")
Back to Journals » Journal of Asthma and Allergy » Volume 15
Association of Interleukin 13 rs20541 Gene Polymorphism and Serum Periostin with Asthma and Allergic Conjunctivitis Among Egyptian Patients
Authors Hafez RA , Hassan ME, Haggag MG, Atef N, Abdallah AL, Gerges MA
Received 2 May 2022
Accepted for publication 15 July 2022
Published 26 July 2022 Volume 2022:15 Pages 971—982
DOI https://doi.org/10.2147/JAA.S373098
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Raghda Abdellatif Hafez,1 Manar E Hassan,2 Maha G Haggag,2 Nora Atef,3 Alshimaa L Abdallah,1 Marian A Gerges1
1Medical Microbiology and Immunology Department, Faculty of Medicine, Zagazig University, Zagazig, Egypt; 2Microbiology, Immunology and Parasitology Department, Research Institute of Ophthalmology, Giza, Egypt; 3Cancer Epidemiology and Biostatistics Department, National Cancer Institute, Cairo University, Cairo, Egypt
Correspondence: Marian A Gerges, Medical Microbiology and Immunology Department, Faculty of Medicine, Zagazig University, Zagazig, 44519, Egypt, Tel +2 01003819530, Email [email protected]
Background: Single nucleotide polymorphisms (SNPs) in the interleukin 13 (IL13) gene are associated with vulnerability to allergic diseases, such as asthma and allergic conjunctivitis (AC). Periostin, as an IL13-induced protein, has emerged as a novel biomarker in several allergic diseases. Data among Egyptian patients are still scarce.
Aim: To find out the association of IL13 rs20541 gene polymorphism and serum levels of periostin with asthma and AC among Egyptian patients.
Patients and Methods: Eighty-one Egyptian allergic patients with asthma, AC, and both asthma and AC (27 each), were enrolled in this case–control study. Twenty-seven age and gender-matched healthy volunteers served as controls. All participants were tested for IL13 rs20541 SNP by real-time polymerase chain reaction, TaqMan method. Serum levels of periostin and IL13 were assessed by ELISA.
Results: Compared to healthy subjects, asthmatic patients had a higher frequency of the homozygous adenine/adenine (AA) genotype at IL13 rs20541 SNP (14.8% vs 3.7%) and a lower frequency of the guanosine/guanosine (GG) genotype (51.9% vs 55.6%), while AC patients had higher GG genotype (70.4% vs 55.6%) with no AA genotype detected, yet no significant difference was noticed (p = 7.053). A significantly higher serum periostin in asthmatic patients compared to controls was found (p = 0.005). Higher levels of serum periostin, although nonsignificant, were recorded in AC patients compared to controls (22.88 ± 10.01ng/mL and 17.51 ± 3.17ng/mL, respectively). Periostin was significantly higher in patients with IL13 AA and GA genotypes compared to those with GG genotype (p = 0.016). A significant positive correlation between serum periostin and serum IL13 among allergic patients was recorded (r = 0.352, p < 0.001).
Conclusion: Among Egyptian patients, serum level of periostin is significantly associated with asthma and positively correlates with IL13 level supporting its utility as a diagnostic biomarker. IL13 rs20541 gene polymorphism does not seem to play an obvious role in asthma and AC, which requires further evaluation.
Keywords: allergic asthma, allergic conjunctivitis, IL13 rs2054, periostin
Introduction
Asthma is a common chronic respiratory disease leading to morbidity, impaired quality of life, and mortality. The overall prevalence of asthma in Egypt was estimated to be 3.5% and 6.7% among children aged 13–14 years and adults, respectively.1,2 Allergic conjunctivitis (AC) is one of the most common allergic conditions worldwide that is estimated to affect 6–30% of the general population, causing significant eye discomfort and affecting people’s daily lives and work.3,4 The coexistence of both disorders has been documented previously, particularly in children, and was found to increase the risk of having an immunoglobulin E (IgE)-mediated allergy.5
Increased concentration of cytokines like interleukin 13 (IL13) plays a critical proinflammatory role in asthma and is mostly concomitant with ocular allergy through the enhancement of IgE production.6,7 Single nucleotide polymorphisms (SNPs) in the IL13 gene are among the polymorphisms most frequently implicated in increased susceptibility to allergic phenotypes in general.8 Previous studies in Egypt have demonstrated a significant association between IL13 genetic polymorphisms and bronchial asthma.9 However, little data exist concerning their association with AC.
Periostin is a 90 kDa matricellular protein as well as an extracellular matrix protein belonging to the fasciclin family. It is produced by epithelial cells, fibroblasts, and endothelial cells and can interact with several cell surface integrin molecules, providing signals for different tissue and organ development and remodeling, such as bones, lungs, skin, and heart.10 As the activity of bone metabolism constitutes the main source of serum periostin, its basal level was found to be age-dependent, ranging from above 100 ng/mL during childhood and adolescence to around 50 ng/mL after the cessation of bone growth in adults.11 However, serum periostin can also be affected by other factors, such as body mass index and smoking.12,13 Periostin has been shown to play an important role in the setting of allergic disorders. In asthmatic patients, periostin was found to be highly expressed in the subepithelial regions of bronchial tissue in response mainly to T helper 2 (Th2) cytokines, such as IL4 and IL13.14 However, periostin-inducing factors other than signature type-2 cytokines have been identified at the sites of allergic diseases such as tumor growth factor β (TGF-β) and histamine.10 The exact role by which periostin exaggerates allergic inflammation in asthma remains to be elucidated; however, its ability to activate nuclear factor-kappa β (NF-kβ) releasing proinflammatory mediators such as IL6 and IL24 has been demonstrated in the setting of allergic skin inflammation.15,16 Additionally, periostin can support αMβ3 integrin-mediated adhesion and migration of IL5-stimulated eosinophils and has been found to correlate with eosinophilic count as with other Th2-type allergic asthma biomarkers such as total IgE serum level, and fractional exhaled nitric oxide (FeNO).17 Based on the previous observations, periostin has emerged as a novel marker signifying type-2 asthma.18 Further reports have identified periostin as a chronic type-2 biomarker reflecting tissue remodeling and lung fibrosis in asthmatic patients and predicting hyporesponsiveness to inhaled steroids as well as the response to Th2 antagonists, such as anti-IgE Abs and anti-IL13 Abs, as therapeutic modalities in steroid-resistant patients.19,20 In spite of this, the utility of periostin as a biomarker in childhood asthma, particularly under the age of 5 years, remains questionable.21
The role of periostin in the diagnosis and monitoring of AC has also been highlighted both in animal and human studies.22,23 This could be of great utility, particularly with chronic forms of AC that could be accompanied by tissue remodeling and corneal fibrosis that would eventually result in vision loss.24
To elucidate these issues among allergic Egyptian patients, this study was designed to determine the association of IL13 gene rs20541 polymorphism and serum levels of periostin with asthma and AC patients.
Patients and Methods
This case–control study included 81 allergic patients (43 females and 38 males) with a median age of 32.73 years old. They were compared with 27 age- and gender-matched apparently healthy control subjects (14 females and 13 males) with a median age of 31.33 years old. The study was done in the Medical Microbiology and Immunology Department, Faculty of Medicine, Zagazig University in collaboration with the Allergy Unit, Research Institute of Ophthalmology, Giza, Egypt.
Ethical Issues
The study protocol was approved by the Institutional Review Board of Zagazig University (approval no. IRB#:5961–26-2-2020). All patients and control subjects provided signed informed consent, and all procedures involving human participants were performed in accordance with the updated 2013 Declaration of Helsinki.
Participants
Enrolled patients were recruited from those attending the Allergy Unit, Microbiology, Immunology and Parasitology Department, Research Institute of Ophthalmology, Giza, Egypt. Enrolled allergic patients were subjected to complete history taking and physical examination by specialist physicians at the outpatient clinics of the Institute and were diagnosed according to the criteria of the Global Strategy for Asthma Management and Prevention Guidelines, 2019 (for asthma) and the Japanese Guidelines for Allergic Conjunctival Diseases (for AC).2,24 Control subjects had no respiratory or eye symptoms and no history of respiratory or conjunctival disorders. A structured questionnaire was applied to allergic patients which inquired about socio-demographic data, possible risk factors such as family history, chronic exposure to dust, and the presence of other diagnosed allergic diseases such as allergic rhinitis, exacerbating factors such as exercise, smoking, menstruation in females, exposure to strong odors, and upper respiratory tract infections, relieving factors such as rest and the administration of bronchodilators. Clinical symptoms and their frequency were also inquired as chest tightness, cough, and wheezing in asthma and itching, blurring, redness, burning sensation, discharge, and photophobia in AC. Further clinical and routine laboratory parameters of recruited patients, eg, complete blood count (CBC), and urine and stool analysis tests were obtained from patients’ medical records. Patients who elicited a positive result for at least one of the tested aeroallergens in the skin prick test were included in the current study. Patients undergoing immunotherapy with autoimmune disorders or any kind of neoplastic disorders, with parasitic infestations, or have allergies other than asthma and AC, pregnant females, and non-Egyptians have been excluded from the current study. Enrolled patients were then classified into 3 groups; the allergic asthma group (clinically diagnosed as having asthma with a positive skin prick test), the AC group (clinically diagnosed as AC with a positive skin test), and those with a clinical diagnosis of both illnesses and having a positive skin test (the third group). Total serum IgE levels were assessed for all enrolled participants.
Sample Size Determination
The sample size was calculated using open EPI according to the recorded mean periostin level among both healthy control and asthma patients (57.32 ± 2.99 ng/mL and 74.67 ± 44.8 ng/mL, respectively) and with a case-to-control ratio of 2:1.25 At a power of 80% of the study and 95% confidence interval, the sample was calculated to be 108 subjects, 27 in each group.
Skin Prick Test
Skin testing was performed using natural allergenic extracts prepared from crude materials in the Allergy Lab, Microbiology and Immunology Unit, Research Institute of Ophthalmology, Giza, Egypt, according to the protocol established by Haggag and Hamed.26,27
The following aeroallergens were included: pollens of (palm, grass, orange), hairs of (cat, dog, rabbit, goat), wool, nicotine, feather mix, house dust, mite, mixed molds, and cockroach. Histamine dihydrochloride (10 mg/mL) was used as a positive control, whereas saline 0.9% was used as a negative control. Subjects were asked to stop antihistamines for 5 days and corticosteroids for 14 days before skin testing. The largest diameter of the wheel was measured and considered positive if it measures 3 mm or more.28
Sampling
Blood samples (9 mL) from each participant were withdrawn and divided into five mL collected in ethylenediaminetetraacetic acid (EDTA) tubes for DNA extraction and 4 mL in a plain, anticoagulant-free, vacutainer for serum separation. Serum was separated by centrifugation at 3000 rpm for 20 minutes and stored at –80℃ until further analysis.
DNA Extraction
DNA was extracted using the GeneJET™ Whole Blood Genomic DNA Purification Mini Kit (Thermo Fisher Scientific) according to the manufacturer’s instructions with a DNA yield of 2–10 μg/200-μL. Extracted DNA was stored at −20℃ for genotyping test.
Genotyping Using TaqMan Real-Time Polymerase Chain Reaction (PCR)
According to Sharifi et al,29 a specific probe of A/G IL13 rs20541 (TaqMan™ SNP Genotyping Assay, human kit, USA)(cat no: 4351379) was applied for IL13 genotyping in all participants using real-time PCR thermal cycler (Applied Biosystems, USA). In a sterile tube, a total reaction volume of 20 µL was set consisting of 9μL of extracted DNA, 10 μL of TaqMan™ genotyping master mix (cat no: 4371353), and 1μL of SNP IL13 probe. Cycling conditions were 95℃ for 10 minutes, followed by 35 cycles at 95℃ for 15 s, annealing at 60℃ for 1 minute, and final extension at 60℃ for 30 s.
Measurement of Serum Periostin, IL13, and Total IgE Levels
Serum periostin was assessed using an ELISA kit (cat. no. 201–12-4519; Shanghai Sun Red Biological Technology Co., Ltd.) according to the manufacturer’s instructions. Optical density (OD) for each sample was measured at 450 nm wavelength. The level of periostin was calculated using calibration curves with a sensitivity of 0.625 ng/mL.
IL13 serum level was measured by an ELISA kit (cat. no. 201–12-0099; Shanghai Sun Red Biological Technology Co., Ltd.) and OD was determined at 450 nm wavelength. Calibration curves were used to determine the level of IL13 with a sensitivity of 0.413 pg/mL.
Serum total IgE level was measured using a specific ELISA kit (cat. no. BDIG29-BA; Bioactiva Diagnostica). Absorbance was measured at a 450 nm wavelength. The results were expressed in IU/mL.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics Version 22. Data were tested for normality using Kolmogorov–Smirnov test and Shapiro–Wilk test. Quantitative data were presented as mean and standard deviation (SD). Qualitative data were presented as numbers and percentages. The comparison of categorical variables was done by using the Chi-square test or Fisher's exact test as appropriate. For normally distributed data, the independent sample t-test was used to compare numerical variables between the two groups, while ANOVA and Tukey post hoc tests were used to compare between the four groups. Mann–Whitney test was used to compare numerical variables between two groups and Kruskal Wallis to compare the four groups of nonnormally distributed variables. Pearson correlation coefficient was used to correlate the period and IL-13 levels. P values of ≤0.05 were considered to be significant. All tests were two-tailed.
Results
The present study included 81 allergic patients and 27 apparently healthy age and gender-matched control subjects. Female predominance among allergic cases was observed (53.1%) (Table 1). Patients with AC were significantly younger than those with asthma (p = 0.02) (Table 2). Regarding residence, 66.7% of allergic patients were from urban areas and this was found to significantly increase the risk of allergy compared to those living in rural areas (OR = 2.50, p = 0.04) (Table 1). Further comparison between the studied groups revealed the significant role of residing in urban areas, particularly in the asthmatic group compared to control subjects (p = 0.044) (Table 2).
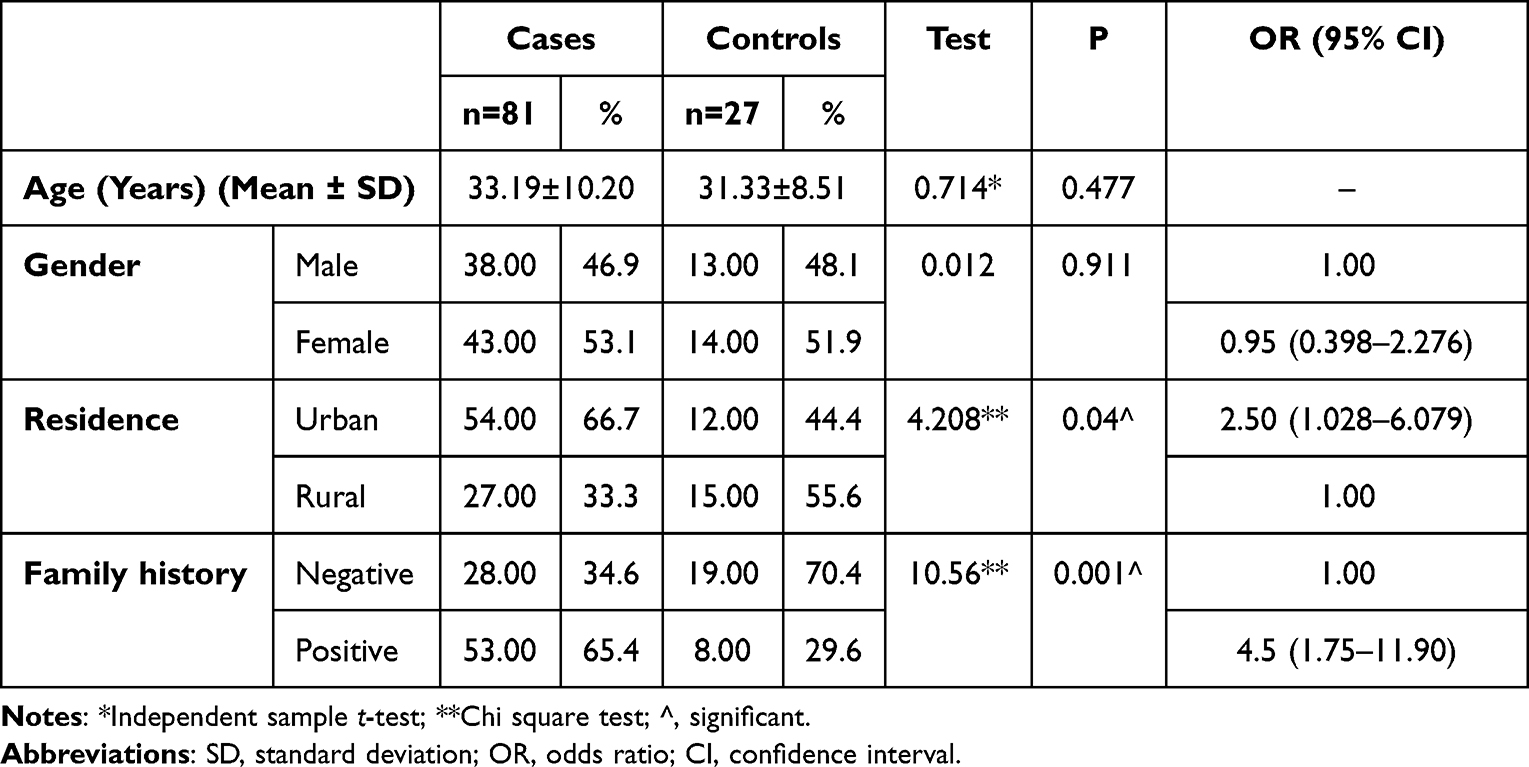 |
Table 1 Socio-Demographics of Allergic Patients and Controls |
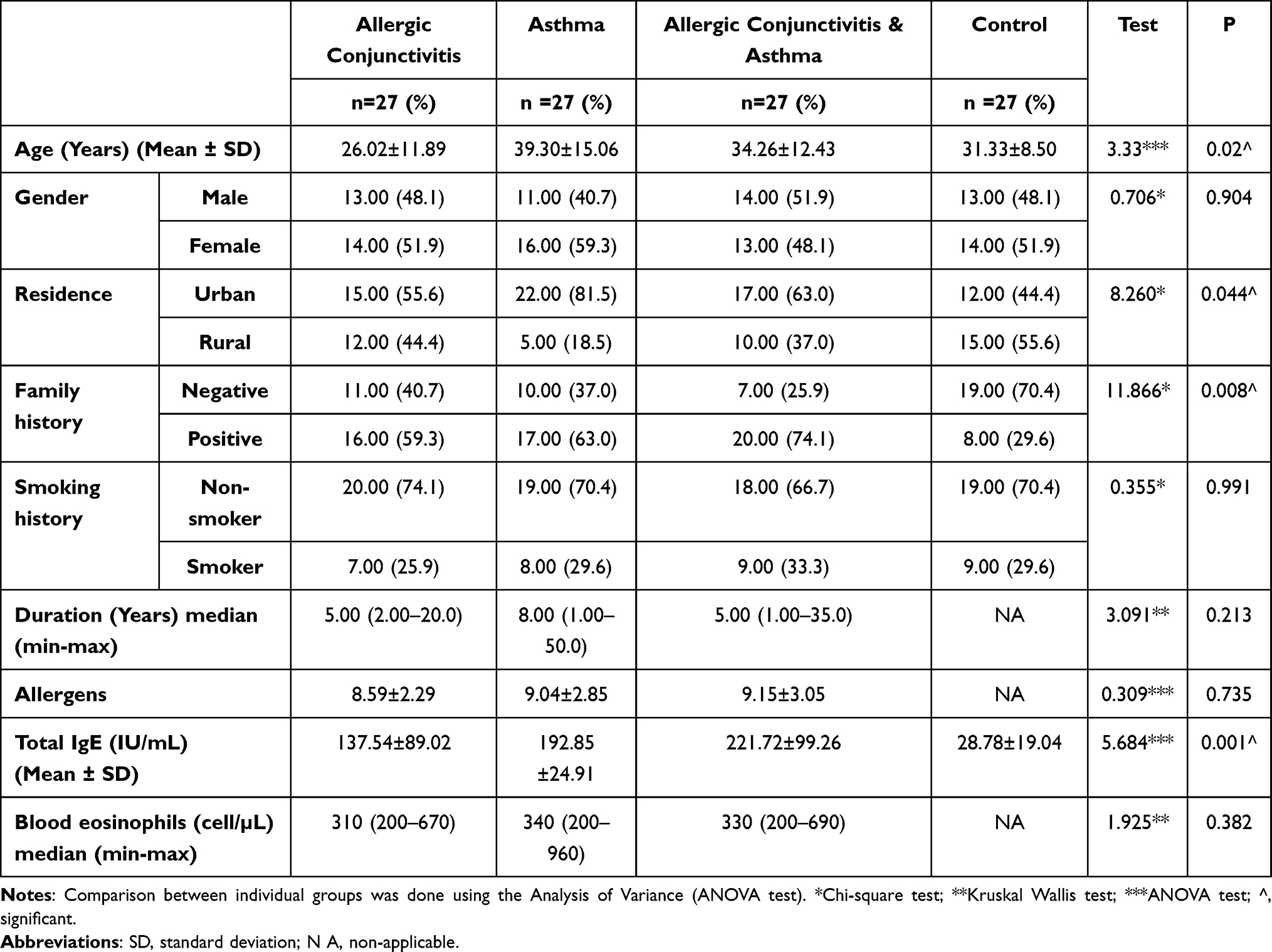 |
Table 2 Characteristics of Different Groups of Allergic Patients and Controls |
Positive family history was found to increase the risk of allergy in the studied patients by 4.50 folds than in control subjects (OR = 4.50, p = 0.001) (Table 1). Among the different patient groups, this was more evident in patients with AC associated with asthma. Total IgE showed significantly higher levels in allergic patients than in control subjects (P = 0.001). No significant differences were noticed between different groups of patients regarding the disease duration, allergen sensitivity, or blood eosinophilic count (Table 2).
Genotype and allele distribution of IL13 gene rs20541 analysis (Table 3, Figure 1) revealed no significant difference between allergic patients in different groups and controls. The homozygous GG genotype showed a higher frequency among the AC group (70.4%), whereas the asthmatic group had a frequency of (51.9%) which was lower than the controls (55.6%). The AA genotype was found to be more frequent in the asthmatic group (14.8%) compared to healthy subjects (3.7%). However, it was not detected among AC group. A higher frequency of the A allele (minor allele) among asthmatics (31.5%) compared to controls (24.1%) was noticed. However, among the AC group, the G allele (major allele) predominated (85.2%) recording a frequency higher than the controls (75.9%), yet no significant differences were recorded.
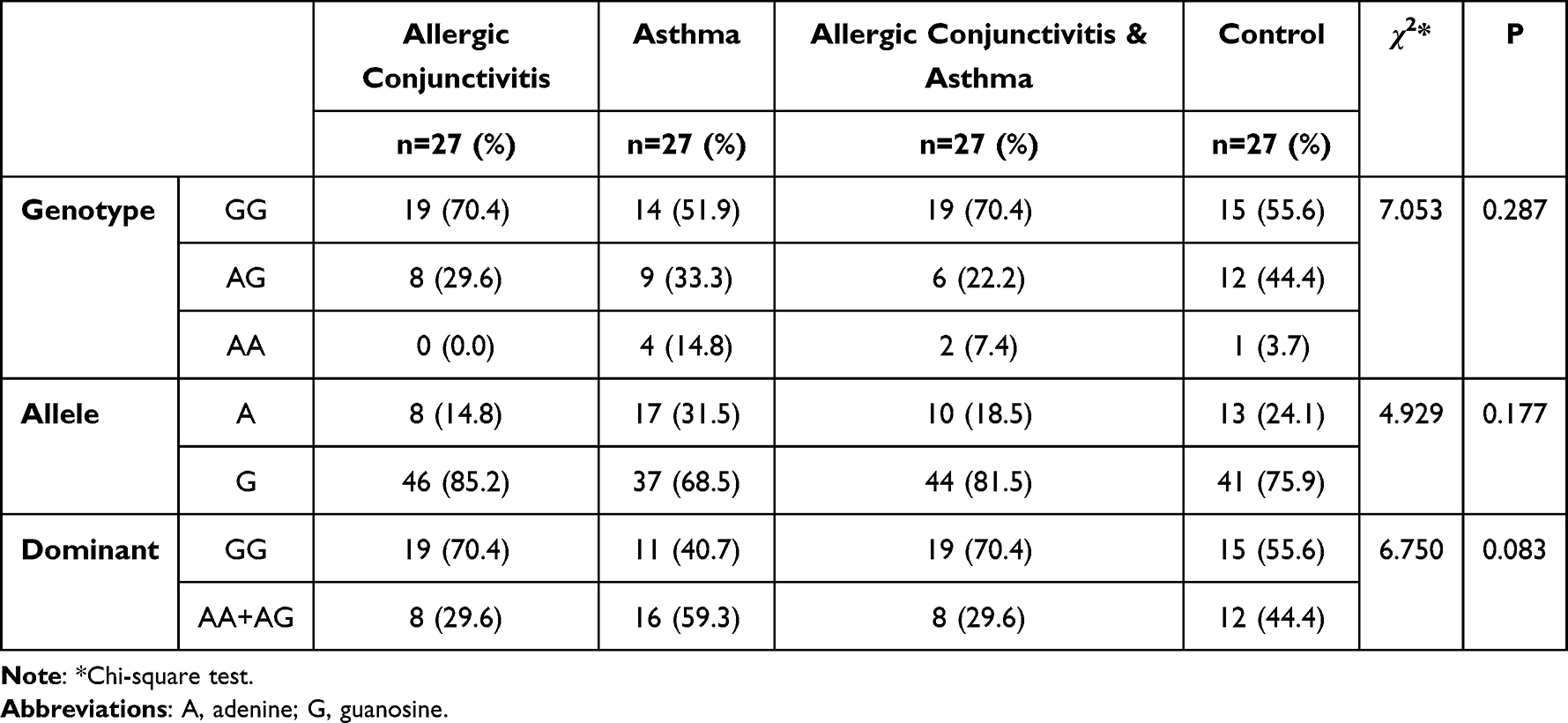 |
Table 3 Allelic and Genotypic Frequency for IL13 rs20541 Gene Polymorphism Among Different Patient Groups and Controls |
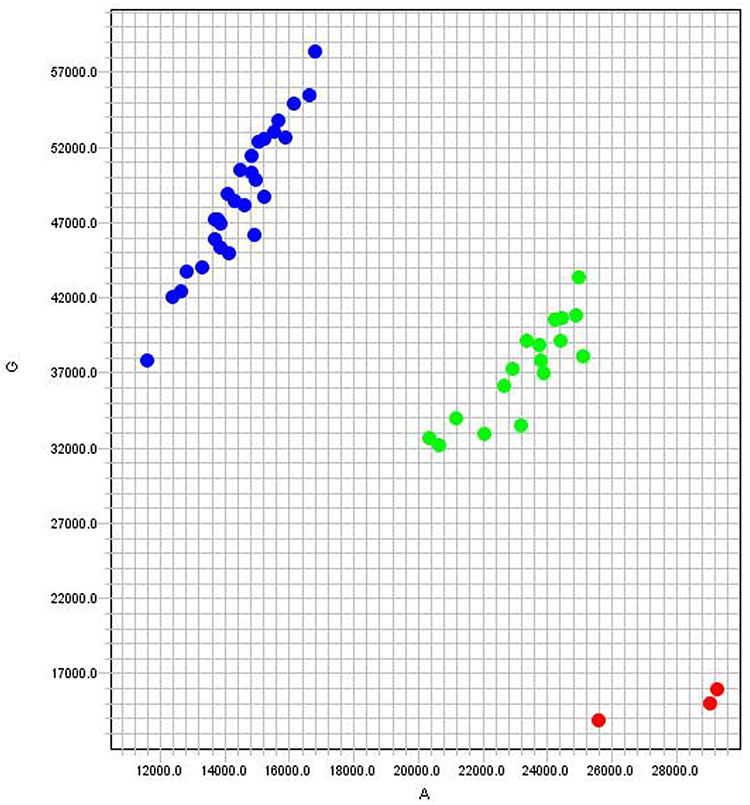 |
Figure 1 Allelic discrimination plot showing the results of IL13 rs20541 SNP genotyping by real-time PCR in 48 examined allergic patients. Blue dots correspond to the homozygous GG genotype (28 patients), green dots correspond to the heterozygous AG genotypes (17 patients), and red dots correspond to the homozygous AA genotype (3 patients). The X-axis represents the fluorescence of allele A while the Y-axis represents that of allele G. Different colors correspond to different fluorescent dyes used in the reaction; FAM (blue), ROX (red), and VIC (green). |
Serum periostin recorded significantly higher levels in asthmatics compared to controls (26.05 ± 10.71 ng/mL, 17.51 ± 3.17 ng/mL, respectively, p = 0.005) as revealed by the post hoc test (Tukey HSD). However, no significant differences were recorded in the other two allergic groups, although they had elevated levels compared to controls (Table 4). A significant positive correlation was found between serum periostin levels and blood eosinophil count of allergic patients (r = 0.849, p < 0.001).
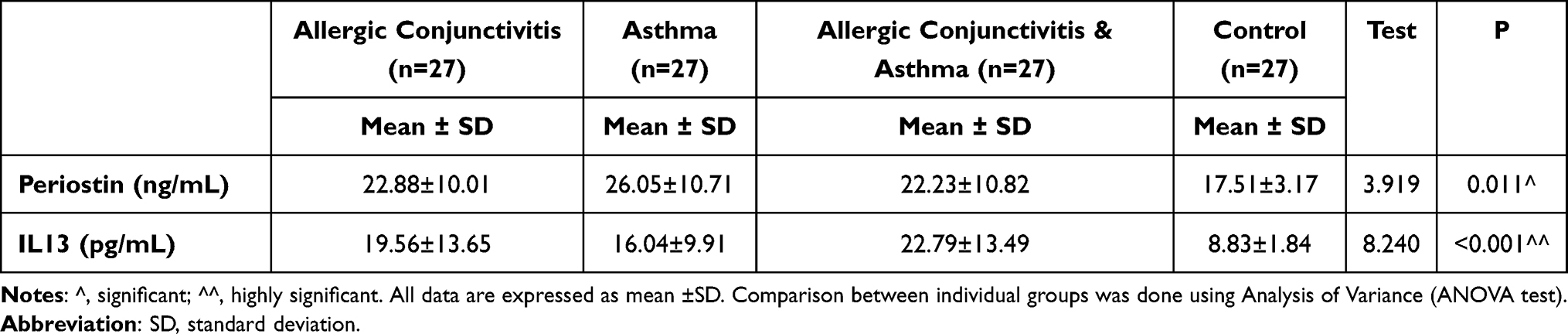 |
Table 4 Serum Levels of Periostin and IL13 Among Different Groups of Patients and Control |
The serum levels of IL13 were further assessed in the studied participants to elucidate the effect of the IL13 rs20541 polymorphism on the expression level of IL13. Significantly higher serum levels in patients with AC and in AC associated with asthma than in control subjects were recorded (p = 0.002, <0.001, respectively) as revealed by the post hoc test. Higher levels of IL-13 were also found in asthmatics (16.04 ± 9.91 pg/mL); however, no significant difference was found compared to controls (8.83 ± 1.84 pg/mL) (Table 4).
Further analysis revealed a higher IL13 level in patients with the AA genotype (22.19 ± 11.68 pg/mL) compared to the other genotypes (GG and AG) (16.56 ± 6.20 and 16.19 ± 10.94 pg/mL, respectively) with no significant difference detected. Interestingly, a significant association between serum periostin levels and the IL13 rs20541 genotype and allele distribution was detected, where significantly higher levels were recorded in patients with AA and AG than in those with GG genotype (p = 0.016) (Table 5). Additionally, a significant positive correlation between serum periostin and serum IL13 (r = 0.352, p < 0.001) was evident (Figure 2).
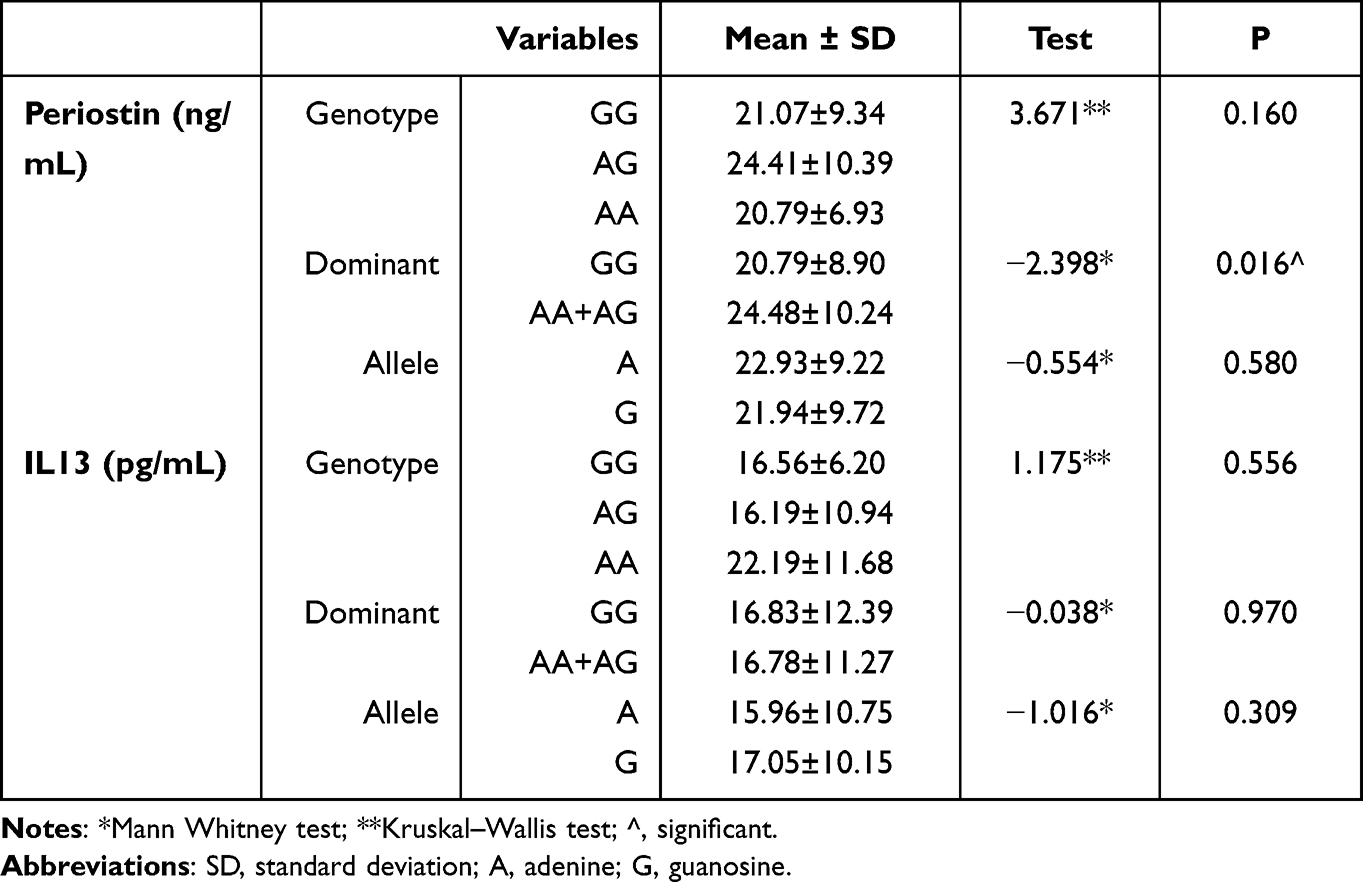 |
Table 5 Relation Between Serum Periostin, Serum IL13, and IL13 rs20541 Alleles and Genotypes Among Allergic Patients (n = 81) |
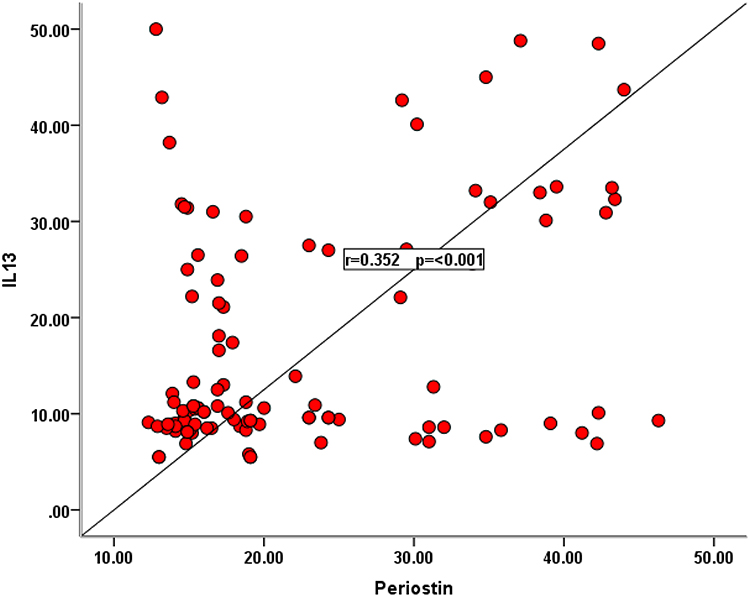 |
Figure 2 A scattered plot curve shows a significant positive correlation (r=0.352, p<0.001) between serum level of periostin and serum level of IL13 among the examined allergic patients (n=81). |
Discussion
Genetic variation among individuals can influence their vulnerability to several diseases including allergic disorders.30 Three groups of allergic patients, including asthma, AC, and both asthma and AC, were investigated and compared to age- and gender-matched apparently healthy control subjects in this work.
Females represented 53.1% of the total cohort of patients in this study. This is consistent with Senna et al who confirmed a female predominance (61.8%) among asthmatics.31 In contrast to this finding, male predominance among allergic patients was reported in other studies.32,33 Although the mechanism underlying this difference is not completely understood, it seems that female sex hormones, particularly estrogen, play an important role in allergic diseases as most immune cells express estrogen receptors and can respond to the hormone favoring the allergic response.34 This is probably achieved through the enhancement of antigen-presenting cell function, intensifying Th2 polarization, increasing class-switching of B cells to IgE production, and encouragement of mast cell and basophil degranulation.35 Not only is the prevalence of asthma affected by sex hormones but also the severity, where hormonal fluctuations in females may have been accompanied by greater bronchial hyperreactivity and worsening of symptoms in some females.36
Residence in urban areas and positive family history were found to significantly increase the risk of allergies among enrolled patients compared to healthy subjects in the current work (OR = 2.50, p = 0.04, and OR = 4.5, p = 0.001, respectively) which comes in agreement with previous reports.37,38
Several studies have reported the SNPs in the IL13 gene to be associated with susceptibility to allergic disorders and their severity.7,39–42 However, meta-analysis studies have shown that the frequencies of different SNPs and their contribution to allergic disorders vary among populations of different ethnicities.43,44
The current work did not find a significant difference between allergic patients as a whole and control subjects regarding the genotype and allele distribution of IL13 rs20541 gene polymorphism. In a previous Egyptian study, the IL13 +2044 polymorphism was significantly associated with bronchial asthma where subjects carrying the A allele were at about 7.39-fold higher risk for developing asthma (OR = 7.389, p < 0.001), furthermore, significant associations between the A allele and more severe asthma and higher total serum IgE levels were found (p < 0.001 and <0.001, respectively).9 The relatively small sample size included in the study could be one factor contributing to this finding. Additionally, the current study investigated a different IL13 SNP (rs20541). However, the contribution and the complex interaction of other genetic polymorphisms, whether in the IL13 gene or in other genes, in the development of a certain allergic phenotype could not be ignored.30
Similarly, Lu et al did not find a significant association between IL13 SNPs and allergic rhinitis. Additionally, and consistent with the current work, Sharifi et al showed no significant difference between Iranian asthmatic patients and control subjects (p = 0.319) regarding IL13 rs20541 G/A polymorphism.29,45
In the current study, a higher percentage of the homozygous (AA) genotype was found in the asthmatic group (14.8%) compared to healthy controls (3.7%). This comes consistent with Imraish et al who reported a significant association between the homozygous (AA) genotype and asthmatic patients compared to control subjects (p = 0.0097).40
The replacement of the G allele, the major allele, by the A allele, the minor one, in IL13 rs20514 has been shown previously to be associated with higher IL13 activity as it results in the replacement of the positively charged arginine by the neutral glutamine increasing the interaction between IL13 and its receptor IL4Rα/IL13Rα1.46
The current study recorded a higher frequency of the minor A allele among asthmatics compared to healthy subjects (31.5% and 24.1%, respectively) yet with no significant difference (p 0.177). A similar finding was reported previously by Farhan et al who reported a frequency of 32% among asthmatics compared to 16% among controls. However, in contrast to the current study, Sharifi et al recorded a higher frequency of the AA genotype among healthy controls compared to asthmatic patients (11% and 7.78%, respectively).29,39
The A allele was further reported to be a risk factor for allergic rhinitis/allergic conjunctivitis asthma in another study (OR 3.06, 95% CI 1.42–6.58, P = 0.004).47 However, in the current study, the A allele was not detected in the group of AC patients. The relatively small number of enrolled patients in the current study may account for that.
When the dominant model was further analyzed, the current study found the frequencies of GA+AA genotypes to be higher in the asthmatic group compared to controls (59.3% and 44.4%, respectively) and to the AC group (29.6%). This comes in line with previous findings.7,39
The exact role of periostin in asthma is still not fully explained. However, it may contribute to several pathogenic processes, such as eosinophil recruitment, subepithelial fibrosis, and mucous production from goblet cells. This could be achieved by its binding to several integrins on various cell types, such as fibroblasts and eosinophils.48 Furthermore, high serum periostin was found to correlate with certain clinical features of asthma, such as older age at the onset of asthma and lower pulmonary function.49 Periostin has also been documented to be implicated in the pathogenesis of AC, whether in animal models or in patients with atopic keratoconjunctivitis.22,23
In the current study, serum periostin in the asthmatic group was significantly higher than in control subjects (p = 0.005). Similar findings were previously reported in Egypt.50
In the AC group and even with elevated serum levels of periostin compared to control subjects (22.88 ± 10.01 ng/mL, 17.51 ±3.17 ng/mL, respectively), no significant difference was noticed. However, the level of serum periostin was found to have a significant positive correlation with blood eosinophil count in allergic patients including those with AC. To our knowledge, this is the first report addressing periostin levels in AC patients in Egypt. Furthermore, few studies have addressed this issue worldwide. Fujishima et al found a significant difference in serum periostin between patients with atopic keratoconjunctivitis (p < 0.001), but not with seasonal AC, compared with control subjects.23
In allergic individuals, the Th2 phenotype predominates, leading to increased production of IL13 and class-switching in B cells to synthesize IgE.51 IL13 serum levels were significantly higher in patients with AC and in patients with AC associated with asthma than in controls (p = 0.002, <0.001, respectively) in the current study. Higher levels were also recorded in the asthmatic group; however, no significant difference was found compared to control subjects. Jebur and Saud revealed that the IL13 level was significantly increased in asthmatics in comparison to healthy individuals (p < 0.001),52 which comes in line with the current findings. However, Davoodi et al reported a lower median serum level of IL13 among asthmatic patients (40.0 pg/mL, 95% CI = 20.0–360.0) than in healthy subjects (58.25 pg/mL, 95% CI = 20.0–370.0).53
The current study did not find a significant association between serum IL13 levels and IL13 genotype and/or allele distribution among allergic patients. Previous findings indicated that the IL13 rs20541 SNP is coding and functional and that the A allele presence is associated with increased IL13 expression,54 which was not demonstrated in the current study. However, the complex interaction between genetic and epigenetic factors of different ethnicities and their implications on gene expression could contribute to this finding.55
On the other hand, serum periostin was significantly higher in patients with IL13 rs20541 AA and AG genotypes than those with GG genotypes (p = 0.016), a finding that may highlight periostin as an important marker for these genotypes in allergic patients. Additionally, a significant positive correlation between serum periostin and IL13 levels in allergic patients was recorded, which further highlights periostin as a useful diagnostic biomarker in allergic diseases. Fujishima et al reported that periostin and IL13 levels in the tears of all patients with ocular allergic disease and healthy controls showed a weak but significant correlation (n = 59, r = 0.3329, p < 0.05) which supports our finding.23
Limitations of the Study
This study is not without limitations, such as the relatively small sample size included without considering the heterogeneity in the clinical aspects (phenotypes) of enrolled patients and the lack of assessment of other coding SNPs in the IL13 gene.
Data Sharing Statement
All data and materials related to the study are included in the current manuscript.
Ethical Approval and Consent to Participate
The study was approved by the Institutional Review Board (IRB), Faculty of Medicine, Zagazig University. (approval no. IRB#:5961-26-2-2020)
Disclosure
The authors report no conflicts of interest.
References
1. Tarraf H, Aydin O, Mungan D, et al. Prevalence of asthma among the adult general population of five Middle Eastern countries: results of the SNAPSHOT program. BMC Pulm Med. 2018;18(1):68.
2. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention; 2019. Available from: www.ginasthma.org.
3. Leonardi A, Castegnaro A, Valerio AL, Lazzarini D. Epidemiology of allergic conjunctivitis: clinical appearance and treatment patterns in a population-based study. Curr Opin Allergy Clin Immunol. 2015;15(5):482–488. doi:10.1097/ACI.0000000000000204
4. Ackerman S, Smith LM, Gomes PJ. Ocular itch associated with allergic conjunctivitis: latest evidence and clinical management. Ther Adv Chronic Dis. 2016;7(1):52–67. doi:10.1177/2040622315612745
5. Michailopoulos P, Almaliotis D, Georgiadou I, et al. Allergic conjunctivitis in patients with respiratory allergic symptoms; a retrospective study in Greece. Med Hypothesis Discov Innov Ophthalmol. 2017;6(1):3–9.
6. Bao K, Reinhardt RL. The differential expression of IL-4 and IL-13 and its impact on type-2 immunity. Cytokine. 2015;75(1):25–37. doi:10.1016/j.cyto.2015.05.008
7. Halwani R, Vazquez-Tello A, Kenana R, et al. Association of IL-13 rs20541 and rs1295686 variants with symptomatic asthma in a Saudi Arabian population. J Asthma. 2018;55(11):1157–1165. doi:10.1080/02770903.2017.1400047
8. Wang Z-D, Lian D, Shen J-L, et al. Association between the interleukin-4, interleukin-13 polymorphisms and asthma: a meta-analysis. Mol Biol Rep. 2013;40(2):1365–1376. doi:10.1007/s11033-012-2180-0
9. Noureldin M, Haroun M, Diab I, Elbanna S, Abdelwahab N. Association of interleukin 13 +2044G/A polymorphism with bronchial asthma development, severity and immunoglobulin E levels in an Egyptian population. Clin Med Diagn. 2014;4:71–77.
10. Izuhara K, Nunomura S, Nanri Y, Ono J, Takai M, Kawaguchi A. Periostin: an emerging biomarker for allergic diseases. Allergy. 2019;74(11):2116–2128. doi:10.1111/all.13814
11. Fujitani H, Kasuga S, Ishihara T, et al. Age-related changes in serum periostin level in allergic and non-allergic children. Allergol Int. 2019;68(2):285–286. doi:10.1016/j.alit.2018.12.006
12. Kimura H, Konno S, Makita H, et al. Serum periostin is associated with body mass index and allergic rhinitis in healthy and asthmatic subjects. Allergol Int. 2018;67(3):357–363. doi:10.1016/j.alit.2017.11.006
13. Takahashi K, Meguro K, Kawashima H, et al. Serum periostin levels serve as a biomarker for both eosinophilic airway inflammation and fixed airflow limitation in well-controlled asthmatics. J Asthma. 2019;56(3):236–243. doi:10.1080/02770903.2018.1455855
14. Sonnenberg-Riethmacher E, Miehe M, Riethmacher D. Periostin in allergy and inflammation. Front Immunol. 2021;12:722170. doi:10.3389/fimmu.2021.722170
15. Masuoka M, Shiraishi H, Ohta S, et al. Periostin promotes chronic allergic inflammation in response to Th2 cytokines. J Clin Invest. 2012;122(7):2590–2600. doi:10.1172/JCI58978
16. Mitamura Y, Nunomura S, Nanri Y, et al. The IL-13/periostin/IL-24 pathway causes epidermal barrier dysfunction in allergic skin inflammation. Allergy. 2018;73(9):1881–1891. doi:10.1111/all.13437
17. Matsumoto H. Serum periostin: a novel biomarker for asthma management. Allergol Int. 2014;63(2):153–160. doi:10.2332/allergolint.13-RAI-0678
18. Woodruff PG, Boushey HA, Dolganov GM, et al. Genome-wide profiling identifies epithelial cell genes associated with asthma and with treatment response to corticosteroids. Proc Natl Acad Sci USA. 2007;104(40):15858–15863. doi:10.1073/pnas.0707413104
19. Corren J, Lemanske RF, Hanania NA, et al. Lebrikizumab treatment in adults with asthma. N Engl J Med. 2011;365(12):1088–1098. doi:10.1056/NEJMoa1106469
20. Hanania NA, Wenzel S, Rosén K, et al. Exploring the effects of omalizumab in allergic asthma: an analysis of biomarkers in the EXTRA study. Am J Respir Crit Care Med. 2013;187(8):804–811. doi:10.1164/rccm.201208-1414OC
21. Anderson HM, Lemanske RF Jr, Arron JR, et al. Relationships among aeroallergen sensitization, peripheral blood eosinophils, and periostin in pediatric asthma development. J Allergy Clin Immunol. 2017;139(3):790–796. doi:10.1016/j.jaci.2016.05.033
22. Asada Y, Okano M, Ishida W, et al. Periostin deletion suppresses late-phase response in mouse experimental allergic conjunctivitis. Allergol Int. 2019;68(2):233–239. doi:10.1016/j.alit.2018.09.007
23. Fujishima H, Okada N, Matsumoto K, et al. The usefulness of measuring tear periostin for the diagnosis and management of ocular allergic diseases. J Allergy Clin Immunol. 2016;138(2):459–467.e2. doi:10.1016/j.jaci.2015.11.039
24. Takamura E, Uchio E, Ebihara N, et al. Japanese Society of Allergology. Japanese guideline for allergic conjunctival diseases. Allergol Int. 2011;60(2):191–203. doi:10.2332/allergolint.11-RAI-0335
25. Elhady M, Abdelmalik M, Abu Farag I, Elattar S, Alwakil I. Serum periostin level in children with bronchial asthma: a comparative study. J Med Sci Clin Res. 2017;5(1):15536–15542. doi:10.18535/jmscr/v5i1.55
26. Bernstein IL, Li JT, Bernstein DI, et al. American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology. Allergy diagnostic testing: an updated practice parameter. Ann Allergy Asthma Immunol. 2008;100(3 Suppl 3):S1–148. doi:10.1016/s1081-1206(10)60305-5
27. Haggag M, Hamed A. Comparison of the efficacy of local nasal and subcutaneous immunotherapy using natural allergen extracts in treatment of allergic rhinitis. Egypt J Med Microbiol. 2008;17:627–635.
28. Heinzerling L, Mari A, Bergmann KC, et al. The skin prick test - European standards. Clin Transl Allergy. 2013;3(1):3. doi:10.1186/2045-7022-3-3
29. Sharifi A, Ghadiri A, Salimi A, Ghandil P, Esmaeili S. Evaluating the distribution of (+ 2044G/A, R130Q) rs20541 and (−1112 C/T) rs1800925 polymorphism in IL-13 gene: an association-based study with asthma in Ahvaz, Iran. Int J Med Lab. 2021;8(1):62–69.
30. March ME, Sleiman PM, Hakonarson H. Genetic polymorphisms and associated susceptibility to asthma. Int J Gen Med. 2013;6:253–265. doi:10.2147/IJGM.S28156
31. Senna G, Latorre M, Bugiani M, et al.; SANI Network Sex differences in severe asthma: results from severe asthma network in Italy-SANI. Allergy Asthma Immunol Res. 2021;13(2):219–228. doi:10.4168/aair.2021.13.2.219
32. Qi Y, Shi P, Chen R, et al. Characteristics of childhood allergic diseases in outpatient and emergency departments in Shanghai, China, 2016–2018: a multicenter, retrospective study. BMC Pediatr. 2021;409:1.
33. Ibrahim BM, Abdel-Latif RS. Correlation of tear film-specific immunoglobulin E assay with the skin prick test in allergic conjunctivitis. Delta J Ophthalmol. 2017;18(3):123–132. doi:10.4103/DJO.DJO_30_17
34. Keselman A, Heller N. Estrogen signaling modulates allergic inflammation and contributes to sex differences in asthma. Front Immunol. 2015;6:568. doi:10.3389/fimmu.2015.00568
35. Fan Z, Che H, Yang S, Chen C. Estrogen and estrogen receptor signaling promotes allergic immune responses: effects on immune cells, cytokines, and inflammatory factors involved in allergy. Allergol Immunopathol. 2019;47(5):506–512. doi:10.1016/j.aller.2019.03.001
36. Thornton J, Lewis J, Lebrun CM, Licskai CJ. Clinical characteristics of women with menstrual-linked asthma. Respir Med. 2012;106(9):1236–1243. doi:10.1016/j.rmed.2012.05.003
37. Desalu OO, Adeoti AO, Ojuawo OB, et al. Urban-rural differences in the epidemiology of asthma and allergies in Nigeria: a population-based study. J Asthma Allergy. 2021;14:1389–1397. doi:10.2147/JAA.S333133
38. Haggag M, Aboelazm A, Al-Gazzar A, Mahmoud M, Hassan M. Immunoblotting technique versus skin prick test for detection of allergen specific immunoglobulin E in allergic conjunctivitis. J Ophthalmol Rel Sci. 2017;1(2):39–50. doi:10.21608/jors.2017.5048
39. Farhan AA, Abbas AA, Rasheed HA. The role of IL-13 polymorphisms in asthma. Ann Trop Med Public Health. 2021;24:242. doi:10.36295/ASRO.2021.24202
40. Imraish A, Abu-Thiab T, Zihlif M. IL-13 and FOXO3 genes polymorphisms regulate IgE levels in asthmatic patients. Biomed Rep. 2021;14(6):55. doi:10.3892/br.2021.1431
41. Accordini S, Calciano L, Bombieri C, et al. An interleukin 13 polymorphism is associated with symptom severity in adult subjects with ever asthma. PLoS One. 2016;11(3):e0151292. doi:10.1371/journal.pone.0151292
42. Ying XJ, Zhao SW, Wang GL, Xie J, Xu HM, Dong P. Association of interleukin-13 SNP rs20541 with allergic rhinitis risk: a meta-analysis. Gene. 2013;521(2):222–226. doi:10.1016/j.gene.2013.03.088
43. Mei Q, Qu J. Interleukin-13 +2044 G/A and +1923C/T polymorphisms are associated with asthma susceptibility in Asians: a meta-analysis. Medicine. 2017;96(51):e9203. doi:10.1097/MD.0000000000009203
44. Xu Y, Li J, Ding Z, et al. Association between IL-13 +1923C/T polymorphism and asthma risk: a meta-analysis based on 26 case-control studies. Biosci Rep. 2017;37(1):BSR20160505. doi:10.1042/BSR20160505
45. Lu MP, Chen RX, Wang ML, et al. Association study on IL4, IL13 and IL4RA polymorphisms in mite-sensitized persistent allergic rhinitis in a Chinese population. PLoS One. 2011;6(11):e27363. doi:10.1371/journal.pone.0027363
46. Madhankumar AB, Mintz A, Debinski W. Alanine-scanning mutagenesis of alpha-helix D segment of interleukin-13 reveals new functionally important residues of the cytokine. J Biol Chem. 2002;277(45):43194–43205. doi:10.1074/jbc.M205047200
47. Ådjers K, Luukkainen A, Pekkanen J, et al. Self-reported allergic rhinitis and/or allergic conjunctivitis associate with IL13 rs20541 polymorphism in Finnish adult asthma patients. Int Arch Allergy Immunol. 2017;172(2):123–128. doi:10.1159/000456009
48. Izuhara K, Conway SJ, Moore BB, et al. Roles of periostin in respiratory disorders. Am J Respir Crit Care Med. 2016;193(9):949–956. doi:10.1164/rccm.201510-2032PP
49. Matsusaka M, Kabata H, Fukunaga K, et al. Phenotype of asthma related with high serum periostin levels. Allergol Int. 2015;64(2):175–180. doi:10.1016/j.alit.2014.07.003
50. Refaat MM, El Sayed E, Abd El-Fattah W, Elbanna AH, Sayed HME. Relationship between sputum periostin level and inflammatory asthma phenotypes in Egyptian patients. J Asthma. 2021;58(10):1285–1291. doi:10.1080/02770903.2020.1786111
51. Qurashi TA, Shah A, Bhat GA, Khan MS, Rasool R, Mudassar S. Atopy in Kashmir-validation from a case-control study with respect to IgE and interleukin genes. Allergy Asthma Clin Immunol. 2021;17(1):119. doi:10.1186/s13223-021-00623-5
52. Jebur MS, Saud AM. Serum levels of total IgE and interleukin-13 in a sample of allergic asthma patients in Baghdad. Iraqi J Sci. 2020;61(12):3208–3214. doi:10.24996/ijs.2020.61.12.8
53. Davoodi P, Mahesh PA, Holla AD, et al. Serum levels of interleukin-13 and interferon-gamma from adult patients with asthma in Mysore. Cytokine. 2012;60(2):431–437. doi:10.1016/j.cyto.2012.05.012
54. Arima K, Umeshita-Suyama R, Sakata Y, et al. Upregulation of IL-13 concentration in vivo by the IL13 variant associated with bronchial asthma. J Allergy Clin Immunol. 2002;109(6):980–987. doi:10.1067/mai.2002.124656
55. Nicodemus-Johnson J, Naughton KA, Sudi J, et al. Genome-wide methylation study identifies an IL-13-induced epigenetic signature in asthmatic airways. Am J Respir Crit Care Med. 2016;193(4):376–385. doi:10.1164/rccm.201506-1243OC
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.