")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Association Between Perceived Stress and Prenatal Depressive Symptoms: Moderating Effect of Social Support
Authors Li P , Wang H, Feng J, Chen G, Zhou Z, Gou X, Ye S, Fan D , Liu Z , Guo X
Received 24 September 2021
Accepted for publication 4 November 2021
Published 16 November 2021 Volume 2021:14 Pages 3195—3204
DOI https://doi.org/10.2147/JMDH.S341090
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Pengsheng Li,1,2,* Haiyan Wang,2,3,* Jinping Feng,2 Gengdong Chen,1,2 Zixing Zhou,1,2 Xiaoyan Gou,2,3 Shaoxin Ye,1,2 Dazhi Fan,1,2 Zhengping Liu,1,2 Xiaoling Guo2
1Foshan Fetal Medicine Research Institute, Affiliated Foshan Maternity & Child Healthcare Hospital, Southern Medical University, Foshan, People’s Republic of China; 2Department of Obstetrics, Affiliated Foshan Maternity & Child Healthcare Hospital, Southern Medical University, Foshan, People’s Republic of China; 3Biobank, Foshan Fetal Medicine Research Institute, Affiliated Foshan Maternity & Child Healthcare Hospital, Southern Medical University, Foshan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoling Guo
Department of Obstetrics, Affiliated Foshan Maternity & Child Healthcare Hospital, Southern Medical University Email [email protected]
Purpose: Prenatal depressive symptoms are an important mental health problem during pregnancy. We aimed to explore the moderating role of social support on the association between perceived stress and prenatal depressive symptoms.
Materials and Methods: A cross-sectional study was conducted at an obstetrics clinic. A total of 1846 women completed a self-administered questionnaire, with a response rate of 91.8%.
Results: Of the 1846 participants, 28.2% reported prenatal depressive symptoms (Edinburgh postnatal depression scale score ≥ 9). After adjusting for demographic characteristics, gestational age, exercise, and passive smoking, both perceived stress (adjusted odds ratio (AOR): 1.210, 95% confidence interval (CI): 1.178– 1.242) and social support (AOR: 0.950, 95% CI: 0.932– 0.968) were associated with prenatal depressive symptoms. Moreover, social support had a moderating effect on the association between perceived stress and prenatal depressive symptoms (p < 0.001), and pregnant women with low social support were more likely to be affected by stress and experience prenatal depressive symptoms.
Conclusion: Our study suggests that higher social support reduces the impact of stress on pregnant women, which in turn, decreases the risk of prenatal depressive symptoms. Therefore, interventions aimed at improving social support should be considered for the prevention and treatment of prenatal depressive symptoms.
Keywords: prenatal depressive symptoms, stress, social support, moderation
Introduction
Pregnancy is a major event in a woman’s life that brings feelings of happiness; however, it is also accompanied by physiological, psychological, and social challenges.1 During pregnancy, if a woman experiences a stressful event and there is a lack of resources to buffer the stress, this can lead to mental health problems, especially prenatal depressive symptoms. Previous studies have reported that the prevalence of depressive symptoms in pregnant women is ranges from 11.4% to 40.0%, which is higher than that in women in general.2–4 Prenatal depressive symptoms increase the risk of a series of serious consequences, such as adverse pregnancy outcomes, substance abuse, and even suicide.5,6 Furthermore, untreated prenatal depressive symptoms may result in a hyperactive hypothalamic–pituitary–adrenal (HPA) axis and altered glucocorticoid feedback, which increases the vulnerability of the offspring to developing brain developmental deficits and emotional, behavioral, and cognitive problems.7
Stress is a common complaint of pregnant women, which includes fear of pregnancy, pregnancy-related symptoms (eg nausea and vomiting, pain, and fatigue), and burdens on family finances.8,9 A previous study reported that 78% of pregnant women had low to moderate psychosocial stress, and 6% had high psychosocial stress.10 During pregnancy, women undergo brain structural, psychological, and behavioral changes to adapt to the new role of raising children.11,12 However, these changes make pregnant women more vulnerable to stress,13 which increases the risk of developing prenatal depressive symptoms.10,14
As physiological and social roles change during pregnancy, the need for social support increases.15 Previous studies have found that providing social support can improve an individual’s social relationships and increase coping resources, thereby reducing the risk of developing mental health problems such as depression and anxiety.16 Emotional and material support from spouses, other family members, friends, and colleagues have a protective effect on maternal mental health17 and birth outcomes.18 More specifically, during pregnancy, high social support has been found to be a protective factor for prenatal depression.19,20
The diathesis-stress model provides a theoretical framework for discussing the relationship between stress (eg stressful life events, trauma, and childhood abuse) and diathesis (eg social support, coping style, and genes) in mental health problems.21 In the diathesis-stress model for depression, there is a synergistic interaction between diathesis and stress, which together produce more than the sum of their separate effects.21,22 Previous studies conducted in non-pregnant populations reported that individuals with low social support are more likely to be affected by stressful events, and thus, are at an increased risk of developing depression.16,23 In addition, studies have reported that during the transition to parenthood, social support can reduce the impact of stress on couples, thus reducing the risk of postpartum depression.24 Therefore, social support may buffer the stressor, which reduces the risk of experiencing prenatal depressive symptoms. However, the impact of social support on the association between perceived stress and depressive symptoms during pregnancy has rarely been discussed. As mentioned above, the social support needs and stressors of pregnant women differ from those of the general population, and whether social support buffers stress during pregnancy remains unclear. Therefore, studying the moderating effect of social support on the association between perceived stress and prenatal depressive symptoms is warranted.
The present study aimed to: 1) examine the association between perceived stress, social support, and prenatal depressive symptoms; and 2) explore the moderating effect of social support on the association between perceived stress and prenatal depressive symptoms.
Materials and Methods
Participants
All participants were recruited from pregnant women who received antenatal care service in the obstetrics clinic at the Affiliated Foshan Maternal & Child Health Hospital, Southern Medical University. Pregnant women were eligible to participate if they were aged 18 years or older and were between weeks 14 and 28 of their pregnancy. After the aim and procedure of the study had been fully explained by a trained interviewer, each woman provided a written informed consent and completed a self-administered questionnaire. A total of 1846 women completed the questionnaire (response rate of 91.8%). All data were collected between May 2020 and April 2021. This study was approved by the Institutional Review Board of the Affiliated Foshan Maternal & Child Health Hospital, Southern Medical University, and was conducted in accordance with the guidelines of the 1975 Declaration of Helsinki.
Measures
Depressive Symptoms
The Edinburgh Postnatal Depression Scale (EPDS) was used to measure depressive symptoms during the previous 7 days.25 The EPDS was originally developed to measure postpartum depressive symptoms; however, recent studies have shown that the EPDS is also useful for measuring prenatal depressive symptoms.26 The Chinese translated version of the EPDS has been verified to have good reliability and validity.27 The total score of the EPDS ranges from 0 to 30 points, and a higher score indicates more severe depressive symptoms. In the Chinese adult population, the cut-off for depressive symptoms is 9 points.27
Perceived Stress
The 14-item perceived stress scale (PSS-14) was used to measure psychological stress during the previous month. The PSS-14 was developed by Cohen et al to measure participants’ perceptions of their lives being unpredictable, uncontrollable, and overloaded.28 The Chinese translated version of the PSS-14 has been shown to have good reliability and validity.29 The total score of the PSS-14 ranges from 0 to 56 points, and a higher score indicates a higher perceived level of stress.
Social Support
The Social Support Rating Scale (SSRS) was used to measure the level of social support and contains 10 items across three dimensions: subjective support, objective support, and usage of support.30 The SSRS was developed in China and has been used widely in Chinese populations. The total score of the SSRS ranges from 0 to 66 points, and a higher score indicates stronger social support.
Covariates
Gestational age, exercise, passive smoking, and demographic characteristics have previously been reported to be associated with depressive symptoms,31,32 thus, they were considered as covariates in the current study. Demographic characteristics included maternal age, education level, marital status, work status, and household income per capita and were assessed by self-reported. Education level was defined by the participants’ highest level of education obtained, and responses included “junior high school or below”, “senior high school” and “college or university”. Marital status was based on participants’ current marital status, and responses included “married” and “unmarried or divorced”. For work status, participants stated whether they were currently “working” or “not working”. Household income per capita was calculated by dividing the total household income in the previous year by the household population. Exercise was assessed according to how much time participants spent exercising daily on average during the past 30 days, and responses were divided into “less than 0.5 hours a day” and “0.5 hours or more a day”. Passive smoking was defined as exposure to secondhand smoke for at least 5 minutes per day, and responses were either “Yes” or “No”.
Statistical Analysis
Depressive symptoms, exercise, passive smoking, and demographic characteristic were assessed using frequency tables for categorical variables and compared using Pearson’s chi-squared test. Maternal age, gestational age, perceived stress, and social support were summarized using means and standard deviations (SDs), and compared using Student’s t-tests. Logistic regression analysis was used to assess the association between perceived stress, social support, and prenatal depressive symptoms, and odds ratios (ORs) were obtained with 95% confidence intervals (CIs). First, a univariate logistic regression model (Model 1) was applied without adjusting for any covariates. Next, variables that were significant at 0.10 level in the univariate analyses or those that are widely reported in the literature were entered in the multivariate logistic regression model (Model 2) to evaluate the independent associations between perceived stress/social support and prenatal depressive symptoms. Third, in model 3, to investigate whether the associations between perceived stress and prenatal depressive symptoms differed between pregnant women with high and low social support, the interaction between perceived stress and social support was tested based on Model 2. If the interaction item was significantly associated with prenatal depressive symptoms, a stratification analysis was performed to measure the association between perceived stress and prenatal depressive symptoms in pregnant women with high and low social support. The stratification of social support was based on the SSRS score. Pregnant women whose score was above or equal to the mean were considered to have a high level of social support, whereas those whose score was below the mean were considered to have a low level of social support. A two-tailed p < 0.05 was considered significant. All data were analyzed using SAS 9.2 (SAS Institute, Inc., Cary, NC).
Results
Characteristics of Participants
Participant characteristics are shown in Table 1. A total of 1846 women were included in the analysis with a mean age of 29.2 years (range 18–47, SD = 4.4) and a mean gestational age of 25.9 weeks (range 16–28, SD = 1.5). More than half the participants had graduated from college or university (58.0%). Most participants were married (98.4%) and working (81.9%), and 42.2% reported that their household income per capita was 5001–10,000 CNY/month. A total of 59.3% of participants reported that they spent less than 0.5 hours a day on exercise, and 19.9% reported passive smoking.
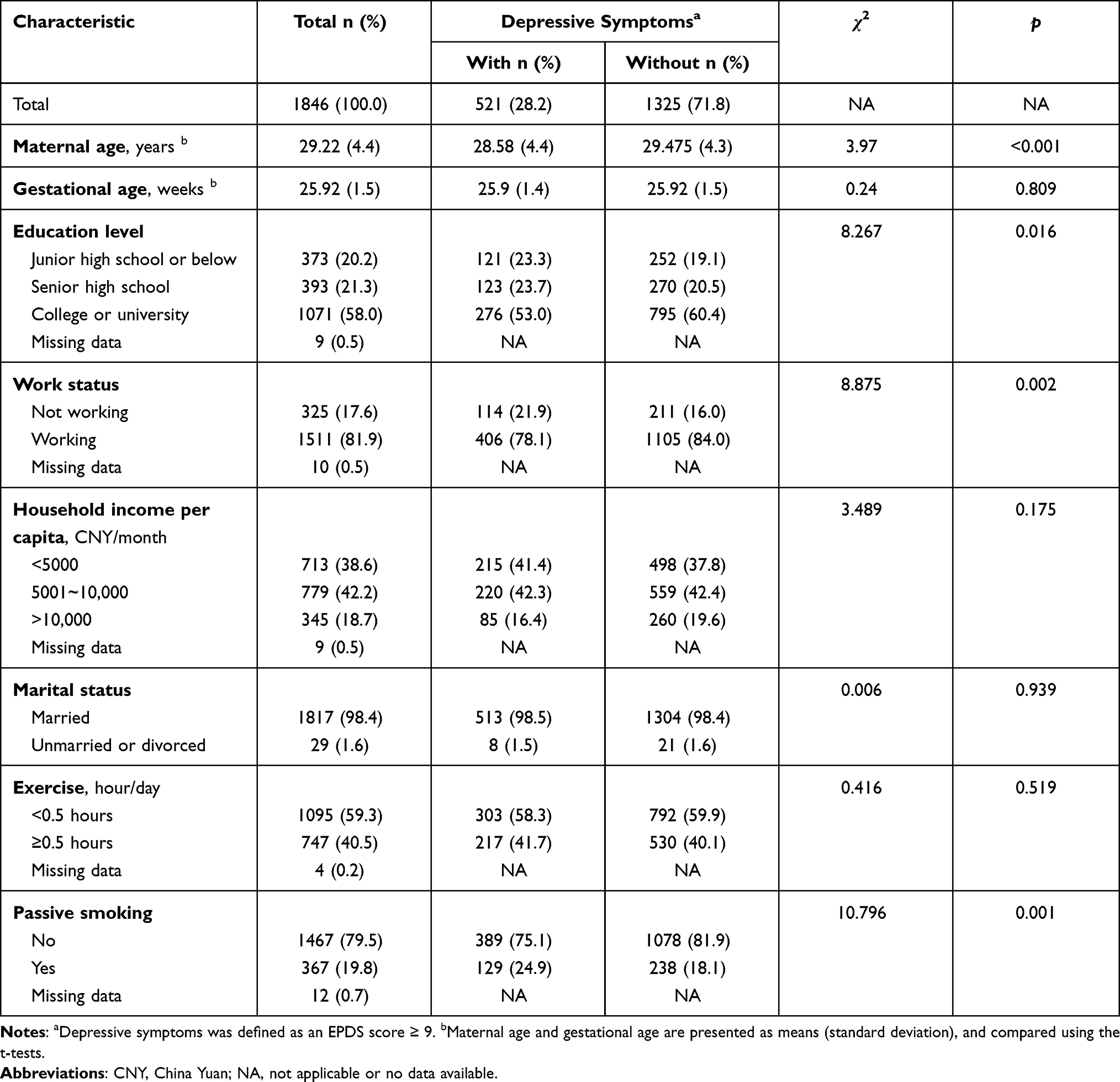 |
Table 1 Characteristic of Participants by Depression Symptoms (N = 1846) |
Depressive Symptoms in Participants
The mean EPDS score of participants was 7.13 (range 0–24, SD = 3.56). Depressive symptoms (EPDS score ≥ 9) were reported in 28.2% of participants. Maternal age, education level, work status, and passive smoking were significantly associated with depressive symptoms (p < 0.05).
Perceived Stress and Social Support
As shown in Table 2, the mean PSS score was 21.15 (range 0–44, SD = 5.90), which was higher in women with depressive symptoms (t = 19.83, p < 0.001). The mean SSRS score was 42.28 (range 19–59, SD = 6.58). Women with depressive symptoms had lower SSRS scores (mean 39.48) than those without depressive symptoms (mean 43.38, t = 11.89, p <0.001). Additionally, all three SSRS component scores (ie subjective support, objective support, and usage of support) were lower in women with depressive symptoms than those without (p < 0.001).
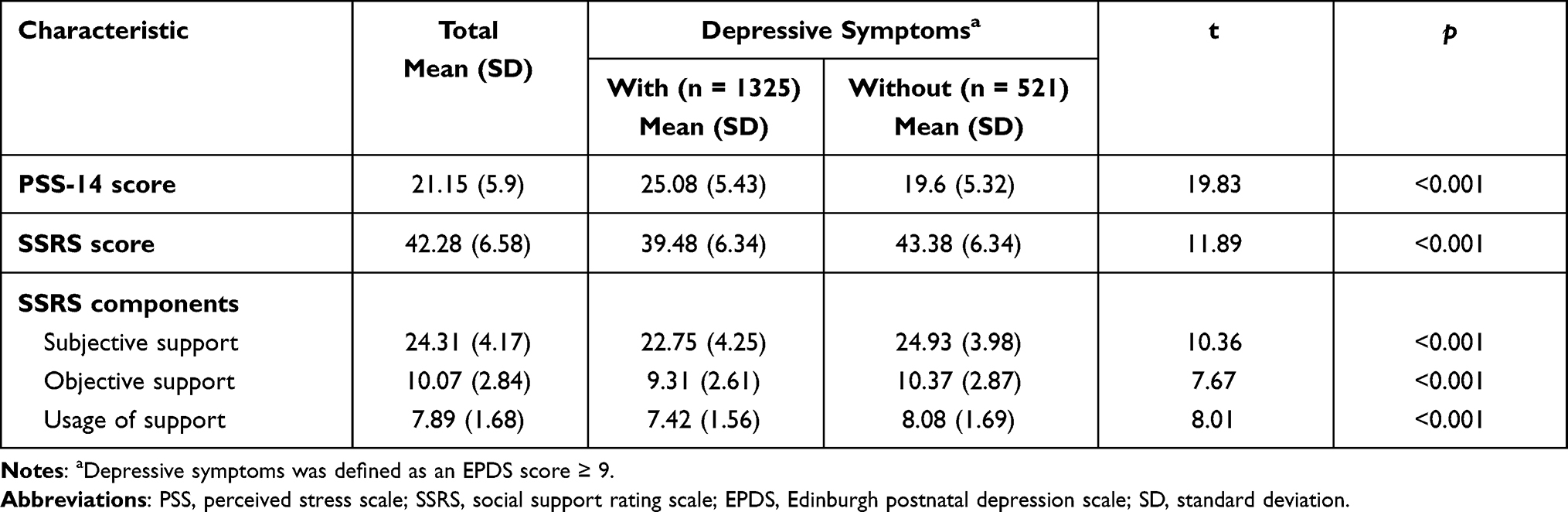 |
Table 2 Perceived Stress and Social Support in Pregnant Women (N = 1846) |
Association Between Perceived Stress, Social Support, and Depressive Symptoms
The unadjusted models showed that perceived stress and social support were significantly associated with depressive symptoms (p < 0.001; Model 1 in Table 3). Furthermore, after adjusting for maternal age, gestational age, education level, work status, household income per capita, marital status, exercise, and passive smoking, a high level of perceived stress increased the risk of developing prenatal depressive symptoms (adjust odds ratio (AOR) = 1.210, 95% CI = 1.178–1.242), whereas a high level of social support decreased the risk of developing prenatal depressive symptoms (AOR = 0.950, 95% CI = 0.932–0.968; Model 2 in Table 3).
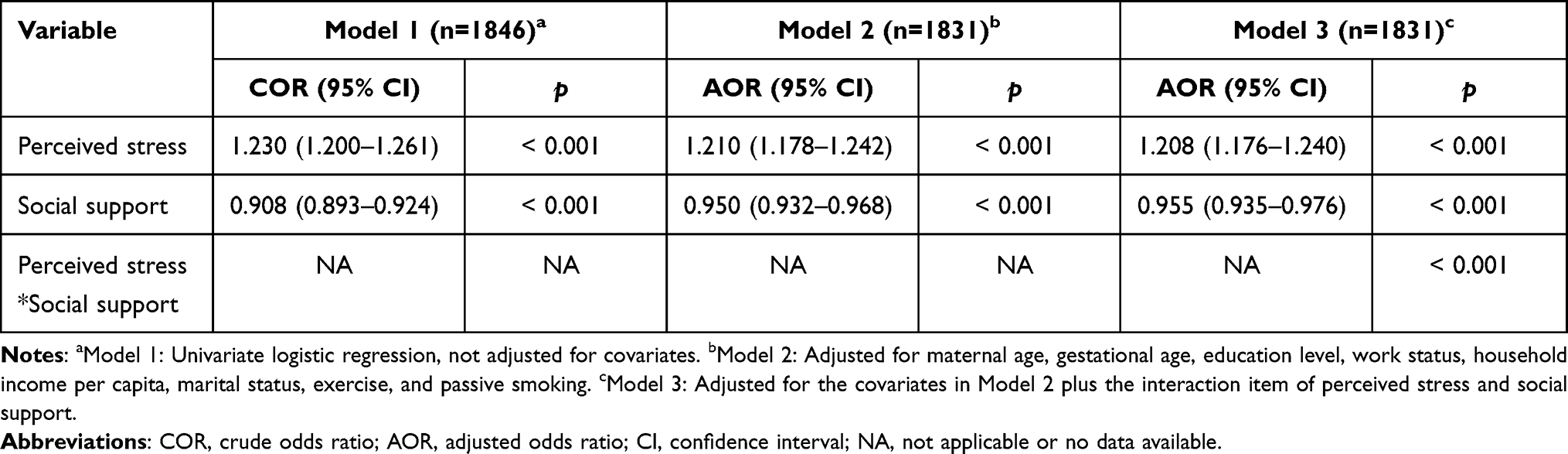 |
Table 3 Associations Between Perceived Stress, Social Support, and Depressive Symptoms |
Moderating Effect of Social Support
In model 3, the interaction item of perceived stress and social support was significant (p < 0.001). To further examine the moderating effect of social support, stratification analyses were conducted separately for women with low and high social support (Table 4). After adjusting for maternal age, gestational age, education level, work status, household income per capita, marital status, exercise, and passive smoking, we found that the strength of the association between perceived stress and depressive symptoms was higher in women with low social support (AOR = 1.236, 95% CI = 1.193–1.281) than in those with high social support (AOR = 1.198, 95% CI = 1.153–1.246).
 |
Table 4 Association Between Perceived Stress and Depressive Symptoms Stratified by Social Support |
Discussion
Depressive symptoms are one of the most common mental health problems among pregnant women. The present study found that the prevalence of depressive symptoms among Chinese pregnant women was 28.2%, which is within the range reported in previous studies on the prevalence of prenatal depressive symptoms (11.4–40.0%),2–4 and suggests that prenatal depressive symptoms remain a significant issue for pregnant women.
Stress is an important risk factor for depressive symptoms. Pregnant women may encounter various stressors before or during pregnancy, such as childhood trauma, intimate partner violence, and stressful life events. To enable the generalization of our findings across all pregnant women, we focused on the perception of stressful life events in this study. Similar to previous studies,10,14 we found that pregnant women with depressive symptoms reported significantly higher levels of perceived stress than did pregnant women without depressive symptoms (25.08 vs 19.60). Moreover, in addition to the influence of stressful life events, previous studies have reported that other stressors such as pandemics, domestic violence, and childhood trauma, increase the risk of depressive symptoms during pregnancy.33–35
The association between stress and prenatal depressive symptoms can be explained in part by the health behavior theory. During pregnancy, chronic stress increases negative health behaviors, such as smoking, drinking, and lack of exercise,36 and these factors have been found to increase vulnerability to the development of prenatal depressive symptoms.37 There was also a study found that perceived stress can lead to negative coping styles in pregnant women, which can increase the risk of mental health problems, such as low well-being.38 Furthermore, chronic stress can lead to dysregulation of the HPA axis, which is an important mechanism underlying depression. During a stressed state, the brain increases circulating cortisol levels by activating the HPA axis, which improves an individual’s ability to cope with stressful events.39 In non-depressed individuals, to reinstate homeostasis, high levels of cortisol bind to glucocorticoid receptors in the hippocampus, paraventricular nucleus, and anterior pituitary, which activates the negative feedback mechanism of the HPA axis and inhibits the further release of cortisol. However, in patients with depression, the sensitivity of the glucocorticoid receptor is impaired, which results in a disrupted negative feedback mechanism of the HPA axis and an increase in circulating cortisol.40 During a normal pregnancy, cortisol levels rise steadily with gestational age; however, in pregnant women with depressive symptoms and high perceived stress, the trajectory of cortisol is characterized by an increase in the first trimester and a sustained high level in the second and third trimesters.41 Moreover, studies have found that corticotropin-releasing hormone and cortisol levels are higher in pregnant women with depression than those without depression.42,43 In addition, DNA methylation in the promoter of the gene encoding the glucocorticoid receptor (NR3C1) and its repressor FKBP51 (FKBP5) has been shown to be higher in pregnant women following exposure to intimate partner violence.44 Thus, dysfunction of the HPA axis may also partly explain the association between stress and depressive symptoms during pregnancy.
Social support is considered a protective factor for mental health. We found that social support decreases the risk of experiencing prenatal depressive symptoms. During pregnancy, pregnant women can obtain support from partners, family, friends, and professionals, which improve their mental health, including symptoms of depression and anxiety.45 Friedman et al reported that a high level of social support reduces the risk of antepartum depression by 22%.46 Conversely, low social support increases the risk of developing depressive symptoms during pregnancy. Lundsberg et al reported that women with unplanned pregnancies had lower social support, and a low level of social support increased their risk of developing depressive symptoms.47 Previous studies have primarily focused on the separate effects of stress or social support on mental health during pregnancy, and few analyses have been based on the diathesis-stress model. One study reported a mediating effect of social support on the relationship between stress and postpartum depression.48 However, the concept of social support includes external objective support, which is not affected by stressors; thus, this form of social support is not suitable for consideration as a mediator. In this study, we found that social support plays a moderating role in the association between perceived stress and depressive symptoms, and more specifically, pregnant women with a low level of social support were more likely than those with a high level of support to suffer the effects of stress that lead to depressive symptoms. Our results suggested that social support may provide an external buffer to stress during pregnancy, thereby reducing the risk of developing prenatal depressive symptoms. This buffering effect of social support may be partly explained by its effect on the HPA axis. Previous studies have suggested that social support reduces cortisol levels. Staufenbiel et al reported a negative correlation between social support and hair cortisol concentration.49 Moreover, Iob et al found that the higher the cumulative exposure to low social support, the higher the cortisol concentration in hair.50 In addition, social support reduces adverse health behaviors, such as cigarette smoking51 and alcohol consumption,52 which increase the vulnerability to developing prenatal depressive symptoms.37
Therefore, social support may be an external factor that plays a protective role against the development of depressive symptoms. Indeed, several researchers have explored improvement in social support as an intervention to prevent and treat depressive symptoms.53,54 Furthermore, recent research has focused on peer support, in addition to the traditional sources of social support, such as family and friends. Unlike family and friends, peers who have encountered similar experiences can more easily understand the situation and needs of pregnant women and provide more appropriate support. Carter et al reported that compared with health care providers, the support provided by peer social workers was more readily accepted by pregnant women with depressive symptoms, and thus, had a greater positive impact.55 Additionally, several studies assessed the effectiveness of the Thinking Healthy Programme for perinatal depression provided by peer volunteers and found that it was effective for women with perinatal depression symptoms to achieve remission.56,57 Thus, after proper training, peer volunteers can be a valuable resource to complement routine mental health services for the prevention and treatment of women with prenatal depressive symptoms. Socioeconomic status has been found negatively correlated with the risk of prenatal depressive symptoms.58 In the current study, most of the participants were from cities, while with a relatively high educational level and socioeconomic status. Therefore, the participants of this study have a relatively low psychosocial risk, which may weaken the association between stress and social support and prenatal depressive symptoms. Previous studies reported that pregnant women in rural areas of China have a higher risk of depression during pregnancy than those in urban areas;59 while in rural areas where there is a lack of professional psychiatric services, it is more difficult and therefore less willing for pregnant women to seek professional help.60 Thus, interventions based on social support for prenatal depressive symptoms may be more effective in rural areas. In fact, peer volunteer-based Thinking Healthy Programme in rural populations has been found cost-effective for depression remission during the six-month period after childbirth.57 In addition, there have been reports that social media can provide pregnant women with social support, such as childbirth experience, parenting knowledge, and psychological support.61 Thus, social media interventions for prenatal depressive symptoms warrant further investigation.
Our study has several strengths. First, our study used a large population-based sample, which allowed us to explore the moderating effect of social support on the association between perceived stress and prenatal depressive symptoms by dividing subjects into high and low social support groups according to their level of social support and conducting stratified analyses. Second, all scales used in this study had been evaluated for their reliability and validity in the Chinese population. However, several limitations of the study should also be considered when interpreting our results. First, because of the cross-sectional nature of the data, causal inferences cannot be made. Second, although the EPDS has been widely used and shown to be reliable for the measurement of perinatal depressive symptoms, it differs from diagnoses made by psychiatrists according to the Diagnostic Statistical Manual of Mental Disorders, Fifth Edition, which should be considered when comparing our findings with those of other studies. Third, previous studies conducted in Western countries reported that smoking and alcohol consumption were associated with the development of perinatal depressive symptoms. However, cases who reported smoking and drinking in our study were close to zero; therefore, these factors were not included in the analysis, and the potential confounding effects of cigarette smoking and alcohol consumption on the association between perceived stress and prenatal depressive symptoms could not be corrected.
Conclusion
Depressive symptoms are an important mental health problem during pregnancy. Both stress and low levels of social support are risk factors for the development of prenatal depressive symptoms. However, few studies have explored the relationship between stress, social support, and prenatal depressive symptoms, based on the diathesis-stress model. Our results suggested that social support plays a moderating role in the association between perceived stress and prenatal depressive symptoms, and pregnant women with a low level of social support are more likely to be affected by stress, which increases the risk of developing prenatal depressive symptoms. Therefore, adequate social support should be provided to pregnant women to prevent the development of prenatal depression symptoms. Furthermore, interventions related to social support, such as peer support and social media support, should be considered for the prevention and treatment of prenatal depressive symptoms.
Acknowledgments
The authors express their gratitude to all the participants in this study.
Funding
This work was supported by Medical Science and Technology Foundation of Guangdong Province (No: C2019090); and Guangdong Basic and Applied Basic Research Foundation (No: 2019A1515111011).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Blount AJ, Adams CR, Anderson-Berry AL, et al. Biopsychosocial factors during the perinatal period: risks, preventative factors, and implications for healthcare professionals. Int J Environ Res Public Health. 2021;18(15):15. doi:10.3390/ijerph18158206
2. Fellmeth G, Fazel M, Plugge E. Migration and perinatal mental health in women from low- and middle-income countries: a systematic review and meta-analysis. BJOG. 2017;124(5):742–752. doi:10.1111/1471-0528.14184
3. Nisar A, Yin J, Waqas A, et al. Prevalence of perinatal depression and its determinants in Mainland China: a systematic review and meta-analysis. J Affect Disord. 2020;277:1022–1037. doi:10.1016/j.jad.2020.07.046
4. Woody CA, Ferrari AJ, Siskind DJ, et al. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J Affect Disord. 2017;219:86–92. doi:10.1016/j.jad.2017.05.003
5. Bennett HA, Einarson A, Taddio A, et al. Depression during pregnancy: overview of clinical factors. Clin Drug Investig. 2004;24(3):157–179. doi:10.2165/00044011-200424030-00004
6. Grigoriadis S, VonderPorten EH, Mamisashvili L, et al. The impact of maternal depression during pregnancy on perinatal outcomes: a systematic review and meta-analysis. J Clin Psychiatry. 2013;74(4):e321–e341. doi:10.4088/JCP.12r07968
7. Van den Bergh B, van den Heuvel MI, Lahti M, et al. Prenatal developmental origins of behavior and mental health: the influence of maternal stress in pregnancy. Neurosci Biobehav Rev. 2020;117:26–64. doi:10.1016/j.neubiorev.2017.07.003
8. Cardwell MS. Stress: pregnancy considerations. Obstet Gynecol Surv. 2013;68(2):119–129. doi:10.1097/OGX.0b013e31827f2481
9. Kuo SH, Yang YH, Wang RH, et al. Relationships between leptin, HCG, cortisol, and psychosocial stress and nausea and vomiting throughout pregnancy. Biol Res Nurs. 2010;12(1):20–27. doi:10.1177/1099800410361534
10. Woods SM, Melville JL, Guo Y, et al. Psychosocial stress during pregnancy. Am J Obstet Gynecol. 2010;202(1):61. doi:10.1016/j.ajog.2009.07.041
11. Hoekzema E, Barba-Müller E, Pozzobon C, et al. Pregnancy leads to long-lasting changes in human brain structure. Nat Neurosci. 2017;20(2):287–296. doi:10.1038/nn.4458
12. Leifer M. Psychological changes accompanying pregnancy and motherhood. Genet Psychol Monogr. 1977;95(1):55–96.
13. Kim P. How stress can influence brain adaptations to motherhood. Front Neuroendocrinol. 2021;60:100875. doi:10.1016/j.yfrne.2020.100875
14. Shakeel N, Eberhard-Gran M, Sletner L, et al. A prospective cohort study of depression in pregnancy, prevalence and risk factors in a multi-ethnic population. BMC Pregnancy Childbirth. 2015;15(1):5. doi:10.1186/s12884-014-0420-0
15. Rini C, Schetter CD, Hobel CJ, et al. Effective social support: antecedents and consequences of partner support during pregnancy. Pers Relatsh. 2006;13(2):207–229. doi:10.1111/j.1475-6811.2006.00114.x
16. Gariépy G, Honkaniemi H, Quesnel-Vallée A. Social support and protection from depression: systematic review of current findings in Western countries. Br J Psychiatry. 2016;209(4):284–293. doi:10.1192/bjp.bp.115.169094
17. Bedaso A, Adams J, Peng W, et al. The relationship between social support and mental health problems during pregnancy: a systematic review and meta-analysis. Reprod Health. 2021;18(1):162. doi:10.1186/s12978-021-01209-5
18. Hetherington E, Doktorchik C, Premji SS, et al. Preterm birth and social support during pregnancy: a systematic review and meta-analysis. Paediatr Perinat Epidemiol. 2015;29(6):523–535. doi:10.1111/ppe.12225
19. Li T, Guo N, Jiang H, et al. Social support and second trimester depression. Midwifery. 2019;69:158–162. doi:10.1016/j.midw.2018.11.012
20. Westdahl C, Milan S, Magriples U, et al. Social support and social conflict as predictors of prenatal depression. Obstet Gynecol. 2007;110(1):134–140. doi:10.1097/01.AOG.0000265352.61822.1b
21. Monroe SM, Simons AD. Diathesis-stress theories in the context of life stress research: implications for the depressive disorders. Psychol Bull. 1991;110(3):406–425. doi:10.1037/0033-2909.110.3.406
22. Colodro-Conde L, Couvy-Duchesne B, Zhu G, et al. A direct test of the diathesis-stress model for depression. Mol Psychiatry. 2018;23(7):1590–1596. doi:10.1038/mp.2017.130
23. Kilpatrick DG, Koenen KC, Ruggiero KJ, et al. The serotonin transporter genotype and social support and moderation of posttraumatic stress disorder and depression in hurricane-exposed adults. Am J Psychiatry. 2007;164(11):1693–1699. doi:10.1176/appi.ajp.2007.06122007
24. Hughes C, Devine RT, Foley S, et al. Couples becoming parents: trajectories for psychological distress and buffering effects of social support. J Affect Disord. 2020;265:372–380. doi:10.1016/j.jad.2020.01.133
25. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry. 1987;150(6):782–786. doi:10.1192/bjp.150.6.782
26. Howard LM, Ryan EG, Trevillion K, et al. Accuracy of the whooley questions and the Edinburgh postnatal depression scale in identifying depression and other mental disorders in early pregnancy. Br J Psychiatry. 2018;212(1):50–56. doi:10.1192/bjp.2017.9
27. Zhao Y, Kane I, Wang J, et al. Combined use of the postpartum depression screening scale (PDSS) and Edinburgh postnatal depression scale (EPDS) to identify antenatal depression among Chinese pregnant women with obstetric complications. Psychiatry Res. 2015;226(1):113–119. doi:10.1016/j.psychres.2014.12.016
28. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396. doi:10.2307/2136404
29. Huang F, Wang H, Wang Z, et al. Psychometric properties of the perceived stress scale in a community sample of Chinese. Bmc Psychiatry. 2020;20(1):130. doi:10.1186/s12888-020-02520-4
30. Shuiyuan X, Desen Y. The effect of social support on physical and psychological health. J Chin Psychiatry. 1987;04:183–187.
31. Gelaye B, Rondon MB, Araya R, et al. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. Lancet Psychiatry. 2016;3(10):973–982. doi:10.1016/S2215-0366(16)30284-X
32. Míguez MC, Vázquez MB. Risk factors for antenatal depression: a review. World J Psychiatry. 2021;11(7):325–336. doi:10.5498/wjp.v11.i7.325
33. Alhusen JL, Ray E, Sharps P, et al. Intimate partner violence during pregnancy: maternal and neonatal outcomes. J Womens Health. 2015;24(1):100–106. doi:10.1089/jwh.2014.4872
34. Lebel C, MacKinnon A, Bagshawe M, et al. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J Affect Disord. 2020;277:5–13. doi:10.1016/j.jad.2020.07.126
35. Wosu AC, Gelaye B, Williams MA. History of childhood sexual abuse and risk of prenatal and postpartum depression or depressive symptoms: an epidemiologic review. Arch Womens Ment Health. 2015;18(5):659–671. doi:10.1007/s00737-015-0533-0
36. Smith T, Johns‐Wolfe E, Shields GS, et al. Associations between lifetime stress exposure and prenatal health behaviors. Stress Health. 2020;36(3):384–395. doi:10.1002/smi.2933
37. Smedberg J, Lupattelli A, Mårdby A-C, et al. The relationship between maternal depression and smoking cessation during pregnancy—a cross-sectional study of pregnant women from 15 European countries. Arch Womens Ment Health. 2015;18(1):73–84. doi:10.1007/s00737-014-0470-3
38. Lau Y, Tha PH, Wong DFK, et al. Different perceptions of stress, coping styles, and general well-being among pregnant Chinese women: a structural equation modeling approach. Arch Womens Ment Health. 2016;19(1):71–78. doi:10.1007/s00737-015-0523-2
39. Menke A. Is the HPA axis as target for depression outdated, or is there a new hope? Front Psychiatry. 2019;10. doi:10.3389/fpsyt.2019.00101
40. Pariante CM, Lightman SL. The HPA axis in major depression: classical theories and new developments. Trends Neurosci. 2008;31(9):464–468. doi:10.1016/j.tins.2008.06.006
41. Peterson GF, Espel EV, Davis EP, et al. Characterizing prenatal maternal distress with unique prenatal cortisol trajectories. Health Psychol. 2020;39(11):1013–1019. doi:10.1037/hea0001018
42. O’Keane V, Lightman S, Marsh M, et al. Increased pituitary–adrenal activation and shortened gestation in a sample of depressed pregnant women: a pilot study. J Affect Disord. 2010;130(1):300–305. doi:10.1016/j.jad.2010.10.004
43. Rich-Edwards JW, Mohllajee AP, Kleinman K, et al. Elevated midpregnancy corticotropin-releasing hormone is associated with prenatal, but not postpartum, maternal depression. J Clin Endocrinol Metab. 2008;93(5):1946–1951. doi:10.1210/jc.2007-2535
44. Serpeloni F, Radtke KM, Hecker T, et al. Does prenatal stress shape postnatal resilience? – an Epigenome-Wide Study on violence and mental health in humans. Front Genet. 2019:10. doi:10.3389/fgene.2019.00269
45. Razurel C, Kaiser B. The role of satisfaction with social support on the psychological health of primiparous mothers in the perinatal period. Women Health. 2015;55(2):167–186. doi:10.1080/03630242.2014.979969
46. Friedman LE, Gelaye B, Sanchez SE, et al. Association of social support and antepartum depression among pregnant women. J Affect Disord. 2020;264:201–205. doi:10.1016/j.jad.2019.12.017
47. Lundsberg LS, Cutler AS, Stanwood NL, et al. Association of pregnancy contexts with depression and low social support in early pregnancy. Perspect Sex Reprod Health. 2020;52(3):161–170. doi:10.1363/psrh.12155
48. Razurel C, Kaiser B, Antonietti J-P, et al. Relationship between perceived perinatal stress and depressive symptoms, anxiety, and parental self-efficacy in primiparous mothers and the role of social support. Women Health. 2017;57(2):154–172. doi:10.1080/03630242.2016.1157125
49. Staufenbiel SM, Koenders MA, Giltay EJ, et al. Recent negative life events increase hair cortisol concentrations in patients with bipolar disorder. Stress. 2014;17(6):451–459. doi:10.3109/10253890.2014.968549
50. Iob E, Kirschbaum C, Steptoe A. Positive and negative social support and HPA-axis hyperactivity: evidence from glucocorticoids in human hair. Psychoneuroendocrino. 2018;96:100–108. doi:10.1016/j.psyneuen.2018.06.008
51. Yun EH, Kang YH, Lim MK, et al. The role of social support and social networks in smoking behavior among middle and older aged people in rural areas of South Korea: a cross-sectional study. Bmc Public Health. 2010;10(1):78. doi:10.1186/1471-2458-10-78
52. Boateng-Poku A, Benca-Bachman CE, Najera DD, et al. The role of social support on the effects of stress and depression on African American tobacco and alcohol use. Drug Alcohol Depend. 2020;209:107926. doi:10.1016/j.drugalcdep.2020.107926
53. Page-Reeves J, Murray-Krezan C, Regino L, et al. A randomized control trial to test a peer support group approach for reducing social isolation and depression among female Mexican immigrants. Bmc Public Health. 2021;21(1):119. doi:10.1186/s12889-020-09867-z
54. Stice E, Rohde P, Gau J, et al. Relation of depression to perceived social support: results from a randomized adolescent depression prevention trial. Behav Res Ther. 2011;49(5):361–366. doi:10.1016/j.brat.2011.02.009
55. Carter R, Cust F, Boath E. Effectiveness of a peer support intervention for antenatal depression: a feasibility study. J Reprod Infant Psychol. 2020;38(3):259–270. doi:10.1080/02646838.2019.1668547
56. Fuhr DC, Weobong B, Lazarus A, et al. Delivering the thinking healthy programme for perinatal depression through peers: an individually randomised controlled trial in India. Lancet Psychiatry. 2019;6(2):115–127. doi:10.1016/S2215-0366(18)30466-8
57. Sikander S, Ahmad I, Atif N, et al. Delivering the thinking healthy programme for perinatal depression through volunteer peers: a cluster randomised controlled trial in Pakistan. Lancet Psychiatry. 2019;6(2):128–139. doi:10.1016/S2215-0366(18)30467-X
58. Lorant V, Deliège D, Eaton W, et al. Socioeconomic inequalities in depression: a meta-analysis. Am J Epidemiol. 2003;157(2):98–112. doi:10.1093/aje/kwf182
59. Chen J, Cross WM, Plummer V, et al. The risk factors of antenatal depression: a cross-sectional survey. J Clin Nurs. 2019;28(19–20):3599–3609. doi:10.1111/jocn.14955
60. Yin J, Nisar A, Waqas A, et al. Psychosocial interventions on perinatal depression in China: a systematic review and meta-analysis. J Affect Disord. 2020;271:310–327. doi:10.1016/j.jad.2020.03.019
61. Baker B, Yang I. Social media as social support in pregnancy and the postpartum. Sex Reprod Healthc. 2018;17:31–34. doi:10.1016/j.srhc.2018.05.003
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.