")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Association of Apolipoprotein E Gene Polymorphism with Ischemic Stroke in Coronary Heart Disease Patients Treated with Medium-intensity Statins
Authors Lv P, Zheng Y, Huang J , Ke J, Zhang H
Received 29 May 2020
Accepted for publication 24 August 2020
Published 23 October 2020 Volume 2020:16 Pages 2459—2466
DOI https://doi.org/10.2147/NDT.S265194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Yuping Ning
Ping Lv,* Yaofu Zheng,* Jun Huang, Junsong Ke, Hongyu Zhang
Department of Cardiology, The First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi 330006, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jun Huang
Department of Cardiology, The First Affiliated Hospital of Nanchang University, 17 Yongwaizheng St, Nanchang, Jiangxi 330006, People’s Republic of China
Tel +86-138 70057352
Fax +86-791-88694579
Email [email protected]
Objective: To study the association of apolipoprotein E(APOE) gene polymorphism with ischemic stroke (IS) in coronary heart disease (CHD) patients treated with medium-intensity statins.
Methods: The retrospective study was performed on 662 samples including 169 CHD subjects complicated with IS, 296 subjects with CHD, and 197 control subjects. The APOE gene was obtained from case files. Univariable and multivariable logistic regression analyses were utilized to recognize the possible risks of CHD and IS.
Results: The frequency of ϵ3-ϵ4 genotype was increased in the CHD group (p=0.013) and CHD-IS group (p=0.001), the frequency of ϵ4 allele was also increased in the CHD group (p=0.047) and the CHD-IS group (p=0.009) compared with control group. ϵ3-ϵ4 genotype was the independent risk for CHD and CHD-IS after adjusting for traditional risk factors with adjusted odds ratio (AOR) 2.210, 95%CI: 1.263– 3.867, p=0.005) and (AOR 2.794, 95%CI: 1.539– 5.072, p=0.002). The ϵ4 allele was also significantly associated with CHD (AOR 2.126, 95%CI: 1.265– 3.575,=0.004) and CHD-IS (AOR 2.740, 95%CI: 1.569– 4.784, p=0.001).
Conclusion: These results demonstrated that ϵ4 allele influenced the development of CHD with or without IS, especially for the genotype of ϵ3-ϵ4. CHD patients carrying the ϵ3-ϵ4 genotype and the ϵ4 allele were significantly associated with the incidence of IS, even if medium-intensity statins had been used.
Keywords: apolipoprotein E, polymorphism, coronary heart disease, ischemic stroke, statins
Introduction
Coronary heart disease (CHD) and stroke cause immense health and economic burdens.1 According to the research conducted by the China National Stroke Registry, ischemic stroke (IS) is a predominant stroke subtype, accounting for 66.7%.2 CHD and IS are both based on atherosclerosis caused by lipid metabolism disorders. As one of the complex heterogeneous diseases of multiple etiologies and major clinical manifestations, IS is not only associated with various traditional risk factors, but also influenced by the gene polymorphism.
Apolipoprotein E (APOE) gene is a common candidate gene which exerts an important role in lipid metabolism. It includes three alleles (ε2, ε3, and ε4) which express three isoforms of proteins (E2, E3, and E4). These alleles of APOE gene constitute six genetypes (ε2-ε2, ε2-ε3, ε2-ε4, ε3-ε3, ε3-ε4, and ε4-ε4),3 among which the most common genotype is ε3-ε3, and ε3 is the most predominant allele in most races.4–6 Allele ε2 is associated with higher level triglyceride (TG), lower level low density lipoprotein cholesterol (LDL-C) in plasma and lower risk of coronary artery disease when compared with ε3 allele. Allele ε4 is associated with higher plasma levels of LDL-C, total cholesterol (TC), apolipoprotein B and increased risk of coronary artery disease compared with ε3 allele.7
Statins are one of the most commonly prescribed medicines worldwide which are utilized to prevent and stabilize atherosclerotic plaque. Statin therapy could also reduce the risk of IS in CHD patients.8–10 In the current clinical practice in China, medium-intensity statins are widely used in the routine treatment of CHD. Whether the routine dose of statins could reduce IS risk in CHD patients was still poorly documented. There was no data demonstrating the relationship between APOE gene polymorphism and IS in CHD patients treated with medium-intensity statins. In this study, we aimed to investigate the association of APOE gene polymorphism with IS in CHD patients treated with medium-intensity statins, of whom the difference on plasma lipid levels between ε4 carriers and ε3-ε3 genotype.
Methods
Inclusion Criteria and Exclusion Criteria of the Study Population
The study complied with the Declaration of Helsinki for investigation in human beings and was approved by the Ethics Committee of The First Affiliated Hospital of Nanchang University. All patient data complied with relevant data protection and privacy regulations.
The single center retrospective study consisted of 662 subjects, all of whom were admitted to the First Affiliated Hospital of Nanchang University between September 2013 and August 2017. All subjects were divided into control group (n=197), CHD group (n=296) and CHD-IS group (n=169). The control group was collected from healthy individuals who visited the Department of Physical Examination Center. All control patients declared that they had no history of CHD and IS, and this was confirmed by electrocardiogram (ECG) and brain computerized tomography (CT). CHD group patients were checked by coronary angiography for at least 50% lumen obstruction in a major coronary artery or one of their branches. CHD-IS group patients included CHD patients complicated with IS, which were diagnosed according to the criteria amended by the Chinese Medical Association in National Cerebrovascular Disease Conference in 2015, with confirmation by brain CT or magnetic resonance imaging (MRI). In the CHD-IS group, IS happened in CHD patients who insisted on taking medium-intensity statins since diagnosed as CHD. Telephone follow-up and checking out prescriptions for outpatients were used to determine if CHD patients were taking statins until the occurrence of IS, and CHD patients who took medium-intensity statins for less than one month when diagnosed as IS were excluded. Medium-intensity statins included atorvastatin (20 mg), rosuvastatin (10 mg), or pitavastatin (2 mg). Other CHD medicines had no special requirements. Exclusion criteria included heart valve disease, atrial fibrillation, hemorrhagic stroke or ischemic stroke before coronary heart disease, neurodegenerative disorders, hepatic and renal diseases, and any form of endocrine or metabolic diseases. Information were obtained from these case files which included age, gender, obesity, discharge diagnosis, history of smoking, dyslipidemia, diabetic mellitus, hypertension, homocysteine (Hcy), APOE genotypes, vital signs, laboratory examination, ECG, head imaging examination (CT or MRI), cardiac ultrasound, coronary arteriography, complications, and the dose of statins.
Definitions
Obesity was defined as body mass index (BMI) ≥25 kg/m2. Cigarette smokers meant someone who had smoked continuously more than one year even if they were no longer a smoker. Hypertension was defined as blood pressure ≥140/90 mmHg or the use of antihypertensive medications. Dyslipidemia were defined as when one had levels of TG ≥1.70 mmol/L, TC ≥5.72 mmol/L, LDL-C ≥3.12 mmol/L, high-density lipoprotein cholesterol (HDL-C) ≤1.0 mmol/L. Diabetic mellitus was defined as fasting plasma glucose ≥6.1 mmol/L and postprandial glucose ≥11.1 mmol/L, and/or diagnosed diabetes mellitus receiving treatment.
Statistical Analysis
All analyses were conducted using the statistical software SPSS statistics 23 (IBM Corporation, Armonk, NY, USA), and followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. Continuous variables were expressed as mean ±SD or median (with IQR), and categorical variables as numbers and percentages. One-way ANOVA followed by posthoc Bonferroni multiple comparison test was used to evaluate the mean difference of the data among the three groups (control, CHD, and CHD-IS). The chi-squared tests and Fisher-F were used for categorical variables. The difference of allele and genotype among the three groups and deviations from Hardy–Weinberg equilibrium were tested by chi-squared tests or Fisher-F. The univariable logistic regression analysis with unadjusted OR and 95%CI were used to explore the association between APOE polymorphism and diseases. Multivariable binary logistic regression analysis with adjusted OR and 95%CI, which followed adjusting for age, sex, smoking history, SBP and Hcy, were used to determine the independent risk factor for development of IS after CHD. A value of p<0.05 was considered statistically significant.
Results
The Baseline Characteristics of the Population in This Study
The demographic and clinical data were shown in Table 1. There was a significant increase in age of the CHD-IS and CHD groups compared with the control group (p=0.009). The proportion of males in the CHD-IS and CHD groups was increased when compared with the control group (p<0.001). Other clinical parameters such as systolic blood pressure (SBP) and Hcy were significantly higher in both CHD-IS and CHD groups when compared with the control group (p<0.001 and p=0.020, respectively). CHD-IS group and CHD group had significantly higher frequencies of smoking and dyslipidemia compared with control group (p=0.003 and p<0.001, respectively). Despite of taking medium-intensity statins, the levels of TC and LDL-C in the CHD-IS and CHD groups still showed significant increase when compared with the control group (p=0.015 and p<0.001, respectively). The lower levels of TC and LDL-C were observed in the CHD-IS group compared with CHD group, but no significant difference was shown (p=0. 241 and p=0.139, respectively). The levels of TG and HDL-C showed no significant difference among three groups (p=0. 211 and p=0.339, respectively).
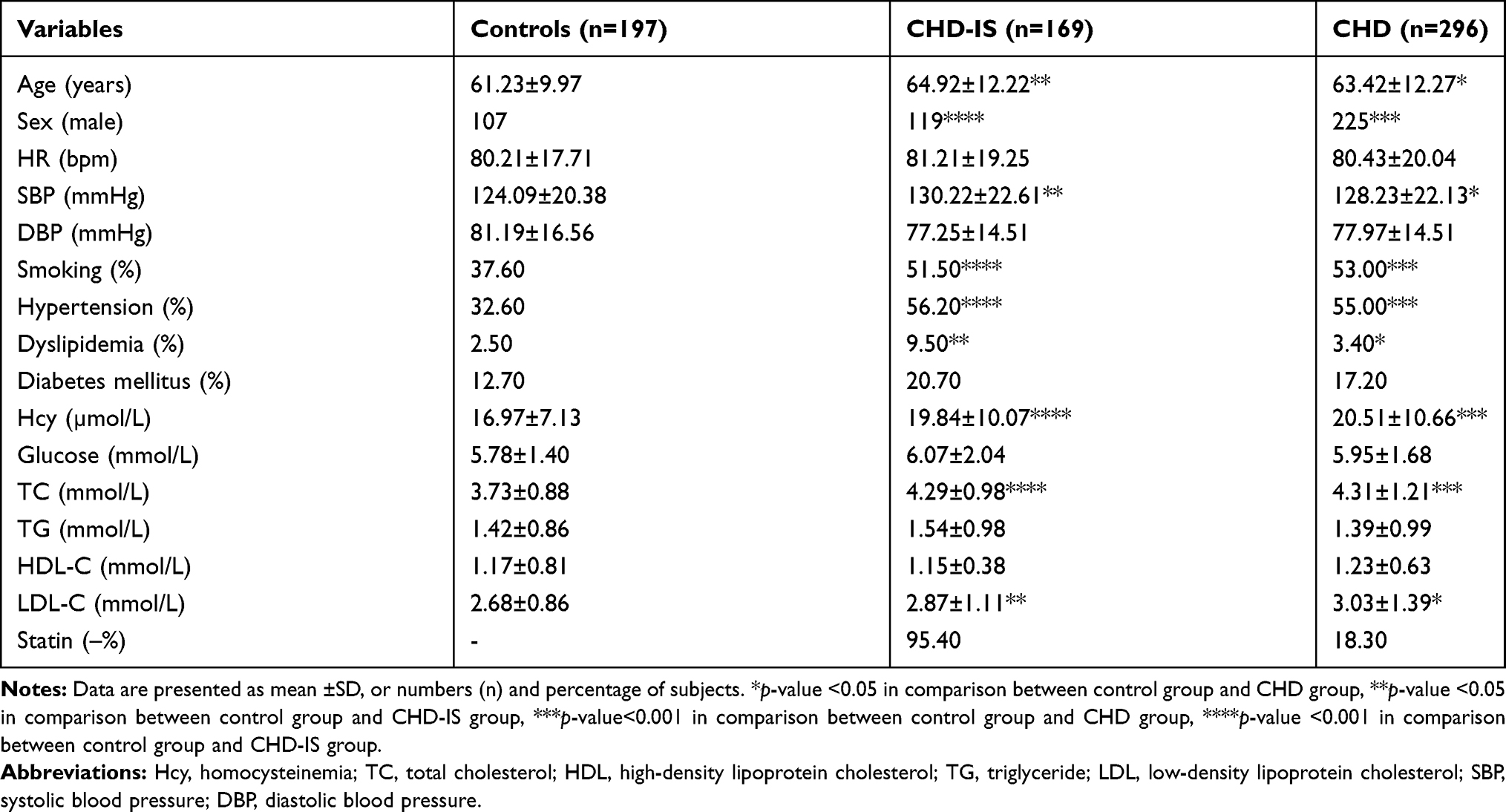 |
Table 1 Demographic and Clinical Data of Different Groups |
The Frequencies of APOE Genotype and ε3, ε4, ε2 Alleles
The genotype distribution of control, CHD, and CHD-IS groups were in Hardy–Weinberg equilibrium (Table 2). The frequency of ε3-ε3 genotype was significantly decreased in the CHD-IS and CHD groups (p<0.001 and p=0.029, respectively) compared with the control group, while ε3 allele was only observed to have a lower prevalence in the CHD-IS group (p=0.002). The frequency of ε3-ε4 genotype was significantly increased in the CHD-IS and CHD groups (p=0.001 and p=0.013, respectively), and the allele of ε4 had a higher prevalence in the CHD-IS and CHD groups (p=0.002 and p=0.014, respectively). In addition, the frequencies of ε2-ε3 genotype and ε2 allele only had an increased tendency in the CHD-IS group compared with the control group, but no significant difference was observed (p=0.210 and p=0.415, respectively). The frequencies of ε2-ε2, ε4-ε4, and ε2-ε4 genotypes had no statistically significant differences observed among three groups (Table 3).
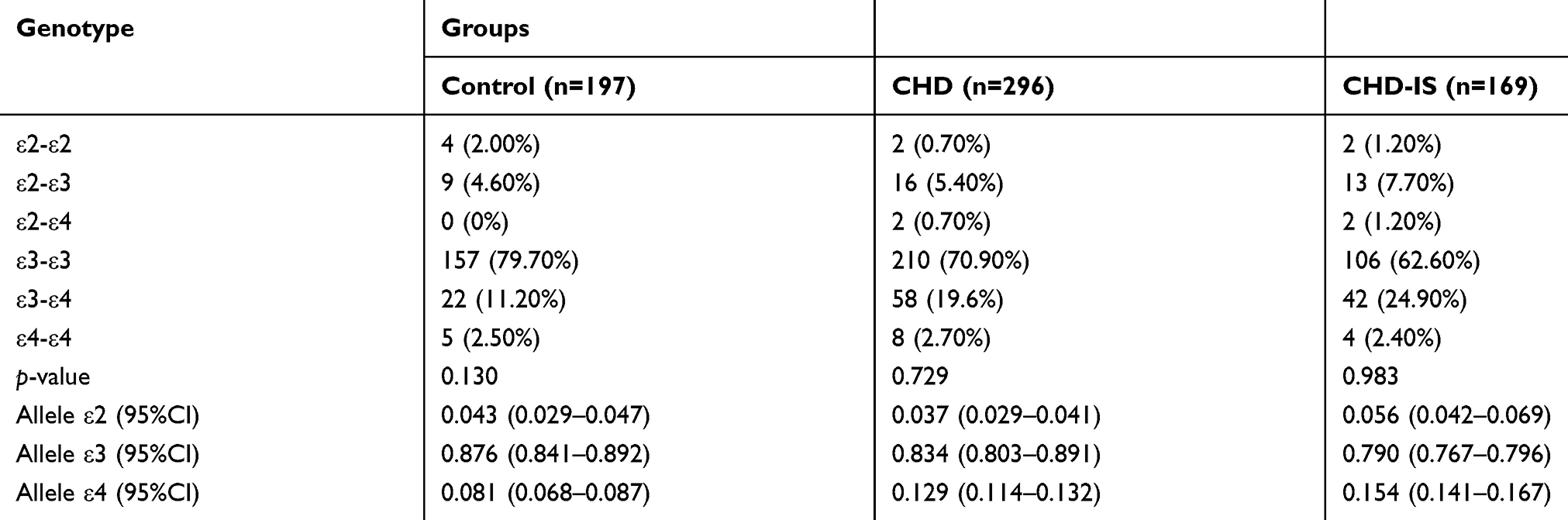 |
Table 2 Genotype and Allele Frequencies Distribution of APOE Gene Polymorphism in the CHD and CHD-IS Groups Compared with the Control Group |
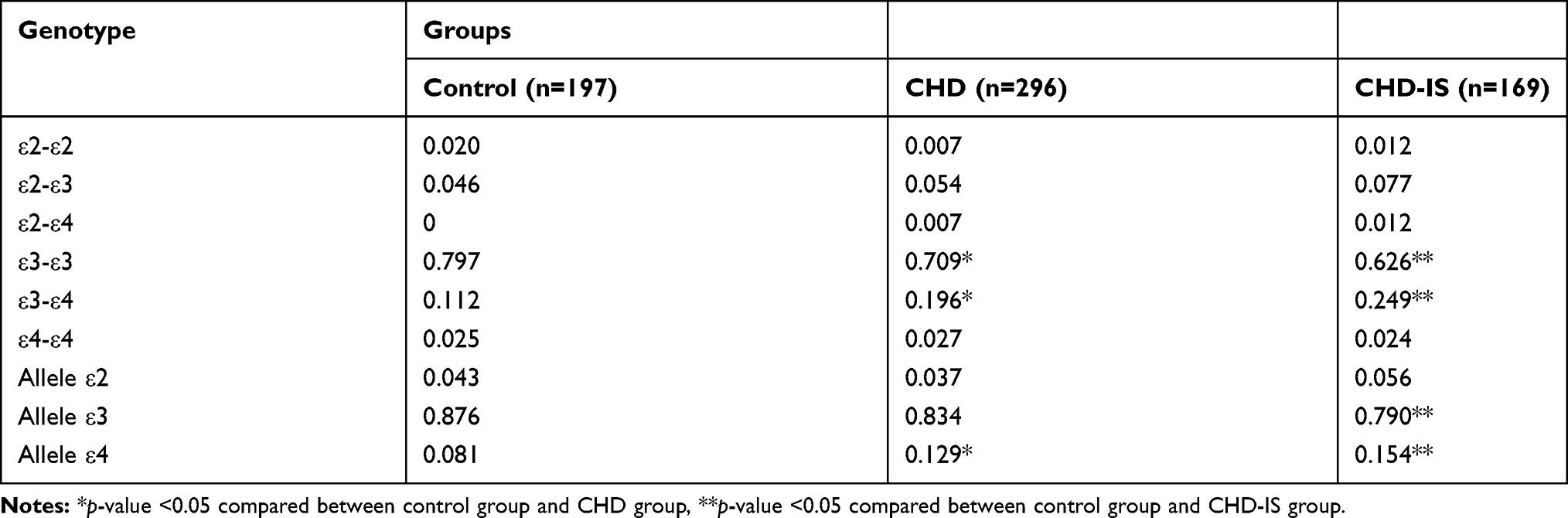 |
Table 3 Genotype and Allele Frequencies Distribution of APOE Gene Polymorphism in the CHD Group and CHD-IS Group Compared with the Control Group |
The Association Between APOE Gene Polymorphism and the Development of CHD and IS
The ε4 allele was associated with low lipid clearance property. Therefore, the ε3-ε4 genotype could be the risk factor for the development of CHD and IS. The ε4 allele increased the risk of both CHD-IS and CHD groups with unadjusted OR 1.964 (95%CI: 1.228–3.142, p=0.005) and 1.666 (95%CI: 1.079–2.572, p=0.021). The ε3-ε4 genotype increased the risk of CHD with unadjusted OR 1.939 (95%CI: 1.143–3.287, p=0.014) and showed the same tendency about CHD-IS with unadjusted OR 2.631 (95%CI: 1.496–4.626, p=0.001) (Table 4). The multivariate binary logistic regression analysis showed that ε3-ε4 genotype was the independent risk factor for development of CHD-IS and CHD after being adjusted for age, sex, smoking history, SBP and Hcy (p=0.002, OR 2.794, 95%CI: 1.539–5.072 and p=0.005, OR 2.210, 95%CI: 1.263–3.867, respectively). Furthermore, the ε4 allele was found to be independent risk factor for development of CHD-IS and CHD (p=0.001, OR 2.740, 95%CI: 1.569–4.784 and p=0.004, OR 2.126, 95%CI: 1.265–3.575, respectively). In the present study, age, male, SBP, and Hcy were also independent risks for CHD-IS and CHD, but smoking was only found to be the independent risk for CHD (Table 5).
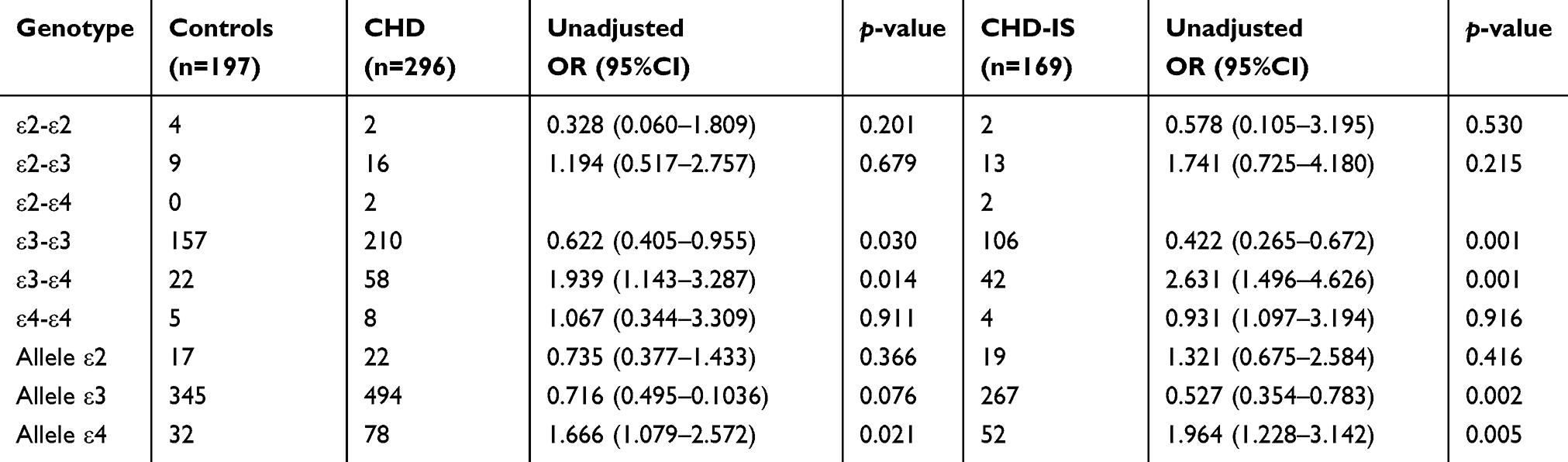 |
Table 4 Associations of APOE Gene Polymorphism with the Risk of the CHD Group and CHD-IS Group Compared with the Control Group Represented as Unadjusted OR |
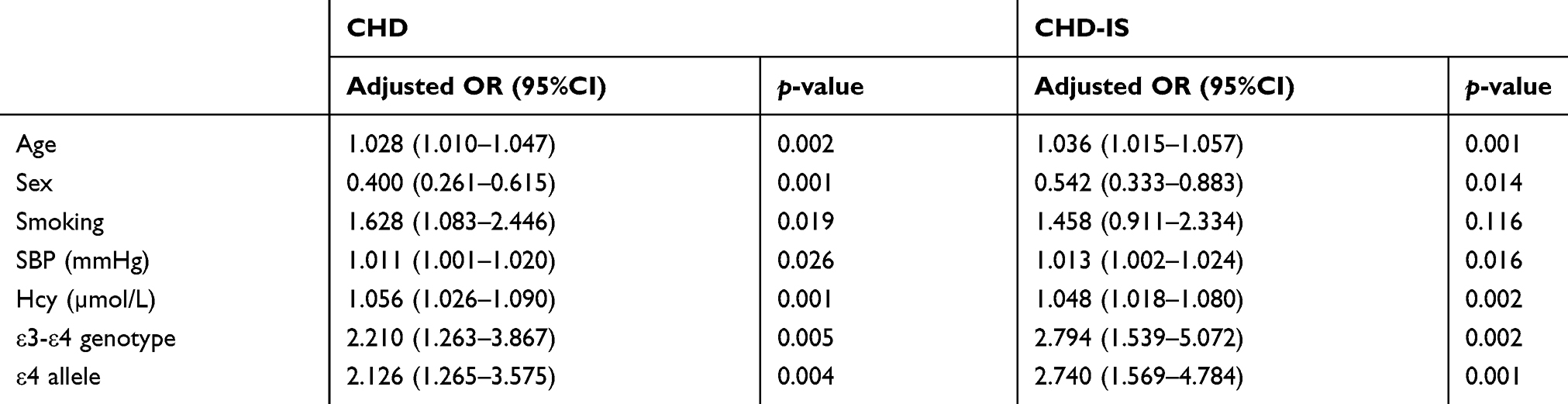 |
Table 5 Association of APOE Gene Polymorphism with the Risk of the CHD Group and CHD-IS Group Compared with the Control Group Represented as Adjusted OR |
The Correlation of ε4 Allele Carriers with Lipid Profiles
The significant differences of APOE distribution among these groups mainly resulted from different frequencies of the ε4 allele. The distributions of ε4 allele frequencies could cause the differences of plasma lipid levels. Even though CHD-IS group patients continuously took medium-intensity statins, the differences of plasma lipid levels were still observed between ε4 carriers and ε3-ε3 genotype in all three groups (Table 6). In the control group and CHD group, the values of TC and LDL-C showed significant elevation in ε4 carriers compared with the ε3-ε3 genotype. However, the values of TG and HDL-C level were observed with no significant difference in ε4 carriers when compared with the ε3-ε3 genotype in the control and CHD groups. In the CHD-IS group, there was significant elevation in TC level but not in LDL-C level in ε4 carriers compared with the ε3-ε3 genotype.
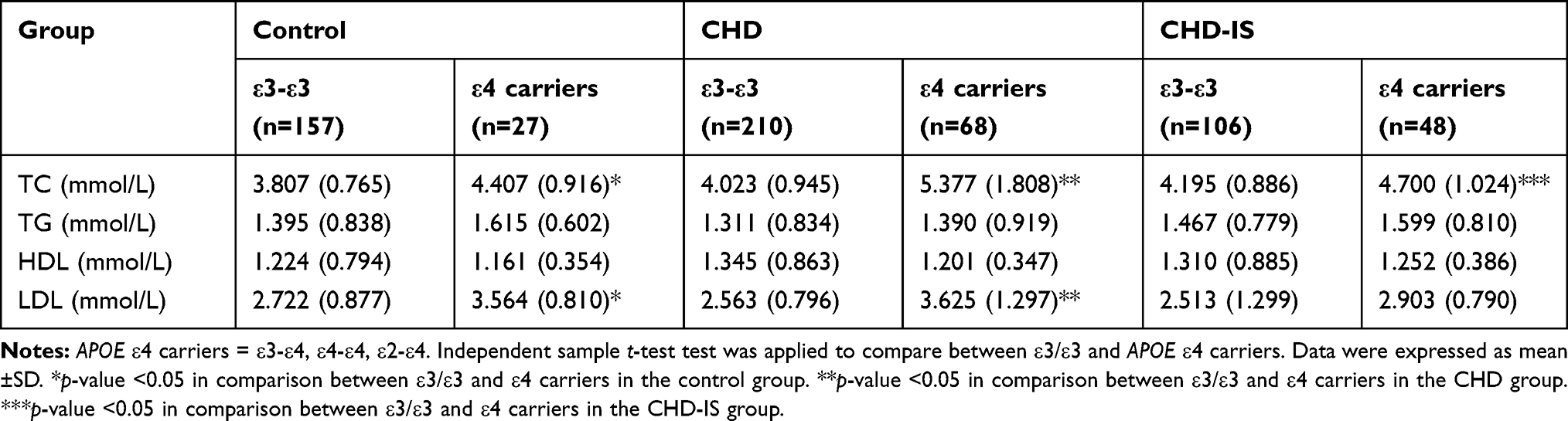 |
Table 6 The Comparation of Fasting Lipid Concentration Between APOE ε4 Carriers and ε3/ε3 Genotypes |
Discussion
Atherosclerosis is a systemic disease caused by lipid metabolism disorders in which coronary arteriosclerosis and cerebral arteriosclerosis can occur simultaneously. Clinical trials had confirmed the beneficial effects of statin treatment in primary and secondary prevention of cardiovascular disease and stroke.11 The statins affected the development of arteriosclerosis by decreasing cholesterol concentration and other mechanisms, which could further prevent the occurrence of IS in CHD patients. Statins could reduce the risk of IS in CHD patients.09–11 IS is the result of complex interactions involving different environmental and genetic factors.3 APOE gene is a common candidate gene which plays an important role in lipid metabolism. The relationship of APOE polymorphism and coronary artery disease had been explored in several ethnic groups, including Caucasian in the USA,12 Italian,13 Turkish,14 Chinese15 and Indian.16 The association between APOE polymorphism and the risk of different subtypes of stroke had been evaluated, the ε4 allele might predict an increased risk for different subtypes of stroke, including IS and hemorrhagic stock.17 The APOE ε4+ genotype was related to more severe intracranial atherosclerosis score.18 The ε4 allele was associated with higher plasma levels of LDL-C, TC, apolipoprotein B and increased the risk of coronary artery disease when compared with ε3 allele.19 ε4 allele was an independent risk factor for myocardial infraction.20 At present clinical practice, medium-intensity statins are widely used in China. However, there is no research demonstrating the relationship between APOE gene polymorphism and IS in CHD patients treated with medium-intensity statins, so it is of great interest for us to study the relationship.
In present study, higher prevalence of elderly, male, higher level of SBP, TC, and LDL-C were observed in CHD group and CHD-IS group, all of which were the established risk factors for CHD and IS. Higher level of SBP damaged the intima of the artery, which promoted the deposition of cholesterol and lipids, and aggravated the formation of atherosclerotic plaque. In addition, our results were consistent with several epidemiological studies in which Hcy was an independent risk factors for stroke.21–23
In the Chinese population, the predominant genotype is ε3-ε3, whereas the most common allele is ε3.5,24 In this study, the ε3-ε3 genotype accounted for 79.7% in the control group, 70.9% in the CHD group and 62.6% in the CHD-IS group respectively. Our results were consistent with previous studies. The ε3-ε4 genotype had an increasing trend, accounting for 11.2% in the control group, 19.6% in the CHD group and 24.9% in the CHD-IS group, respectively. While the frequency of ε2-ε2 genotype and the ε2 allele was lower in the three groups. The ε3-ε4 genotype and ε4 allele had significantly higher prevalence in the CHD group compared with control group (p=0.006 and p=0.007, respectively). Compared with the control group, the ε3-ε4 genotype and ε4 allele in the CHD-IS group had significantly higher prevalence (p=0.001 and p=0.005, respectively). After being adjusted for age, sex, smoking history, SBP and Hcy, the multivariable binary logistic regression analysis showed that ε3-ε4 genotype was 2.21-fold higher risk (p=0.005), while ε4 allele caused 2.126-fold higher risk (p=0.004) for the development of CHD. ε3-ε4 genotype demonstrated 2.794-fold higher risk (p=0.002) while ε4 allele caused 2.74-fold higher risk (p=0.001) for the development of IS in CHD patients treated with medium-intensity statins. These data suggested that ε3-ε4 genotype and ε4 allele were the independent risk factors for the development of CHD and CHD-IS. Medium-intensity statins therapy did not completely prevent IS in CHD patients with the ε3-ε4 genotype or the ε4 allele.
The TC and LDL-C levels were significantly elevated in the CHD and CHD-IS groups compared with the control group (p<0.001 and p=0.015, respectively) (Table 1). The levels of TC and LDL-C were lower in the CHD-IS group than that in the CHD group, which could have resulted from more use of medium-intensity statins in the CHD-IS group, but there was no significant difference (p=0. 241 and p=0.139, respectively). APOE gene polymorphism could play important role in lipid metabolism.25 It was mainly the different frequencies of the ε4 allele that led to significant differences in APOE distribution among these groups. These distributions of the ε4 allele frequencies could cause the differences in plasma lipid levels. Although patients of the CHD-IS group continuously took medium-intensity statins when they were diagnosed with IS, the differences of plasma lipid levels still existed because of ε4 carriers and ε3-ε3 genotype among the three groups (Table 6). In CHD group, the levels of TC and LDL-C of ε4 carriers were significantly higher than those of ε3-ε3 genotype. In the CHD-IS group, there was no significant difference in LDL-C level between ε4 carriers and ε3-ε3 genotype, but TC level of ε4 carriers increased significantly. In this study, the patients of CHD-IS group were limited to taking medium-intensity statins, and ε4 allele was still associated with higher plasma TC level when compared with ε3-ε3 genotype.
There were also some limitations in this study. Firstly, the sample size in this study was limited. Secondly, in order to more truly study the effect of CHD treatment on the incidence rate of IS, we chose the most routine dose of statin in practical application. While other studies suggested that intensive-dose statin treatment could be more favorable for reducing the incidences of all strokes.26
Our study supported that the ε4 allele was an independent risk factor for the development of CHD by affecting the plasma lipid levels, and the main genotype was ε3-ε4. The ε4 allele and ε3-ε4 genotype were firstly found to be the major predictors for development of IS in CHD patients treated with medium-intensity statins. Therefore, high-intensity statins would be needed for CHD patients who carried ε4 allele to prevent the development of IS more effectively.
Funding
There was no funding for this work.
Disclosure
No conflict of interest exits in the submission of this manuscript, and the manuscript is approved by all authors for publication. The authors report no conflicts of interest in this work. Ping Lv and Yaofu Zheng contributed equally to this work and are co-first authors for this study.
References
1. Benjamin EJ, Virani SS, Callaway CW, et al. Heart disease and stroke statistics—2018 update: a report from the American Heart Association. Circulation. 2018;137(12):e67–e492.
2. Wang Y, Cui L, Ji X, et al. The China National Stroke Registry for patients with acute cerebrovascular events: design, rationale, and baseline patient characteristics. Int J Stroke off J Int Stroke Soc. 2011;6(4):355–361. doi:10.1111/j.1747-4949.2011.00584.x
3. Lahiri DK, Sambamurti K, Bennett DA. Apolipoprotein gene and its interaction with the environmentally driven risk factors: molecular, genetic and epidemiological studies of Alzheimer’s disease. Neurobiol Aging. 2004;25(5):651–660. doi:10.1016/j.neurobiolaging.2003.12.024
4. Tanyanyiwa DM, Marais AD, Byrnes P, et al. The influence of ApoE genotype on the lipid profile and lipoproteins during normal pregnancy in a Southern African population. Afr Health Sci. 2016;16(3):853–859. doi:10.4314/ahs.v16i3.28
5. Yin R, Pan S, Wu J, et al. Apolipoprotein E gene polymorphism and serum lipid levels in the Guangxi Hei Yi Zhuang and Han populations. Exp Biol Med. 2008;233(4):409–418. doi:10.3181/0709-RM-254
6. Afef R, AliNadia B, Aroua C, et al. Association between ACE polymorphism, cognitive phenotype and APOE E4 allele in a Tunisian population with Alzheimer disease. J Neural Transm. 2016;123(3):317–321. doi:10.1007/s00702-015-1468-3
7. Guang-Da X, You-Ying L, Zhi-Song C, et al. Apolipoprotein e4 allele is predictor of coronary artery disease death in elderly patients with type 2 diabetes mellitus. Atherosclerosis. 2004;175(1):77–81. doi:10.1016/j.atherosclerosis.2004.02.015
8. Pedersen TR, Kjekshus J, Berg K, et al. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Atherosclerosis Supple. 2004;5(3):81–87.
9. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339(19):1349–1357. doi:10.1056/NEJM199811053391902
10. Plehn JF, Davis BR, Sacks FM, et al. Reduction of stroke incidence after myocardial infarction with pravastatin: the Cholesterol and Recurrent Events (CARE) study. The Care Investigators Circulation. 1999;99(2):216–223.
11. Baigent C, Keech A, Kearney P, et al. Efficacy and safety of cholesterol-lowering treatment - reply. The Lancet. 2006;367(9509):470–471. doi:10.1016/S0140-6736(06)68171-3
12. Eichner JE, Kuller LH, Orchard TJ, et al. Relation of apolipoprotein E phenotype to myocardial infarction and mortality from coronary artery disease. Am J Cardiol. 1993;71(2):160–165. doi:10.1016/0002-9149(93)90732-R
13. Corbo RM, Vilardo T, Ruggeri M, et al. Apolipoprotein E genotype and plasma levels in coronary artery disease. A case-control study in the Italian population. Clin Biochem. 1999;32(3):217–222.
14. Attila G, Acartürk E, Eskandari G, et al. Effects of apolipoprotein E genotypes and other risk factors on the development of coronary artery disease in Southern Turkey. Clinica Chimica Acta. 2001;312(1):191–196. doi:10.1016/S0009-8981(01)00624-6
15. Yangchun Z, Dayi H, Xiufang H, et al. Apolipoprotein E polymorphism in northern Chinese elderly patients with coronary artery disease. J Geriatric Cardiol. 2006;3(2):95–98.
16. Chaudhary R, Likidlilid A, Peerapatdit T, et al. Apolipoprotein E gene polymorphism: effects on plasma lipids and risk of type 2 diabetes and coronary artery disease. Cardiovasc Diabetol. 2012;11(1):36. doi:10.1186/1475-2840-11-36
17. Chen C, Zhiping H. ApoE polymorphisms and the risk of different subtypes of stroke in the Chinese population: a comprehensive meta-analysis. Cerebrovasc Dis. 2016;41(3–4):119–138. doi:10.1159/000442678
18. Abboud S, Viiri LE, Lütjohann D, et al. Associations of apolipoprotein E gene with ischemic stroke and intracranial atherosclerosis. Eur J Hum Genet. 2008;16(8):955–960. doi:10.1038/ejhg.2008.27
19. Singh P, Singh M, Bhatnagar D, et al. Apolipoprotein E polymorphism and its relation to plasma lipids in coronary heart disease. Indian J Med Sci. 2008;62(3):105–112. doi:10.4103/0019-5359.39613
20. Kumar P, Luthra K, Dwivedi M, et al. Apolipoprotein E gene polymorphisms in patients with premature myocardial infarction: a case-controlled study in Asian Indians in North India. Albion. 2003;23(Pt 4):382–387.
21. Wu XQ, Ding J, Ge AY, et al. Acute phase homocysteine related to severity and outcome of atherothrombotic stroke. Eur J Intern Med. 2013;24(4):362–367. doi:10.1016/j.ejim.2013.01.015
22. Wang CY, Chen ZW, Zhang T, et al. Elevated plasma homocysteine level is associated with ischemic stroke in Chinese hypertensive patients. Eur J Intern Med. 2014;25(6):538–544. doi:10.1016/j.ejim.2014.04.011
23. Han L, Wu Q, Wang C, et al. Homocysteine, ischemic stroke, and coronary heart disease in hypertensive patients. Stroke. 2015;46(7):1777–1786. doi:10.1161/STROKEAHA.115.009111
24. Hao L, Ping M, Changhou X, et al. Apolipoprotein E polymorphism and the risk of intracranial aneurysms in a Chinese population. BMC Neurol. 2016;16(1):14. doi:10.1186/s12883-016-0537-z
25. Anoop S, Meena MK, Luthra K. E polymorphism in cerebrovascular & coronary heart diseases. Ind J Med Res. 2010;132(4):363–378.
26. Wang J, Chen D, D B L, et al. Comparison of the efficacy and safety of intensive-dose and standard-dose statin treatment for stroke prevention. Medicine. 2016;95(39):e4950. doi:10.1097/MD.0000000000004950
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.