")
Back to Journals » Nature and Science of Sleep » Volume 14
Association of Excessive Daytime Sleepiness with Cerebral Small Vessel Disease in Community-Dwelling Older Adults
Authors Zhao J, Kong Q, Wang M, Huang H, Zhou X, Guo Y, Zhang Y, Wu L, Yu Z, Luo X
Received 8 January 2022
Accepted for publication 5 April 2022
Published 21 April 2022 Volume 2022:14 Pages 765—773
DOI https://doi.org/10.2147/NSS.S357586
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ahmed BaHammam
Jing Zhao, Qianqian Kong, Minghuan Wang, Hao Huang, Xirui Zhou, Yinping Guo, Yi Zhang, Lingshan Wu, Zhiyuan Yu, Xiang Luo
Department of Neurology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China
Correspondence: Xiang Luo, Department of Neurology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China, Tel +86 27-83663337, Email [email protected]
Purpose: Excessive daytime sleepiness (EDS) and cerebral small vessel disease (CSVD) are common problems among older adults; however, their association is not clear. The present study aimed to investigate the frequency of EDS in CSVD patients and the relationship between EDS and neuroimaging markers of CSVD.
Patients and Methods: We conducted a cross-sectional study among 1076 community-dwelling older adults aged 55– 85 years. EDS was measured using the Epworth Sleepiness Scale (ESS), and EDS was defined as an ESS score greater than 10. Binary logistic regression was performed to assess the association between EDS and neuroimaging markers of CSVD.
Results: Of the 1076 participants (mean age: 65.58 ± 6.46 years, 60.5% female), the prevalence of EDS was 10.0%. EDS was more frequent in participants with CSVD than in the total sample (20.0% vs 10.0%, p < 0.001). In fully adjusted models, EDS was significantly correlated with CSVD burden (OR = 1.39, 95% CI 1.16 to 1.68, p < 0.001), the severity of white matter hyperintensities (WMH) (OR = 1.33, 95% CI 1.14 to 1.54, p < 0.001), and presence of lacunes (OR = 2.47, 95% CI 1.53 to 4.00, p < 0.001) but not with the presence of cerebral microbleeds (CMBs) (OR=1.54, 95% CI 0.92 to 2.56, p = 0.099) or severity of enlarged perivascular spaces (EPVS) in basal ganglia (OR = 1.16, 95% CI 0.70 to 1.92, p = 0.564).
Conclusion: We found a high frequency of EDS symptoms in CSVD individuals. Further, EDS was significantly associated with WMH, lacunes, and CSVD burden. Our findings further suggest patients with CSVD may exhibit abnormal sleep-wake patterns.
Keywords: cerebral small vessel disease, daytime sleepiness, sleep disorders, white matter hyperintensities, lacunes
Introduction
Cerebral small vessel disease (CSVD) is common in the older population, and the incidence of CSVD increases with age.1 CSVD is a progressive syndrome characterized by clinical, neuroimaging, and neuropathologic presentations related to the small vessels of the brain.2 The primary neuroimaging markers of CSVD include recent small subcortical infarcts, lacunes, white matter hyperintensities (WMH), enlarged perivascular spaces (EPVS), cerebral microbleeds (CMBs), and atrophy.3 The clinical manifestations of CSVD are heterogeneous. Clinically, CSVD is associated with stroke, cognitive impairment, gait dysfunction, mood disorders, and urinary disorders.2 In recent years, growing evidence suggests that CSVD is also associated with sleep disorders.4–8
Obstructive sleep apnea (OSA) is a common sleep-related breathing disorder and has been validated as an independent risk factor for stroke and ischemic heart disease.7,9 A meta-analysis including fourteen observational studies showed that OSA was associated with features of CSVD, specifically WMH and asymptomatic lacunar infarction (ALI).6 Prior work has also reported that CSVD is associated with other sleep disorders, like insomnia and periodic limb movements (PLM).4,5,8 For example, the occurrence of insomnia in older adults with CSVD is higher than that among general older adults,4 and Kang et al found that the PLM index was positively correlated with neuroimaging markers of CSVD (eg, WMH, lacunes, EPVS).8
Excessive daytime sleepiness (EDS) is a common sleep symptom among older adults, and is a typical symptom of OSA.10 EDS is defined as the inability to maintain wake and alertness during the major waking episodes of the day.11 EDS may increase the risk of accidents and injuries (eg, motor vehicle crashes, work-related accidents) due to decreased alertness, and negatively influence cognition and quality of life.12–14 Moreover, published summary data from cohort studies showed that EDS is associated with greater risks of cardiovascular disease (CVD) events, coronary heart disease, stroke, and all-cause mortality among older adults.11,15 Therefore, EDS is a major public health problem. Currently, studies have revealed that EDS is frequently associated with central nervous system (CNS) diseases, such as Alzheimer’s disease (AD), Parkinson’s disease (PD), headache, multiple sclerosis, and amyotrophic lateral sclerosis (ALS).16–19 However, to our knowledge, no study has focused on the association between neuroimaging markers of CSVD and EDS. Thus, the present study examined the prevalence of EDS in CSVD patients and investigated the association between EDS and neuroimaging makers of CSVD.
Materials and Methods
Study Population
This study is an ongoing community-based study in older residents in Wuhan, China. Eligible residents aged 55 years or older and living in the communities of Wuhan were invited to participate in the study. Exclusion criteria for the present study include inability to live unaided; life expectancy less than 1 year; diagnosis of any neurodegenerative disease (eg, AD, PD); diagnosis of any psychiatric disease (eg, major depression, schizophrenia); stroke, trauma, or infection during the past 3 months; magnetic resonance imaging (MRI) contraindications; and failure to communicate and complete an interview due to any reasons.
From November 2020 to October 2021, a total of 1177 community residents participated in the present study. All examinations such as brain MRI and cognitive assessment were completed within one day. This study was approved by the Institutional Review Board of Tongji Hospital (No. S105) and was carried out in accordance with the Declaration of Helsinki. All participants provided written informed consent.
Sleep Assessment
EDS was assessed using the Epworth Sleepiness Scale (ESS) which consists of eight questions. The ESS score varies between 0 and 24. A higher score indicates a higher sleep propensity and a score > 10 represents EDS.20
Sleep quality over the past month was measured using the Pittsburgh Sleep Quality Index (PSQI), a questionnaire based on self-reported experiences. The PSQI consists of 19 items ranging from 0 to 21. A global PSQI score of 5 or more indicates poor sleep quality.21
The potential risk of OSA was assessed using the STOP-Bang questionnaire, which includes eight items (snoring, tiredness, observed apnea, high blood pressure, body mass index, age, neck circumference, and gender). A score ≥ 3 indicates moderate-to-severe OSA.22
Neuropsychological Assessment
All study participants underwent extensive neuropsychological testing, which included the following items: (1) neurocognitive screening assessments: Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA); (2) processing speed: Trail Making Test A (TMT-A), Stroop words, Stroop color; (3) executive function: Trail Making Test B (TMT-B), Stroop interference, Digit Span Test (backward), Verbal Fluency Test (VFT); (4) memory: Auditory Verbal Learning Test (AVLT); (5) language: Boston Naming Test (BNT).23 Performance in the four cognitive domains was made comparable by converting cognitive test scores to age, sex, and education adjusted z-scores.24 Z scores for the TMT and Stroop were multiplied by −1 so that higher z scores indicate better performance.
MRI Assessment
Brain MRI was obtained using a single 3T MRI scanner (United Imaging, Shanghai, China). Following predefined standardized protocols, the MRI included at least five sequences: T1-weighted, T2-weighted, fluid-attenuated inversion recovery (FLAIR), diffusion-weighted imaging (DWI), and susceptibility-weighted imaging (SWI) (see Supplementary Table 1 for detailed MRI protocols).
Two trained radiologists, who were blinded to all the clinical data, rated the neuroimaging markers of CSVD based on the STandards for ReportIng Vascular changes on nEuroimaging (STRIVE) criteria.3
Lacunes were defined as round or ovoid cerebrospinal fluid (CSF) containing cavities with a surrounding rim of hyperintensity in subcortical regions that range from 3 to 15 mm in diameter. The severity of the periventricular WMH (PWMH) and deep WMH (DWMH) was assessed using the Fazekas scale.25 CMBs were defined as rounded hypointense lesions (2–10 mm in diameter) on SWI sequences. EPVS were defined as round, ovoid, or linear lesions, generally smaller than 3 mm in diameter with a CSF-like signal on all sequences. The severity of EPVS in the basal ganglia (BG) was rated according to the number of spaces in a unilateral slice containing the maximum EPVS: 0 = no EPVS, 1 = 1–10 EPVS, 2 = 11–20 EPVS, 3 = 21–40 EPVS, and 4 = 40 or more EPVS. EPVS score ≥ 2 in BG was defined as moderate-to-severe EPVS.26
The total burden of the CSVD was evaluated using the total CSVD score (from 0 to 4 points). One point was awarded for any of the following: Fazekas score 3 for PWMH or 2–3 for DWMH, any lacune, any CMB, and EPVS score ≥ 2 in BG.27
The presence of CSVD referred to a criterion previously published.28 Participants with moderate to severe CSVD burden with a total CSVD score > 1 were considered a part of the CSVD group. Participants in the CSVD group were then divided into EDS+ and EDS- subgroups based upon the presence or absence of EDS, respectively.
Assessment of Other Variables
Age, sex, height, weight, education level, smoking, and alcohol consumption were recorded using a standardized questionnaire. Depressive symptoms were measured using the Hamilton Depression Rating Scale (HAMD).29 Participants’ self-reported medical history and medication use were also documented.
Statistical Analysis
The data were analyzed using SPSS version 21.0 software (SPSS Inc., Chicago, IL, USA). The demographic variables of the participants are presented as mean (standard deviation), or frequency (percentage) when appropriate. The inter-group difference was compared using the Student’s t-tests (for continuous variables with a normal distribution), Mann–Whitney U-tests (for continuous variables with a non-normal distribution), or χ2 tests (for categorical variables). Binary logistic regressions were conducted to assess the association between EDS and neuroimaging markers of CSVD. Statistical models were initially adjusted for age and sex (Model 1) and then further adjusted for education level, smoking status, hypertension, diabetes, HAMD score, PSQI score, and a STOP-Bang score ≥ 3 (Model 2). In addition, we performed a stratified analysis according to diabetes status. A significance threshold of p < 0.05 was considered statistically significant.
Results
Subject Characteristics
A total of 1076 participants were included in the final analyses. The flow chart of the present study is shown in Figure 1. Table 1 shows the demographic and clinical data of the participants. The mean age of participants was 65.58 ± 6.46 years, and most participants were female (60.5%); 108 (10.0%) participants had EDS.
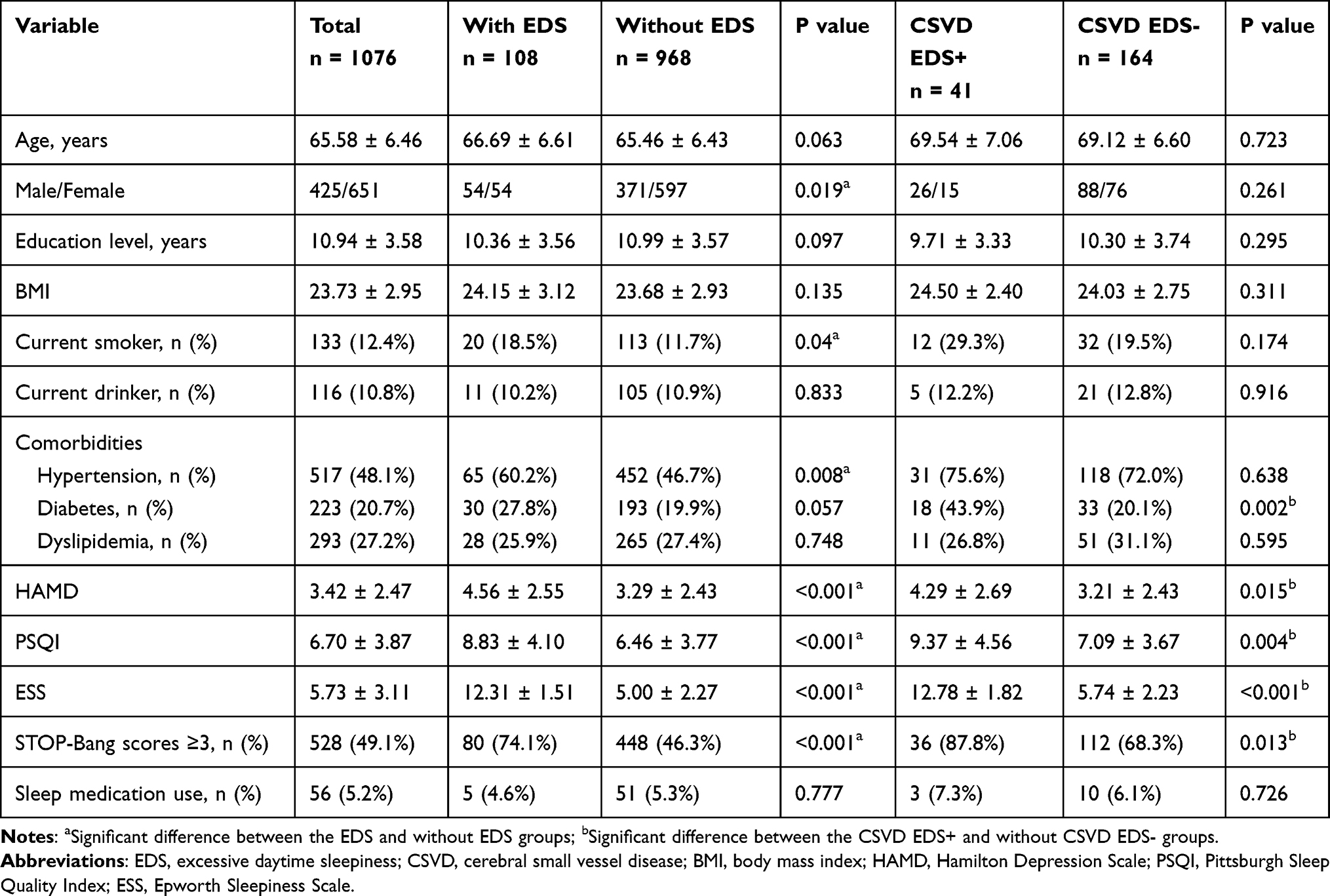 |
Table 1 Characteristics of the Participants |
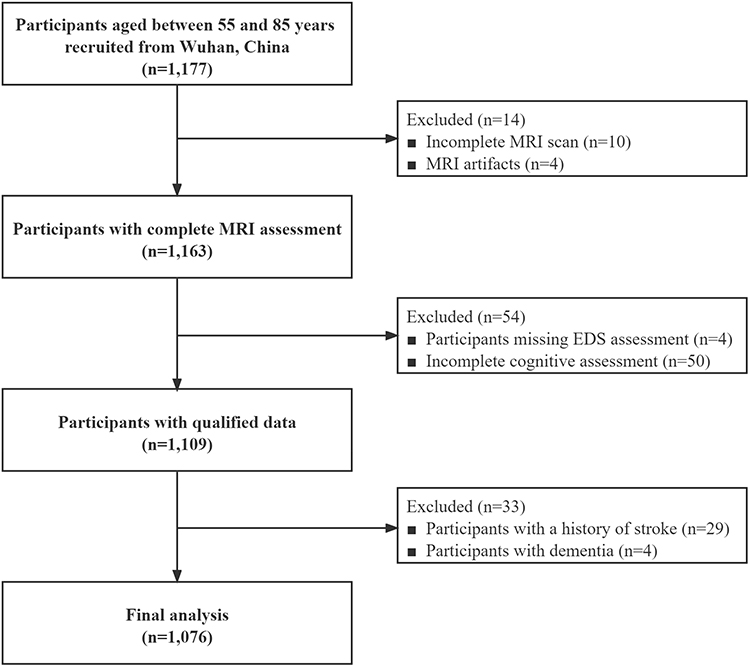 |
Figure 1 Flow chart. Abbreviations: MRI, magnetic resonance imaging; EDS, excessive daytime sleepiness. |
Participants presenting with EDS were more likely to be male, current smokers, have hypertension, poorer sleep quality, greater depression, and a higher risk of moderate-to-severe OSA than participants without EDS (Table 1).
Among neuroimaging markers of CSVD, the EDS group demonstrated more severe WMH (p < 0.001), EPVS in BG (p = 0.023), a higher risk of lacunes (p < 0.001), CMBs (p = 0.018), and a higher CSVD burden (p < 0.001) compared to those without EDS (Table 2).
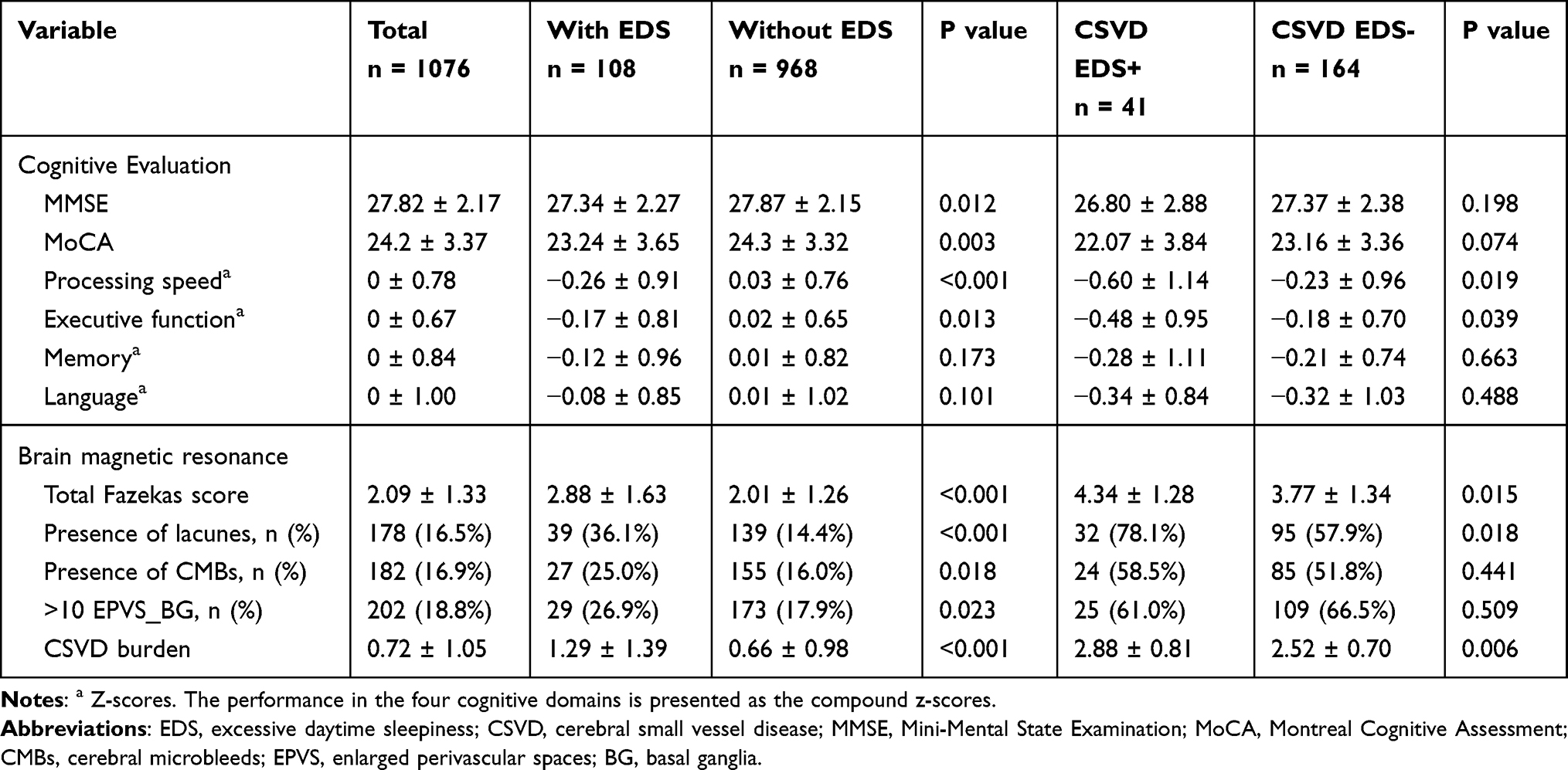 |
Table 2 Cognitive and Neuroimaging Characteristics of the Participants |
Participants with EDS demonstrated lower global cognition (MMSE, p = 0.012; MoCA, p = 0.003), significantly worse performance on processing speed (p < 0.001) and executive function (p = 0.013) compared to participants without EDS, while no differences in memory (p = 0.173) or language (p = 0.101) were observed between groups (Table 2).
Clinical Data of CSVD Participants with and without EDS
Of the 1076 participants, 205 participants met criteria for CSVD. Of the participants that met criteria for CSVD, 41 also met criteria for EDS (EDS+), while 164 did not (EDS-). The prevalence of EDS in the CSVD group was notably higher than that of our total sample (20.0% vs 10.0%, p < 0.001).
Within the CSVD group, EDS+ participants had a higher risk of diabetes (p = 0.002), moderate-to-severe OSA (p = 0.013), poorer sleep quality (PSQI, p = 0.004), and greater depressive symptoms (HAMD, p = 0.015) compared to EDS- participants (Table 1). Regarding cognitive performance, the CSVD EDS+ group demonstrated poorer performance on measures of processing speed (p = 0.019), and executive function (p = 0.039) than the CSVD EDS- group (Table 2). In addition, the CSVD EDS+ group had a higher risk of lacunes (p = 0.018), WMH (p = 0.015) and CSVD burden (p = 0.006) compared with CSVD EDS- group, while there was no significant difference in the presence of CMBs (p = 0.441) and EPVS severity in BG (p = 0.509) (Table 2).
Associations Between EDS and CSVD Markers
Associations among CSVD neuroimaging markers and EDS are shown in Table 3. In our total sample, EDS was significantly correlated with CSVD burden (OR = 1.54, 95% CI 1.30 to 1.82, p < 0.001), total Fazekas score (OR = 1.50, 95% CI 1.31 to 1.72, p < 0.001), and presence of lacunes (OR = 3.05, 95% CI 1.95 to 4.77, p < 0.001), but not with the presence of CMBs (OR = 1.58, 95% CI 0.98 to 2.54, p = 0.061) or severity of EPVS in BG (OR = 1.48, 95% CI 0.92 to 2.38, p = 0.108) (adjusted for age and sex). Further adjusting for education level, smoking status, hypertension, diabetes, HAMD score, PSQI score and a STOP-Bang score of ≥ 3 did not attenuate these associations. Additionally, results did not differ when stratifying for diabetes (Supplementary Table 2).
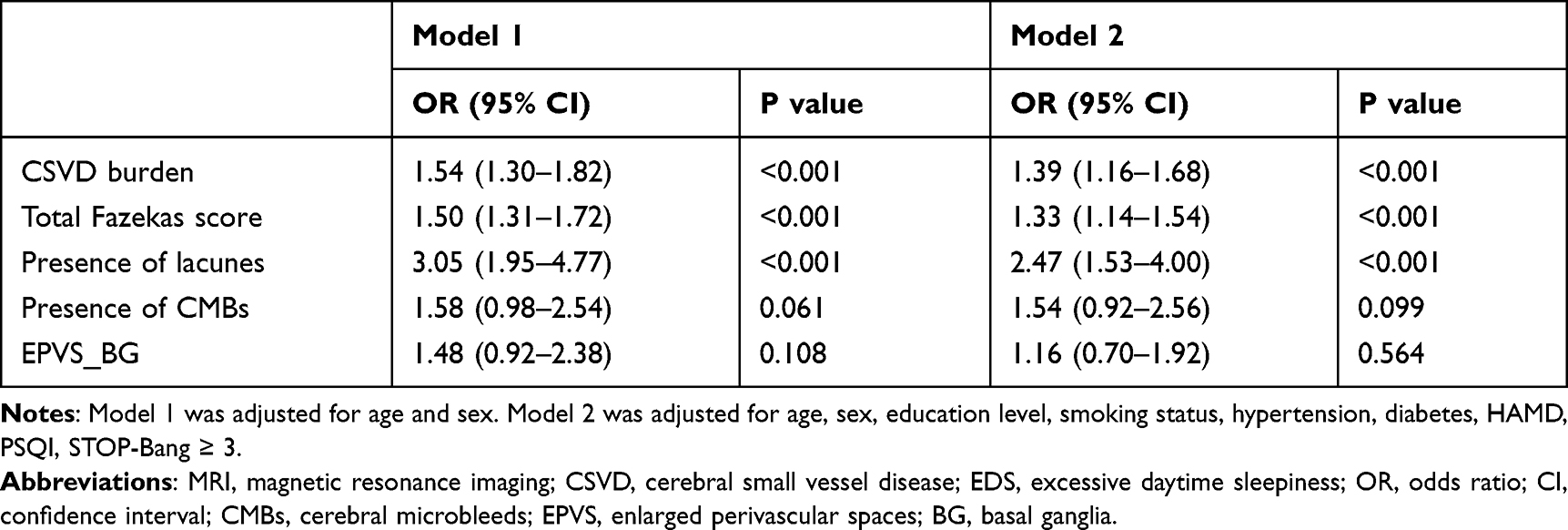 |
Table 3 Association Between MRI Markers of CSVD and EDS |
Discussion
To our knowledge, this is the first study to investigate the incidence of EDS in CSVD patients and the association between EDS and neuroimaging markers of CSVD. In this community-based study, we found that the prevalence of EDS in participants with CSVD was 20.0%, which was notably higher than that of our total sample (10.0%). Further, EDS was related to neuroimaging markers of CSVD, in particular, WMH and lacunes. However, no association between EDS and CMBs or EPVS was observed.
Previous studies have revealed that patients with neurological diseases (eg, PD, AD, ALS) have a higher incidence of EDS than the general population.16,18 In the present study, participants with CSVD had a higher frequency of EDS compared to participants in the overall sample. The prevalence of EDS in our sample was 10.0%, which is similar to previously reported values in an Asian multi-ethnic population (9%).30 Several epidemiological studies demonstrate that the prevalence of EDS ranges from 5% to 30%.31 The difference in prevalence rates may be partially explained by the difference in socio-demographic characteristics and cultural factors, which may have influenced the response to the questionnaire.
Recently, the association between CSVD and circadian rhythm disruption has gained attention. Some studies have revealed that sleep disorders (insomnia, OSA, PLM),4–8 abnormal circadian blood pressure (BP) (non-dipping, reverse-dipping BP patterns),32 and disturbed 24-hour activity rhythms (interdaily instability, intradaily variability)33,34 are correlated with neuroimaging markers of CSVD. EDS represents one of the clinical symptoms of circadian rhythm disruption. Results from the present study demonstrate that EDS is associated with greater CSVD burden, WMH severity, and lacunes. These associations persist after controlling for potential confounders. In summary, our study provides new clinical evidence for the existence of circadian rhythm disruption in CSVD patients.
Although the present study revealed a relationship between CSVD and EDS, the underlying pathophysiology is unclear. WMH in cholinergic pathways may affect the integrity of the adjacent medial cholinergic pathways.35 An autopsy study in a patient with cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) showed that cortical cholinergic projections from the nucleus basalis of Meynert (nbM) could be influenced by white matter lesions.36 Most cholinergic input into the cerebral cortex originates from the nbM (in the basal forebrain).37 The majority of these cholinergic axons are unmyelinated; therefore, they may be more vulnerable to aging or damage in WM.35,38 The presence of lacunes is mainly located in the thalamus, basal ganglia, or frontal white matter,39 and thus may affect the integrity of cholinergic pathways. The basal forebrain cholinergic system is involved in regulating the sleep-wake cycle.40 We thus speculated that EDS may be due to impairments caused by CSVD in the cholinergic system.
CSVD is associated with cognitive decline and the subsequent development of dementia.41 A meta-analysis of prospective studies observed that WMH was associated with decline in global cognitive performance, processing speed, and executive function.42 CMBs and EPVS were also associated with cognitive decline.43–45 The specific mechanism of cognitive decline in CSVD patients is unclear but may be related to the disruption of cortical-subcortical networks.46 Interestingly, a growing body of research suggests an association between EDS and cognitive impairment.15,47,48 A longitudinal study showed that EDS was associated with cognitive decline 4 years later in a community-dwelling older population.49 In the present study, CSVD patients with EDS demonstrated worse cognitive performance, especially regarding measures of processing speed and executive function, compared to CSVD patients without EDS. The mechanism for the effect of EDS on cognitive impairment in patients with CSVD is currently unknown. Thus, further studies are needed to extend and confirm these preliminary findings.
EDS is highly prevalent in older adults. Unfortunately, EDS is frequently overlooked because it is considered a part of normal aging.10 EDS is associated with many adverse outcomes, including cardiovascular diseases and mortality.12,50 CSVD is a slowly progressive disease, and patients with CSVD are often asymptomatic, making them less likely to be aware of the insidious disease progression.51 Individuals with asymptomatic CSVD may develop various clinical syndromes (eg, stroke, dementia, mood disorders), which may increase the risk of mortality.52 The present study found that EDS was associated with neuroimaging markers of CSVD, and CSVD patients with EDS showed worse cognitive performance. Given that EDS is a potential low-cost biomarker, it is necessary to perform EDS screenings, assessments, and treatments among community-dwelling older adults.
The strengths of the current study include a large sample size of community-dwelling older adults, comprehensive evaluation of CSVD markers, and neuropsychological assessments. However, the present study has several limitations. First, the nature of a cross-sectional study limits causal inferences. Further, prospective or interventional studies are needed to clarify the relationship between CSVD and EDS. Second, due to the fact that sleep disorders were assessed only by self-reported questionnaires without polysomnography or actigraphy, subjective bias may exist in sleep assessment. However, it is difficult to perform objective sleep measures in a relatively large population-based study. Third, this study is limited to the Chinese population, and therefore may not be generalizable to other populations.
Conclusion
Overall, findings from the present study suggest a high frequency of EDS symptoms in CSVD individuals. Further, EDS was significantly associated with a greater presence of WMH and lacunes but was not associated with CMBs and EPVS. Our findings suggest that older adults with CSVD may exhibit abnormal sleep-wake patterns, expanding the clinical spectrum of CSVD. Finally, prospective studies are necessary to assess the direction of the relationship between EDS and CSVD.
Abbreviations
EDS, excessive daytime sleepiness; CSVD, cerebral small vessel disease; ESS, Epworth Sleepiness Scale; OR, odds ratio; CI, confidence interval; WMH, white matter hyperintensities; CMBs, cerebral microbleeds; EPVS, enlarged perivascular spaces; OSA, obstructive sleep apnea; PLM, periodic limb movements; CNS, central nervous system; AD, Alzheimer’s disease; PD, Parkinson’s disease; ALS, amyotrophic lateral sclerosis; MRI, magnetic resonance imaging; PSQI, Pittsburgh Sleep Quality Index; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; TMT-A, Trail Making Test A; TMT-B, Trail Making Test B; VFT, Verbal Fluency Test; AVLT, Auditory Verbal Learning Test; BNT, Boston Naming Test; FLAIR, fluid-attenuated inversion recovery; DWI, diffusion-weighted imaging; SWI, susceptibility-weighted imaging; STRIVE, STandards for ReportIng Vascular changes on nEuroimaging; CSF, cerebrospinal fluid; PWMH, periventricular white matter hyperintensities; DWMH, deep white matter hyperintensities; BG, basal ganglia; HAMD, Hamilton Depression Rating Scale; CADASIL, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy; nbM, nucleus basalis of Meynert.
Acknowledgments
The authors thank all participating subjects.
Funding
This study was supported by the National Nature Science Foundation of China (82171385 to X. Luo), Key Research and Development Program of Hubei Province (2020BCA070 to X. Luo), the Application Foundation Frontier Special Project of Wuhan Science and Technology Bureau (2020020601012226 to X. Luo), the Flagship Program of Tongji Hospital (2019CR106 to X. Luo).
Disclosure
The authors declare no conflicts of interest for this work.
References
1. de Leeuw FE, de Groot JC, Achten E, et al. Prevalence of cerebral white matter lesions in elderly people: a population based magnetic resonance imaging study. The Rotterdam Scan Study. J Neurol Neurosurg Psychiatry. 2001;70(1):9–14. doi:10.1136/jnnp.70.1.9
2. Wardlaw JM, Smith C, Dichgans M. Small vessel disease: mechanisms and clinical implications. Lancet Neurol. 2019;18(7):684–696. doi:10.1016/S1474-4422(19)30079-1
3. Wardlaw JM, Smith EE, Biessels GJ, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013;12(8):822–838. doi:10.1016/S1474-4422(13)70124-8
4. Wang J, Chen X, Liao J, et al. The influence of non-breathing-related sleep fragmentation on cognitive function in patients with cerebral small vessel disease. Neuropsychiatr Dis Treat. 2019;15:1009–1014. doi:10.2147/NDT.S193869
5. Del Brutto OH, Mera RM, Zambrano M, Lama J, Del Brutto VJ, Castillo PR. Poor sleep quality and silent markers of cerebral small vessel disease: a population-based study in community-dwelling older adults (The Atahualpa Project). Sleep Med. 2015;16(3):428–431. doi:10.1016/j.sleep.2014.10.023
6. Chokesuwattanaskul A, Lertjitbanjong P, Thongprayoon C, et al. Impact of obstructive sleep apnea on silent cerebral small vessel disease: a systematic review and meta-analysis. Sleep Med. 2020;68:80–88. doi:10.1016/j.sleep.2019.11.1262
7. Del Brutto OH, Mera RM, Zambrano M, Castillo PR. Relationship between obstructive sleep apnea and neuroimaging signatures of cerebral small vessel disease in community-dwelling older adults. The Atahualpa Project. Sleep Med. 2017;37:10–12. doi:10.1016/j.sleep.2017.06.009
8. Kang MK, Koo DL, Shin JH, Kwon HM, Nam H. Association between periodic limb movements during sleep and cerebral small vessel disease. Sleep Med. 2018;51:47–52. doi:10.1016/j.sleep.2018.06.018
9. Culebras A. Sleep, stroke and poststroke. Neurol Clin. 2012;30(4):1275–1284. doi:10.1016/j.ncl.2012.08.017
10. Crowley K. Sleep and sleep disorders in older adults. Neuropsychol Rev. 2011;21(1):41–53. doi:10.1007/s11065-010-9154-6
11. Wang L, Liu Q, Heizhati M, Yao X, Luo Q, Li N. Association between excessive daytime sleepiness and risk of cardiovascular disease and all-cause mortality: a systematic review and meta-analysis of Longitudinal Cohort Studies. J Am Med Dir Assoc. 2020;21(12):1979–1985. doi:10.1016/j.jamda.2020.05.023
12. Howard ME, Desai AV, Grunstein RR, et al. Sleepiness, sleep-disordered breathing, and accident risk factors in commercial vehicle drivers. Am J Respir Crit Care Med. 2004;170(9):1014–1021. doi:10.1164/rccm.200312-1782OC
13. Boulos MI, Murray BJ. Current evaluation and management of excessive daytime sleepiness. Can J Neurol Sci. 2010;37(2):167–176. doi:10.1017/S0317167100009896
14. Okamura T, Ura C, Miyamae F, et al. Excessive daytime sleepiness is related to subjective memory impairment in late life: a cross-sectional community-based study. Psychogeriatrics. 2016;16(3):196–201. doi:10.1111/psyg.12139
15. Newman AB, Spiekerman CF, Enright P, et al.; The Cardiovascular Health Study Research Group. Daytime sleepiness predicts mortality and cardiovascular disease in older adults. J Am Geriatr Soc. 2000;48(2):115–123. doi:10.1111/j.1532-5415.2000.tb03901.x
16. Maestri M, Romigi A, Schirru A, et al. Excessive daytime sleepiness and fatigue in neurological disorders. Sleep Breath. 2020;24(2):413–424. doi:10.1007/s11325-019-01921-4
17. Bonanni E, Maestri M, Tognoni G, et al. Daytime sleepiness in mild and moderate Alzheimer’s disease and its relationship with cognitive impairment. J Sleep Res. 2005;14(3):311–317. doi:10.1111/j.1365-2869.2005.00462.x
18. Liu S, Huang Y, Tai H, et al. Excessive daytime sleepiness in Chinese patients with sporadic amyotrophic lateral sclerosis and its association with cognitive and behavioural impairments. J Neurol Neurosurg Psychiatry. 2018;89(10):1038–1043. doi:10.1136/jnnp-2018-318810
19. Simuni T, Caspell-Garcia C, Coffey C, et al. Correlates of excessive daytime sleepiness in de novo Parkinson’s disease: a case control study. Mov Disord. 2015;30(10):1371–1381. doi:10.1002/mds.26248
20. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
21. Buysse DJ, Reynolds CF
22. Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108(5):812–821. doi:10.1097/ALN.0b013e31816d83e4
23. Zhu W, Huang H, Yang S, et al. Cortical and subcortical grey matter abnormalities in white matter hyperintensities and subsequent cognitive impairment. Neurosci Bull. 2021;37(6):789–803. doi:10.1007/s12264-021-00657-0
24. Rijnen SJM, Meskal I, Emons WHM, et al. Evaluation of normative data of a widely used computerized neuropsychological battery: applicability and effects of sociodemographic variables in a dutch sample. Assessment. 2020;27(2):373–383. doi:10.1177/1073191117727346
25. Fazekas F, Chawluk JB, Alavi A, Hurtig HI, Zimmerman RA. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. AJR Am J Roentgenol. 1987;149(2):351–356. doi:10.2214/ajr.149.2.351
26. Doubal FN, MacLullich AM, Ferguson KJ, Dennis MS, Wardlaw JM. Enlarged perivascular spaces on MRI are a feature of cerebral small vessel disease. Stroke. 2010;41(3):450–454. doi:10.1161/STROKEAHA.109.564914
27. Staals J, Makin SD, Doubal FN, Dennis MS, Wardlaw JM. Stroke subtype, vascular risk factors, and total MRI brain small-vessel disease burden. Neurology. 2014;83(14):1228–1234. doi:10.1212/WNL.0000000000000837
28. Amier RP, Marcks N, Hooghiemstra AM, et al. Hypertensive exposure markers by MRI in relation to cerebral small vessel disease and cognitive impairment. JACC Cardiovasc Imaging. 2021;14(1):176–185. doi:10.1016/j.jcmg.2020.06.040
29. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56–62. doi:10.1136/jnnp.23.1.56
30. Ng TP, Tan WC. Prevalence and determinants of excessive daytime sleepiness in an Asian multi-ethnic population. Sleep Med. 2005;6(6):523–529. doi:10.1016/j.sleep.2005.01.007
31. Jaussent I, Morin CM, Ivers H, Dauvilliers Y. Natural history of excessive daytime sleepiness: a population-based 5-year longitudinal study. Sleep. 2020;43(3). doi:10.1093/sleep/zsz249
32. Chokesuwattanaskul A, Cheungpasitporn W, Thongprayoon C, et al. Impact of circadian blood pressure pattern on silent cerebral small vessel disease: a systematic review and meta-analysis. J Am Heart Assoc. 2020;9(12):e016299. doi:10.1161/JAHA.119.016299
33. Zuurbier LA, Ikram MA, Luik AI, et al. Cerebral small vessel disease is related to disturbed 24-h activity rhythms: a population-based study. Eur J Neurol. 2015;22(11):1482–1487. doi:10.1111/ene.12775
34. Sommer R, Yu L, Schneider JA, Bennett DA, Buchman AS, Lim ASP. Disrupted rest-activity rhythms and cerebral small vessel disease pathology in older adults. Stroke. 2021;52(7):2427–2431. doi:10.1161/STROKEAHA.120.030870
35. Bohnen NI, Muller ML, Kuwabara H, Constantine GM, Studenski SA. Age-associated leukoaraiosis and cortical cholinergic deafferentation. Neurology. 2009;72(16):1411–1416. doi:10.1212/WNL.0b013e3181a187c6
36. Mesulam M, Siddique T, Cohen B. Cholinergic denervation in a pure multi-infarct state: observations on CADASIL. Neurology. 2003;60(7):1183–1185. doi:10.1212/01.WNL.0000055927.22611.EB
37. Mesulam MM, Geula C. Nucleus basalis (Ch4) and cortical cholinergic innervation in the human brain: observations based on the distribution of acetylcholinesterase and choline acetyltransferase. J Comp Neurol. 1988;275(2):216–240. doi:10.1002/cne.902750205
38. Selden NR, Gitelman DR, Salamon-Murayama N, Parrish TB, Mesulam MM. Trajectories of cholinergic pathways within the cerebral hemispheres of the human brain. Brain. 1998;121(Pt 12):2249–2257. doi:10.1093/brain/121.12.2249
39. Ishii N, Nishihara Y, Imamura T. Why do frontal lobe symptoms predominate in vascular dementia with lacunes? Neurology. 1986;36(3):340–345. doi:10.1212/WNL.36.3.340
40. Basta M, Koutentaki E, Vgontzas A, et al. Objective daytime napping is associated with disease severity and inflammation in patients with mild to moderate dementia1. J Alzheimers Dis. 2020;74(3):803–815. doi:10.3233/JAD-190483
41. Prins ND, Scheltens P. White matter hyperintensities, cognitive impairment and dementia: an update. Nat Rev Neurol. 2015;11(3):157–165. doi:10.1038/nrneurol.2015.10
42. Debette S, Markus HS. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: systematic review and meta-analysis. BMJ. 2010;341:c3666. doi:10.1136/bmj.c3666
43. Werring DJ, Frazer DW, Coward LJ, et al. Cognitive dysfunction in patients with cerebral microbleeds on T2*-weighted gradient-echo MRI. Brain. 2004;127(Pt 10):2265–2275. doi:10.1093/brain/awh253
44. Ding J, Sigurethsson S, Jonsson PV, et al. Space and location of cerebral microbleeds, cognitive decline, and dementia in the community. Neurology. 2017;88(22):2089–2097. doi:10.1212/WNL.0000000000003983
45. Ding J, Sigurethsson S, Jonsson PV, et al. Large perivascular spaces visible on magnetic resonance imaging, cerebral small vessel disease progression, and risk of dementia: the Age, Gene/Environment Susceptibility-Reykjavik Study. JAMA Neurol. 2017;74(9):1105–1112. doi:10.1001/jamaneurol.2017.1397
46. Hilal S, Mok V, Youn YC, Wong A, Ikram MK, Chen CL. Prevalence, risk factors and consequences of cerebral small vessel diseases: data from three Asian countries. J Neurol Neurosurg Psychiatry. 2017;88(8):669–674. doi:10.1136/jnnp-2016-315324
47. Merlino G, Piani A, Gigli GL, et al. Daytime sleepiness is associated with dementia and cognitive decline in older Italian adults: a population-based study. Sleep Med. 2010;11(4):372–377. doi:10.1016/j.sleep.2009.07.018
48. Tsapanou A, Gu Y, Manly J, et al. Daytime sleepiness and sleep inadequacy as risk factors for dementia. Dement Geriatr Cogn Dis Extra. 2015;5(2):286–295. doi:10.1159/000431311
49. Nakakubo S, Doi T, Makizako H, et al. Sleep condition and cognitive decline in Japanese community-dwelling older people: data from a 4-year longitudinal study. J Sleep Res. 2019;28(4):e12803. doi:10.1111/jsr.12803
50. Endeshaw Y, Rice TB, Schwartz AV, et al. Snoring, daytime sleepiness, and incident cardiovascular disease in the health, aging, and body composition study. Sleep. 2013;36(11):1737–1745. doi:10.5665/sleep.3140
51. Zhang K, Jiang Y, Wang Y, et al. Associations of arterial stiffness and carotid atherosclerosis with cerebral small vessel disease in a rural community-based population. J Atheroscler Thromb. 2020;27(9):922–933. doi:10.5551/jat.52530
52. Rensma SP, van Sloten TT, Launer LJ, Stehouwer CDA. Cerebral small vessel disease and risk of incident stroke, dementia and depression, and all-cause mortality: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2018;90:164–173. doi:10.1016/j.neubiorev.2018.04.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.