")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Association Between Rural Residence and In-Hospital and 30-Day Mortality Among Veterans Hospitalized with COPD Exacerbations
Authors Fortis S, O'Shea AMJ , Beck BF, Comellas A , Vaughan Sarrazin M , Kaboli PJ
Received 11 September 2020
Accepted for publication 11 December 2020
Published 2 February 2021 Volume 2021:16 Pages 191—202
DOI https://doi.org/10.2147/COPD.S281162
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Richard Russell
Spyridon Fortis,1,2 Amy MJ O’Shea,1,3 Brice F Beck,1 Alejandro Comellas,1,2 Mary Vaughan Sarrazin,1,3 Peter J Kaboli1,3
1Center for Access & Delivery Research & Evaluation (CADRE), Iowa City VA Health Care System, Iowa City, IA, USA; 2Pulmonary, Critical Care and Occupational Medicine, University of Iowa Hospitals and Clinics, Iowa City, IA, USA; 3Department of Internal Medicine, Division of General Internal Medicine, University of Iowa Roy J. and Lucille A. Carver College of Medicine, Iowa City, IA, USA
Correspondence: Spyridon Fortis
Pulmonary, Critical Care and Occupational Medicine, University of Iowa Hospitals and Clinics, 200 Hawkins Drive – C33 GH, Iowa City, IA 52242, USA
Email [email protected]
Background: We explored the relationship between rural residency and in-hospital mortality in patients hospitalized with COPD exacerbations.
Methods: We retrospectively analyzed COPD hospitalizations from 2011 to 2017 at 124 acute care Veterans Health Administration (VHA) hospitals in the US. Patient residence was classified using Rural Urban Commuting Area codes as urban, rural, or isolated rural. We stratified patient hospitalizations into quartiles by travel time from patient residence to the nearest VHA primary care provider clinic and hospital. Multivariate analyses utilized generalized estimating equations with a logit link accounting for repeated hospitalizations among patients and adjusting for patient- and hospital-level characteristics.
Results: Of 64,914 COPD hospitalizations analyzed, 43,549 (67.1%) were for urban, 18,673 (28.8%) for rural, and 2,692 (4.1%) for isolated rural veterans. In-hospital mortality was 4.9% in urban, 5.5% in rural, and 5.2% in isolated rural veterans (P=0.008). Thirty-day mortality was 8.3% in urban, 9.9% in rural, and 9.2% in isolated rural veterans (P< 0.001). Travel time to a primary care provider and VHA hospital was not associated with in-hospital mortality among isolated rural and rural veterans. In the multivariable analysis, compared to urban veterans, isolated rural patients did not have increased mortality. Rural residence was not associated with in-hospital (OR=0.87; 95% CI=0.67– 1.12, P=0.28) but was associated with increased 30-day mortality (OR=1.13; 95% CI=1.04– 1.22, P=0.002). Transfer from another acute care hospital (OR=14.97; 95% CI=9.80– 17.16, P< 0.001) or an unknown/other facility (OR=33.05; 95% CI=22.66– 48.21, P< 0.001) were the strongest predictors of increased in-hospital mortality compared to patients coming from the outpatient sector. Transfer from another acute care facility was also a risk factor for 30-day mortality.
Conclusion: Potential gaps in post-discharge care of rural veterans may be responsible for the rural–urban disparities. Further research should investigate the exact mechanism that inter-hospital transfers affect mortality.
Keywords: pulmonary disease, chronic obstructive, epidemiology, mortality
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of mortality in the US1 and worldwide2 and is associated with high morbidity3 and resource utilization,3 including costs due to clinic visits, chronic therapy, and frequent hospitalizations.3,4 Patients with COPD experience exacerbations of the disease, defined as worsening of their respiratory symptoms, which occur more often as the disease progresses. Severe COPD exacerbations requiring admission to the hospital are associated with increased mortality,5–9 and are responsible for 70% of the direct healthcare costs of the disease.4,10
The prevalence of COPD is approximately 8% and 5% in adults living in rural and urban areas, respectively, according to a Center of Disease Control (CDC) report.11 In 2015, rural Medicare patients experience 27% more hospitalizations and 71% more deaths than urban patients.11 Rural residence is also an independent risk factor for COPD exacerbations and this association persists after accounting for lung function and demographics.12
Rural residence is an independent risk factor for 30-day hospital mortality in patients hospitalized with COPD exacerbation after adjusting for patient- and hospital-level characteristics.13 Rural patients hospitalized with COPD exacerbations have higher 30-day mortality relative to urban patients13 which may result from suboptimal care prior to, during, or after hospitalization. Suboptimal care prior to COPD hospitalization or delay to receive appropriate care due to poor access may result in increased mortality among rural patients.14 It is unknown whether the rural residence is a risk factor for in-hospital mortality. We hypothesized that rural COPD patients have increased in-hospital mortality compared to urban patients. To investigate our hypothesis, we examined mortality of all COPD hospitalizations in the Veterans Health Administration (VHA) for rural and urban veterans. Moreover, we examined whether demographics, comorbidities, transfer from another hospital, hospital-level characteristics, and travel time to the nearest VHA primary care provider or hospital can explain the disparity in mortality between rural and urban patients.
Methods
This retrospective cohort study included all hospitalizations for a COPD exacerbation to 124 acute care VHA hospitals with a discharge date between October 1, 2011 (fiscal year 2011) to September 30, 2017 (fiscal year 2017). More than 9 million veterans are enrolled in the VHA, the largest health system in the US, with 1,255 inpatient and outpatient health care facilities.15 This work was approved by the Institutional Review Boards and Research and Development Committee at the Iowa City VA Health Care System [IRB 201712713]. The study was conducted in accordance with the Declaration of Helsinki. Patient informed consent was not required by Institutional Review Boards and Research and Development Committee at the Iowa City VA Health Care System because the study examined only existing patient-level data. Patients’ data were kept confidential.
Setting
We extracted data for hospitalizations between October 1, 2011 (fiscal year 2011) to September 30, 2017 (fiscal year 2017) from the Veterans Informatics and Computing Infrastructure (VINCI), an integrated system that includes VHA’s electronic health records and administrative data retrospectively after October 2018. Admissions to VHA acute care hospitals were identified via the Corporate Data Warehouse using the inpatient domain. These datasets contain patient demographics including residential address and ZIP code, diagnosis, and procedure codes during admission, admission source, admission, and discharge dates.
Definitions
The study cohort was identified by the International Classification of Diseases, Ninth and Tenth Revisions, Clinical Modification (ICD-9-CM and ICD-10-CM) using 1) a principal diagnosis of COPD exacerbation (ICD-9-CM codes: 491.xx, 492.x, 429.0, or 496 or ICD-10-CM codes: J41, J43, J43.1, J43.2, J43.8, J43.9, J44.0, J44.1, J41.8, J42, or J44.9) or 2) a principal diagnosis of acute respiratory failure (ICD-9-CM: 518.81, 518.82, or 518.84; ICD-10-CM: J96.00, J96.01, J96.02, J96.11, J96.12, J96.20, J96.21, J96.22, J96.90, J96.92, or R06.03) with a secondary COPD diagnosis as previously done.16 Although the accuracy of ICD codes to diagnose COPD is above 70%, especially in the elderly individuals,17–19 we validated the accuracy using spirometric and radiographic data from our facility. We found that of 285 patients with a COPD diagnosis based on ICD codes, 226 (79.3%) had an FEV1/FVC<0.7 and/or an FEV1<80% with a residual volume or residual volume/total lung capacity ratio>120%, and another 29 (10.2%) had radiographic emphysema in the chest CT by the radiology report (total 89.5% of patients had objective findings of COPD).
Patient and facility rurality were defined using ZIP codes based on the Rural Urban Commuting Area (RUCA) codes. RUCA codes reflect measures of urbanization, commuting, and population density.13,–20–23 RUCA codes were further condensed to designate an area as urban (RUCA codes: 1 and 1.1), rural (RUCA codes: 2, 2.1, 3, 4, 4.1, 5, 5.1, 6, 7, 7.1, 7.2, 8, 8.1, 8.2, and 9), and isolated rural (RUCA codes: 10, 10.2, 10.2, and 10.3) categories as defined by the VHA Office of Rural Health.24
A series of variables for each patient were created indicating: 1) risk-adjustment variables describing baseline patient characteristics, such as age, sex, Area Deprivation Index (ADI), race, and comorbidities; 2) travel time to a VHA primary care provider and VHA hospital; and 3) facility characteristics including COPD-case volume and facility complexity. ADI reflects socio-economic level of patient’s residential location.25,26 Comorbidities were defined using ICD-9-CM and ICD-10-CM diagnosis codes within 1 year of admission in either the inpatient, outpatient, or fee basis data files, except pneumonia which was defined based on the presence of the corresponding diagnosis code during the hospitalization as previously.27 In addition, obstructive sleep apnea was defined using ICD-9 diagnosis codes 327.2 or 780.57, or ICD-10 diagnosis codes G47.30–G47.39. We also obtained laboratory values that can be reliably retrieved in medical records: hematocrit, white blood cells, serum sodium, and creatinine within 24 hours (most abnormal) from the admission.13 Admission from another acute care hospital (inter-hospital transfer) was defined as direct transfer from another hospital without transfer to another lower intensity facility. If the patient transferred from another facility with unknown characteristics, that facility was defined as unknown/other facility. Travel time to the nearest VHA primary care physician and VHA hospital was determined from VHA Planning Systems and Support Group (PSSG) geo-coded enrollment files. PSSG calculates distances to the nearest primary and tertiary care VHA sites for all VHA enrolled patients using actual longitude and latitude coordinates of VHA patient residences and nearest VHA facilities. Travel distances are estimated using geospatial technologies that reflects roads and average driving conditions.13
Hospital rurality was defined according to the RUCA algorithm and the ZIP code of the facility. Hospital complexity was defined by the VHA as 1 (high resource), 2 (medium resource), and 3 (low resource).24 Hospital COPD-case volume was classified as high (above the median) or low (below the median) based on their total COPD volume during the study period.
Admissions with a missing patient residential rurality classification (n=885) and admissions to VHA hospitals in US territories (ie, Puerto Rico, US Virgin Islands, and American Samoa) were excluded (n=428). We also excluded admissions to non-acute care VHA hospitals (n= 2,282).
Outcomes
The primary outcome, in-hospital mortality, was defined using the date of death listed in the VHA Vital Status File and the occurrence of this date between the admission and discharge date inclusive. The secondary outcome, 30-day mortality, was defined as the occurrence of death within 30 days from admission.
Statistical Analysis
Unadjusted bivariate analyses were performed to compare patient-level and hospital-level characteristics between urban, rural, and isolated rural veterans using ANOVA test for continuous or chi-square for categorical variables. We compared the admission source between white and black patients using chi-square test to examine whether inter-hospital transfer rates vary between races.
Next, admissions were stratified by race, hospital rurality, COPD hospital-volume, hospital complexity, and admission source. We compared in-hospital mortality in each stratum using the chi-square test. Subsequently, we stratified patient admissions into quartiles by travel time from patient residence to the nearest VHA primary care provider clinic and hospital. Using the Cochran-Armitage trend test, we examined the association of travel time with in-hospital mortality.
In the univariate analysis, we also created logistic regression models with patient and hospital characteristics as the independent variables accounting for repeated admissions and in-hospital (Supplementary Table 1) and 30-day mortality (Supplementary Table 2) as the dependent variables. Variables with a P-value≤0.1 in the univariate analysis were considered for the multivariate analysis. To examine which factors can explain the increased mortality in rural patients relative to urban patients, we created several multivariable logistic regression models by adding and removing relevant variables accounting for repeated admissions (Supplementary Table 3). We also created a logistic regression model with in-hospital mortality as the dependent variable and a logistic regression model with 30-day mortality as the dependent variable adjusted for all the variables that had a P-value≤0.1 in the univariate analysis. Multicollinearity was assessed using pair-wise correlation and weighted regression to assess the information matrix. All statistical analysis were conducted using SAS Enterprise Guide, 2014 SAS Institute Inc.
Results
Of 64,914 total admissions for COPD to 124 VHA hospitals over the study period included in the analysis, 43,549 were from urban (67.1%), 18,673 (28.8%) from rural, and 2,692 (4.1%) from isolated rural areas. Table 1 shows the characteristics of the study cohort, stratified by residence location. In-hospital mortality was 4.9% in urban, 5.5% in rural, and 5.2% in isolated rural veterans admitted with COPD (P=0.008). Thirty-day mortality was 8.3% in urban, 9.9% in rural, and 9.2% in isolated rural veterans (P<0.001).
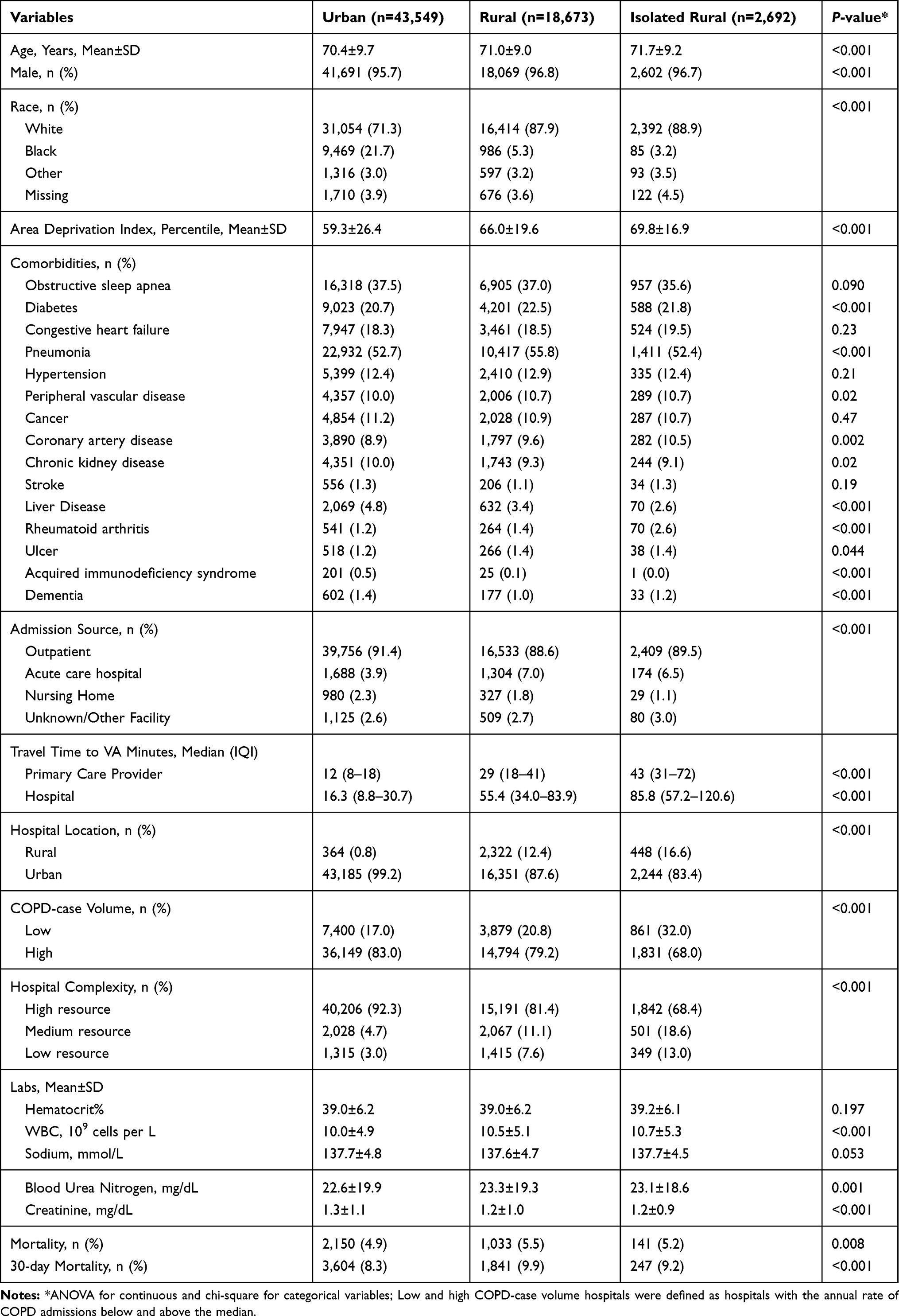 |
Table 1 Characteristics of Patients Admitted with a COPD Hospitalization by Residence Location |
Table 2 shows unadjusted in-hospital mortality in urban, rural, and isolated rural veterans stratified by race, hospital location, COPD-case volume, facility complexity, and admission source. White veterans were more likely to be admitted from an acute care hospital (inter-hospital transfer) (n=2,636; 5.3%) than black individuals (n=296; 2.8%) (Supplementary Table 4). In unadjusted analyses, travel time (Q1 represents the shortest and Q4 the longest travel time) to the nearest VHA primary care provider and hospital was not associated with in-hospital mortality for isolated rural and rural veterans (Figure 1 and Supplementary Table 5). However, travel time to the VHA hospital was associated with increased in-hospital mortality for urban patients in Q1 (<0.001).
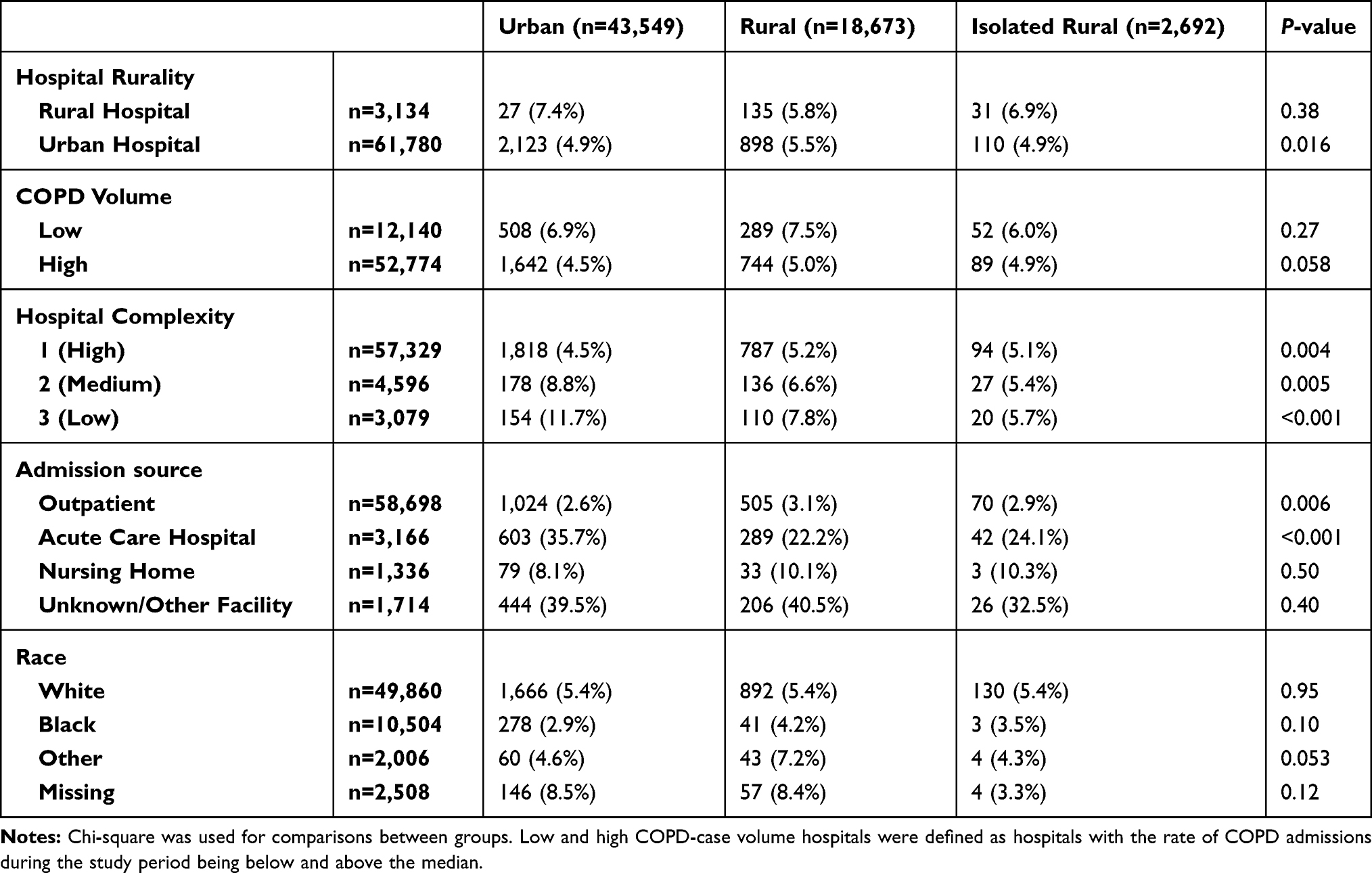 |
Table 2 Unadjusted in-Hospital Mortality for Rural and Urban Residing Veterans Stratified by Hospital Rurality, Volume, Complexity, and Admission Source |
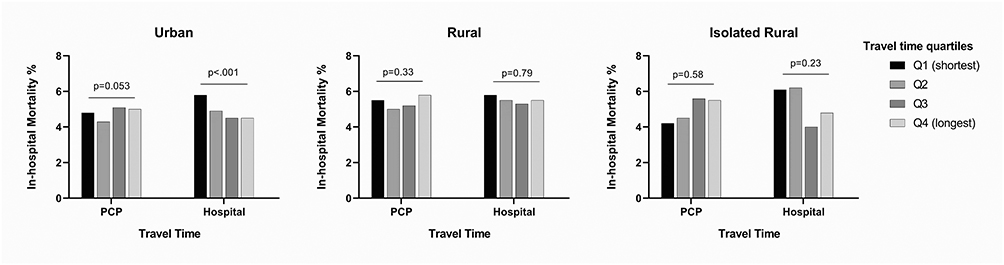 |
Figure 1 Unadjusted in-hospital mortality by travel time to the nearest Veterans Health Administration primary care provider and hospital. In-hospital mortality between quartiles was compared by Cochran-Armitage Trend Test. Abbreviations: PCP, primary care physician; Q1, first (shortest travel time) quartile; Q2, second quartile; Q3, third quartile; Q4, fourth (longest travel time) quartile. |
In unadjusted analysis, rural residents (but not isolated rural residents) had significantly increased in-hospital mortality relative to the mortality in urban Veterans with an odds ratio (OR) of 1.13 (95% CI=1.04–1.22; P=0.002) (Supplementary Table 1). The association of rural residence and in-hospital mortality remained after adjusting for hospital rurality (OR=1.005; 95% CI=1.001–1.01; P=0.015) or for hospital COPD-volume (OR=1.005; 95% CI=1.001–1.01, P=0.010) (Supplementary Table 3). However, when demographics, ADI, or admission source (inter-hospital transfers) were included in the models, the association of rural residence with in-hospital mortality was no longer present. In the final multivariable logistic regression model that included demographics, ADI, comorbidities, admission source, and hospital characteristics (Figure 2 and Supplementary Table 6), rural residence (OR=0.87; 95% CI=0.67–1.12, P=0.28) was not associated with in-hospital mortality. With outpatient admission source as the reference, transfer from another acute care hospital (OR=12.97; 95% CI=9.80–17.16, P<0.001) or unknown/other facility (OR=33.05; 95% CI=22.66–48.21, P<0.001) were the strongest predictors of increased in-hospital mortality, whereas obstructive sleep apnea (OR=0.51; 95% CI=0.39–0.67, P<0.001) was inversely associated with in-hospital mortality.
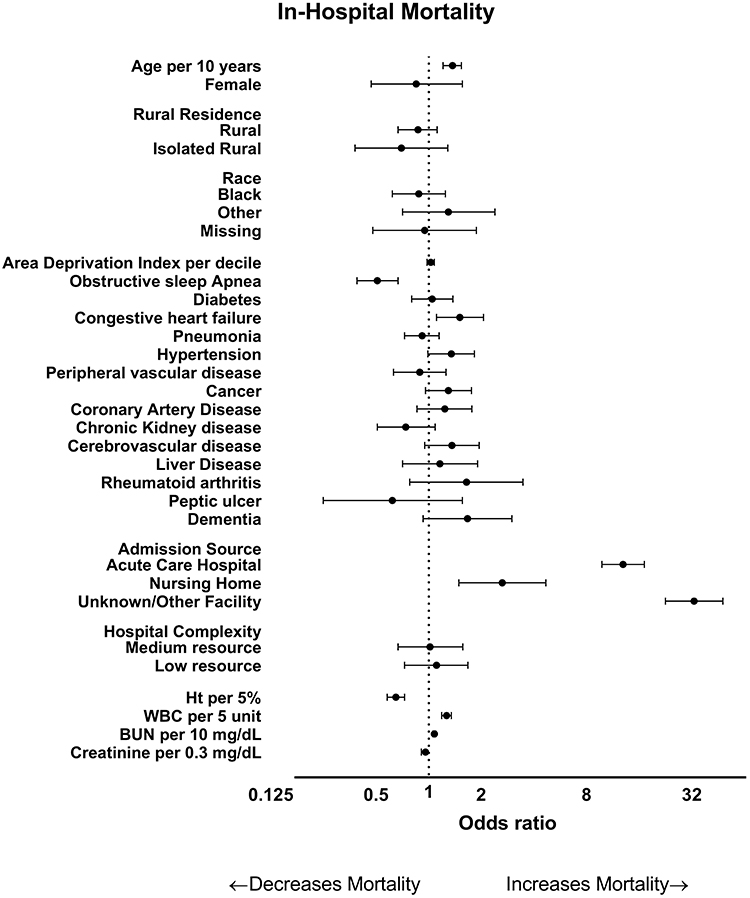 |
Figure 2 Multivariable logistic regression model for in-hospital mortality. Odds ratio with 95% confidence intervals are shown (x-axis) on log scale with base of 2. Low COPD-case volume hospitals were defined as hospitals with the annual rate of COPD admissions below the median. |
In adjusted 30-day mortality analysis (Figure 3 and Supplementary Table 7), rural residence is an independent risk factor for mortality (OR=1.13; 95% CI=1.04–1.22, P<0.001). Transfer from another acute care hospital was the stronger predictor of increased 30-day mortality (OR=3.02; 95% CI=2.69–3.39, P<0.001), whereas black race (OR=0.73;95% CI=0.65–0.81, P<0.001) and obstructive sleep apnea (OR=0.66;95% CI=0.61–0.71, P<0.001) were inversely associated with 30-day mortality.
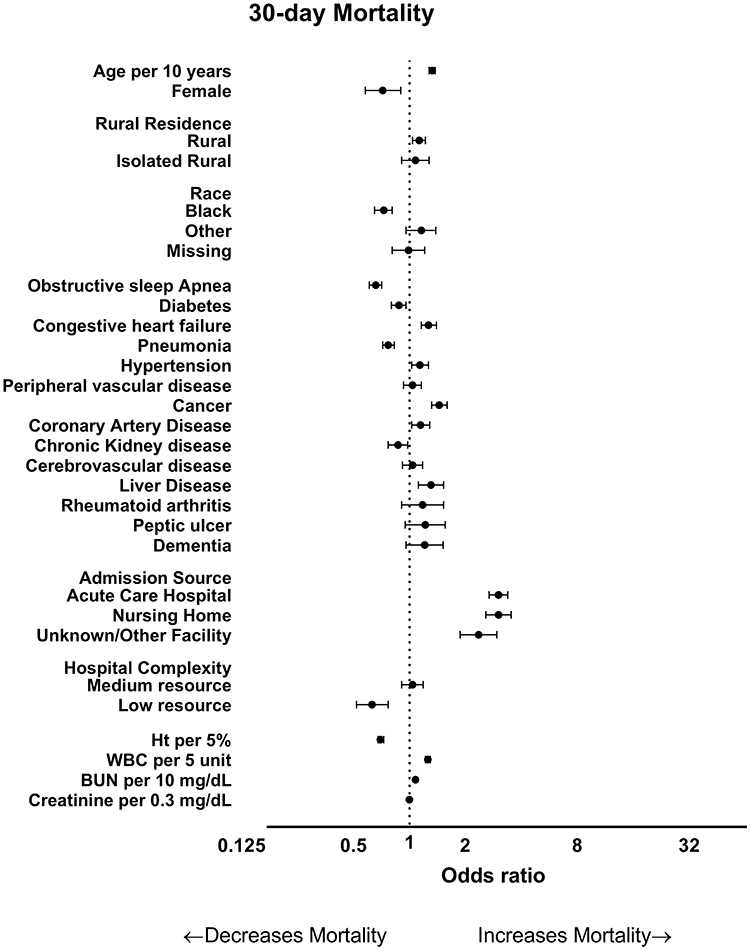 |
Figure 3 Multivariable logistic regression model for 30-day mortality. Odds ratio with 95% confidence intervals are shown (x-axis) on log scale with base of 2. Low COPD-case volume hospitals were defined as hospitals with the annual rate of COPD admissions below the median. |
Discussion
In a retrospective cohort study of veterans hospitalized with a COPD exacerbation at a VHA hospital, rural veterans but not isolated rural veterans have significantly increased unadjusted in-hospital mortality compared to urban veterans. Rural veterans have higher in-hospital mortality after adjusting for hospital location or hospital volume, but this association with increased mortality goes away after adjusting for demographics, socio-economic level of the residential location, hospital resources, or admission source (where the patient came from). Thus, rural residence does not appear to be an independent risk factor for in-hospital mortality. However, rural residence is an independent risk factor for 30-day mortality, suggesting potential gaps in post-discharge care of rural veterans may contribute to previously reported higher risk of death for rural patients with COPD. Travel time to the nearest VHA primary care provider and hospital among rural veterans was not associated with in-hospital mortality, indicating that the increased mortality is not associated with a potential disparity in access to healthcare. Transfer from another acute-care hospital is strongly associated with increased mortality, while black race is associated with reduced 30-day mortality.
Approximately 19.3% of all Americans reside in rural areas according to the US Census Bureau.28 The age-adjusted death rate for COPD is higher among rural residents than those living in urban areas.29 Among the most common diseases (heart disease, cancer, stroke), COPD is the only one where the mortality gap between rural and urban is increasing. The burden on COPD is even larger in VHA as more than a quarter of Veterans reside in rural areas30 and the prevalence of smoking31,32 and COPD is higher among them.33–35
Environmental factors have been implicated as potential causes of observed rural–urban disparities, with agriculture-related exposure being associated with COPD exacerbations.12,36 However, European studies suggest that agriculture exposure may be protective.37,38 Higher prevalence of comorbidities in rural patients may also be responsible for rural–urban disparities in COPD.29 Our findings confirm that after adjusting for demographics and comorbidities, patient residence was not associated with in-hospital mortality.
The association of obstructive sleep apnea with lower mortality in our cohort seems counter-intuitive with a first glance because obstructive sleep apnea is a known risk factor for mortality.39 Nevertheless, obstructive sleep apnea may indicate misdiagnosis of hypercapnic respiratory failure due to obesity hypoventilation syndrome which is associated with relatively low short-term mortality40–42 and lower than that in COPD-related respiratory failure.43 Another paradoxical finding is the association of pneumonia with reduced 30-day mortality. We have no good explanation of that but we could assume that the co-existing pneumonia may be confounded by early administration of antibiotic use which is associated with improved outcomes in COPD.44
Race is another important factor that may affect COPD outcomes. Although black race is considered a risk factor for developing COPD,45 COPD-related death rates in black patients are lower than the rates in white individuals.46 The effect of race on COPD outcomes is unclear.47–51 Prior research from our group has shown that black individuals are more likely to receive mechanical ventilation for COPD exacerbation than white veterans.52 The protective effect of black race may also be confounded by the inter-hospital transfers. We observed fewer black than white individuals transferred from another acute care facility, and inter-hospital transfer was the strongest risk factor for mortality.
A disparity in access to healthcare is a potential reason for rural–urban disparities. In a non-VA study, a pulmonologist was available within a 10-mile distance for only 35% of rural areas in the US14 with pulmonary specialist availability being associated with reduced emergency room and hospital visits.53 Early follow-up with a pulmonologist after hospital discharge has been shown to reduce COPD-related re-admissions.54 Although a primary care physician is usually available within a 10-mile distance in rural areas and almost all individuals had access to one within 50 miles,14 there are concerns that rural and remote healthcare practitioners may lack the knowledge, experience, and confidence to manage COPD patients according to a survey conducted by the Australian Lung Foundation.55 A study from the Minneapolis VHA HealthCare System though showed while fewer patients had spirometries in rural clinics, COPD-related quality metrics including immunizations and medication prescriptions were similar between rural and urban clinics.56
We extended the literature by showing a lack of association between travel time to the nearest VHA primary care provider/hospital and in-hospital mortality, suggesting that delays to access of care cannot explain the increased mortality in rural patients with COPD. On the other hand, urban veterans who reside close to a VHA hospital had increased in-hospital mortality. There are several potential reasons for this, including ambulance transfer patterns for the sickest patients, socio-economic factors, or patients with longer travel time to the nearest VHA hospital may have sought care in non-VHA facilities and we did not capture them in the analysis.57 Likely for the same reason, we observed mortality rates in isolated rural veterans were between the mortality rates in urban and rural patients, respectively.
The increased in-hospital mortality in rural veterans compared to the mortality in urban veterans is likely confounded by inter-hospital transfers. Inter-hospital transfers increase mortality because they may result in delays in receiving appropriate care, such as antibiotics and initiating non-invasive mechanical ventilation. These delays are associated with increased COPD-related hospital mortality.44,58 Moreover, patients requiring transfers are likely sicker that those not transferred.
Hospital volume may also play a role in the care of COPD patients. Earlier studies have shown that admission to a high volume hospital is associated with favorable outcomes in COPD,59 but a recent study showed no association.60 Improvement in care of COPD and widespread use of non-invasive ventilation, which is the most effective treatment for COPD respiratory failure and can be available in almost every hospital, may explain this.16 In our study, COPD-volume did not seem to affect mortality.
In addition, our findings suggest potential gaps in post-discharge care of rural veterans as rural residence is an independent risk factor for 30-day mortality but not for in-hospital mortality. Rural patients may not have access to pulmonary rehabilitation or even to their primary care physician, when patients are recovering from acute illness.
This study has limitations that should be considered. It was conducted in a single healthcare system with a predominantly male population. In addition, our study did not take into consideration Veterans who did not use the VHA for their medical care. Therefore, our findings may not be generalizable outside of the VHA. We did not have smoking exposure data. Because we did not have spirometric data, we cannot confirm the diagnosis of COPD or adjust for lung function severity. Nevertheless, we validated the diagnostic accuracy of ICD codes using spirometric and radiographic data from one site (our hospital). Comorbidities and age, which were used in our models, are also associated with spirometric COPD.19 We do not have data regarding causes of death. Moreover, we used only data for patients admitted to VHA hospitals. Rural veterans may be hospitalized at civilian hospitals more often than urban veterans due to travel distances and convenience. Conditions like pneumonia may mimic COPD exacerbation but it is unlikely that patients with pneumonia were misdiagnosed with COPD because pneumonia would be associated with increased mortality which was not observed.61 We did not consider physiological parameters like partial pressure of CO2 in the arterial blood which indicate the severity of the patients on the admission. However, we would expect that if rural patients were sicker on admission due to longer time to reach a VHA hospital, we would have seen an increased mortality in those who live in the most remote areas. We did not include laboratory variables like serum bicarbonate which may provide prognostic information as we have no reliable way to capture them in all the facilities. In addition, we did not examine adherence of interventions known to be associated with favorable outcomes (eg, antibiotic or non-invasive ventilation use).44,58
Conclusions
Rural residence is not an independent risk factor for in-hospital mortality, but it is associated with increased 30-day mortality after hospitalization due to COPD exacerbation suggesting potential gaps in post-discharge care of rural veterans. Further, travel time to the nearest primary care physician and hospital is not associated with in-hospital mortality. Inter-hospital transfer is the stronger predictor of increased in-hospital mortality. Further research should investigate the exact mechanism that inter-hospital transfers affect mortality.
Abbreviations
ADI, Area Deprivation Index; CDC, center of disease control; COPD, chronic obstructive pulmonary disease; ICD-9-CM and ICD-10-CM, International Classification of Diseases, Ninth and Tenth Revisions, Clinical Modification; OR, odds ratio; RUCA, rural urban commuting area; VHA, Veterans Health Administration.
Acknowledgments
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States Government.
Author Contributions
Concept and design: Spyridon Fortis, Amy O’Shea, Alejandro Comellas, Mary Vaughan Sarrazin, Peter Kaboli.
Acquisition, analysis, or interpretation of data: Spyridon Fortis, Amy O’Shea, Brice Beck, Alejandro Comellas, Mary Vaughan Sarrazin, Peter Kaboli.
Drafting of the manuscript: Spyridon Fortis, Amy O’Shea, Peter Kaboli.
Critical revision of the manuscript: All authors.
Statistical Analysis: Spyridon Fortis, Amy O’Shea, Brice Beck, Mary Vaughan Sarrazin.
Obtained funding: Spyridon Fortis.
Spyridon Fortis had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The work reported here was supported by the Department of Veterans Affairs, Veterans Health Administration, Office of Rural Health, Veterans Rural Health Resource Center (Award # 14380), and the Health Services Research and Development (HSR&D) Service through the Comprehensive Access and Delivery Research and Evaluation (CADRE) Center (CIN 13-412).
Disclosure
Dr Fortis reports grants from Office of Rural Health, during the conduct of the study; has received grants from American Thoracic Society and Fisher & Paykel to study the effect of heat humidified high flow air on COPD and has consulted Genentech in a study examining the effect of omalizumab on obstructive lung disease. Alejandro Comellas reports grants from NIH, personal fees from GSK Consultant, and non-financial support from VIDA, outside the submitted work. The authors report no other potential conflicts of interest for this work.
This paper was presented at the Virtual American Thoracic Society Conference name as a poster presentation/conference talk with interim findings. The poster’s abstract was published in “Poster Abstracts” in American Journal of Respiratory and Critical Care Medicine 2020;201:A4581 https://doi.org/10.1164/ajrccm-conference.2020.201.1_MeetingAbstracts.A4581.
References
1. National Center for Health Statistics. Health, United States 2015 with Special Feature on Racial and Ethnic Health Disparities. Hyattsville, MD: US Dept. Health and Human Services; 2016.
2. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
3. Wheaton AG, Ford ES, Cunningham TJ, Croft JB. Chronic obstructive pulmonary disease, hospital visits, and comorbidities: National Survey of Residential Care Facilities, 2010. J Aging Health. 2015;27(3):480–499. doi:10.1177/0898264314552419
4. Darnell K, Dwivedi AK, Weng Z, Panos RJ. Disproportionate utilization of healthcare resources among veterans with COPD: a retrospective analysis of factors associated with COPD healthcare cost. Cost Eff Resour Alloc. 2013;11:13. doi:10.1186/1478-7547-11-13
5. McGhan R, Radcliff T, Fish R, Sutherland ER, Welsh C, Make B. Predictors of rehospitalization and death after a severe exacerbation of COPD. Chest. 2007;132(6):1748–1755. doi:10.1378/chest.06-3018
6. Nannini LJ. Hospitalization due to COPD exacerbation. Chest. 2012;142(6):1697. doi:10.1378/chest.12-2204
7. Groenewegen KH, Schols AM, Wouters EF. Mortality and mortality-related factors after hospitalization for acute exacerbation of COPD. Chest. 2003;124(2):459–467. doi:10.1378/chest.124.2.459
8. Ai-Ping C, Lee KH, Lim TK. In-hospital and 5-year mortality of patients treated in the ICU for acute exacerbation of COPD: a retrospective study. Chest. 2005;128(2):518–524. doi:10.1378/chest.128.2.518
9. Seneff MG, Wagner DP, Wagner RP, Zimmerman JE, Knaus WA. Hospital and 1-year survival of patients admitted to intensive care units with acute exacerbation of chronic obstructive pulmonary disease. JAMA. 1995;274(23):1852–1857. doi:10.1001/jama.1995.03530230038027
10. Sullivan SD, Ramsey SD, Lee TA. The economic burden of COPD. Chest. 2000;117(2 Suppl):5S–9S. doi:10.1378/chest.117.2_suppl.5S
11. Croft JB, Liu Y, Xu F. Urban-rural county and state differences in chronic obstructive pulmonary disease — United States, 2015. MMWR Morb Mortal Wkly Rep. 2018. doi:10.15585/mmwr.mm6707a1
12. Burkes RM, Gassett AJ, Ceppe AS, et al. Rural residence and COPD exacerbations: analysis of the SPIROMICS Cohort. Ann Am Thorac Soc. 2018;15(7):808–816. doi:10.1513/AnnalsATS.201710-837OC
13. Abrams TE, Vaughan-Sarrazin M, Fan VS, Kaboli PJ. Geographic isolation and the risk for chronic obstructive pulmonary disease-related mortality: a cohort study. Ann Intern Med. 2011;155(2):80–86. doi:10.7326/0003-4819-155-2-201107190-00003
14. Croft JB, Lu H, Zhang X, Holt JB. Geographic accessibility of pulmonologists for adults with COPD: United States, 2013. Chest. 2016;150(3):544–553. doi:10.1016/j.chest.2016.05.014
15. Affairs UDoV. Veterans health administration; 2020. Available from: https://www.va.gov/health/.
16. Lindenauer PK, Stefan MS, Shieh MS, Pekow PS, Rothberg MB, Hill NS. Hospital patterns of mechanical ventilation for patients with exacerbations of COPD. Ann Am Thorac Soc. 2015;12(3):402–409. doi:10.1513/AnnalsATS.201407-293OC
17. Macaulay D, Sun SX, Sorg RA, et al. Development and validation of a claims-based prediction model for COPD severity. Respir Med. 2013;107(10):1568–1577. doi:10.1016/j.rmed.2013.05.012
18. Cooke CR, Joo MJ, Anderson SM, et al. The validity of using ICD-9 codes and pharmacy records to identify patients with chronic obstructive pulmonary disease. BMC Health Serv Res. 2011;11:37. doi:10.1186/1472-6963-11-37
19. Ho TW, Ruan SY, Huang CT, Tsai YJ, Lai F, Yu CJ. Validity of ICD9-CM codes to diagnose chronic obstructive pulmonary disease from National Health Insurance claim data in Taiwan. Int J Chron Obstruct Pulmon Dis. 2018;13:3055–3063. doi:10.2147/COPD.S174265
20. O’Shea AMJ, Fortis S, Vaughan Sarrazin M, Moeckli J, Yarbrough WC, Schacht Reisinger H. Outcomes comparison in patients admitted to low complexity rural and urban intensive care units in the veterans health administration. J Crit Care. 2019;49:64–69. doi:10.1016/j.jcrc.2018.10.013
21. Ohl M, Tate J, Duggal M, et al. Rural residence is associated with delayed care entry and increased mortality among veterans with human immunodeficiency virus infection. Med Care. 2010;48(12):1064–1070. doi:10.1097/MLR.0b013e3181ef60c2
22. Ohl ME, Perencevich E, McInnes DK, et al. Antiretroviral adherence among rural compared to urban veterans with HIV infection in the United States. AIDS Behav. 2013;17(1):174–180. doi:10.1007/s10461-012-0325-8
23. Service USDoAER. Rural-urban commuting area codes; 2010. Available from: https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes.aspx.
24. VHA office of rural health; 2015. Available from: https://www.ruralhealth.va.gov/aboutus/ruralvets.asp#atlas.
25. Kind AJ, Jencks S, Brock J, et al. Neighborhood socioeconomic disadvantage and 30-day rehospitalization: a retrospective cohort study. Ann Intern Med. 2014;161(11):765–774. doi:10.7326/M13-2946
26. Kind AJH, Buckingham WR. Making neighborhood-disadvantage metrics accessible - the neighborhood atlas. N Engl J Med. 2018;378(26):2456–2458. doi:10.1056/NEJMp1802313
27. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–1139. doi:10.1097/01.mlr.0000182534.19832.83
28. Michael Ratcliffe CB, Holder K, Fields A. Defining rural at the U.S. Census Bureau.American Community Survey and Geography Brief; 2016. Available from: https://www.census.gov/content/dam/Census/newsroom/press-kits/2016/brief_defining_rural.pdf.
29. Moy E, Garcia MC, Bastian B, et al. Leading causes of death in Nonmetropolitan and Metropolitan Areas- United States, 1999–2014. MMWR Surveill Summ. 2017;66(1):1–8. doi:10.15585/mmwr.ss6601a1
30. Affairs UDoV. Office of Rural Health; 2019. Available from: https://www.ruralhealth.va.gov/aboutus/ruralvets.asp#def.
31. Brown DW. Smoking prevalence among US veterans. J Gen Intern Med. 2010;25(2):147–149. doi:10.1007/s11606-009-1160-0
32. Klevens RM, Giovino GA, Peddicord JP, Nelson DE, Mowery P, Grummer-Strawn L. The association between veteran status and cigarette-smoking behaviors. Am J Prev Med. 1995;11(4):245–250. doi:10.1016/S0749-3797(18)30453-7
33. Murphy DE, Chaudhry Z, Almoosa KF, Panos RJ. High prevalence of chronic obstructive pulmonary disease among veterans in the urban midwest. Mil Med. 2011;176(5):552–560. doi:10.7205/MILMED-D-10-00377
34. Thompson WH, St-Hilaire S. Prevalence of chronic obstructive pulmonary disease and tobacco use in veterans at Boise Veterans Affairs Medical Center. Respir Care. 2010;55(5):555–560.
35. Sharafkhaneh A, Petersen NJ, Yu HJ, Dalal AA, Johnson ML, Hanania NA. Burden of COPD in a government health care system: a retrospective observational study using data from the US Veterans Affairs population. International journal of chronic obstructive pulmonary disease. 2010;5:125–132.
36. Terry DR, Nguyen H, Kim JA, Islam MR. Factors contributing to COPD hospitalisations from 2010 to 2015: variation among rural and metropolitan Australians. Clin Respir J. 2019;13(5):306–313. doi:10.1111/crj.13012
37. Borlee F, Yzermans CJ, van Dijk CE, Heederik D, Smit LA. Increased respiratory symptoms in COPD patients living in the vicinity of livestock farms. Eur Respir J. 2015;46(6):1605–1614. doi:10.1183/13993003.00265-2015
38. Iversen L, Hannaford PC, Price DB, Godden DJ. Is living in a rural area good for your respiratory health? Results from a cross-sectional study in Scotland. Chest. 2005;128(4):2059–2067. doi:10.1378/chest.128.4.2059
39. He J, Kryger MH, Zorick FJ, Conway W, Roth T. Mortality and apnea index in obstructive sleep apnea. Experience in 385 male patients. Chest. 1988;94(1):9–14. doi:10.1378/chest.94.1.9
40. Nowbar S, Burkart KM, Gonzales R, et al. Obesity-associated hypoventilation in hospitalized patients: prevalence, effects, and outcome. Am J Med. 2004;116(1):1–7. doi:10.1016/j.amjmed.2003.08.022
41. Castro-Anon O, Perez de Llano LA, De la Fuente Sanchez S, et al. Obesity-hypoventilation syndrome: increased risk of death over sleep apnea syndrome. PLoS One. 2015;10(2):e0117808. doi:10.1371/journal.pone.0117808
42. Budweiser S, Riedl SG, Jorres RA, Heinemann F, Pfeifer M. Mortality and prognostic factors in patients with obesity-hypoventilation syndrome undergoing noninvasive ventilation. J Intern Med. 2007;261(4):375–383. doi:10.1111/j.1365-2796.2007.01765.x
43. Carrillo A, Ferrer M, Gonzalez-Diaz G, et al. Noninvasive ventilation in acute hypercapnic respiratory failure caused by obesity hypoventilation syndrome and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(12):1279–1285. doi:10.1164/rccm.201206-1101OC
44. Rothberg MB, Pekow PS, Lahti M, Brody O, Skiest DJ, Lindenauer PK. Antibiotic therapy and treatment failure in patients hospitalized for acute exacerbations of chronic obstructive pulmonary disease. JAMA. 2010;303(20):2035–2042. doi:10.1001/jama.2010.672
45. Foreman MG, Zhang L, Murphy J, et al. Early-onset chronic obstructive pulmonary disease is associated with female sex, maternal factors, and African American race in the COPDGene Study. Am J Respir Crit Care Med. 2011;184(4):414–420. doi:10.1164/rccm.201011-1928OC
46. Kenneth D, Kochanek SLM, Xu J, Arias E. Deaths: Final Data for 2017. Reports NVS, ed. Vol. 68. National Center for Health Statistics; 2019
47. Mannino DM, Buist AS, Petty TL, Enright PL, Redd SC. Lung function and mortality in the United States: data from the First National Health and Nutrition Examination Survey follow up study. Thorax. 2003;58(5):388–393. doi:10.1136/thorax.58.5.388
48. Afessa B, Morales IJ, Scanlon PD, Peters SG. Prognostic factors, clinical course, and hospital outcome of patients with chronic obstructive pulmonary disease admitted to an intensive care unit for acute respiratory failure. Crit Care Med. 2002;30(7):1610–1615. doi:10.1097/00003246-200207000-00035
49. Putcha N, Han MK, Martinez CH, et al. Comorbidities of COPD have a major impact on clinical outcomes, particularly in African Americans. Chronic Obstr Pulm Dis. 2014;1(1):105–114. doi:10.15326/jcopdf.1.1.2014.0112
50. Kirkpatrick DP, Dransfield MT. Racial and sex differences in chronic obstructive pulmonary disease susceptibility, diagnosis, and treatment. Curr Opin Pulm Med. 2009;15(2):100–104. doi:10.1097/MCP.0b013e3283232825
51. Dransfield MT, Bailey WC. COPD: racial disparities in susceptibility, treatment, and outcomes. Clin Chest Med. 2006;27(3):463–471, vii. doi:10.1016/j.ccm.2006.04.005
52. Cannon KT, Sarrazin MV, Rosenthal GE, Curtis AE, Thomas KW, Kaldjian LC. Use of mechanical and noninvasive ventilation in black and white chronic obstructive pulmonary disease patients within the Veterans Administration health care system. Med Care. 2009;47(1):129–133. doi:10.1097/MLR.0b013e3181809150
53. Kim M, Ren J, Tillis W, Asche CV, Kim IK, Kirkness CS. Explaining the link between access-to-care factors and health care resource utilization among individuals with COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:357–367. doi:10.2147/COPD.S95717
54. Gavish R, Levy A, Dekel OK, Karp E, Maimon N. The association between hospital readmission and pulmonologist follow-up visits in patients with COPD. Chest. 2015;148(2):375–381. doi:10.1378/chest.14-1453
55. Johnston CL, Maxwell LJ, Maguire GP, Alison JA. How prepared are rural and remote health care practitioners to provide evidence-based management for people with chronic lung disease? Aust J Rural Health. 2012;20(4):200–207. doi:10.1111/j.1440-1584.2012.01288.x
56. Swanson EJ, Rice KL, Rector TS, Westanmo AD, Duane PG. Quality of chronic obstructive pulmonary disease-related health care in rural and urban veterans affairs clinics. Fed Pract. 2017;34(6):27–32.
57. Wong ES, Rinne ST, Hebert PL, Cook MA, Liu CF. Hospital distance and readmissions among VA-medicare dual-enrolled veterans. J Rural Health. 2016;32(4):377–386. doi:10.1111/jrh.12191
58. Roberts CM, Stone RA, Buckingham RJ, et al. Acidosis, non-invasive ventilation and mortality in hospitalised COPD exacerbations. Thorax. 2011;66(1):43–48. doi:10.1136/thx.2010.153114
59. Dres M, Tran TC, Aegerter P, et al. Influence of ICU case-volume on the management and hospital outcomes of acute exacerbations of chronic obstructive pulmonary disease*. Crit Care Med. 2013;41(8):1884–1892. doi:10.1097/CCM.0b013e31828a2bd8
60. Mehta AB, Douglas IS, Walkey AJ. Hospital noninvasive ventilation case volume and outcomes of acute exacerbations of chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2016;13(10):1752–1759. doi:10.1513/AnnalsATS.201610-777LE
61. Saleh A, Lopez-Campos JL, Hartl S, Pozo-Rodriguez F, Roberts CM; European CAt. The effect of incidental consolidation on management and outcomes in COPD exacerbations: data from the European COPD Audit. PLoS One. 2015;10(7):e0134004. doi:10.1371/journal.pone.0134004
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.