")
Back to Journals » Psychology Research and Behavior Management » Volume 15
Association of Driving Fitness and Driving Efficacy in the Elderly with Generalized Anxiety Disorder
Authors Park MO
Received 7 June 2022
Accepted for publication 31 August 2022
Published 16 September 2022 Volume 2022:15 Pages 2649—2658
DOI https://doi.org/10.2147/PRBM.S376990
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Myoung-Ok Park
Department of Occupational Therapy, Division of Health Science, Baekseok University, Cheonan-si, Chungcheongnam-do, Republic of Korea
Correspondence: Myoung-Ok Park, Department of Occupational Therapy, Division of Health Science, Baekseok University, 1, Baekseokdaehak-ro, Dongnam-gu, Cheonan-si, Chungcheongnam-do, Republic of Korea, Tel +82-10-9999-8636, Fax +82– 41-550-2185, Email [email protected]
Purpose: The purpose of this study was to investigate the relationship between driving fitness and driving efficacy in elderly patients with generalized anxiety disorder and identify factors influencing anxiety.
Methods: The anxiety level, driving efficacy, and driving performance were assessed for 45 elderly drivers who had been diagnosed with or were suspected of having an anxiety disorder in the past. The Korean-Self-rating Anxiety Scale (K-SAS), Korean-Adelaide Driving Self-Efficacy Scale (K-ADSES), and Korean-Drivers 65 Plus (K-D65+) were used as test tools. Factors affecting anxiety and the differences between the groups with high anxiety symptoms and anxiety in the normal range were analyzed.
Results: There were differences in driving efficiency and driving performance between elderly drivers with anxiety scores in the normal range and those with mild-to-moderate anxiety (p < 0.05). Significant factors (p < 0.001) influencing driving anxiety in the high anxiety group were GAD duration (β = 0.170), driving difficulty (β = 10.648), drug use (β = 0.656), traffic sign/signal awareness (β = − 0.870).
Conclusion: Our results suggest that a combination of a driving rehabilitation approach and interventions that can provide emotional support and reduce mental health anxiety, as well as exposure treatment for driving performance training, may be necessary for driving rehabilitation of the elderly with generalized anxiety disorder.
Keywords: generalized anxiety disorder, elderly, driving-fitness, driving efficacy
Introduction
The ageing of society is linked to several problems worldwide. In the United States, where the percentage of elderly people aged 60 years or over is higher than that of Korea, the number of elderly drivers with driver’s licenses reached 41,700,000 in 2016, a 34% increase from 2007.1 Generalized anxiety disorder (GAD) in the elderly is the most common anxiety disorder, with a high prevalence of 7.3% in the community.2 The prevalence of GAD was found to be 11.2% in a sample of elderly primary care patients.3 GAD is a chronic disorder with no chance of remission. Elderly individuals with GAD have a high occurrence of comorbidities consisting of other mental and physical diseases.4 Depression disorders, cognitive disorders, and drug or alcohol use disorders are common psychiatric comorbidities. Physical disorders include cardiovascular diseases such as angina pectoris and arrhythmia, chronic obstructive pulmonary disease, respiratory diseases such as pneumonia, endocrine system diseases such as diabetes, nervous system diseases such as convulsive diseases, other gastric ulcers, and urinary tract infections.5 Moreover, patients with GAD complain of somatic symptoms of anxiety with widespread patterns and symptoms that can appear in various organs and tend to become chronic.6 Anxiety disorders are secondary to depression when depression and GAD occur together.7 Further, as geriatric GAD is highly related to depression, antidepressants are preferred for its treatment.8
Various factors affect anxiety, including vulnerability in emotional management, which lowers self-esteem and creates difficulties in participation in activities.9 Self-efficacy and individual driving fitness in driving performance are factors that must be understood to drive safely. In the case of adult drivers with anxiety disorder, it was reported that the higher the anxiety symptoms, the higher the error, negligence in safe driving behavior, general violation of traffic laws and the higher the rate of aggressive violation.10 In addition, according to a previous study, the biological evidence that mental fatigue could be the cause of serious traffic accidents was presented. Mental fatigue was measured by measuring brain waves during driving for normal people. As a result, there was a clear difference between the alpha wave representing stability and the beta wave representing anxiety. This means increased anxiety when driving.11
According to previous studies, elderly people drive to perform housework, go to grocery stores, go to hospitals, and their driving habits are different from those of young drivers.12 Elderly drivers have shorter driving distances than younger drivers and complain of difficulties in driving, such as long-distance trips.13 In particular, elderly drivers have a habit of avoiding driving at night and on heavily congested roads and have difficulty turning left at an intersection with no left-turn signal, driving in rain or fog, and driving at sunrise and sunset.14 In addition, the elderly with visual and cognitive impairments had a greater risk of accidents, and elderly drivers with dementia, such as Alzheimer’s disease, had more difficulty driving.15 Another previous study investigated the relationship between symptoms of internalized emotional distress and self-reported aberrant driving behavior. As a result, it was reported that the higher the emotional distress composite index of the elderly, the higher the possibility of showing a greater aberrant driving behavior. The categories of emotional distress included factor elements of anxiety, suicidal thoughts, and temper.16 Elderly drivers with GAD in psychiatric disorders show difficulties in driving performance due to loss of function due to emotional anxiety symptoms.17 In this study, the driving fitness and driving efficacy of the elderly with GAD were explored to identify factors that should be considered for safe driving by the elderly with GAD.
Materials and Methods
Participants
45 elderly drivers with GAD in Seoul and Gyeonggi provinces were selected to participate in this study. The general criteria for the participants were that they were elderly drivers with more than one year of driving experience. The selection of candidates was via community organizations where many elderly drivers can meet. For the recruitment of study participants, an official letter was sent to the occupational therapy team leader working at community health centers, mental health centers, and welfare centers to ask for cooperation in the selection of study participants. A total of 5 institutions were selected. The target group evaluated the elderly who were over 60 years of age and who had been diagnosed with GAD by specialists in psychiatry and family medicine, who were driving, had stopped driving, or wanted to resume. The evaluation of the contact targets was conducted by five occupational therapists working at the institution and the research director. In addition, the research director trained eight evaluators on the purpose of this study, the purpose of evaluation, and the evaluation method at the time of the survey and conducted pre-education so that there were no errors between evaluators. Due to COVID-19, the interview was conducted over the phone and Face Talk SNS. In addition, research tools for questions about driving efficacy and performance were distributed online to collect information. Participants who consented to the study in the pre-telephone interview were given consent again by e-mail online and consent was obtained.
Forty-five copies of the general information and questionnaire-type evaluation used in the study were initially distributed by email. In the subject selection process, 60 elderly drivers were connected, but 12 people who did not meet the recruitment criteria and 3 people who refused to participate in the study were excluded and distributed.
This study was approved by the research ethics committee of Baekseok University (BUIRB-202202-HR-041), and the participants were briefed about the purpose and methods, procedure, and ethical issues based on the Declaration of Helsinki.
Measurements
Korean-Self-Rating Anxiety Scale (K-SAS)
The Korean self-assessment anxiety scale (K-SAS) developed by Lee was used to assess the anxiety of the elderly subjects.18 The scales were “I’m more nervous and anxious these days than before (anxiousness)”, “I’m outright afraid (fear)”, “I am embarrassed and helpless over trifles (panic)”, “I have weakened nerves and cannot control my mind (mental disintegration)”, “Everything will be fine (apprehension)”, “My hands and feet are trembling and restless (tremor)”, “I have a headache, my neck is heavy, or my back hurts (body aches and pains)”, “I am weak and tired for no reason (fatigue)”, “My mind is stable and I can sit comfortably for a long time (restlessness)”, “My chest hurts”, “I’m pounding (palpitation)”, “I’m having a hard time because I’m dizzy (dizziness)”, “I feel like fainting or fainting (faintness)”, “There are times when I feel this”, “I don’t feel stuffy (dyspnea)”, “I suffer from cramps or numbness in my hands (paresthesia)”, “I have trouble with digestion (indigestion)”, “I urinate often (urinary frequency)”, “My hands are usually hot and sweaty (sweating)”, “My face turns red easily and gets hot (face flushing)”, “I fall asleep easily and sleep deeply (insomnia)”, and “I have frightening dreams (nightmares).” The responses were assessed using a Likert 4-point scale, from 1 (never) to 4 (always), ranging from 20 to 80 and including 5 inverse questions, with higher scores indicating higher levels of anxiety. Generally, 20‒44 is considered the normal range; 45‒59 indicates a mild-to-moderate anxiety level; 60‒74 a severe anxiety level; over 75 an extreme anxiety level. The maximum score is 80. Test–retest reliability was observed with r = 0.98 and internal consistency r = 0.96.18
Korean-Adelaide Driving Self-Efficacy Scale (K-ADSES)
ADSES is a measurement tool of self-efficacy for elderly drivers developed by George et al in 2007.19 It consists of 12 topics which one encounters on a daily basis while driving such as “driving in your local area” and “driving in heavy traffic.” The response for each item is based on a 10-point scale, ranging from 0 (not confident) to 10 (completely confident). According to a study by George et al19 the internal consistency of this assessment was 0.98, indicating high reliability. K-ADSES determines the driving efficacy of older drivers and was standardized in the Korean version in 2019 by Park et al. K-ADSES’s Cronbach’s α value for the entire item was 0.975. The test–retest reliability of K-ADSES indicated a significant correlation with an Internal Classification Coefficient (ICC) of 0.813.20
Korean-Drivers 65 Plus (K-D65+)
K-Drivers 65 Plus is a self-reporting-type evaluation tool that determines the driving fitness of older drivers and was standardized in the Korean version in 2018.21 It includes a total of 15 questions, including “I have many thoughts when I’m driving”, “If I’m really angry, it affects my driving”, and “I have regular visual examinations to maintain my best eyesight”, with responses on three scales: “I often do”, “I sometimes do”, and “I don’t.” Questions 14 and 15 are structured to respond on three scales: Never, One to two times, Three times and more. It includes self-driving evaluation items consisting of 15 items, and responses to items are on a 3-point scale ranging from “often” to “not at all” from items 1 to 13, and questions 14 and 15 are ‘It is on a 3-point scale ranging from “never” to ‘more than 3 times’.
The subject counts the number of “triangle” and “square”, weights them with “x3” and “x5”, respectively, and then checks the summed score. The score of the evaluation tool ranges from 0 to 75, and if it is 15 or less, it is judged that there is quality as safe driving, and if it is 16 to 34, it is judged that driving is due to a lack of qualifications as a safe driver. A score of 35 or higher is recommended not to drive for safety.
The internal consistency of K-Drivers 65 plus was as low as 0.575, but the retest reliability (internal classification coefficient, ICC) showed a significant correlation with 0.95.
Study Procedure
First, the research director provided a detailed explanation of the study and obtained consent to participate in the study from the study subjects selected by the occupational therapists at each institution. The explanations and consent to participate in the study were given over the phone and on the internet due to COVID-19. In addition, the study description and evaluation documents were distributed via email so that the examination could be conducted by the institution’s occupational therapist.
Statistical Analysis
The general characteristics of the study participants were subjected to descriptive statistics and frequency analysis. The difference between driving fitness and driving efficacy by anxiety level was investigated through the t-test. The relationship between participants’ anxiety, driving fitness, and driving efficacy was analyzed through Spearman correlation analysis. Stepwise multiple regression analysis was conducted by selecting the factors affecting the anxiety level as independent variables such as the participants’ general characteristics, driving fitness, and driving efficacy. All statistical analyses used SPSS 20.0 ver., with a significance level at α=0.05.
Results
General Characteristics of Participants
The average age of all participants in the study was 65.89 years; there were 37 men (82.2%) and 8 women (17.8%); and 37 (82.2%) participants were employed. Regarding their academic records, 16 (36.6%) participants were high school graduates, 14 (31.1%) were university graduates, and 10 (22.2%) middle school graduates and the other five participants (11%) had an unspecified educational level. The average driving experience of all the study participants was 30.11 years; 29 (64.4%) participants had a class 1 driver’s license; 5 (11.1%) participants had a class 2 driver’s license; 11 (24.4%) had a heavy vehicle driver’s license; 74 (64.9%) people drove sedans. When asked, 44 (97.8%) participants confirmed that they found it difficult to drive. One (2.2%) respondent had a traffic accident, while 5 (11.1%) respondents almost had a traffic accident within the past six months. The average duration of generalized anxiety disorder of the participants was 16.20 months (Table 1).
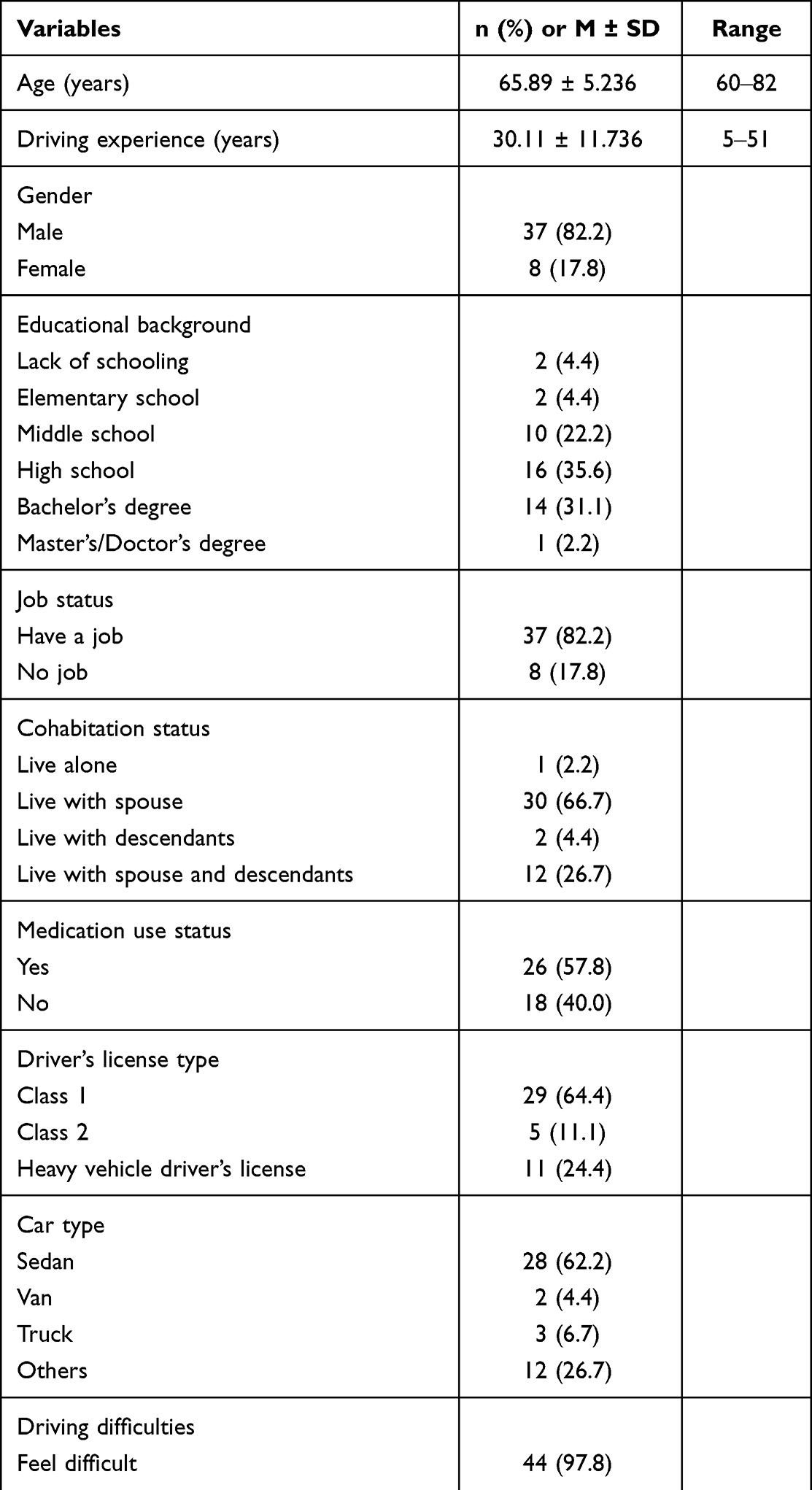 |
Table 1 General Characteristics of Participants (N = 45) |
Description About Generalized Anxiety Levels, Driving Efficacy, and Driving Habits of Participants
To find out the mean and distribution of K-SAS, K-ADSES, and K-D 65+ of all participants, a t-test was performed. The average anxiety score of the elderly drivers who participated in the study was 46.46 points out of 80 points. When the anxiety test was performed again at the beginning of this study, 17 patients (37.8%) were found to have anxiety in the normal range, and the remaining had mild-to-moderate anxiety. The elderly were 28 (62.2%). The driving efficacy of all participants was evaluated as a K-ADSES score of 116.31 ± 17.39 and the driving habits as a K-Driver 65 plus score of 19.76 ± 12.38 (Table 2).
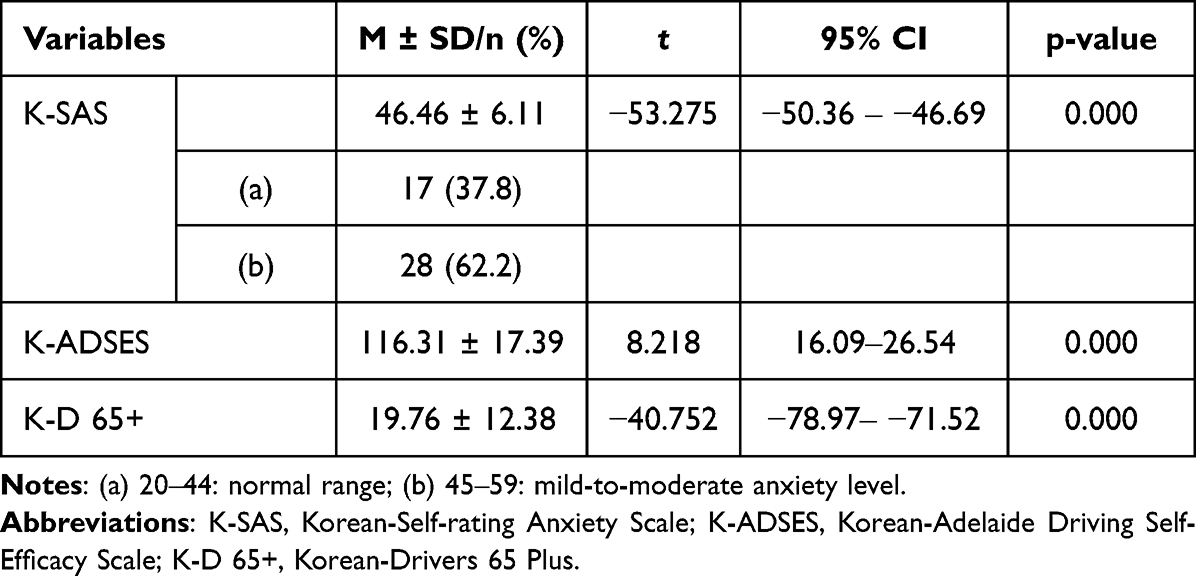 |
Table 2 Description About Anxiety Levels, Driving Efficacy, and Driving Habits of Participants (N = 45) |
Comparison of Driving Efficacy and Driving Habits by Anxiety Levels
The K-ADSES and K-Driver 65 plus scores were compared according to the anxiety level of the elderly participants in this study. The K-ADSES scores were 40.00 ± 2.06 in the normal range group and 50.39 ± 3.92 in the mild-to-moderate anxiety group, indicating a significant difference between the two groups (p = 0.000). The K-Driver 65 plus scores were 24.88 ± 13.72 in the normal anxiety group and 16.64 ± 10.57 in the mild-to-moderate anxiety group, showing a significant difference between the two groups (p = 0.000). That is, drivers with high anxiety showed low self-efficacy and driving fitness. Also, both driving efficacy and fitness significantly differed as a function of anxiety levels (Table 3).
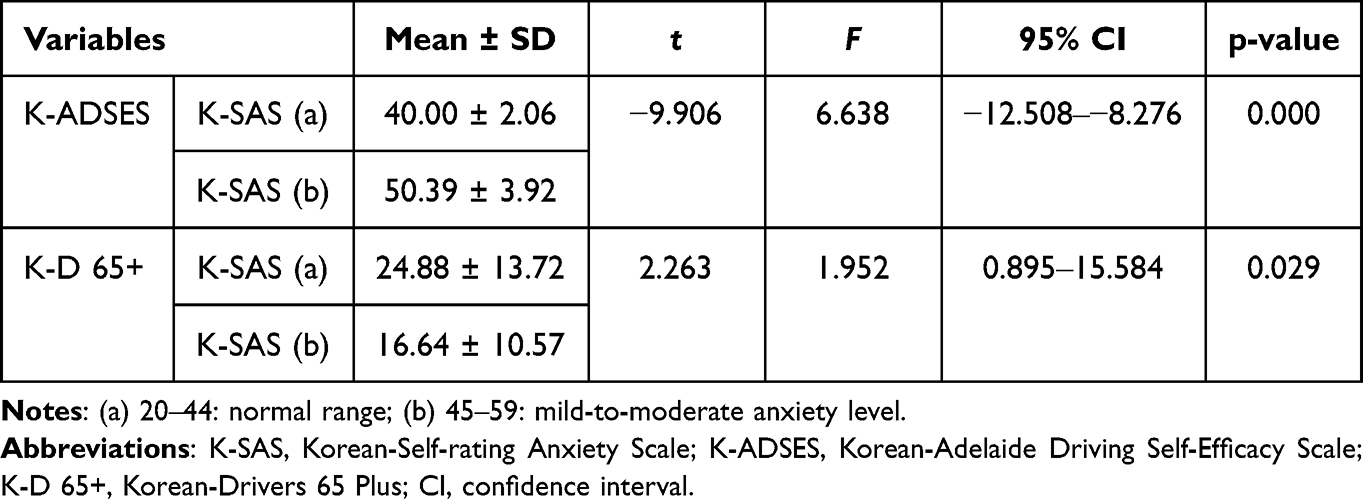 |
Table 3 Anxiety Levels, Driving Efficacy, and Driving Fitness Among Participants with Normal and Mild-to-Moderate Anxiety Levels (N = 45) |
Spearman Correlation Between Driving Efficacy and Driving Habits Among Participants with Different Anxiety Levels
Analyzing the Spearman correlation between the total scores of K-ADSES and K-Driver 65 plus according to the anxiety levels of the participants revealed a linear correlation between the total K-Driver 65 plus score and the total K-SAS score in the mild-to-moderate anxiety group (r = 0.424, p = 0.028). In other words, anxiety and driving suitability were strongly related to participants with mild or moderate anxiety (Table 4).
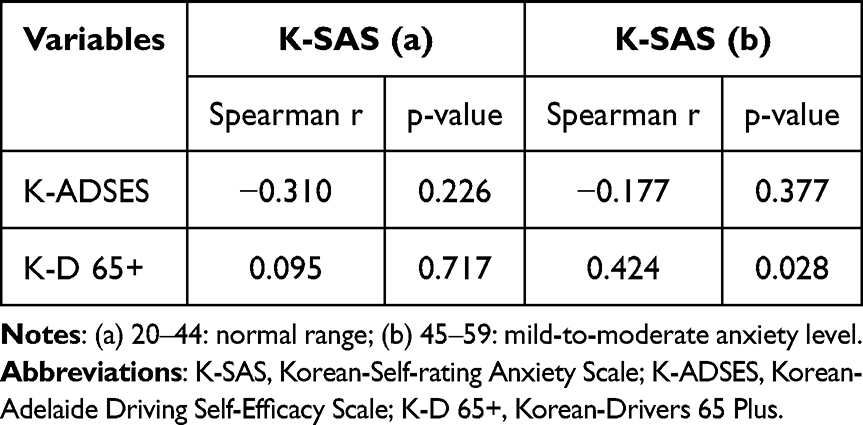 |
Table 4 Spearman Correlation Between Driving Efficacy and Driving Habits for Participants with Different Anxiety Levels (N = 45) |
Stepwise Multiple Regression to Identify Factors Affecting Anxiety
Factors affecting the total K-SAS score for anxiety were analyzed through stepwise multiple regression analysis. The dependent variable was the total K-SAS score; the independent variables were the general characteristics; the sub-items and total K-ADSES and K-Driver 65 plus scores were selected as variables for analysis. In the group whose total anxiety score was in the normal range, the following were found to be significantly influencing factors: GAD duration (β = 0.102, p = 0.009), seat belt wearing (β =−0.522, p = 0.017), and highway driving (β = −0.408, 0.043) affected the group were factors. The explanatory power of this model was adjusted R2=0.681 (p = 0.003).
In the group whose total anxiety score was in the mild-to-moderate range, the following were found to be significantly influencing factors: GAD duration (β = 0.170, p = 0.000), driving difficult (β = 10.648, p = 0.000), medication use (β = 0.656, p = 0.0002) and traffic sign/signal awareness (β = −0.870, p = 0.013). The explanatory power of this model was very reliable with the corrected R2=0.793 (p = 0.000) (Tables 5 and 6).
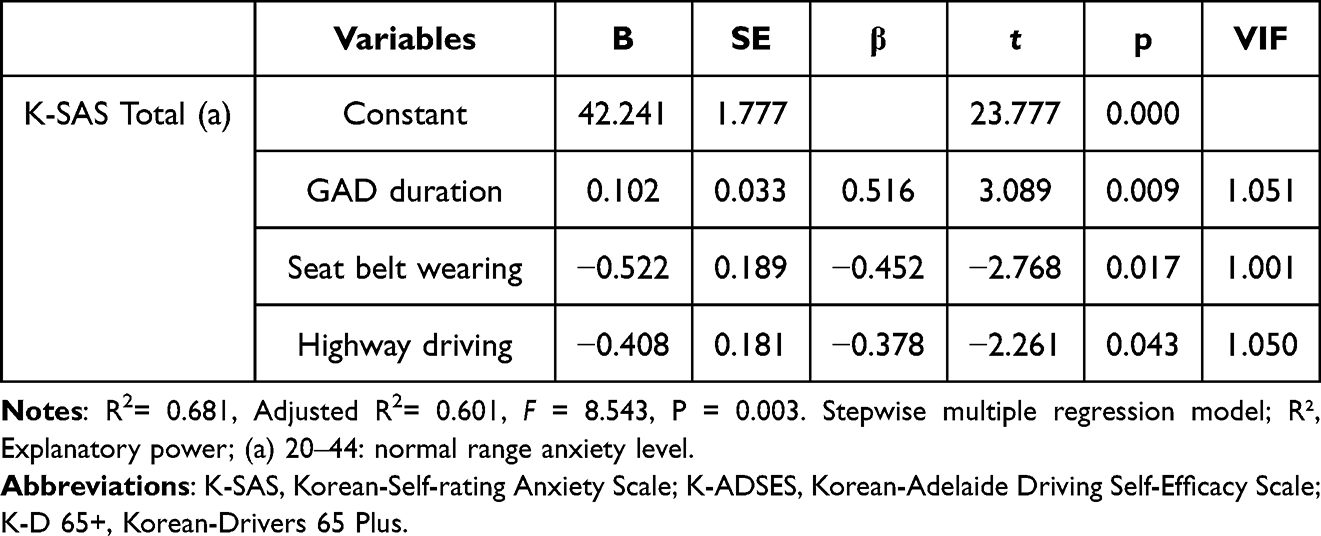 |
Table 5 Identification of Factors Affecting Anxiety Using Stepwise Multiple Regression Analysis in Participants with Normal Anxiety Level (N = 17) |
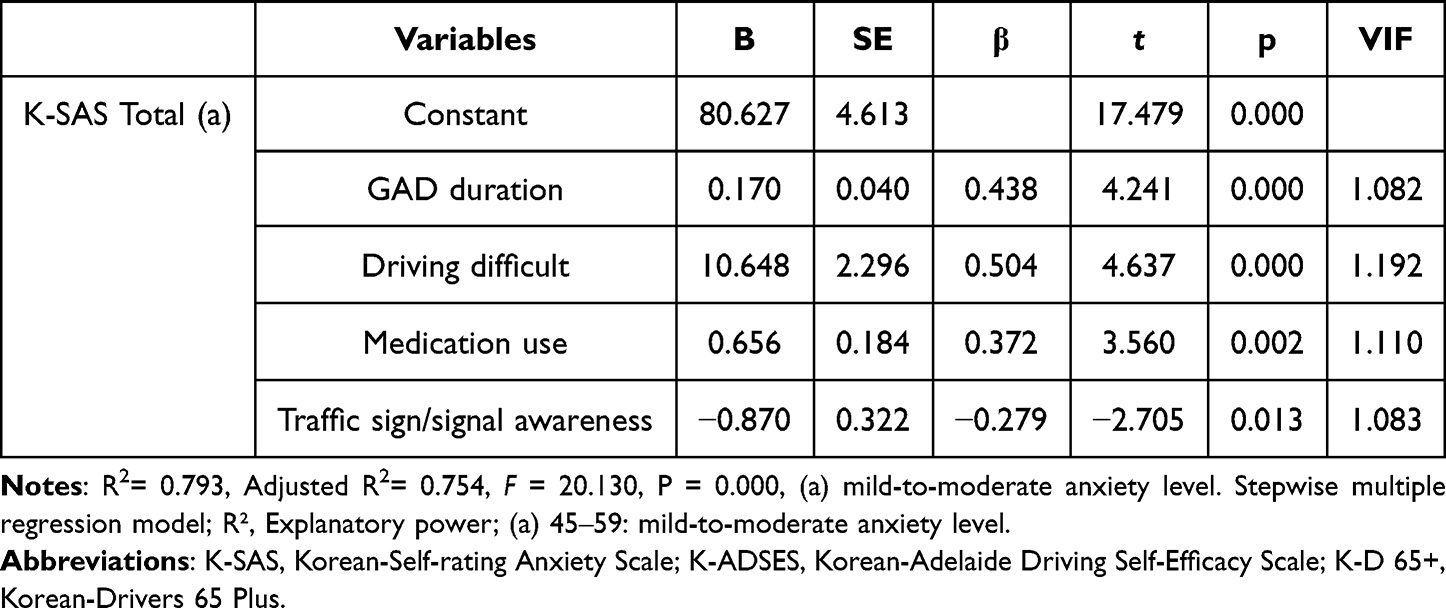 |
Table 6 Identification of Factors Affecting Anxiety Using Stepwise Multiple Regression Analysis in Participants with Mild-to-Moderate Anxiety Levels (N = 28) |
Discussion
Deterioration of motor function and the ability to process visual, perceptual, and cognitive information due to aging are factors that make it difficult for older drivers to drive safely.22 These changes in physical, cognitive, and mental functions can also lead to reduced confidence and self-efficacy in driving in older drivers.23
Difficulties in driving performance due to normal aging appear in normal elderly individuals.24 However, elderly people with GAD may have more difficulties in driving due to emotional anxiety and accompanying physical symptoms.25 The elderly participants in this study were those who had been suspected or diagnosed with anxiety disorder symptoms by a psychiatrist. Their current level of anxiety was examined through the K-SAS test at the beginning of this study. The results revealed that 62.2% of the elderly participants had mild-to-moderate anxiety levels higher than normal. An examination of the difference in K-ADSES scores between the groups with normal anxiety levels and mild-to-moderate anxiety showed a significant difference in the average K-SAS scores: it was approximately 10 points higher in the group with the higher anxiety levels.
The higher the total K-ADSES score, the lower is the sense of efficacy for driving performance.20 Thus, the differences between the two groups indicate that the driving efficacy of the group with higher anxiety decreased during self-driving, making it difficult for these participants to drive safely. According to a previous study conducted in New Zealand, 1170 elderly drivers over 65 years of age were surveyed to determine whether they had any fear of driving. Of all participants, 62.3% reported no driving anxiety; 27.0% reported mild anxiety; and 10.7% reported having moderate-to-maximum levels of driving anxiety.26 The New Zealand study was conducted on general elderly drivers; however, this study was conducted on elderly participants who were previously diagnosed with GAD by a psychiatrist or family medicine doctor or received warnings or instructions about the possibility of GAD. Our results showed a relationship between anxiety symptoms and driving performance when the feeling of driving efficacy decreased in the group complaining of mild-to-moderate anxiety, as evaluated by the total K-SAS scores. An examination of driving fitness based on the K-Driver 65 plus scores revealed that the anxiety score was ~24 points in the normal anxiety-level group and ~16 points in the group with mild-to-moderate anxiety. The t score was high because of the driving fitness test.
The higher the total K-Driver 65 plus score, the more suitable is the driving performance.21 Based on this interpretation, the group with mild-to-moderate anxiety showed a lower driving fitness than the normal anxiety range group. According to a study published in 2008 on the driving performance of 208 people with mental health illness, only 33 obtained a driver’s license, and the remaining 84% failed the driving test.27 Previous studies suggesting that driving fitness decreases when there is a problem with mental function support the results of this study. Analysis of the relationship between each group’s driving efficacy and fitness and the total anxiety score revealed a stronger correlation between the average K-Driver 65 plus score and the K-SAS score in the group with mild-to-moderate anxiety than in the normal anxiety-level group.
A previous study examining the degree of accident severity and stress for anxious drivers reported that the higher the stress history for various situations in life, the more vulnerable was the driving behavior.28 This finding also suggests that anxiety is related to the driving fitness of elderly drivers. The factors affecting the total anxiety score in each group were identified through stepwise multiple regression analysis. In the case of the normal anxiety-level group, the longer the GAD duration, the more not wearing a belt seat, and the more difficult it was to drive at high speed had an effect on overall anxiety. The reliability of this model was 68%, indicating moderate reliability.
For the mild-to-moderate anxiety group, more factors appeared to influence the total anxiety score. In particular, the longer the GAD duration and the longer the drug administration period, the higher the anxiety. On the other hand, it was found that the more difficulties they had in driving, the more anxious they felt, and the less they recognized traffic signs and signals, the more anxious they felt. These factors showed a high reliability at 79%.
In both the case where the anxiety index falls into the normal category and the group with a relatively high anxiety index, the GAD period was a factor influencing the overall anxiety score. In the case of elderly drivers whose anxiety index is in the normal range, the difficulty of driving without a seat belt or driving on the highway served as a factor that made them feel more anxious. On the other hand, psychological factors such as difficulty in self-driving during the GAD as well as groups with higher overall anxiety index than the middle were included.
It is known that the more drugs you take, the greater the anxiety, so it is intended to relieve anxiety symptoms through medication, but anxiety is relatively high as much as the dose. In addition, in this group, the fewer traffic signals and signal recognition, the higher the anxiety score, which is estimated to be due to the shorter concentration on the signal and the lower the level of cognitive information processing.
In summary, the group with a high anxiety score frequently took drugs, and the greater the anxiety, the lower the self-sensing driving efficacy. Similarly, previous studies have reported that stress from uncertain situations commonly experienced in modern society, such as fear, helplessness, risk and uncontrollable situations, poses a risk to driver behavior of all ages.29
A study by Dula et al30 reported that the higher the overall anxiety level, the more dangerous was the driving behavior in 1121 normal adults. Regardless of the sex difference, it was reported that the higher the anxiety level, the more risky was the driving performance, with the more anxious group causing significantly more accidental collisions than the group with the medium or low anxiety levels. Another study investigated the relationship between driving behavior and anxiety characteristics and reported that aggressive behavioral characteristics were related to signal violation. A negative correlation between driving error and age was reported by one study.31 Based on these findings, it could be inferred that the more anxious the elderly driver, the lower the driving performance and the higher the accident risk. This evidence highlights the importance of driving rehabilitation training combined with mental health interventions to reduce physical and emotional anxiety and increase the understanding of driving situations for the elderly with GAD.
This study has limitations such as the difficulties encountered in face-to-face evaluation because of restrictions due to the COVID-19 pandemic and the small number of study participants due to selective subject selection. Further investigation is required to determine the feasibility of assessing driving performance based on anxiety scores for a greater number of elderly people with anxiety disorders. In this study, only the GAD level of the elderly was considered. Since the cognitive level of the elderly can affect depression and driving, it is necessary to investigate the effect of cognitive level, depression level, and driving in future studies.
Finally, this study highlights the importance of virtual reality-based driving exposure therapy performed in the existing driving rehabilitation domain in addition to intervention techniques to improve mental health functions to reduce the anxiety of elderly drivers with GAD.
Conclusion
In summary, this study has a very important meaning in that it identifies factors affecting the driving performance of the elderly with general anxiety disorder and explores the difference between driving suitability and driving efficacy according to anxiety levels. This study showed that the driving efficacy and driving suitability of GAD elderly differed according to the anxiety index. In particular, in the case of GAD elderly with moderate-to-high anxiety, the sense of efficacy for driving was further reduced and the suitability of basic driving performance such as traffic sign recognition and signal recognition was lowered. This study will serve as a basis for consideration when supporting driving rehabilitation for elderly drivers with GAD in the clinic.
Ethics Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Baekseok University (BUIRB-202202-HR-041). All participants agreed on the consent form before participating in the study.
Acknowledgments
The author would like to thank the elderly and caregivers who participated in the study. This study was supported by Baekseok University research fund in 2022.
Disclosure
The author declares no conflicts of interest in this work.
References
1. National Highway Traffic Safety Administration. Traffic Safety Facts: 2016 Data: Older Population. Washington (DC): NHTSA; 2018.
2. Wittchen HU. Generalized anxiety disorder: prevalence, burden, and cost to society. Depress Anxiety. 2002;16:
3. Haller H, Cramer H, Lauche R, et al. The prevalence and burden of subthreshold generalized anxiety disorder: a systematic review. BMC Psychiatry. 2014;14:128. doi:10.1186/1471-244X-14-128
4. Flint AJ. Generalised anxiety disorder in elderly patients. Drugs Aging. 2005;22:
5. Alwahhabi F. Anxiety symptoms and generalized anxiety disorder in the elderly: a review. Harv Rev Psychiatry. 2003;11:
6. Blazer DG. Generalized anxiety disorder and panic disorder in the elderly: a review. Harv Rev Psychiatry. 1997;5:
7. Kendler KS, Neale MC, Kessler RC, et al. Major depression and generalized anxiety disorder: same genes, (partly) different environments? Arch. Gen Psychiatry. 1992;49:
8. Zhang X, Norton J, Carrière I, et al. Generalized anxiety in community-dwelling elderly: prevalence and clinical characteristics. J Affect Disord. 2015;172:
9. Cisler JM, Olatunji BO, Feldner MT, et al. Emotion regulation and the anxiety disorders: an integrative review. J Psychopathol Behav Assess. 2010;32:
10. Shahar A. Self-reported driving behaviors as a function of trait anxiety. Accid Anal Prev. 2009;41:241–245. doi:10.1016/j.aap.2008.11.004
11. Zhao C, Zhao M, Liu J, et al. Electroencephalogram and electrocardiograph assessment of mental fatigue in a driving simulator. Accid Anal Prev. 2012;45:83–90. doi:10.1016/j.aap.2011.11.019
12. Morisset N, Terrade F, Somat A. Perceived self-efficacy and risky driving behaviors. Swiss J Psychol. 2010;69:
13. Fernandez C, Mirman JH, Stavrinos D. Comparing the Factor Structure of the Driving Habits Questionnaire Be-Tween Different Age Groups. Transportation Research Board 97th Annual Meeting; 2018: 5333.
14. Gruber N, Mosimann UP, Müri RM, et al. Vision and night driving abilities of elderly drivers. Traffic Inj Prev. 2013;14:
15. Nakano Y, Kojima T, Kawanaka H, et al. Study of improving the cognitive ability of elderly drivers. In: 16th International IEEE Conference on Intelligent Transportation Systems. 2013:
16. Bernstein JP, DeVito A, Calamia M. Associations between emotional symptoms and self-reported aberrant driving behaviors in older adults. Accid Anal Prev. 2019;127:28–34. doi:10.1016/j.aap.2019.02.024
17. Silverstone T. The influence of psychiatric disease and its treatment on driving performance. Int Clin Psychopharmacol. 1988;3(Suppl 1):
18. Lee JH. Development of the Korean form of Zung’s self-rating anxiety scale. Yeungnam Univ J Med. 1996;13:
19. George S, Clark M, Crotty M. Development of the Adelaide driving self-efficacy scale. Clin Rehabil. 2007;21:
20. Park MO, Kim MJ. Psychometric characteristics for clinical application of Korean version of Adelaide driving self efficacy scale. Korean J Occup Ther. 2019;27:
21. Han SW, Lee JS, Kim SK, et al. The Standardization of the Korean Drivers 65 plus to identify driving fitness of senior drivers. Korean J Occup Ther. 2018;26:
22. Akinwuntan AE, Feys H, DeWeerdt W, et al. Prediction of driving after stroke: a prospective study. Neurorehabil Neural Repair. 2006;20:417–423. doi:10.1177/1545968306287157
23. Ragland DR, Satariano WA, MacLeod KE. Driving cessation and increased depressive symptoms. J Gerontol a Biol Sci Med Sci. 2005;60:
24. Ball K, Rebok G. Evaluating the driving ability of older adults. J Appl Gerontol. 1994;13:
25. Leblanc MF, Desjardins S, Desgagné A. Sleep problems in anxious and depressive older adults. Psychol Res Behav Manag. 2015;8:
26. Taylor JE, Connolly MJ, Brookland R, et al. Understanding driving anxiety in older adults. Maturitas. 2018;118:
27. De Las Cuevas C, Ramallo Y, Sanz EJ. Psychomotor performance and fitness to drive: the influence of psychiatric disease and its pharmacological treatment. Psychiatry Res. 2010;176:236–241. doi:10.1016/j.psychres.2009.02.013
28. Clapp JD, Olsen SA, Danoff-Burg S, et al. Factors contributing to anxious driving behavior: the role of stress history and accident severity. J Anxiety Disord. 2011;25:592–598. doi:10.1016/j.janxdis.2011.01.008
29. Gwyther H, Holland C. The effect of age, gender and attitudes on self-regulation in driving. Accid Anal Prev. 2012;45:19–28. doi:10.1016/j.aap.2011.11.022
30. Dula CS, Adams CL, Miesner MT, et al. Examining relationships between anxiety and dangerous driving. Accid Anal Prev. 2010;42:2050–2056. doi:10.1016/j.aap.2010.06.016
31. Pourabdian S, Azmoon H. The relationship between trait anxiety and driving behavior with regard to self-reported Iranian accident involving drivers. Int J Prev Med. 2013;4:1115–1121.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.