")
Back to Journals » International Journal of General Medicine » Volume 13
Association of Serum Levels of Vitamin D with Blood Pressure Status in Northern Iranian Population: The PERSIAN Guilan Cohort Study (PGCS)
Authors Joukar F, Naghipour M, Hassanipour S, Salari A, Alizadeh A, Saeidi-Saedi H, Mansour-Ghanaei F
Received 1 January 2020
Accepted for publication 20 February 2020
Published 11 March 2020 Volume 2020:13 Pages 99—104
DOI https://doi.org/10.2147/IJGM.S244472
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Farahnaz Joukar,1,2,* Mohammadreza Naghipour,1,* Soheil Hassanipour,1,2 Arsalan Salari,3 Ahmad Alizadeh,4 Hamid Saeidi-Saedi,2 Fariborz Mansour-Ghanaei1,2,4
1Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Rasht, Iran; 2GI Cancer Screening and Prevention Research Center, Guilan University of Medical Sciences, Rasht, Iran; 3Department of Cardiology, Cardiovascular Diseases Research Center, Heshmat Hospital, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran; 4Caspian Digestive Disease Research Center, Guilan University of Medical Sciences, Rasht, Iran
*These authors contributed equally to this work
Correspondence: Fariborz Mansour-Ghanaei
Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Razi Hospital, Sardar-Jangle Ave., P.O. Box: 41448-95655, Rasht, Iran
Tel +98-1315535116
Fax +98-1315534951
Email [email protected]
Background: Evidence in the last decades has indicated an association between vitamin D and cardiovascular risk factors including blood pressure. The present study aimed to determine whether serum 25-hydroxyvitamin D is independently associated with blood pressure in a large population-based study.
Methods: The study was based on subjects from PERSIAN Guilan Cohort Study (PGCS), a prospective, population-based cohort study in Guilan, Iran. In 9520 men and women, aged 35– 70 years, serum 25-hydroxyvitamin D, systolic and diastolic blood pressure were measured. Multiple logistic and linear regression analyses were conducted with adjustments for demographic factors (age and gender), anthropometric characteristics (waist circumference and body mass index), lifestyle variables (physical activity, alcohol, and smoking consumption), and renal function (serum creatinine).
Results: Fully adjusted linear regression analyses revealed a weak but statistically significant negative association between serum 25-hydroxyvitamin D levels and systolic blood pressure (β = – 0.02, 95% CI= − 0.052 to − 0.0001, P-value=0.04), whereas vitamin D status was not significantly associated with diastolic blood pressure (β = – 0.01, 95% CI= − 0.026 to 0.009, P-value=0.3). Serum 25-hydroxyvitamin D status showed no significant association with the presence of hypertension (OR 1.09, 95% CI=0.94 to 1.25 for the lowest (25OHD < 12 ng/mL) versus the highest (25OHD ≥ 20 ng/mL) category).
Conclusion: Lower serum vitamin 25 (OH) D levels were associated with higher systolic blood pressure; however, it was not associated with diastolic blood pressure and presence of hypertension.
Keywords: vitamin D, blood pressure, Guilan cohort study, Iran
Introduction
Vitamin D deficiency is prevalent in the Islamic Republic of Iran.1 Vitamin D has been known to maintaining bone health and mineral homeostasis for many decades, but recent research has shown that vitamin D receptors are present on a wide range of tissues, including the myocardium and the endothelium, proposing a much wider variety of physiological functions for vitamin.2–4
Clinical and epidemiological evidence in the last decades has indicated an association between vitamin D and cardiovascular risk factors including blood pressure.5,6 Evidence demonstrates that vitamin D may regulate blood pressure by direct vascular effect via vitamin D receptors on endothelial cells,7 and regulating the renin-angiotensin system via effects on the juxtaglomerular apparatus.8,9
Most observational studies found that low serum vitamin D levels are associated with the risk of hypertension,10 and with higher rates of cardiovascular events11 and increased mortality rates,12,13 but this relationship disappeared after adjustment for confounding factors in some studies.14 Although interventional studies have suggested that vitamin D supplementation may reduce mortality,15 recent systematic reviews and meta-analysis on the effects of vitamin D supplementation on blood pressure reduction found weak evidence to support a small blood pressure lowering effects of vitamin D and thus advised against using as an antihypertensive agent.16,17
However, the association of vitamin D and blood pressure (BP) has been explored in previous studies, but the results are conflicting may be due to small sample sizes, study populations heterogeneity, and methodological differences. Thus, the present study was conducted to determine if the associations between blood pressure and vitamin D could be found in a large population-based study based on data from The PERSIAN Guilan Cohort Study (PGCS), a prospective, population-based cohort study in Guilan, Iran.
Materials and Methods
Study Population
The PERSIAN Guilan Cohort Study (PGCS) is a prospective, population-based cohort study in Guilan, the northern province of Iran, recruited between October 8, 2014, and January 20, 2017, as part of the Prospective Epidemiological Research Studies in Iran (PERSIAN).18 The Climate of Guilan province based on the Köppen Climate Classification was humid subtropical climate and its Biotope was Forests and woodland.19 There was one predominant ethnic group in this province, that was Gilaci20. Different districts of the province were chosen to include different socioeconomic status levels including urban areas and 39 villages. This area was selected due to its long-term population stability, high population density, a relative similarity in demographic and behavioral characteristics. The sampling and data collection methods have been previously described in detail.20,21 In total, 9520 persons (aged 35–70 years) participated in the study. The study was approved by the local ethical committee and written informed consent was obtained from all participants.18
Data Collection
Measurement of Vitamin D
Blood samples were collected from all individuals using Vacutainers (Greiner Bio-One International GmbH, Kremsmunster, Austria). Whole blood samples were collected in EDTA (K3) tubes (Becton Dickinson, France). Serum 25-Hydroxyl vitamin D was determined by using a commercially available electrochemiluminescence immunoassay with Roche Elecsys 2010 and Cobas E411 auto analyzer (Roche Diagnostics GmbH, Mannheim, Germany).
A level that was less than 12 ng/mL (30 nmol/L) was defined as vitamin D deficiency, 12 to 20 ng/mL (50 nmol/L) was defined as vitamin D insufficiency (≥20 defined as vitamin D sufficiency) and greater than 100 ng/mL (250 nmol/mL) was defined as vitamin D toxicity.22
Measurement of Blood Pressure
Blood pressure (mmHg) was measured after 10-min rest period twice in the right arm with participants in a seated position, back supported and legs uncrossed in a quiet room after 10-min intervals, using Richter auscultatory mercury sphygmomanometers (MTM Munich, Germany).20 The mean of the two measurements was used in the analyses.
Hypertension was defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg and/or a prior diagnosis of hypertension by a health professional or current use of antihypertensive drugs.18
Other Measurements
Information on potential confounding factors that may affect vitamin D status and Blood pressure and their association were collected. These variables were included demographic factors (age and gender), anthropometric characteristics, lifestyle variables (physical activity, alcohol, and smoking consumption), and renal function.
Anthropometric characteristics including weight (kg), height (cm), waist circumferences (cm) are measured using US National Institutes of Health protocols and have been previously described in detail.20
Smoking status was categorized as nonsmoker or current smoker (tobacco, cigarettes, hookah, cigar, and pipe), and alcohol consumption was classified as none or current use. The level of physical activity was estimated by metabolic equivalent rates (METs) of self-reported daily activities of participants that have been previously described in detail.23 Renal impairment was assessed by serum creatinine (µmol L).
Ethical Consideration
The present study was approved by Ethics Committee of Guilan University of Medical Sciences
(Ethic code: IR.GUMS.REC.1397.129)
Statistical Analyses
Differences in Characteristics of the participants according to the vitamin D status (sufficient, deficiency, insufficiency) were analyzed using the chi-square test and ANOVA followed by a Bonferroni. Multiple linear regression analyses were performed to assess the associations between systolic or diastolic blood pressure (dependent variables) and vitamin D levels (independent variables). In addition, we used categorical vitamin D status to detect possible nonlinear relations. Logistic regression analyses were used to evaluate the associations between vitamin D status (independent variables) and the presence of hypertension (dependent variable). All regression analyses were adjusted for potential confounding by demographic factors (age and gender), anthropometric characteristics (waist circumference and BMI), lifestyle variables (physical activity, alcohol, and smoking consumption), and renal function (serum creatinine)
All analyses were performed with the use of SPSS version 16.0 (SPSS Inc., Chicago, IL, USA). A P-value of less than 0.05 was considered significant.
Results
A total of 9520 women and men aged 35 years to 70 were included in this study. The mean age of the study population was 51.45 ± 8.9 years and 46.5% of participants were men. About 45.7% of individuals were from urban areas. Forty-eight percent of the study participants were educated in high school or less. The mean serum 25-Hydroxyl vitamin D concentration of participants was 21.75 ± 12.3 ng/mL in the study population. Characteristics of the study population according to 25-hydroxyvitamin D level are shown in Table 1. Vitamin D deficiency and insufficiency were found in 20.6% and 29% of subjects, respectively. Participants with vitamin D deficiency were younger, less educated, more likely to be women and rural residence, had a higher BMI and Waist circumference, and were less physically active.
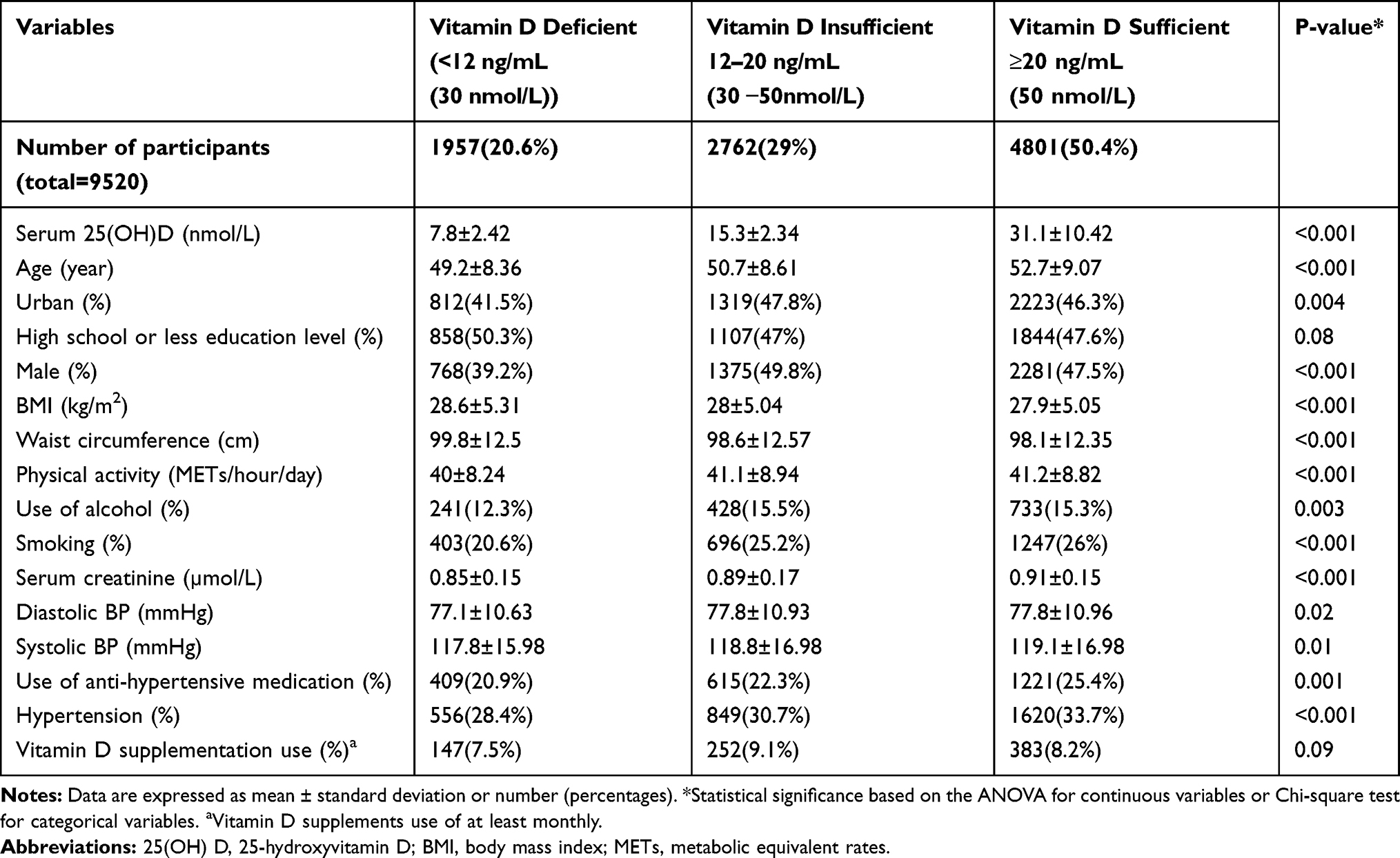 |
Table 1 Characteristics of Study Population According to Serum 25-Hydroxyl Vitamin D Levels |
The assessment of the associations between systolic or diastolic blood pressure and Serum 25-Hydroxyl vitamin D levels by multiple linear regression analyses have shown serum 25OHD levels were not statistically significantly associated with diastolic blood pressure unadjusted and after adjustment for potential confounders (Table 2). In contrast, higher 25OHD levels were associated with higher systolic blood pressure, and this association reversed and remained statistically significant after adjustment for demographic factors, anthropometric characteristics, lifestyle variables, renal function, and anti-hypertensive medication or vitamin D supplementation (Table 2). Fully adjusted regression coefficients for 25OHD in relation to systolic blood pressure were −0.02 (P value= 0.04), it means an increase in serum 25OHD of 1 nmol/L was associated with a 0.02 mmHg decrease in systolic blood pressure (Table 2).
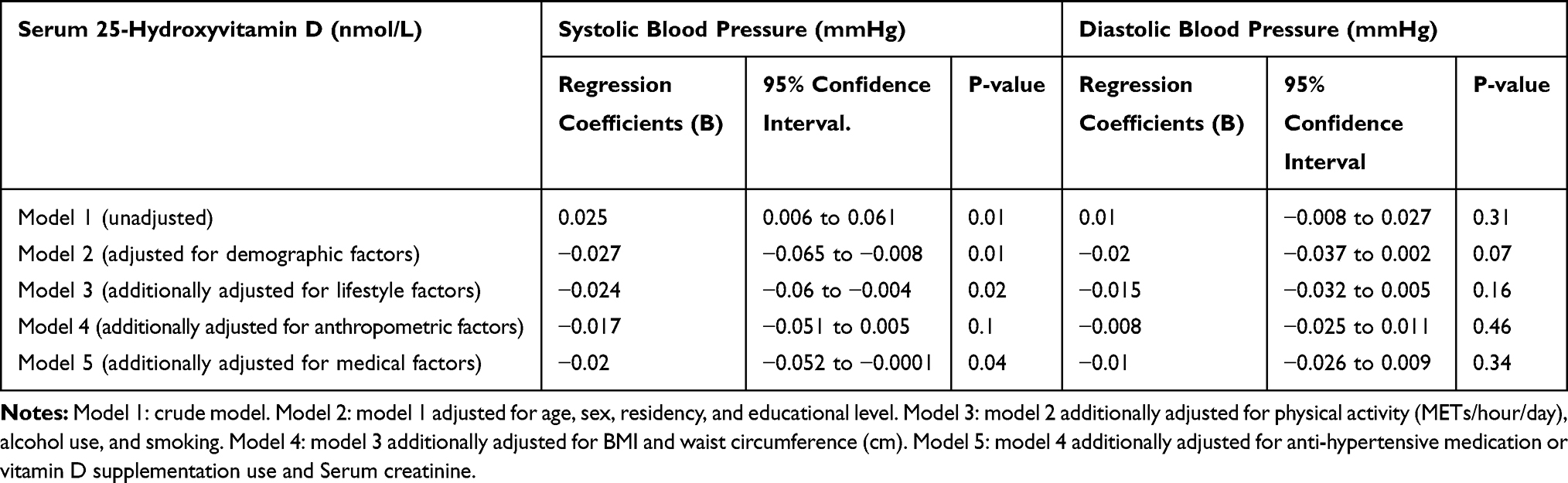 |
Table 2 Associations of Serum 25-Hydroxyvitamin D with Systolic and Diastolic Blood Pressure from Linear Regression Analysis |
Thirty-one percent of the study population had hypertension. Non-linear association between vitamin D status and the presence of hypertension evaluated with Logistic regression analyses (Table 3). There was no significantly Non-linear association between Serum 25OHD status and the presence of hypertension in unadjusted logistic regression analyses and after adjustment for potential confounders (Table 3).
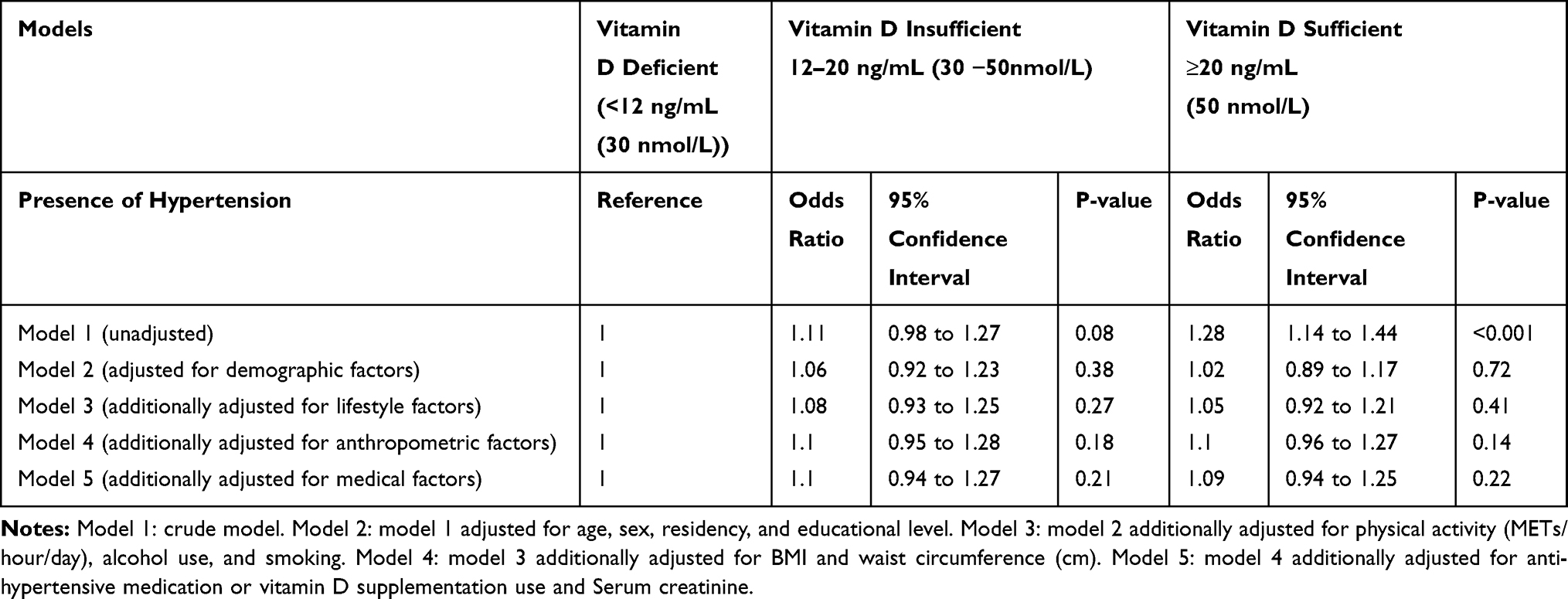 |
Table 3 Associations of 25-Hydroxyvitamin D Status with the Presence of Hypertension Using Logistic Regression Analysis |
Discussion
In this population-based study of 9520 women and men, there was a weak but statistically significant negative association between serum 25-hydroxyvitamin D levels and systolic blood pressure, which an increase in serum 25OHD of 1 nmol/L was associated with a 0.02 mmHg decrease in systolic blood pressure.
The observed association between serum 25-hydroxyvitamin vitamin D levels and systolic blood pressure is consistent with other studies finding.24–27 The underlying mechanisms are maybe a potent endocrine suppressor effect of vitamin D on renin biosynthesis to regulate the renin-angiotensin system.28 In addition, the vitamin D receptors (VDR) lacking in Mice have elevated renin and angiotensin II production, leading to hypertension.29 On the other hand, vitamin D is indirectly associated with blood pressure due to the role in the regulation of calcium absorption from the gut17 and in the maintenance of calcium homeostasis via interaction with parathyroid hormone.30 Interestingly, vitamin D seems to reduce free radicals local production, with benefits on vascular health.31,32 However, this association may be confounding by UVA irradiation, as shown in a study that UVA irradiation of human skin was associated with a significant drop in blood pressure.33
In contrast, in the current study, vitamin D status was not significantly related to diastolic blood pressure. The evidence of evaluating the effectiveness of vitamin D supplementation in blood pressure reduction from a systematic review and meta-analyses of the randomized controlled trials have provided evidence of a small but statistically significant reduction in systolic blood pressure but not diastolic blood pressure34 that was agreed with the present study’s findings. The lack of association between serum vitamin D level and diastolic blood pressure in the present study was consistent with results in previous observational studies.35 Also, no significant correlations were obtained between vitamin D level and blood pressure variables in a previous study including middle-aged hypertensive and high normal blood pressure patients.36
The current study revealed that Serum 25OHD status was not significantly related to the presence of hypertension. This result is broadly in line with those of previous studies,37,38 although they contrast with the small association between Serum 25OHD status and presence of hypertension in some previous studies.10,39 However, our analysis includes a much larger sample size than previous studies and controls potential confounders by advance analyses.
Limitations of This Study
Cross-sectional design was the limitation of the current study, which did not permit us to determine the order of events. Also, we cannot completely exclude residual confounders, despite our detailed adjustment for confounding because our study was not randomized.
Conclusion
In conclusion, the present population-based study demonstrated that lower serum vitamin 25 (OH) D levels were associated with higher systolic blood pressure; however, it was not associated with diastolic blood pressure and presence of hypertension. These findings must be confirmed in cohort studies and randomized clinical trials. The possible implication of the present study for clinical practice was special attention to serum vitamin D levels in hypertensive patients.
Acknowledgments
This study was supported financially by Guilan University of Medical Sciences, Rasht, Iran. (Ethic code: IR.GUMS.REC.1397.129)
Disclosure
The authors report no conflicts of interest in this work.
References
1. Heshmat R, Mohammad K, Majdzadeh S, Forouzanfar M, Bahrami A, Ranjbar Omrani G. Vitamin D deficiency in Iran: a multi-center study among different urban areas. Iran J Public Health. 2008;37(1):72–78.
2. Suda T, Masuyama R, Bouillon R, Carmeliet G. Physiological functions of vitamin D: what we have learned from global and conditional VDR knockout mouse studies. Curr Opin Pharmacol. 2015;22:87–99. doi:10.1016/j.coph.2015.04.001
3. Khammissa R, Fourie J, Motswaledi M, Ballyram R, Lemmer J, Feller L. The biological activities of vitamin D and its receptor in relation to calcium and bone homeostasis, cancer, immune and cardiovascular systems, skin biology, and oral health. Biomed Res Int. 2018;2018:9.
4. Bhatt N, Ali A, Waly M. Non-skeletal benefits of vitamin D. Can J Clin Nutr. 2019;7(1):141–159. doi:10.14206/canad.j.clin.nutr.2019.01.12
5. Pilz S, Verheyen N, Grübler MR, Tomaschitz A, März W. Vitamin D and cardiovascular disease prevention. Nat Rev Cardiol. 2016;13(7):404. doi:10.1038/nrcardio.2016.73
6. Censani M, Hammad HT, Christos PJ, Schumaker T. Vitamin D deficiency associated with markers of cardiovascular disease in children with obesity. Glob Pediatr Health. 2018;5:2333794X17751773. doi:10.1177/2333794X17751773
7. Ni W, Watts SW, Ng M, Chen S, Glenn DJ, Gardner DG. Elimination of vitamin D receptor in vascular endothelial cells alters vascular function. Hypertension. 2014;64(6):1290–1298. doi:10.1161/HYPERTENSIONAHA.114.03971
8. Li YC. Vitamin D and the renin-angiotensin system. Vitamin D. 2018:825–847. Elsevier.
9. Turin A, Bax JJ, Doukas D, et al. Interactions among vitamin D, atrial fibrillation, and the renin-angiotensin-aldosterone system. Am J Cardiol. 2018;122(5):780–784. doi:10.1016/j.amjcard.2018.05.013
10. Afzal S, Nordestgaard BG. Vitamin D, hypertension, and ischemic stroke in 116 655 individuals from the general population: a genetic study. Hypertension. 2017;70(3):499–507. doi:10.1161/HYPERTENSIONAHA.117.09411
11. Mozos I, Marginean O. Links between vitamin D deficiency and cardiovascular diseases. Biomed Res Int. 2015;2015:12.
12. Gaksch M, Jorde R, Grimnes G, et al. Vitamin D and mortality: individual participant data meta-analysis of standardized 25-hydroxyvitamin D in 26916 individuals from a European consortium. PLoS One. 2017;12(2):e0170791. doi:10.1371/journal.pone.0170791
13. Trongtrakul K, Feemuchang C. Prevalence and association of vitamin D deficiency and mortality in patients with severe sepsis. Int J Gen Med. 2017;10:415–421. doi:10.2147/IJGM.S147561
14. Grübler MR, März W, Pilz S, et al. Vitamin-D concentrations, cardiovascular risk and events-a review of epidemiological evidence. Rev Endocr Metab Disord. 2017;18(2):259–272. doi:10.1007/s11154-017-9417-0
15. Witham MD, Nadir MA, Struthers AD. Effect of vitamin D on blood pressure: a systematic review and meta-analysis. J Hypertens. 2009;27(10):1948–1954.
16. Beveridge LA, Struthers AD, Khan F, et al. Effect of vitamin D supplementation on blood pressure: a systematic review and meta-analysis incorporating individual patient data. JAMA Intern Med. 2015;175(5):745–754. doi:10.1001/jamainternmed.2015.0237
17. Wu L, Sun D. Effects of calcium plus vitamin D supplementation on blood pressure: a systematic review and meta-analysis of randomized controlled trials. J Hum Hypertens. 2017;31(9):547. doi:10.1038/jhh.2017.12
18. Mansour-Ghanaei F, Joukar F, Naghipour MR, et al. The PERSIAN Guilan Cohort study (PGCS). Arch Iran Med. 2019;22:1.
19. Climate-Data.org. Climate: Iran. Available from: https://en.climate-data.org/country/66/.
20. Poustchi H, Eghtesad S, Kamangar F, et al. Prospective epidemiological research studies in Iran (the PERSIAN Cohort Study): rationale, objectives, and design. Am J Epidemiol. 2017;187(4):647–655. doi:10.1093/aje/kwx314
21. Eghtesad S, Mohammadi Z, Shayanrad A, et al. The PERSIAN cohort: providing the evidence needed for healthcare reform. Arch Iran Med. 2017;20(11):691.
22. Giustina A, Adler RA, Binkley N, et al. Controversies in vitamin D: summary statement from an international conference. J Clin Endocrinol Metab. 2019;104(2):234–240. doi:10.1210/jc.2018-01414
23. Karyani AK, Matin BK, Soltani S, et al. Socioeconomic gradient in physical activity: findings from the PERSIAN cohort study. BMC Public Health. 2019;19(1):1312. doi:10.1186/s12889-019-7715-z
24. Van Ballegooijen AJ, Cepelis A, Visser M, Brouwer IA, Van Schoor NM, Beulens JW. Joint association of low vitamin D and vitamin K status with blood pressure and hypertension. Hypertension. 2017;69(6):1165–1172. doi:10.1161/HYPERTENSIONAHA.116.08869
25. Kim J. Association between serum vitamin D, parathyroid hormone and metabolic syndrome in middle-aged and older Korean adults. Eur J Clin Nutr. 2015;69(4):425. doi:10.1038/ejcn.2014.192
26. Zaleski A, Taylor B, Armstrong B, et al. Associations of 25-hydroxyvitamin D with the blood pressure response to maximal exercise among healthy adults. Int J Sport Nutr Exerc Metab. 2019;29(3):303–308. doi:10.1123/ijsnem.2017-0424
27. Moreira JSR, de Paula TP, Sperb LF, Miller MEP, Azevedo MJ, Viana LV. Association of plasma vitamin D status with lifestyle patterns and ambulatory blood pressure monitoring parameters in patients with type 2 diabetes and hypertension. Diabetes Res Clin Pract. 2018;139:139–146. doi:10.1016/j.diabres.2018.02.038
28. McMullan CJ, Borgi L, Curhan GC, Fisher N, Forman JP. The effect of vitamin D on renin-angiotensin-system activation and blood pressure-a randomized control trial. J Hypertens. 2017;35(4):822. doi:10.1097/HJH.0000000000001220
29. Martorell S, Hueso L, Gonzalez-Navarro H, Collado A, Sanz M-J, Piqueras L. Vitamin D receptor activation reduces angiotensin-II–induced dissecting abdominal aortic aneurysm in apolipoprotein E–knockout mice. Arterioscler Thromb Vasc Biol. 2016;36(8):1587–1597. doi:10.1161/ATVBAHA.116.307530
30. Vimaleswaran KS, Cavadino A, Berry DJ, et al. Association of vitamin D status with arterial blood pressure and hypertension risk: a mendelian randomisation study. Lancet Diabetes Endocrinol. 2014;2(9):719–729. doi:10.1016/S2213-8587(14)70113-5
31. Valcheva P, Cardus A, Panizo S, et al. Lack of vitamin D receptor causes stress-induced premature senescence in vascular smooth muscle cells through enhanced local angiotensin-II signals. Atherosclerosis. 2014;235(2):247–255. doi:10.1016/j.atherosclerosis.2014.05.911
32. Del Pinto R, Ferri C. Inflammation-accelerated senescence and the cardiovascular system: mechanisms and perspectives. Int J Mol Sci. 2018;19:12. doi:10.3390/ijms19123701
33. Opländer C, Volkmar CM, Paunel-Görgülü A, et al. Whole body UVA irradiation lowers systemic blood pressure by release of nitric oxide from intracutaneous photolabile nitric oxide derivates. Circ Res. 2009;105(10):1031–1040. doi:10.1161/CIRCRESAHA.109.207019
34. Wu SH, Ho SC, Zhong L. Effects of vitamin D supplementation on blood pressure. South Med J. 2010;103(8):729–737. doi:10.1097/SMJ.0b013e3181e6d389
35. Kheirouri S, Mohajeri M, Avesta L. Association of vitamin D with blood pressure and obesity in prinzmetal angina. Prog Nutr. 2019;21(1–S):173–177.
36. Mozos I, Jianu D, Gug C, Stoian D. Links between high-sensitivity C-reactive protein and pulse wave analysis in middle-aged patients with hypertension and high normal blood pressure. Dis Markers. 2019;2019;(3):1–9.
37. Snijder M, Lips P, Seidell J, et al. Vitamin D status and parathyroid hormone levels in relation to blood pressure: a population‐based study in older men and women. J Intern Med. 2007;261(6):558–565. doi:10.1111/jim.2007.261.issue-6
38. Chen S, Sun Y, Agrawal DK. Vitamin D deficiency and essential hypertension. J Am Soc Hypertens. 2015;9(11):885–901. doi:10.1016/j.jash.2015.08.009
39. Ke L, Mason RS, Kariuki M, Mpofu E, Brock KE. Vitamin D status and hypertension: a review. Integr Blood Press Control. 2015;8:13.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.