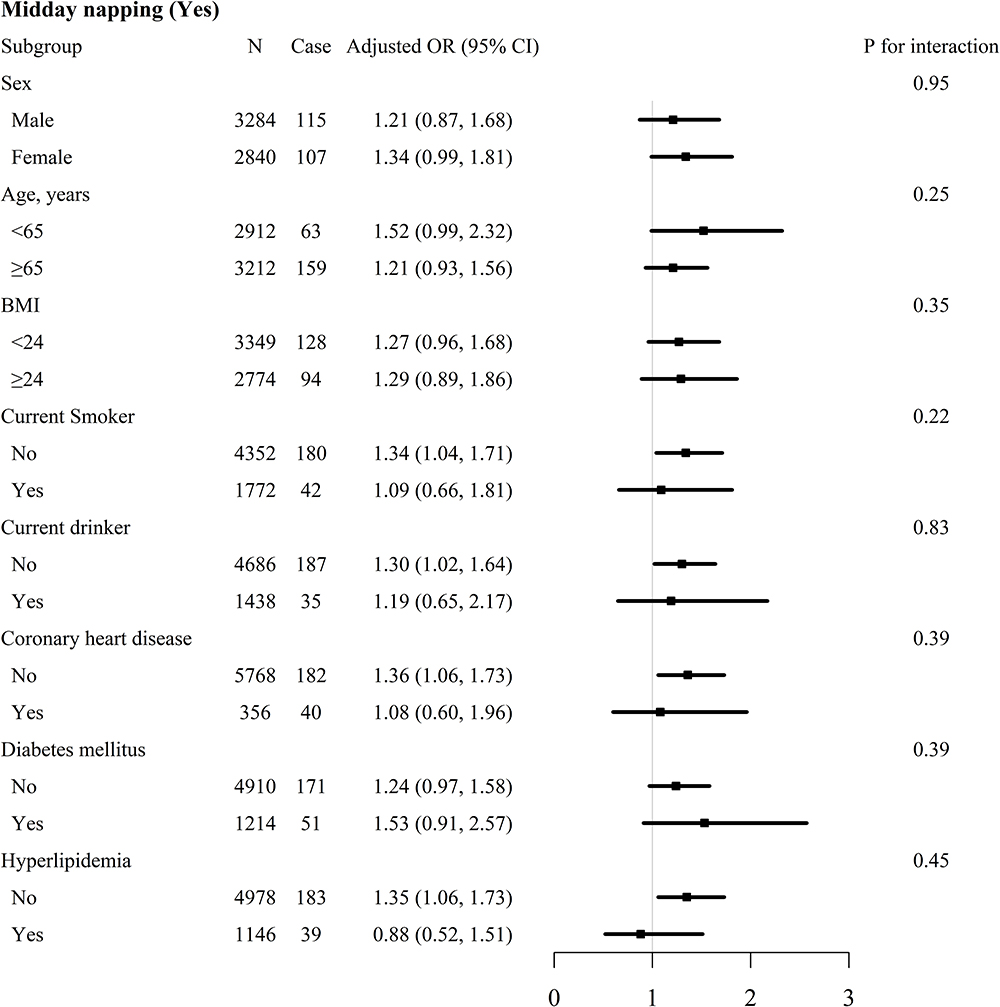 |
Figure 3 Subgroup analyses of the effect of midday napping on incident AF risk. Each subgroup analysis adjusted, if not stratified, for age, sex, BMI, physical activity, smoking, drinking, SBP, DBP, duration of hypertension, diabetes mellitus, hyperlipidemia, CHD, antihypertensive agents, antidiabetes agents, lipid-lowering agents, FPG, TG, HDL-C, LDL-C, eGFR, snoring status and sleep duration. |
Discussion
In this large cross-sectional study of the middle-aged and older hypertensive population, we examined the association between sleep duration, midday napping and the risk of AF. The main findings were that both short sleep duration (≤5 hours) and midday napping were significantly associated with higher risk of AF among patients with hypertension. Moreover, we observed significant joint effects of sleep duration and midday napping on the risk of incident AF. Furthermore, the relationships remained statistically significant after adjusting for potential confounding variables.
Several studies have reported that short sleep duration was significantly associated with higher risk of AF. Genuardi et al conducted a large observational study referred for polysomnography consisted of 31,206 subjects found that short sleep duration was associated with a 2.01-fold increased risk for current AF and a 1.44-fold increased risk for future AF.14 A Mendelian Randomization Analysis also showed that short sleep duration was associated with the higher risk of incident AF.15 However, the present findings were inconsistent with that of the study by Song et al on 87,693 participants (mean age, 50.24 years) in China.13 They found that long sleep duration (≥8 hours) was associated with incident AF during median follow-up of 7.89 years; Nevertheless, the total number of incident AF (n=322) during follow-up was comparatively low. Moreover, the Multi-Ethnic Study of Atherosclerosis indicated that sleep duration was not associated with AF risk; however, the small number of events may have limited power.27 Moreover, a longitudinal cohort study of 14 millions California residents found that insomnia was associated with a 30% to 42% higher risk of AF, supporting the concept that sleep disruption was an independent risk factor of incident AF.28 It is of note that the risk of AF with short sleep duration appeared to be more obvious in patients with CHD. It is well known that coronary artery disease was an important risk factor of incident AF.8 Thus, it is reasonable to assume that CHD might amplify the detrimental effect of short sleep duration on AF.
Several possible mechanisms may explain the relationship between short sleep duration and AF. One important biological pathway is through oxidative stress and inflammation, as previous studies have demonstrated that sleep deprivation could lead to the increase of oxidative stress and the release of inflammatory factors, which could promote the occurrence of AF.29,30 Moreover, short sleep duration and low sleep efficiency were associated with an elevated level of biomarkers of autonomic tone, additional pathways predisposing to AF.31 A cross-sectional study showed that sleep deprivation can increase QT interval and electromechanical delay in young adults, which are linked to AF.32 Short sleep duration has been demonstrated to be associated with obesity, diabetes, metabolic syndrome and myocardial infarction, all these diseases are contributed to AF incidence.16,18,19,21
We also found that midday napping was an independent risk factor for AF. To date, this is the first study to investigate the relationship between daytime napping and AF in hypertensive patients. Although the underlying mechanisms between daytime napping and AF are unclear, some epidemiologic and physiologic evidences might explain it. Midday napping is regarded as a risk factor for diabetes, CHD and metabolic syndrome,34–36 which are associated with the risk of AF. Midday napping, especially longer napping, might reflect an overall sedentary lifestyle, which is link to incident AF.36
The strength of this study was the first to evaluate the relationship between sleep duration, midday napping and AF in a large hypertension cohort. Moreover, this study stressed the importance of moderate sleep duration for AF prevention in hypertensive patients. However, several potential limitations need to be addressed in this study. First, this study was a cross-sectional design, our results cannot provide a cause and effect association between short sleep duration, midday napping and the risk of AF. Although multivariate correction, it was difficult to exclude any potential confounding effect. Second, information on sleep duration and midday napping was collected from the questionnaire, which might overestimated actual sleep duration. However, it was unrealistic to obtain objective measurements of sleep duration in a large sample population. And the method of obtaining sleep time and nap information through questionnaire has been reported in numerous studies.37,38 Third, we did not collect detailed information about nap time. Therefore, we could not perform regression analysis to clarify the association between nap duration and the risk of AF. Moreover, data about sleep apnoea was not collected, which may limit further exploration of whether this relationship could be modified by this factor. However, we collect the data about snoring, which is the the main symptom of sleep apnea. And we adjusted snoring status as a confounder in the statistical analysis. Fourth, a single assessment of sleep patterns at baseline was not satisfactory to reflect the dynamic change of sleep behaviors, which could lead to non-differential misclassification of sleep behaviors. Finally, AF was diagnosed based on electrocardiogram and medical record in this study, without ambulatory electrocardiogram monitoring. Therefore, AF incidence can be underestimated due to electrocardiogram could not capture paroxysmal AF. However, inaccuracy of ascertainment of AF would also tend to bias findings toward the null hypothesis.
Conclusion
In this large cross-sectional study, we found that short sleep duration and midday napping were independently and jointly associated with higher risks of AF in patients with hypertension. Further research is needed to confirm our results in external populations and identify the potential mechanisms of the relationship.
Data Sharing Statement
The data are not publicly available due to privacy or ethical restrictions.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institute of Biomedicine, Anhui Medical University, Hefei, China. Informed written consent was obtained from all patients before their enrollment in this study.
Acknowledgments
We acknowledge the contribution of all staff who participated in this study as well as the study participants who shared their time with us. Yurong Xiong and Yun Yu are co-first authors for this study.
Funding
This work was supported by the Jiangxi Science and Technology Innovation Platform Project (20165BCD41005), Fund project of the Second Affiliated Hospital of Nanchang University (2016YNQN12034, 2019YNLZ12010, IIT-I-2021-00).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation. 2020;141:e139–596. doi:10.1161/CIR.0000000000000757
2. Guo Y, Tian Y, Wang H, Si Q, Wang Y, Lip GYH. Prevalence, incidence, and lifetime risk of atrial fibrillation in China. Chest. 2015;147:109–119. doi:10.1378/chest.14-0321
3. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137:263–272. doi:10.1378/chest.09-1584
4. Stewart S, Hart CL, Hole DJ, McMurray JJ. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am J Med. 2002;113:359–364. doi:10.1016/S0002-9343(02)01236-6
5. Miyasaka Y, Barnes ME, Gersh BJ, et al. Coronary ischemic events after first atrial fibrillation: risk and survival. Am J Med. 2007;120:357–363. doi:10.1016/j.amjmed.2006.06.042
6. Bansal N, Fan D, Hsu CY, Ordonez JD, Marcus GM, Go AS. Incident atrial fibrillation and risk of end-stage renal disease in adults with chronic kidney disease. Circulation. 2013;127:569–574. doi:10.1161/CIRCULATIONAHA.112.123992
7. Miyasaka Y, Barnes ME, Bailey KR, et al. Mortality trends in patients diagnosed with first atrial fibrillation: a 21-year community-based study. J Am Coll Cardiol. 2007;49:986–992. doi:10.1016/j.jacc.2006.10.062
8. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2021;42:373–498. doi:10.1093/eurheartj/ehaa612
9. Schnabel RB. Can we predict the occurrence of atrial fibrillation? Clin Cardiol. 2012;35(Suppl 1):5–9. doi:10.1002/clc.20963
10. Perez MV, Wang PJ, Larson JC, et al. Risk factors for atrial fibrillation and their population burden in postmenopausal women: the women’s health initiative observational study. Heart. 2013;99:1173–1178. doi:10.1136/heartjnl-2013-303798
11. Benjamin EJ, Levy D, Vaziri SM, D’Agostino RB, Belanger AJ, Wolf PA. Independent risk factors for atrial fibrillation in a population-based cohort. The Framingham heart study. JAMA. 1994;271:840–844. doi:10.1001/jama.1994.03510350050036
12. Khawaja O, Sarwar A, Albert CM, Gaziano JM, Djoussé L. Sleep duration and risk of atrial fibrillation (from the Physicians’ health study). Am J Cardiol. 2013;111:547–551. doi:10.1016/j.amjcard.2012.10.038
13. Song Q, Liu X, Hu W, et al. Long sleep duration is an independent risk factor for incident atrial fibrillation in a Chinese population: a prospective cohort study. Sci Rep UK. 2017;7. 1–7.
14. Genuardi MV, Ogilvie RP, Saand AR, et al. Association of short sleep duration and atrial fibrillation. Chest. 2019;156:544–552. doi:10.1016/j.chest.2019.01.033
15. Zhao J, Yang F, Zhuo C, et al. Association of sleep duration with atrial fibrillation and heart failure: a Mendelian randomization analysis. Front Genet. 2021;12. 193.
16. Yang L, Xu Z, He M, et al. Sleep duration and midday napping with 5-year incidence and reversion of metabolic syndrome in middle-aged and older Chinese. Sleep. 2016;39:1911–1918. doi:10.5665/sleep.6214
17. Shan Z, Ma H, Xie M, et al. Sleep duration and risk of type 2 diabetes: a meta-analysis of prospective studies. Diabetes Care. 2015;38:529–537. doi:10.2337/dc14-2073
18. Lawman HG, D. Fryar C, Gu Q, Ogden CL. The role of prescription medications in the association of self-reported sleep duration and obesity in U.S. adults, 2007–2012. Obesity. 2016;24:2210–2216. doi:10.1002/oby.21600
19. Gottlieb DJ, Redline S, Nieto FJ, et al. Association of usual sleep duration with hypertension: the Sleep Heart Health Study. Sleep. 2006;29:1009–1014. doi:10.1093/sleep/29.8.1009
20. van den Berg JF, Miedema HM, Tulen JH, et al. Long sleep duration is associated with serum cholesterol in the elderly: the Rotterdam study. Psychosom Med. 2008;70:1005–1011. doi:10.1097/PSY.0b013e318186e656
21. Wang X, Liu X, Song Q, Wu S. Sleep duration and risk of myocardial infarction and all-cause death in a Chinese population: the Kailuan study. Sleep Med. 2016;19:13–16. doi:10.1016/j.sleep.2015.09.027
22. Kallistratos MS, Poulimenos LE, Manolis AJ. Atrial fibrillation and arterial hypertension. Pharmacol Res. 2018;128:322–326. doi:10.1016/j.phrs.2017.10.007
23. Xiong Y, Wangsheng F, Wang S, et al. Positive association between body fat percentage and hyperuricemia in patients with hypertension: the China H-type hypertension registry study. Nutr Metab Cardiovasc Dis. 2021;31(11):3076–3084. doi:10.1016/j.numecd.2021.07.002
24. Li M, Zhan A, Huang X, et al. Positive association between triglyceride glucose index and arterial stiffness in hypertensive patients: the China H-type Hypertension Registry Study. Cardiovasc Diabetol. 2020;19. doi:10.1186/s12933-020-01124-2
25. Vgontzas AN, Zoumakis E, Bixler EO, et al. Adverse effects of modest sleep restriction on sleepiness, performance, and inflammatory cytokines. J Clin Endocrinol Metab. 2004;89:2119–2126. doi:10.1210/jc.2003-031562
26. Washio M, Kobashi G, Okamoto K, et al. Sleeping habit and other life styles in the prime of life and risk for ossification of the posterior longitudinal ligament of the spine (OPLL): a case-control study in Japan. J Epidemiol. 2004;14:168–173. doi:10.2188/jea.14.168
27. Kwon Y, Gharib SA, Biggs ML, et al. Association of sleep characteristics with atrial fibrillation: the multi-ethnic study of atherosclerosis. Thorax. 2015;70:873–879. doi:10.1136/thoraxjnl-2014-206655
28. Christensen MA, Dixit S, Dewland TA, et al. Sleep characteristics that predict atrial fibrillation. Heart Rhythm. 2018;15:1289–1295. doi:10.1016/j.hrthm.2018.05.008
29. Kanagasabai T, Ardern CI. Contribution of inflammation, oxidative stress, and antioxidants to the relationship between sleep duration and cardiometabolic health. Sleep. 2015;38:1905–1912. doi:10.5665/sleep.5238
30. Hu YF, Chen YJ, Lin YJ, Chen SA. Inflammation and the pathogenesis of atrial fibrillation. Nat Rev Cardiol. 2015;12:230–243. doi:10.1038/nrcardio.2015.2
31. Castro-Diehl C, Diez Roux AV, Redline S, et al. Sleep duration and quality in relation to autonomic nervous system measures: the multi-ethnic study of atherosclerosis (Mesa). Sleep. 2016;39:1927–1940. doi:10.5665/sleep.6218
32. Ö ESEN, Akçakoyun M, Açar G, et al. Acute sleep deprivation is associated with increased atrial electromechanical delay in healthy young adults. Pacing Clin Electrophysiol. 2011;34:1645–1651. doi:10.1111/j.1540-8159.2011.03186.x
33. Zheng R, Niu J, Wu S, et al. Gender and age differences in the association between sleep characteristics and fasting glucose levels in Chinese adults. Diabetes Metab. 2021;47:101174. doi:10.1016/j.diabet.2020.07.001
34. Yamada T, Hara K, Shojima N, Yamauchi T, Kadowaki T. Daytime napping and the risk of cardiovascular disease and all-cause mortality: a prospective study and dose-response meta-analysis. Sleep. 2015;38:1945–1953. doi:10.5665/sleep.5246
35. Pan Z, Huang M, Huang J, Yao Z, Lin Z. Association of napping and all-cause mortality and incident cardiovascular diseases: a dose-response meta analysis of cohort studies. Sleep Med. 2020;74:165–172. doi:10.1016/j.sleep.2020.08.009
36. Ford ES, Caspersen CJ. Sedentary behaviour and Cardiovascular disease: a review of prospective studies. Int J Epidemiol. 2012;41:1338–1353. doi:10.1093/ije/dys078
37. Gale C, Martyn C. Larks and owls and health, wealth, and wisdom. BMJ. 1998;317:1675–1677. doi:10.1136/bmj.317.7174.1675
38. Lan TY, Lan TH, Wen CP, Lin YH, Chuang YL. Nighttime sleep, Chinese afternoon nap, and mortality in the elderly. Sleep. 2007;30:1105–1110. doi:10.1093/sleep/30.9.1105
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.