")
Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 15
Association of IL-6 and TGF-β Gene Polymorphisms with the Risk of Thoracolumbar Osteoporotic Vertebral Compression Fractures
Authors Xiong Y, He Y, Peng Y, Geng Y
Received 26 November 2021
Accepted for publication 9 February 2022
Published 19 April 2022 Volume 2022:15 Pages 351—358
DOI https://doi.org/10.2147/PGPM.S351372
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Yi Xiong,1 Ye He,2 Yan Peng,3 Yun Geng4
1Department of Orthopaedic, The Central Hospital of Enshi Tujia and Miao Autonomous Prefecture, Hubei, People’s Republic of China; 2Department of Preventive Treatment of Diseases,Shaanxi Meixian Hospital of Traditional Chinese Medicine, Shaanxi, People’s Republic of China; 3Department of Medical Examination, Yili Kazak Autonomous Prefecture Hospital of Traditional Chinese Medicine, Xinjiang, People’s Republic of China; 4Department of Pharmacology, Shandong First Medical University and Shandong Academy of Medical Sciences, Shandong, People’s Republic of China
Correspondence: Yun Geng, Tel/Fax +86-531-59556066, Email [email protected]
Purpose: Osteoporotic vertebral compression fracture (OVCF) is a common disease in the elderly, and genetic factors play a key role in its occurrence. The present study was conducted to investigate the association between interleukin-6 (IL-6) and the transforming growth factor (TGF-β) gene polymorphisms and the occurrence of thoracolumbar OVCF.
Patients and Methods: This case–control study recruited 146 patients with OVCF and 144 osteoporosis patients as the control group. Genotypes of the IL-6 rs1800796 and TGF-β rs1982073 were analyzed by sequencing. Genotype distribution and allelic frequencies were investigated by the χ2 test. Odds ratios (OR) and 95% confidence intervals (CI) evaluated the relationship of IL-6 or TGF-β polymorphism and OVCF susceptibility.
Results: Allele G and genotype GG of IL-6 rs1800796 was more frequent in patients with OVCF (40.07% vs.28.47%; 19.18% vs.7.64%) compared with controls. GG genotype (OR=3.394, 95% CI=1.560– 7.385, P < 0.001) and G allele (OR=1.680, 95% CI=1.187– 2.376, P < 0.001) of IL-6 rs1800796 was significantly associated with increased risk of OVCF. What is more, CT and TT genotypes (41.78 vs.51.39; 19.86 vs.26.39) and allele T (40.75 vs 52.08) of TGF-β rs1982073 were less frequent in OVCFs, more common in controls and protective against OVCF risk (OR=0.436, 95% CI=0.228– 0.835, P = 0.012; OR=0.615, 95% CI=0.443– 0.855, P = 0.004).
Conclusion: Our results suggest that the G allele and GG genotype of IL-6 rs1800796 may contribute to increased susceptibility to OVCF in elderly Chinese. In contrast, CT and TT genotypes and the T allele of TGF-β rs1982073 may contribute to lower susceptibility of OVCF.
Keywords: OVCF, IL-6, TGF-β, gene polymorphisms
Introduction
As the higher frequency complication of osteoporosis, osteoporotic vertebral compression fractures (OVCF) are the most common clinical fracture, and there are nearly 1.4 million new cases per year.1 Epidemiology shows that the thoracolumbar vertebral body is the most common site for osteoporotic fractures, and the incidence of thoracolumbar OVCF accounts for 53% of all fragility fractures.2 It can cause severe and long-term low back pain, even disability, and seriously affect the quality of life.3 Pathogenesis of OVCF is complicated, and individual nutrition, genetic factors, environment, and living habits are all risk factors. Genetic factors are particularly important, which determine about 70–80% of peak bone mass during individual growth.4 Recently, with the maturity and popularization of gene sequencing technology, a large number of single nucleotide polymorphisms (SNPs) have been found in the gene, which is closely related to many diseases, including OVCF.5
Interleukin-6 (IL-6) is a multifunctional cytokine that is involved in immune regulation and inflammation and promotes B cell differentiation and T cell proliferation.6 The human IL-6 gene is located on human chromosome 7p21 and contains 5 exons and 4 introns. The current research on IL-6 gene polymorphism mainly focuses on SNPs in the promoter region, such as −597G/A (re1800797), −572G/C (rs1800796), −174G/C (rs1800795). They affect the expression level of IL-6 by regulating gene transcription and expression strength, and then make differences in the susceptibility of the population to diseases such as COVID-19,7 coronary artery disease,8 and type 2 diabetes.9 IL-6 polymorphism has been reported to be involved in bone loss,10 fracture,11 and osteoarthritis.12 In addition, the transforming growth factor (TGF-β), as a multifunctional growth factor and osteogenic factor, is reported to be abundant in bone and take leading to bone formation, differentiation, absorption, remodeling, and matrix metabolism.13 TGF-β SNPs include +896T/C (rs1982073), +915G/C (rs1800471), +29T/C (re1800470), −509C/T (rs1800469), it was associated with the susceptibility of aortic dissection,14 hepatitis15 and gastrointestinal adenocarcinoma.16 What’s more, in bone metabolism, IL-6 can affect the metabolism of calcium and vitamin D and affect the metabolism of connective tissue, especially cartilage and bone.17 It has also been reported that inhibition of the TGF-β signaling pathway, a key pathway in bone metabolism, differentially regulates the inflammatory mediators IL-6 and MCP-1 thereby further regulating bone metabolism.18
Recent studies have found that SNPs of IL-6 and TGF-β are associated with susceptibility to osteoporosis.19,20 Clinical studies have confirmed elevated IL-6 mRNA levels in OVCF patients,21 and IL-6 may promote RANKL levels in osteoblasts and activate its signaling pathway causing bone destruction.22 rs1800795 and rs1800796 are the two SNPs of IL-6 most studied, and rs1800796 is strongly related to the risk of osteoporosis.20 However, TGF-β rs1982073 was closely related to the low bone mineral density and was the main risk factor for osteopenia and osteoporosis.19,23 Therefore, we conducted this study to test our suspicion that IL-6 rs1800796 and TGF-β rs1982073 are potentially associated with OVCF.
Materials and Methods
Participants of This Research
The present research was a case–control study to evaluate the effects of IL6 rs1800796 and TGF-β rs1982073 on OVCF. Current research was conducted following the declaration of Helsinki with the approval by the Medical Ethics Committee of Shandong First Medical University and Shandong Academy of Medical Sciences (Approval NO. 201789) and informed consent of the subjects.
From June 2017 to December 2019, elderly patients diagnosed with thoracolumbar OVCF in our hospital were selected. Inclusion criteria were: a) patients > 60 years; b) patients diagnosed with T11-L2 single-level thoracolumbar OVCF on MRI and CT scan (defined as vertebral height loss > 25%),24 and there was tenderness or percussion pain in the vertebrae or lower lumbar vertebrae; c) The diagnostic criteria for osteoporosis are based on the criteria of the World Health Organization:25 the bone mineral density (BMD) T-score of −2.5 standard deviations (SD) or lower assessed by dual-energy X-ray absorptiometry (DEXA). Exclusion criteria included: a) pathological fracture caused by spine infection or tumor; b) with neurology defects; c) spinal surgery history and severe fractures; d) intake of drugs affecting bone metabolism such as bisphosphonates, calcium or vitamin D, hormones. Through the above screening, 146 patients with OVCF (61 male/85 female; mean age 71.9±4.21 years) were included. Meanwhile, 144 elderly people with osteoporosis (75 male/69 female; mean age 70.98±5.84 years) who came to our hospital for physical examination during the same period were selected as the control group. All of them were examined by DXA and the first finding of BMD was −2.5 or lower, and no intake of drugs affecting bone metabolism or anti-osteoporosis within the last six months. In addition, MRI and CI showed no evidence of fracture, and their age was matched to the patients with OVCF. The basic clinical information of both patients is recorded in Table 1.
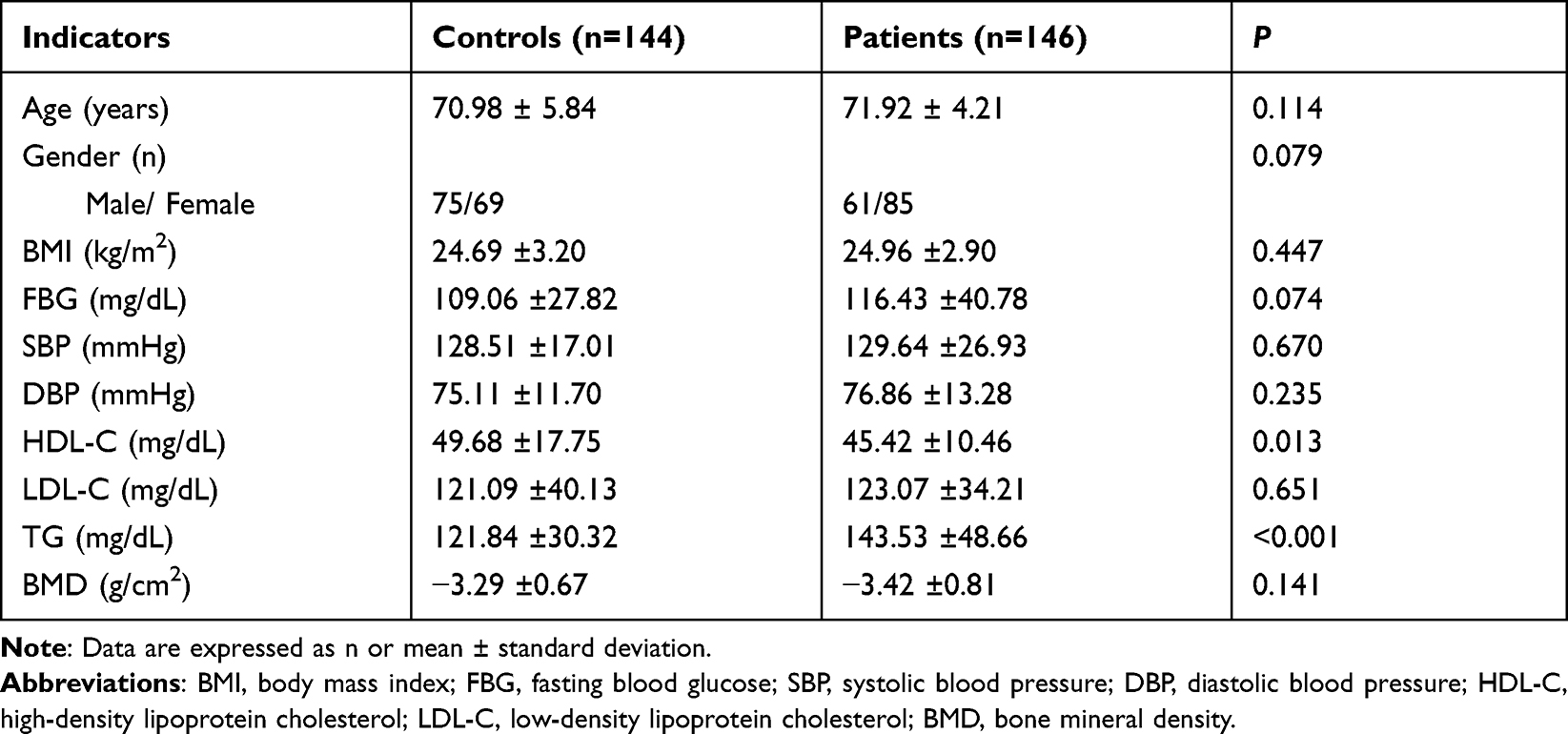 |
Table 1 Clinical Information of the Subjects |
Specimen Collection
Venous blood from each subject’s upper extremity was collected into an EDTA-coated anticoagulant tube. Partial blood samples from the subjects were used to analyze fasting blood glucose (FBG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), total cholesterol (TC), and triglyceride (TG) using the modular automatic biochemical analyzer (Olympus AU640). The remaining peripheral blood samples were used for genetic analyses. Some blood was centrifuged to collect the supernatant, and the expression levels of IL-6 and TGF-β in the subjects were measured using a commercial enzyme-linked immunosorbent assay kit.
DNA Extraction and Genotyping Analysis
According to the manufacturer's protocol, genomic DNA is extracted and isolated from peripheral venous blood using Tiangen DNA Extraction Kit. The concentration and purity (absorbance ratios from 1.8 to 2.0 at the length of A260/A280) of each DNA sample were measured on the NanoDrop 2000 spectrophotometer (Thermo Fisher Scientific) and stored at −20°C.
The amplification and genotyping of the polymorphic target fragments of IL-6 rs1800796 and TGF-β rs1982073 were performed by polymerase chain reaction (PCR) and sequencing. IL-6 rs1800796 was amplified by forward (5’-GGAGACGCCTTGAAGTAACTGC-3’) and reverse (5’-GAGTTTCCTCTGACTCCATCGCAG-3’) primers and TGF-β rs1982073 was amplified by forward (5’-TTCCCTCGAGGCCCTCCTA-3’) and reverse (5’-GCCGCAGCTTGGACAGGATC-3’) primers. The PCR procedure for DNA amplification was pre-denaturation at 95°C for 1 min, 40 cycles of denaturation at 95°C for the 30s, annealing at 55 °C for 30s, and extension at 72°C for 30s. PCR products were purified and analyzed by DNA sequencing by an automatic ABI3730xL DNA analyzer (Applied Biosystems). Perform genotype analysis on randomly selected (5%) samples by blind method, with 100% consistency.
Statistical Analysis
Analysis was performed by SPSS 23.0 software. Student’s t-test and ANOVA tests were applied to compare the differences between two or more groups, and the measurement data were presented by means and SD. The Chi-square test was performed on counting data, and it was applied to estimate the deviation of the genotype frequencies from the Hardy-Weinberg equilibrium (HWE). The association of IL-6 and TGF-β with OVCF susceptibility was measured by odds ratio (OR) and 95% confidence interval (CI). P < 0.05 was considered statistically significant.
Results
General Characteristics of Subjects
Demographic data of the participants are presented in Table 1. One hundred and forty-six patients with OVCF (61 male/85 female; mean age 71.9±4.21 years) and 144 controls (75 male/69 female; mean age 70.98±5.84 years) were included in this study. There was no significant difference between the two groups in age, gender, BMI, and biochemical indicators such as FBG, SBP, SDP, LDL-C, and BMD (P > 0.05). However, the level of HDL-C of OVCF patients was lower than that of the control group, the TG of patients was significantly higher than that of the control group (P < 0.05). In addition, ELISA was also applied to detect the difference in serum levels of IL-6 and TGF-β between the two groups, and it was confirmed that the serum levels of IL-6 were significantly higher in patients than in controls, while TGF-β was significantly lower (P < 0.001, Figure 1).
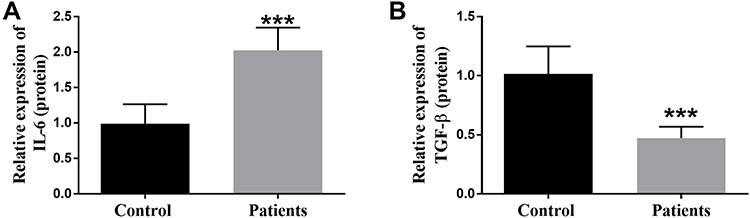 |
Figure 1 The expression levels of IL-6 (A) and TGF-β (B) in controls and patients serum were measured by enzyme-linked immunosorbent assay. ***P < 0.001 versus the Control groups. |
Association Between IL-6 rs1800796 Polymorphism and OVCF Risk
Alleles and genotype frequencies of IL-6 rs1800796 of subjects are presented in Table 2. The control group of 144 subjects met the HWE of genotype distributions (P > 0.05). And compared with the control group, the frequency of the G allele of IL-6 rs1800796 was higher in the OVCF group (40.07% vs 28.47%, P < 0.01). In addition, GG of IL-6 rs1800796 genotype was more common in patients with OVCF than in controls (19.18% vs 7.64%, P < 0.01). What’s more, allele G of IL-6 rs1800796 was associated with higher risk by 1.68-fold of OVCF (95% CI=1.187–2.376), and genotype GG was associated with a 3.394-fold higher risk of OVCF (95% CI 1.56–7.385). The results suggest that the G allele and GG genotype of IL-6 rs1800796 are more common in patients with OVCF and are associated with OVCF susceptibility.
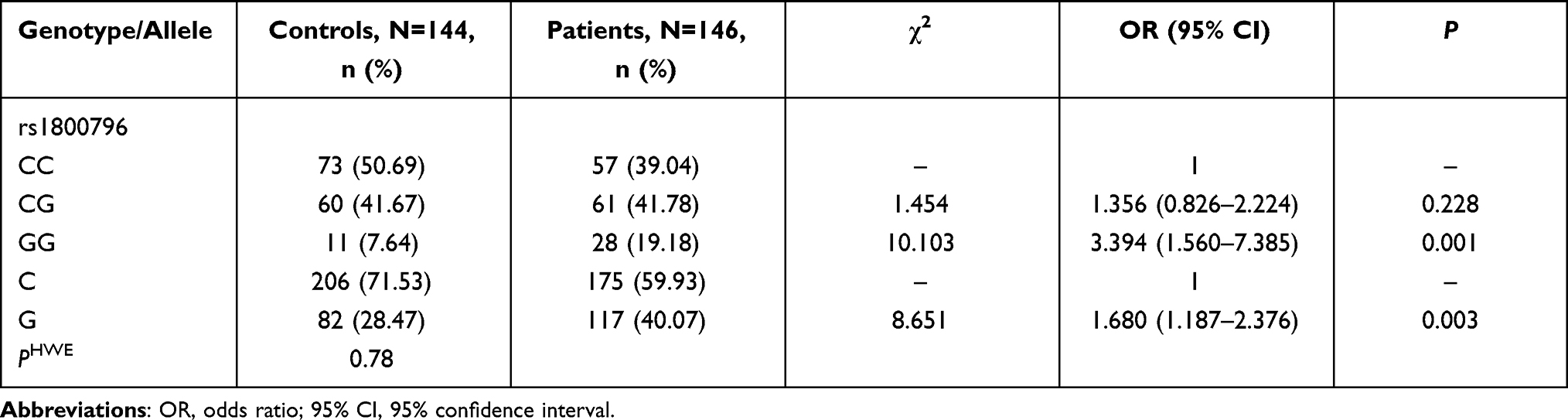 |
Table 2 Frequency Distribution of IL-6 Gene rs1800796 Genotype and Allele in Controls and Patients Groups |
Association Between TGF-β rs1982073 Polymorphism and OVCF Risk
Subsequently, alleles and genotype frequencies of TGF-β rs1982073 in the control group and OVCF group were also analyzed. The distribution of genotypes in controls did not deviate from HWE (P > 0.05, Table 3). The frequency of the T allele was lower in the patients with OVCF than in the control group (40.75% vs.52.08%, P =0.004). Similarly, CT and TT genotypes were significantly reduced in patients with OVCF and were more common in controls (41.78% vs 51.39%; 26.39% vs.19.86%, P < 0.05). Furthermore, the TGF-β rs1982073 T allele was associated with a low risk of OVCF (OR = 0.615, 95% CI= 0.443–0.855, P = 0.004), and CT (OR = 0.471, 95% CI=0.272–0.817, P = 0.007) and TT (OR=0.436, 95% CI=0.228–0.835, P = 0.012) genotypes were associated with lower OVCF compared with genotype CC. The results suggest that TNF-β rs1982073 T allele and genotype CT and TT are associated with a low risk of OVCF.
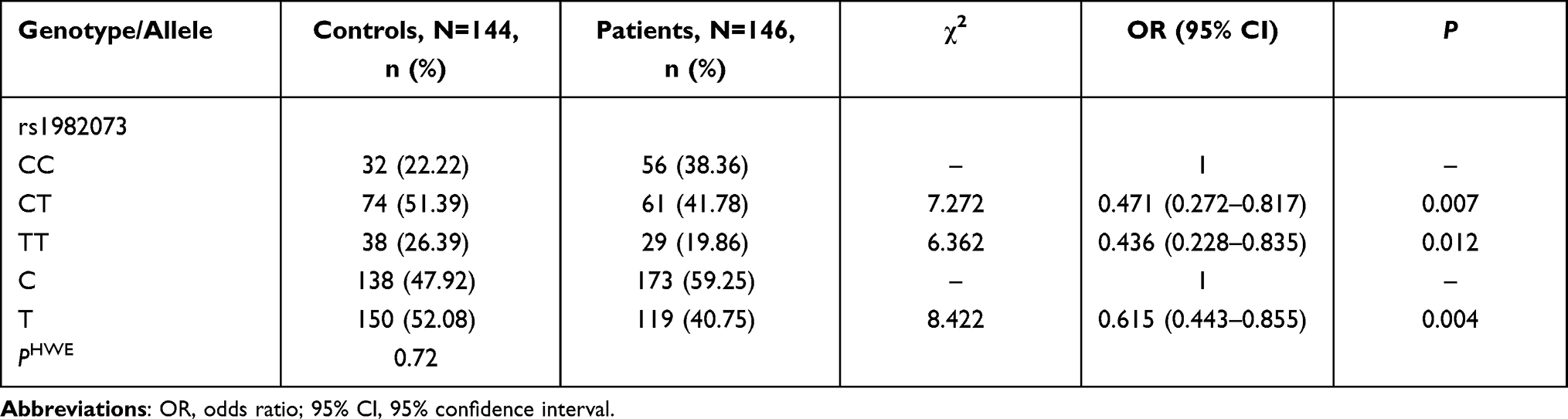 |
Table 3 Frequency Distribution of TGF-β Gene rs1982073 Genotype and Allele in Controls and Patients Groups |
Discussion
Vertebral fractures are the most common outcome and complication of osteoporosis, especially OVCF, and occur most frequently in the thoracolumbar lumbar segment.26 When patients with osteoporosis are hit by external forces such as falls and traffic accidents, and a load of external forces exceeds the load limit that the vertebral body can bear, kyphosis of the vertebral body and thoracolumbar fracture damage will result in OVCF of the thoracolumbar segment.27 And it is more common in the elderly population, its morbidity and mortality are high.28 However, conservative treatment such as bed rest, immobilization, analgesia, and bracing should only be used in patients without neurological dysfunction.29 Surgical treatments such as percutaneous kyphoplasty (PKP) have been widely used to treat OVCF, but have the disadvantages of refracture, back pain, infection, and adjacent vertebral fractures.30 Recent investigations have shown that the role of genetic factors, including gene polymorphism, is central in pathogenicity studies and has a synergistic effect with OVCF risk factors.31 Therefore, polymorphic studies can effectively screen the high-risk elderly population for OVCF occurrence and effectively prevent its occurrence in the early stage. Recent studies have emphasized the regulatory role of bone and immune cells as well as immune cell products such as cytokines, chemokines, and growth factors on bone resorption and bone formation. In this study, we investigated the association between the polymorphisms of IL-6 rs1800796 and TGF-β rs1982073 and the occurrence of OVCF in the thoracolumbar segment. In addition to OVCF patients, osteoporosis patients were also recruited as the control group. There were no remarkedly differences in clinical basic information and BMD between the two groups. However, HDL-C was decreased and TG was significantly elevated in OVCF patients, which was consistent with previous studies.32 This suggests that the subjects in our study are representative to a certain extent.
IL-6 is a multifunctional chemotactic cytokine secreted by macrophages, Th12 cells, and endothelial cells, which take a leading role in regulating inflammation and immune response. The latest investigation has found that IL-6 is also a key regulator of osteoblast formation, bone resorption, and fracture. Studies have shown that after a hip injury, IL-6 levels can be detected within 1h, and the concentration increases to a peak within 4–6h.33 In mice, the level of IL-6 reached the peak at 24h after fracture.34 IL-6 gene is located on chromosome 7q21.3 and contains 5 exons and 4 introns. At present, its common promoter regions SNPs included rs1800796, rs1800795, rs1800797, and rs10499563.35 Among them, rs1800796 confirmed to be the most common SNP in Asian populations,36 is the 572-cytosine mutation to guanine, which promotes the transcription of IL-6 promoter and causes an abnormal increase of IL-6 level.
One study found that rs1800796 was associated with fractures in older women compared with other SNPs of IL-6.11 More importantly, IL-6 rs1800796 were significantly correlated with BMD, while BMD is a key indicator of bone strength and the most effective predictor of fracture risk.37 What’s more, osteoporosis is a common complication and clinical outcome of OVCF, and IL-6 rs1800796 is also associated with osteoporosis.37 Therefore, we suspected that IL-6 rs1800796 might be related to OVCF. To verify our hypothesis, we conducted a case–control study and found that the G allele frequency of IL-6 rs1800796 was 28.47% in the control group and 40.07% in OVCF patients, which was remarkedly higher than the controls. The CG genotype did not differ significantly between the two groups, but the purified GG genotype was more common in the case group. We also found that both the G allele and GG genotype of rs1800796 polymorphism of IL-6 were related to a higher risk of OVCF.
TGF-β belongs to the TGF-β superfamily and is a pleiotropic cytokine and immunomodulator, which not only participates in the immune response but also plays a key role in normal development and physiology. In addition, TGF-β also is synthesized by osteoblasts and is highly expressed in bone, and its level is related to the proliferation and differentiation of osteoblasts.38 In addition, osteoblasts produce TGF-β, which is secreted in a latent form and then deposited into the bone matrix. During the resorption phase, osteoblasts release and activate TGF-β from the bone matrix so that this molecule affects the bone microenvironment. Also TGF-β binds to bone resorption and formation and recruits bone progenitor cells to the site of bone resorption.39 TGF-β gene is located in the long arm of chromosome 19, and the gene is described as 5 SNPs, which are −800G/A (rs1800468) and −509C/T (rs1800469) promoter region and +896T/C (rs1982073), +915G/C (rs1800471), +29T/C (re1800470) coding region, respectively. Multiple studies have confirmed that TGF-β polymorphism is associated with disease susceptibility. Such as rs1982073 and rs1800471 were associated with psoriasis susceptibility.40 Importantly, it was found that TGF-β rs1982073 may be related to the risk of fracture osteoporosis, and osteoarthritis.41 Genotype CT+CC of TGF-β rs1982073 is significantly reduced in patients with osteopenia or osteoporosis in the lumbar spine and tibia.42 As OVCF is a common complication and clinical outcome of osteoporosis, we focused on the correlation between the allele and genotype of TGF-β rs1982073 and OVCF. Similar to the genotypes in osteoporosis, rs1982073 CT and TT genotypes were more common in osteoporosis patients and significantly reduced in OVCF patients. The T allele was also more common in osteoporosis patients and significantly reduced in patients. And TGF-β rs1982073 T allele and CT and TT genotypes were related to low risk of OVCF. That is, CC genotype and allele C are more relevant to patients with OVCF. Finally, a major limitation of this study was the failure to examine in time the G allele and GG genotype of IL-6 re1800796 as well as the CT and TT genotypes and T allele of TGF-β rs1982073 in predicting the potential risk of vertebral compression fractures in patients with osteoporosis. This will be addressed in our next in-depth study. In addition, to ensure that two groups were comparable, we therefore included osteoporotic patients with no significant difference in BMD as a control group, which narrowed the effect of BMD in this study, which is a limitation of this study, and this will be noted in the next studies.
Conclusion
In conclusion, our current study shows that the G allele and GG genotype of IL-6 rs1800796 may contribute to increased susceptibility to OVCF in elderly Chinese. In contrast, CT and TT genotypes and the T allele of TGF-β rs1982073 may contribute to lower susceptibility of OVCF.
Ethics Statement
The current research was conducted following the declaration of Helsinki with the approval of the Shandong First Medical University and Shandong Academy of Medical Sciences Ethics Committee and informed consent of the subjects.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Huang D, Ying J, Xu D, et al. Comparison of percutaneous kyphoplasty with or without pedicle screw fixation in osteoporotic thoracolumbar vertebral fractures: a Retrospective Study. Dis Markers. 2021;2021:4745853. doi:10.1155/2021/4745853
2. Ballane G, Cauley JA, Luckey MM, El-Hajj Fuleihan G. Worldwide prevalence and incidence of osteoporotic vertebral fractures. Osteoporos Int. 2017;28(5):1531–1542. doi:10.1007/s00198-017-3909-3
3. Lai PL, Tai CL, Chen LH, Nien NY. Cement leakage causes potential thermal injury in vertebroplasty. BMC Musculoskelet Disord. 2011;12:116. doi:10.1186/1471-2474-12-116
4. Vincze A, Gaal J, Griger Z. Bone health in idiopathic inflammatory myopathies: diagnosis and management. Curr Rheumatol Rep. 2021;23(7):55. doi:10.1007/s11926-021-01016-8
5. Ahn TK, Kim JO, An HJ, et al. 3’-UTR Polymorphisms of Vitamin B-related genes are associated with osteoporosis and osteoporotic vertebral compression fractures (OVCFs) in postmenopausal women. Genes. 2020;11(6). doi:10.3390/genes11060612
6. Alkhuriji AF, Al Omar SY, Babay ZA, et al. Association of IL-1beta, IL-6, TNF-alpha, and TGFbeta1 gene polymorphisms with recurrent spontaneous abortion in polycystic ovary syndrome. Dis Markers. 2020;2020:6076274. doi:10.1155/2020/6076274
7. Karcioglu Batur L, Hekim N. Correlation between interleukin gene polymorphisms and current prevalence and mortality rates due to novel coronavirus disease 2019 (COVID-2019) in 23 countries. J Med Virol. 2021;93(10):5853–5863. doi:10.1002/jmv.27127
8. Rai H, Colleran R, Cassese S, Joner M, Kastrati A, Byrne RA. Association of interleukin 6-174 G/C polymorphism with coronary artery disease and circulating IL-6 levels: a systematic review and meta-analysis. Inflamm Res. 2021;70:1075–1087. doi:10.1007/s00011-021-01505-7
9. Martinez-Ramirez OC, Salazar-Pina DA, de Lorena RM, et al. Association of NFkappabeta, TNFalpha, IL-6, IL-1beta, and LPL polymorphisms with Type 2 diabetes mellitus and biochemical parameters in a Mexican population. Biochem Genet. 2021;59(4):940–965. doi:10.1007/s10528-021-10047-w
10. Moffett SP, Zmuda JM, Cauley JA, et al. Association of the G-174C variant in the interleukin-6 promoter region with bone loss and fracture risk in older women. J Bone Miner Res. 2004;19(10):1612–1618. doi:10.1359/JBMR.040707
11. Ponce de Leon-suarez V, Valdes-Flores M, Miranda-Duarte A, et al. Association of the IL6 rs1800796, but not of the IL6 rs1800795, IL6R rs4845617 and rs2228145 polymorphisms with hip fracture in elderly Mexican women. Aging Clin Exp Res. 2018;30(4):407–410. doi:10.1007/s40520-017-0779-7
12. Oldefest M, Dusterhoft S, Desel C, et al. Secreted Frizzled-related protein 3 (sFRP3)-mediated suppression of interleukin-6 receptor release by A disintegrin and metalloprotease 17 (ADAM17) is abrogated in the osteoarthritis-associated rare double variant of sFRP3. Biochem J. 2015;468(3):507–518. doi:10.1042/BJ20141231
13. Badshah Y, Shabbir M, Hayat H, et al. Genetic markers of osteoarthritis: early diagnosis in susceptible Pakistani population. J Orthop Surg Res. 2021;16(1):124. doi:10.1186/s13018-021-02230-x
14. Chang Y, Yuan Q, Jiang P, Sun L, Ma Y, Ma X. Association of gene polymorphisms in MYH11 and TGF-beta signaling with the susceptibility and clinical outcomes of DeBakey type III aortic dissection. Mamm Genome. 2021;4:1–9.
15. Noh IC, Ahmad I, Suraiya S, Musa NF, Nurul AA, Ruzilawati AB. Cytokine (IL-10, IL-6, TNF-alpha and TGF-beta1) gene polymorphisms in chronic Hepatitis C Virus infection among Malay male drug abusers. Biomedicines. 2021;9(9). doi:10.3390/biomedicines9091115
16. Zhang Q, Liu F, Qin L, et al. Characterization of TGFbeta-associated molecular features and drug responses in gastrointestinal adenocarcinoma. BMC Gastroenterol. 2021;21(1):284. doi:10.1186/s12876-021-01869-4
17. Harsanyi S, Zamborsky R, Krajciova L, Kokavec M, Danisovic L. Genetic study of IL6, GDF5 and PAPPA2 in association with developmental dysplasia of the hip. Genes. 2021;12(7). doi:10.3390/genes12070986
18. Geurts J, Juric D, Muller M, Scharen S, Netzer C. Novel ex vivo human osteochondral explant model of knee and spine osteoarthritis enables assessment of inflammatory and drug treatment responses. Int J Mol Sci. 2018;19(5):1314.
19. Sun J, Zhang C, Xu L, Yang M, Yang H. The transforming growth factor-beta1 (TGF-beta1) gene polymorphisms (TGF-beta1 T869C and TGF-beta1 T29C) and susceptibility to postmenopausal osteoporosis: a meta-analysis. Medicine. 2015;94(4):e461. doi:10.1097/MD.0000000000000461
20. Chen B, Li HZ. Association of IL-6 174G/C (rs1800795) and 572C/G (rs1800796) polymorphisms with risk of osteoporosis: a meta-analysis. BMC Musculoskelet Disord. 2020;21(1):330. doi:10.1186/s12891-020-03334-x
21. Ralston SH. Do genetic markers aid in risk assessment? Osteoporos Int. 1998;8 Suppl 1:S37–42.
22. Arron JR, Choi Y. Bone versus immune system. Nature. 2000;408(6812):535–536. doi:10.1038/35046196
23. Taha IM, Abdu Allah AM, Hamoudah MAF, Justin Carlus S. Transforming growth factor-beta1 gene polymorphism and osteoporosis in postmenopausal Egyptian women. Cell Mol Biol (Noisy-le-Grand). 2017;63(11):53–57. doi:10.14715/cmb/2017.63.11.10
24. Lei F, He W, Tian X, et al. Prophylactic percutaneous kyphoplasty treatment for nonfractured vertebral bodies in thoracolumbar for osteoporotic patients. Biomed Res Int. 2020;2020:8593516. doi:10.1155/2020/8593516
25. Kanis JA, Kanis JA. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: synopsis of a WHO report. WHO Study Group. Osteoporos Int. 1994;4(6):368–381. doi:10.1007/BF01622200
26. Wang E, Lin J, Xu G, Wang X, Chen M. Effect of PKP on serum sost in patients with VERTEaBRAL compression fractures. Acta Ortop Bras. 2020;28(6):323–326. doi:10.1590/1413-785220202806228603
27. Wang C, Zhang Y, Chen W, Yan SL, Guo KJ, Feng S. Comparison of percutaneous curved kyphoplasty and bilateral percutaneous kyphoplasty in osteoporotic vertebral compression fractures: a randomized controlled trial. BMC Musculoskelet Disord. 2021;22(1):588. doi:10.1186/s12891-021-04469-1
28. Ahn TK, Kim JO, Kumar H, et al. Polymorphisms of miR-146a, miR-149, miR-196a2, and miR-499 are associated with osteoporotic vertebral compression fractures in Korean postmenopausal women. J Orthop Res. 2018;36(1):244–253. doi:10.1002/jor.23640
29. Ji C, Rong Y, Wang J, et al. Risk factors for refracture following primary osteoporotic vertebral compression fractures. Pain Physician. 2021;24(3):E335–E340.
30. Feng L, Feng C, Chen J, Wu Y, Shen JM. The risk factors of vertebral refracture after kyphoplasty in patients with osteoporotic vertebral compression fractures: a study protocol for a prospective cohort study. BMC Musculoskelet Disord. 2018;19(1):195. doi:10.1186/s12891-018-2123-6
31. Kim JO, Han SH, Lee YH, et al. Association of plasminogen activator inhibitor-1 (PAI-1) gene polymorphisms with osteoporotic vertebral compression fractures (OVCFs) in postmenopausal women. Int J Mol Sci. 2016;17(12). doi:10.3390/ijms17122062
32. Wang Y, Dai J, Zhong W, Hu C, Lu S, Chai Y. Association between serum cholesterol level and osteoporotic fractures. Front Endocrinol (Lausanne). 2018;9:30. doi:10.3389/fendo.2018.00030
33. Xiong Z, Cao S, Zhou L, et al. Intraoperative periarticular injection can alleviate the inflammatory response and enhance joint function recovery after hip arthroplasty in elderly patients with osteoporotic femoral neck fractures. Medicine. 2021;100(7):e24596. doi:10.1097/MD.0000000000024596
34. Chen L, Cheng S, Sun K, et al. Changes in macrophage and inflammatory cytokine expressions during fracture healing in an ovariectomized mice model. BMC Musculoskelet Disord. 2021;22(1):494. doi:10.1186/s12891-021-04360-z
35. He B, Pan B, Pan Y, et al. IL-4/IL-4R and IL-6/IL-6R genetic variations and gastric cancer risk in the Chinese population. Am J Transl Res. 2019;11(6):3698–3706.
36. Park BL, Lee HS, Kim YJ, et al. Association between interleukin 6 promoter variants and chronic hepatitis B progression. Exp Mol Med. 2003;35(2):76–82. doi:10.1038/emm.2003.11
37. Eftekhari H, Hosseini SR, Pourreza Baboli H, et al. Association of interleukin-6 (rs1800796) but not transforming growth factor beta 1 (rs1800469) with serum calcium levels in osteoporotic patients. Gene. 2018;671:21–27. doi:10.1016/j.gene.2018.05.118
38. Xu X, Yang J, Ye Y, et al. SPTBN1 Prevents primary osteoporosis by modulating osteoblasts proliferation and differentiation and blood vessels formation in bone. Front Cell Dev Biol. 2021;9:653724. doi:10.3389/fcell.2021.653724
39. Greene B, Russo RJ, Dwyer S, et al. Inhibition of TGF-beta increases bone volume and strength in a mouse model of osteogenesis imperfecta. JBMR Plus. 2021;5(9):e10530. doi:10.1002/jbm4.10530
40. Ahmed BT, Saeed MY, Noori SH, Amin DM. TGF-beta1 gene polymorphism and its correlation with serum level of TGF-beta1 in Psoriasis Vulgaris among Iraqi people. Clin Cosmet Investig Dermatol. 2020;13:889–896. doi:10.2147/CCID.S281585
41. Cong Y, Ru JY, Bao NR, Guo T, Zhao JN. A single nucleotide polymorphism in the TGF-β1 gene (rs1982073 C>T) may contribute to increased risks of bone fracture, osteoporosis, and osteoarthritis: a meta-analysis. Clin Rheumatol. 2016;35(4):973–985. doi:10.1007/s10067-014-2840-7
42. Utennam D, Tungtrongchitr A, Phonrat B, Tungtrongchitr R, Preutthipan S. Association of T869C gene polymorphism of transforming growth factor-beta1 with low protein levels and anthropometric indices in osteopenia/osteoporosis postmenopausal Thai women. Genet Mol Res. 2012;11(1):87–99. doi:10.4238/2012.January.13.2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.