")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Association of Depression with Metabolic Syndrome in Highly Educated Ethnic Koreans of China: A Case–Control Study
Authors Wen Y, Liu G, Shang Y, Wang Q
Received 6 September 2020
Accepted for publication 30 November 2020
Published 8 January 2021 Volume 2021:17 Pages 57—66
DOI https://doi.org/10.2147/NDT.S280716
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Yan Wen,1 Guohui Liu,2 Yawen Shang,1 Qing Wang1
1Department of Endocrinology, China-Japan Union Hospital of Jilin University, Changchun, Jilin 130033, People’s Republic of China; 2Department of Cardiovascular, China-Japan Union Hospital of Jilin University, Changchun, Jilin 130033, People’s Republic of China
Correspondence: Qing Wang
Department of Endocrinology, China-Japan Union Hospital of Jilin University, 126 Xian-tai Street, Changchun, Jilin 130033, People’s Republic of China
Tel/Fax +86-13504310592
Email [email protected]
Background: Ethnic Koreans in China are a distinct minority group. Highly educated populations are at high risk of depression. The aim of this study was to explore the associations of depression and metabolic syndrome (MS) in highly educated ethnic Koreans in China, and determine whether the associations were dependent on gender.
Methods: From March 11th to 27th 2017, the natural population of 18– 70 year olds was continuously screened at Yanbian Korean Autonomous Region. Those who met the inclusion criteria were invited to complete Zung Self-Rating Depression Scale (SDS). The people with SDS > 53 were assigned to depression group and those with SDS ≤ 53 were assigned to the control group. Demographic characteristics, clinical factors, life-style factors and family history were collected and compared. Besides, associations of depression with MS and its components were estimated by Spearman correlation analysis and logistic regression analysis.
Results: The depression group included 367 highly educated ethnic Koreans with depression status and the control group consisted of 388 age-, education-, and gender-matched ethnic Koreans without depression. A significantly higher prevalence of MS was observed in males and females with depression status relative to the control subjects (males, 28.5% vs 6.3%, X2 = 16.162, P-value < 0.001; females, 33.0% vs 7.5%, X2 = 57.896, P-value < 0.001). Depression status was positively correlated with MS in males (r = 0.311, P-value < 0.01) and females (r = 0.332, P-value < 0.01). After adjusting for potential confounding factors, mild and moderate depression statuses were found to be significantly associated with MS development in male and female ethnic Koreans, respectively.
Conclusion: Our findings suggest a close link between depression and MS independent of gender in highly educated ethnic Koreans of China.
Keywords: depression, metabolic syndrome, ethnic Koreans, self-rating scale for depression, waist circumference
Background
Metabolic syndrome (MS) is defined as a combination of central obesity, hyperglycemia, and hypertension.1 This pathologic condition has become a global health hazard attributed largely to increased consumption of high calorie low fiber fast food and decreased physical activity, causing a heavy burden on the modern world.2,3 Convincing evidence shows that an increased risk of MS is present in patients with a range of psychiatric disorders, such as depressive disorder.4 Therefore, research on occurrence of MS in patients with depressive disorder is of extraordinary significance.
A rich body of evidence has established a bidirectional relationship between depression and MS.5–9 Prevalence of MS is significantly higher in inpatients with depressive disorder compared to healthy control subjects.10,11 Moreover, a population-based study by Moreira et al reported that association of depression symptoms with MS components is independent of diagnosis.12 Because of the high suicide rate in South Korea, there has been a growing interest in deciphering the associations between the two diseases in Koreans. For instance, a recent study using a nationally representative sample of Korean population found that depression is significantly associated with MS and its components.13 Han et al investigated 4.7 million Korean adults, and found that MS and its components are potential risk factors for major depressive disorder.14 Furthermore, a cross-sectional study reported that diagnosed depression is related to MS in Korean women.15 However, there are also studies that found no association between depression and MS.16,17 Since there is remarkable disparity in incidences of MS components between males and females,18 more studies on exploring the associations of MS and depression in male and female Koreans, respectively, are required.
Generally, education was regarded as a protective factor for depression. However, some studies also reported that well-educated undergraduates were at higher risk of depression compared to the general population.19,20 According to a meta-analysis based on 35 papers of 226,653 Chinese subjects, the pooled prevalence of MS was 24.5%, with a prevalence of 19.2% in males and 27.0% in females.21 China is a multi-ethnic country of 56 nationalities and one distinct minority is ethnic Koreans (Chaoxian). In light of this, the aim of this study was to investigate the relationships of depression with MS and its components in males and females, respectively in highly educated ethnic Koreans in the Yanbian Korean Autonomous Region of China, Potential risk factors for MS were uncovered as well.
Materials and Methods
Ethics Statement
This was a case–control study conducted in accordance with the Declaration of Helsinki. The study was approved by Independent Ethics Committee for Clinical Research of Zhongda Hospital, affiliated to Southeast University (2016ZDSYLL092-P01) and the Ethics Committee of China-Japan Union Hospital of Jilin University (No. 2017022201). Written informed consent was obtained from all participants.
Study Participants
From March 11th to 27th, 2017, the natural population of 18–70 year olds was continuously screened according to household registration of Yanbian Korean Autonomous Region. We contacted everyone who fulfilled the inclusion criteria to ask whether they were willing to participate in this study. The people willing to participate were invited to the community health centers of the Yanbian Korean Autonomous Region in China to complete the Zung Self-Rating Depression Scale (SDS). The people with SDS score ≥ 53 were assigned to depression group and those with SDS score < 53 were assigned to control group. Inclusion criteria for the depression group were listed as follows: ethnic Koreans in China; aged from 20 to 70 years, including employed after retirement; senior college degree or above; SDS score ≥ 5322 and capable of effective communication, writing, and expressing themselves. Exclusion criteria were: pregnancy; serious cardio-cerebral vascular diseases; incomplete information, and retirees. The flow chart of this study was displayed in Figure 1. Of the 1776 people attending the centers, a total of 367 subjects who fulfilled the criteria were enrolled inthe depression group, including 91 males and 276 females. Meanwhile, 388 age-, education- and gender-matched ethnic Koreans without depression (SDS score < 53) were used as the control group (95 males and 293 females).
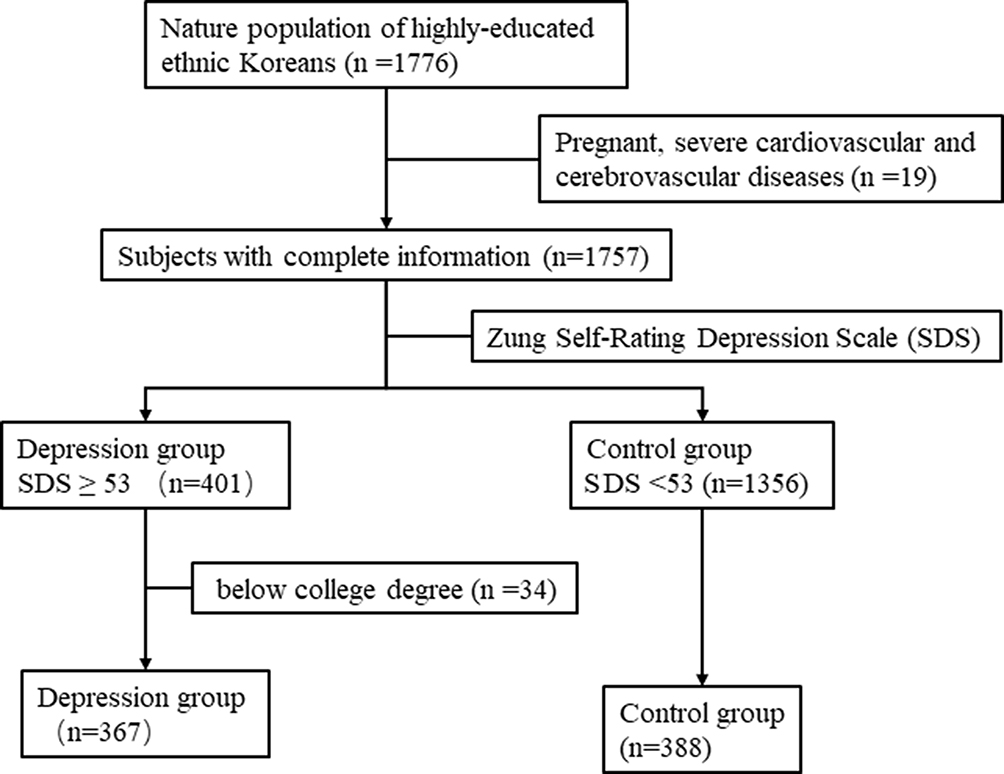 |
Figure 1 e flow chart of this study. SDS, Zung Self-Rating Depression Scale. |
For each participant, demographic characteristics (age and gender), clinical factors, life-style factors (smoking, alcohol consumption, and weekly exercise) and family history of relevant diseases including hypertension, diabetes mellitus (DM), dyslipidemia, and cardiovascular diseases were collected by means of a unified questionnaire administrated by well-trained endocrinologists.
Anthropometric and Metabolic Measures
Anthropometric factors including height, weight, blood pressure, and waist circumference (WC) were measured. Height was measured without shoes and hat to the nearest 0.1 cm. Measurement of height was in kilograms to the nearest 0.1 Kg, followed by calculation of BMI using the formula: BMI=Kg/m2. WC data were collected by measuring midway between the lowest rib margin and the superior iliac crest, to the nearest 0.1 cm. Blood pressure was measured by using sphygmomanometer according to standard procedures. Serum levels of glucose, total triglycerides (TG) and high-density lipoprotein-cholesterol (HDL-C) were measured by drawing fasting venous blood.
According to the guidelines established by World Health Organization (WHO),23 cigarette smoking was defined as those who had smoked more than 100 cigarettes or 150 g tobacco leaves up until the research, and smoked at least one time during the last month before the research. Alcohol drinking referred to consuming 30 g alcohol or more every week for a whole year or more.24
Diagnosis of MS was established according to the revised National Cholesterol Education Program definition.25 In addition to abdominal obesity defined based on an Asian-specific threshold of WC ≥ 90 cm for men and ≥ 80 cm for women, as suggested by the International Diabetes Foundation,26 at least two of the following four abnormalities were needed for diagnosis: elevated serum TG (≥ 1.7 mmol/L), or receiving specific treatment for this abnormality; decreased HDL level (< 1.03 mmol/L for men and < 1.29 mmol/L for women) or receiving specific treatment for this abnormality; systolic blood pressure (SBP) ≥ 130 mmHg and/or diastolic blood pressure (DBP) ≥ 85 mmHg, or receiving specific therapy for this disorder; fasting blood glucose (FBG) ≥ 5.6 mmol/L or having a diagnosis of type 2 diabetes mellitus (DM).
Statistical Analysis
Statistical analysis was carried out using SPSS (version 24.0) software. Continuous data were expressed as mean ± SD, while categorical data were expressed as frequencies and percentages. Comparison was conducted using Student’s t-test or Rank-Sum test for continuous data, and using Chi-Squared test or Fischer’s exact test for categorical data. Spearman correlation analysis was performed to estimate the associations of MS and its components with depression. Uni- and multi-variate logistics regression analysis was used to identify potential risk factors for MS based on a conceptual model with three hierarchical levels. The first level did not control for any confounding factor; the second level controlled for age and a family history of relevant diseases; the third level controlled for age, a family history of relevant diseases, cigarette smoking and alcohol drinking. The results were reported as odds ratio (OR) and 95% confidence interval (CI). P-value < 0.05 was defined as statistical significance.
Results
Comparisons of MS and Its Components Between the Subjects with Depression Status and the Control Subjects
A total of 755 participants were enrolled in the study. There were 186 males including 91 males with depression status and 95 male control subjects, and 569 females including 276 females with depression status and 293 female control subjects. Prevalence of MS was 17.2% in male participants, and 19.9% in female participants. Comparison of MS and its components was conducted in males and females, respectively. As shown in Table 1, there was a significantly higher prevalence of MS (28.5% vs 6.3%, X2 = 16.162, P-value <0.001) and greater WC in the males with depression status compared to the male control subjects (86.93 ± 7.02 cm vs 84.80 ± 5.87 cm, X2 = −2.255, P-value <0.001). The females with depression status had a significantly increased prevalence of MS (33.0% vs 7.5%, X2 = 57.896, P-value < 0.001), greater WC (78.02 ± 7.12 cm vs 75.79 ± 6.30 cm, X2 = −3.956, P-value < 0.001), elevated SBP (125.81 ± 16.94 mmHg vs 124.63 ± 20.58 mmHg, X2 = −0.745, P-value < 0.001), increased TG (1.35 (0.87, 2.00) vs 1.05 (0.70,1.66), X2 = −0.395, P-value < 0.001) and a higher prevalence of a family history of relevant diseases (23.9% vs 16.7%, X2 = 4.570, P-value = 0.033), and markedly decreased level of HDL-C (1.50 ± 0.52 mmol/L vs 1.61 ± 0.30 mmol/L, X2 = 3.065, P-value = 0.002) compared to the female control subjects.
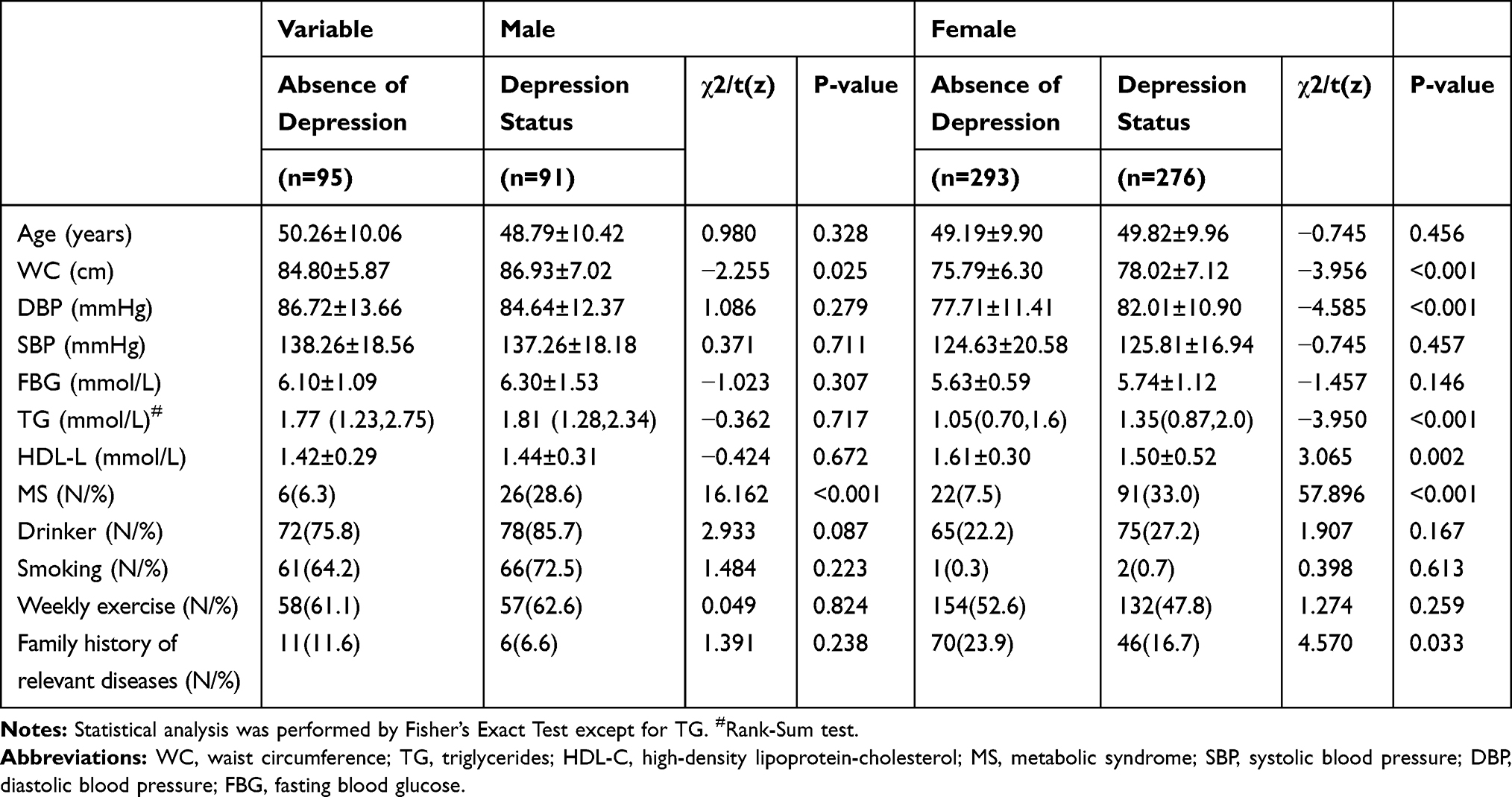 |
Table 1 Comparison of Demographic, Anthropometric and Metabolic Variables Between the Subjects with and without Depression |
Relationship of Depression with MS and Its Components in Males and Females
According to results of Spearman correlation analysis (Table 2), depression status was positively correlated with MS (r = 0.311, P-value < 0.01) and WC (r = 0.243, P-value < 0.01) in males. As for females (Table 3), positive associations were found between depression status and MS (r = 0.332, P-value < 0.01), WC (r = 0.239, P-value < 0.01), TG (r = 0.210, P-value < 0.01), SBP (r = 0.258, P-value < 0.01), and DBP (r = 0.103, P-value < 0.05).
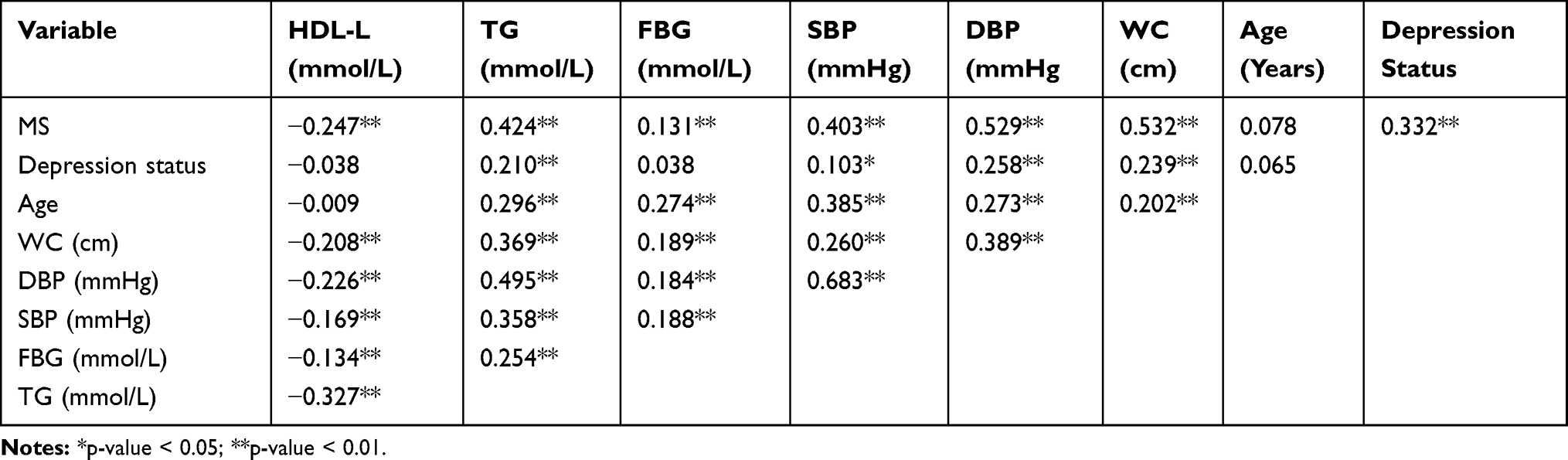 |
Table 2 Correlations of Depression Status with MS and its Components in Males |
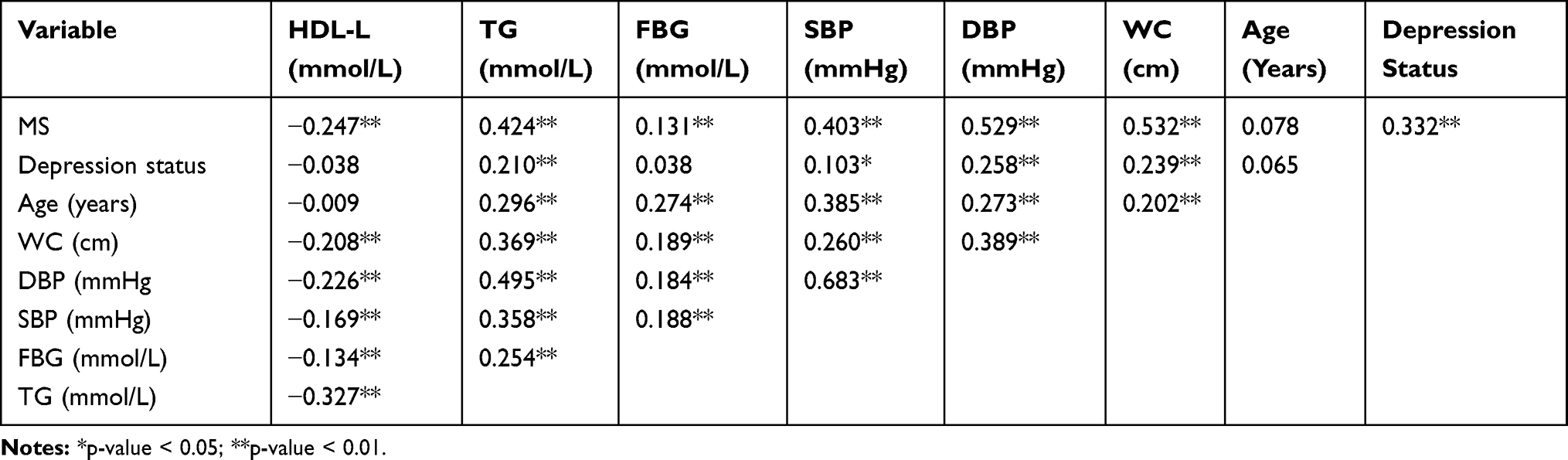 |
Table 3 Correlations of Depression Status with MS and its Components in Females |
Determination of Potential Risk Factors for MS by Logistic Regression Analysis
Chi-squared test was performed to evaluate the associations of depression, anthropometric and metabolic factors with MS in males and females, respectively. Table 4 showed that depression status (χ2 = 17.984, P-value < 0.001), WC (t = −12.053, P-value < 0.001), and SBP (t = −4.464, P-value<0.001) were significantly associated with MS in males. Depression status (χ2 = 63.853, P-value < 0.001), WC (t = −14.972, P-value < 0.001), DBP (t = −23.956, P-value < 0.001), SBP (t = −10.953, P-value < 0.001), FBG (t = −2.629, P-value = 0.010), TG (z =−10.098, P-value < 0.001), and HDL-C (z =−5.897, P-value < 0.001) were significantly related to MS in females. These significant variables were further subjected to multi-variate logistics regression analysis.
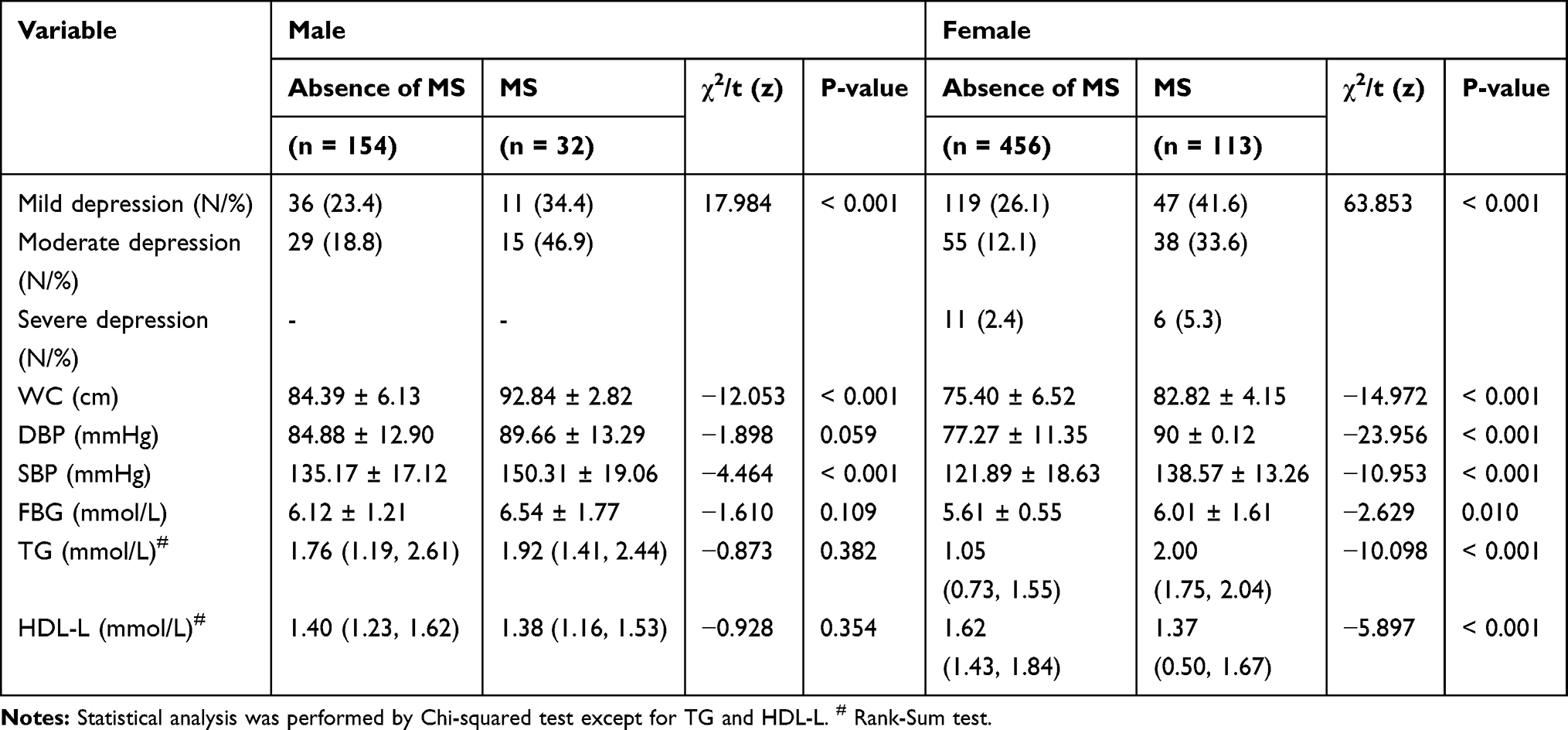 |
Table 4 Analysis of Factors Related with MS by Chi-Squared Test |
Results of multi-variate logistics regression analysis for male and female ethnic Koreans were displayed in Tables 5 and 6, respectively. After adjustment for age, a family history of relevant diseases, cigarette smoking, alcohol drinking, higher WC (OR = 1.562, 95% CI = 1.276–1.912) and elevated SBP (OR = 1.069, 95% CI = 1.020–1.120) were associated with an increased risk for MS in all male participants (Table 5). As for depression severity, mild and moderate depression statuses (OR = 5.942, 95% CI = 1.224–28.853; OR = 9.707, 95% CI = 2.050–45.969) were related to a higher risk for MS in all male subjects (Table 5). Male subjects with severe depression were not found in the current study. In female participants, mild (OR = 7.195, 95% CI = 3.000–17.258), moderate (OR = 8.991,95% CI = 3.724–21.709), and severe (OR = 6.599, 95% CI = 1.390–31.338) depression statuses, increased WC (OR = 1.365, 95% CI = 1.247–1.495), elevated SBP (OR = 1.052, 95% CI = 1.026–1.078), DBP (OR = 1.092, 95% CI = 1.040–1.145), and TG (OR = 2.150, 95% CI = 1.478–3.128) were associated with a higher risk for MS after controlling for the same confounding factors (age, a family history of relevant diseases, cigarette smoking and alcohol drinking, Table 6). On the contrary, higher level of HDL-C was correlated with a decreased risk for MS in females (Table 6). These results revealed that mild and moderate depression statuses, increased WC and SBP as well as elevated HDL-L were associated with MS in highly educated ethnic Koreans of China, regardless of gender.
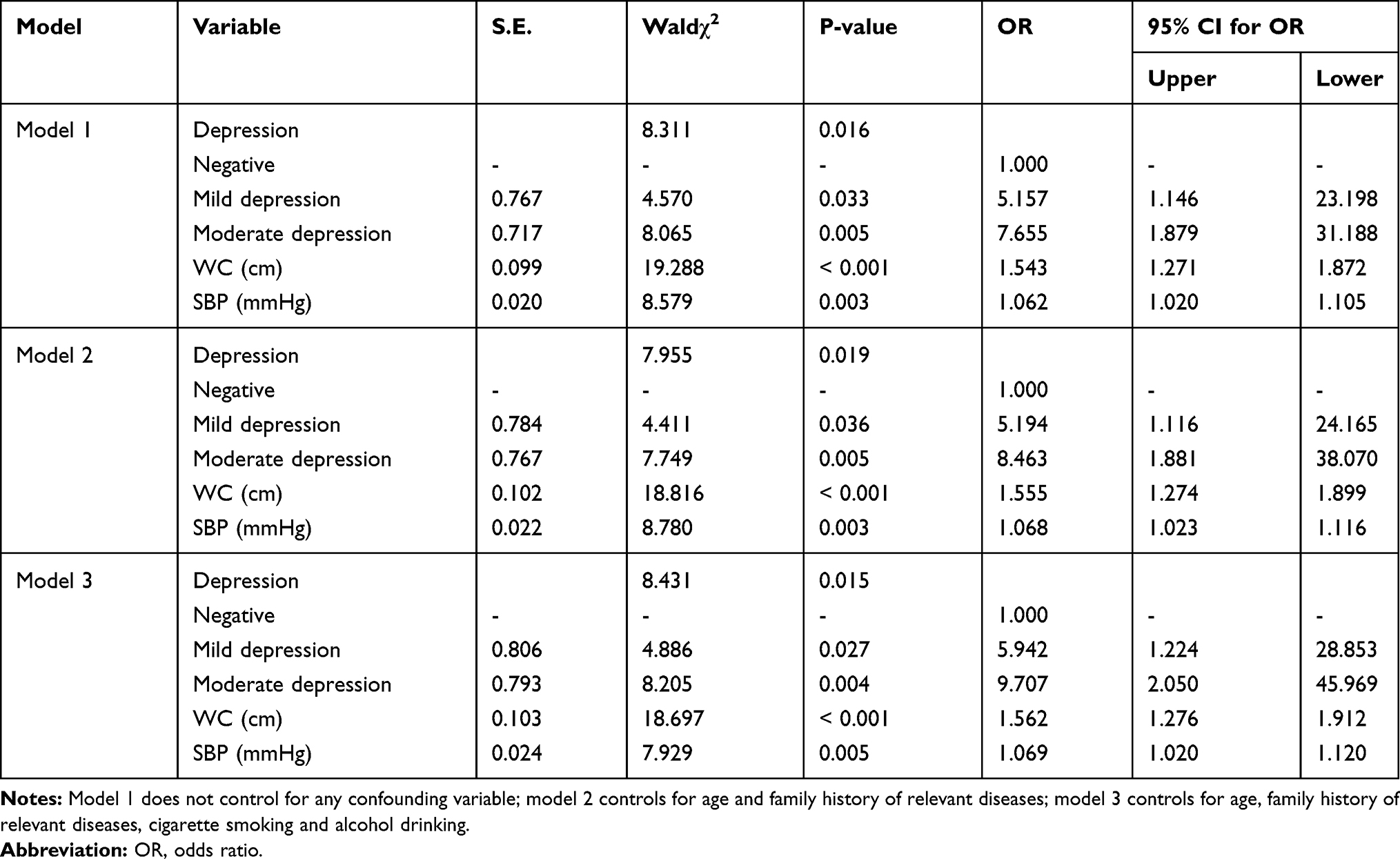 |
Table 5 Identification of the Factors Associated with the Presence of MS in Males by Multi-Variate Logistic Regression Analysis |
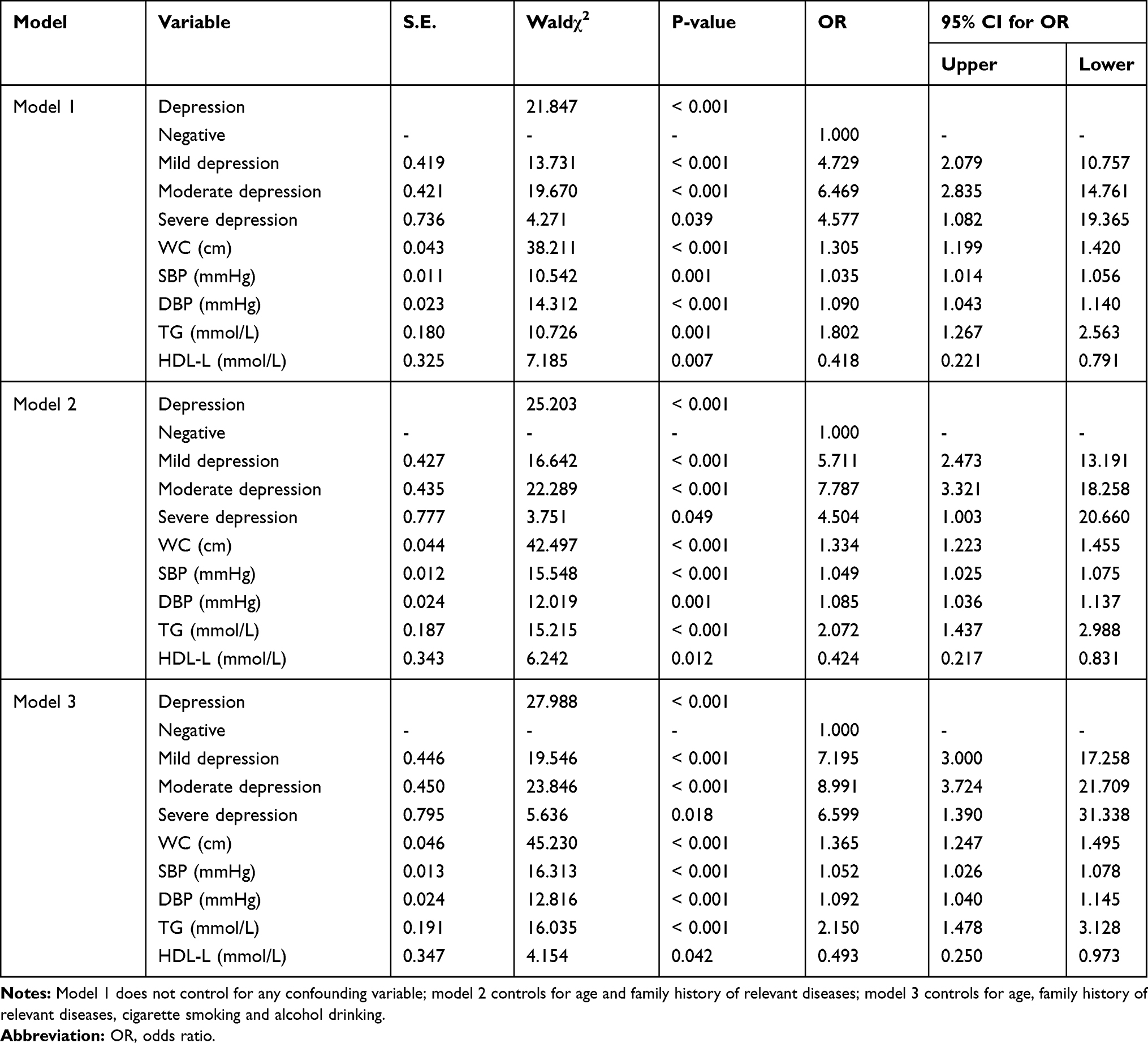 |
Table 6 Identification of the Factors Associated with the Presence of MS in Females by Multi-Variate Logistic Regression Analysis |
Discussion
China has 56 ethnic groups, with the Han nationality having the largest population. Ethnic Koreans are a minority nationality in China. This research studied the associations of depression with MS in highly educated ethnic Koreans of China. The current study found that depression status was positively correlated with MS in all participants (highly educated ethnic Koreans of China).
Depressive symptoms were assessed using the Zung’s SDS in this study. It comprises 20 self-report items with a total score ranging from 20 to 80.27 The cut-off scores of SDS are different among different populations. Zung recommended a cut-off of index scores of 50 in the US. Dunstan et al suggested that an index score of 55 might be more appropriate for Australian population.28 In a recent study, Dunstan et al recommended an SDS raw score of 50 as the cut-off point.29 Based on previous relevant studies by psychiatry professionals in China,30 SDS score greater than 53 was adopted as the cutoff point for positive depression status.
No consensus has been achieved regarding gender-dependent differences in the association between depression and MS. Research on healthy employed people in Israel showed that depression is associated with an increased risk for MS, elevated WC and increased glucose level in women, and for elevated WC only in men.31 Sekita et al revealed that increased depressive symptoms are associated with MS in Japanese men following adjustment for several demographic characteristics and life-style factors. Yet, they did not find any convincing evidence for significant association in women.32 Another study reported similar association of long-term depression with emergency of MS in Japanese men.33 Nonetheless, female gender was found to be related to consistent risk for depression in a large population-based sample of Mexican-Americans, with significant association between MS and depression.34 A 7-year follow-up study conducted in Finland concluded that depression may be a critical predisposing factor for MS in women rather than men.35 In the current study, significant differences were observed in the prevalence of MS between the male participants with and without depression status, and between the female participants with and without depression status. Moreover, depression status was positively correlated with MS in both male and female participants. These results suggest that the association between depression and MS is independent of gender in highly educated ethnic Koreans. These inconsistent findings between our study and previous studies may be due to different ethnic groups and education levels of participants.
This study found positive correlations of depression status with WC, TG, SBP and DBP in female participants, and with WC only in male participants. Consistently, increasing studies have proven that obesity increases the risk for developing depression.36,37 Mattei et al demonstrated that enlarged WC was associated with anxiety symptoms in Italian.38 This finding may be explained by disparity in hormones, social and economic factors, and social roles between male and female ethnic Koreans. Greater WC in males than females may be another reason. Noticeably, moderate and severe depression was shown to be associated with MS in female participants. Females may lose weight because of poor diet and sleep disturbances caused by severe depression, and thus are less likely to develop MS.
Some hypotheses have been proposed concerning the mechanisms between the associations of MS and depression.39 Disturbances in hypothalamus-pituitary-adrenal (HPA) axis, autonomic nervous system, and immune system may play important roles in the mechanisms.40,41 Besides, peripheral hormones, such as leptin and ghrelin may be involved in the pathophysiology as well.42 There is also a hypothesis that anxious-depression should be regarded as a chronic inflammatory state.43–45 This association might be explained by the fact that pro‐inflammatory cytokines trigger the transcriptional induction of indoleamine 2,3‐dioxygenase, rate‐limiting enzyme of tryptophan–kynurenine pathway.46 Further, Rioli et al confirmed this hypothesis and found depressive symptoms were associated with C-reactive protein levels.47
Some limitations of this study should be mentioned. No male participants with severe depression were found in this study due to limited sample size. Therefore, a prospective study based on a large number of highly educated ethnic Koreans is needed to validate these findings. Depression severity was determined by using SDS in this study. SDS score ≥ 53 is not sufficient for diagnosis of depressive disorder. Subjects with moderate or severe depression in this study were advised to consult a psychiatrist for further examination. Moreover, further detailed studies are necessary to elucidate the molecular mechanisms behind the associations between the two diseases.
Conclusion
Taken together, our study suggests that depression correlates with MS and is a potential risk factor for MS in well-educated ethnic Koreans in China, regardless of gender. Effective treatment of depression in patients with comorbid depression and MS may alleviate MS and improve the quality of life of patients. Results of this study could aid in development of gender-specific preventative and therapeutic strategies against the two diseases. Further studies using a large cohort of highly educated ethnic Koreans are required to replicate these results.
Abbreviations
MS, metabolic syndrome; WC, waist circumference; TG, total triglycerides; HDL-C, high-density lipoprotein-cholesterol; OR, odds ratio; DM, diabetes mellitus; CI, confidence interval; HPA, hypothalamus-pituitary-adrenal.
Data Sharing Statement
Not applicable. This study was only the primary research, and further study has been in progress.
Ethics Approval and Consent to Participate
This was a case–control study approved by Independent Ethics Committee for Clinical Research of Zhongda Hospital, affiliated to Southeast University (2016ZDSYLL092-P01) and the Ethics Committee of China-Japan Union Hospital of Jilin University (No. 2017022201). Written informed consent was obtained from all participants.
Consent for Publication
Written informed consent was obtained from participants.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Key R&D Program of China (Program No. 2016YFC1305700) and the National Key Scientific Instrument and Equipment Development Project of China (Program No. 51627808).
Disclosure
The authors declare that they have no competing interests.
References
1. Punthakee Z, Goldenberg R, Diabetes Canada Clinical Practice Guidelines Expert Committee, et al. Definition, classification and diagnosis of diabetes, prediabetes and metabolic syndrome. Can J Diabetes. 42;2018:S10–S15. doi:10.1016/j.jcjd.2017.10.003
2. Saklayen MG. The global epidemic of the metabolic syndrome. Curr Hypertens Rep. 2018;20(2):12.
3. Dall TM, Yang W, Halder P, et al. The economic burden of elevated blood glucose levels in 2012: diagnosed and undiagnosed diabetes, gestational diabetes mellitus, and prediabetes. Diabetes Care. 2014;37(12):3172–3179. doi:10.2337/dc14-1036
4. Penninx BW, Lange SM. Metabolic syndrome in psychiatric patients: overview, mechanisms, and implications. Dialogues Clin Neurosci. 2018;20(1):63–73.
5. McIntyre RS, Rasgon NL, Kemp DE, et al. Metabolic syndrome and major depressive disorder: co-occurrence and pathophysiologic overlap. Curr Diab Rep. 2009;9(1):51–59. doi:10.1007/s11892-009-0010-0
6. Hiles SA, Révész D, Lamers F, Giltay E, Penninx BW. Bidirectional prospective associations of metabolic syndrome components with depression, anxiety, and antidepressant use. Depress Anxiety. 2016;33(8):754–764. doi:10.1002/da.22512
7. Gheshlagh RG, Parizad N, Sayehmiri K. The relationship between depression and metabolic syndrome: systematic review and meta-analysis study. Iran Red Crescent Med J. 2016;18(6):e26523.
8. Tang F, Wang G, Lian Y. Association between anxiety and metabolic syndrome: a systematic review and meta-analysis of epidemiological studies. Psychoneuroendocrinology. 2017;77:112–121. doi:10.1016/j.psyneuen.2016.11.025
9. Pan A, Keum N, Okereke OI, et al. Bidirectional association between depression and metabolic syndrome: a systematic review and meta-analysis of epidemiological studies. Diabetes Care. 2012;35(5):1171–1180. doi:10.2337/dc11-2055
10. Grover S, Nebhinani N, Chakrabarti S, Avasthi A. Prevalence of metabolic syndrome among patients with depressive disorder admitted to a psychiatric inpatient unit: a comparison with healthy controls. Asian J Psychiatr. 2017;27:139–144. doi:10.1016/j.ajp.2017.02.030
11. Vancampfort D, Stubbs B, Mitchell AJ, et al. Risk of metabolic syndrome and its components in people with schizophrenia and related psychotic disorders, bipolar disorder and major depressive disorder: a systematic review and meta-analysis. World Psychiatry. 2015;14(3):339–347. doi:10.1002/wps.20252
12. Moreira FP, Jansen K, de Azevedo Cardoso T, et al. Metabolic syndrome in subjects with bipolar disorder and major depressive disorder in a current depressive episode: population-based study: metabolic syndrome in current depressive episode. J Psychiatr Res. 2017;92:119–123. doi:10.1016/j.jpsychires.2017.03.025
13. Ko J, Han K, Shin C, et al. Association of metabolic syndrome and its components with suicidal ideation and depression in adults: a nationally representative sample of the korean population. J Affect Disord. 2019;249:319. doi:10.1016/j.jad.2019.02.049
14. Han K-M, Kim MS, Kim A, et al. Chronic medical conditions and metabolic syndrome as risk factors for incidence of major depressive disorder: a longitudinal study based on 4.7 million adults in south korea. J Affect Disord. 2019;257:486–494. doi:10.1016/j.jad.2019.07.003
15. Park SJ, Roh S, Hwang J, et al. Association between depression and metabolic syndrome in korean women: results from the korean national health and nutrition examination survey (2007–2013). J Affect Disord. 2016;205:393–399. doi:10.1016/j.jad.2016.08.022
16. Yu S, Yang H, Guo X, et al. Metabolic syndrome and depressive symptoms among rural northeast general population in China. BMC Public Health. 2017;17(1):43. doi:10.1186/s12889-016-3913-0
17. Hildrum B, Mykletun A, Midthjell K, et al. No association of depression and anxiety with the metabolic syndrome: the Norwegian HUNT study. Acta Psychiatr Scand. 2009;120(1):14–22. doi:10.1111/j.1600-0447.2008.01315.x
18. Rochlani Y, Pothineni N, Mehta J. Metabolic syndrome: does it differ between women and men? Cardiovasc Drugs Ther. 2015;29(4):329–338. doi:10.1007/s10557-015-6593-6
19. Ibrahim A, Kelly S, Adams C, et al. A systematic review of studies of depression prevalence in university students. J Psychiatr Res. 2013;47(3):391–400. doi:10.1016/j.jpsychires.2012.11.015
20. Othman N, Ahmad F, El Morr C, Ritvo P. Perceived impact of contextual determinants on depression, anxiety and stress: a survey with university students. Int J Ment Health Syst. 2019;13(1):17. doi:10.1186/s13033-019-0275-x
21. Li R, Li W, Lun Z, et al. Prevalence of metabolic syndrome in mainland china: a meta-analysis of published studies. BMC Public Health. 2016;16(1):296. doi:10.1186/s12889-016-2870-y
22. Yin W, Pang L, Cao X, et al. Factors associated with depression and anxiety among patients attending community‐based methadone maintenance treatment in China. Addiction. 2015;110(Suppl 1):51–60. doi:10.1111/add.12780
23. World Health Organization. Guidelines for the conduct of tobacco smoking survey of the general population: report of a who meeting held in helsinki, finland, 29 november- 4december 1982. 1983
24. Li J, Fan S, Li Y, et al. Incidence of obesity and its modifiable risk factors in chinese adults aged 35–74 years: a prospective cohort study. Zhonghua Liu Xing Bing Xue Za Zhi. 2014;35(4):349–353.
25. Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an american heart association/national heart, lung, and blood institute scientific statement. Circulation. 2005;112(17):2735–2752. doi:10.1161/CIRCULATIONAHA.105.169404
26. Alberti K, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; american heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation. 2009;120(16):1640–1645.
27. Zung WWK. A self-rating depression scale. Arch Gen Psychiatry. 1965;12(1):63–70. doi:10.1001/archpsyc.1965.01720310065008
28. Dunstan DA, Scott N, Todd AK. Screening for anxiety and depression: reassessing the utility of the Zung scales. BMC Psychiatry. 2017;17(1):329. doi:10.1186/s12888-017-1489-6
29. Dunstan DA, Scott N. Clarification of the cut-off score for Zung’s self-rating depression scale. BMC Psychiatry. 2019;19(1):177. doi:10.1186/s12888-019-2161-0
30. Wang CF, Cai ZH, Xu Q. Evaluation analysis of self-rating disorder scale in 1340 people. Chin J Nervous Ment Dis. 2009;12:267–268.
31. Toker S, Shirom A, Melamed S. Depression and the metabolic syndrome: gender-dependent associations. Depress Anxiety. 2008;25(8):661–669. doi:10.1002/da.20379
32. Sekita A, Arima H, Ninomiya T, et al. Elevated depressive symptoms in metabolic syndrome in a general population of japanese men: a cross-sectional study. BMC Public Health. 2013;13(1):862. doi:10.1186/1471-2458-13-862
33. Viinamäki H, Heiskanen T, Lehto S, et al. Association of depressive symptoms and metabolic syndrome in men. Acta Psychiatr Scand. 2009;120(1):23–29. doi:10.1111/j.1600-0447.2008.01333.x
34. Olvera RL, Williamson DE, Fisher-Hoch SP, Vatcheva KP, McCormick JB. Depression, obesity, and metabolic syndrome: prevalence and risks of comorbidity in a population-based study of mexican americans. J Clin Psychiatry. 2015;76(10):e1300. doi:10.4088/JCP.14m09118
35. Vanhala M, Jokelainen J, Keinänen‐Kiukaanniemi S, et al. Depressive symptoms predispose females to metabolic syndrome: a 7‐year follow‐up study. Acta Psychiatr Scand. 2009;119(2):137–142. doi:10.1111/j.1600-0447.2008.01283.x
36. Lazarevich I, Camacho MEI, Del Consuelo Velázquez-Alva M, et al. Relationship among obesity, depression, and emotional eating in young adults. Appetite. 2016;107:639–644. doi:10.1016/j.appet.2016.09.011
37. Lasserre AM, Glaus J, Vandeleur CL, et al. Depression with atypical features and increase in obesity, body mass index, waist circumference, and fat mass: a prospective, population-based study. JAMA Psychiatry. 2014;71(8):880–888. doi:10.1001/jamapsychiatry.2014.411
38. Mattei G, Padula MS, Rioli G, et al. Metabolic syndrome, anxiety and depression in a sample of Italian primary care patients. J Nerv Ment Dis. 2018;206(5):316–324.
39. Marazziti D, Rutigliano G, Baroni S, et al. Metabolic syndrome and major depression. CNS Spectr. 2014;19(4):293–304. doi:10.1017/S1092852913000667
40. Jabben N, Nolen WA, Smit JH, et al. Co-occurring manic symptomatology influences hpa axis alterations in depression. J Psychiatr Res. 2011;45(9):1208–1213.
41. Licht CM, Vreeburg SA, van Reedt Dortland AK, et al. Increased sympathetic and decreased parasympathetic activity rather than changes in hypothalamic-pituitary-adrenal axis activity is associated with metabolic abnormalities. J Clin Endocrinol Metab. 2010;95(5):2458–2466. doi:10.1210/jc.2009-2801
42. Zarouna S, Wozniak G, Papachristou AI. Mood disorders: A potential link between ghrelin and leptin on human body? World J Exp Med. 2015;5(2):103–109. doi:10.5493/wjem.v5.i2.103
43. Camacho A. Is anxious-depression an inflammatory state? Med Hypotheses. 2013;81(4):577–581. doi:10.1016/j.mehy.2013.07.006
44. Maes M. The cytokine hypothesis of depression: inflammation, oxidative & nitrosative stress (IO&NS) and leaky gut as new targets for adjunctive treatments in depression. Neuro Endocrinol Lett. 2008;29(3):287–291.
45. Maes M, Kubera M, Obuchowiczwa E, et al. Depression’s multiple comorbidities explained by (neuro)inflammatory and oxidative & nitrosative stress pathways. Neuro Endocrinol Lett. 2011;32(1):7–24.
46. Oxenkrug GF. Metabolic syndrome, age-associated neuroendocrine disorders, and dysregulation of tryptophan-kynurenine metabolism. Ann N Y Acad Sci. 2010;1199(1):1–14. doi:10.1111/j.1749-6632.2009.05356.x
47. Rioli G, Tassi S, Mattei G, et al. The association between symptoms of anxiety, depression, and cardiovascular risk factors: results from an italian cross-sectional study. J Nerv Ment Dis. 2019;207(5):340–347. doi:10.1097/NMD.0000000000000969
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.