")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Association Between Serum Asprosin and Diabetic Nephropathy in Patients with Type 2 Diabetes Mellitus in the Community: A Cross-Sectional Study
Authors Xu L, Cui J, Li M, Wu Q, Liu M, Xu M, Shi G, Yin J, Yang J
Received 24 February 2022
Accepted for publication 9 June 2022
Published 18 June 2022 Volume 2022:15 Pages 1877—1884
DOI https://doi.org/10.2147/DMSO.S361808
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ming-Hui Zou
Linxin Xu,1,2,* Junfang Cui,3,* Mina Li,2 Qianqian Wu,2 Ming Liu,2 Minggang Xu,4 Guoliang Shi,4 Jianhong Yin,2 Jing Yang1,2
1First Clinical Medical College, Shanxi Medical University, Taiyuan, People’s Republic of China; 2Department of Endocrinology, First Hospital of Shanxi Medical University, Shanxi Medical University, Taiyuan, Shanxi, 030001, People’s Republic of China; 3Department of Geratology, First Hospital of Shanxi Medical University, Shanxi Medical University, Taiyuan, 030001, People’s Republic of China; 4Department of Endocrinology, Changzhi Second People’s Hospital, Changzhi, 046000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Yang; Jianhong Yin, Tel +86-351-4639756, Email [email protected]; [email protected]
Objective: To explore the association between serum asprosin and diabetic nephropathy (DN) in patients with type 2 diabetes mellitus (T2DM) in the community.
Methods: In this cross-sectional study, we retrospectively collected the clinical data of T2DM patients from a community health service center in southeastern Shanxi Province between November 2019 and July 2021. Logistic regression analysis was used to calculate the odds ratio (OR) and the 95% confidence interval (95% CI) of asprosin levels on the risk of DN.
Results: Among 498 T2DM patients included in this study, 221 had microalbuminuria, 105 had massive albuminuria, and 172 did not have any signs of nephropathy. Serum asprosin level was positively correlated with diastolic blood pressure, body mass index, triglycerides, aspartate aminotransferase, alanine aminotransferase, creatinine, ACR and albumin-to-creatinine ratio (all P < 0.05) and negatively correlated with low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, fasting plasma glucose, HbA1c and estimated glomerular filtration rate (all P < 0.05). After adjusting for covariates, increased asprosin was associated with diabetic nephropathy (all OR = 2.560, 95% CI: 1.1592– 4.116; P < 0.001).
Conclusion: The risk of DN significantly increases with serum asprosin levels, especially among female patients.
Keywords: asprosin, type 2 diabetes mellitus, diabetic nephropathies, creatinine, albuminuria, logistic models, community health services
Background
Asprosin is a recently discovered fasting-induced protein hormone mainly secreted by the white adipose tissue and recruited by the liver and brain.1,2 Plasma asprosin levels can be modulated by physical activity, where anaerobic exercises increase their level, while aerobic exercises decrease it.2 When reaching the liver, asprosin exerts a glucogenic effect through an olfactory G-protein-coupled receptor (OR4M1), and upon crossing the blood–brain barrier, it stimulates appetite-modulating neurons in the arcuate nucleus of the hypothalamus.3 Recent experimental and clinical studies have shown that serum asprosin concentration is higher in subjects with metabolic syndrome and T2DM compared to controls.4 Serum asprosin was found to be positively related to the systolic blood pressure, blood urea nitrogen, creatinine, uric acid, calcium channel blockers, while negatively related with glomerular filtration rate, metformin, and acarbose therapy;5 however, its specific pathways and targets are not yet fully understood.
Diabetic nephropathy (DN) is one of the most common T2DM complications, which often results in end-stage renal disease being the major cause of T2DM death.6 In the series of recently published clinical studies, increased circulating asprosin levels were associated with the early stage of DN in T2DM,7,8 as well as the progression of DN and renal function,5 thus suggesting a possible role of adipokines in the pathogenesis of both T2DM and nephropathy. It is evidenced by serum asprosin level being independently correlated with urinary albumin/creatinine ratio in T2DM patients6 that circulating asprosin may affect the renal homeostasis via insulin resistance, multiple cytokine imbalance, chronic inflammation and endothelial dysfunction. However, the specific role of asprosin in DN, its relationship with glucose and lipid metabolism, markers of inflammation, and renal function need to be further investigated.
The purpose of this cross-sectional study was to explore the association between serum asprosin and diabetic nephropathy in patients with type 2 diabetes mellitus in the community setting and evaluate its prognostic value for future clinical practice.
Methods
Study Design and Subjects
In this cross-sectional study, we retrospectively collected the clinical data of type 2 diabetic patients from a community health service center in southeastern Shanxi Province between November 2019 and July 2021. Inclusion criteria related to T2DM patients who met the WHO diagnostic criteria for T2DM in 1999.9 Exclusion criteria were the following: 1) patients with type 1 diabetes mellitus; 2) diabetes caused by other endocrine diseases; 3) diabetic ketoacidosis and diabetic hyperosmolar coma; 4) urinary tract infection; 5) patients with severe dysfunction of the liver, kidney and other organs, severe infection and malignant tumor; 6) patients with communication disorders such as mental illness.
This study was approved by the ethics committee of the First Hospital of Shanxi Medical University (No. 2019 [K056]), and all study participants provided informed written consent. The study kept patient data confidential and complied with the Declaration of Helsinki.
Grouping and Serum Asprosin Detection
Before asprosin detection, all participants fasted for 8–10h. Venous blood was collected the next morning and centrifuged for 15 minutes, after which supernatant was absorbed to determine serum asprosin level. Centrifuge (3000 rpm, 13.5 cm radius) for 15 min, take the supernatant, and all blood samples were stored at −80℃. Serum asprosin level was determined by enzyme-linked immunosorbent assay (ELISA) method using a ready-to-use detection kit by Herb (Shanghai, Biotechnology Co., LTD). All samples were tested by double-well repetition, with inter-batch difference <11% and intra-batch difference <8%. According to the tertile of serum asprosin, all patients were divided into three subgroups: low-level asprosin group (T1), medium-level group (T2), and high-level asprosin group (T3).
Participants were additionally divided into three groups, according to the urinary albumin-to-creatinine ratio (ACR)10 that was repeatedly detected for 3 times, or urinary albumin that was increased 2 out of 3 times, excluding infection and other factors. According to the value of the ACR, the participants were divided into a standard group (ACR < 30 mg/g), microalbuminuria group (30≤ ACR ≤300 mg/g), and macroalbuminuria group (ACR > 300 mg/g).
Data Collection and Definition
Height, weight, waist circumference, and blood pressure of the patients were collected, and the Body Mass Index (BMI) (weight/(height*height)) was calculated. Criteria for the diagnosis of hypertension was based on the Chinese Guidelines for the Prevention and Treatment of Hypertension (2010)[systolic blood pressure ≥ 140 and/or diastolic blood pressure ≥90mmHg (1mmHg = 0.133kpa)]. Experienced nurses collect venous blood samples (empty stomach and 2 hours after meals), the blood volume is about 2–3mL. It is used to measure aspartate transaminase (AST) (Reference range 15–40 U/L), alanine aminotransferase (ALT) (Reference range 9–50 U/L), serum uric acid (SUA) (Reference range 210–440µmol/L), creatinine (CRE) (Reference range 64–104µmol/L), total cholesterol (TC) (Reference range 64–104µmol/L), triglycerides (TG) (Reference range 0.2–1.7mmol/L), low-density lipoprotein cholesterol (LDL-C) (Reference range 0–3.12mmol/L), high-density lipoprotein cholesterol (HDL-C) (Reference range ≧1.04mmol/L), fasting blood glucose (FPG) (Reference range 3.9–6.1 mmol/l), and 2-hour blood glucose (2hPG) (Reference range 3.9–7.9mmol/L) were collected. Furthermore, urinary albumin/creatinine, glycosylated hemoglobin (HbA1c) (Reference range 4.8–5.9%), glomerular filtration rate (eGFR), and asprosin levels were also collected.
Estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula proposed by Levey et al11 for female, eGFR (mL/min per 1.73 m2) = 144× [Scr (mg/dL)/0.7]−0.329 × [0.993] age if Scr ≤0.7 mg/dL and 144× [Scr (mg/dL)/0.7]−1.209 × [0.993]age if Scr >0.7 mg/dL; and for male, eGFR (mL/min per 1.73 m2) = 141× [Scr (mg/dL)/0.9]−0.411 × [0.993]age if Scr ≤0.9 mg/dL and 141× [Scr (mg/dL)/0.7]−1.209 × [0.993]age if Scr >0.9 mg/dL.
Statistical Analysis
SPSS 22.0 (IBM Corp., Armonk, NY, USA) was used for data analysis. The Q-Q plots were employed for normality testing. The data conforming to the normal distribution were presented in the form of mean ± standard deviation (mean ± SD), and those not conforming to the normal distribution were presented in the form of the median (range). The categorical data were presented as frequency (constituent ratio or percentage). Analysis of variance or Kruskal–Wallis H-test was used to compare the statistical differences of quantitative data, while Chi-square test or Fisher exact test was used for categorical data. With regard to the analysis of the correlation between serum asprosin and other variables of the patients, the Pearson correlation coefficient was calculated when the data met bivariate normal distribution; otherwise, the Spearman correlation coefficient was calculated. Multivariate stepwise linear regression were used to analyze the associations of SUA with age, duration of T2DM, SBP, DBP, BMI, TC, TG, LDL-C, HDL-C, FPG, HbA1c, AST, ALT, Cre, ACR and eGFR. Univariate and multivariate logistic regression analyses were performed to identify factors independently associated with DN in patients with T2DM. The multivariate logistic regression analysis used the “enter” method (ie, simultaneous entry of all factors into the logistic regression equation), and odds ratios (ORs) and 95% confidence intervals (95% CIs) were calculated. Two models were used for the multivariate logistic regression analyses: Model 1, without adjusted variable; Model 2, with adjusted for duration of diabetes mellitus, systolic blood pressure, glycated hemoglobin, estimated glomerular filtration rate; Model 3, model 2 with additional adjustment for age, BMI, triglycerides and ACEI/ARB drug use; sersum asprosin tertile 1, <295.4 pg/mL for total, <282.0 pg/mL for male and <266.2 pg/mL for female; sersum asprosin tertile 2, 295.4–367.0 pg/mL for total, 282.0–315.6 pg/mL for male and 266.2–344.5 pg/mL for female; sersum asprosin tertile 3, >344.5 pg/mL for total, >315.6 pg/mL for male and >344.5 pg/mL for female. P < 0.05 was considered statistically significant.
Results
Of the 498 patients with type 2 diabetes included in this study, 221 had microalbuminuria, 105 had macroalbuminuria, and 172 had no evidence of any renal disease. To indicate covariates affecting the urinary albumin-to-creatinine ratio in this study, patients were classified according to the presence or absence of microalbuminuria (30 ≤ ACR ≤ 300 mg/g) and macroalbuminuria (ACR > 300 mg/g). SBP, ALT, TG, FPG, HbA1c, SUA, CRE, asprosin (P < 0.05) were significantly higher in the microalbuminuria and macroalbuminuria groups than those without albuminuria (P < 0.05)), while eGFR (P < 0.05) was significantly lower than in non-albuminuric participants, both male and female. BMI was significantly higher in the microalbuminuria and macroalbuminuria groups in all and female (P < 0.05), there was no statistical difference in BMI among male patients (P>0.05), but there was an increasing trend. Patients with microalbuminuria and macroalbuminuria had longer disease duration and blood pressure than normal subjects. Additionally, subjects with microalbuminuria had a higher ratio of angiotensin-converting enzyme inhibitor (ACEI)/angiotensin II receptor blocker (ARB) compared to participants without albuminuria. The detailed characteristics of the included patients are shown in Table 1.
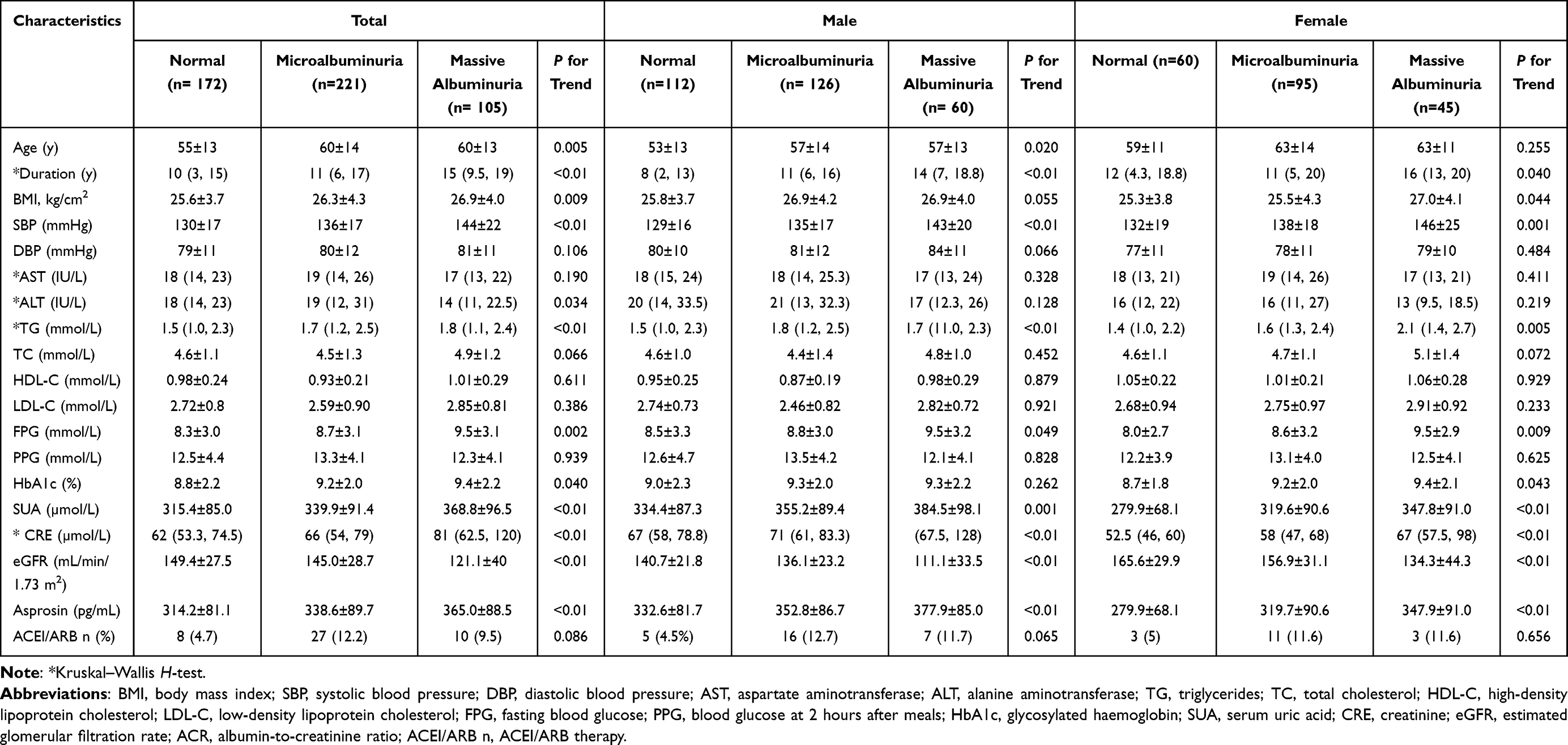 |
Table 1 Comparison of the Clinical Characteristics of Patients with T2DM in the Community Between Those with DN and Those without DN |
Pearson correlation analysis showed that serum asprosin level was positively correlated with diastolic blood pressure (DBP), BMI, triglycerides (TG), aspartate Aminotransferase (AST), alanine Aminotransferase (ALT), creatinine, and ACR (P < 0.05), and negatively correlated with low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), FPG, HbA1c, and eGFR (P < 0.05) (Table 2). In addition, in both male and female patients, the level of asprosin was positively correlated with BMI, TG, AST, ACR, and creatinine (P < 0.05) and negatively correlated with HDL-C and eGFR (P < 0.05). Specifically, in male patients, asprosin was positively correlated with ALT (P < 0.05), and negatively correlated with FPG and HbA1c (P < 0.05) (Table 2). Multiple linear regression analysis (using the stepwise method) revealed that BMI (positively), ACR (positively) and eGFR (negatively) were independently related to asprosin in total, male and female with T2DM (P < 0.05) (Table 2). Multiple linear regression also indicated that asprosin level was positively associated with AST (P < 0.05), and negatively correlated with FPG in total and male (P < 0.05) but not female (P>0.05) (Table 2). Asprosin level was positively associated with TG in total and female (P < 0.05) but not male (P>0.05) (Table 2).
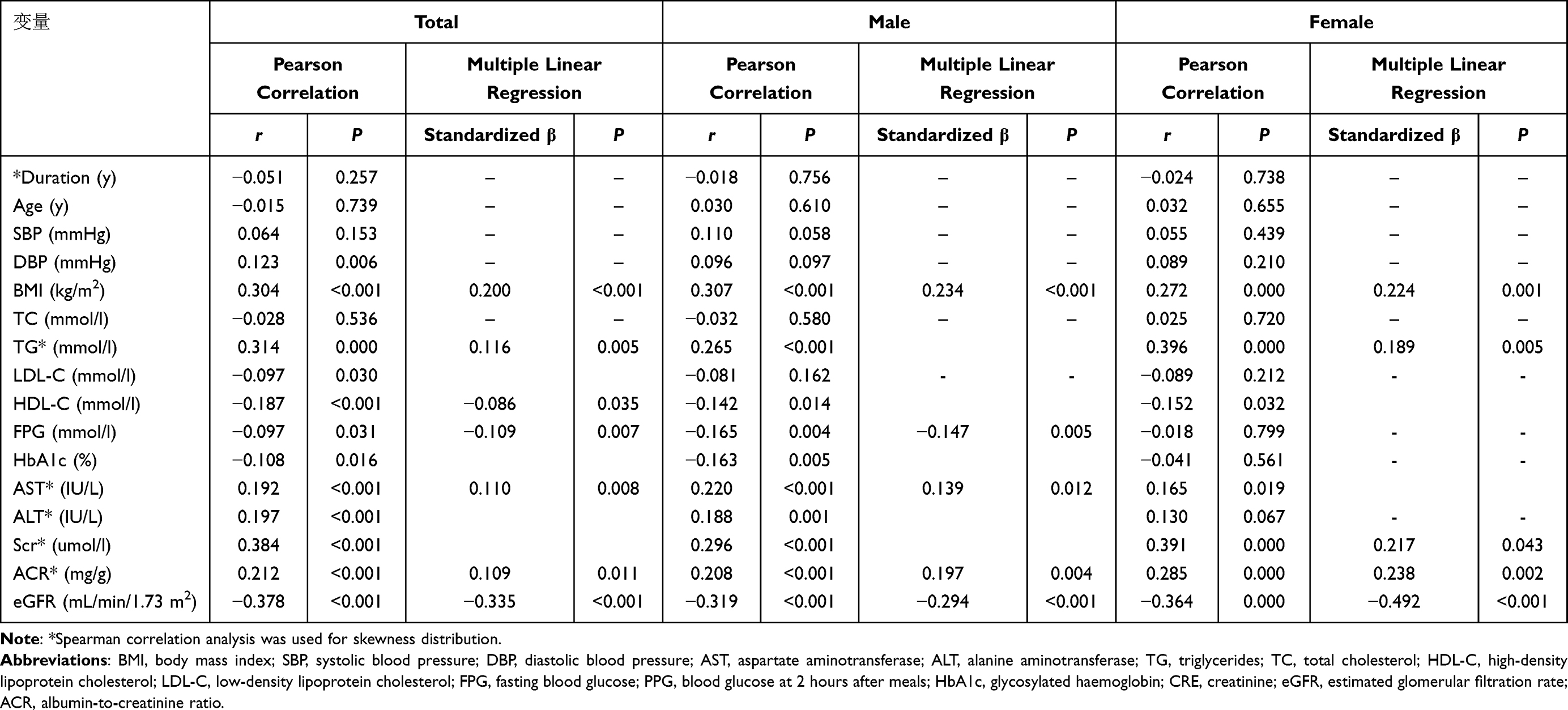 |
Table 2 Association Between Serum Asprosin and Other Covariates in Patients with Type 2 Diabetes |
Logistic regression analysis (using asprosin tertile 1 as the reference group) after adjustment for duration of diabetes mellitus, systolic blood pressure, glycated hemoglobin, estimated glomerular filtration rate revealed that the odds of DN were significantly increased for tertile 2 and tertile 3 in total patients, in male and in female (Table 3). After further adjustment for age, BMI, triglycerides and ACEI/ARB drug use, asprosin tertiles were not associated with DN in male, whereas the odds of DN remained significantly elevated for tertile 3 in female(Table 3). However, there appeared to be trends toward increased odds of DN for tertile 2 and 3 in male (P value for trend= 0.129) (Table 3).
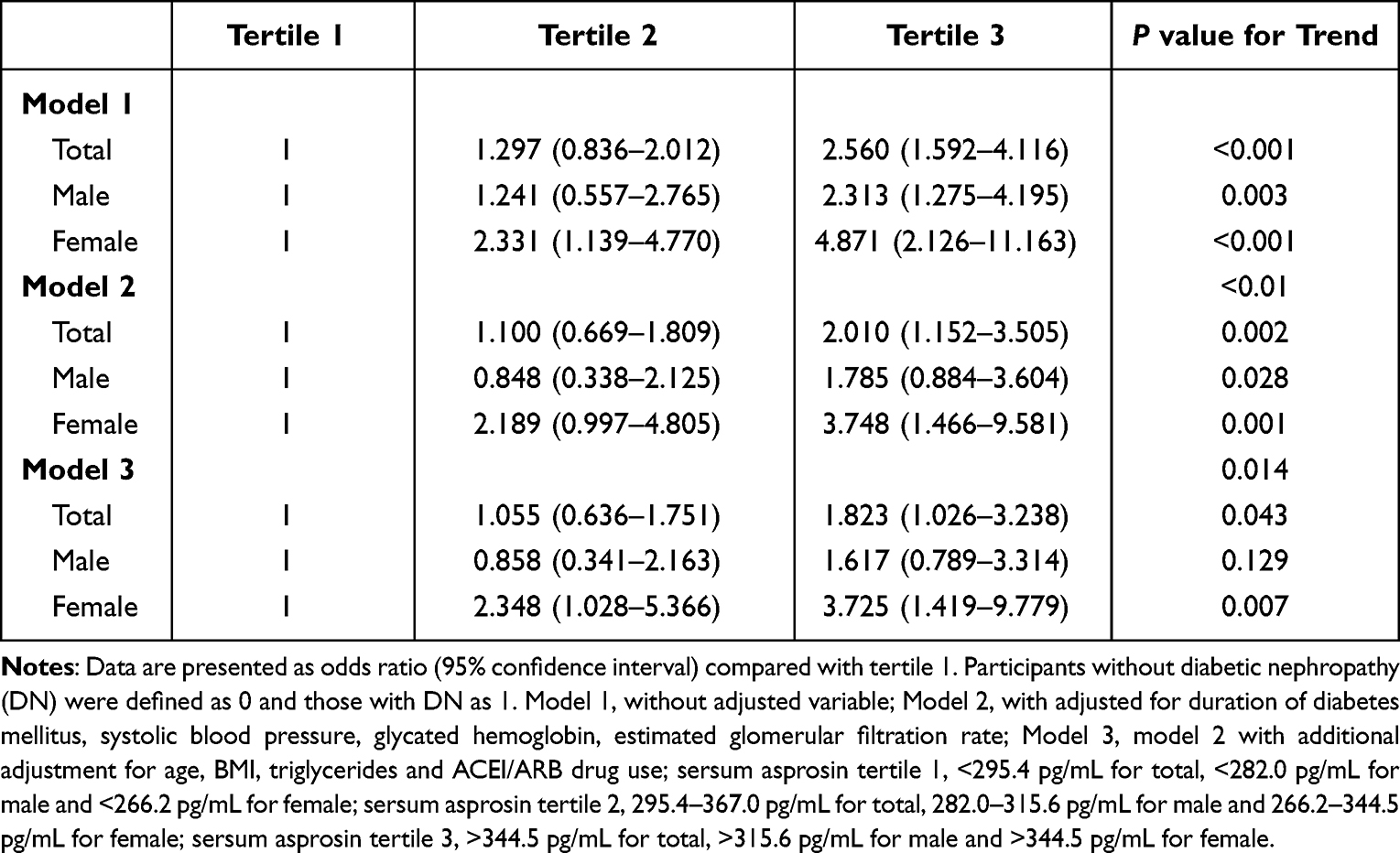 |
Table 3 Multiple Stepwise Logistic Regression Analysis of the Ratio of Serum Asprosin to Risk of Diabetic Nephropathy |
The prevalence of DN according to tertiles of asprosin. When all study participants were analyzed together, the prevalence of DN increased progressively from the lowest asprosin tertile to the highest asprosin tertile (56.6%, 62.9% and 76.9%; P for trend <0.001). Progressive increases in DN prevalence with increasing asprosin tertile (from lower to upper) were also observed in male (48.3%, 53.7% and 68.3%; P for trend <0.001) and female (53.0%, 72.5% and 84.6%; P for trend <0.001).
Discussion
The aim of this retrospective cross-sectional study was to explore the association between new serum prognostic marker asprosin and diabetic nephropathy in patients with type 2 diabetes mellitus in the community setting. Our results revealed that patients with T2DM in the community was that asprosin was higher in the massive albuminuria group than in the normal group and microalbuminuria group for both women and men. Serum asprosin level was positively correlated with DBP, BMI, TG, AST, ALT, creatinine, and ACR, and negatively correlated with LDL-C, HDL-C, FPG, HbA1c, and eGFR. Results of multiple stepwise logistic regression analysis showed that increased serum level of asprosin (upper tertile) was the independent risk factor for diabetic nephropathy in T2DM patients, especially among female patients. To the best of our knowledge, the present study is among the first clinical reports on asprosin in diabetic nephropathy, with the additional advantage of a large sample size and community setting.
The comprehensive management of T2DM patients in the community is the key and weak link in the comprehensive prevention and treatment of diabetes.12 The prevention and treatment of diabetic nephropathy requires early intervention on the risk factors of diabetic nephropathy while controlling blood sugar, so as to minimize the risk of death. Few studies have previously reported an association between elevated serum asprosin and T2DM,4–8 especially in community-based patients with type 2 diabetes. A community study involving 30 subjects with normal glucose tolerance, 42 T2DM patients without diabetic nephropathy (DKD), and 33 T2DM patients with early DKD7 reported significantly increased ORs for early diabetic nephropathy. Asprosin may be associated with diabetic microvascular complications. A recent study involving 212 hospitalized patients with T2DM reported an association between elevated serum asprosin concentrations and DN in logistic regression analysis. The results obtained in this study after adjusting for covariates by analyzing community-based T2DM patients by sex are consistent with previous reports showing that patients in the upper asprosin tertile had a significantly increased risk of diabetic nephropathy. Furthermore, we found that elevated asprosin levels were associated with an increased prevalence of DN. Despite a larger sample size, including a higher proportion of female patients and other variability compared to previous studies, asprosin was associated with renal function, ACR persisted (r=0.384, P<0.001 for creatinine; r=0.212, P<0.001). 0.001 ACR). Circulating asprosin can be used as a novel serum biomarker for DN assessment.
The function of asprosin under physiological conditions, although not completely understood, seems to be opposite to that of insulin, with low glucose levels (fasting) stimulating asprosin production and high levels (feeding condition) inhibiting it.13 In obese cases, insulin resistance or diabetes, asprosin levels are pathologically elevated, increasing appetite and disturbing the energy homeostasis,4,14 while administration of anti-asprosin antibodies can both normalize its concentration and reduce food intake.2 Accordingly, in the clinical setting asprosin was found to be negatively correlated with changes in blood glucose (r = −0.502, P < 0.001) and changes in C-peptide (r = −0.467, P < 0.001) in individuals with normal glucose tolerance, but not in T2DM patients.4 Circulating asprosin levels were also found to be negatively correlated with eGFR (r = - 0.311, P = 0.007) and positively correlated with ACR (r = 0.345, P = 0.002),7 as well as HbA1c, FBG, TC, LDL-C, IL-6, and TNF-α in T2DM patients.8 In the present study, the obtained results confirmed expected positive correlation links between serum asprosin and BMI, TG, AST, ALT, creatinine, and ACR, negative links with LDL-C, HDL-C, FPG, HbA1c, and eGFR, among which creatinine and eGFR had the strongest correlation coefficient. One of the less expected findings was the weak link between asprosin and DBP (but not SBP), more prominent in male patients, which was also mentioned in the study by Deng et al6 in T2DM and by Wang et al15 in obese children who are insulin resistant. Those findings might be partly explained by the ability of asprosin to modulate cardiac mitochondrial functions16 and the relationship between DBP and exercising in the conditions of cholesterolemia and insulin resistance.17,18 Future studies should further explore the relationship between exercising and asprosin in T2DM.
It is important to note that asprosin circulation under physiological conditions as well as in T2DM has a distinct gender characteristic.19,20 All previous studies have reported that plasma levels of asprosin are lower in women,4–8 while the link between exercising effort and increase in asprosin is stronger.21 The present study was undertaken in the community setting, which allowed us to exclude some external factors and compare representative samples of male and female T2DM patients. We found that although serum levels were lower in the female population, links to ACR and creatinine were more evident, negative link to HbA1c was weak and insignificant (r=−0.041, P=0.561), while correlation links to ALT and AST were present only in the male population. As there is a notable lack of studies focusing on gender differences and statistically insignificant inclusion of female patients into recent asprosin studies, it is of essential importance to further explore these differences and the relationship between asprosin and DN, specifically in the female population.
This study has certain limitations. First, this was a cross-sectional study that assessed asprosin in a nonuniform manner at different points of time; thus, we did not discuss dynamic changes of serum asprosin level and the incidence of diabetic nephropathy. Second, affected by factors such as region, sample size, population characteristics, etc, whether there is a causal relationship between serum asprosin and DN needs to be confirmed by future prospective studies. Last, physical activity and medication were not evaluated in this study, so the effect on asprosin could not be more clearly reflected, which is also a limitation of this study.
Conclusion
Elevated serum asprosin was associated with the occurrence of diabetic nephropathy in community T2DM patients in Changzhi City, Shanxi Province, and with the increase of serum asprosin level, the risk of diabetic nephropathy was significantly increased, especially in women. It is suggested that asprosin may play a role in the occurrence and development of diabetic nephropathy in T2DM patients. Therefore, serum asprosin level is expected to be a predictor of early diagnosis of diabetic nephropathy, and future studies should consider the relationship between asprosin and DN in female population.
Funding
This study was supported by the China Diabetes Research Fund, China Foundation for International Medical Exchanges (Z-2017-26-1902-3) and the Youth Scientific research project of Basic Research Program of Shanxi Province (20210302124289).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Luís C, Fernandes R, Soares R, von Hafe P. A state of the art review on the novel mediator asprosin in the metabolic syndrome. Porto Biomed J. 2020;5(6):e108. doi:10.1097/j.pbj.0000000000000108
2. Mazur-Bialy AI. Asprosin-A fasting-induced, glucogenic, and orexigenic adipokine as a new promising player. Will it be a new factor in the treatment of obesity, diabetes, or infertility? A review of the literature. Nutrients. 2021;13(2):620. doi:10.3390/nu13020620
3. Hoffmann JG, Xie W, Chopra AR. Energy regulation mechanism and therapeutic potential of asprosin. Diabetes. 2020;69(4):559–566. doi:10.2337/dbi19-0009
4. Zhang X, Jiang H, Ma X, Wu H. Increased serum level and impaired response to glucose fluctuation of asprosin is associated with type 2 diabetes mellitus. J Diabetes Investig. 2020;11(2):349–355. doi:10.1111/jdi.13148
5. Wang R, Lin P, Sun H, Hu W. Increased serum asprosin is correlated with diabetic nephropathy. Diabetol Metab Syndr. 2021;13(1):51. doi:10.1186/s13098-021-00668-x
6. Deng X, Zhao L, Guo C, et al. Higher serum asprosin level is associated with urinary albumin excretion and renal function in type 2 diabetes. Diabetes Metab Syndr Obes. 2020;13:4341–4351. doi:10.2147/DMSO.S283413
7. Zhang H, Hu W, Zhang G. Circulating asprosin levels are increased in patients with type 2 diabetes and associated with early-stage diabetic kidney disease. Int Urol Nephrol. 2020;52(8):1517–1522. doi:10.1007/s11255-020-02509-8
8. Goodarzi G, Setayesh L, Fadaei R, et al. Circulating levels of asprosin and its association with insulin resistance and renal function in patients with type 2 diabetes mellitus and diabetic nephropathy. Mol Biol Rep. 2021;48(7):5443–5450. doi:10.1007/s11033-021-06551-2
9. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
10. American Diabetes Association. 11. Microvascular complications and foot care: standards of medical care in diabetes-2021 [published correction appears in Diabetes Care. 2021 Sep;44 (9): 2186–2187]. Diabetes Care. 2021;44(Suppl 1):S151–S167. doi:10.2337/dc21-S011
11. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate [published correction appears in Ann Intern Med. 2011 Sep 20;155 (6): 408]. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
12. Miklavcic JJ, Fraser KD, Ploeg J, et al. Effectiveness of a community program for older adults with type 2 diabetes and multimorbidity: a pragmatic randomized controlled trial. BMC Geriatr. 2020;20(1):174. doi:10.1186/s12877-020-01557-0
13. Romere C, Duerrschmid C, Bournat J, et al. Asprosin, a fasting-induced glucogenic protein hormone. Cell. 2016;165(3):566–579. doi:10.1016/j.cell.2016.02.063
14. Duerrschmid C, He Y, Wang C, et al. Asprosin is a centrally acting orexigenic hormone. Nat Med. 2017;23(12):1444–1453. doi:10.1038/nm.4432
15. Wang M, Yin C, Wang L, et al. Serum asprosin concentrations are increased and associated with insulin resistance in children with obesity. Ann Nutr Metab. 2019;75(4):205–212. doi:10.1159/000503808
16. Wen MS, Wang CY, Yeh JK, et al. The role of Asprosin in patients with dilated cardiomyopathy. BMC Cardiovasc Disord. 2020;20(1):402. doi:10.1186/s12872-020-01680-1
17. Brett SE, Ritter JM, Chowienczyk PJ. Diastolic blood pressure changes during exercise positively correlate with serum cholesterol and insulin resistance. Circulation. 2000;101(6):611–615. doi:10.1161/01.cir.101.6.611
18. Schultz MG, Sharman JE. Exercise hypertension. Pulse. 2014;1(3–4):161–176. doi:10.1159/000360975
19. Li X, Liao M, Shen R, et al. Plasma asprosin levels are associated with glucose metabolism, lipid, and sex hormone profiles in females with metabolic-related diseases. Mediators Inflamm. 2018;2018:7375294. doi:10.1155/2018/7375294
20. Wei F, Long A, Wang Y. The Asprosin-OLFR734 hormonal signaling axis modulates male fertility. Cell Discov. 2019;5:55. doi:10.1038/s41421-019-0122-x
21. Wiecek M, Szymura J, Maciejczyk M, Kantorowicz M, Szygula Z. Acute anaerobic exercise affects the secretion of asprosin, irisin, and other cytokines - a comparison between sexes. Front Physiol. 2018;9:1782. doi:10.3389/fphys.2018.01782
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.