")
Back to Journals » Clinical Interventions in Aging » Volume 17
Association of Elevated Thyroid Stimulating Hormone with Atherosclerotic Cardiovascular Disease and Its Mortality in Elderly Community-Dwelling Chinese
Authors Wang Y, Liu C, Liu L, Chen X, Wei L, Liu J, Peng S, Pi J, Zhang Q, Tomlinson B , Chan P , Zhang L, Fan H, Zheng L, Liu Z, Zhang Y
Received 27 March 2022
Accepted for publication 30 June 2022
Published 2 August 2022 Volume 2022:17 Pages 1139—1150
DOI https://doi.org/10.2147/CIA.S368219
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
YingLu Wang,1,* Chang Liu,1,* Liping Liu,1,* Xiaoli Chen,1 Lu Wei,1 Jie Liu,1 Sheng Peng,2 Jingjiang Pi,3 Qi Zhang,3 Brian Tomlinson,4 Paul Chan,5 Lin Zhang,1 Huimin Fan,1 Liang Zheng,1 Zhongmin Liu,1 Yuzhen Zhang1
1Key Laboratory of Arrhythmias of the Ministry of Education of China, Research Center for Translational Medicine, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China; 2Department of Emergency Medicine, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China; 3Department of Cardiology, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China; 4Faculty of Medicine, Macau University of Science and Technology, Macau, People’s Republic of China; 5Division of Cardiology, Department of Internal Medicine, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan, Republic of China
*These authors contributed equally to this work
Correspondence: Yuzhen Zhang; Zhongmin Liu, Key Laboratory of Arrhythmias of the Ministry of Education of China, Research Center for Translational Medicine, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China, Tel +86 21-61569673, Email [email protected]; [email protected]
Purpose: With increase of population aging, the prevalence of atherosclerotic cardiovascular disease (ASCVD) and elevated serum thyroid stimulating hormone (TSH) in elderly is increasing. High TSH level was reported to be associated with ASCVD and CVD mortality; however, few are studied in Chinese population, especially in the elderly. This study aimed to investigate the prevalence of elevated serum TSH and ASCVD in an elderly population of Chinese community and to explore the association between high serum TSH and ASCVD or CVD mortality.
Patients and Methods: We conducted a study involving 3814 adults who were at least 60 years of age. Questionnaires, physical examinations, and laboratory blood samples were collected in 2014, and a 78-months follow-up for cardiovascular and all-cause mortality was performed till December of 2020. Logistics regression was used to analyze the association between TSH and ASCVD. We used Cox models to assess the hazard ratios (HRs) for all-cause and CVD mortality across changes in serum TSH.
Results: In this study, the prevalence of the elevated serum TSH was 19.8%, and significantly higher in women than in men (24.5% vs 13.9%, p < 0.001). The prevalence of ASCVD was 21.7%. In logistics regression models, elevated TSH was associated with ASCVD after adjusting for the risk factors of ASCVD in people over the age of 70 years (adjusted OR 1.054, P = 0.014). After a follow-up of 6.5 years, total 441 (11.6%) all-cause death and 174 (4.6%) death of CVD were observed. In Cox regression model, no significant correlation was found between TSH and all-cause mortality or CVD mortality in the elderly population.
Conclusion: In the elderly population, there is high prevalence of elevated serum TSH and ASCVD. Elevated TSH seemed to be not associated with risk of all-cause or CVD mortality.
Keywords: cardiovascular disease, thyroid stimulating hormone, mortality, community-dwelling elderly
Introduction
Arteriosclerotic cardiovascular disease (ASCVD) remains the leading cause of cardiovascular disease (CVD) morbidity and mortality globally. With population aging, ASCVD prevalence rates and CVD mortality are increasing.1–3 Therefore, it is necessary to find and control the risk factors to reduce ASCVD progression and CVD mortality. Subclinical hypothyroidism (SCH) is defined as elevated thyroid-stimulating hormone (TSH) concentrations with normal free thyroxine (T4) levels. The prevalence of SCH has been reported to be between 4% and 20% in general populations and especially higher in elderly women.4–6 A fairly wide, but reproducible reference range for TSH, typically 0.5–4.5 mIU/L, was established in large populations.4,7 However, this TSH range should be applied to define normal thyroid function in general populations has been debated over the past 15 years, and serum TSH distribution curves shift to higher concentrations with increasing age. There are guidelines agreed to raise the target serum TSH in elderly above 70 years to avoid overtreatment.8,9 Therefore, the current range of reference values in elderly population may require more careful application.
Several studies showed that elevated TSH was associated with many major risk factors of ASCVD, such as a significantly higher risk of hypertension, diabetes, and hyperlipidemia in adults with higher TSH.10–14 These findings were mostly conducted in the general population, the levels of TSH might fluctuate in the elderly and the factors that cause fluctuations might be different from the general population.15 The association of elevated TSH and the risk of CVD mortality remain controversial as well. A meta-analysis of prospective cohort studies of the association between elevated TSH and CVD or all-cause mortality found that elevated TSH modestly increased the risk of both CVD and all-cause mortality.16 However, some studies showed there was no association between elevated TSH and CVD or mortality in the elderly, although the number of studies conducted was small,5,17,18 and one study showed that elevated TSH levels reduced the risk of all-cause mortality.19 Therefore, the elevated TSH for the risk of ASCVD and CVD mortality remains to be established in the elderly and one study showed that elevated TSH levels reduced the risk of all-cause mortality.
Based on the high prevalence of ASCVD and elevated TSH in the elderly Chinese population, as well as the uncertainty of the association between elevated TSH and CVD. We recruited community residents aged ≥60 years to evaluate the prevalence of elevated serum TSH and ASCVD, and to investigate the relationship between elevated serum TSH and ASCVD or CVD mortality and provide evidence of age-specific TSH reference value division in elderly population.
Materials and Methods
Study Population
The Shanghai Elderly Cardiovascular Health Study (SHECHS) is a community population-based study of non-institutionalized adults aged ≥60 years. The design details were as previously described. Participants having history of thyroid disease or taking medication affecting the thyroid such as thyroxine, antithyroid drugs, or glucocorticoid were excluded, and 3814 participants having complete baseline data were followed up 78 months for all-cause and cardiovascular mortality.
The SHECHS study was conducted according to the principles established in the Declaration of Helsinki of 1975 and approved by the Institutional Review Board of Shanghai East Hospital affiliated with Tongji Medical College, and all participants provided informed written consent at enrollment.
Data Collection
The standard clinic for participants in the study included an interview, physical examination, and laboratory tests. The participants attended Gaohang community medical center in the morning after overnight fasting for at least 10 hours and their blood samples were taken, with serum TSH, glucose, lipids, renal and hepatic function in tubes without anticoagulant and HbA1c and other tests in tubes containing EDTA. The blood samples were measured within 2 hours in the Blood Laboratory of Tongji Medical School affiliated Shanghai East Hospital. Serum total cholesterol (TC), low-density lipoprotein cholesterin (LDL-C), high-density lipoprotein cholesterin (HDL-C), fasting serum glucose (FG), and triglycerides (TG) were measured enzymatically on the Roche Cobas8000 c702 Biochemistry system. Blood HbA1c was measured by ion-exchange high-performance liquid chromatography on the ToSoH G8 analyzer. Information regarding smoking status, alcohol intake, physical activity, cancer, and medication history including hypertension, diabetes mellitus, and hypercholesterolemia were obtained from the medical questionnaire.
Study-Outcome Definitions
Serum TSH level was measured by chemiluminescent immunoassay (Roche Diagnostics GmbH, Mannheim, Germany) and the measuring range was 0.005–100 mIU/L. A normal Serum TSH reference range, 0.27–4.20 mIU/L, was used according to a cross-sectional study of 15,008 elderly people in 10 cities of China,20 and high TSH as a serum TSH level over 4.20 mIU/L and low TSH as less than 0.270 mIU/L.
We defined hypertension as an average of two measurements of systolic blood pressure (SBP) ≥140 mmHg or diastolic blood pressure (DBP) ≥90 mmHg or normal BP with concomitant use of anti-hypertensive drugs.21 We defined diabetes mellitus (DM) as fasting serum glucose (FG) ≥7.0 mmol/L or normal FG with concomitant use of insulin or oral hypoglycemic agents.22 We defined hyperlipidemia as TC ≥6.2 mmol/L or TG ≥2.3 mmol/L or normal blood lipid with concomitant use of lipid-lowering medications.23
We defined clinical ASCVD as having a history of myocardial infarction (MI), coronary or other arterial revascularization, stable or unstable angina, stroke, transient ischemic attack (TIA) or peripheral artery disease and was confirmed by review of the outpatient medical records of primary care in the community health centers.24 We defined CVD death as death due to cardiovascular diseases, and CVD events included ischemic heart disease, hemorrhagic and other nonischemic stroke, hypertensive heart disease, other cardiovascular and circulatory diseases, ischemic stroke, cardiomyopathy and myocarditis, rheumatic heart disease, congestive heart failure, aortic aneurysm, atrial fibrillation and flutter, endocarditis peripheral vascular disease.25 To establish a diagnosis, a panel of 3 physicians reviewed each cardiovascular event according to pre-established criteria.
Mortality Surveillance
We followed up the participants for mortality by the death report cards from Centers for Disease Control and Prevention in Pudong New District, Shanghai, China, dated from the last examination to the date of death till December 31, 2020, and the primary endpoints were death and CVD death.
Statistical Analysis
Descriptive statistics were calculated for all variables and significant differences in continuous variables were determined by ANOVA and Students t-test, and categorical percentile values were compared by Chi-squared test (χ2-test). The population was divided into groups according to age, gender, and TSH levels for analysis. Binary-logistic regression analysis was used to examine the association of ASCVD with serum TSH by estimating odds ratios (ORs) and 95% confidence intervals (CIs). Kaplan–Meier survival curves by TSH groups were used to summarize the time to death up to 78 months of follow-up. We used Cox proportional hazard models to estimate the hazard ratios (HRs) and 95% CIs for all-cause and CVD mortality across changes in serum TSH. Hazards ratios for serum TSH as a risk factor for CVD were examined with Cox proportional hazards regression. The models were age- and sex-adjusted and then further adjusted for hypertension (SBP), diabetes mellitus (HbA1c), hyperlipidemia (TC, TG, HDL-C), obesity (body mass index, BMI), creatinine and homocysteine. All statistical analysis was performed using SPSS20.0 software (SPSS Inc, Chicago, IL, USA) and a two-tailed P value <0.05 for a statistical test was considered to be statistically significant.
Results
Demographic and Clinical Characteristics of Participants
The baseline characteristics of the participants are presented in Table 1. Among the 3814 participants with a mean age of 72.2 years, 1682 were male and 2132 were female. The mean serum TSH level was 3.49 mIU/L, with a higher level in female than in male (3.76 mIU/L vs 3.14 mIU/L, P < 0.001). A significantly increased TSH levels in 70–79 and ≥80 years groups compared to the participants aged less than 70 years (3.19 mIU/L and 3.47 mIU/L vs 3.97 mIU/L P < 0.01), and the participants aged ≥80 years had highest level, the prevalence of ASCVD was 21.7% and increased with age (17.1% vs 24.9% vs 27.3% in three age group correspondingly). Also, the highest value of waist circumference, SBP, FG, HDL-C, and the lowest DBP, TG, was observed in the oldest group.
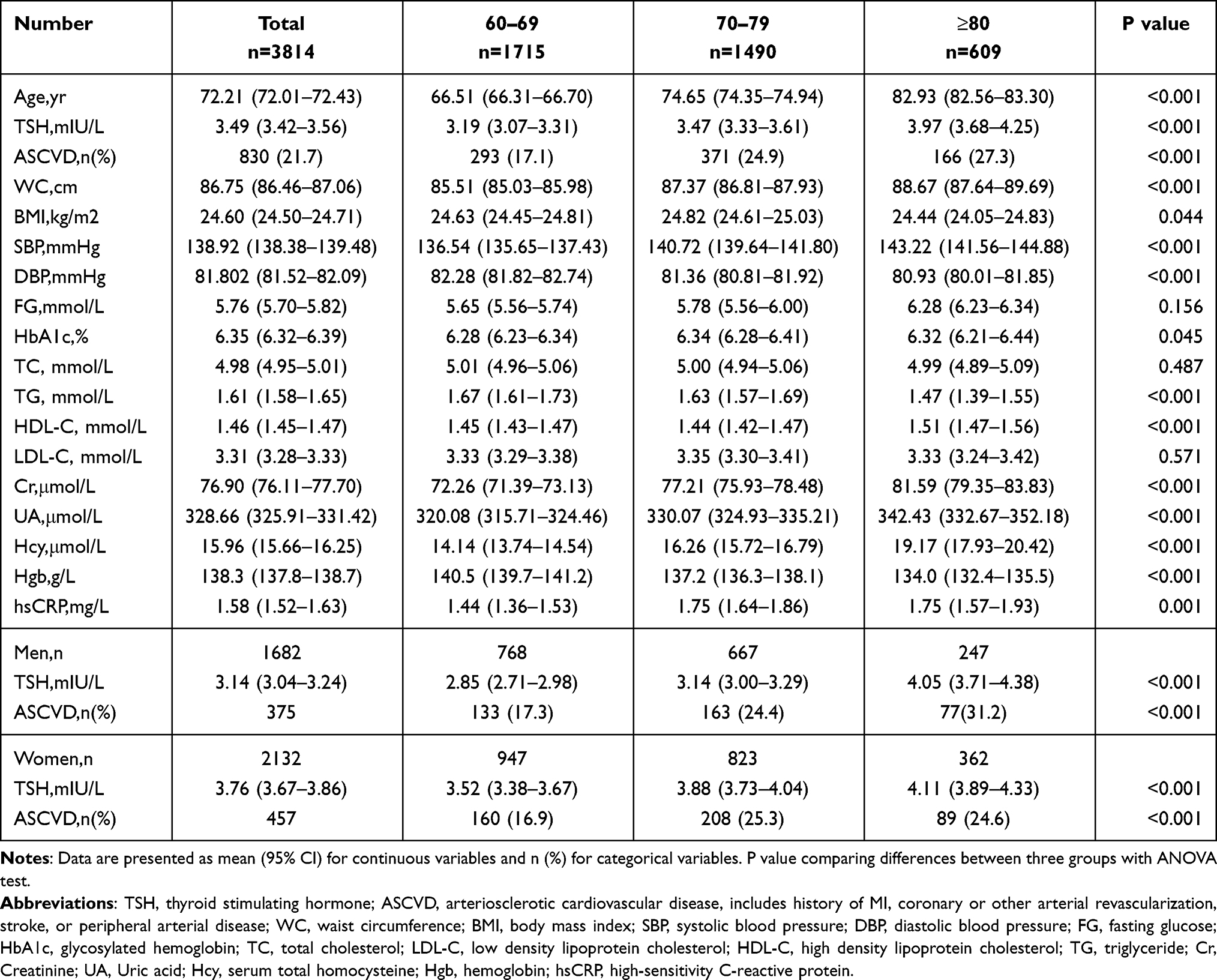 |
Table 1 Baseline Characteristics of Participants Stratified by Age and Gender |
Prevalence of Elevated TSH in Different Gender and Age Groups
The prevalence of elevated serum TSH level in the community elderly population is shown in Table 2 and Figure 1. Serum TSH levels were classified as low (<0.27 mIU/L), medium (0.27–4.20 mIU/L) or high (≥4.2 mIU/L) TSH levels. The prevalence of high TSH in the whole cohort was 19.8%, nearly twice as common in females compared to males (24.5% in females vs 13.9% in males, P < 0.001). Then, we divided high TSH level into mild (4.2–10 mIU/L) and severe (≥10 mIU/L) TSH level to further investigate whether there were differences in the degree of TSH elevation between groups. High TSH prevalence in females was mostly mild TSH elevation with no significant change in severe elevation between genders, and high TSH prevalence increased with aging in both genders (17.1% vs 20.6% vs 25.3%, P < 0.001). There were only 14 participants whose serum TSH level less than 0.27 in the community elderly population with no difference between men and women, and none of them was over 80 years old.
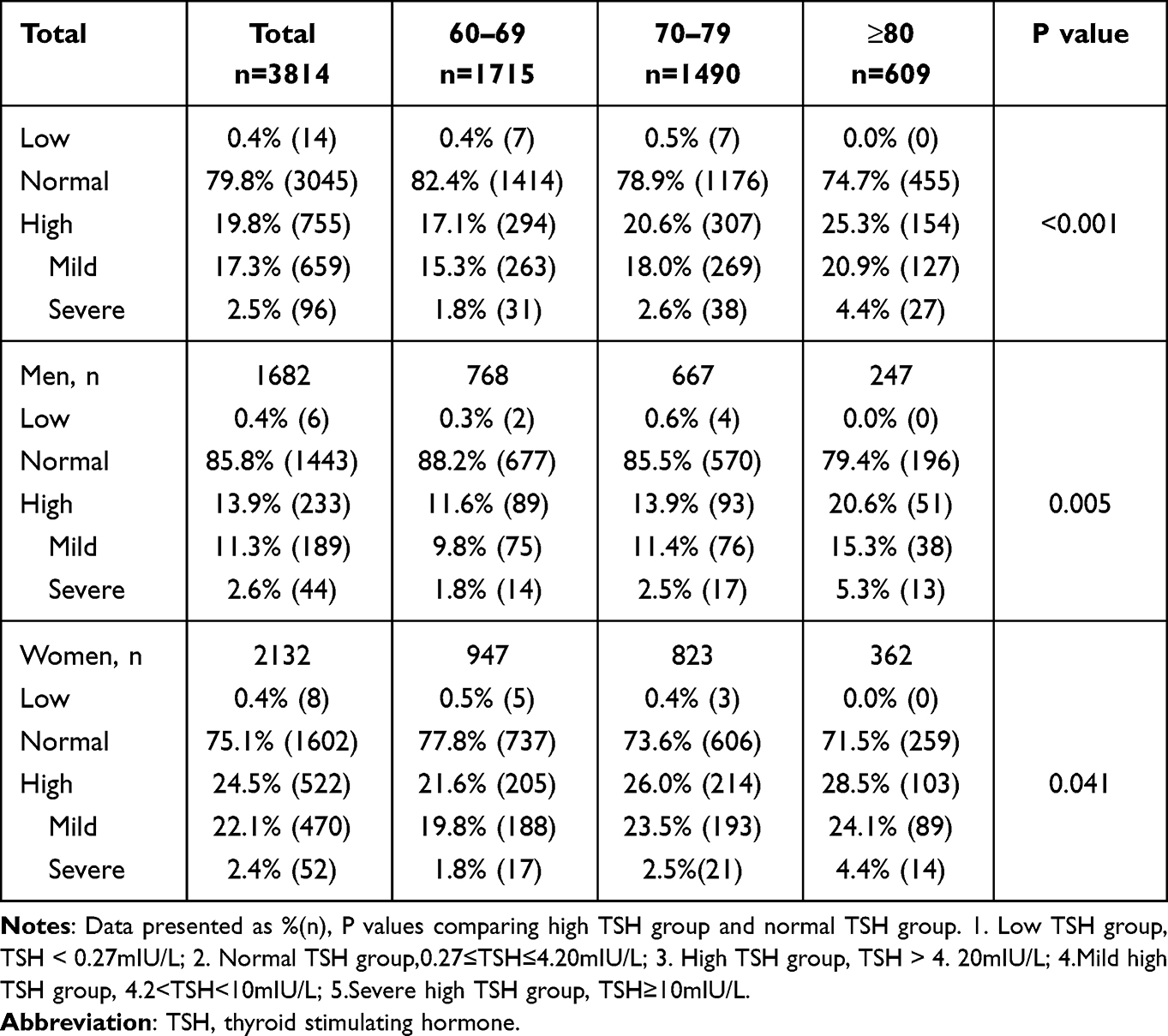 |
Table 2 Prevalence of TSH Stratified by Age and Gender |
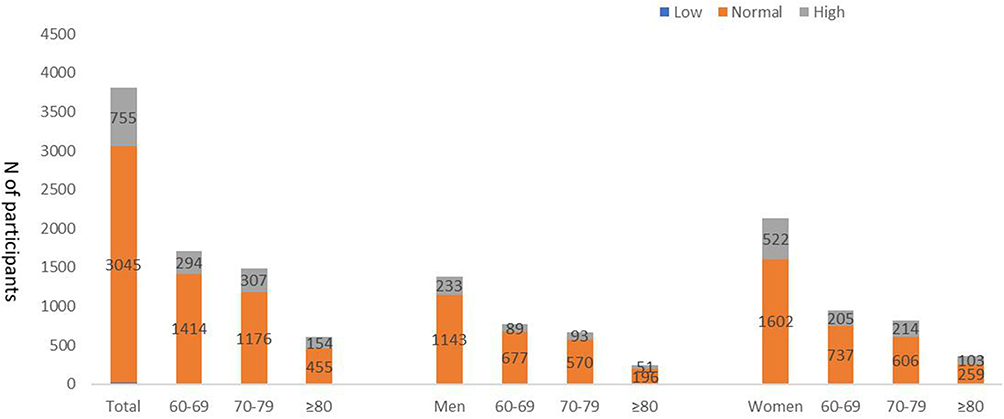 |
Figure 1 Prevalence of TSH stratified by age and gender. 1. Low TSH group, TSH<0.27mIU/L; 2. Normal TSH group, 0.27≤TSH≤4.20mIU/L; 3. High TSH group, TSH>4.20mIU/L. Abbreviation: TSH, thyroid stimulating hormone. |
Association of High TSH with ASCVD and Risk Factor Multivariate Assessment
Next, analysis of normal and high TSH participants was performed to observe the association of elevated serum TSH level with ASCVD and the risk factors. In multivariate-adjusted logistic regression models, we found that elevated TSH was not significantly associated with ASCVD. However, a subgroup analysis was performed among 2099 people older than 70 years, and the association of elevated TSH level with ASCVD was significantly different as shown in Table 3 and Figure 2A. The different associations were observed even after further adjusting for the risk factors of ASCVD including hypertension (SBP), diabetes (HbA1c), obesity (BMI), TC, HDL, TG, homocysteine and creatinine (model 2, model multivariate adjusted OR 1.054, 95% CI 1.011–1.100, P = 0.014). These results suggest that elevated TSH is associated with ASCVD in this elderly Chinese community population. However, there is no association between TSH and ASCVD by gender after adjusting for the risk factors of ASCVD.
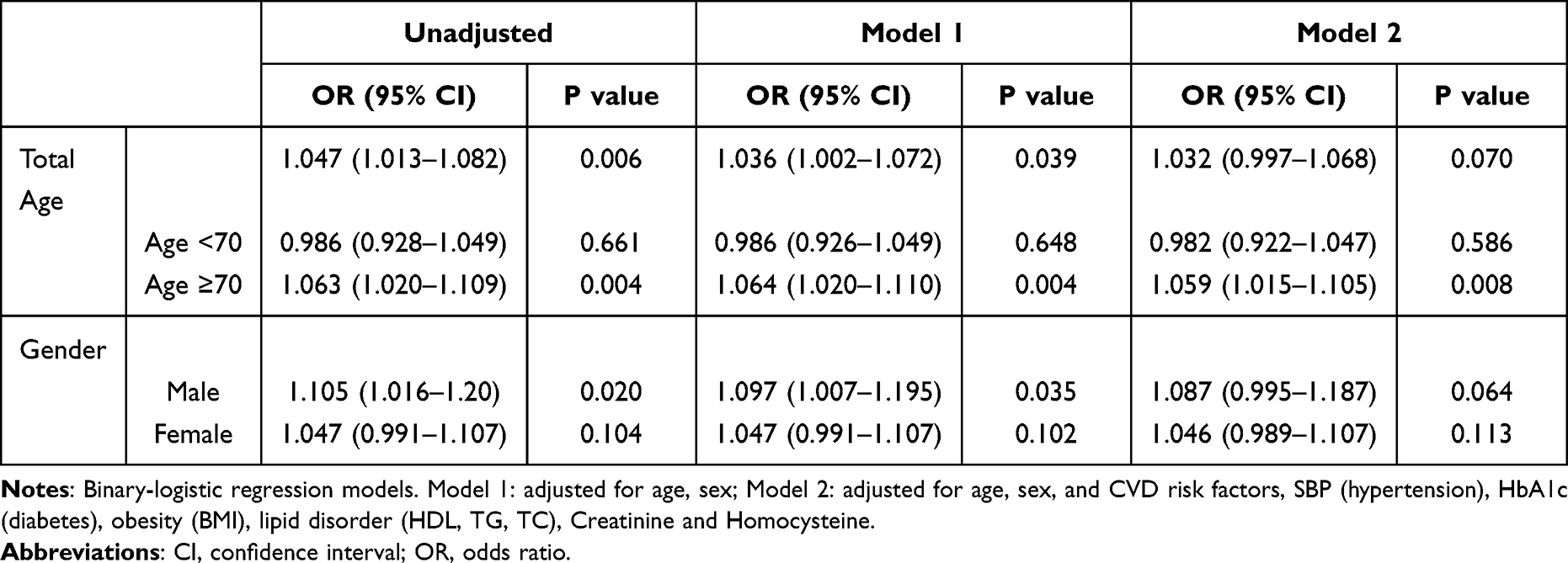 |
Table 3 Multivariate-Adjusted Odds Ratios of TSH and ASCVD Stratified by Age and Gender |
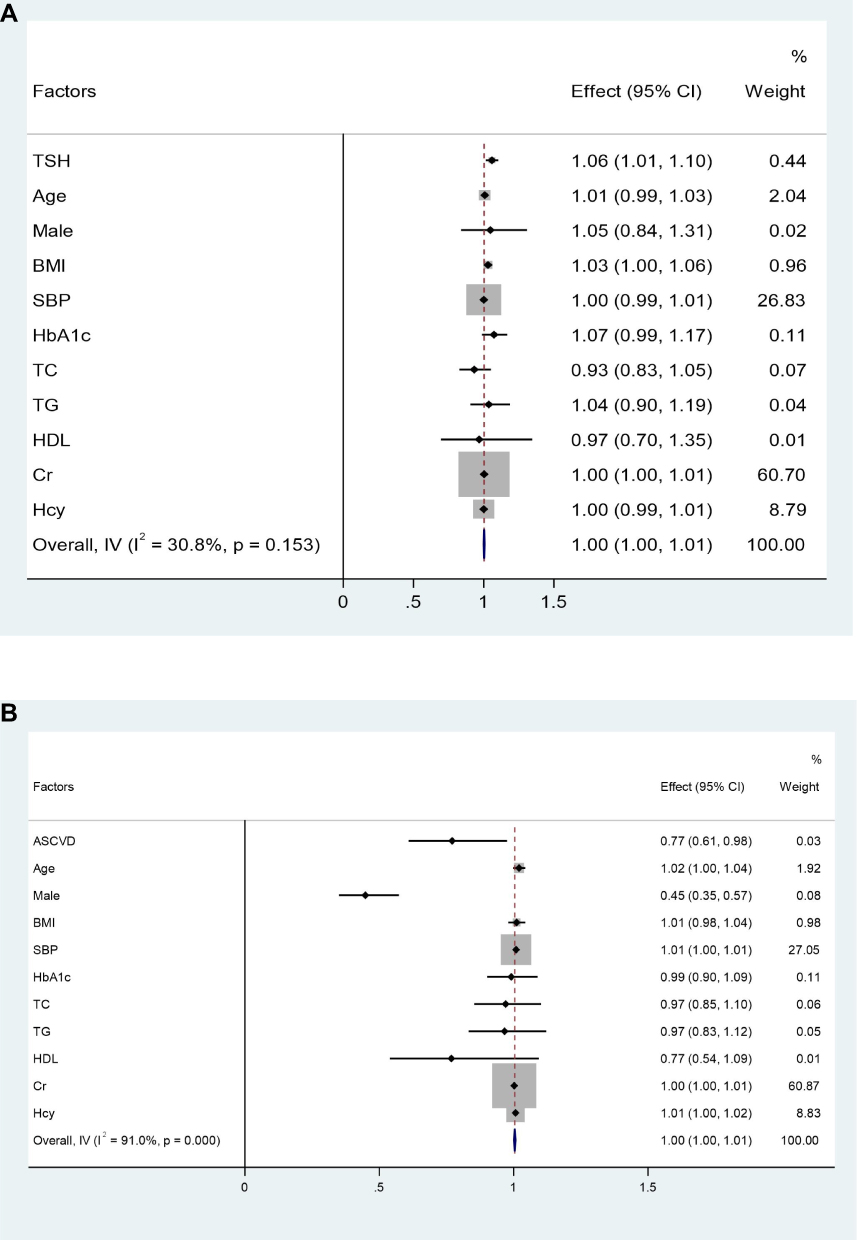 |
Figure 2 (A) Analysis of ASCVD risk factors in Age≥70 years. Binary-logistics regression models. Normal TSH group, 0.27≤TSH≤4.20mIU/L; High TSH group, TSH>4.20mIU/L. Model1: adjusted for age, and sex. Model2: adjusted for age, sex, and CVD risk factors, SBP (hypertension), HbA1c (diabetes), obesity (BMI), lipid disorder (HDL, TG, TC), Creatinine and Homocysteine. (B) Analysis of high TSH levels risk factors in Age ≥70 years. Binary-logistics regression models. Normal TSH group, 0.27≤TSH≤4.20mIU/L; High TSH group, TSH>4.20mIU/L. Model1: adjusted for age, and sex. Model2: adjusted for age, sex, and CVD risk factors, SBP (hypertension), HbA1c (diabetes), obesity (BMI), lipid disorder (HDL, TG, TC), Creatinine and Homocysteine. Abbreviations: CI, confidence interval; OR, odds ratio. |
There are significant higher ASCVD in elevated TSH group compared with normal TSH group (Supplementary Table S1, P = 0.002). We found more ASCVD, hypertension, DM but less smokers in the high TSH group, and homocysteine increased but Hgb decreased in high TSH group. Then, we investigated the association between ASCVD risk factors and elevated TSH levels using multivariable-adjusted binary-logistic regression with the same models, and found that age, being female, and hypertension (SBP) were associated with elevated TSH (Figure 2B). These results suggest that elevated TSH is associated with ASCVD by its risk factors including age, gender, blood pressure, but to a modest degree in this elderly Chinese community population.
Association of Elevated Serum TSH with All-Cause and CVD Mortality
Further analysis of normal and high TSH participants was performed to observe the association of elevated serum TSH level with all-cause and CVD mortality. Participants of 3800 were enrolled during a 78-months follow-up period, with 194 (5.0%) were lost for relocation or other reasons. There were 441 deaths from all-causes and 174 deaths from CVD, and cardiovascular deaths account for 39.5% of all-cause deaths. In the entire cohort, all-cause mortality was 11.6% and CVD mortality was 4.6%. We compared characters between the survival and CVD death groups in Supplementary Table S2. Compared to the survivors, serum TSH level was higher in CVD decedents (3.43 vs 4.29, P < 0.001), and decedents had a higher prevalence of ASCVD (40.8% vs 21.1%, P < 0.001), a higher prevalence of hypertension (74.7% vs.56.1%, P < 0.001), and a higher prevalence of diabetes (28.7% vs.15.5%, P < 0.001).
Kaplan–Meier survival analysis for all-cause and CVD mortality in elderly participants is shown in Figure 3. The results showed a median survival time for CVD mortality of 74.6 (74.2–75.0) and 73.86 (72.92–74.76) months for participants in normal and high TSH groups, respectively. After 20 months, survivors in high TSH group tended to be lower than those in normal TSH group, especially in women. The difference of all-cause mortality between two groups was similar.
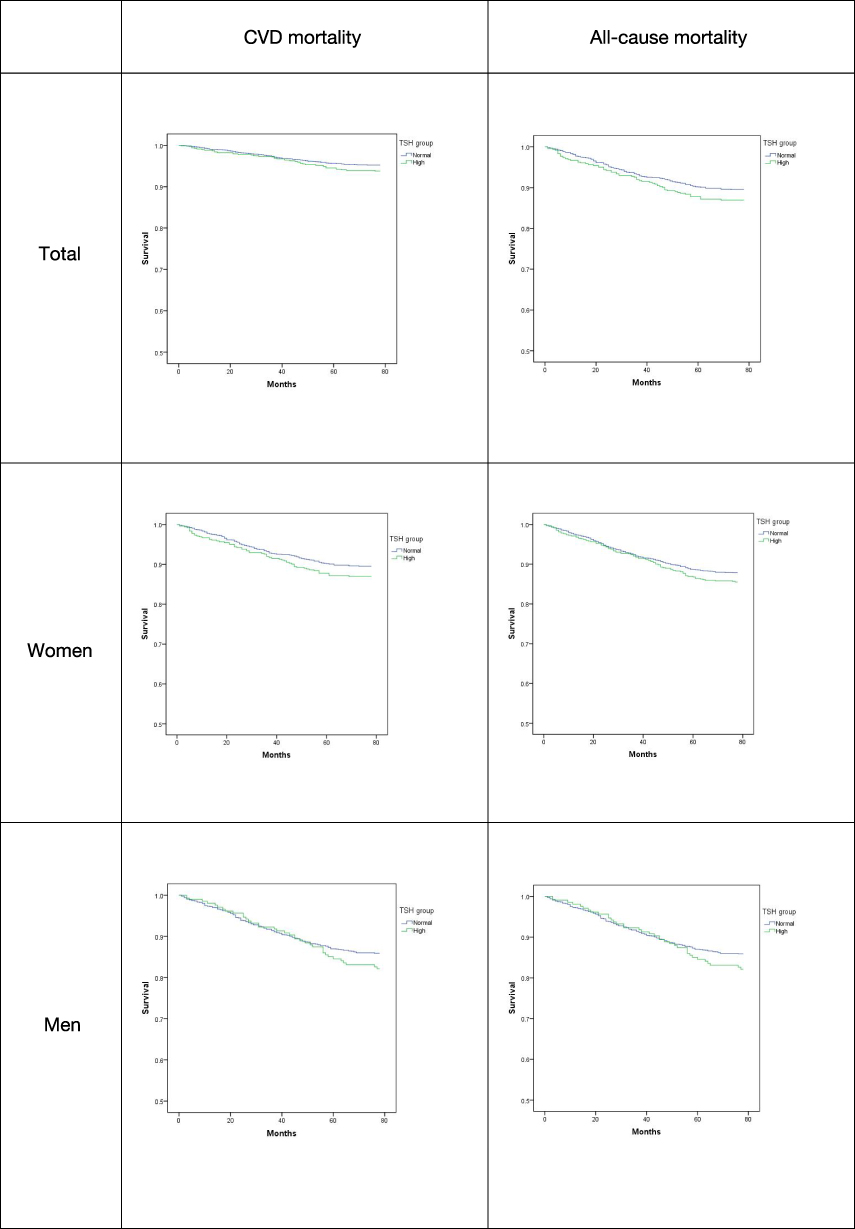 |
Figure 3 Estimated survival among TSH groups with Kaplan-Meier survival analysis. Kaplan-Meier plots of survival with all-cause or CVD death by TSH levels. Normal TSH group, 0.27≤TSH≤4.20mIU/L; High TSH group, TSH>4.20mIU/L. |
The association of elevated TSH level and CVD mortality is shown in Table 4, and three multivariate-adjusted COX regression models were performed with adjusted stratification variables (age, gender, and CVD risk factors, SBP (hypertension), HbA1c (diabetes), BMI (obesity), HDL, TG, creatinine, homocysteine, Hgb and hsCRP). No association was observed between TSH and all-cause mortality or CVD mortality in this elderly population.
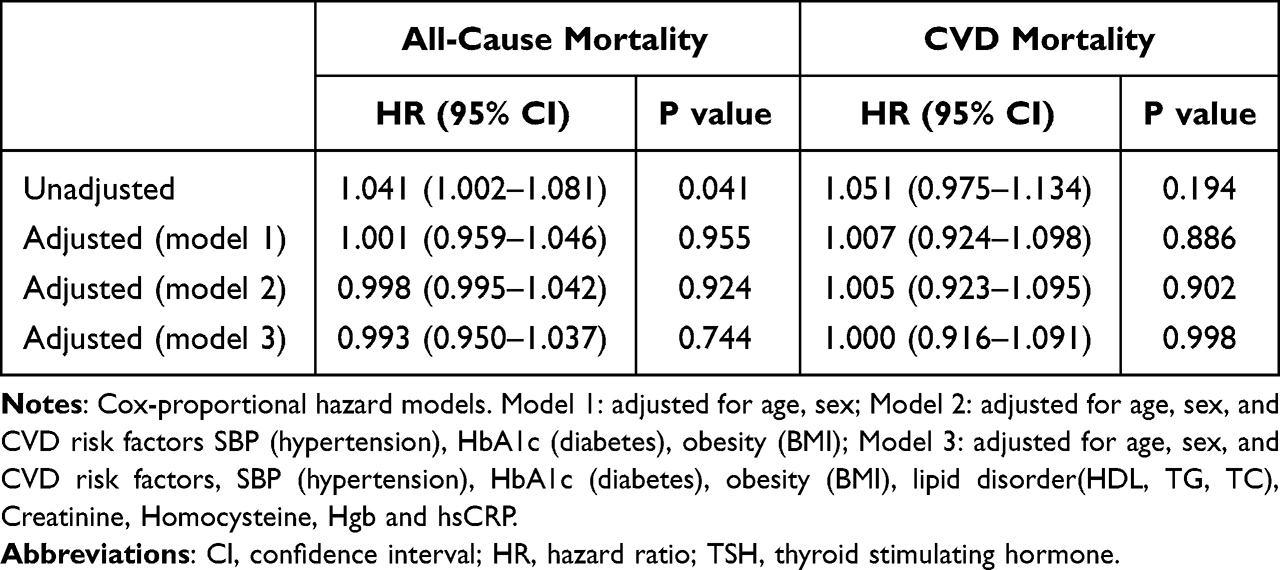 |
Table 4 Multivariable–Adjusted Hazard Ratios for TSH and CVD Death |
Discussion
In this community-based study, we found high prevalence of elevated TSH and ASCVD in the elderly Chinese. Elevated TSH was modestly associated with ASCVD but was not associated with CVD mortality or all-cause mortality.
Elevated TSH should play a different role in predisposing to ASCVD people above or below the age of 70. We observed an association of elevated TSH with increased ASCVD risk in the elderly aged 70 years and over. Also, we found that high TSH was correlated with several main risk factors of ASCVD including age, gender, and SBP (hypertension). In consistent with our study, several studies showed a correlation between elevated TSH and ASCVD and its risk factors as age, gender, hypertension, diabetes, and lipid metabolism abnormalities.26–28
TSH was considered to be associated with increased blood pressure by changing myocardial oxygen consumption, myocardial contractility and output, and systemic vascular resistance.29–31 Similarly, elevated TSH can be associated with increased insulin resistance through a variety of mechanisms, and insulin resistance is important for diabetes development and progression.32 In consistent with the reference findings, we demonstrated higher prevalence of hypertension and diabetes in the high TSH group than in the normal TSH group in our elderly population-based study (Supplementary Table S1). Therefore, we may pay more attention to monitor and control blood pressure and blood glucose in the elevated TSH patients to improve survival of the elderly community residents.
As for a slight increase in TSH levels (below 10 mIU/mL) not associated with the increased mortality in elderly, we did not observe a correlation between elevated TSH and CVD or all-cause mortality in the elderly community residents through a 78-month follow-up period. Our finding is in consistent with some prior studies investigating the relation between TSH levels and the risk of mortality.33,34 Moreover, several meta-analysis also showed that elevated TSH was not associated with CVD or all-cause mortality,35 and also a community-based study with over 20 years follow-up supported no association between elevated TSH and CVD or all-cause mortality, and participants aged 65 years and older did not show significant difference.36 However, there is still debate and some studies indicated an association of elevated TSH level with increased mortality.11,37–39 Further we will follow-up longer time to increase the mortality numbers and clarify whether elevated TSH level is correlated with CVD or all-cause mortality in the elderly community residents.
There are three potential mechanisms that may explain the lack of association between high TSH levels and the risk of mortality. First, the elderly was reported to be not sensitive to adrenergic stimulation and the hypothalamic-pituitary feedback system.40–42 Second, their metabolic rate and energy expenditure were proved to be slow. These factors may reduce the risk of death from high TSH levels in the elderly. Finally, a study tracking estimates of persistence, resolution and progression of subclinical hypothyroidism showed that the duration of TSH elevation was not long enough, and TSH elevation could recover in a short time. The low degree and short duration of TSH elevation were not sufficient to cause negative events associated with CVD death.42
Our study showed no gender difference of the correlation between TSH and ASCVD. Consistent with our results, a study showed an association of elevated TSH and ASCVD risk with no gender difference in older age.43 However, another 12-year follow-up study found a significantly higher risk of ASCVD in women.44 Elevated TSH is common in elderly women, and the association of ASCVD or mortality is usually weak, therefore the associations between gender deserves further study.
In addition to gender difference, serum TSH level increases with age and may normally compensate in those aged 65 and older. This provides evidence that elderly population might require a specific serum TSH reference value and we recommend age-specific serum TSH reference range in elderly to evaluate the thyroid function status in order to prevent misdiagnosis and mistreatment.
Limitations
The current study has several limitations: First, we lacked the data of FT3, FT4 or other related indices to assess thyroid function more comprehensively. Second, serum TSH was not measured again during the follow-up period, so it was impossible to determine the thyroid function status of the participants at the time of the outcome event. Monitoring serum TSH changes over time may be helpful to understand the association between elevated serum TSH level and clinical outcomes. Third, the mean follow-up time was 6.5 years, and some thyroid dysfunction may occur after a longer period of time. The studies of elderly population in this area are not sufficient and more follow-up or perspective intervention studies are required to confirm the association.
Conclusion
In conclusion, there was high prevalence of elevated serum TSH level and ASCVD in the elderly of Gaohang community population, Shanghai, China. Elevated TSH was associated with ASCVD and the risk factors, especially in the age group of those over 70 years. However, the elevated TSH level was not associated with increased risk of all-cause or CVD mortality. These findings support the necessity and importance of evaluation of subclinical thyroid dysfunction in clinical practice and provides evidence of a specific serum TSH reference value require in order to prevent misdiagnosis and mistreatment in the elderly population.
Acknowledgments
We would like to acknowledge the reviewers for their helpful comments and the editors for their kind work on this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the funds from the National Natural Science Foundation of China (81970234, 82130016, 81970233, 82170257, 81970232, 81903171, 82070456, 82170477), Shanghai Rising-Star Program (20QA1408100, 21QA1401400), Shanghai Science and Technology innovation Action Plan (19JC1414500), The National Key R&D Program of China (2017YFA0105604), Health System Academic Leader Training Plan of Pudong District Shanghai (PWRd2018-06), Young Medical Talents Training Program of Pudong Health Bureau of Shanghai (PWRq2021-04) and Peak Disciplines (Type IV) of Institutions of Higher Learning in Shanghai.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Liyuan M, Yazhe W, Wen W, Weiwei C. Interpretation of the report on cardiovascular diseases in China (2017). Chin J Cardiol. 2018;23(1):3–6.
2. Lloyd-Jones DM, Hong Y, Labarthe D, et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association’s strategic impact goal through 2020 and beyond. Circulation. 2010;121(4):586. doi:10.1161/CIRCULATIONAHA.109.192703
3. Kochanek KD, Murphy S, Xu J. Arias EJNdb. Mortality U S. 2016;2017(293):1–8.
4. Hollowell J, Serum TSH, Flanders WD. T4, and Thyroid Antibodies in the United States Population (1988 to 1994): national health and nutrition examination survey (NHANES III). J Clin Endocr Metabolism. 2002;87:489–499. doi:10.1210/jcem.87.2.8182
5. Cappola AR, Fried LP, Arnold AM, et al. Thyroid Status. Cardiol Risk Mortality Older Adults. 2006;295(9):1033–1041.
6. Boelaert K; Boelaert, and Kristien. Thyroid dysfunction in the elderly. Nat Rev Endocrinol. 2013;9:194–204. doi:10.1038/nrendo.2013.30
7. Baloch Z, Carayon P, Conte-Devolx B, Demers LM. Laboratory medicine practice guidelines. Laboratory support for the diagnosis and monitoring of thyroid disease. Thyroid. 2003;13(1):3–126. doi:10.1089/105072503321086962
8. Sue W, Parle JV, Roberts LM, et al. Prevalence of subclinical thyroid dysfunction and its relation to socioeconomic deprivation in the elderly: a community-based cross-sectional survey. J Clin Endocr Metabolism. 2006;91(12):4809–4816. doi:10.1210/jc.2006-1557
9. Ruggeri RM, Trimarchi F, Biondi B. Management Of Endocrine Disease: l-Thyroxine replacement therapy in the frail elderly: a challenge in clinical practice. Eur J Endocrinol. 2017;177(4):R199–R217. doi:10.1530/EJE-17-0321
10. Floriani C, Gencer B, Collet TH, Rodondi N. Subclinical thyroid dysfunction and cardiovascular diseases: 2016 update. Eur Heart J. 2018;39(7):7.
11. Ochs N, Auer R, Bauer DC, et al. Meta-analysis: subclinical thyroid dysfunction and the risk for coronary heart disease and mortality. Ann Intern Med. 2008;148(11):832–845. doi:10.7326/0003-4819-148-11-200806030-00225
12. Walsh JP, Bremner AP, Bulsara MK, et al. Subclinical thyroid dysfunction as a risk factor for cardiovascular disease. Arch Intern Med. 2005;165(21):2467–2472. doi:10.1001/archinte.165.21.2467
13. Razvi S, Pearce SH. Subclinical hypothyroidism and cardiovascular disease-reply. Arch Intern Med. 2012;172(19):1523–1524. doi:10.1001/2013.jamainternmed.597
14. Rodondi N, den Elzen WP, Bauer DC, et al. Subclinical hypothyroidism and the risk of coronary heart disease and mortality. JAMA. 2010;304(12):1365–1374. doi:10.1001/jama.2010.1361
15. Jones DD, May KE, Geraci S. Subclinical thyroid disease. Lancet. 2012;123(6):502–504.
16. Razvi S, Weaver JU, Vanderpump MP, Pearce SHS. The incidence of ischemic heart disease and mortality in people with subclinical hypothyroidism: reanalysis of the whickham survey cohort. J Clin Endocr. 2010;95(4):1734–1740. doi:10.1210/jc.2009-1749
17. Misa I, Masazumi A, Shinichiro I, et al. Risk for ischemic heart disease and all-cause mortality in subclinical hypothyroidism. J Clin Endocrinol Metab. 2004;89(7):3365–3370.
18. Selmer C, Olesen JB, Hansen ML, et al. Subclinical and overt thyroid dysfunction and risk of all-cause mortality and cardiovascular events: a large population study. J Clin Endocr. 2014;99(7):2372–2382. doi:10.1210/jc.2013-4184
19. Gussekloo J. Thyroid status, disability and cognitive function, and survival in old age. J Am Med Assoc. 2005;292(21):2591–2599. doi:10.1001/jama.292.21.2591
20. Zhai XD, Zhang L, Chen LL, et al. An age-specific serum thyrotropin reference range for the diagnosis of thyroid diseases in older adults: a cross-sectional survey in China. Thyroid. 2018;28(12):1571–1579. doi:10.1089/thy.2017.0715
21. Brosius FC, Hostetter TH, Kelepouris E, et al. REPRINT Detection of chronic kidney disease in patients with or at increased risk of cardiovascular disease. Hypertension. 2006;48(4):751–755. doi:10.1161/CIRCULATIONAHA.106.177321
22. Juonala M, Magnussen CG, Berenson GS, Venn A. Childhood adiposity, adult adiposity, and cardiovascular risk factors. NEJM. 2011;365(20):1876. doi:10.1056/NEJMoa1010112
23. Wu YF, Zhao D, Zhou BF, et al. Cut offs and risk stratification of dyslipidemia in Chinese adults. Zhonghua Xin Xue Guan Bing Za Zhi. 2007;35(5):428.
24. Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the primary prevention of cardiovascular disease. J Am Coll Cardiol. 2019;74(10):e177–e232. doi:10.1016/j.jacc.2019.03.010
25. Roth GA, Huffman MD, Moran AE, et al. Global and regional patterns in cardiovascular mortality from 1990 to 2013. Circulation. 2015;132(17):1667. doi:10.1161/CIRCULATIONAHA.114.008720
26. Silva N, Santos O, Morais F, et al. Subclinical hypothyroidism represents an additional risk factor for coronary artery calcification, especially in subjects with intermediate and high cardiovascular risk scores. Eur J Endocrinol. 2014;171(3):327–334. doi:10.1530/EJE-14-0031
27. Stratigou T, Dalamaga M, Antonakos G, et al. Hyperirisinemia is independently associated with subclinical hypothyroidism: correlations with cardiometabolic biomarkers and risk factors. Endocrine. 2018;61(1):83–93. doi:10.1007/s12020-018-1550-3
28. Wu J, Tao Y, Gu H, Sui J. Association between cardiovascular risk factors and serum thyrotropin concentration among healthy Chinese subjects and subjects with unsuspected subclinical hypothyroidism. Clin Lab. 2016;62(5):807–814. doi:10.7754/Clin.Lab.2015.150809
29. Asvold BO, Bjøro T, Nilsen TI, Vatten LJ. Association between blood pressure and serum thyroid-stimulating hormone concentration within the reference range: a population-based study. J Clin Endocr Metabolism. 2007;92(3):841–845. doi:10.1210/jc.2006-2208
30. Bielecka-Dabrowa A, Godoy B, Suzuki T, Banach M, von Haehling S. Subclinical hypothyroidism and the development of heart failure: an overview of risk and effects on cardiac function. Clin Res Cardiol. 2019;108(3):225–233. doi:10.1007/s00392-018-1340-1
31. Klein I, Ojamaa K. Thyroid hormone and the cardiovascular system. N Engl J Med. 2001;344:257–268.
32. Haghi AR, Solhjoo M, Tavakoli MH. Correlation between subclinical hypothyroidism and dyslipidemia. Iran J Pathol. 2017;12(2):106–111.
33. Bensenor IM, Olmos RD, Lotufo PA. Hypothyroidism in the elderly: diagnosis and management. Clin Interv Aging. 2012;7:97–111. doi:10.2147/CIA.S23966
34. Pearce SH, Razvi S, Yadegarfar ME, et al. Serum thyroid function, mortality and disability in advanced old age: the Newcastle 85+ Study. J Clin Endocrinol Metab. 2016;101(11):4385–4394. doi:10.1210/jc.2016-1935
35. Singh S, Duggal J, Molnar J, Maldonado F, Barsano CP, Arora R. Impact of subclinical thyroid disorders on coronary heart disease, cardiovascular and all-cause mortality: a meta-analysis. Int J Cardiol. 2008;125(1):41–48. doi:10.1016/j.ijcard.2007.02.027
36. Vanderpump MP, Tunbridge WM, French JM, et al. The incidence of thyroid disorders in the community: a twenty-year follow-up of the Whickham Survey. Clin Endocrinol. 2010;43(1):55–68.
37. McQuade C, Skugor M, Brennan DM, Hoar B, Stevenson C, Hoogwerf BJ. Hypothyroidism and moderate subclinical hypothyroidism are associated with increased all-cause mortality independent of coronary heart disease risk factors: a PreCIS database study. Thyroid. 2011;21(8):837–843. doi:10.1089/thy.2010.0298
38. Moon S, Kim MJ, Yu JM, Yoo HJ, Park YJ. Subclinical hypothyroidism and the risk of cardiovascular disease and all-cause mortality: a meta-analysis of prospective cohort studies. Thyroid. 2018;28(9):1101–1110. doi:10.1089/thy.2017.0414
39. Yang L-B, Jiang D-Q, Qi W-B, et al. Subclinical hyperthyroidism and the risk of cardiovascular events and all-cause mortality: an updated meta-analysis of cohort studies. Eur J Endocrinol. 2012;167(1):75–84. doi:10.1530/EJE-12-0015
40. Silva JE. Thyroid-adrenergic interactions: physiological and clinical implications. Thyroid. 2008;18(2):157–165.
41. Surks MI, Hollowell JG. Age-specific distribution of serum thyrotropin and antithyroid antibodies in the U.S. population: implications for the prevalence of subclinical hypothyroidism. J Clin Endocrinol Metab. 2007;92(12):4575–4582. doi:10.1210/jc.2007-1499
42. Somwaru LL, Rariy CM, Arnold AM, Cappola AR. The natural history of subclinical hypothyroidism in the elderly: the cardiovascular health study. J Clin Endocr. 2012;97(6):1962–1969. doi:10.1210/jc.2011-3047
43. Lindeman RD, Romero LJ, Schade DS, Wayne S, Baumgartner RN, Garry P. Impact of subclinical hypothyroidism on serum total homocysteine concentrations, the prevalence of coronary heart disease (CHD), and CHD risk factors in the new mexico elder health survey. Thyroid. 2003;13(6):595–600. doi:10.1089/105072503322238863
44. Svold BO, Bjro T, Platou C, Vatten L. Thyroid function and the risk of coronary heart disease: 12‐year follow‐up of the HUNT Study in Norway. Clin Endocrinol. 2012;77:6.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.