")
Back to Journals » Psychology Research and Behavior Management » Volume 13
Association of COVID-19 Pandemic with undergraduate Medical Students’ Perceived Stress and Coping
Authors Abdulghani HM , Sattar K , Ahmad T , Akram A
Received 17 August 2020
Accepted for publication 7 October 2020
Published 30 October 2020 Volume 2020:13 Pages 871—881
DOI https://doi.org/10.2147/PRBM.S276938
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Hamza Mohammad Abdulghani, Kamran Sattar, Tauseef Ahmad, Ashfaq Akram
Department of Medical Education, College of Medicine, King Saud University, Riyadh, Kingdom of Saudi Arabia
Correspondence: Kamran Sattar
Department of Medical Education, College of Medicine, King Saud University, Riyadh, Kingdom of Saudi Arabia
Email [email protected]
Purpose: The COVID-19 pandemic poses a major challenge for medical students’ learning and has become a potential stressor, with a profound influence on their psychological well-being. We aimed to determine the effect of the current pandemic on undergraduate medical students’ learning. We also explored the association of their stress level with coping strategies, educational, and psychological variables.
Materials and Methods: This is a cross-sectional design study, and participants were the 1st to 5th year medical students. A self-administered questionnaire (18 items) and a well-known Kessler 10 Psychological Distress questionnaire (10 items) were used to collect the data related to perceived stress with an association of educational, psychological, and coping variables.
Results: The prevalence of overall stress was significantly higher (χ 2= 16.3; P=0.000) in female medical students, ie, (40%) as compared to the male students (16.6%), and was highest (48.8%) during the 3rd medical year. It was also noted that the most effective strategy, embraced by students to cope with the severe stress, was “indulging in religious activities” (OR= 1.08; P=0.81). Furthermore, 22.3% of students had perceived severe stress as they did not prefer online learning. Similarly, those students who have not believed or refused the online learning or disagree in “there is pleasure in the study due to COVID” they have significantly higher stress (χ 2=39.7; P=0.000) 21.5% mild, 17.8% of moderate, and 21.2% severe.
Conclusion: We found that the COVID-19 pandemic has induced stress and changes in medical students’ educational attitudes and strategies. The results exhibited that the predominance of stress is higher in females than males, and also more stress was perceived by the students during their transitional year, ie, 3rd medical year (from pre-clinical to clinical) and also the respondents who regularly did religious meditation were at lower levels of stress. COVID-19’s influence on medical education and students’ well-being will be felt at an extended level, which necessitates an appropriate plan for preparedness.
Keywords: COVID-19, undergraduate medical education, learning, wellbeing, stress, coping
A Letter to the Editor has been published for this article.
A Response to Letter has been published for this article.
Background
The recent pandemic of the novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), also called COVID-19 arisen from Wuhan, China, and has and global effect triggering colossal intimidations to human health. The present pandemic poses more danger to human lives as COVID-19 has varied epidemiological features, thus, making it more transmittable than earlier pandemics such as SARS-CoV and MERS-CoV.1 This situation has alarmingly threatened the entire world,2 and people in many countries were asked (who have possibly come into contact with the infection) to be quarantined. The quarantine is a state of voluntary home constraints, termination of public gatherings, as well as travel limitations.3
It is witnessed that during the present COVID-19 pandemic, many schools and universities have deferred regular teaching activities. Health education is seen to be challenging4 and currently interrupted.5 One of the most significant changes made was the termination of teaching sessions in-person (face to face), and most of which were substituted by video lectures6 or live streams.7 Such circumstances have negative bearings on the mental health of medical students. Students have high levels of anxiety and depression,8 which leads to a detrimental impact on the cognitive functioning and learning of medical students.9
The coping strategies can be divided into two specific types; problem-oriented and emotion-oriented coping.10 Coping strategies are a set of acts or a method of thinking used to cope with a stressful or uncomfortable situation or to change one’s response to such a situation.11
Strategies to cope with stress are cognitive and behavioral skills (developed in reaction to a stressful event), which have the purpose of decreasing momentary aversive qualities and improving personal control perception. The current pandemic conditions have affected educational happenings. Moreover, students’ routine life, as well as psychological health, could not remain unaffected. Therefore, we aimed to determine the effect of the current pandemic on undergraduate medical students’ learning and the association of their stress level with coping strategies, educational, and psychological variables, particularly during this isolation time. Therefore, our objectives are to collect undergraduate medical students’ responses concerning:
- Learning, during COVID-19 pandemic, using educational variables.
- Identification of stress level and coping strategies, utilising multiple psychological variables.
Methods
Study Design
We conducted a descriptive study utilizing quantitative strategies in gathering the information. It is a cross-sectional design study.
Settings and Participants
This study was conducted at the department of medical education, college of medicine, King Saud University (KSU), Riyadh, Saudi Arabia. The participants were the 1st to 5th year medical students. In the current COVID situation, most of the universities conducted online classes around the world; similarly, one of the oldest universities in Saudi Arabia (KSU) also conducts online sessions in the current situation. In this study, all participation was entirely voluntary, and the participants were able to respond at their convenience and time. Privacy was ensured, and whoever agreed to participate and give the viewpoint about the online learning class. This study was conducted from April 2020 to May 2020.
Instrument
In the current study, we have utilized a validated Psychological Distress instrument Kessler-10 (K10), which was developed by Kessler et al.12 This instrument has been generally used in populace-based epidemiological studies to quantify the stress and was translated in different languages, including Arabic, to measure the level of stress and seriousness related to psychological symptoms in population surveys.4,13,14 The K10 comprises ten questions in the form of “how often in the past month did you feel” and offers explicit side effects, such as “none of the time” to “all of the time” and were counted from 1 to 5 correspondingly. All the questions were ordered to get an absolute score. The absolute scores were deciphered as follows: A score of 20 is considered not to reflect the stress of any level; a score of 20–24 is of mild stress; 25–29 is of moderate stress, and 30–50 is of severe stress.12 Furthermore, a self-administered questionnaire was designed after an exhaustive literature review to achieve the objectives of the study related to the educational, psychological, and coping variables. There were a total of 23 items in the initially drafted version, which went under exclusive discussion among a panel of four medical educationists from an extensive teaching background. As a result of two meetings and extensive discussion among the panel, 18 items were agreed upon.
Data Collection
The study protocol was approved by the institutional review board of college of medicine, King Saud University. A written informed consent was provided to all participants and their participation was voluntary. Also, we described that the information would remain strictly confidential.
A self-administered questionnaire with 18 items, and a 10-items validated questionnaire (Actual English version with Arabic translation), ie, “Kessler 10 Psychological Distress” (K10)’ was used.12 Both questionnaires were distributed online through a google form. All medical students were provided with a written consent form to be informed about the objective of the study and clarified the various constituents of the questionnaires. We collected demographic information in the first part, second part comprised of distress instrument (Kessler 10) to observe the medical students’ activities during the past four weeks, the third part contained the academic variables with six items, the fourth part asked about psychological variables with five items. Finally, we patterned the students coping strategies with seven items in the current COVID-19 situation.
Statistical Analysis
Numerical data were entered and analyzed in Microsoft Excel using SPSS Statistics, version 22.0 (IBM Corporation, Armonk, NY, USA). The prevalence of a result variable was estimated along with confidence intervals of 95%. Pearson’s chi-square test and odds ratios (ORs) were used to determine and quantify the associations between a definite outcome and the variables being considered. During the entire study, the statistical significance level has been established as P<0.05.
Results
The demographic information of participants includes gender, age, marital status, residences, and year of study. A total of 352 participants agreed to take part, and after a careful evaluation, 243 completed responses were received and included in the study, with a response rate of 69.03%. Among 243 medical students, there were 163 (67.1%) male and 80 (32.9%) female students. The age of the study participants was 20.6±1.6 (mean± standard deviation [SD]). The participants’ year of study was from 1 to 5, and the K10 stress score was normally distributed among them (Table 1). The level of stress was reported as no stress 109 (44.9%), mild stress 75 (30.9%), moderate stress 28 (11.5%), and severe stress 31 (12.8%) (Table 1).
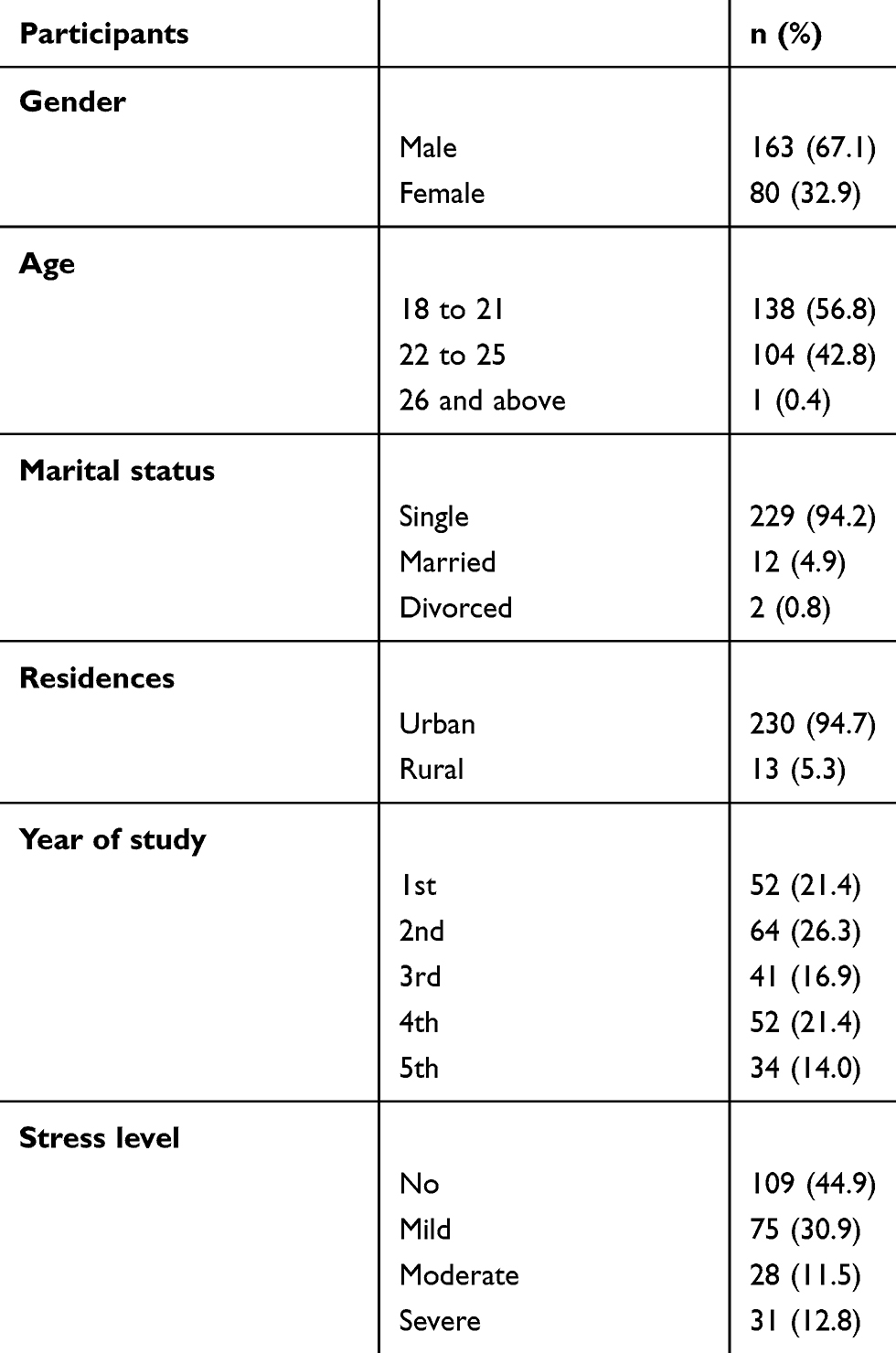 |
Table 1 Demographic Information of Participants |
The prevalence of overall stress was significantly higher (χ2= 16.3; P=0.000) in female medical students, ie, (40%) as compared to the male students (16.6%). Moreover, the prevalence of the stress was highest among the year of study at 3rd year (48.8%), whereas, by 5th year (24.3%), 1st year (25%), 4th year (17.3%), and 2nd year only (9.4%) levels (χ2= 23.71; P=0.000) (Table 2). The severe stress was significantly higher, ie, (~10 times) in the female medical students (OR= 9.91; P=<0.0001). The age groups of 18 to 21 years’ have severe stress, which was significantly (3-times) higher (OR= 3.15; P=0.01) as compared to other age groups measured (Table 3). The mild level of stress was more common in the 5th year medical students (OR= 4.68; P=0.017), 1st year students (OR= 2.14; P=0.18), and 2nd year students (OR= 2.03; P=0.19) (Table 3). The moderate stress was also significant in the 5th year medical students (OR= 20.6; P=0.007). However, the prevalence of severe stress was significantly greater (OR= 13.5; P=0.0002) in the 3rd year as compared to other years explored.
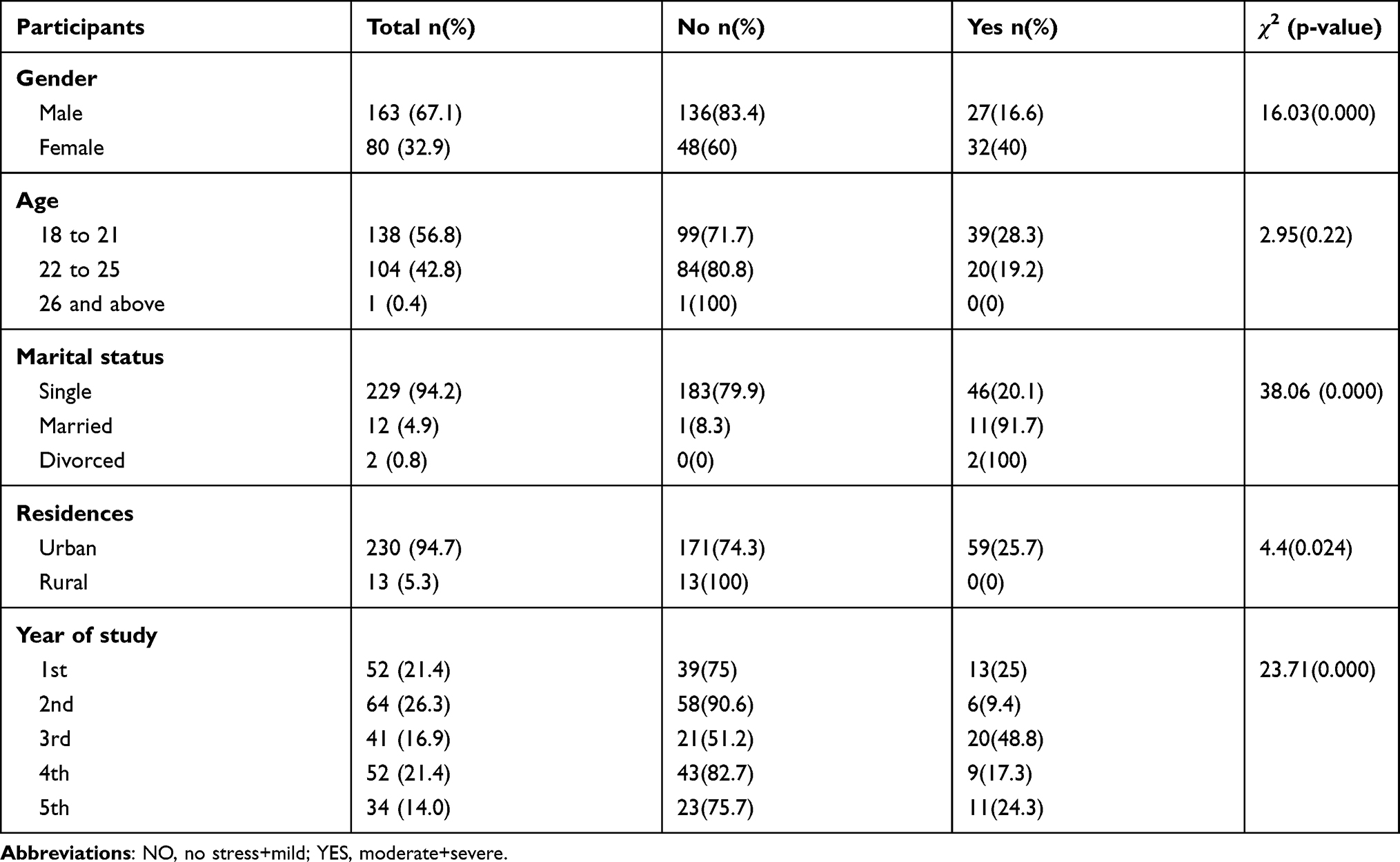 |
Table 2 Overall Stress Level in Medical Students with Demographic Information |
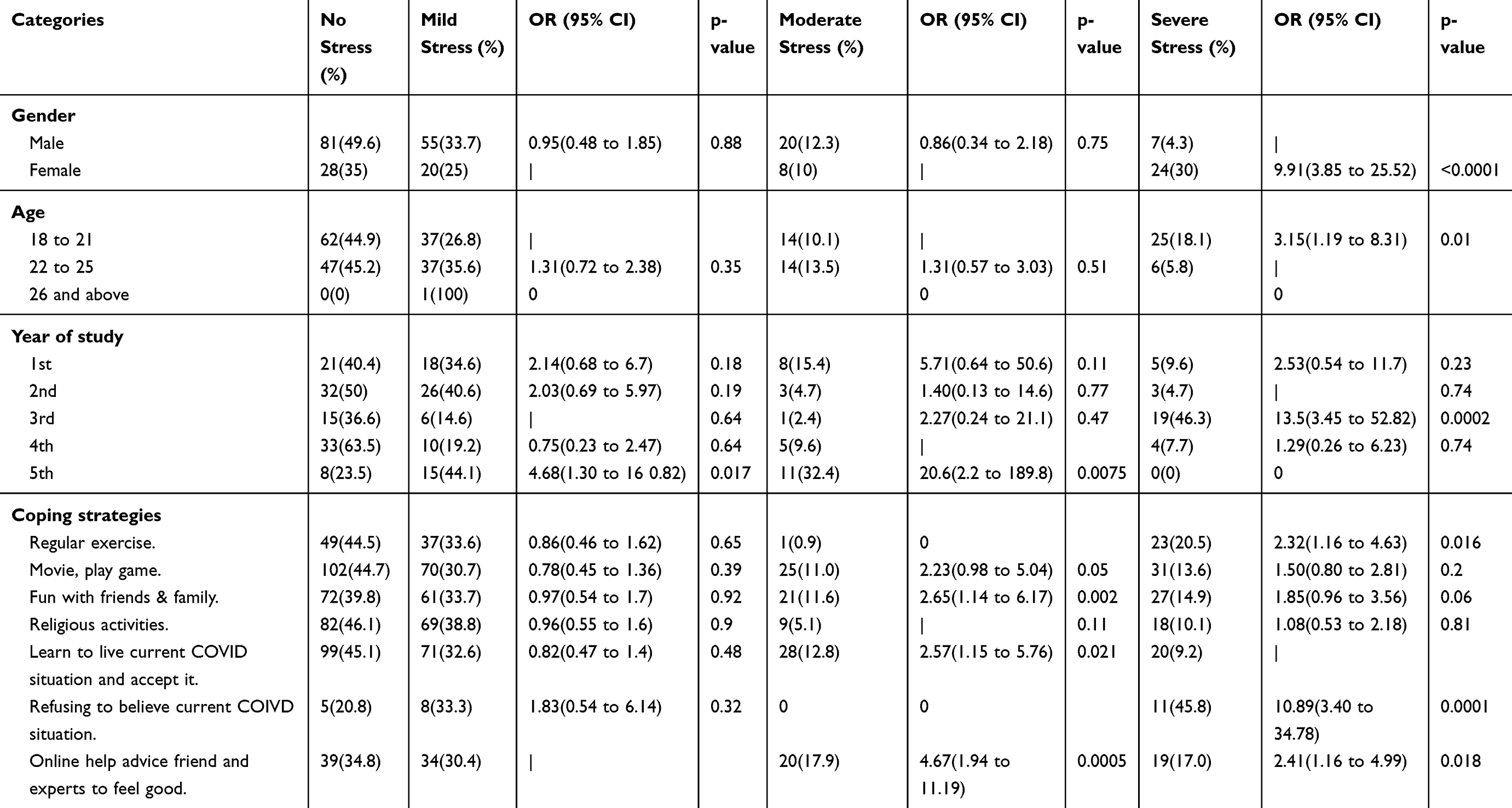 |
Table 3 Associations Between Stress Levels and Different Variables |
The coping strategies to deal with mild stress were found to be recorded as “regular exercise” (OR= 0.86; P=0.65), “watching online movies” playing online games’ (OR= 0.78; P=0.39), “online fun with family and friends” (OR= 0.97; P=0.92), “religious activities” (OR= 0.96; P=0.90) and “learning to live in current COVID situation and accept it” (OR= 0.82; P=0.48). The strategies embraced by students to cope with the severe stress were “indulging in religious activities” (OR= 1.08; P=0.81), “watching online movies and playing online games” (OR= 1.5; P=0.2), and “online fun with family and friends.” Moreover, those students who were found refusing to accept the current COVID situation have almost the 2-times higher level of mild stress level (OR= 1.83; P=0.32) and almost 11-time higher level of severe stress (OR= 10.89; P=0.0001) (Table 3).
The current study also found that the association between medical student’s academic variables and stress levels, as20.3% of the medical students who agreed that “online learning has become a burden” have significant (χ2=17.8; P=0.007) levels of severe stress. Moreover, 41.2% of students who responded as “neutral” about “online learning content is difficult to understand” have exhibited mild (22%), moderate (16%), and severe (16%) stress. Regarding “online learning material is not enough for study,” neutral respondents showed moderate to severe stress. Additionally, 46.1% of students agreed that “regular class lecture is easy to understand” they had significantly higher (χ2=35.2; P=0.000) levels of severe stress (in other words, they have shown their inclination towards regular class lectures instead of current online sessions). Similarly, those students who were not able to manage the time for their online learning; found to show significantly high levels of severe stress (20.4%) level (Table 4).
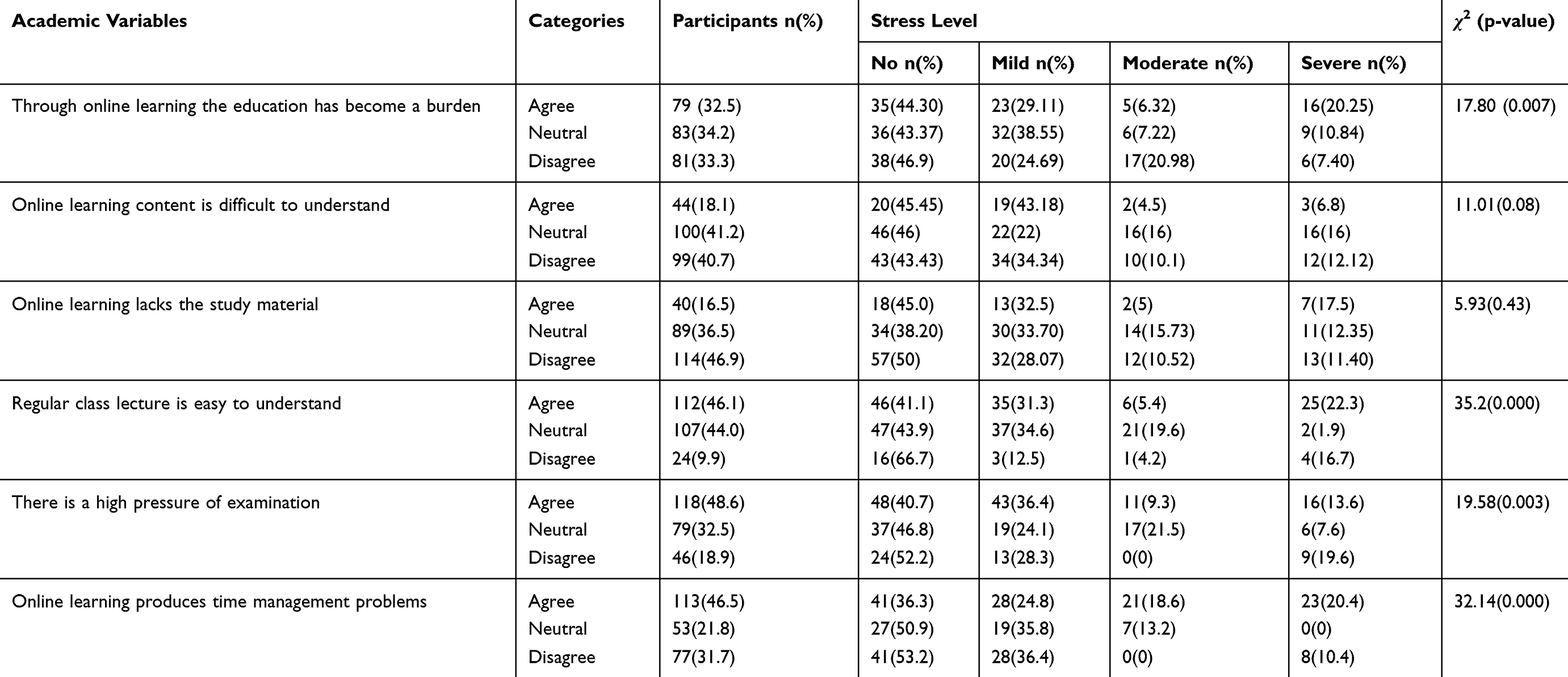 |
Table 4 Stress Level in Medical Students with Academic Variables |
Table 5 outlines that 25.9% of students reported having difficulty concentrating during the “online learning session.” Whereas 26.4% of the students were among those who responded as being “neutral,” yet their levels of severe stress were higher as compared to others. Most of the students (58.4%) reported that they have anxiety before online learning sessions, and shown that they have 26.1% mild, 7.7% of moderate, and 15.5% of severe stress. Similarly, those students who have not believed or refused the online learning or disagree in “there is pleasure in the study due to COVID” they have significantly higher stress (χ2=39.7; P=0.000) 21.5% mild, 17.8% of moderate, and 21.2% severe stress. Moreover, 72% of the students reported (agree/disagree) for they have no anxiety about performance in their examination, among them, the stress level was significantly higher (χ2=17.3; P=0.008), 29.7% of mild stress, 12.6% of moderate stress and 17.7% of severe stress (Table 5).
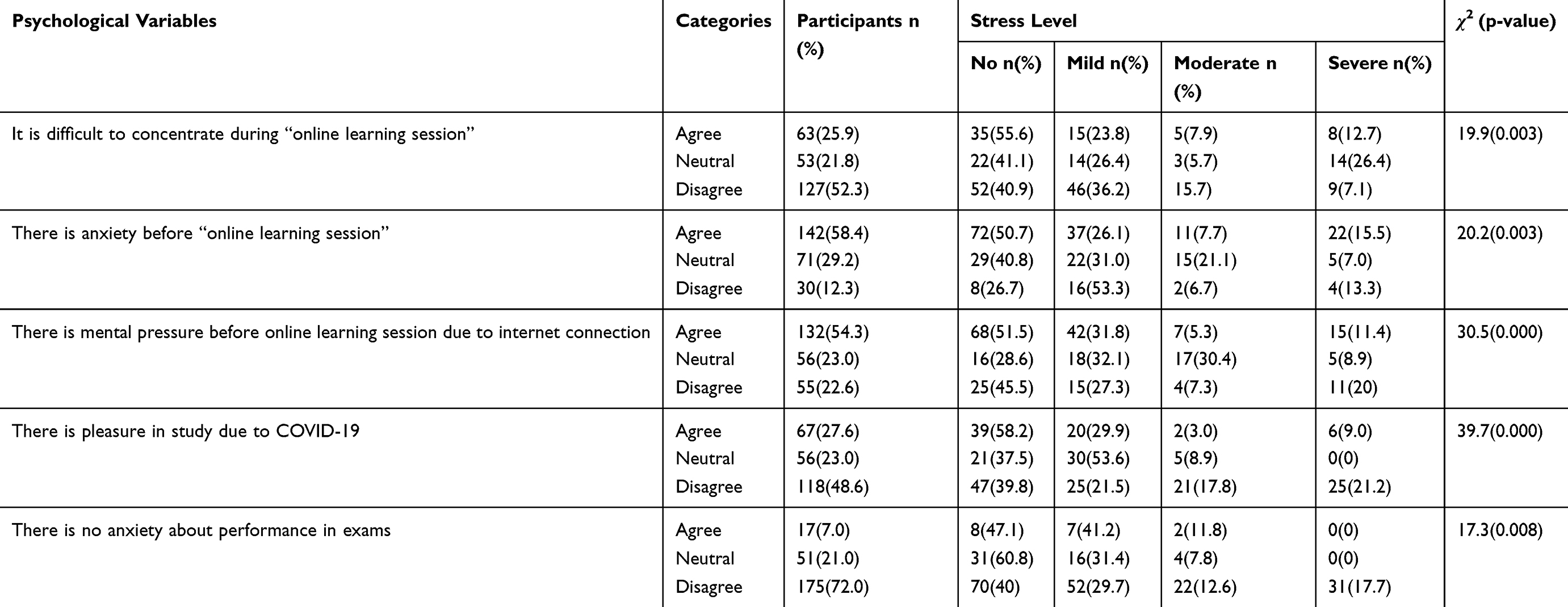 |
Table 5 Stress Level in Medical Students with Psychological Variables |
Discussion
We observe that several countries have been calling on their citizens to isolating at home or in isolation premises because of the coronavirus global pandemic in December 2019. Medical students in Saudi Arabia are living quarantined within their residential facilities during the latest COVID-19 pandemic, with the present lockdown situation. Prevalence of anxiety and depression among people who quarantined in south-western China during the COVID-19 outbreak.15
Owing to academic stress, medical students had a greater risk of physical and mental health issues than non-medical students. Our study found that the majority of the respondents have stress. Recently16 similar findings were observed and earlier17 reported as the majority of medical students (73%) were found to be stressed. The essence of their academic life makes medical students vulnerable to depression and anxiety. A pandemic situation may augment such negative feelings.18 Stress has numerous adverse effects on their mental, emotional, and physical health.19 High stress may have detrimental implications for cognitive function and learning abilities.13 Our previous study explored the stress of medical students during the quarantine time found that one-fourth of the participating medical students felt saddened during the quarantine period.20
The transition from pre-clinical to clinical year (ie, approaching into 3rd year) is a major turning point, leading to significant changeover in terms of students learning needs and teaching patterns, hence has a significant impact on medical students’ well-being. Such changes pose challenges, particularly important to those who are on the verge of transition from student to doctor, a transformation that has long been recognized as challenging.21 Our study also found that stress occurrence was at peak amongst the 3rd year students, as they exhibited significantly higher levels of severe stress. According to a study17, stress was found to be substantially greater in Second and Third MBBS students than in First MBBS students (p < 0.05). Students’ gender also represents a significant factor in the susceptibility to stress represented by medical and psychological symptoms. We found that female students have shown significantly higher levels of stress as compared to male students. There is a substantial variance of stress levels even when compared between females, from medical and non-medical courses. More female medical students (48.6%) reported being frequently stressed due to studies than non-medical female students.22
Learning using the internet and related tools for educational purposes, without geographical limitations is known as online learning or E-learning. Our study also established the connection between academic measures and the stress rates of medical students as “severe stress” was apparent for the students who considered online learning “during pandemic” as a burden. On the contrary, other studies found that although the level of acceptance towards E-learning is still low, yet, more than 55% of the students found it to be useful and time-saving,23 useful, and effective24 Furthermore, our study recorded that online learning yielded “time management problems” for the majority of the students, whereas, other studies found that “online platforms” provide support for those who have time management problems25 as well as technology can be used to shrink the total time students need to be in a class.26 As a current finding, 41.2% of students who responded as “neutral” about “online learning content is difficult to understand” have exhibited stress. Such an inference is likely as the respondents might not have a clear consideration of the emerging and fast-evolving situation.27 Regarding “online learning material not enough for study,” neutral respondents showed moderate to severe stress. The provision of sufficient material is very crucial, but this remained a challenge, as the pandemic was not expected, and the preparedness of the faculty was not achieved by many medical schools. As previously reported28 that effective online modality requires to engage all relevant faculty members and departments. This shall deal with the problem of inadequate learning material. Learning is difficult in the current pandemic situation, and students had perceived severe stress as they agreed that “regular class lecture is easy to understand”. This favoring of regular classes is not a new finding. Studies have reported that online healthcare development skills pose a new challenge for the learning of medical students.29,30 With an available wide range of support from the Saudi government to the academic sector, in general, and medical in particular, we see a huge transformation of academic resources to be based and augmented through E-learning in Saudi universities. This finding is consistent with the future perspective stated in AMEE guide 32, that the E-learning will be an increasingly global activity, providing opportunities to take your courses to the rest of the world and introduce the rest of the world to your courses, and can thus become a classroom anywhere.31
In this study, we also have explored the connection between various psychological variables and perceived stress. We found that the students who gained pleasure studying during COVID-19 (which was predominantly through an online platform) were found to be least stressed. Results of another study also found that the students felt it as enjoyable.24 One more important finding was about the item exploring for “There is anxiety before online learning session” where a mixed response was received, almost half of the respondents agreed and found not to have stressed. At the same time, another half also agreed with the item and was found to have a varying percentage of mild, moderate, or even severe stress. This is consistent with the results of studies18,32,33 reporting high test anxiety among students whereas another study21 reported medium test anxiety. This variation in the degree of test anxiety may relate to the complexity of certain topics, different items designed by different staff, and also the interest in the topic. Regarding another survey item, the majorities (72%) of our participants were of the opinion that there is anxiety about performance in exams, and among them (60%) had shown mild, moderate, and severe stress. Similarly,34 Tsegay et al reported that a significant percentage (52.30%) of medical students in Ethiopia had troubling test anxiety, and about 65% students had exam anxiety.35 Both studies also showed a strong link between test anxiety and the female gender. Studies carried out abroad have shown that the prevalence of depression and anxiety among medical students varied between 1.4–73.5%36 and 28–85%.37,38 Nevertheless, the anxiety dominance data from our study were lower than the global data. Furthermore, anxiety is frequently synonymous with mental illness and or considered as the apprehensive mental state,39 which is interpreted as a sign of weakness, and students may have underscored their symptoms. Our participants were from the nation’s leading medical institution; they might have been more resilient and better dealing with stress than other medical students.
Literature suggests that the coping strategies are significant, with their context reflected by social support, particularly within the family, and emotional, with the passions of medical students being the most important factor in the fight against stress. Each person relies, as in any challenging situation, on different coping mechanisms. While unprepared, it is always challenging for medical students to cope.40 The commonly used coping strategies amongst our responded students were “regular exercise,” “watching online movies & playing online games,” “online fun with family and friends,” religious activities,’ and “learning to live in COVID-19 situation and accept it.” As reported in our study, the most effective coping strategy to deal with severe stress was “religious activities” as practiced by the majority of the “severely stressed” students. Coping with religion includes cognitive, emotional, or behavioral responses to stress. Another study suggested that religious participation in response to life stressors could be particularly important for certain groups.41
Limitations and Implications
This study has limitation about the data collection setting as the subjects were from one region of Saudi Arabia.
In the future, we wish to have in-depth assessment of this same cohort and comparing it with multiple institutes in different countries. We would like to suggest, more exploratory events need to be carried out. This might highlight the difference (if found any) about COVID-19 pandemic, on students learning and stress, but in a different time phase.
Conclusions
Due to the potential implications of COVID-19, and for the future of medical education, the learning of medical students is under a close focus and is transformed. This study assessed the frequency and associated factors of stress among the medical students and shed some light on the effectiveness of their coping strategies during the COVID-19 outbreak in Riyadh, Saudi Arabia. The results exhibited that the predominance of stress is higher in females than males, and also, the respondents who regularly did religious meditation were at lower levels of stress.
Although every student might have a different personal story about how COVID-19 has influenced their education, there is no doubt that COVID-19’s influence will be felt at an extended level, which necessitates an appropriate preparedness plan.
Ethics Approval and Consent to Participate
The study protocol was approved by the institutional review board college of medicine, KSU. Before completing the questionnaires, all participants were provided with a written consent to participate in the study.
Acknowledgment
The authors extend their appreciation to the Deanship of Scientific Research at King Saud University for funding this work through research group no.RG-1441-411
Disclosure
The authors declare that they have no competing interests.
References
1. Meo SA, Al-Khlaiwi T, Usmani AM, Meo AS, Klonoff DC, Hoang TD. Biological and epidemiological trends in the prevalence and mortality due to outbreaks of novel coronavirus COVID-19. J King Saud Univ Sci. 2020;32(4):2495–2499. doi:10.1016/j.jksus.2020.04.004
2. Haleem A, Javaid M, Vaishya R, Deshmukh SG. Areas of academic research with the impact of COVID-19. Am J Emerg Med. 2020;38(7):1524–1526. doi:10.1016/j.ajem.2020.04.022
3. Usher K, Bhullar N, Jackson D. Life in the pandemic: social isolation and mental health. J Clin Nurs. 2020;29(15–16):2756–2757. doi:10.1111/jocn.15290
4. Abdulghani HM, Ponnamperuma AAAG, Mahmoud ES, Alfaris EA. Stress and its effects on medical students: a Cross-sectional Study at a College of Medicine in Saudi Arabia. J Health Popul Nutr. 2011;29(5):516–522. doi:10.3329/jhpn.v29i5.8906
5. Rose S. Medical student education in the time of COVID-19. JAMA. 2020;323(21):2131. doi:10.1001/jama.2020.5227
6. Ahmad T, Sattar K, Akram A. Medical professionalism videos on YouTube: content exploration and appraisal of user engagement. Saudi J Biol Sci. 2020;27(9):2287–2292. doi:10.1016/j.sjbs.2020.06.007
7. Ferrel MN, Ryan JJ. The impact of COVID-19 on medical education. Cureus. 2020;12(3):e7492.
8. Peterlini M, TibeÂrio LFLC, Saadeh A, Pereira JCR, Martins MA. Anxiety and depression in the first year of medical residency training. Med Educ. 2002;36:66–72. doi:10.1046/j.1365-2923.2002.01104.x
9. Dahlin M, Joneborg N, Runeson B. Stress and depression among medical students: a cross-sectional study. Med Educ. 2005;39(6):594–604. doi:10.1111/j.1365-2929.2005.02176.x
10. Folkman S. Stress: appraisal and coping. In: Gellman MD, Turner JR, editors. Encyclopedia of Behavioral Medicine. New York, NY: Springer; 2013:1913–1915.
11. APA. Coping Strategy. American Psychological Association. APA; 2020. Available from: https://dictionary.apa.org/coping-strategy.
12. Kessler RC, Andrews G, Colpe LJ, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002;32(6):959–976. doi:10.1017/S0033291702006074
13. Abdulghani HM, Irshad M, Al Zunitan MA, et al. Prevalence of stress in junior doctors during their internship training: a cross-sectional study of three Saudi medical colleges’ hospitals. Neuropsychiatr Dis Treat. 2014;10:1879–1886. doi:10.2147/NDT.S68039
14. Abdulghani HM. Stress and depression among medical students: a cross sectional study at a medical college in Saudi Arabia. Pak J Med Sci. 2008;24(1):6.
15. Lei L, Huang X, Zhang S, Yang J, Yang L, Xu M. Comparison of prevalence and associated factors of anxiety and depression among people affected by versus people unaffected by quarantine during the COVID-19 epidemic in Southwestern China. Med Sci Monit. 2020;26:e924609. doi:10.12659/MSM.924609
16. Francis B, Gill JS, Yit Han N, et al. Religious coping, religiosity, depression and anxiety among medical students in a multi-religious setting. Int J Environ Res Public Health. 2019;16:2.
17. Saravanan C, Wilks R. Medical students’ experience of and reaction to stress: the role of depression and anxiety. Sci World J. 2014;2014:737382. doi:10.1155/2014/737382
18. Husky MM, Kovess-Masfety V, Swendsen JD. Stress and anxiety among university students in France during Covid-19 mandatory confinement. Compr Psychiatry. 2020;102:152191. doi:10.1016/j.comppsych.2020.152191
19. Yusoff MSB, Jie TY, Esa AR. Stress, stressors and coping strategies among house officers in a Malaysian Hospital. ASEAN J Psychiatr. 2011;12(1):xx–xx.
20. Meo SA, Alomar AA, Abukhalaf AA, Sattar K, Klonoff DC. COVID-19 pandemic: impact of quarantine on medical students’ mental wellbeing and learning behaviors. Pak J Med Sci. 2020;36:S1–S6. doi:10.12669/pjms.36.COVID19-S4.2809
21. Teagle AR, George M, Gainsborough N, Haq I, Okorie M. Preparing medical students for clinical practice: easing the transition. Perspect Med Educ. 2017;6(4):277–280. doi:10.1007/s40037-017-0352-2
22. Al-Dabal BK, Koura MR, Rasheed P, Al-Sowielem L, Makki SM. A comparative study of perceived stress among female Medical and Non-Medical University students in Dammam, Saudi Arabia. Sultan Qaboos Univ Med J. 2010;10(2):231–240.
23. Khan MA, Ahmed SN, Aldarmahi A, Subahi A, Shirah B, Algahtani H. Perception of students about E-learning: a single-center experience from Saudi Arabia. Dr Sulaiman Al Habib Med J. 2020.
24. Costa A, Costa A, Olsson IAS. Students’ acceptance of e-learning approaches in laboratory animal science training. Lab Anim. 2019;23677219879170.
25. Wu XV, Chan YS, Tan KHS, Wang W. A systematic review of online learning programs for nurse preceptors. Nurse Educ Today. 2018;60:11–22. doi:10.1016/j.nedt.2017.09.010
26. Lauren M, Michael MW, Richard CA. Taxonomy to define courses that mix face-to-face and online learning. Learn Sci Faculty Publ. 2016;2. Available from: https://scholarworks.gsu.edu/ltd_facpub/2. Accessed October 24, 2020.
27. Khamees D, Brown CA, Arribas M, Murphey AC, Haas MRC, House JB. In crisis: medical students in the COVID-19 pandemic. AEM Educ Train. 2020;4(3):284–290. doi:10.1002/aet2.10450
28. Bediang G, Stoll B, Geissbuhler A, et al. Computer literacy and E-learning perception in Cameroon: the case of yaounde faculty of medicine and biomedical sciences. BMC Med Educ. 2013;13:57.
29. Triola MM, Friedman E, Cimino C, Geyer EM, Wiederhorn J, Mainiero C. Health information technology and the medical school curriculum. Am J Manag Care. 2010;16(12 Suppl HIT):Sp54–Sp56.
30. Thompson P. The digital natives as learners: technology use patterns and approaches to learning. Comput Educ. 2013;65:12–33. doi:10.1016/j.compedu.2012.12.022
31. Ellaway R, Masters K. AMEE guide 32: e-learning in medical education part 1: learning, teaching and assessment. Med Teach. 2008;30(5):455–473. doi:10.1080/01421590802108331
32. Kolagari S, Modanloo M, Rahmati R, Sabzi Z, Ataee AJ. The effect of computer-based tests on nursing students’ test anxiety: a Quasi-experimental Study. Acta Inform Med. 2018;26(2):115–118. doi:10.5455/aim.2018.26.115-118
33. Saheb Alzamani M, Zirak A. Students‘ learning and study strategies in Isfahan University of medical sciences and their relationship with test anxiety. Iran J Med Educ. 2011;11(1):58–68.
34. Tsegay L, Shumet S, Damene W, Gebreegziabhier G, Ayano G. Prevalence and determinants of test anxiety among medical students in Addis Ababa Ethiopia. BMC Med Educ. 2019;19(1):423. doi:10.1186/s12909-019-1859-5
35. Khoshhal KI, Khairy GA, Guraya SY, Guraya SS. Exam anxiety in the undergraduate medical students of Taibah University. Med Teach. 2017;39(sup1):S22–S26. doi:10.1080/0142159X.2016.1254749
36. Rotenstein LS, Ramos MA, Torre M, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and meta-analysis. JAMA. 2016;316(21):2214–2236. doi:10.1001/jama.2016.17324
37. Ahmed I, Banu H, Al-Fageer R, Al-Suwaidi R. Cognitive emotions: depression and anxiety in medical students and staff. J Crit Care. 2009;24(3):e1–e7. doi:10.1016/j.jcrc.2009.06.003
38. Brenneisen Mayer F, Souza Santos I, Silveira PSP, et al. Factors associated to depression and anxiety in medical students: a multicenter study. BMC Med Educ. 2016;16(1):282. doi:10.1186/s12909-016-0791-1
39. Crocq MA. The history of generalized anxiety disorder as a diagnostic category. Dialogues Clin Neurosci. 2017;19(2):107–116.
40. Murray E, Krahe C, Goodsman D. Are medical students in prehospital care at risk of moral injury? Emerg Med J. 2018;35(10):590–594. doi:10.1136/emermed-2017-207216
41. Ahrens CE, Abeling S, Ahmad S, Hinman J. Spirituality and well-being: the relationship between religious coping and recovery from sexual assault. J Interpers Violence. 2010;25(7):1242–1263. doi:10.1177/0886260509340533
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.