")
Back to Journals » Cancer Management and Research » Volume 11
Association of caveolin-1 protein expression with hepatocellular carcinoma: a meta-analysis and literature review
Authors Zhang Y, Fan W, Wu J, Dong J, Cui Z
Received 9 November 2018
Accepted for publication 7 March 2019
Published 31 May 2019 Volume 2019:11 Pages 5113—5122
DOI https://doi.org/10.2147/CMAR.S194033
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kenan Onel
Yan Zhang,1,* Wenjuan Fan,2,* Jiang Wu,1 Jinglong Dong,1 Zhanjun Cui3
1Department of Pathology, Huaihe Hospital, Henan University, Kaifeng 475000, People’s Republic of China; 2Medical Bioengineering Key Laboratory, Luohe Medical College, Luohe 462002, People’s Republic of China; 3School of Basic Medical Sciences, Henan University, Kaifeng 475004, People’s Republic of China
*These authors contributed equally to this work
Background: Aberrant expression of caveolin-1 (CAV-1) is involved in the pathogenesis of hepatocellular carcinoma (HCC); however, the results have been inconsistent due to the small size of sample in the individual study.
Methods: We performed a meta-analysis and evaluated the association of CAV-1 protein overexpression and clinicopathological significance by using Review Manager 5.2. Pooled ORs and HR with corresponding CIs were calculated.
Results: Nine studies were included in the meta-analysis with 810 HCC and 172 cirrhosis patients. CAV-1 protein overexpression was correlated with the risk of cirrhosis; OR was 3.25, p=0.01. Furthermore, the rate of CAV-1 protein overexpression was significantly higher in HCC with cirrhosis than HCC without cirrhosis, suggesting that the CAV-1 protein overexpression likely initiated carcinogenesis in liver with cirrhosis and subsequently contributed to the progression of HCC. In addition, CAV-1 protein overexpression was strongly associated with poor differentiated HCC and invasion; ORs were 2.61 and 2.71, respectively. CAV-1 protein overexpression was strongly correlated with poor overall survival in patients with HCC; HR was 0.4, p=0.03.
Conclusions: In summary, CAV-1 protein overexpression is at risk for liver cirrhosis and HCC derived from cirrhosis, and CAV-1 is also a promising prognostic predictor in HCC.
Keywords: hepatocellular carcinoma, caveolin-1, prognosis, diagnosis, overexpression
Background
Hepatocellular carcinoma (HCC) is the sixth most common malignancy worldwide and the third leading cause cancer-related mortality globally.1–3 Although many advances have been made in the diagnosis and management of HCC, the prognosis of patients with HCC remains poor due to late diagnosis, high recurrence, and metastasis.4,5 Therefore, it is critical to identify biomarkers for diagnosis and predict the prognosis of patients with HCC.
Caveolins are a family of scaffolding proteins that coat 50 to 100 nm plasma membrane invaginations known as caveolae.6 There are three isoforms in the caveolin family: caveolin-1,7 caveolin-2,8 and caveolin-3.8–13 Caveolin-1 is expressed in most cell types such as adipocytes, epithelial cells, and fibroblasts, where the protein is typically found co-expressed with caveolin-2.8,14 Caveolin-2 is incapable of forming caveolae alone. Caveolin-3 has similar structure and function as caveolin-1, but caveolin-3 is expressed in skeletal, cardiac, and smooth muscle cells.15 Recent evidence indicates that CAV-1 plays important roles in carcinogenesis by regulating cell proliferation, and its roles differ among distinct histological tumor types.16 The aberrant expression of CAV-1 is involved in the pathogenesis of a variety of cancers. CAV-1 can act as a tumor suppressor or initiator, depending on the tissue of origin.17 Overexpression of CAV-1 in hepatocarcinogenesis has been shown to protect HCC cells from apoptosis and enhance HCC cells’ migration and invasion abilities.18–21 However, the results were controversial due to the study’s small sample size. In the present study, we pooled nine studies and performed a meta-analysis to evaluate the relationship between the overexpression of CAV-1 and clinicopathological significance in HCC.
Methods
Search strategy and selection criteria
To identify relevant published literature, we searched PubMed (1966 ~ 2018), Web of Science (1945 ~ 2018), EMBASE (1980 ~ 2018), and Google scholar.
The following terms were used for searching: caveolin-1 or CAV-1 and HCC, liver cancer or HCC. We included studies that met the following criteria: 1) the association between CAV-1 overexpression and clinicopathological significance in HCC; 2) the association of CAV-1 overexpression and prognosis in HCC patients. Articles were excluded if: 1) the study utilized the same population or overlapping database, 2) the study is about the association between CAV-1 mRNA expression and clinicopathological significance, 3) the studies utilized cell lines, mice, or human grafts; 4) conference abstracts, case reports, reviews, letters, editorials, and expert opinion that contain insufficient data. The detailed information of nine relevant citations is summarized in Table 1.
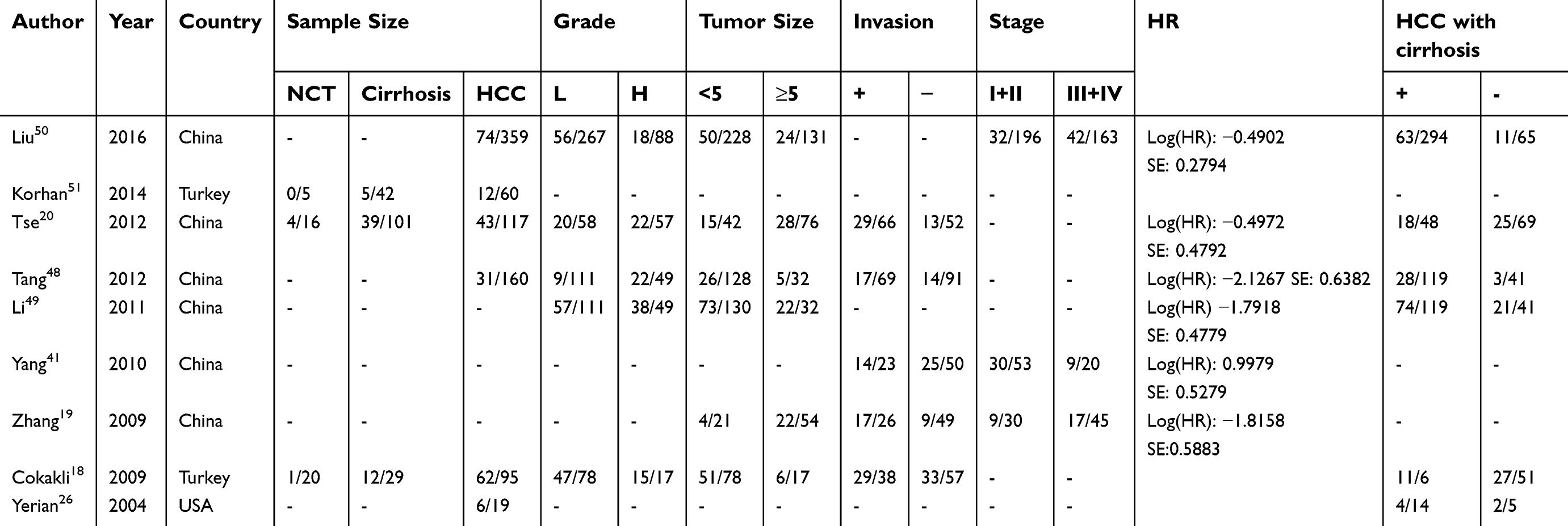 | Table 1 Main characteristics of included studies |
Data extraction and study assessment
Two reviewers extracted data from selected studies independently. Any discontent was discussed, and a consensus was reached for all issues. The following items were collected from each study: first author’s name, year of publication, number of patients, stage of HCC, grade of HCC, overall survival (Kaplan Meier survival curve), CAV-1 expression, the quality of selection, comparability, exposure, and outcomes for study participants.
Statistics analysis
ORs with 95% CIs were calculated by using a fixed- or random-effect model depending on heterogeneity (a fixed-effect model for I2<50%, a random-effect model for I2>50%). Further analysis was performed to compare CAV-1 overexpression among HCC versus normal tissue, cirrhosis versus normal liver, high grade of HCC versus low grade of HCC, and advanced stage HCC versus early stage HCC. Raw data were obtained from Kaplan–Meier survival curve, replotting on the log–log scale. This estimates the Cox regression coefficient. The output is the log HR and its standard error. HR with a 95% confidence interval was calculated for the association between CAV-1 expression and prognosis. All p-values were two-sided. Funnel plots were used to detect publication bias. All analysis was performed with Review Manager 5.2.
Results
Five hundred and twenty-five articles from database PubMed, Web of Science, Embase, and Google Scholar were screened, and nine articles were included in the meta-analysis (Figure 1). There were 810 HCC and 172 cirrhosis patients involved in the present study. Table 1 summarizes the clinicopathological characteristics of the patients from all of the included studies.
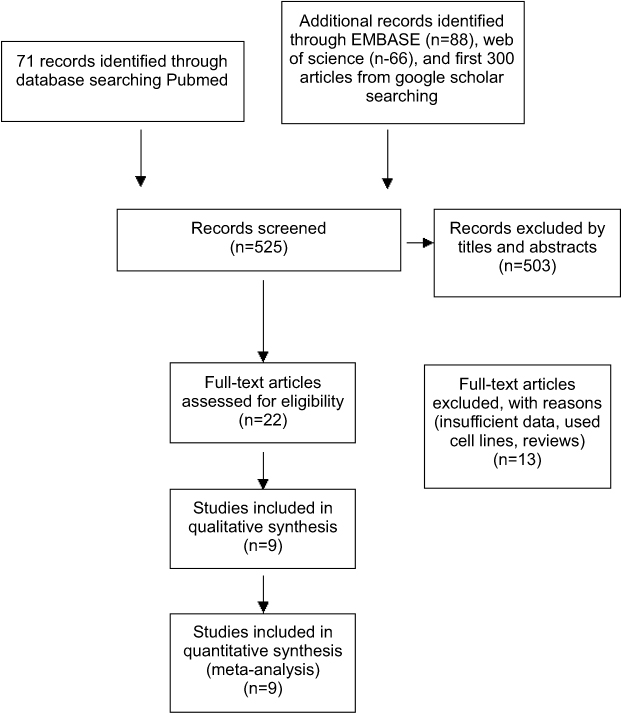 | Figure 1 Flowchart of study selection. |
Newcastle Ottawa Quality Assessment Scale (NOQAS) was utilized to assess the quality of all included studies. The scales allocate a maximum of nine points for the quality of selection, comparability, exposure, and outcomes for study participants, and a score ≥7 indicates a good quality. Of the studies, three scored eight points, five scored seven points, and one scored six points. The studies were of a relatively high quality (
The rate of CAV-1 protein overexpression in HCC was not significantly higher than in normal liver tissue; OR was 5.36 with 95% CI 0.65–44.49, z=1.56, p=0.12 (Figure 2). However, CAV-1 protein overexpression was more frequently observed in cirrhosis than in normal liver tissues; OR was 3.25 with 95% CI 1.26–8.42, z=2.43, p=0.01 (Figure 3A). Furthermore, the frequency of CAV-1 protein overexpression in HCC with cirrhosis was significantly higher than in HCC without cirrhosis (Figure 3B); OR was 1.48 with 95% CI 1.01–2.17, z=2.00, p=0.05. The results indicate that the overexpression of CAV-1 protein can potentially contribute to the development of cirrhosis and subsequently lead to liver carcinogenesis. Whereas the frequency of CAV-1 protein overexpression in HCC was not significantly higher than in cirrhotic liver, OR was 1.53 with 95% CI 0.75–3.12, z=1.17, p=0.24 (Figure 3C).
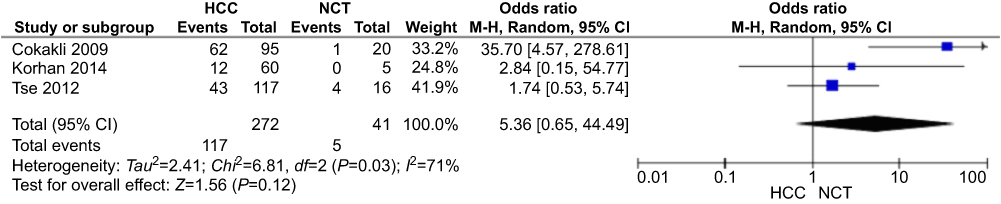 | Figure 2 The pooled OR from three studies including 272 HCC patients and 41 normal liver specimen. The studies included investigating the CAV-1 overexpression between HCC and normal liver tissues. 272 HCC patients and 41 normal liver specimen with the combined OR being 5.36 (95% CI=0.65–44.49, p =0.12) are shown.Abbrevitions: HCC, Hepatocellular carcinoma; NCT, Normal control tissue;OR, Odds ratio. |
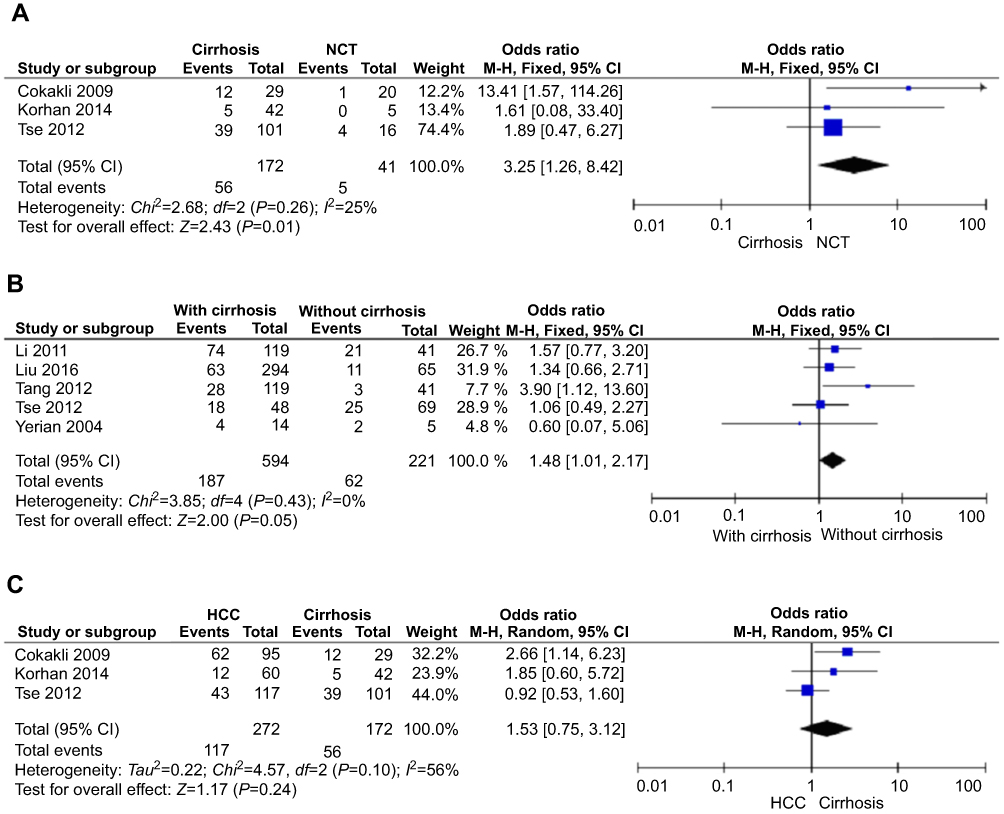 | Figure 3 The pooled OR from studies in normal liver, cirrhosis, and HCC. (A) The studies included investigating the CAV-1 overexpression between 172 patients with cirrhosis and 41 normal liver specimens. The combined OR was 3.25, 95% CI=1.26–8.42, p=0.01. (B) The pooled OR from 5 studies included 594 HCC with cirrhosis patients and 221 HCC without cirrhosis patients, OR=1.48 (95% CI=1.01–2.17, p=0.03). (C) The studies included investigating CAV-1 overexpression between 272 patients with HCC and 172 patients with cirrhosis. The combined OR was 1.53, 95% CI=0.75–3.12, p=0.24.Abbreviations: HCC, Hepatocellular carcinoma; NCT, Normal control tissue;OR: Odds ratio. |
Overexpression of CAV-1 protein was correlated with high grade of HCC; OR was 2.61 with 95% CI 1.09–6.26, z=2.16, p=0.03 (Figure 4). The rate of CAV-1 protein overexpression was higher in stage III–IV HCC than in stage I–II, but there was no significant difference; pooled OR was 1.43 with 95% CI 0.95–2.17, z=6.79, p=0.09 (Figure 5). Overexpression of CAV-1 protein was strongly associated with HCC invasion, and the rate of CAV-1 protein overexpression in HCC with metastasis was 2.71 times higher than in HCC without metastasis; 95% CI was 1.26–8.42, z=2.12, p=0.03 (Figure 6). No statistically significant correlation was found between the rate of CAV-1 protein overexpression and the size of tumor; OR was 0.97 with 95% CI 0.58–1.62, z=0.12, p=0.90 (Figure 7).
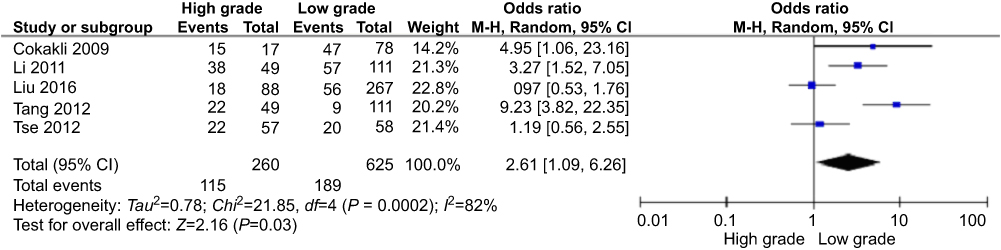 | Figure 4 The pooled OR from studies in high and low grade of HCC. Pooled results of CAV-1 overexpression in different grades of HCC. The OR was 2.61, 95% CI=1.09–6.26, p=0.03.Abbreviations: HCC, Hepatocellular carcinoma; ORs, Odds ratio; CI, Confidence interval. |
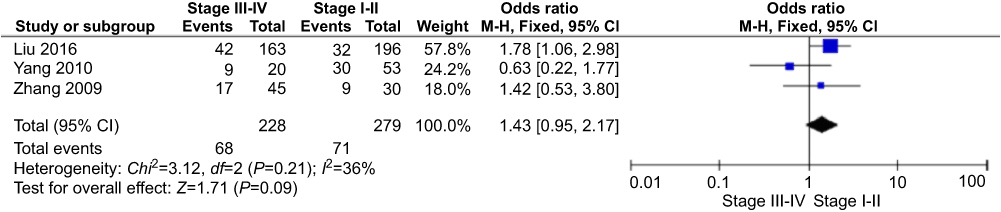 | Figure 5 The pooled ORs from studies in different stages of HCC. Pooled results of CAV-1 overexpression in different stages of HCC. The pooled OR was 1.43, 95% CI=0.95–2.17, p=0.09.Abbreviations: HCC, Hepatocellular carcinoma; ORs, Odds ratio; CI, Confidence interval. |
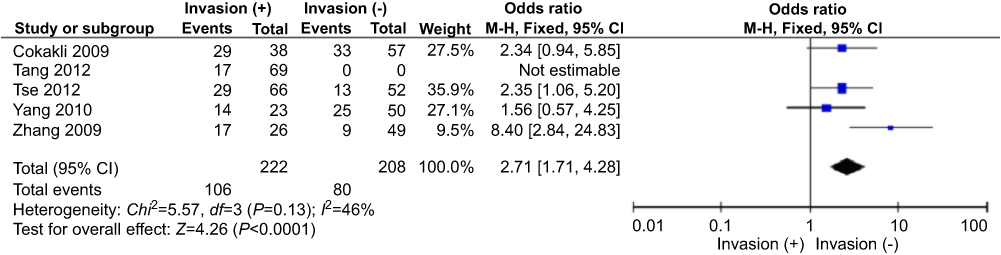 | Figure 6 The pooled ORs from studies in different status of invasion. The pooled OR was 2.71, 95% CI=1.71–4.28, p<0.0001.Abbreviations: ORs, Odds ratio; CI, Confidence interval. |
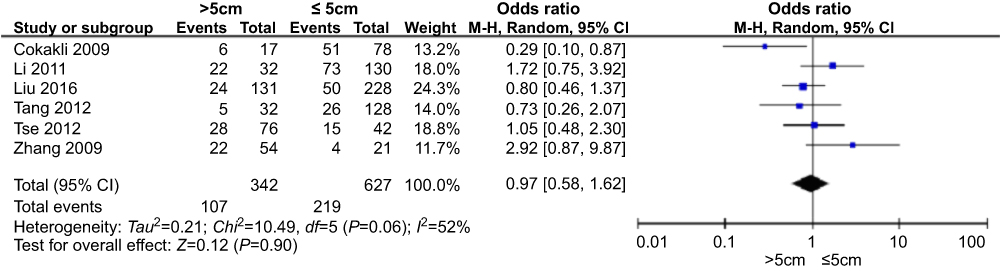 | Figure 7 The pooled ORs from studies in different sizes of HCC. The pooled OR was 0.97, 95% CI=0.58–1.62, p=0.90.Abbreviations: HCC, Hepatocellular carcinoma; ORs, Odds ratio, CI: Confidence interval. |
CAV-1 protein overexpression was also closely related to poor overall survival in patients with HCC; pooled HR was 0.40 with 95% CI 0.17–0.93, z=6.79, p=0.01 (Figure 8).
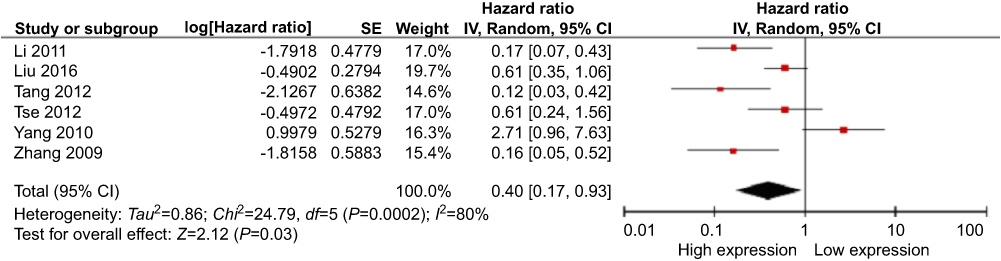 | Figure 8 The pooled HR from studies for the association of CAV-1 expression with overall survival of HCC patients. Five studies are eligible for evaluation of OS and CAV-1 overexpression with 719 HCC patients. The pooled HR for OS showed that CAV-1 overexpression was associated with worse survival in HCC, HR=0.40, 95% CI=0.17–0.93, Z=2.12, p=0.03.Abbreviations: HCC, Hepatocellular carcinoma, HR: Hazard ratio; CI, Confidence interval. |
A sensitivity analysis was performed by removing one study at a time, and the ORs were not significantly changed, indicating the stability of the present meta-analysis (S1, S2, S3, S4, S5, and S6). The funnel plots were largely symmetric (Figure 9), suggesting that publication biases do not exist in the meta-analysis of the relationship between CAV-1 overexpression and clinicopathological significance.
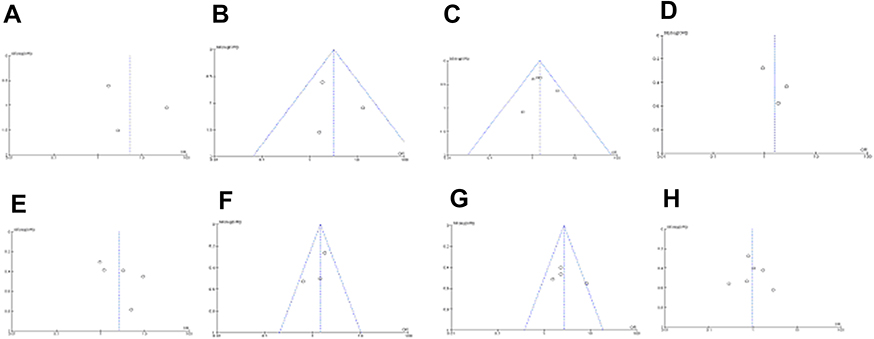 | Figure 9 Funnel plots of publication bias in the meta-analysis of CAV-1 overexpression and clinicopathological features. (A) CAV-1 overexpression in HCC vs normal liver tissues, (B) Cirrhosis vs normal liver tissues, (C) HCC with cirrhosis vs HCC without cirrhosis, (D) HCC vs cirrhosis, (E) different grades of HCC, (F) different stages of HCC, (G) different status of invasion in HCC, (H) different sizes of HCC.Abbreviations: HCC, Hepatocellular carcinoma. |
Discussion
Caveolins are a family of scaffolding proteins that coat 50 to 100 nm plasma membrane invaginations.6,22 Lipid rafts play an important role in signaling crosstalk via bringing different proteins into proximity and promote interactions among receptors and intracellular signaling proteins.23 Cirrhotic liver is related to macroregenerative and dysplastic nodules which are HCC precursor lesions. Our data indicate that the CAV-1 protein overexpression in cirrhosis is significantly higher than in normal liver, suggesting that CAV-1 protein overexpression plays an important role in cirrhosis which then acts as an initiator of carcinogenesis. However, the rate of CAV-1 protein overexpression in HCC is not significantly increased compared to the rate of CAV-1 protein overexpression in normal liver. This is in line with the report that CAV-1 was overexpressed in cirrhotic liver24,25 and was underexpressed in HCC.26 Additionally, we found that the frequency of CAV-1 protein overexpression in HCC with cirrhosis is higher than in HCC without cirrhosis. Our data indicate that CAV-1 overexpression likely plays an essential role in liver cirrhosis, subsequently contributing to the development of the HCC that derived from cirrhosis.
There are three isoforms in caveolin family: caveolin-1, caveolin-2, and caveolin-3. Engeman et al reported that the genes encoding caveolin-1 were co-localized at D7S522 locus on human chromosome 7q31.1, which was commonly deleted in cancers of breast,27,28 colon,29,30 kidney,31 prostate,32,33 ovary,34 lung,35 and head and neck.36 Therefore, they proposed that the caveolin-1 gene may be a tumor-suppressor gene candidate, its loss influences cancer cell survival and growth, and favor tumor progression,37–42 indicating loss of CAV1 regulation is a critical step in the acquisition of transformed phenotype.43 However, in later tumor stages, a re-expression of CAV1 seems to support invasion and metastasis.44,45 CAV1 overexpression may act as an initiator during the early stage and promote invasion at late stages. Whether or not CAV1 functions as a suppressor during the development of HCC, further investigation is needed to be carried out.
Lipid rafts play a pivotal role in signaling crosstalk through bringing different proteins into proximity and facilitating interactions between receptors and intracellular signaling proteins.23 CAV-1 function as scaffolding proteins that contribute to the assembly of a complex molecular platform, regulating endocytosis and transcytosis of molecules on the cell surface, and organizing signaling proteins that participate in cell proliferation, adhesion, and migration.17,46 Our data indicate that the overexpression of CAV-1 in HCC is linked to an unfavorable clinicopathological status, including a low degree of differentiation and metastasis. Previous studies demonstrated that the disruption of CAV-1 expression in invasive HCC cells suppresses in vitro migration and invasion,18,20,21 and also in vivo tumorigenicity and metastasis.20,21,47 Our results are in agreement with the previous reports. Present data showed that the rate of CAV-1 protein overexpression was higher in stage III–IV HCC than in stage I-II, but there was no significant difference due to small number of sample.
Previous studies showed controversial results of the relationship between CAV-1 protein overexpression and overall survival due to a small samples size.19,20,41,48–50 Yang et al reported that CAV-1 overexpression was correlated with better prognosis. However, our pooled HR from six studies indicate that the CAV-1 overexpression was significantly correlated with poor prognosis in patients with HCC. The high heterogeneity is due to the result from Yang et al’s study. Taken together, CAV-1 protein overexpression can potentially be a prognostic predictor for patients with HCC.
There are a few limitations. First, the criteria for the definition of overexpression of CAV-1 protein varied across the included studies. Second, confounders may exist when looking at the association of CAV-1 overexpression with overall survival since some of the included studies did not adjust for important risk factors such as age, tumor size, and HCC stage.
Conclusions
Our results suggest that the overexpression of CAV-1 protein is associated with the risk of cirrhosis which is an early event of carcinogenesis in the liver and is associated with HCC that was derived from cirrhosis. CAV-1 is correlated with an unfavorable clinicopathological status, including a low degree of differentiation and metastasis. The overexpression of CAV-1 protein is associated with poor overall survival, suggesting that the overexpression of CAV-1 protein predicts a poor prognosis in patients with HCC.
Abbreviation list
CAV-1, caveolin-1; HCC, hepatocellular carcinoma; NOQAS, Newcastle Ottawa Quality Assessment Scale; NCT, normal control tissue.
Availability of data and material
All data generated and analyzed during this study are included in this published article.
Author contributions
All authors contributed to data analysis, drafting or revising the articles, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. van Malenstein H, van Pelt J, Verslype C. Molecular classification of hepatocellular carcinoma anno 2011. Eur J Cancer. 2011;47(12):1789–1797. doi:10.1016/j.ejca.2011.04.027
2. Tang A, Hallouch O, Chernyak V, Kamaya A, Sirlin CB. Epidemiology of hepatocellular carcinoma: target population for surveillance and diagnosis. Abdom Radiol (NY). 2018;43(1):13–25. doi:10.1007/s00261-017-1209-1
3. Mitchell KA. Hepatocellular carcinoma: histologic considerations: pure, mixed, and motley. J Clin Gastroenterol. 2013;47(Suppl):S20–S26. doi:10.1097/MCG.0b013e318291f237
4. El-Serag HB, Marrero JA, Rudolph L, Reddy KR. Diagnosis and treatment of hepatocellular carcinoma. Gastroenterology. 2008;134(6):1752–1763. doi:10.1053/j.gastro.2008.02.090
5. Forner A, Bruix J. Locoregional treatment for hepatocellular carcinoma: from clinical exploration to robust clinical data, changing standards of care. Hepatology. 2008;47(1):5–7. doi:10.1002/hep.22152
6. Ketteler J, Klein D. Caveolin-1, cancer and therapy resistance. Int J Cancer. 2018;143:2092–2104. doi:10.1002/ijc.v143.9
7. Glenney JR
8. Scherer PE, Lewis RY, Volonte D, et al. Cell-type and tissue-specific expression of caveolin-2. Caveolins 1 and 2 co-localize and form a stable hetero-oligomeric complex in vivo. J Biol Chem. 1997;272(46):29337–29346.
9. Parton RG. Caveolae and caveolins. Curr Opin Cell Biol. 1996;8(4):542–548.
10. Scherer PE, Lisanti MP. Association of phosphofructokinase-M with caveolin-3 in differentiated skeletal myotubes. Dynamic regulation by extracellular glucose and intracellular metabolites. J Biol Chem. 1997;272(33):20698–20705.
11. Okamoto T, Schlegel A, Scherer PE, Lisanti MP. Caveolins, a family of scaffolding proteins for organizing “preassembled signaling complexes” at the plasma membrane. J Biol Chem. 1998;273(10):5419–5422.
12. Tang Z, Okamoto T, Boontrakulpoontawee P, Katada T, Otsuka AJ, Lisanti MP. Identification, sequence, and expression of an invertebrate caveolin gene family from the nematode Caenorhabditis elegans. Implications for the molecular evolution of mammalian caveolin genes. J Biol Chem. 1997;272(4):2437–2445.
13. Tang Z, Scherer PE, Okamoto T, et al. Molecular cloning of caveolin-3, a novel member of the caveolin gene family expressed predominantly in muscle. J Biol Chem. 1996;271(4):2255–2261.
14. Scherer PE, Okamoto T, Chun M, Nishimoto I, Lodish HF, Lisanti MP. Identification, sequence, and expression of caveolin-2 defines a caveolin gene family. Proc Natl Acad Sci USA. 1996;93(1):131–135.
15. Filippini A, Sica G, D’Alessio A. The caveolar membrane system in endothelium: from cell signaling to vascular pathology. J Cell Biochem. 2018;119(7):5060–5071. doi:10.1002/jcb.26793
16. Fu P, Chen F, Pan Q, et al. The different functions and clinical significances of caveolin-1 in human adenocarcinoma and squamous cell carcinoma. Onco Targets Ther. 2017;10:819–835. doi:10.2147/OTT.S123912
17. Williams TM, Lisanti MP. Caveolin-1 in oncogenic transformation, cancer, and metastasis. Am J Physiol Cell Physiol. 2005;288(3):C494–C506. doi:10.1152/ajpcell.00458.2004
18. Cokakli M, Erdal E, Nart D, et al. Differential expression of Caveolin-1 in hepatocellular carcinoma: correlation with differentiation state, motility and invasion. BMC Cancer. 2009;9:65. doi:10.1186/1471-2407-9-65
19. Zhang ZB, Cai L, Zheng SG, Xiong Y, Dong JH. Overexpression of caveolin-1 in hepatocellular carcinoma with metastasis and worse prognosis: correlation with vascular endothelial growth factor, microvessel density and unpaired artery. Pathol Oncol Res. 2009;15(3):495–502. doi:10.1007/s12253-008-9144-7
20. Tse EY, Ko FC, Tung EK, et al. Caveolin-1 overexpression is associated with hepatocellular carcinoma tumourigenesis and metastasis. J Pathol. 2012;226(4):645–653. doi:10.1002/path.3957
21. Wang S, Jia L, Zhou H, Shi W, Zhang J. Knockdown of caveolin-1 by siRNA inhibits the transformation of mouse hepatoma H22 cells in vitro and in vivo. Oligonucleotides. 2009;19(1):81–88. doi:10.1089/oli.2008.0166
22. Razani B, Woodman SE, Lisanti MP. Caveolae: from cell biology to animal physiology. Pharmacol Rev. 2002;54(3):431–467.
23. Coleman DT, Bigelow R, Cardelli JA. Inhibition of fatty acid synthase by luteolin post-transcriptionally down-regulates c-Met expression independent of proteosomal/lysosomal degradation. Mol Cancer Ther. 2009;8(1):214–224. doi:10.1158/1535-7163.MCT-08-0722
24. Goh BJ, Tan BT, Hon WM, Lee KH, Khoo HE. Nitric oxide synthase and heme oxygenase expressions in human liver cirrhosis. World J Gastroenterol. 2006;12(4):588–594.
25. Mookerjee RP, Wiesenthal A, Icking A, et al. Increased gene and protein expression of the novel eNOS regulatory protein NOSTRIN and a variant in alcoholic hepatitis. Gastroenterology. 2007;132(7):2533–2541. doi:10.1053/j.gastro.2006.12.035
26. Yerian LM, Anders RA, Tretiakova M, Hart J. Caveolin and thrombospondin expression during hepatocellular carcinogenesis. Am J Surg Pathol. 2004;28(3):357–364.
27. Chiu WT, Lee HT, Huang FJ, et al. Caveolin-1 upregulation mediates suppression of primary breast tumor growth and brain metastases by stat3 inhibition. Cancer Res. 2011;71(14):4932–4943. doi:10.1158/0008-5472.CAN-10-4249
28. Bonuccelli G, Casimiro MC, Sotgia F, et al. Caveolin-1 (P132L), a common breast cancer mutation, confers mammary cell invasiveness and defines a novel stem cell/metastasis-associated gene signature. Am J Pathol. 2009;174(5):1650–1662. doi:10.2353/ajpath.2009.080648
29. Goetz JG, Minguet S, Navarro-Lerida I, et al. Biomechanical remodeling of the microenvironment by stromal caveolin-1 favors tumor invasion and metastasis. Cell. 2011;146(1):148–163. doi:10.1016/j.cell.2011.05.040
30. Bender FC, Reymond MA, Bron C, Quest AF. Caveolin-1 levels are down-regulated in human colon tumors, and ectopic expression of caveolin-1 in colon carcinoma cell lines reduces cell tumorigenicity. Cancer Res. 2000;60(20):5870–5878.
31. Ruan H, Li X, Yang H, et al. Enhanced expression of caveolin-1 possesses diagnostic and prognostic value and promotes cell migration, invasion and sunitinib resistance in the clear cell renal cell carcinoma. Exp Cell Res. 2017;358(2):269–278. doi:10.1016/j.yexcr.2017.07.004
32. Ayala G, Morello M, Frolov A, et al. Loss of caveolin-1 in prostate cancer stroma correlates with reduced relapse-free survival and is functionally relevant to tumour progression. J Pathol. 2013;231(1):77–87. doi:10.1002/path.4217
33. Klein D, Schmitz T, Verhelst V, et al. Endothelial Caveolin-1 regulates the radiation response of epithelial prostate tumors. Oncogenesis. 2015;4:e148. doi:10.1038/oncsis.2015.9
34. Sayhan S, Diniz G, Karadeniz T, et al. Expression of caveolin-1 in peritumoral stroma is associated with histological grade in ovarian serous tumors. Ginekol Pol. 2015;86(6):424–428.
35. Duregon E, Senetta R, Bertero L, et al. Caveolin 1 expression favors tumor growth and is associated with poor survival in primary lung adenocarcinomas. Tumour Biol. 2017;39(2):1010428317694311. doi:10.1177/1010428317694311
36. Vered M, Lehtonen M, Hotakainen L, et al. Caveolin-1 accumulation in the tongue cancer tumor microenvironment is significantly associated with poor prognosis: an in-vivo and in-vitro study. BMC Cancer. 2015;15:25. doi:10.1186/s12885-015-1584-3
37. Engelman JA, Zhang XL, Lisanti MP. Genes encoding human caveolin-1 and −2 are co-localized to the D7S522 locus (7q31.1), a known fragile site (FRA7G) that is frequently deleted in human cancers. FEBS Lett. 1998;436(3):403–410.
38. Diaz-Valdivia N, Bravo D, Huerta H, et al. Enhanced caveolin-1 expression increases migration, anchorage-independent growth and invasion of endometrial adenocarcinoma cells. BMC Cancer. 2015;15:463. doi:10.1186/s12885-015-1584-3
39. Yang G, Timme TL, Frolov A, Wheeler TM, Thompson TC. Combined c-Myc and caveolin-1 expression in human prostate carcinoma predicts prostate carcinoma progression. Cancer. 2005;103(6):1186–1194. doi:10.1002/cncr.20905
40. Sunaga N, Miyajima K, Suzuki M, et al. Different roles for caveolin-1 in the development of non-small cell lung cancer versus small cell lung cancer. Cancer Res. 2004;64(12):4277–4285. doi:10.1158/0008-5472.CAN-03-3941
41. Yang SF, Yang JY, Huang CH, et al. Increased caveolin-1 expression associated with prolonged overall survival rate in hepatocellular carcinoma. Pathology. 2010;42(5):438–445. doi:10.3109/00313025.2010.494293
42. Wu KN, Queenan M, Brody JR, et al. Loss of stromal caveolin-1 expression in malignant melanoma metastases predicts poor survival. Cell Cycle. 2011;10(24):4250–4255. doi:10.4161/cc.10.24.18551
43. Senetta R, Stella G, Pozzi E, Sturli N, Massi D, Cassoni P. Caveolin-1 as a promoter of tumour spreading: when, how, where and why. J Cell Mol Med. 2013;17(3):325–336. doi:10.1111/jcmm.12030
44. Ando T, Ishiguro H, Kimura M, et al. The overexpression of caveolin-1 and caveolin-2 correlates with a poor prognosis and tumor progression in esophageal squamous cell carcinoma. Oncol Rep. 2007;18(3):601–609.
45. Ho CC, Kuo SH, Huang PH, Huang HY, Yang CH, Yang PC. Caveolin-1 expression is significantly associated with drug resistance and poor prognosis in advanced non-small cell lung cancer patients treated with gemcitabine-based chemotherapy. Lung Cancer. 2008;59(1):105–110. doi:10.1016/j.lungcan.2007.07.024
46. Pike LJ. Growth factor receptors, lipid rafts and caveolae: an evolving story. Biochim Biophys Acta. 2005;1746(3):260–273. doi:10.1016/j.bbamcr.2005.05.005
47. Zhou H, Jia L, Wang S, et al. Divergent expression and roles for caveolin-1 in mouse hepatocarcinoma cell lines with varying invasive ability. Biochem Biophys Res Commun. 2006;345(1):486–494. doi:10.1016/j.bbrc.2006.03.246
48. Tang Y, Zeng X, He F, Liao Y, Qian N, Toi M. Caveolin-1 is related to invasion, survival, and poor prognosis in hepatocellular cancer. Med Oncol. 2012;29(2):977–984. doi:10.1007/s12032-011-9900-5
49. Li LLYTYQ N, Zhang H, Li W, Tao K. Clinical significance of caveolin-1 in hepatocellular carcinoma. Mod Oncol. 2011;19(11).
50. Liu WR, Jin L, Tian MX, et al. Caveolin-1 promotes tumor growth and metastasis via autophagy inhibition in hepatocellular carcinoma. Clin Res Hepatol Gastroenterol. 2016;40(2):169–178. doi:10.1016/j.clinre.2015.06.017
51. Korhan P, Erdal E, Kandemis E, et al. Reciprocal activating crosstalk between c-Met and caveolin 1 promotes invasive phenotype in hepatocellular carcinoma. PLoS One. 2014;9(8):e105278. doi:10.1371/journal.pone.0105278
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.