")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Association Between NLR and NAFLD in Adults Exposed to Famine in Early Life
Authors Liu Y, Zhong Z, Li Z, Li X, Zhang S, Sun J, Zhai J, Liu X , Liu M
Received 1 April 2022
Accepted for publication 4 August 2022
Published 23 August 2022 Volume 2022:15 Pages 1561—1568
DOI https://doi.org/10.2147/RMHP.S368369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mecit Can Emre Simsekler
Ying Liu,1,* Zhifang Zhong,1,* Zhihong Li,1,* Xin Li,2 Shengkun Zhang,2 Jie Sun,1 Jingfang Zhai,3 Xuekui Liu,4 Min Liu1
1Department of Ultrasound, Xuzhou Central Hospital, Xuzhou, People’s Republic of China; 2Department of Obstetrical and Gynecological, Xuzhou Central hospital, Xuzhou, People’s Republic of China; 3Prenatal Diagnosis Center, Xuzhou Central Hospital, Xuzhou, People’s Republic of China; 4Department of Endocrinology, Xuzhou Central hospital, Xuzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Min Liu, Department of Ultrasound, Xuzhou Central Hospital, Jiefang Road 199#, Xuzhou, 221009, People’s Republic of China, Email [email protected] Xuekui Liu, Department of Endocrinology, Xuzhou Central Hospital, Jiefang Road 199#, Xuzhou, 221009, People’s Republic of China, Email [email protected]
Aim: Exposure to famine in early life has been shown to increase the prevalence of non-alcoholic fatty liver disease (NAFLD). Neutrophil-to-lymphocyte ratio (NLR) is a risk factor for developing NAFLD. However, it is not clear that the association between NLR and NAFLD in individuals who were exposed to famine in early life.
Methods: To match for age, we selected two group populations from Xuzhou city, China, on two different occasions, 2013 and 2017. The group recruited in 2013 included participants who were born during a period of great famine in China. Participants in the another group recruited in 2017 were born between 1965 and 1968. Clinical characteristics of individuals as well as serology indexes were examined for all participants. Ultrasonography to diagnose NAFLD was performed by trained doctors. A total of 10,574 participants were included in the final analysis.
Results: Individuals born during the famine period have a higher NAFLD prevalence than those who had not been exposed to famine and these findings were similar for both sexes (male: 57.6% vs 48.9%, female: 47.6% vs 40.3%). The prevalence of NAFLD according to NLR quartiles in those exposed to famine was 49.5%, 52.7%, 52.9% and 55.5% for Q1, Q2, Q3 and Q4 NLR, respectively, and was higher than that in non-exposed to famine group. After adjusting for age, BMI, and other metabolic variables, the association between NLR and NAFLD disappeared in the non-famine group. The non-linear relationship between NLR and NAFLD was found in those who had been exposed to famine.
Conclusion: Individuals who were exposed to famine in early life have a higher prevalence of NAFLD than those who were not exposed. Compared with lower NLR levels, elevated NLR is a risk factor for developing NAFLD. However, there is a non-linear relationship between NLR and the risk of developing NAFLD.
Keywords: non-alcoholic fatty liver disease, famine, neutrophil-to-lymphocyte ratio, non-linear relationship
Introduction
The prevalence of non-alcoholic fatty liver disease (NAFLD) has risen rapidly in the past dozen years.1 According to WHO, the global prevalence of NAFLD is 25.2%,2 and in Africa is 31.8%.3 NAFLD is defined by the presence of steatosis in more than 5% of hepatocytes in individuals who are non-drinker, or in the absence of excessive alcohol consumption or other chronic liver diseases. NAFLD ranges from simple steatosis to non-alcoholic steatohepatitis (NASH) with or without hepatic fibrosis.4 As a chronic metabolic liver disease, NAFLD has been linked with chronic inflammation activation.5 A backdrop of literature demonstrated the role of two main inflammatory pathways, JNK-AP-1 and IKK-NF-κB, in the development of NAFLD.6 The neutrophil-to-lymphocyte ratio (NLR), which is also a low-cost and accessible indicator of inflammation, has been reported to play a role in patients with inflammatory bowel disease,7 thyroiditis8 and hepatocellular carcinoma.9 However, controversies regarding the relationship between NLR and NAFLD remain. For example, Abdel-Rzaik et al found a positive correlation between NLR and NAFLD,10 but Wen11 reported there a negative correlation between elevated NLR levels and fibrosis in patients with NAFLD.
In addition to inflammation, malnutrition in early life is also a risk factor for NAFLD. Inadequate food supply is the primary cause of malnutrition, the role of nutrition in NAFLD was proved by many studies.12–14 Qi15 suggested that individuals who exposed to famine in early life, have a higher risk of developing NAFLD than those who unexposed to famine. Liu et al16 also found that adults born during a famine period had a higher prevalence of NAFLD. However, prior studies have not matched famine and control cohorts for age, which is an important factor of liver diseases and therefore an important confounder that should be accounted for.17 From 1959 to 1962, there was a great famine in mainland China, and in which approximately 30 million people have died of starvation.18 Our study includes individuals born between 1959 and 1962 in China to evaluate the harms of famine in the context of liver disease. Specifically, we recruited two groups of age-matched participants and investigated the association between NLR and NAFLD prevalence.
Subjects and Methods
Subjects
We enlisted two groups; one group included individuals born at the peak of the great Chinese famine of 1959 to 1962 [famine period group (BF)]. A total of 6318 individuals were included in the BF group and took part in the preliminary survey. Four thousand five hundred and seventeen of participants born between 1965 and 1968 were recruited to the non-famine group (BNF). Participants who meet the inclusion and exclusion criteria were included in the final analysis. The inclusion criteria were as follows: 1) the individuals who were non-drinkers or consumed less than 140g (for males) or less than 70 g (for females) of alcohol per week 2) signed an informed consent and volunteered to participate in this study. The exclusion criteria were as follows: 1) patients with hepatitis B, alcoholic fatty liver, liver cirrhosis, or liver cancer; 2) patients with mental health issues; 3) individuals who were not able to undergo Ultrasound examination; 4) participants who migrated from non-famine place after birth in 1959~1962.
A total of 10,547 participants were included in this study, 6125 participants were included in the BF group and 4422 individuals were included in the BNF group.
Data Collected
Age is a well-recognized risk factor for NAFLD.17 To minimize the influence of age in our results, and ensure patients were age-matched, we collected research data for the BF group in 2013, and collected research data for the BNF group in 2017.
All participants were examined by trained medical workers in the Xuzhou Central Hospital, Xuzhou city, China. The examination included a questionnaire, general physical testing, serological tests, and ultrasound examinations. Age, sex, drinking history and smoking, history of liver disease, hypertension and type 2 diabetes were collected in the questionnaire. Height, weight, body mass index (BMI)), systolic blood pressure (SBP), diastolic blood pressure (DBP) data were collected by trained doctors. Serological tests included total cholesterol (TC), triglycerides (TG), low-density lipoprotein (LDL), high-density lipoprotein (HDL), apolipoprotein A (APO-A), apolipoprotein B (APO-B), total protein (TB), albumin (ALB), and fasting plasma glucose (FPG). Blood routine tests included red blood cell (RBC) counts, white blood cell (WBC) counts, hemoglobin (HB), platelet counts (PLT), and neutrophil (NEUT) and lymphocyte (LYM) counts. NLR was estimated by NEUT/LYM. This study was approved by the ethics committee of Xuzhou Central hospital, China; all participants gave informed consent.
Diagnosis of NAFLD
The gold standard NAFLD diagnosis of NAFLD is fine needle aspiration biopsy. However, liver biopsy can be dangerous and is not suitable for populational screening given high costs. In this study, we screened patients using ultrasound examination. To confirm the diagnosis, individuals were screened by two trained sonographers; in the event of disagreement, the patient was examined by a senior physician. Diagnosis was performed according to NAFLD criteria using ultrasound,4,19 the abdominal ultrasonography scan was performed using a 3.5-MHz transducer (LOGIQ9E, GE, USA).
Statistical Analyses
Continuous data were tested normality as presented as means ± SD; comparison between groups was done using the Student’s t-test. Non-normal data were transformed by log and tested by Skewness-Kurtosi. Multi-factor logistic regression restricted cubic spline analysis and was used to analyze the association between NLR and the risk of NAFLD. SPSS 21.0 (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp) was used to analyze and manage the data. Calculations were based on a 2-sided t-test at the 5% level of significance.
Results
Participants Clinical Characteristics
In the present study, a total of 10,547 participants who were identified as non-drinkers or consumed less than 140g (for males) or less than 70 g (for females) of alcohol per week were included into the final analysis. In female participants, we found that weight, BMI, DBP, TG, HDL, LDL, APO-B, ALB, WBC, RBC, HB, PLT, LYC were significantly different between the two groups, with participants who were born during the famine period having higher TG, LDL, RBC, HB and PLT levels than those who were not born during the famine period. In male participants, we found that SBP, DBP, TC, HDL, LDL, APO-B, TP, ALB, WBC, RBC, HB, PLT, LYC and NEUT were significantly different between the two groups, with males born during the famine period having higher SBP, LDL, TP, HB, PLT and NEUT. Individuals who were born during the non-famine had a higher LYC. There were no significant differences in smoking, type 2 diabetes and hypertension history between the two groups (Table 1).
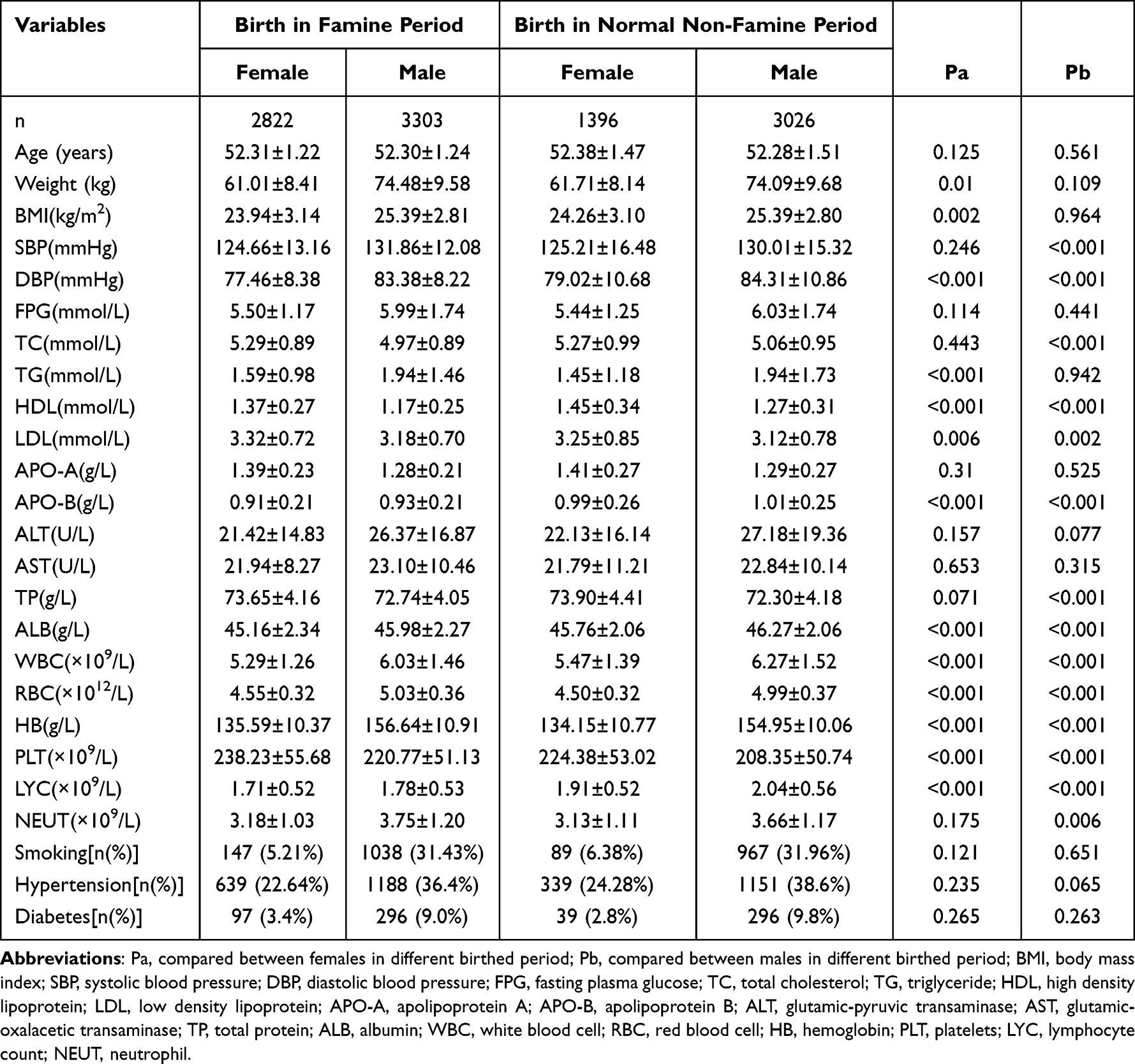 |
Table 1 The Clinical Characteristic of Participants According to Different Birth Period and Sex |
NAFLD Prevalence and Different NLR Levels
In this study, we found that NAFLD prevalence was of 52.9% (3242/6125) in the BF group, and 46.1% (2040/4422) in the NBF group, with a statistically significant difference between the two groups (P < 0.001). We split our sample into four subgroups, according NLR quartiles. NAFLD prevalence was different between the two groups and across the four subgroups. In the NLR Q1 subgroup, the prevalence of NAFLD was 49.5% in the BF group, and 44.4% in the BNF group (P = 0.008). In the NLR Q2 subgroup, the prevalence of NAFLD was 52.7% in the BF group and 47.5% in the BNF group (P = 0.007). In the NLR Q3 subgroup, the prevalence of NAFLD was 52.9% in the BF group and 46.6% in the BNF group (P = 0.002). In the NLR Q4 subgroup, the prevalence of NAFLD was 55.3% in the BF group and 46.3% in the BNF group (P < 0.001). We observed increased NAFLD prevalence with increasing NLR levels in the BF group (P = 0.016) but not in the BNF group (P = 0.438) (Figure 1).
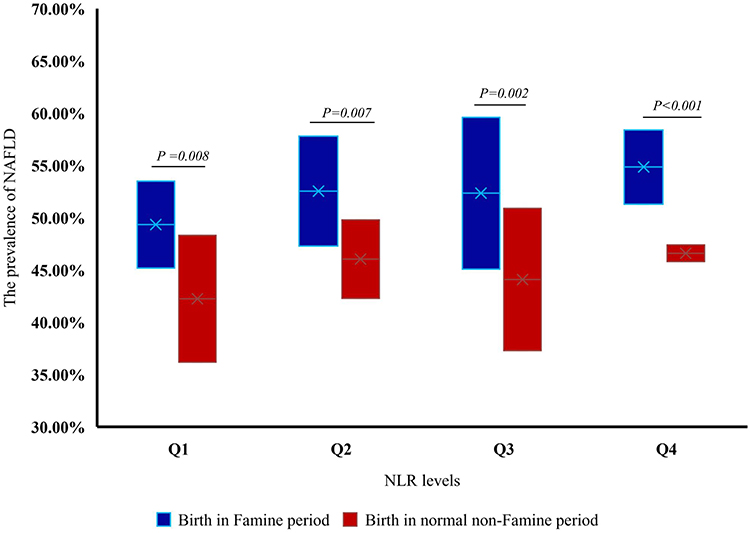 |
Figure 1 The prevalence of non-alcoholic fatty liver disease (NAFLD) of two groups in different categories of neutrophil-to-lymphocyte ratio (NLR). Q1: NLR < 1.429%; Q2: NLR≥1.429%, NLR <1.860%; Q3: NLR≥1.860%, NLR<2.389%; Q4: NLR≥2.389%. |
Sex and NLR Associated with NAFLD Prevalence
We examined NAFLD prevalence according to sex. Our results show that males in the BF group have higher NAFLD prevalence than those in the BNF group (52.5% vs 43.8%). Similar findings were observed in females (36.1% in the BF group vs 29.5% in the BNF group). Further, we analyzed the association between NLR and NAFLD prevalence in both sexes (Figure 2). Regardless of sex, NAFLD prevalence increases with NLR levels in the BF group. In the BNF group, NAFLD prevalence in females increased with NAR levels, but the trend was not found in male participants.
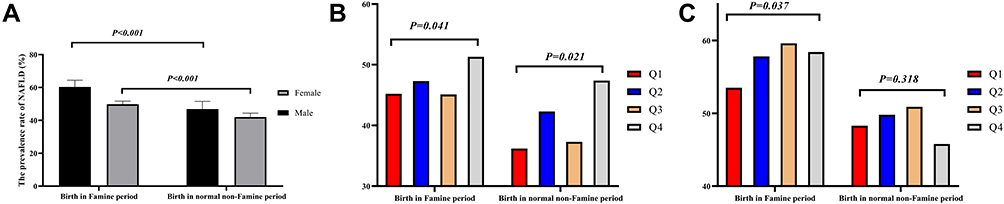 |
Figure 2 The prevalence of non-alcoholic fatty liver disease (NAFLD) in different categories of neutrophil-to-lymphocyte ratio (NLR) and different gender. (A) The prevalence of NAFLD of two groups in different gender. (B) The prevalence of NAFLD of female participants in two groups in different categories of NLR. Q1: NLR < 1.429%; Q2: NLR≥1.429%, NLR <1.860%; Q3: NLR≥1.860%, NLR<2.389%; Q4: NLR≥2.389%. (C) The prevalence of NAFLD of male participants in two groups in different categories of NLR. Q1: NLR < 1.429%; Q2: NLR≥1.429%, NLR <1.860%; Q3: NLR≥1.860%, NLR<2.389%; Q4: NLR≥2.389%. |
Association Between NLR and NAFLD in Different Groups According to Sex
We performed multi-factor logistic regression analysis to explore the relationship between NAR and NAFLD in both groups according to sex (Table 2). We found that after adjusting for age, BMI, blood lipid levels, FPG, WBC, RBC, smoking status, and diabetes and hypertension history, the participants born during the famine period with higher NLR level had a higher risk of NAFLD than those born during the non-famine period. In the BNF group, we did not observe that the risk of NAFLD was increased with NLR levels, after adjusting for metabolic factors. Females in Q4 NLR of the BF group had an increased risk of 31.8% to develop NAFLD than those in Q1 NLR level. For males, the risk of NAFLD increased by 26.3% in Q4 NLR of the BF group compared to those in Q1 level (Table 2).
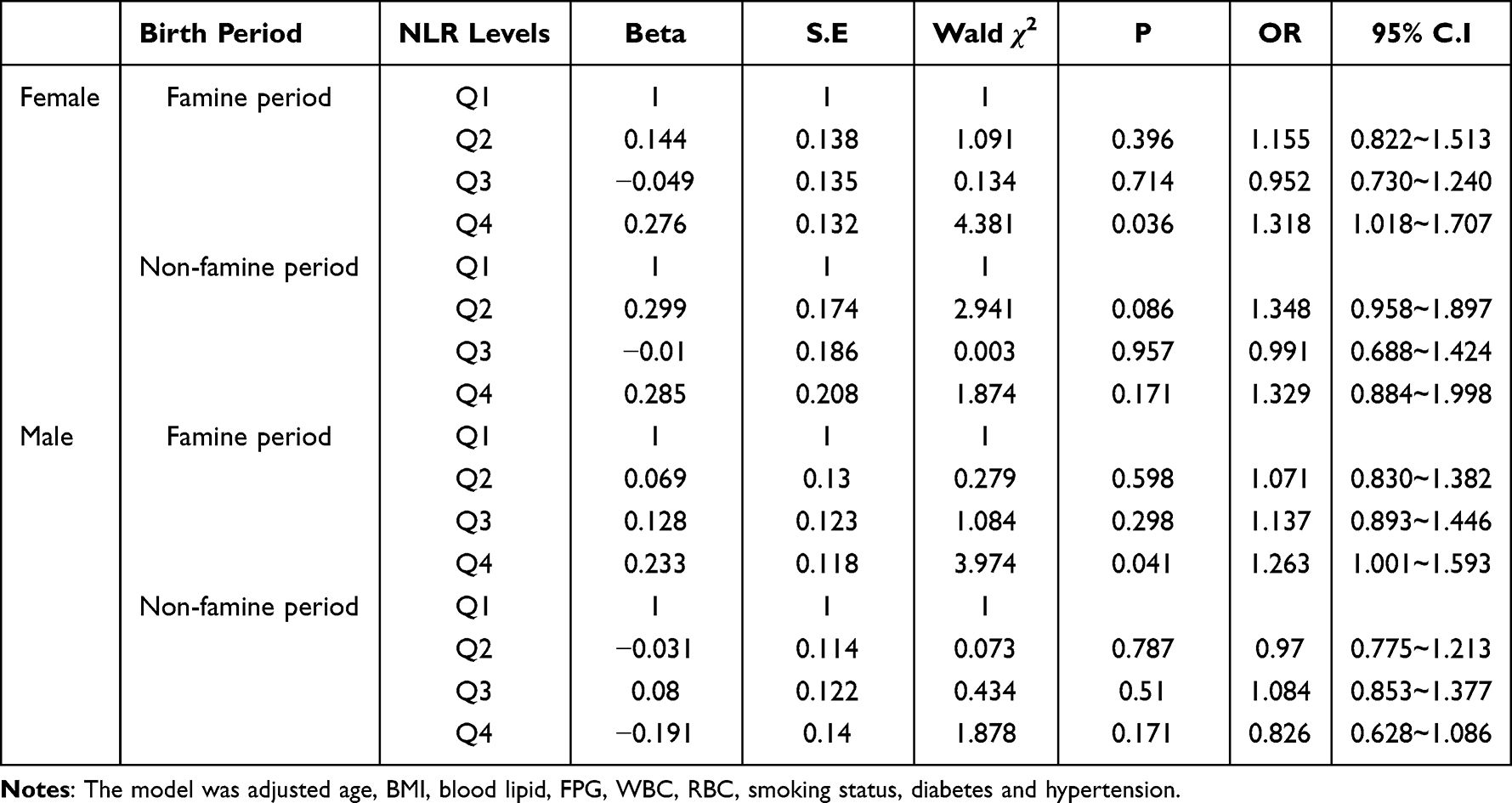 |
Table 2 The Association Between NLR and NAFLD Using the Multi-Factor Regression Analysis |
The Association Between NLR and the Risk of NAFLD in BF Group
So far, our results suggest a relationship between NLR and the risk of NAFLD. However, it remains unclear whether this is a linear association. After adjusting for age, BMI, blood lipids, FPG, WBC, RBC, smoking status, and diabetes and hypertension history, we found non-linear relationship between NLR and the risk of NAFLD in both sexes. In males, the risk of NAFLD increased with increasing NLR when NLR was below 2%, while NLR was above 2%, the association between NLR and NAFLD was non-linear (Figure 3B). In females, we found that when NLR was below 3%, the risk of NAFLD increased with NLR, but when NLR was more than 3%, the risk of NAFLD reduced with increasing NLR (Figure 3A).
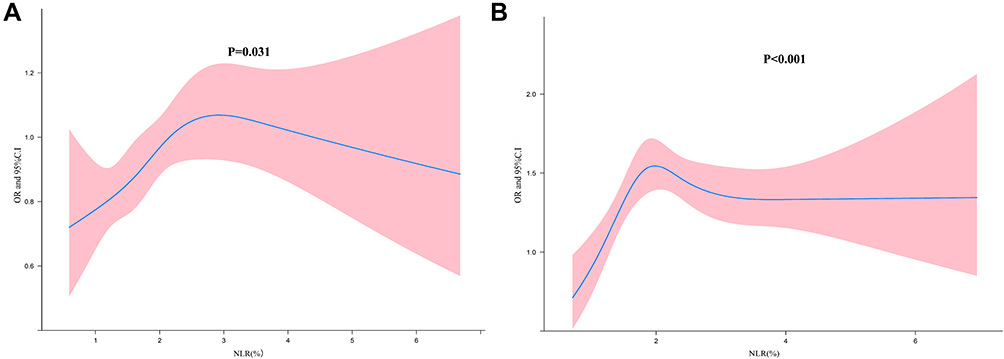 |
Figure 3 The association between NLR level and the risk of NAFLD under different gender in BF group. (A) The females; (B) the males. |
Discussion
In this study, which included 10,547 participants, we found that exposure to famine in early life increased the prevalence of NAFLD. We also found a non-linear relationship between NLR and the risk of developing NAFLD in individuals who were born during the famine period. To our knowledge, this is the first study to explore the non-linear relationship between NLR and the risk of NAFLD in individuals who were born during the famine period.
In our study, NAFLD prevalence was found to be higher in BF group and is higher than in NBF group. Previous studies have also shown that exposed to famine in early life is a risk factor for NAFLD.20 A larger study by Lu21 showed that women and men exposed to famine had a significantly higher risk of NAFLD than those not exposed. Data from Chongqing city suggest similar results.22 Our study indicated that the male prevalence of NAFLD (57.6%) was higher than that of women (47.6%) in the BF group. Compared with previous studies, our research suggests a higher prevalence of NAFLD, which might be related not only to fetal and childhood malnutrition but also influenced by adulthood lifestyle.23 The participants in this study were recruited from the Jiangsu province, which is the richest region in China. Exposure to famine in early life, poor lifestyle and an abundance of diet in adulthood might all contribute to a higher risk of NAFLD.24 Song XC reported that the prevalence of NAFLD in Jiangsu was 36.80% in 2016,25 higher than that in the Beijing and Jiangxi provinces in China. Age is also a key risk factor of NAFLD.17 Participants in our sample have a mean age 53.05±1.38 years old, an age in which there is high incidence of NAFLD.
In this study, we analyzed the relationship between NLR and NAFLD in BF group. The results show that NLR is the risk of NAFLD in participants who were born during the famine period and in females who were non-exposed to famine. The NLR is a systemic inflammatory factor that is known to contribute to the first line of defense against infection and plays a major anti-inflammatory role.26 Previous studies reported that NLR was associated with liver diseases. For example, Li et al27 found that NLR was a marker for predicting mortality of hepatitis B virus-related decompensated cirrhosis. A study by Khoury et al28 found a significant independent correlation between NLR and advanced inflammation and fibrosis in patients with NAFLD. The ABUND study,8,29 which was conducted by professor Gulali Aktas, found some serum levels of inflammatory markers, such as NLR and serum uric acid to high-density lipoprotein–cholesterol ratio, were related with NAFLD. However, a negative relationship between NLR and NAFLD was reported by Wen.11 These seemingly controversial results might relate with the non-linear relationship between NLR levels and the risk of NAFLD. In our study, we found that when NLR was less than 3% in women or 2% in men, there was a linear relationship between NLR and the risk of developing NAFLD. However, when NLR was above 3% in women or 2% in men, the relationship between NLR and NAFLD was non-linear. In the women, our results showed a reduced risk of developing NAFLD with NLR level above 3% (Figure 3).
To the best of our knowledge, this is the first study to find a non-linear association between NLR and NAFLD. Previous studies showed that increased NRL levels were related to inflammatory activation;30 NAFLD can be considered a low-grade inflammation state and elevated NLR levels increase the risk of developing NAFLD.31 The pathophysiological mechanisms underlying the relationship between NLR and NAFLD might be related to oxidative stress.32 A study in rats study showed that reducing neutrophil myeloperoxidase could induce oxidative stress and activate inflammation.26 Accumulation of neutrophils and lymphocytes in the liver promotes the progression of NAFLD, but also act as anti-inflammatory factors, and injury repair.33,34 Therefore, based on our results, we considered that NLR might have a promoting effect in the early inflammation process, but a repairing role in the later stages of inflammation.
Our study is an age-matched, large cross-sectional study. Although we found a non-linear association between NLR and the risk of developing NAFLD in individuals who were exposed to famine in early life, this study also has some limitations. First, our study is a cross-sectional study and is not able to explore the causal relationship between changes in NLR and NAFLD. Second, all participants were recruited from Xuzhou city and might not be generalizable to other races and populations. Third, we did not collect the detailed data of physical activity and dietary habit because of restriction of data collection method. The interaction effect of physical activity, dietary habit and exposure to famine in early life were not assessed.
In summary, we found that the individuals who were exposed to famine in early life have a higher NAFLD prevalence than those who were not exposed to famine. Elevated NLR is a risk factor of developing NAFLD, and there is a non-linear relationship between NLR and the risk of developing NAFLD. These findings further our understanding of the role of inflammation in NAFLD. NLR may be useful to diagnose and follow subjects with hepatic steatosis, especially for the individuals exposed to famine in early life.
Data Sharing Statement
All data generated or analyzed during this study are included in this manuscript.
Ethics Approval and Consent to Participate
The study was reviewed and approved by the ethics committee of the Xuzhou Central Hospital. The no. of ethics committee approval is XZXY-LJ-20201110-060.
Acknowledgments
We acknowledge and thank all participants for their cooperation and sample contributions.
Funding
This work was supported by the Xuzhou Municipal Science and Technology Bureau (KC21208) and the Xuzhou Health Commission (XWKYHT20210559).
Disclosure
All authors declare that there is no duality of interest associated with this manuscript.
References
1. Huang DQ, El-Serag HB, Loomba R. Global epidemiology of NAFLD-related HCC: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2021;18(4):223–238. doi:10.1038/s41575-020-00381-6
2. Younossi ZM, Golabi P, de Avila L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol. 2019;71(4):793–801. doi:10.1016/j.jhep.2019.06.021
3. Kaya E, Yılmaz Y. Non-alcoholic fatty liver disease: a growing public health problem in Turkey. Turk J Gastroenterol. 2019;30(10):865–871. doi:10.5152/tjg.2019.18045
4. Papatheodoridi M, Cholongitas E. Diagnosis of Non-alcoholic Fatty Liver Disease (NAFLD): current concepts. Curr Pharm Des. 2018;24(38):4574–4586. doi:10.2174/1381612825666190117102111
5. Buzzetti E, Pinzani M, Tsochatzis EA. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism. 2016;65(8):1038–1048. doi:10.1016/j.metabol.2015.12.012
6. Kauppinen A, Suuronen T, Ojala J, Kaarniranta K, Salminen A. Antagonistic crosstalk between NF-κB and SIRT1 in the regulation of inflammation and metabolic disorders. Cell Signal. 2013;25(10):1939–1948. doi:10.1016/j.cellsig.2013.06.007
7. Posul E, Yilmaz B, Aktas G, Kurt M. Does neutrophil-to-lymphocyte ratio predict active ulcerative colitis? Wien Klin Wochenschr. 2015;127(7–8):262–265. doi:10.1007/s00508-014-0683-5
8. Aktas G, Sit M, Dikbas O, et al. Elevated neutrophil-to-lymphocyte ratio in the diagnosis of Hashimoto’s thyroiditis. Rev Assoc Med Bras. 2017;63(12):1065–1068. doi:10.1590/1806-9282.63.12.1065
9. Bae BK, Park HC, Yoo GS, Choi MS, Oh JH, Yu JI. The significance of systemic inflammation markers in intrahepatic recurrence of early-stage hepatocellular carcinoma after curative treatment. Cancers. 2022;14(9):2081. doi:10.3390/cancers14092081
10. Abdel-Razik A, Mousa N, Shabana W, et al. A novel model using mean platelet volume and neutrophil to lymphocyte ratio as a marker of nonalcoholic steatohepatitis in NAFLD patients: multicentric study. Eur J Gastroenterol Hepatol. 2016;28(1):e1–e9. doi:10.1097/MEG.0000000000000486
11. WenYi J, Ting Q, PiaoPiao Y, JinMing W. Association between neutrophil-to-lymphocyte ratio with inflammatory activity and fibrosis in non-alcoholic fatty liver disease. Turk J Gastroenterol. 2022;33(1):53–61. doi:10.5152/tjg.2022.20715
12. Emamat H, Farhadnejad H, Movahedian M, Tangestani H, Mirmiran P, Hekmatdoost A. Dietary sodium intake in relation to non-alcoholic fatty liver disease risk: a case-control study. Nutr Food Sci. 2021;51(3):541–550. doi:10.1108/NFS-05-2020-0183
13. Emamat H, Ghalandari H, Tangestani H, Abdollahi A, Hekmatdoost A. Artificial sweeteners are related to non-alcoholic fatty liver disease: microbiota dysbiosis as a novel potential mechanism. EXCLI J. 2020;19:620–626. doi:10.17179/excli2020-1226
14. Berna G, Romero-Gomez M. The role of nutrition in non-alcoholic fatty liver disease: pathophysiology and management. Liver Int. 2020;40(Suppl 1):102–108. doi:10.1111/liv.14360
15. Qi H, Hu C, Wang S, et al. Early life famine exposure, adulthood obesity patterns and the risk of nonalcoholic fatty liver disease. Liver Int. 2020;40(11):2694–2705. doi:10.1111/liv.14572
16. Liu J, Wang G, Wu Y, et al. Early-life exposure to famine and risk of metabolic associated fatty liver disease in Chinese adults. Nutrients. 2021;13(11):4063. doi:10.3390/nu13114063
17. Alqahtani SA, Schattenberg JM. NAFLD in the Elderly. Clin Interv Aging. 2021;16:1633–1649. doi:10.2147/CIA.S295524
18. Srichaikul K, Hegele RA, Jenkins DJA. Great Chinese famine and the effects on cardiometabolic health for future generations. Hypertension. 2022;79(3):532–535. doi:10.1161/HYPERTENSIONAHA.121.18546
19. European Association for the Study of the L, European Association for the Study of D, European Association for the Study of O. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. 2016;64(6):1388–1402. doi:10.1016/j.jhep.2015.11.004
20. Wang Y, Jin J, Peng Y, Chen Y. Exposure to Chinese famine in the early life, adulthood obesity patterns, and the incidence of hypertension: a 22-year cohort study. Ann Nutr Metab. 2021;77(2):109–115. doi:10.1159/000515060
21. Wang N, Chen Y, Ning Z, et al. Exposure to famine in early life and nonalcoholic fatty liver disease in adulthood. J Clin Endocrinol Metab. 2016;101(5):2218–2225. doi:10.1210/jc.2016-1076
22. Zheng X, Ren W, Gong L, Long J, Luo R, Wang Y. The great Chinese famine exposure in early life and the risk of nonalcoholic fatty liver disease in adult women. Ann Hepatol. 2017;16(6):901–908. doi:10.5604/01.3001.0010.5281
23. Jung UJ, Choi MS. Obesity and its metabolic complications: the role of adipokines and the relationship between obesity, inflammation, insulin resistance, dyslipidemia and nonalcoholic fatty liver disease. Int J Mol Sci. 2014;15(4):6184–6223. doi:10.3390/ijms15046184
24. Yan S, Hou W, Wu H, et al. Prenatal exposure to the Chinese famine and the risk of metabolic syndrome in adulthood across consecutive generations. Eur J Clin Nutr. 2020;74(8):1229–1236. doi:10.1038/s41430-020-0561-3
25. Song X, Ma Q, Mao J, et al. Analysis of related risk factors of nonalcoholic fatty liver disease. Jiangsu J Prev Med. 2016;27(1):21–25.
26. Tavasoli S, Eghtesadi S, Vafa M, Moradi-Lakeh M, Sadeghipour A, Zarnani AH. High dose pomegranate extract suppresses neutrophil myeloperoxidase and induces oxidative stress in a rat model of sepsis. Int J Vitamin Nutr Res. 2019;89(5–6):271–284. doi:10.1024/0300-9831/a000563
27. Li X, Wu J, Mao W. Evaluation of the neutrophil‐to‐lymphocyte ratio, monocyte‐to‐lymphocyte ratio, and red cell distribution width for the prediction of prognosis of patients with hepatitis B virus‐related decompensated cirrhosis. J Clin Lab Anal. 2020;34(11). doi:10.1002/jcla.23478
28. Khoury T, Mari A, Nseir W, Kadah A, Sbeit W, Mahamid M. Neutrophil-to-lymphocyte ratio is independently associated with inflammatory activity and fibrosis grade in nonalcoholic fatty liver disease. Eur J Gastroenterol Hepatol. 2019;31(9):1110–1115. doi:10.1097/MEG.0000000000001393
29. Kosekli MA, Kurtkulagii O, Kahveci G, et al. The association between serum uric acid to high density lipoprotein-cholesterol ratio and non-alcoholic fatty liver disease: the abund study. Rev Assoc Med Bras. 2021;67(4):549–554. doi:10.1590/1806-9282.20201005
30. Rodriguez-Rodriguez E, Lopez-Sobaler AM, Ortega RM, Delgado-Losada ML, Lopez-Parra AM, Aparicio A. Association between neutrophil-to-lymphocyte ratio with abdominal obesity and healthy eating index in a representative older Spanish Population. Nutrients. 2020;12(3):855. doi:10.3390/nu12030855
31. Saltiel AR, Olefsky JM. Inflammatory mechanisms linking obesity and metabolic disease. J Clin Invest. 2017;127(1):1–4. doi:10.1172/JCI92035
32. Li Z, Wu K, Zou Y, Gong W, Wang P, Wang H. PREX1 depletion ameliorates high-fat diet-induced non-alcoholic fatty liver disease in mice and mitigates palmitic acid-induced hepatocellular injury via suppressing the NF-κB signaling pathway. Toxicol Appl Pharmacol. 2022;448:116074. doi:10.1016/j.taap.2022.116074
33. Parthasarathy G, Revelo X, Malhi H. Pathogenesis of nonalcoholic steatohepatitis: an overview. Hepatol Commun. 2020;4(4):478–492. doi:10.1002/hep4.1479
34. Daiber A, Steven S, Weber A, et al. Targeting vascular (endothelial) dysfunction. Br J Pharmacol. 2017;174(12):1591–1619. doi:10.1111/bph.13517
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.