")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Association of Higher Rates of Type 2 Diabetes (T2DM) Complications with Psychological and Demographic Variables: Results of a Cross-Sectional Study
Authors Łukasiewicz A, Cichoń E, Kostecka B, Kiejna A, Jodko-Modlińska A, Obrębski M , Kokoszka A
Received 14 April 2022
Accepted for publication 14 September 2022
Published 28 October 2022 Volume 2022:15 Pages 3303—3317
DOI https://doi.org/10.2147/DMSO.S369809
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Gian Paolo Fadini
Agnieszka Łukasiewicz,1 Ewelina Cichoń,2,3 Barbara Kostecka,4 Andrzej Kiejna,2,3 Aleksandra Jodko-Modlińska,4 Marcin Obrębski,4 Andrzej Kokoszka4
1Faculty of Nursing in Warsaw, University of Humanities and Economics in Lodz, Warsaw, Poland; 2Institute of Psychology, WSB University in Toruń, Toruń, Poland; 3Collegium of Psychological Studies, University of Lower Silesia, Wrocław, Poland; 4 2nd Department of Psychiatry, Medical University of Warsaw, Warsaw, Poland
Correspondence: Andrzej Kokoszka, Tel/Fax +48 22 326 58 92, Email [email protected]
Introduction: The aim of this study was to assess the relationship between the occurrence and number of T2DM complications with sociodemographic (age, sex, habitation, education), clinical (duration of diabetes, HbA1c (%), BMI) and psychological (well-being, sense of influence on the diabetes course, coping styles) variables.
Methods: A total of 2574 adult patients were assessed using The Sense of Influence on the Diabetes Course Scale, WHO-5 Well-Being Index, and the Brief Method of Evaluating Coping with Disease. Hierarchical Regression Analysis was conducted with number of complications as the dependent variable and three sets of variables entered in sequential steps: (a) sociodemographic; (b) clinical and (c) psychological factors. Logistic regression analysis was used to examine the association of these variables with diabetes complications’ occurrence.
Results: A higher number of complications and higher odds ratios of occurrence of complications were associated with sociodemographic and clinical variables, poor well-being, low perception of influence on the diabetes course, and an emotion-oriented coping style. The logistic regression indicated that participants with HbA1c > 7% (in comparison with HbA1c ≤ 7%) and with high risk of depression (in comparison with no risk of depression) had respectively 68% and 86% higher odds of developing complications.
Discussion: The number of complications has weak but statistically significant relations with psychological and clinical factors.
Conclusion: The results support the rationale of including the psychosocial factors in the context of diabetes management.
Keywords: type 2 diabetes, glycemic control, psychosocial factors, HbA1c, diabetes complications, well-being
Introduction
Epidemiological data indicate a global increase of diabetes prevalence and estimate the number of patients at 415 million.1 Despite having access to appropriate diagnostic and treatment methods, a significant number of patients with type 2 diabetes mellitus (T2DM) do not comply optimally with therapeutic recommendations (in particular with appropriate diet and exercise) and have long-term excessively high blood glucose levels, which leads to serious complications related to angiopathic, neuropathic, nephropathic, and retinopathic changes. The number of complications has rarely been considered in studies, despite being an important indicator of the severity of diabetes and risk of mortality. A study by Young et al2 has shown that people with 1 complication did not have an increased risk of death, while in patients with 2 complications, the risk of death was almost double (hazard ratio [HR] = 1.90, 95% confidence interval [CI] = [1.27–2.83]); in people with 4 complications, it was almost 3.5-fold greater, and in people with 5 or more complications it was over 7 times higher. The analysis of the operating characteristic curves showed that both the Diabetes Complications Severity Index and the simple complication rate are good predictors of mortality2.
It is worth noting that according to the recent guidelines of the American Diabetes Association,
Building positive health behaviors and maintaining psychological well-being are foundational for achieving diabetes treatment goals and maximizing quality of life.3
There are only a few studies that take into account the relationship between psychosocial factors and the number of diabetes complications. A study by Lang et al4 is one of the few that assessed this relationship. Among 10,246 consecutive patients with T2DM aged >40 years (M = 65.7; SD = 10.05) and suffering from diabetes for ≥3 years (M = 7.00; SD = 5.00), complications were observed in 53.1% (polyneuropathy [32.4%], cardiovascular diseases [17.2%], retinopathy [5.6%], nephropathies [5.6%], nonhealing wounds [3%], amputation [0.9%]).4 The mean number of complications was 1.5 (SD = 1.95). There was a weak but significant correlation of the number of complications with age only (Spearman rho = 0.15; p < 0.001), but few variables, including no psychosocial ones, were controlled. In a study by Habtewold et al,5 only depression was found to be associated with ≥3 complications; Nouwen6 also found 2-way relationships between depression and the number of complications. Other studies have shown that when diabetes duration is controlled, the rates of hypoglycemia, rates of cardiovascular complications, and mortality increase sharply with age, but the rates of microvascular complications remain stable or decrease.7
Only few studies have so far investigated the number of diabetes complications. Most of the work to date has focused on identifying factors related to the occurrence of individual complications (eg, cardiovascular and vascular). The greatest attention was paid to depression and its associations with vascular complications. A meta-analysis of 9 longitudinal studies involving over 1 million patients from 5 countries has found that depression was associated with a 38% increase in risk of macrovascular complications (HR = 1.38; 95% CI: 1.30–1.47) and 33% risk of microvascular complications (HR = 1.33; 95% CI: 1.25–1.41).6 A meta-analysis of 27 cross-sectional studies revealed significant associations of depression with retinopathy, nephropathy, neuropathy, macroangiopathy, and sexual dysfunctions.8 A literature review suggests a bidirectional relation between depression and the occurrence of diabetes complications. Results of a study of 385 patients with T2DM, among whom depression was diagnosed in 37.6%, suggest the presence of the following risk factors: diabetic foot, cardiovascular diseases, eye complications and erectile dysfunction.9 The occurrence of depression was not related to age, sex, duration of diabetes, and glycated hemoglobin (HbA1c) levels. In a similar study involving 264 people with T2DM, depression was diagnosed in 44.7% of patients, and the results’ analysis showed that the risk factors included: low monthly income per family, presence of ≥3 diabetes complications, presence of diabetic nephropathy, negative life events, and low level of social support.5 As suggested in a study by Tyagi et al,10 obesity in T2DM patients may be associated with a higher risk of developing stress and depression.
As shown above, psychological factors beyond depression are rarely taken into account in studies on diabetic complications. As far as clinical variables are considered, attention is also drawn to the fact that the duration of diabetes is an important factor in the pathogenesis of complications.11–13 Sociodemographic variables constitute an important group of factors that are rarely analyzed in the context of diabetes complications. Sociodemographic factors associated with the risk of diabetes complications are mainly age and sex.7,14,15 For example, it has been shown that men with diabetes are at greater risk of developing vascular complications than women; other sociodemographic variables, such as age and place of residence, were not significant predictors of vascular complications.14
The analysis of literature used to develop the Psychodiabetic Kit16 shows that apart from depression, also styles of coping with stress and, above all, the perception of self-influence on the disease course, are among the most important psychological factors related to diabetes management.16 It is worth mentioning that with appropriate therapeutic interventions, psychological factors accompanying diabetes can be significantly improved, which was proved in the study by Jiang et al,17 with 265 type 2 diabetes patients. In comparison to routine education, the self-efficacy-focused structured education program (SSEP) resulted in increasing diabetes self-efficacy, diabetes self-management behaviors, diabetes knowledge and reducing diabetes distress during the 12-month follow-up. Sustainable benefits in low-density lipoprotein, HbA1c level, waist circumference, and total cholesterol were also noted.
Perception of self-influence on the disease course is defined as
The extent of belief about one’s own abilities to shape the disease course.16
Patients’ lifestyle and compliance with medical recommendations have an impact on the course of the disease. Taking pro-health measures by patients and their involvement in the therapeutic process depend on their perception of self-influence on the diabetes course. The usefulness of this concept has been confirmed in other studies, where it was related to the management of disease in patients with schizophrenia and in those receiving dialysis therapy.18–21
Coping is most strongly associated with perception of self-influence on the disease course. The lack of it or a very low perception of self-influence on a stressor implies activation of avoidance or emotion-oriented coping. Coping is an adaptation activity that takes effort and aims to diminish physical, social, or psychological burdens linked to stressful life events.22,23 According to the authors of one of the most frequently cited study, coping styles can be classified as emotions-oriented, avoidance-oriented, or task-oriented.23 This classification was expanded by the best solution–oriented coping style.16,24 The coping styles mentioned above can be further divided into maladaptive (emotions, avoidance) and adaptive (task, best solution). The use of task-oriented coping styles or a search for the best solution requires experiencing some degree of sense of influence on the disease, and the lack of it is associated with the use of emotions-oriented or avoidance-oriented styles. The concepts of the perception of self-influence on the disease course and coping styles have been used in research on diabetes. Results from a study of a large group of people with T2DM have indicated that patients who had problems with adherence to treatment when switching from human insulin to its analogues had a low perception of self-influence on the disease course and used maladaptive coping styles.25 A series of studies has shown that people using maladaptive coping styles and those who have a low sense of perception of self-influence on the disease course choose less advanced insulin injectors than people with a high perception of self-influence on the disease course and using adaptive coping styles.26,27 In people with T2DM, a low perception of self-influence on the disease course is associated with high HbA1c levels, while a high perception of self-influence on the disease course is related to a lower risk of excessive body-mass index (BMI) in this group of patients.28
Aim
The aim of this study was to assess the relationship between the number of complications of diabetes with psychological factors (well-being, sense of influence on the diabetes course, coping styles), sociodemographic variables (age, sex, education, place of residence) and clinical variables (disease duration [years], BMI [kg/m2], HbA1c [%]).
Materials and Methods
This work is a part of the project “Psychosocial factors related to adherence to the recommendations of therapy with two-phase insulin analogues”.25 A previous article presents the relationship between well-being, coping styles, perception of self-influence on the diabetes course as well as sociodemographics with HbA1c and BMI among people with advanced type 2 diabetes.28 This study is the second part of the data analysis and focuses on factors related to the number of diabetes complications.
Study Design
An observational study was carried out during regular visits, conducted by 343 doctors experienced in clinical studies. The outpatient clinics operated by the researching physicians were situated all over Poland. The study enrolled 2574 consecutive adult participants with T2DM.
Diabetes was diagnosed according to the Polish guidelines;29 thus, the sample included patients with symptoms of hyperglycemia and random blood glucose concentration ≥200 mg/dL (≥11.1 mmol/L) or fasting glucose ≥126 mg/dL (≥7.0 mmol/L, based on 2 measurements on separate occasions), or blood glucose at 120 minutes during an oral glucose tolerance test (OGTT) ≥200 mg/dL (≥11.1 mmol/L). Patients had to be adults and were selected using diagnostic criteria of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) for the non–insulin-dependent diabetes mellitus (E11).30 The other inclusion criteria were: accessibility of data on HbA1c (%) levels and a switch to treatment with an insulin analogue after previous use of human insulin mixtures. The study was conducted during standard medical visits between days 1 and 61 of treatment with insulin analogues; thus, it is highly possible that the HbA1c (%) levels analyzed were from the period of treatment with human insulin mixtures. The number of patients who declined participation in the study was not controlled.
Ethical Considerations
The protocol of the study was approved by the Bioethics Committee of the Medical University of Warsaw, Poland. All patients were presented with oral and written information about the research. All participants gave their written informed consent after a thorough explanation of the procedures involved and prior to participation/inclusion in the study. The study conformed to the principles outlined in the Declaration of Helsinki.31
Research Tools and Measurements
Data on sociodemographics, disease course and course of treatment were collected from patients’ medical records and included information about age, sex, level of education, place of residence, height and weight, duration of diabetes, HbA1c levels (%), presence and type of diabetes complications, previous treatment with human insulin, treatment duration (years), current treatment with insulin analogues, and date of therapy change. BMI (kg/m2) was calculated based on height and weight data obtained from medical records. The study was conducted during regular medical visits; therefore, the measurement of psychological factors was limited to brief methods. Tools used to measure psychological variables are recommended by the Polish Diabetes Association, they have also been extensively described in literature, and presented during conferences and workshops for physicians. Therefore, most of the Polish doctors were familiar with the measurement methods, which included:
The clinical assessment of the sense of patients’ influence on the diabetes course was assessed by a physician on the Likert scale, which was used when creating the Brief Measure to Assess Perception of Self-Influence on the Disease Course, version for diabetes.32 The physicians’ evaluation score was based on the clinical knowledge of the patient and ranged from 0 to 4, where 0 represented the lowest possible sense of influence (no influence), and 4, the highest sense of influence on the diabetes course.
A more detailed description of the ranges is the following:
0 – Very low sense of influence: patients passively undergo treatment or avoid it, do not attach importance to their health condition, have unreflective expectations of simple and uncomplicated recommendations, do not see the relationship between their own behavior (forgetting about medications, forgetting about visits) and their health, refuse to participate in educational activities, do not adhere to dietary and exercise recommendations.
4 – Very high sense of influence: patients are interested in their disease and its treatment and actively participate in it, they use the available methods of education and are aware of the possibility of reducing the risk of complications by systematically following all therapeutic recommendations.
The WHO-5 Well-Being Index was initially used mainly in the diagnosis of depression in the general population of elderly people at risk of developing mental disorders.33 Currently, it is a tool with a wide range of applications, including the international study of Diabetes Attitudes Wishes and Needs and Diabetes Attitudes Wishes and Needs 2 (DAWN2).34,35 The use of the WHO-5 Well-Being Index to assess the outcomes of psychiatric treatment in a day ward was also described; the tool was used as one of the methods of assessing depression in the international study of this mood disorder in diabetes.36,37
A recent study indicated that the Polish version of the WHO-5 Well-Being Index is a reliable and valid outcome measure for outpatients with T2DM, and can be useful in screening for depression in diabetic patients.38 The sensitivity of this scale for depression screening is 93%, and specificity, 64%. In our study, the reliability of the WHO-5 Well-Being Index was high (Cronbach α = 0.876).
The following score ranges were indicated for the risk of depression: >13 points – no risk of depression; 8–13 points – requiring clinical verification of depression; ≤7 points or at least one of the questions rated with 0 or 1 – high probability of depression.
The questionnaire consists of 4 descriptions of stressful situations and 4 possible answers – alternative behaviors, which correspond to 4 styles of coping with stress, focused on: avoidance, emotions, task, and search for the best solution. Reliability for individual styles of coping with stress, measured with the Cronbach coefficient, in the version for men is: α = 0.67 for the avoidance-oriented style; 0.68 for the emotions-oriented style; 0.75 for the task-oriented style, 0.59 for the best solution–oriented style. In the version for women, these values are, respectively, 0.65, 0.67, 0.71, and 0.55.
For the purpose of this study, 2 items were distinguished, the total results of which correlate to the greatest extent with the result of the entire questionnaire. The 2 selected questions concern the attitude towards health and social problems. In some of the analyzes, responses to questions were aggregated, distinguishing between adaptive (task-oriented and best solution–oriented), maladaptive (avoidance-oriented and emotions-oriented), and mixed styles.
BMI was calculated based on height and weight data obtained from patient medical records.
HbA1c levels reflect the mean blood glucose concentration for about 3 months after the test, with the majority (about 60%) of HbA1c (%) being produced in the last month before the measurement.
Statistical Analysis
Categorical data were presented as numbers (N) and percentages (%). Continuous data (eg, disease duration in years) were presented as mean (M) and standard deviation (SD), median (Me), lower (Q1) and upper quartiles (Q3), and extreme values (Min-Max).
First, multiple regression analysis was performed using a hierarchical method to verify the possibility associations between complications in patients with diabetes and the clinical and sociodemographic variables, psychological factors (depression risk measured with the WHO-5 Well-Being Index, level of sense of influence on the diabetes course, and coping styles). In the first step, the following sociodemographic characteristics were introduced to the regression analysis: age, sex, place of residence (rural areas, town, city) and the level of education (primary, secondary, higher). In the next step, clinical variables were introduced into the model: duration of diabetes (years), HbA1c (%) levels, and BMI (kg/m2). The variables measured on the ordinal scale (eg, place of residence) were recoded using the Dummy Coding method (coded variables: 0 = no, 1 = yes). Finally, the designed model included WHO-5 Well-Being Index results, degree of sense of influence on the diabetes course and coping styles to assess a unique contribution of these psychological factors in explaining variance in the number of complications of diabetes.
The variance inflation factors (VIFs) were estimated to detect the degree of multicollinearity between independent variables (IV) in regression analysis. VIFs are standard statistics to evaluate artificial inflation of the variance of a regression coefficient. A rule of thumb is that VIF >10 indicates multicollinearity.39 A higher value of VIF indicates a more problematic collinearity between variables.39 However, there is no clear consensus on the permissible threshold value of VIFs. For example, Hair suggests that even VIFs >4 indicate a possible problem with multicollinearity.40 In this study, the maximum value of VIF was 3.65 . These results allow us to assume that there is no multicollinearity among the explained variables.
A logistic regression analysis was also performed to determine the relationship between the sociodemographic variables (sex, age, place of residence, level of education), medical characteristics (HbA1c level [%], duration of diabetes [years], BMI [kg/m2]), psychological factors (risk of depression, sense of influence on the diabetes course, coping styles), and occurrence of complications among patients with T2DM.
While linear regression model is used to assess relationships between IVs and outcome variable expressed as continuous variable (number of diabetes complications), logistic regression is applied to assess relationships of IVs with categorical variables (the odds/probability of occurring diabetes complications).41 Thus, linear regression is useful for regression problems whereas logistic regression is applicable for classification tasks mainly. Logistic regression is commonly used in healthcare to identify factors related to diseases and plan preventive measures.42 Moreover, unlike linear regression, the relationships between the IVs and outcome variables (dependent variables; DV) is not presumed to be a linear function.43 The relationship between the outcome and the IV is specified by an odds ratio (OR) instead of a multiplicative factor. Simple comparisons of values of ORs for various IVs allow to identify the most important factors for outcome variable.43 It is important to notice that the independent variables included in a regression analysis are commonly called predictor variables or predictors,41 but in this study, the term “effect” refers to a correlation pattern, not necessarily to causal relations.
The logistic regression model included dummy variables for:
- Sex – males as the reference group;
- Place of residence – rural area as the reference group;
- Education level – primary education as the reference group;
- HbA1c level – HbA1c ≤7% as the reference group;
- Risk of depression – “no risk of depression” as the reference group;
- Coping style – “emotions-oriented style” as the reference group.
All statistical analyses were performed with SPSS, version 27 for Windows.44 The level of significance was set at p < 0.05 in all statistical tests.
Results
Sociodemographic and Psychological Characteristics and Health Profile of the Sample
The study included a large sample (N = 2574) spanning a wide age range (22–94 years), with a mean age of 63.58 years (SD = 9.58). The study sample consisted of 1381 women (53.7%) and 1171 men (45.5%) with T2DM, after a switch in treatment from human insulin mixtures to an insulin analogue. More than half of the patients (51.8%) had a secondary level of education, 34.3% had primary education and 13.2% had higher education. 35% of participants were living in cities, 38.8% in towns, and 25.3% in rural areas.
The duration of treatment for T2DM in the study sample ranged from 2 to 43 years (M = 10.24; SD = 6.10), with the minimum duration of 4 months and the maximum of 74 years. The BMI ranged from 16.18 to 56.19 kg/m2 (M = 29.69; SD = 4.41). Overweight occurred among 45.1% patients with diabetes, obesity occurred among 41.6% and only 11.1% of participants were of normal weight. The HbA1c level ranged from 4.10% to 15% (M = 7.99; SD = 1.11). The number of complications ranged from 0 to 4 (M = 1.16; SD = 1.06) and no complications of diabetes were reported by 31.1% of patients. Only 19 patients (0.7%) had simultaneously no complications, their BMI level was normal, and their HbA1c level was below 7%.
The majority of patients were not at risk of depression (69%), but among about 30% participants, the risk of depression was identified (M = 15.36; SD = 4.65). The majority of participants used a mixed coping style (54.4%). On the Scale of Clinical Assessment of the Sense of Influence on the Diabetes Course, participants’ scores ranged from 0 to 4 points (M = 2.56; SD = 0.96). Detailed statistics are presented in Table 1.
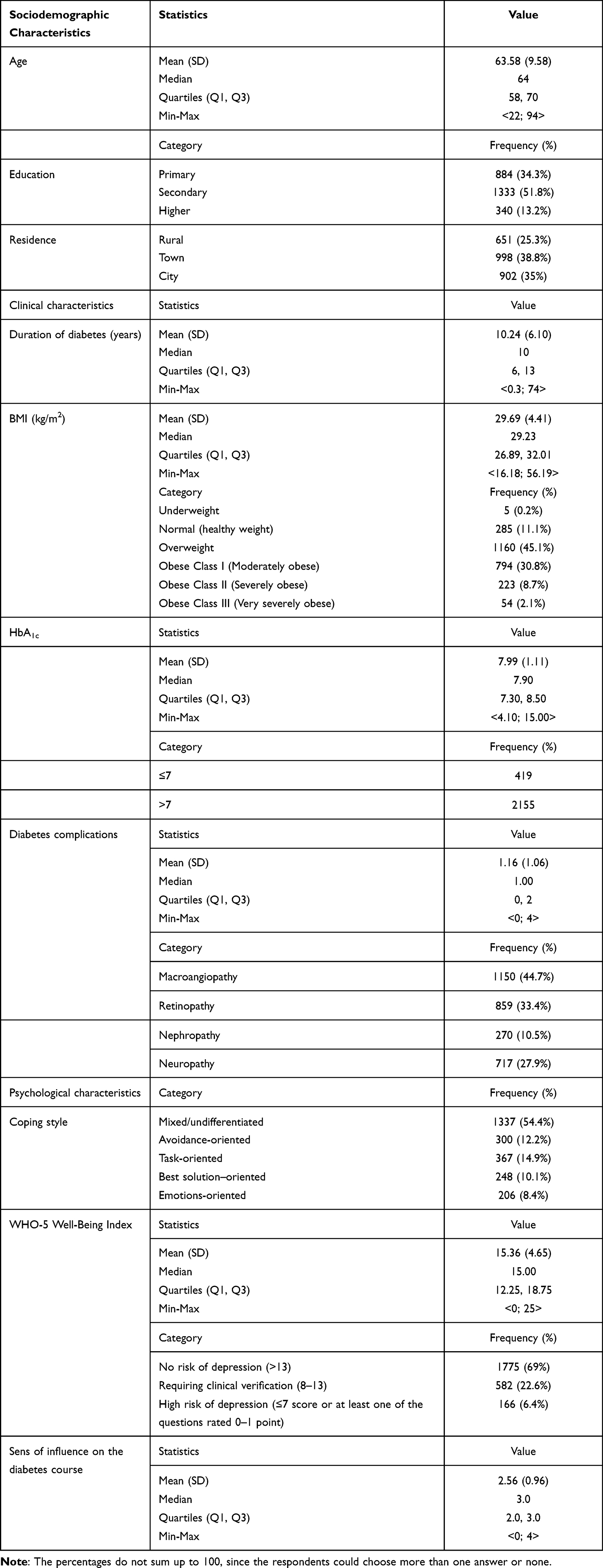 |
Table 1 Sociodemographic, Clinical, and Psychological Characteristics of Patients with Type 2 Diabetes Mellitus in the Study Sample (N = 2574) |
The Three-Step Hierarchical Regression Analysis for the Number of Diabetes Complications
Multiple regression analysis using a hierarchical method indicated that the psychological factors (risk of depression, sense of influence on the diabetes course, coping style) were important factors for of the number of diabetes complications, F(15, 2289) = 46.41; p < 0.001 when clinical and sociodemographic variables were included in the model.
The hierarchical multiple regression at step one revealed that sociodemographic variables significantly contributed to the regression model, with F (6, 2298) = 44.18 and p < 0.001, and accounted for about 10% of the variance of the number of diabetes complications. Furthermore, the analysis indicated that inclusion of the clinical variables into the model explained additional 11% of variation in the number of diabetes complications and made a significant change in the R² parameter: ∆F (3, 2295) = 105.42, p < 0.001, ∆R2 = 0.11. Inclusion of psychological factors explained an additional 2.1% of variation in the dependent variable (DV). The change in the R² was significant: ∆F (6, 2289) = 10.54, p < 0.001, ∆R2 = 0.019.
Finally, the analysis showed that sex was significantly associated with the number of diabetes complications (β = −0.09, t = −4.88, p < 0.001), with females having fewer complications than males. It was shown that the older the age, the more diabetes complications are present (β = 0.15, t = 7.26, p < 0.001). Participants with a higher education level had significantly fewer complications than patients with primary education (β = −0.06, t = −2.73, p = 0.006). The higher the HbA1c (%) levels and BMI (kg/m2) and the longer the duration of diabetes (years), the more complications of diabetes were observed.
Also, psychological factors turned out to be significant variables related to the number of diabetes complications. It was shown that the higher the WHO-5 Well-Being Index and sense of influence on the diabetes course, the smaller the number of diabetes complications (β = −0.10, t = −4.88, p < 0.001 and β = −0.05, t = −2.08, p = 0.038, respectively). Participants with mixed and best solution–oriented coping styles had significantly fewer complications than patients with an emotions-oriented coping style (β = −0.07, t = −2.12, p = 0.034 and β = −0.05, t = −1.97, p = 0.048, respectively).
Detailed statistics are presented in Table 2.
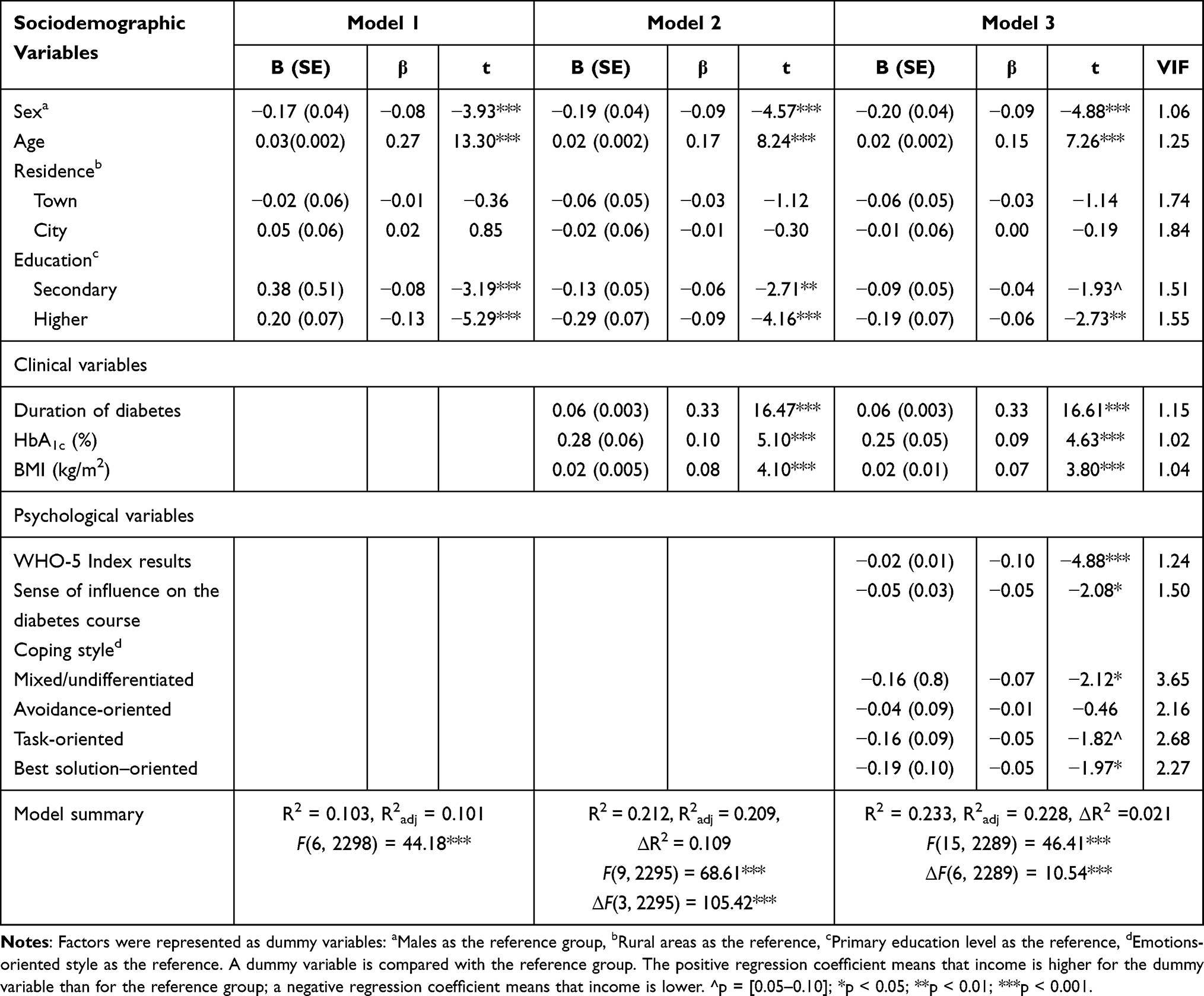 |
Table 2 A Summary of the Three-Step Hierarchical Regression Analysis for the Number of Diabetes Complications Among Patients with Type 2 Diabetes Mellitus in the Study Sample (N = 2574) |
Odds Ratios for Occurrence of Complications Among Patients with T2DM
The logistic regression model including sociodemographic characteristics was statistically significant, χ2(6) = 235.90, p < 0.001. The model explained 14.1% (Nagelkerke R2) of the variance of complications in diabetes mellitus. Overall, sociodemographic background allow to correctly classify 72.4 cases.
The second model added 3 clinical factors, which increased the explanatory power of the model to about 26.1% of the variance, and the classification accuracy reached 75.3%. All clinical factors had significant associations with occurrence of complications: HbA1c (%) levels, duration of T2DM (years), and BMI (kg/m2) (p < 0.001 in all cases). Model 2 shows that when clinical variables are added to the model, sociodemographic factors are still significant for occurrence of T2DM complications (see Table 3). When clinical factors were included into the model, it turned out that patients living in cities had lower odds of having complications than those living in rural areas (OR = 0.654).
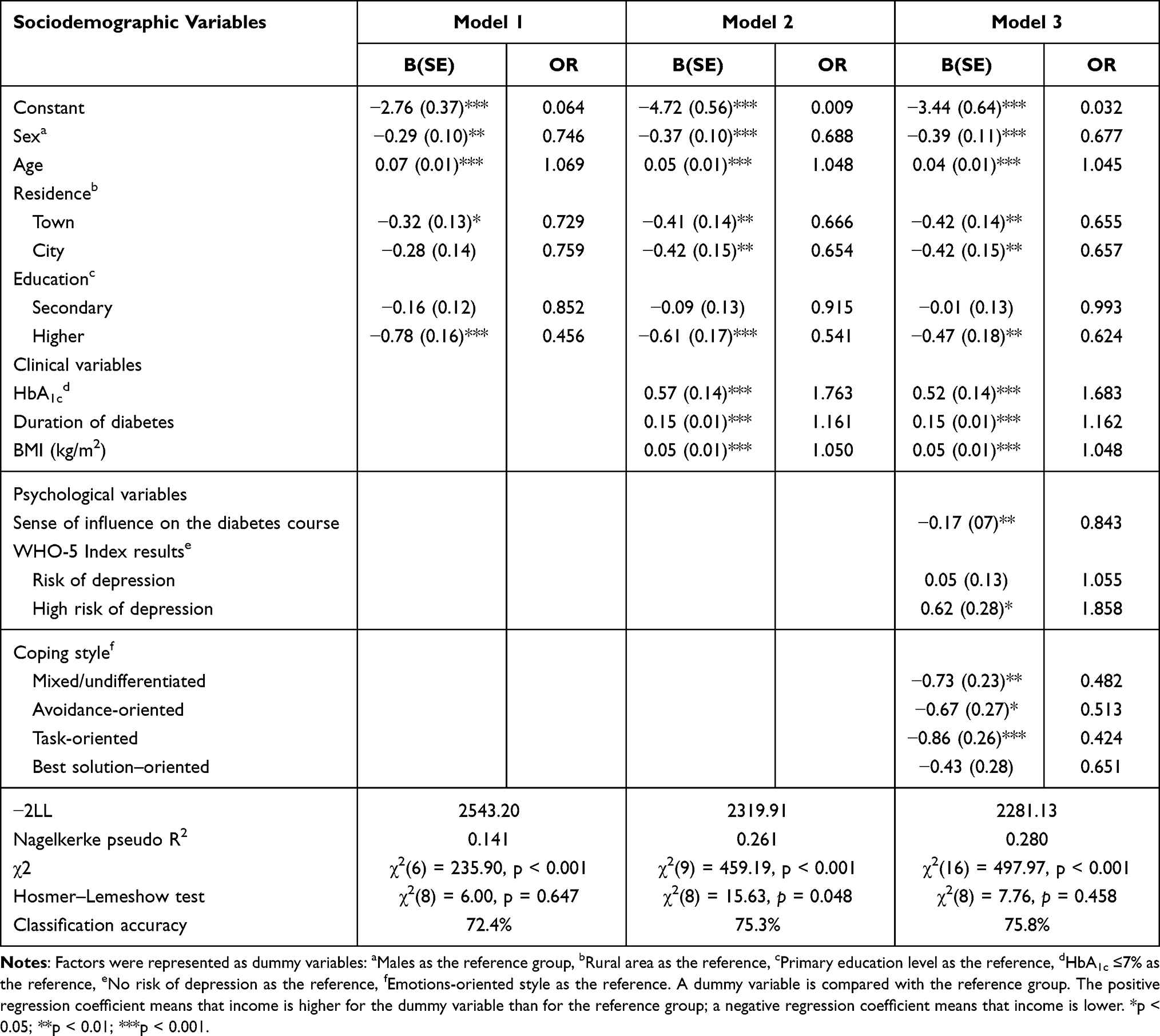 |
Table 3 Logistic Regression of Sociodemographic, Clinical, and Psychological Variables and the Occurrence of Complications of Type 2 Diabetes Mellitus in the Study Population (N = 2574) |
The logistic regression model including sociodemographic characteristics and clinical and psychological factors (Model 3) was statistically significant: χ2(16)=497.97, p < 0.001. The final model explained 28% (Nagelkerke R2) of the variance of complications in diabetes mellitus and correctly classified 75.8% of cases.
Females had lower odds to exhibit complications of diabetes mellitus than males (OR = 0.677). Age increase was associated with increased odds of complications in diabetes (OR = 1.045). Patients living in towns and cities had significantly lower odds of suffering complications (OR = 0.655 and OR = 0.657, respectively) than patients from rural areas. It was also shown that patients with a higher level of education had lower odds of complications than patients who completed only primary education (OR = 0.624).
The ORs for clinical variables indicated that patients with HbA1c >7% had about 68% higher odds of diabetes complications than participants with HbA1c ≤7% (OR = 1.683). When duration of diabetes (years) and BMI (kg/m2) are considered, an increase in the odds of occurrence of complications (about 16% and 5%, respectively) can be seen.
Patients at high risk of depression had about 86% higher odds of the occurrence of complications (OR = 1.858) than those without the risk of depression. Additionally, participants with mixed, avoidance-oriented, and task-oriented coping styles had lower odds of complications of diabetes mellitus than patients using an emotions-oriented style. Detailed statistics are presented in Table 3.
Discussion
The main aim of this study was to test the relationships between the number of complications in T2DM and sociodemographic, clinical and psychological variables. An additional goal was to estimate, on the basis of the above-mentioned variables, the odds ratios of prevalence of diabetes complications.
In the part concerning the number of complications, sex, age, and the level of education turned out to be significant factors associated with the number of complications. The results showed that females had fewer complications than males. The older age was associated with more diabetes complications. Also, patients with primary school level education had significantly more complications than those with higher education. This may indicate the need to adapt educational materials for patients with a lower level of education. Also, disease-related variables remained significant factors in the final model: the higher the HbA1c level (%), the longer the diabetes duration (years), and the higher the BMI (kg/m2), the more complications of diabetes. Although the relationships between the number of complications and age as well as diabetes duration were the strongest in the regression model, the significant associations of psychological variables with the number of complications of T2DM deserve special attention. The final regression model including all of the mentioned variables explained about 23% variance of the number of diabetes complications, of which psychological variables explained 2% of the variance. For comparison, in a previous study, a similar set of variables accounted for only 7% of variance of HbA1c levels and 3% of variance of BMI.28 It was shown that, considering psychological factors, the strongest relationships were between well-being (lower risk of depression) and the number of complications. Namely, the better the well-being, the fewer complications of diabetes. Moreover, the use of mixed and best solution–oriented coping styles turned out to be associated with the presence of fewer complications than in the case of an emotions-oriented coping style. A similar relationship strength was observed between the sense of influence on the diabetes course and number of complications. The findings indicated that the lower the sense of influence, the more complications of diabetes are reported.
According to our best knowledge, this is the first study to investigate the relationships of both- coping styles and the sense of influence on the diabetes course with number of complications of T2DM. Its relevance in the context of diabetes management, apart from depression and anxiety, has been confirmed while developing the Psychodiabetic Kit.16
In a project study by Kokoszka,25 low sense of influence on the diabetes course and maladaptive coping styles were found among patients with T2DM, who had problems with adherence to treatment when switching from human insulin to its analogues. Also, maladaptive coping styles and low sense of influence on the diabetes course turned out to be associated with choosing less advanced insulin injectors.26,27 Low sense of influence on the diabetes course in people with T2DM additionally turned out to be associated with high HbA1c levels, while a high sense of influence on the diabetes course was associated with lower risk of excessive BMI.27
As already mentioned, despite the fact that certain studies considered perception of self-influence on the disease course and coping styles, they did not analyze the number of complications and focused on diabetes-related emotional distress45 or treatment adherence.27 Of note, the number of complications is crucial as it reflects disease severity, and investigating factors associated with this variable seems justified. To the best of our knowledge, out of variables analyzed in the present study, only exacerbation of depressive symptoms has been analyzed in the context of the number of diabetes complications. In one of the few studies,46 the number of complications was significantly correlated with the risk of depression, and the highest risk occurred in the case of 4 to 6 complications at baseline.
In our study, we were also interested in the odds of the occurrence of diabetes complications based on the selected variables. While linear regression allows for estimation of the number of diabetes complications, logistic regression enables classifying patients into one of two categories (complications vs no complications) using a given set of independent variables. When it comes to the occurrence of complications of T2DM, sociodemographic variables also turned out to be important factors. The results indicated that women had 32% lower odds to develop complications than men, and the chance of complications increased by 4.5% with each year of life. This relationship is consistent with results described by other authors.7,14,15 Patients living in towns and cities had about 34% lower odds to suffer from T2DM complications than those living in rural areas. This may result not only from poorer access to advanced healthcare but also lower health awareness and knowledge about diabetes complications, which was noticed in another Polish study47 and might indicate the need to spread awareness of pro-health behaviors and behaviors conducive to the development of diabetes complications among residents of rural areas. In line with the mentioned study,47 also a lower education level turned out to be a factor associated with occurrence of complications. Patients with higher education had about 38% lower odds of developing complications of diabetes mellitus than those with a primary education level. Furthermore, for a one-unit increase in duration of diabetes (years) and BMI (kg/m2), the odds of occurrence of complications increased by, respectively, about 16% and 5%. Participants with HbA1c >7% had 68% higher odds of suffering from complications of diabetes mellitus than participants with HbA1c ≤7%. The odds of complications increased by about 86% in patients with poor well-being compared to those who were not at risk of depression. Also, coping styles turned out to be significantly associated with increased odds of complications occurrence. Mixed, avoidance-oriented, and task-oriented coping styles were associated with lower odds of complications (about 52%, 49%, and 58%, respectively) compared with an emotions-oriented coping style. This is a very important finding suggesting that efforts aimed at developing a task-oriented coping style and general increase of problem-solving abilities are the key aspect of diabetes management. The ability to systematically implement the established treatment plan and adapt to the current requirements of the situation is indeed one of the conditions for effective coping.48
The final regression model including all of the mentioned variables explained about 28% of the variance of complications occurrence and correctly classified 75.8% of cases. Although we cannot infer on causality, it seems to confirm the importance of psychological factors in the context of diabetes complications. The importance of psychosocial variables in the context of diabetes complications was also emphasized by Hackett and Steptoe.49
A meta-analysis by Nouwen et al6 has shown that although the relationship between diabetes complications and depression seems to be bidirectional, the risk of diabetes complications occurrence in people with depression is higher than the risk of depression development in those with diabetes complications.6 There are some reports suggesting a beneficial effect of psychological interventions on glycemic control (eg, acceptance and commitment therapy50 or mindfulness-based stress reduction program51); however, as concluded in available reviews, the impact of psychological interventions aimed at treatment of depressive symptoms or modification of psychosocial stress factors remains unclear and requires further investigation, especially in a long-term observation. Nevertheless, studies emphasize the significant impact of psychological interventions on reducing the level of anxiety, depression, and diabetes-related distress in people with T2DM.49,52 Taking into account both the evidence from these reports and the results of our study, supplementing diabetes management with supportive psychological interventions may have potentially significant benefits. Social support may also be an important factor in addressing diabetes complications. In a systematic review by Strom and Egede,53 higher social support turned out to be associated not only with reduced psychosocial symptoms but also with better clinical outcomes and adaptation of beneficial lifestyle activities. It is worth noting that both estimation of the odds for having complications and identification of the factors associated with the number of complications in T2DM are important not only for improving the quality of life in the disease but also for reducing the risk of mortality.2 Verification of sociodemographic and clinical variables is relatively simple for a clinician, but the psychological assessment of a patient is not routine during a standard medical visit, if only due to the limited time available. However, since psychological variables are significant factors for complications and may constitute risk factors for their development, it seems very important to assess this aspect of the patient’s functioning using the simplest and shortest methods possible, available to people without specialist psychological education. For this reason, such tools were used in this study. Also, due to time constraints during the standard medical visit, the amount of data on the course of the disease and its treatment has been limited to the most relevant information.
The strength of our research is the large number of enrolled participants with advanced diabetes (treated for >3 years in >90% of patients), which allowed us to assess the actual relationships of the studied psychological and sociodemographic factors with the number of complications developed and observed clinically after a longer duration of the disease. The analyzes concerned people treated with mixtures of human insulins when a decision was made to replace the mixtures with insulin analogues. However, as this is a retrospective evaluation of the results of the pivotal study aimed at assessing difficulties in using insulin analogues, the reasons for this decision were not controlled. It can be assumed with high probability that the patients either did not have satisfactory treatment results, as shown by HbA1c levels >7% in 80.8% of individuals or had problems with adverse effects in the course of treatment with insulin mixtures. In a study by Kokoszka,25 hypoglycemia was frequently reported in those patients (31.6%). Another limitation of our study is the representativeness of the sample, which is difficult to assess, as the number of refusals was not recorded. Patients who refused to participate in the study may have had more advanced depression or more severe symptoms of T2DM. However, it seems important that the doctors who acted as interviewers included patients who were under their care and therefore knew them and had access to disease records. This can be beneficial in terms of the accuracy of the information obtained.
Conclusion
- The number of complications has weak but statistically significant relations with psychosocial and clinical factors, including sociodemographic (older age, male sex, lower education level), clinical (high HbA1c level [%], long duration of the disease [years], high BMI [kg/m2]), and psychological (poor well-being, low sense of influence on the diabetes course, maladaptive coping styles).
- Poorly educated people, living in rural areas, the elderly, those with a longer duration of the disease (years), men, people with high BMI (kg/m2) and HbA1c (%) levels, with poor well-being, low sense of influence on the diabetes course, and using emotions-oriented coping styles are at higher odds for the onset of diabetes complications. The logistic regression analysis model taking into account all the above mentioned variables accounted for almost 30% of the variance.
- The results support the thesis that assessment of the number of complications is a measure that reflects the severity of the course of diabetes and that sense of influence on the disease course is an important psychological factor related to the management of diabetes.
Acknowledgments
The research is based on selected data from a database of the study “Psychosocial factors related to adherence to the recommendations of therapy with two-phase insulin analogues.” The Foundation for the Development of Psychiatry and Psychotherapy in Warsaw was the sponsor of the project within the meaning of the GCP and carried out the study, which was also approved by the Bioethics Committee of the Medical University of Warsaw. The used data was previously analyzed by Agnieszka Łukasiewicz, MD, in her PhD thesis entitled “Relations of psychological and sociodemographic factors with general characteristics of the diabetes course: current – level of glycated hemoglobin and Body Mass Index and longterm – number of complications.” The thesis was prepared under the supervision of Łukasz Gawęda and it was defended in 2019 at the 2nd Faculty of Medicine, Medical University of Warsaw.
Disclosure
Andrzej Kokoszka received an honorarium as the principal investigator of the study “Psychosocial factors related to adherence to the recommendations of therapy with two-phase insulin analogues”, after applying for a research grant from Novo Nordisk, Poland, for the Foundation for the Development of Psychiatry and Psychotherapy in Warsaw. Novo Nordisk Poland sponsored his participation in a meeting of Psychosocial Aspects of Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy Powered by TCPDF (www.tcpdf.org) of Diabetes (PSAD) Study Group. The PSAD Study Group is an official Study Group of the European Association for the Study of Diabetes (EASD). The authors report no other conflicts of interest in this work.
References
1. Ogurtsova K, da Rocha Fernandes JD, Huang Y, et al. IDF diabetes atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 2017;128:40–50. doi:10.1016/j.diabres.2017.03.024
2. Young BA, Lin E, Von Korff M, et al. Diabetes complications severity index and risk of mortality, hospitalization, and healthcare utilization. Am J Manag Care. 2008;14:15–23.
3. American Diabetes Association [ADA]. Glycemic targets: standards of medical care in diabetes – 2022. Diabetes Care. 2022;40(1):10–38.
4. Lang BV, Marković BB. Prevalence of comorbidity in primary care patients with type 2 diabetes and its association with elevated HbA1c: a cross-sectional study in Croatia. Scand J Prim Health Care. 2016;34:66–72. doi:10.3109/02813432.2015.1132886
5. Habtewold TD, Alemu SM, Haile YG. Sociodemographic, clinical, and psychosocial factors associated with depression among type 2 diabetic outpatients in Black Lion General Specialized Hospital, Addis Ababa, Ethiopia: a cross-sectional study. BMC Psychiatry. 2016;16:103. doi:10.1186/s12888-016-0809-6
6. Nouwen A, Adriaanse MC, van Dam K, et al. European Depression in Diabetes (EDID) research consortium. Longitudinal associations between depression and diabetes complications: a systematic review and meta-analysis. Diabet Med. 2019;36:1562–1572. doi:10.1111/dme.14054
7. Huang ES, Laiteerapong N, Liu JY, John PM, Moffet HH, Karter AJ. Rates of complications and mortality in older patients with diabetes mellitus: the diabetes and aging study. JAMA Intern Med. 2014;174:251–258. doi:10.1001/jamainternmed.2013.12956
8. De Groot M, Anderson R, Freedland K, Clouse RE, Lustman PJ. Association of depression and diabetes complications: a meta-analysis. Psychosom Med. 2001;63:619–630. doi:10.1097/00006842-200107000-00015
9. Albasheer OB, Mahfouz MS, Solan Y, et al. Depression and related risk factors among patients with type 2 diabetes mellitus, Jazan area, KSA: a cross-sectional study. Diabetes Metab Syndr. 2018;12:117–121. doi:10.1016/j.dsx.2017.09.014
10. Tyagi K, Agarwal NB, Kapur P, Kohli S, Jalali RJ. Evaluation of stress and associated biochemical changes in patients with type 2 diabetes mellitus and obesity. Diabetes Metab Syndr Obes. 2021;14:705–717. doi:10.2147/DMSO.S294555
11. Lagani V, Koumakis L, Chiarugi F, Lakasing E, Tsamardinos I. A systematic review of predictive risk models for diabetes complications based on large scale clinical studies. J Diabetes Complications. 2013;27:407–413. doi:10.1016/j.jdiacomp.2012.11.003
12. Donnelly R, Emslie-Smith AM, Gardner ID, Morris AD. Vascular complications of diabetes. BMJ. 2000;320:1062–1066. doi:10.1136/bmj.320.7241.1062
13. Ganda OP, Arkin CF. Hyperfibrinogenemia: an important risk factor for vascular complications in diabetes. Diabetes Care. 1992;15:1245–1250. doi:10.2337/diacare.15.10.1245
14. Wolde HF, Atsedeweyen A, Jember A, et al. Predictors of vascular complications among type 2 diabetes mellitus patients at University of Gondar Referral Hospital: a retrospective follow-up study. BMC Endocr Disord. 2018;18:1–8. doi:10.1186/s12902-018-0280-0
15. Kautzky-Willer A, Harreiter J, Pacini G. Sex and gender differences in risk, pathophysiology and complications of type 2 diabetes mellitus. Endocr Rev. 2016;37:278–316. doi:10.1210/er.2015-1137
16. Kokoszka A, Jodko-Modlińska A, Obrębski M, Ostasz-Ważny J, Radzio R. Psychodiabetic kit and its application in clinical practice and research. In: Masuo K, editor. Type 2 Diabetes. Intech; 2013:507–531.
17. Jiang X-J, Jiang H, Chen Y, et al. The effectiveness of a self-efficacy-focused structured education program (SSEP) in improving metabolic control and psychological outcomes of type 2 diabetes patients: a 12-month follow-up of a multicenter randomized controlled trial. Diabetes Metab Syndr Obes. 2021;14:305–313. doi:10.2147/DMSO.S290029
18. Kokoszka A, Telichowska-Leśna A, Radzio R. Krótka skala poczucia wpływu na przebieg choroby – wersja dla schizofrenii [Brief measure to assess perception of self-influence on the disease course. Version for schizophrenia]. Psychiatr Pol. 2008;4:503–513.
19. Gawęda Ł, Buciński P, Staniszewski K, Słodki Z, Sym A, Kokoszka A. Związki wglądu w chorobę, poczucia wpływu na jej przebieg, stylów radzenia sobie z chorobą z objawami psychopatologicznymi w schizofrenii [Relationships between insight, self-influence on illness course, coping styles and psychopathology in schizophrenia]. Psychiatria. 2008;5:124–133.
20. Wilczek-Rużyczka E, Halicka D. Wgląd w chorobę i poczucie wpływu na jej przebieg a funkcjonowanie społeczne pacjentów ze schizofrenią [Insight into illness and a sense of the impact on its course and social functioning of patients with schizophrenia]. Psychiatr Psychol Klin. 2013;13:50–57.
21. Orzechowski W, Buczek W, Szczerba JE, et al. Underdiagnosis of major depressive episodes in hemodialysis patients: the need for screening and patient education. J Clin Med. 2021;10:4109. doi:10.3390/jcm10184109
22. Lazarus RS, Folkman S. Stress, Appraisal and Coping. New York, USA: Springer; 1984.
23. Lazarus RS, Folkman S. Transactional theory and research on emotions and coping. Eu J Pers. 1987;1:141–169. doi:10.1002/per.2410010304
24. Kokoszka A, Radzio R, Kot W. Krótka Metoda Oceny Radzenia Sobie z Chorobą: wersja dla mężczyzn i kobiet [Brief method of evaluating coping with disease: versions for men and women]. Diabetologia Praktyczna. 2008;9:1–11.
25. Kokoszka A. Treatment adherence in patients with type 2 diabetes correlates with different coping styles, low perception of self-influence on disease and depressive symptoms. Patient Prefer Adherence. 2017;11:587–595. doi:10.2147/PPA.S124605
26. Kokoszka A, Sieradzki J. Styl radzenia sobie z chorobą a wybór rodzaju wstrzykiwacza insuliny u chorych na cukrzycę typu 2 rozpoczynających insulinoterapię [The relations between the style of coping and the choice of injector type at the beginning of insulinotherapy in type 2 diabetes]. Diabetologia Praktyczna. 2004;5:67–74.
27. Kokoszka A, Sieradzki J. Poczucie wpływu na przebieg choroby a sposób leczenia cukrzycy [Relations between the feeling of influence on the course of disease and the management with diabetes]. Diabetologia Praktyczna. 2005;6:1–5.
28. Łukasiewicz A, Kiejna A, Cichoń E, Jodko-Modlińska A, Obrębski M, Kokoszka A. Relations of well-being, coping styles, perception of self-influence on the diabetes course and sociodemographic characteristics with HbA1c and BMI among people with advanced type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2022;15:407–418. doi:10.2147/DMSO.S320909
29. Diabetes Poland. Guidelines of the management of diabetic patients. A position of diabetes Poland. J Diabetes. 2014;12(Suppl A).1–101
30. World Health Organization. The ICD-10 Classification of Mental and Behavioral Disorders: Clinical Description and Diagnostic Guidelines. Geneva; 1992.
31. American Medical Association. World Medical Association declaration of Helsinki ethical principles for medical research involving human subjects. JAMA. 2013;310:2191–2194. doi:10.1001/jama.2013.281053
32. Kokoszka A. Krótka metoda oceny poczucia wpływu na przebieg choroby: opis wersji dla osób z cukrzycą [Brief measure to assess perception of self-influence on the disease course. Version for diabetes]. Prz Lek. 2005;62:742–745.
33. Heun R, Bonsignore M, Barkow K, Jessen F. Validity of the five-item WHO well-being index (WHO-5) in an elderly population. Eur Arch Psychiatry Clin Neurosci. 2001;251:27–31. doi:10.1007/BF03035123
34. Peyrot M, Rubin RR, Lauritzen T, Snoek FJ, Matthews DR, Skovlund SE. Psychosocial problems and barriers to improved diabetes management: results of the Cross-National Diabetes Attitudes, Wishes and Needs (Dawn) Study. Diabet Med. 2005;22:1379–1385. doi:10.1111/j.1464-5491.2005.01644.x
35. Peyrot M, Burns KK, Davies M, et al. Diabetes Attitudes Wishes and Needs 2 (DAWN2): a multinational, multi-stakeholder study of psychosocial issues in diabetes and person-centred diabetes care. Diabetes Res Clin Pract. 2013;99:174–184. doi:10.1016/j.diabres.2012.11.016
36. Newnham EA, Hooke GR, Page AC. Monitoring treatment response and outcomes using the World Health Organization’s wellbeing index in psychiatric care. J Affect Disord. 2010;122:133–138. doi:10.1016/j.jad.2009.06.005
37. Lloyd CE, Nouwen A, Sartorius N, et al. Prevalence and correlates of depressive disorders in people with type 2 diabetes: results from the International Prevalence and Treatment of Diabetes and Depression (INTERPRET-DD) study, a collaborative study carried out in 14 countries. Diabet Med. 2018;35:760–769. doi:10.1111/dme.13611
38. Cichoń E, Kiejna A, Kokoszka A, et al. Validation of the Polish version of WHO-5 as a screening instrument for depression in adults with diabetes. Diabetes Res Clin Pract. 2020;159:107970. doi:10.1016/j.diabres.2019.107970
39. Hair JF
40. Hair JF, Black WC, Blac B, Babin BJ, Anderson RE. Multivariate Data Analysis: A Global Perspective.
41. Speelman D. Logistic regression. In: Glynn D, Robinson JA, editors. Corpus Methods for Semantics: Quantitative Studies in Polysemy and Synonymy. Amsterdam: John Benjamins; 2014:487–533.
42. Peng CYJ, Manz BD, Keck J. Modeling categorical variables by logistic regression. Am J Health Behav. 2001;25(3):278–284. doi:10.5993/AJHB.25.3.15
43. Worster A, Fan J, Ismaila A. Understanding linear and logistic regression analyses. Can J Emerg Med. 2007;9(2):111–113. doi:10.1017/S1481803500014883
44. IBM Corp. IBM SPSS statistics for windows, version 27.0. Armonk, NY: IBM Corp; 2020.
45. Karlsen B, Oftedal B, Bru E. The relationship between clinical indicators, coping styles, perceived support and diabetes-related distress among adults with type 2 diabetes. J Adv Nurs. 2011;68(2):391–401. doi:10.1111/j.1365-2648.2011.057
46. Deschênes SS, Burns RJ, Pouwer F, Schmitz N. Diabetes complications and depressive symptoms: prospective results from the Montreal Diabetes Health and Well-Being Study. Psychosom Med. 2017;79:603–612. doi:10.1097/PSY.0000000000000447
47. Araszkiewicz A, Piasecka D, Wierusz-Wysocka B. Ocena wiedzy pacjentów z typem 2 cukrzycy na temat przewlekłych powikłań choroby [Assessment of patients’ knowledge concerning late diabetic complications in type 2 diabetes]. Nowiny Lekarskie. 2012;81(2):158–163.
48. Heszen-Niejodek I. Stres i radzenie sobie – główne kontrowersje [Stress and coping - main controversies]. In: Heszen-Niejodek I, Ratajczak Z, editors. Człowiek w sytuacji stresu [A person in a stressful situation]. Katowice: Wydawnictwo Uniwersytetu Śląskiego; 2000:12–43.
49. Hackett RA, Steptoe A. Psychosocial factors in diabetes and cardiovascular risk. Curr Cardiol Rep. 2016;18:95. doi:10.1007/s11886-016-0771-4
50. Gregg JA, Callaghan GM, Hayes SC, Glenn-Lawson JL. Improving diabetes self-management through acceptance, mindfulness, and values: a randomized controlled trial. J Consult Clin Psychol. 2007;75(2):336–343. PMID: 17469891. doi:10.1037/0022-006X.75.2.336
51. Dreger LC, Mackenzie C, McLeod B. Feasibility of a mindfulness-based intervention for aboriginal adults with type 2 diabetes. Mindfulness. 2015;6:264–280. doi:10.1007/s12671-013-0257-z
52. Noordali F, Cumming J, Thompson JL. Effectiveness of mindfulness-based interventions on physiological and psychological complications in adults with diabetes: a systematic review. J Health Psychol. 2017;22:965–983. doi:10.1177/1359105315620293
53. Strom JL, Egede LE. The impact of social support on outcomes in adult patients with type 2 diabetes: a systematic review. Curr Diab Rep. 2012;12:769–781. doi:10.1007/s11892-012-0317-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.