")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Association Between Serum Ferritin Concentration and Risk of Adverse Maternal and Fetal Pregnancy Outcomes: A Retrospective Cohort Study
Authors Yang L, Wu L, Liu Y, Chen H, Wei Y, Sun R, Shen S, Zhan B, Yang J, Deng G
Received 4 July 2022
Accepted for publication 13 September 2022
Published 19 September 2022 Volume 2022:15 Pages 2867—2876
DOI https://doi.org/10.2147/DMSO.S380408
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Gian Paolo Fadini
Lanyao Yang1,2 *, Lanlan Wu3 *, Yao Liu,3 Hengying Chen,4 Yuanhuan Wei,3 Ruifang Sun,3 Siwen Shen,3 Bowen Zhan,1,2 Jianjun Yang,1,2 Guifang Deng3
1Department of Nutrition and Food Hygiene, School of Public Health and Management, Ningxia Medical University, Yinchuan, People’s Republic of China; 2Key Laboratory of Environmental Factors and Chronic Disease Control, School of Public Health and Management, Ningxia Medical University, Yinchuan, People’s Republic of China; 3Department of Clinical Nutrition, Union Shenzhen Hospital of Huazhong University of Science and Technology, Shenzhen, People’s Republic of China; 4Department of Maternal and Child Health, School of Public Health, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guifang Deng, Department of Clinical Nutrition, Union Shenzhen Hospital of Huazhong University of Science and Technology, No. 89 Taoyuan Road, Shenzhen, Guangdong, 518052, People’s Republic of China, Email [email protected] Jianjun Yang, Department of Nutrition and Food Hygiene, School of Public Health and Management, Ningxia Medical University, No. 1160 Shengli Road, Yinchuan, Ningxia, 750004, People’s Republic of China, Email [email protected]
Objective: This study evaluated the associations of serum ferritin (SF) concentration during pregnancy with the risk of adverse maternal and fetal pregnancy outcomes.
Methods: We conducted a retrospective study of 2327 pregnant women from 2015 to 2020 in Guangdong, China. SF concentrations were measured at 16– 18th and 28– 32th week of gestation. Logistic regression models were applied to estimate the association between SF concentration and the risk of adverse pregnancy outcomes.
Results: After multivariable adjustment, the odds ratio (OR) of the highest quartile of SF concentration at 16– 18th week of gestation was 1.43 (95% confidence interval [CI]: 1.09, 1.89) for gestational diabetes mellitus (GDM) and 1.79 (95% CI: 1.15, 2.79) for small for gestational age (SGA) when compared with the lowest quartile. At 28– 32th week of gestation compared with the lowest quartile, women with SF in the highest quartile had an increased risk of SGA (OR: 1.62; 95% CI: 1.01, 2.62). Moreover, the lowest quartile of SF concentration decreased risk of SGA by 90% (95% CI: 0.01, 0.80) when compared with the highest quartile among pregnancy women with GDM.
Conclusion: Elevated SF concentrations increased the risk of GDM and SGA during pregnancy. Maintaining an appropriately low level of maternal SF at 28– 32th week of gestation in women with GDM could reduce the risk of SGA.
Keywords: ferritin, adverse pregnancy outcomes, gestational diabetes mellitus, small for gestational age
Introduction
Nutritional needs are increased to supply the growing fetus and placenta, thus, nutrient such as iron deficiencies can easily occur during pregnancy.1 Iron is a trace element essential for physiological functions, which is stored in the body as ferritin.2,3 Maternal iron deficiency anaemia (IDA), usually accompanied by a drop in ferritin, unsurprisingly, is therefore prevalent among pregnant women across the globe, affecting about 42% of them.4,5 IDA is widely recognized worldwide as a factor associated with adverse maternal and fetal outcomes. IDA may restrict the body’s oxygen circulation, leading to oxidative stress or chronic hypoxia,3,6 which is related to higher risk of low birth weight (LBW), preterm delivery and neonatal IDA,7 which in turn can have long-lasting effects on intelligence, motor and behavioral development, and increase risk of IDA in future generations.8
However, it is worth noting that iron is a double-edged sword in the body system, with both iron deficiency and iron excess causing varying degrees of damage to health.9 In addition to synthesizing hemoglobin and mediating cell growth and development, iron is also a redox-active transitional metal with strong oxidation properties.3 Therefore, it is crucial to assess the iron status of the body during pregnancy. Among them, serum ferritin (SF) is the most used clinically. Previous animal and epidemiological studies observed a significant association between excess SF storage and glucose metabolism disorders,10–12 and others have found a positive association between ferritin and type 2 diabetes.13,14 Then, some epidemiological studies have investigated the relationship between high SF concentrations and the incidence of gestational diabetes mellitus (GDM), but the results have been controversial. A case–control study from Western Asia showed that high SF levels were associated with an increased incidence of GDM,15 as confirmed in a prospective observational study by Cheng et al of 851 Chinese subjects.16 However, a prospective observational study from Lebanon did not find any significant association between a high SF concentration and the incidence of GDM in early pregnancy.17 Furthermore, the relation between SF and adverse maternal and fetal pregnancy outcomes had also attracted attention. Recent studies indicated that SF concentrations were negatively correlated with birth weight in the third trimester, but this relationship is not significant in the second trimester.1,18 Rahman et al only observed that elevated SF at gestational week 30 were positively associated with low birth weight (LBW).18 Thus far, research on the association between high SF concentrations and more comprehensive adverse maternal and fetal pregnancy outcomes has been relatively limited. Besides, few studies have investigated differences in the effects of SF on pregnant women with and without GDM.
SF concentration change dramatically with the progresses of pregnancy because of physiological changes in maternal blood volume and increased iron requirements for the placenta and fetus.9 In contrast to the measurement of SF concentrations from blood samples collected at single time points in previous studies, we collected blood samples at different time points to reliably analyze the relationship between high SF concentrations and the risk of adverse maternal and fetal pregnancy outcomes. Thus, we aimed to evaluate the relation between SF with the risk of development of GDM, and explore the association between SF concentrations and the risk of adverse pregnancy outcomes by detecting the SF concentration in different gestation stage in Chinese women.
Materials and Methods
Study Population
We conducted a retrospective study of 2419 pregnant women who had scheduled prenatal visits and planned to deliver their babies at the Union Shenzhen Hospital of the Huazhong University of Science and Technology from January 2015 to November 2020. All clinical data from the first antenatal examination to delivery were obtained from the hospital record information system and analyzed anonymously. Based on the following inclusion criteria, we established a cohort of pregnant women: 1) women aged ≥18 years; 2) singleton pregnancy; and 3) availability of complete medical records (including prenatal examination and delivery records). Participants with any of the following exclusion criteria were excluded: 1) twin and multiple pregnancy (n = 11); 2) pre-conceptional diabetes (n = 15); 3) hepatitis, or impaired liver function (n = 48); 4) nephritis or impaired kidney function (n = 5); 5) cardiovascular diseases (n = 3); and 6) acute respiratory infections (n = 10). Ultimately, after 92 pregnant women were excluded, 2327 pregnant women were included. Participants wrote informed consent forms at the beginning of the study. The protocol for this study was approved by the Ethics Committee of the Union Shenzhen Hospital of Huazhong University of Science and Technology (No. 2019072644) and carried out in accordance with the Declaration of Helsinki developed by the World Medical Association.
Laboratory Measurements
Venous blood samples were collected from the pregnant women at 16–18th and 28–32th weeks of gestation, and various biochemical indexes were measured. SF and hemoglobin concentrations were analyzed by a 7600–010 automatic analyzer (Hitachi, Tokyo, Japan) and hematology analyzer (Sysmex XN90000, Japan), respectively. The mean SF concentrations were derived from the average values measured at 16–18th and 28–32th weeks of gestation. The changes of SF concentrations were determined by subtracting the SF measured at 16–18th weeks of gestation from that measured at 28–32th weeks of gestation. The trajectory of SF concentrations was determined by the median concentration of SF at 16–18th and 28–32th weeks of gestation as the standard.
Maternal and Fetal Characteristics
Information on the maternal age, weight, height, educational background, pregnancy smoking and alcohol consumption status, history of diseases, history of gestation, and conception method were collected using questionnaires and by reviewing records in the hospital information system. Maternal body mass index (BMI) (kg/m2) was calculated as weight (kg) divided by height squared (m2). Parity was interpreted as the number of live or stillborn infants before this pregnancy. The gestational age at delivery (weeks) was determined by the time of the last menstrual period until the time of delivery.
Information on the gender and physical characteristics of the newborns was obtained by reviewing records in the hospital information system. Neonatal weight, height, head circumferences and chest circumferences were measured at the time of birth using infant length and weight measuring instrument and soft ruler, respectively.
Definitions of the Adverse Maternal and Fetal Pregnancy Outcomes
We designated GDM, premature birth, macrosomia, LBM, large for gestational age (LGA), and SGA as adverse maternal and fetal pregnancy outcomes. The 75-g oral glucose tolerance test was conducted as recommended by the International Association of Diabetes and Pregnancy Research Groups (IADPSG).19 At 24–28th week of gestation, maternal blood samples were collected at 0, 1, and 2 h after the administration of 75 g of glucose (loading dose) to determine the serum glucose concentration. Based on the IADPSG criteria, GDM was diagnosed when one of the following criteria were met: fasting plasma glucose ≥5.1 mmol/L; 1-h plasma glucose ≥10.0 mmol/L; or 2-h plasma glucose ≥8.5 mmol/L. Premature birth was defined as the birth of a newborn whose gestational age was <37 weeks. Following the latest standards in China, newborns with a weight of >4000 g were determined as macrosomia, those with a weight of <2500 g were designated as LBW, and those with a birth weight below the 10th percentile or above the 90th percentile of the average weight of other newborns of the same gestational age were defined as being SGA and LGA, respectively.20 Similarly, according to the 10th or 90th percentile of the same age newborns, we define short state at birth, tall stature at birth, small head circumference and big head circumference, respectively.20
Statistical Analyses
Participants were divided into four groups based on the SF concentration quartiles. Continuous variables were expressed as the median (quartiles) and categorical variables as percentages (%). Differences between groups were assessed using Kruskal–Wallis test for continuous variables, or chi-square test for categorical variables. Using the lowest groups as the reference group for all subjects, logistic regression analysis was performed to assess the ORs and 95% CIs for the risk of adverse maternal and fetal pregnancy outcomes. Baseline variables that were considered clinically relevant or that showed a univariate relationship with outcome were entered into multivariable adjusted models. Finally, the multivariable-adjusted model was adjusted for age, BMI, education background, smoking status, alcohol consumption status, parity, abortion history, conception method, thalassemia history and hemoglobin concentrations. Furthermore, pregnant women with or without GDM were divided into two subgroups, logistic regression analysis was performed using the fourth SF concentration quartile as the reference group. The association of the changes and the mean SF concentrations with pregnancy outcomes were also analyzed. SPSS version 21.0 (SPSS Inc., Chicago, IL, USA) was used to analyze our data. A two-sided P value <0.05 was considered as statistically significant.
Results
Participant Characteristics
We conducted a retrospective study of 2327 Chinese pregnant women. As presented in Table 1, significant differences in terms of the maternal alcohol consumption status, hemoglobin concentrations, the 1-h and 2-h post-load glucose concentrations, and SF at 16–18th and 28–32th week of gestation were detected between the four quartiles (all P < 0.05). We found that the prevalence of GDM and SGA (P = 0.026 and P = 0.029, respectively) was significantly elevated in the higher quartiles of SF concentration. No significant difference was discovered in other indicators.
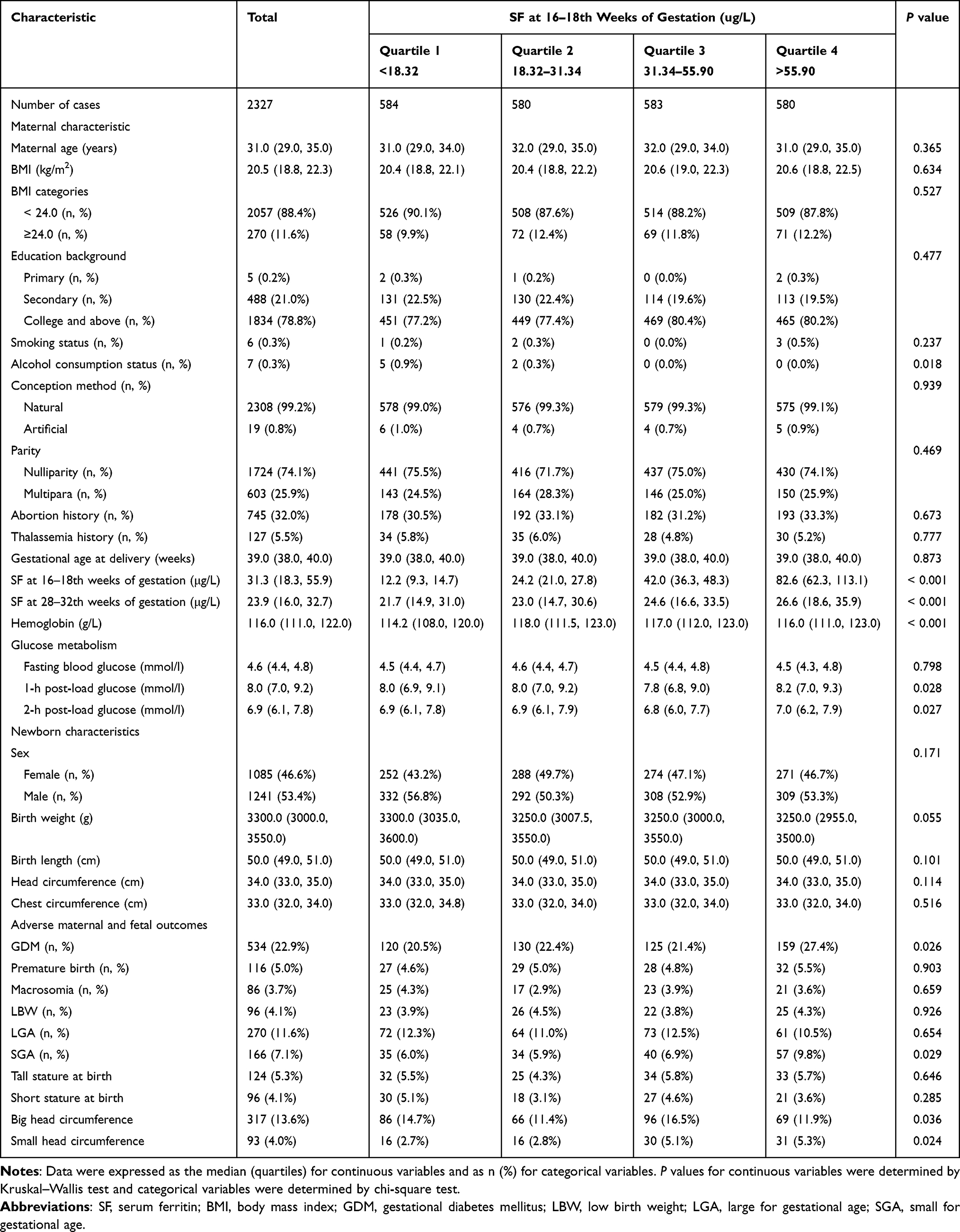 |
Table 1 Baseline Characteristics of Participants According to Quartiles of SF at 16–18th Weeks of Gestation |
Association Between SF Concentration and the Risk of GDM
In Table 2, we found that the SF concentration at 16–18th weeks of gestation increased and the incidence of GDM changed, with values of 20.5%, 22.4%, 21.4% and 27.4%. After adjusting for the covariates, the highest SF concentration quartile was significantly associated with an increased risk of developing GDM (AOR: 1.43, 95% CI: 1.09, 1.89) when compared with the lowest quartile. Each SD increase in the SF concentration was associated with a 16% (AOR: 1.16, 95% CI: 1.05, 1.27) increase in the risk of developing GDM.
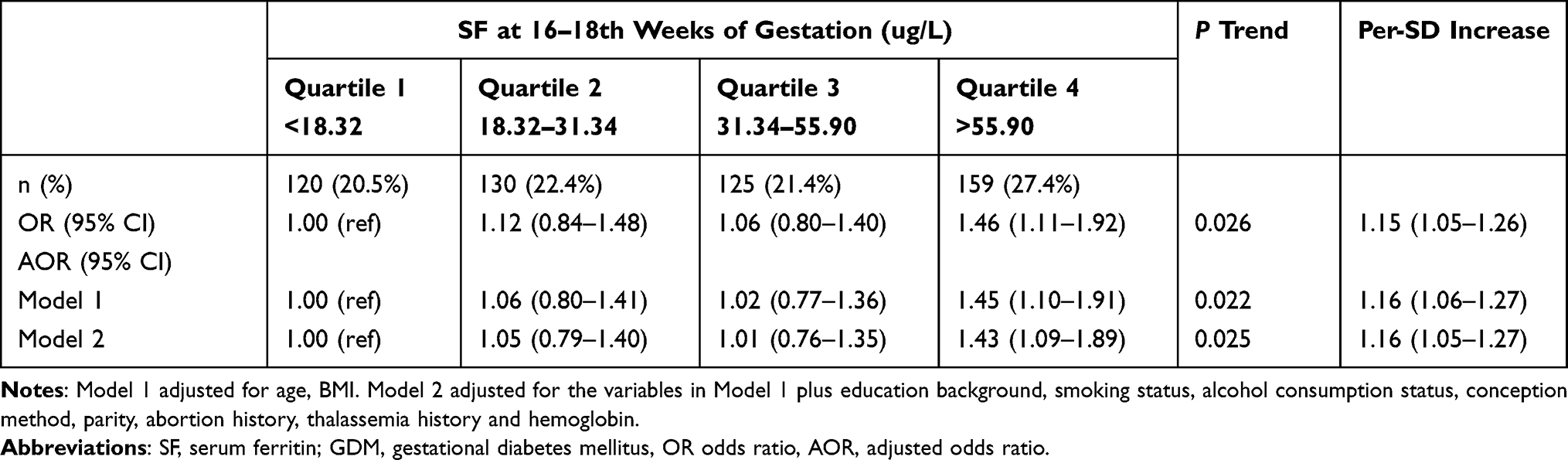 |
Table 2 Odds Ratios (95% Confidence Intervals) for the Occurrence of GDM According to the SF at 16–18th Weeks of Gestation |
Association Between SF Concentration and the Risk of Adverse Pregnancy Outcomes
As shown in Tables 3 and 4, the AOR for SGA in the highest SF concentration quartile compared with the lowest quartile was 1.79 (95% CI: 1.15, 2.79) at 16–18th weeks of gestation and 1.62 (95% CI: 1.01, 2.62) at 28–32th weeks of gestation. Each SD increase in the SF concentration at 16–18th weeks of gestation was associated with a 21% (AOR: 1.21, 95% CI: 1.06, 1.38) increase in the risk of SGA; the same increase at 28–32th weeks of gestation was associated with a 17% (AOR: 1.17, 95% CI: 1.03, 1.34) increase in the risk of SGA. In Supplementary Table 1, compared with the lowest quartile, the AOR of Small head circumference in the highest SF concentration quartile was 2.05 (95% Cl: 1.10, 3.80) and 1.97 (95% Cl: 1.05, 3.69) at 16–18 weeks of gestation and 28–32 weeks of gestation, respectively. We also found the same association between SF concentration and larger body length (AOR: 2.01, 95% CI: 1.15, 3.50) at 28–32 weeks of gestation. No significant difference was observed between SF concentration and other pregnancy outcomes.
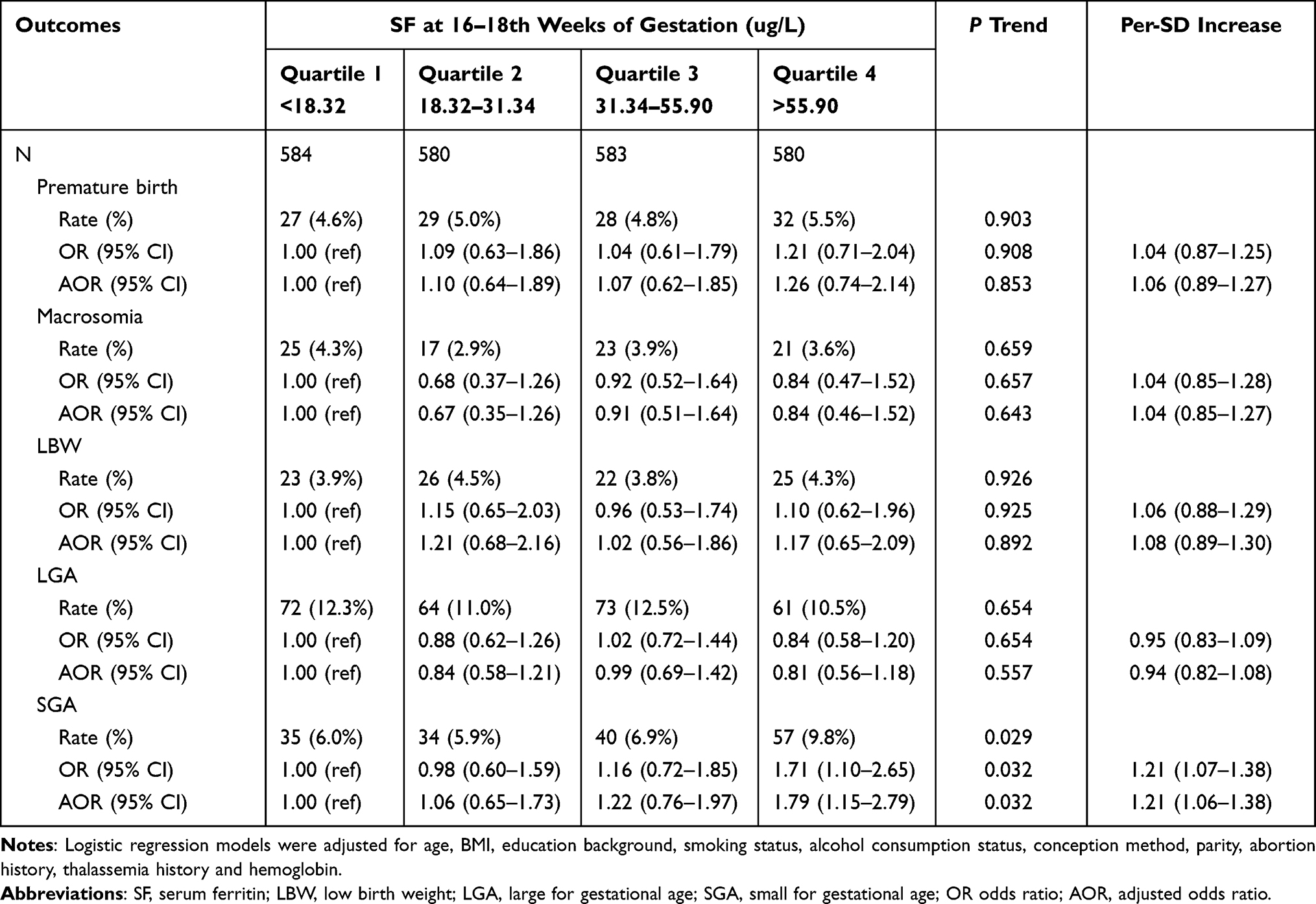 |
Table 3 Odds Ratios (95% Confidence Intervals) for the Occurrence of Adverse Maternal and Fetal Outcomes According to the SF at 16–18th Weeks of Gestation |
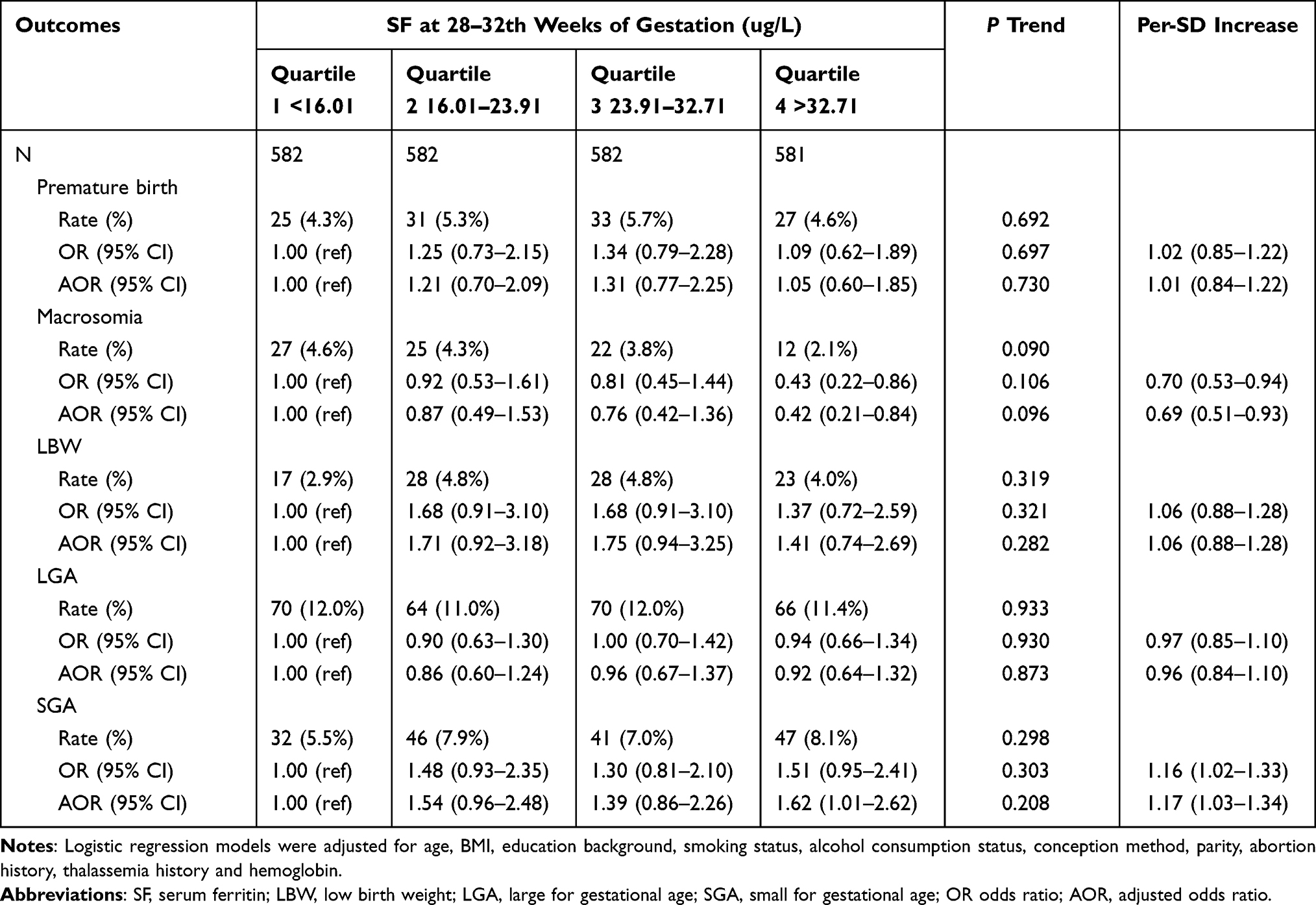 |
Table 4 Odds Ratios (95% Confidence Intervals) for the Occurrence of Adverse Maternal and Fetal Outcomes According to the SF at 28–32th Weeks of Gestation |
Association Between SF Concentration at 28–32th Week of Gestation and the Risk of Adverse Pregnancy Outcomes Among Pregnancy Women with and without GDM
Figure 1 outlines that the lowest SF concentration quartile was significantly associated with a 90% decreased risk of SGA (AOR: 0.10, 95% CI: 0.01, 0.80) when compared with the highest quartile among pregnancy women with GDM. There was no significant difference between SF concentration and adverse pregnancy outcomes among pregnancy women without GDM.
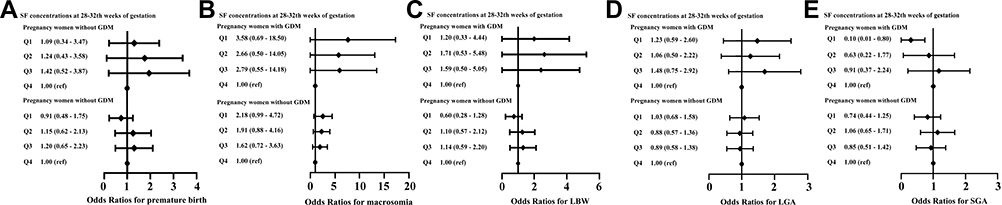 |
Figure 1 The association between SF and the risk of adverse pregnancy outcomes among pregnancy women with and without GDM. The model was adjusted for age, BMI, education background, smoking status, alcohol consumption status, conception method, parity, abortion history, thalassemia history and hemoglobin. |
The Association Between the Mean, Changes and Trajectory of SF Concentration and the Risk of Adverse Pregnancy Outcomes
In Supplementary Table 2, the highest quartile of mean SF concentration had a 78% (OR: 1.78, 95% CI: 1.15, 2.74) increased risk of SGA. The associations between the changes of SF concentration across the 16–18th and 28–32th week of gestation with adverse pregnancy outcomes are presented in Supplementary Table 3. The AOR for the risk of SGA in the highest quartile was 1.61 (95% CI: 1.04, 2.50) when compared with the lowest quartile. As shown in Supplementary Table 4, compared with the low-to-low-level, the high-to-high level was significantly associated with a 63% increase in SGA risk (AOR: 1.63, 95% CI: 1.06, 2.51).
Discussion
In this retrospective cohort study among Chinese pregnancy women, we observed an increased risk of GDM with elevated SF concentration at 16–18th week of gestation, and the elevated SF concentration at both 16–18th and 28–32th week of gestation was associated with the increased risk of SGA. It is worth mentioning that low SF concentration at 28–32th week of gestation had a decreased risk of SGA among pregnant women with GDM. Moreover, the study also found that more drastic changes in SF concentrations across the 16–18th and 28–32th week of gestation were attributed to a higher risk of developing SGA. The same effect was seen with higher mean SF concentration.
A series of studies have reported the relationship between SF concentration and insulin resistance (IR). SF is a major ferrous storage globulin with a complex structure and is an indicator of iron storage.17,21 Excess iron can catalyze excessive reactive oxygen species (ROS) production.3 ROS are produced by aerobic cells during normal metabolism and can induce cell apoptosis or damage tissues through the cellular oxidative stress response.22,23 Under normal physiological conditions, the generation and elimination of ROS are dynamically balanced. As iron storage increases, the excess iron ions increase the amount of ROS produced.24,25 Consequently, high amounts of iron can restrict the synthesis and secretion of insulin through oxidative stress, leading to the development of IR and the accelerated progression of GDM.26 Second, excess iron is also involved in the development of IR by activating nuclear factor-κ B in macrophages and Kupffer cells, which in turn increases the release of tumor necrosis factor a and downregulates insulin signaling.27,28 Consistent with most studies, our study discovered that elevated SF concentrations at the second trimester (16–18th week of gestation) were associated with an increased risk of the developing of GDM. Similar results were reported by a case–control study from Western Asia15 and another prospective cohort study from China,29 that is, high SF concentrations at 14–18th week of gestation were associated with an increased incidence of GDM (OR: 2.72, 95% CI: 1.76, 4.21). Although our study did not record SF concentrations in the first trimester, several studies that focused on the first trimester of pregnancy have reported results consistent with our findings. A prospective observational study of 851 people observed that elevated SF concentrations in the first trimester were associated with an increased risk of GDM (OR: 2.31, 95% CI: 1.30, 4.10).16 However, a few studies have come to a different conclusion. Chan et al conducted a randomized controlled trial and found no significant difference in the risk of GDM between groups with high SF concentrations and corresponding control groups (OR: 1.04, 95% CI: 0.70, 1.53).30 Another prospective observational study from Lebanon indicated that there were no significant associations between high SF and the incidence of GDM in early pregnancy.17 However, the overall SF concentration recorded in their study was low and the cut-off value for the highest SF concentration quartile was only 38.5 g/L,17 whereas the cut-off value for our study was 55.9 μg/L, which may be the reason for the different results.
Few studies have paid attention to the association between a high SF concentration and the risk of adverse pregnancy outcomes. A retrospective cohort study of 11,581 people from China reported that low SF concentrations were not only correlation with an increased risk of macrosomia (OR: 1.27, 95% CI: 1.07, 1.51), but also with a reduced risk of LBW (OR: 0.68, 95% CI: 0.49, 0.93) and SGA (OR: 0.74, 95% CI: 0.63, 0.86).31 Shaji Geetha et al found that higher maternal serum ferritin concentrations were associated with higher risk of preeclampsia.32 No consistent associations were present of maternal ferritin in early pregnancy with the risks of gestational hypertensive disorders as reported in a population-based prospective cohort study among 5983 pregnant women.33 Similar associations were found in our study, with elevated SF concentrations associated with an increased risk of SGA. However, we did not discover any significant associations between SF concentration and the risks of macrosomia, gestational hypertensive disorders and LBW. The reason for the discrepancy may be explained by the different ethnicities of the participants, variations in study design, time points of SF concentration measurement, diagnostic criteria, and other confounding factors.18,31,34,35 In their study, iron deficiency (ferritin < 12 ug/L) accounted for 52% of the total population,31 compared with only 12% in our cohort. Moreover, the time points of SF concentration measurement were also later than ours. Rahman’s study showed that the elevated SF concentration at the 30th week of pregnancy was associated with the increased risk of LBW, while no such correlation was found at the 14th week of pregnancy.18 The mechanism underlying the adverse effect of high SF concentrations on maternal and perinatal outcomes remains unclear. The possible mechanisms are as follows: First, higher maternal ferritin may affect fetal development through oxidative stress, lipid peroxidation, and DNA damage in placental cells.36 Then, notably, iron build-up may also increase blood viscosity and reduce uteroplacental blood flow, thereby impairing fetal development.37
One striking finding from this study was the risk of SGA reduced with the appropriate decrease of SF concentrations at 28–32th week of gestation among pregnancy women with GDM. In China, GDM is routinely diagnosed at 24–28 weeks of gestation by the 75-g oral glucose tolerance test. We can predict and intervene it by measuring SF concentration as early as possible, and get a better prognosis. Another interesting finding from our study was that more drastic increases in SF concentrations from the 16–18th to 28–32th week of gestation were associated with a higher risk of developing SGA. Compared with the low-to-low-level of the trajectory SF concentrations, the high-to-high level had higher risk of SGA. In addition, the risk of SGA increased with the mean SF concentration at 16–18th and 28–32th week of gestation. These results further emphasize the importance of monitoring SF concentrations throughout pregnancy. In China, routine iron supplementation is generally recommended from the third month of pregnancy and regular blood tests are performed at each trimester of pregnancy.38 Our studies may suggest maintaining a slightly lower value rather than a larger value within the normal range of serum ferritin, shortening follow-up intervals and increasing the number of follow-up, providing personalized guidance for pregnant women with respect to iron supplementation based on SF concentration at different stages of pregnancy to mitigate the risk of adverse maternal and fetal pregnancy outcomes.
There are several limitations to this study. First, all of the subjects included were from China. This relatively limited population source might have led to selection bias. Second, although the major risk factors were recognized and adjusted for in the model, some unmeasured or unknown residual confounders remained. For instance, we lacked information on inflammatory markers, which may have affected our results as acute or chronic inflammation can affect SF concentrations.39,40 We excluded women with known inflammatory diseases to minimize this effect.
Conclusion
Elevated SF concentrations at 16–18th week of gestation were associated with increased risks of GDM and SGA. At 28–32th week of gestation, women with higher SF concentrations faced an increased risk of SGA. Furthermore, the risk of SGA reduced with the appropriate decrease of SF concentrations at 28–32th week of gestation among pregnancy women with GDM. Therefore, SF concentration is a good indicator of the risk of adverse maternal and fetal pregnancy outcomes and can help provide personalized guidance for pregnant women with respect to iron supplementation at different stages of pregnancy.
Highlights
- The risk of SGA reduced with the appropriate decrease of SF concentrations at 28–32th weeks of gestation among pregnancy women with GDM;
- More drastic changes in SF concentrations across the 16–18th and 28–32th weeks of gestation were attributed to a higher risk of developing SGA;
- Higher mean SF concentration contributes to developing SGA;
- The association between SF and adverse maternal and fetal pregnancy outcomes was studied in a relatively large sample.
Abbreviations
SF, Serum ferritin; GDM, Gestational diabetes mellitus; OR, Odds ratio; AOR, Adjusted odds ratio; CI, Confidence interval; SGA, Small for gestational age; IDA, Iron deficiency anaemia; BMI, Body mass index; LBW, Low birth weight; LGA, large for gestational age; ROS, Reactive oxygen species; IR, insulin resistance.
Data Sharing Statement
To protect the privacy of pregnant women, the datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Participants written informed consent forms at the beginning of the study. The protocol for this study was approved by the Ethics Committee of the Union Shenzhen Hospital of Huazhong University of Science and Technology (No. 2019072644) and all methods were performed in accordance with the relevant guidelines and regulations (Declaration of Helsinki).
Acknowledgments
We thank the mothers and children who participated in this study and all the doctors and nurses in the Department of gynecology and obstetrics of Union Shenzhen Hospital of Huazhong University of Science and Technology for their effort and time to take part in this study.
Funding
This study was supported by the National Natural Science Foundation of China [grant number 82103821], the Shenzhen Science and Technology Innovation Committee [grant number JCYJ20190809102203602; JCYJ20210324112400002] and the Guangdong Basic and Applied Basic Project [grant number 2019A1515110456].
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Puerto A, Trojan A, Alvis-Zakzuk NR, et al. Iron status in late pregnancy is inversely associated with birth weight in Colombia. Public Health Nutr. 2021;24(15):5090–5100. doi:10.1017/S136898002100166X
2. Lal A. Iron in health and disease: an update. Indian J Pediatr. 2020;87(1):58–65. doi:10.1007/s12098-019-03054-8
3. Koleini N, Shapiro JS, Geier J, Ardehali H. Ironing out mechanisms of iron homeostasis and disorders of iron deficiency. J Clin Invest. 2021;131(11). doi:10.1172/JCI148671
4. World Health Organization. Guideline: Daily Iron and Folic Acid Supplementation in Pregnant Women. Geneva: World Health Organization; 2012.
5. Black RE, Victora CG, Walker SP, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382(9890):427–451. doi:10.1016/S0140-6736(13)60937-X
6. Gozzelino R, Arosio P. Iron homeostasis in health and disease. Int J Mol Sci. 2016;17(1):130. doi:10.3390/ijms17010130
7. Finkelstein JL, Kurpad AV, Bose B, Thomas T, Srinivasan K, Duggan C. Anaemia and iron deficiency in pregnancy and adverse perinatal outcomes in Southern India. Eur J Clin Nutr. 2020;74(1):112–125. doi:10.1038/s41430-019-0464-3
8. Murray-Kolb LE, Beard JL. Iron deficiency and child and maternal health. Am J Clin Nutr. 2009;89(3):946S–950S. doi:10.3945/ajcn.2008.26692D
9. Fisher AL, Nemeth E. Iron homeostasis during pregnancy. Am J Clin Nutr. 2017;106(Suppl 6):1567S–1574S. doi:10.3945/ajcn.117.155812
10. Feng Y, Feng Q, Lv Y, Song X, Qu H, Chen Y. The relationship between iron metabolism, stress hormones, and insulin resistance in gestational diabetes mellitus. Nutr Diabetes. 2020;10(1):17. doi:10.1038/s41387-020-0122-9
11. Ryan BJ, Van Pelt DW, Guth LM, et al. Plasma ferritin concentration is positively associated with in vivo fatty acid mobilization and insulin resistance in obese women. Exp Physiol. 2018;103(11):1443–1447. doi:10.1113/EP087283
12. Tran TN, Tran HD, Tran-Huu T, Tran DM, Tran QN. A cross-sectional study of serum ferritin levels in Vietnamese adults with metabolic syndrome. Diabetes Metab Syndr Obes. 2022;15:1517–1523. doi:10.2147/DMSO.S360689
13. Wang X, Fang X, Zheng W, et al. Genetic support of A causal relationship between iron status and type 2 diabetes: a Mendelian randomization study. J Clin Endocrinol Metab. 2021;106(11):e4641–e4651. doi:10.1210/clinem/dgab454
14. Shang X, Zhang R, Wang X, Yao J, Zhao X, Li H. The relationship of hyperferritinemia to metabolism and chronic complications in type 2 diabetes. Diabetes Metab Syndr Obes. 2022;15:175–182. doi:10.2147/DMSO.S348232
15. Amiri FN, Basirat Z, Omidvar S, Sharbatdaran M, Tilaki KH, Pouramir M. Comparison of the serum iron, ferritin levels and total iron-binding capacity between pregnant women with and without gestational diabetes. J Nat Sci Biol Med. 2013;4(2):302–305. doi:10.4103/0976-9668.116977
16. Cheng Y, Li T, He M, et al. The association of elevated serum ferritin concentration in early pregnancy with gestational diabetes mellitus: a prospective observational study. Eur J Clin Nutr. 2020;74(5):741–748. doi:10.1038/s41430-019-0542-6
17. Zein S, Rachidi S, Awada S, et al. High iron level in early pregnancy increased glucose intolerance. J Trace Elem Med Biol. 2015;30:220–225. doi:10.1016/j.jtemb.2014.09.004
18. Rahman SM, Siraj MS, Islam MR, Rahman A, Ekstrom EC. Association between maternal plasma ferritin level and infants’ size at birth: a prospective cohort study in rural Bangladesh. Glob Health Action. 2021;14(1):1870421. doi:10.1080/16549716.2020.1870421
19. American Diabetes A. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl 1):S81–90.
20. Capital Institute of P, Coordinating study Group of Nine Cities on the Physical G, Development of C. Growth standard curves of birth weight, length and head circumference of Chinese newborns of different gestation. Zhonghua Er Ke Za Zhi. 2020;58(09):738–746. doi:10.3760/cma.j.cn112140-20200316-00242
21. Shi HBK, Stemmler TL, Philpott CC, Philpott CC. A cytosolic iron chaperone that delivers iron to ferritin. Science. 2008;320(5880):1207–1210. doi:10.1126/science.1157643
22. Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national crosssectional study. BMJ. 2020;369:m997. doi:10.1136/bmj.m997
23. Tofano RJ, Pescinni-Salzedas LM, Chagas EF, et al. Association of metabolic syndrome and hyperferritinemia in patients at cardiovascular risk. Diabetes Metab Syndr Obes. 2020;13:3239–3248. doi:10.2147/DMSO.S271050
24. Eren E, Aykal G, Sayrac S, Erol O, Ellidag HY, Yilmaz N. Relationship between thioredoxin and thioredoxin-binding protein in patients with gestational diabetes mellitus. J Matern Fetal Neonatal Med. 2017;30(2):164–168. doi:10.3109/14767058.2016.1163685
25. Klisic A, Isakovic A, Kocic G, et al. Relationship between oxidative stress, inflammation and dyslipidemia with fatty liver index in patients with type 2 diabetes mellitus. Exp Clin Endocrinol Diabetes. 2018;126(6):371–378. doi:10.1055/s-0043-118667
26. Li W, Sun Z. Study on the correlation between the expression of serum ferritin and gestational diabetes mellitus. Open J Obstet Gynecol. 2020;10(08):1135–1140. doi:10.4236/ojog.2020.1080106
27. Nguyen-Ngo C, Jayabalan N, Salomon C, Lappas M. Molecular pathways disrupted by gestational diabetes mellitus. J Mol Endocrinol. 2019;63(3):R51–R72. doi:10.1530/JME-18-0274
28. She H, Xiong S, Lin M, Zandi E, Giulivi C, Tsukamoto H. Iron activates NF-kappaB in Kupffer cells. Am J Physiol Gastrointest Liver Physiol. 2002;283(3):G719–726. doi:10.1152/ajpgi.00108.2002
29. Zhang X, Wu M, Zhong C, et al. Association between maternal plasma ferritin concentration, iron supplement use, and the risk of gestational diabetes: a prospective cohort study. Am J Clin Nutr. 2021;114(3):1100–1106. doi:10.1093/ajcn/nqab162
30. Chan KK, Chan BC, Lam KF, Tam S, Lao TT. Iron supplement in pregnancy and development of gestational diabetes--a randomised placebo-controlled trial. BJOG. 2009;116(6):789–797. doi:10.1111/j.1471-0528.2008.02014.x
31. Yuan X, Hu H, Zhang M, et al. Iron deficiency in late pregnancy and its associations with birth outcomes in Chinese pregnant women: a retrospective cohort study. Nutr Metab. 2019;16:30. doi:10.1186/s12986-019-0360-9
32. Shaji Geetha N, Bobby Z, Dorairajan G, Jacob SE. Increased hepcidin levels in preeclampsia: a protective mechanism against iron overload mediated oxidative stress? J Matern Fetal Neonatal Med. 2022;35(4):636–641. doi:10.1080/14767058.2020.1730322
33. Taeubert MJ, Wiertsema CJ, Vermeulen MJ, et al. Maternal iron status in early pregnancy and blood pressure throughout pregnancy, placental hemodynamics, and the risk of gestational hypertensive disorders. J Nutr. 2022;152(2):525–534. doi:10.1093/jn/nxab368
34. He Y, Ching Wan Ma R, McIntyre HD, et al. Comparing IADPSG and NICE diagnostic criteria for GDM in predicting adverse pregnancy outcomes. Diabetes Care. 2022;45(9):2046–2054. doi:10.2337/dc22-0579
35. Erbetta K, Almeida J, Waldman MR. Racial, ethnic and nativity inequalities in gestational diabetes mellitus: the role of racial discrimination. SSM Popul Health. 2022;19:101176. doi:10.1016/j.ssmph.2022.101176
36. Casanueva E, Viteri F. Iron and oxidative stress in pregnancy. J Nutr. 2003;133(5Suppl 2):1700S–1708S. doi:10.1093/jn/133.5.1700S
37. Stangret A, Wnuk A, Szewczyk G, Pyzlak M, Szukiewicz D. Maternal hemoglobin concentration and hematocrit values may affect fetus development by influencing placental angiogenesis. J. Matern Fetal Neonatal Med. 2017;30(2):199–204. doi:10.3109/14767058.2016.1168395
38. Wu L, Sun R, Liu Y, et al. High hemoglobin level is a risk factor for maternal and fetal outcomes of pregnancy in Chinese women: a retrospective cohort study. BMC Pregnancy Childbirth. 2022;22(1):290. doi:10.1186/s12884-022-04636-9
39. Kell DB, Pretorius E. Serum ferritin is an important inflammatory disease marker, as it is mainly a leakage product from damaged cells. Metallomics. 2014;6(4):748–773. doi:10.1039/c3mt00347g
40. Suchdev PS, Williams AM, Mei Z, et al. Assessment of iron status in settings of inflammation: challenges and potential approaches. Am J Clin Nutr. 2017;106(Suppl6):1626S–1633S. doi:10.3945/ajcn.117.155937
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.