")
Back to Journals » Clinical and Experimental Gastroenterology » Volume 12
Association Between Gastric Lymphoid Follicles (Precursor Of MALT Lymphomas) And H. pylori Infection At A Referral Hospital In Iran
Authors Bashiri H, Esmaeilzadeh A, Vossoughinia H, Ghaffarzadegan K, Raziei HR, Bozorgomid A
Received 26 July 2019
Accepted for publication 10 October 2019
Published 29 October 2019 Volume 2019:12 Pages 409—413
DOI https://doi.org/10.2147/CEG.S224823
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Koulaouzidis
Homayoon Bashiri,1,2 Abbas Esmaeilzadeh,3 Hassan Vossoughinia,3 Kamran Ghaffarzadegan,4 Hamid Reza Raziei,5 Arezoo Bozorgomid1
1Infectious Diseases Research Center, Kermanshah University of Medical Sciences, Kermanshah, Iran; 2Department of Internal Medicine, Faculty of Medicine, Kermanshah University of Medical Sciences, Kermanshah, Iran; 3Gastroenterology and Hematology Department, Faculty of Medicine, Ghaem Hospital, Mashhad, Iran; 4Pathology Department, Education and Research Department, Razavi Hospital, Mashhad, Iran; 5Department of Oncology and Radiology, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
Correspondence: Arezoo Bozorgomid
Infectious Diseases Research Center, Kermanshah University of Medical Sciences, Kermanshah, Iran
Tel +98 918 872 8269
Email [email protected]
Purpose: Mucosa-associated lymphoid tissue (MALT) is the most common endoscopic finding in Helicobacter pylori positive patients that can progress to MALT lymphoma after a prolonged antigenic contact. This study was aimed to evaluate the prevalence of lymphoid follicles and aggregates (precursors of MALT lymphomas) in gastric mucosal biopsies and their correlation with H. pylori infection.
Patients and methods: In this study, 100 patients who had undergone an upper gastrointestinal endoscopy were enrolled. Five biopsy specimens were taken each patient through screening endoscopy and histopathological changes were evaluated and graded using the Wotherspoon System. The clinical background and H. pylori infection status were also investigated.
Results: Among the 100 cases in our series, 79 patients (79%) showed evidence of MALT in at least one biopsy specimen taken from the stomach and 21 cases (21%) had no evidence of MALT. H. pylori infection was detected in 74 (74%) patients. Lymphoid follicles were detected more frequently in H. pylori-positive patients (59%) compared to H. pylori-negative cases (3%) (P<0.001).
Conclusion: The frequency of lymphoid follicles and aggregates in gastric mucosal is associated with H. pylori infection. Further community-based studies in larger sample sizes using a combination of microscopic methods and PCR assay are required for effective monitoring of H. pylori infection.
Keywords: gastritis, Helicobacter pylori, lymphoid aggregate, lymphoid follicle
Introduction
Helicobacter pylori (H. pylori) is a spiral, gram-negative bacterium that causes chronic gastritis, peptic ulcer disease and is associated with the development of gastric cancer.1 Its prevalence is about 4.4 billion individuals in worldwide, affecting more than half of the world’s population.2 Chronic infection of the stomach by H. pylori is being increasingly recognized as a precursor of mucosa-associated lymphoid tissue (MALT) lymphoma.3 Gastric cancer is the fifth most common cancer. It is that estimated about one million new cases and 783,000 related deaths occur every year.4 Gastric MALT lymphoma accounts for only 1-6% of all gastric malignancies and about 50% of primary gastric lymphomas.5
H. pylori infection serves as an antigenic driver that can activate innate immune system. As a result of this phenomenon, the immune and gastric epithelial cells respond by the secretion antimicrobial peptides and cytokines (pro- and anti-inflammatory).6 Immune response accelerates the formation of lymphoid follicles in the gastric mucosa.6 This statement is supported by the fact that about 75% of low-grade gastric MALT lymphoma can be improved by eradication of H pylori infection with antibiotic therapy.7
Mucosa-associated lymphoid tissue (MALT) lymphoma is defined as an extranodal low-grade marginal zone B cell lymphomas.8 Although the stomach is the most common site of MALT lymphomas, it in healthy individuals does not have organized or diffuses lymphoid tissue.9 Symptoms associated with gastric MALT lymphoma are generally non-specific and signs including dyspepsia, vague epigastric pain, bloating and heartburn; anemia, melena as well as hematemesis are common in this disease.10 The clinical diagnosis of gastric MALT lymphoma depends largely on clinical symptoms, endoscopic examination and histopathologic finding of gastric biopsy tissue.10
Studies have shown that the incidence of gastric cancer in Iran, unlike developed countries, has increased over the past 30 years.11,12 This study was designed to determine the prevalence of gastric lymphoid follicles and aggregates (precursors of MALT lymphomas) in gastric mucosal biopsies and evaluate its correlation with H. pylori infection.
Materials And Methods
This cross-sectional study was conducted in 100 consecutive patients admitted to Imam Reza Hospital (a referral center affiliated with Kermanshah University of Medical Sciences) Kermanshah, Iran for endoscopic screening. Five biopsy specimens were taken from each patient through endoscopy (1 from incisura angularis, 2 from antrum, lesser and greater curvature and 2 from cardia, lesser and greater curvature). Biopsy specimens were fixed in 10% formalin and embedded in paraffin. Then, 4-µm paraffin sections were stained with hematoxylin and eosin and Giemsa. All the available slides were evaluated for the presence of lymphoid aggregates, lymphoid follicles and other pathological changes in gastric mucosa by two pathologists, independently. The Wotherspoon scoring system was used for scoring gastric lymphoid infiltrates. Based on the histological scoring system of the Wotherspoon, a score of 2 or less is categorized as benign gastritis and a score of 3 or 4 represents suspicious MALT lymphoma cases.13
To detect the presence of H. pylori, all biopsy specimens were evaluated by rapid urease test and Gram staining. Patients were considered positive for H. pylori if it was detected on histological and/or bacteriological examination. Exclusion criteria were a history of H. pylori eradication, a history of consumption of proton pump inhibitors (PPIs), H2-receptor blockers or antibiotics within 2 weeks prior to endoscopy and a history of gastric surgery or gastric neoplasms.
Associations between categorical variables were evaluated with Chi-squared test and Fisher’s exact test. The P < 0.05 was considered as statistically significant.
Results
This study was conducted in 40 men and 60 women aged 22–62 years old (median: 49 years). The distribution of biopsy specimens according to the histological score in each gastric region is summarized in Table 1. Seventy-nine patients (79%) showed evidence the presence of MALT in at least one biopsy specimen taken from the stomach and 21 cases (21%) had no evidence of MALT.
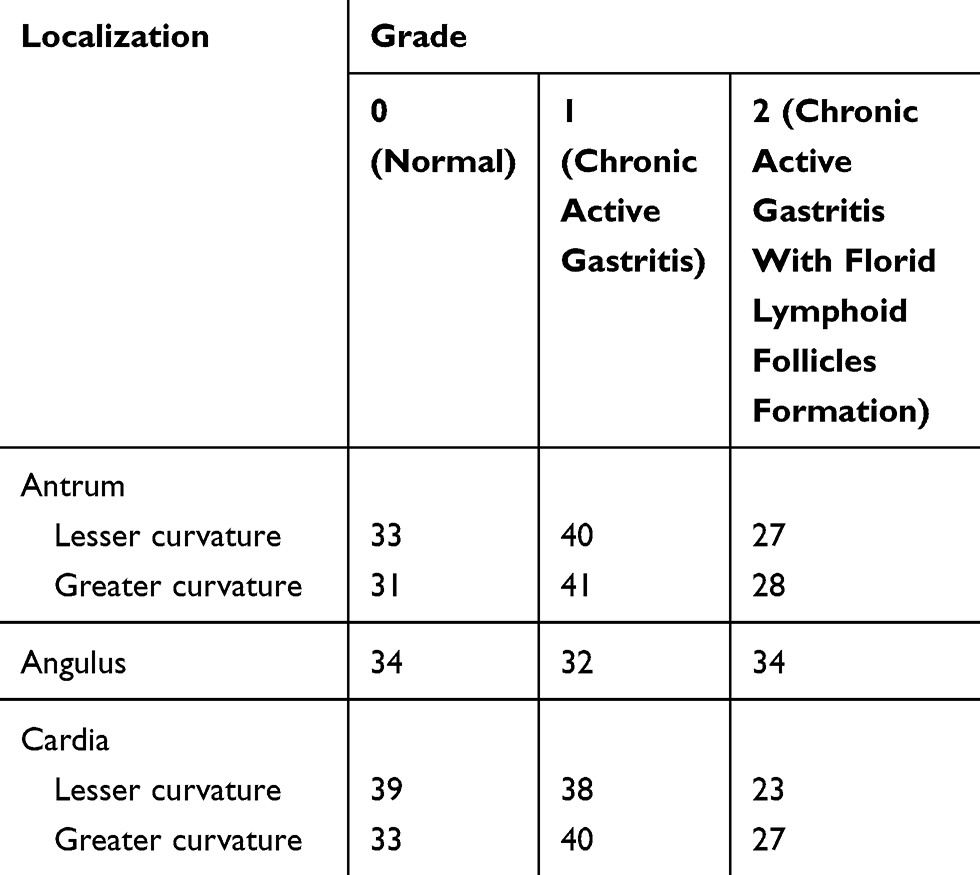 |
Table 1 Frequency Of Graded Histological Variables In Patients Admitted To Imam Reza Hospital, Kermanshah, Iran |
Overall, H. pylori was detected in 74 (74%) patients. The relationship between mucosa-associated lymphoid tissue and H. pylori infection is shown in Table 2, indicating that 71% of the patients with mucosa-associated lymphoid tissue had H. pylori infection as opposed to 8% of them who did not (P<0.001). Additionally, lymphoid follicles were detected more frequently in H. pylori-positive patients (59%) compared to H. pylori-negative cases (3%) (Table 3).
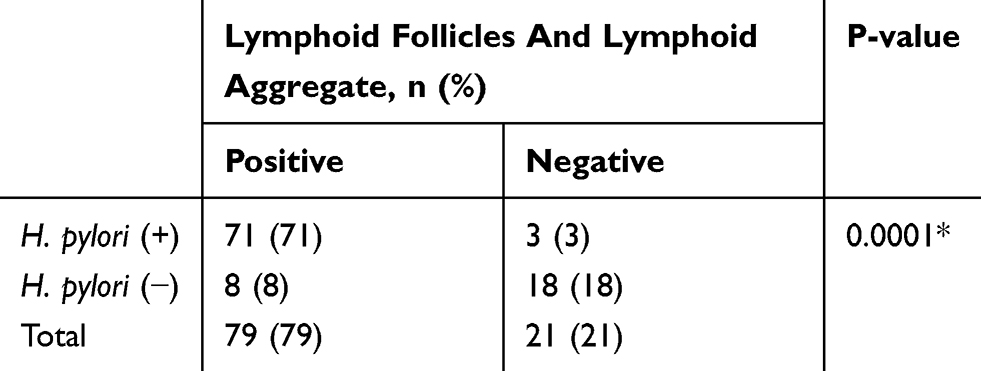 |
Table 2 The Distribution Of Helicobacter pylori According To Presence Lymphoid Follicles And Lymphoid Aggregate |
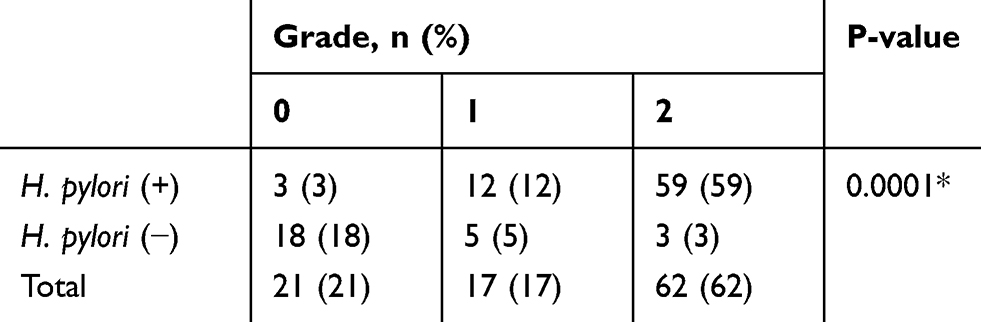 |
Table 3 Histological Grading Of All Biopsies In Relation To The Presence Of Helicobacter pylori |
Discussion
This study evaluated the prevalence of lymphoid follicles and aggregates (precursors of MALT lymphomas) in gastric mucosal biopsies and correlates them with H. pylori infection at a referral hospital in the western part of Iran. MALT lymphomas are non-Hodgkins B-cell neoplasms derived from lymphoid aggregates in the lamina propria.8 According to previous reports, lymphoid follicles and aggregates in the gastric mucosa are a specific the immune response to H. pylori.14 This organism serves as an antigenic driver that can activate the immune system and accelerate lymphoid follicles proliferation in the gastric mucosa.6
In the present study, the prevalence of H. pylori infection was 74%. The prevalence of H. pylori ranges from 15.1% to 87.7% in previous publications depending on the socioeconomic status, hygiene and sanitary conditions.15 Improvements in these factors lead to a decrease in the prevalence of H. pylori and consequently in the peptic ulcer disease. The host immune response, especially the functionality of cytotoxic T-cells (killer T-cells), plays a key role in the outcome of H. pylori infection.14 Although half of the world’s population is infected with this bacterium, only about 3% of all H. pylori infected subjects present with gastric adenocarcinoma.16 Some reports have described that H. pylori cagA-positive strains have enhanced pathogenicity by stimulating cell transformation.17
Iran is one of the largest developing countries in the Middle East with highly diverse dietary factors, lifestyle preferences, socioeconomic and hygiene conditions. According to the 2012 Census results, Iran has a population of 80.28 million and about one-third of the population lives below the national poverty line.18 In a study conducted by Solimany et al, findings indicated a growing rate of gastric malignancy incidence in Kermanshah Province, where we carried out this study.19 The clinical diagnosis of gastric MALT lymphoma depends largely on clinical symptoms, endoscopic examination and histopathologic finding of gastric biopsy tissue.10 Countries with high incidence of gastric cancer, such as Japan and South Korea, have implemented gastric cancer screening programs using endoscopy for several decades.20,21 During the last years, endoscopy has been widely used as a part of health screening. However, few studies have reported some side effects for endoscopic screening, such as infections, false-positive results, and overdiagnosis.22 Although upper gastrointestinal endoscopy is an invasive procedure, further evaluation of the impact of endoscopic screening is needed regarding the balance of cost and mortality reduction.
Fakhro et al found that the prevalence of lymphoid follicles and aggregates was 31.4% and 24.5% in gastric biopsy specimens in patients with dyspepsia, respectively.23 Also, authors reported that the odds ratio of developing lymphoid follicles in H. pylori-positive patients compared to H. pylori-negative cases was 11:1. Kalebi et al found that the prevalence of lymphoid follicles was 11% among adult patients seen at a referral hospital in Kenya and all these patients had H pylori infection.24 Garg et al also reported that there are lymphoid aggregates and lymphoid follicles in 25% and 19% of subjects, respectively.25 In our study, prevalence of lymphoid follicles and aggregates in gastric mucosa in patients with H. pylori infection was 62% and 38%, respectively and lymphoid follicles were detected more frequently in H. pylori-positive patients (59%) compared to H. pylori-negative cases (3%) (P<0.001). The differences in prevalence can be explained by differences in the number and site of biopsy specimens, methods of H. pylori detection, and study populations. Furthermore, the bacterial load in biopsy specimens is generally low and irregular.26 It appears that prevalence of lymphoid follicles and aggregates in oxyntic mucosa (14.8–44.0%) is lower than antral mucosa.27
Previous studies showed that H. pylori is associated with an increased risk of gastric adenocarcinomas.28,29 Persistent inflammation of the stomach by H. pylori leads to the transition from normal mucosa to chronic superficial gastritis which may then progress to atrophic gastritis and intestinal metaplasia, and eventually to dysplasia and adenocarcinoma.28,29 There is no evidence to support the association between atrophic gastritis and gastric lymphoma.30 Although both gastric adenocarcinomas and MALT lymphomas occur as a consequence of chronic gastric inflammation, differentiating them from each other is important because the prognosis and treatment options differ.
Conclusion
Our findings showed that the formation of gastric lymphoid follicles and aggregates significantly correlated with H. pylori infection. Early diagnosis and eradication of H. pylori infection in suspicious MALT lymphomas detected via histopathological evaluation will improve the patient’s quality of life and possibly prevent gastric cancer. Further community-based studies in larger sample sizes using a combination of microscopic methods and PCR assay are required for effective monitoring of H. pylori infection.
Ethics Approval And Consent To Participate
All the participants provided written informed consent prior to the study and this study was conducted in accordance with the Declaration of Helsinki. The protocol was approved by the Mashhad University of Medical Sciences Ethics Committee (8103907).
Data Sharing Statement
The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request and were received permission for use by the Mashhad University of Medical Sciences Ethics Committee.
Acknowledgments
The authors want to thank their colleagues in Imam Reza Therapeutic Educational hospital of Kermanshah, Iran for their contribution to the patient’s diagnosis. This study was funded by Mashhad University of Medical Sciences, Mashhad, Iran (No code: 2127).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alfarouk KO, Bashir AH, Aljarbou AN, et al. The possible role of Helicobacter pylori in gastric cancer and its management. Front Oncol. 2019;9:75. doi:10.3389/fonc.2019.00075
2. Hooi JK, Lai WY, Ng WK, et al. Global prevalence of Helicobacter pylori infection: systematic review and meta-analysis. Gastroenterology. 2017;153(2):420–429. doi:10.1053/j.gastro.2017.04.022
3. Floch P, Mégraud F, Lehours P. Helicobacter pylori strains and gastric MALT lymphoma. Toxins. 2017;9(4):132. doi:10.3390/toxins9040132
4. Rawla P, Barsouk A. Epidemiology of gastric cancer: global trends, risk factors and prevention. Prz Gastroenterol. 2019;14(1):26–38. doi:10.5114/pg.2018.80001
5. Nakamura S, Matsumoto T. Gastrointestinal lymphoma: recent advances in diagnosis and treatment. Digestion. 2013;87(3):182–188. doi:10.1159/000350051
6. Chmiela M, Karwowska Z, Gonciarz W, Allushi B, Stączek P. Host pathogen interactions in Helicobacter pylori related gastric cancer. World J Gastroenterol. 2017;23(9):1521–1540. doi:10.3748/wjg.v23.i9.1521
7. Zullo A, Hassan C, Cristofari F, et al. Effects of Helicobacter pylori eradication on early stage gastric mucosa–associated lymphoid tissue lymphoma. Clin Gastroenterol Hepatol. 2010;8(2):105–110. doi:10.1016/j.cgh.2009.07.017
8. Bacon CM, Du M-Q, Dogan A. Mucosa-associated lymphoid tissue (MALT) lymphoma: a practical guide for pathologists. J Clin Pathol. 2007;60(4):361–372. doi:10.1136/jcp.2005.031146
9. Isaacson PG, Du MQ. Gastrointestinal lymphoma: where morphology meets molecular biology. J Pathol. 2005;205(2):255–274. doi:10.1002/path.1703
10. Hu Q, Zhang Y, Zhang X, Fu K. Gastric mucosa-associated lymphoid tissue lymphoma and Helicobacter pylori infection: a review of current diagnosis and management. Biomark Res. 2016;4:15. doi:10.1186/s40364-016-0068-1
11. Jenabi E, Saatchi M, Khazaei S, et al. National distribution of stomach cancer incidence in Iran: a population-based study. Adv Hum Biol. 2019;9(1):89–93. doi:10.4103/AIHB.AIHB_37_18
12. Rahimi F, Heidari M. Time trend analysis of stomach cancer incidence in the west of Iran. J Health Dev. 2012;1(2):100–111.
13. Wotherspoon AC, Diss T, Pan L, et al. Regression of primary low-grade B-cell gastric lymphoma of mucosa-associated lymphoid tissue type after eradication of Helicobacter pylori. Lancet. 1993;342(8871):575–577. doi:10.1016/0140-6736(93)91409-f
14. Kuo S-H, Cheng A-L. Helicobacter pylori and mucosa-associated lymphoid tissue: what’s new. Hematology Am Soc Hematol Educ Program. 2013;2013(1):109–117. doi:10.1182/asheducation-2013.1.109
15. Toscano EP, Madeira FF, Dutra-Rulli MP, et al. Epidemiological and clinical-pathological aspects of Helicobacter pylori infection in brazilian children and adults. Gastroenterol Res Pract. 2018;2018:8454125. doi:10.1155/2018/8454125
16. Correa P, Piazuelo MB. Helicobacter pylori infection and gastric adenocarcinoma. US Gastroenterol Hepatol Rev. 2011;7(1):59–64.
17. Kalaf EA, Al-Khafaji ZM, Yassen NY, Al-Abbudi FA, Sadwen SN. Study of the cytoxin-associated gene a (CagA gene) in Helicobacter pylori using gastric biopsies of Iraqi patients. Saudi J Gastroenterol. 2013;19(2):69–74. doi:10.4103/1319-3767.108474
18. Statistical Centre of Iran. Summary and statistical report of the 2012 population and housing census. Tehran: Population census commission Mazandaran Province: population census commission Amol County. 2012.
19. Solimany A, Khoramdad M, Khademi N, Delpisheh A. Spatio-temporal study of gastric cancer incidence in Kermanshah Province, Iran during the years 2009–2014. Asian Pac J Cancer Prev. 2018;19(10):2871–2876. doi:10.22034/APJCP.2018.19.10.2871
20. Chung SJ, Park MJ, Kang SJ, et al. Effect of annual endoscopic screening on clinicopathologic characteristics and treatment modality of gastric cancer in a high‐incidence region of Korea. Int J Cancer. 2012;131(10):2376–2384. doi:10.1002/ijc.27501
21. Choi KS, Jun JK, Lee HY, et al. Performance of gastric cancer screening by endoscopy testing through the National Cancer Screening Program of Korea. Cancer Sci. 2011;102(8):1559–1564. doi:10.1111/j.1349-7006.2011.01982.x
22. Hamashima C. Benefits and harms of endoscopic screening for gastric cancer. World J Gastroenterol. 2016;22(28):6385–6392. doi:10.3748/wjg.v22.i28.6385
23. Fakhro ARE, Bahaa El Din AF, Farid IMA, Jamsheer HM. The association between Helicobacter pylori infection and lymphoid reaction in patients suffering from dyspepsia in Bahrain. Saudi J Gastroenterol. 1999;5(3):129–133.
24. Kalebi A, Rana F, Mwanda W, Lule G, Hale M. Histopathological profile of gastritis in adult patients seen at a referral hospital in Kenya. World J Gastroenterol. 2007;13(30):4117–4121. doi:10.3748/wjg.v13.i30.4117
25. Garg B, Sandhu V, Sood N, Sood A, Malhotra V. Histopathological analysis of chronic gastritis and correlation of pathological features with each other and with endoscopic findings. Pol J Pathol. 2012;63(3):172–178.
26. Pokhrel N, Khanal B, Rai K, Subedi M, Bhattarai NR. Application of PCR and microscopy to detect Helicobacter pylori in gastric biopsy specimen among acid peptic disorders at tertiary care centre in Eastern Nepal. Can J Infect Dis Med Microbiol. 2019;2019. doi:10.1155/2019/3695307
27. Zaitoun A. The prevalence of lymphoid follicles in Helicobacter pylori associated gastritis in patients with ulcers and non-ulcer dyspepsia. J Clin Pathol. 1995;48(4):325–329. doi:10.1136/jcp.48.4.325
28. Ishaq S, Nunn L. Helicobacter pylori and gastric cancer: a state of the art review. Gastroenterol Hepatol Bed Bench. 2015;8(Suppl 1):S6–S14.
29. Díaz P, Valenzuela Valderrama M, Bravo J, Quest AFG. Helicobacter pylori and gastric cancer: adaptive cellular mechanisms involved in disease progression. Front Microbiol. 2018;9:5. doi:10.3389/fmicb.2018.00005
30. Ishikura N, Usui Y, Ito H, et al. Helicobacter pylori (HP) infection alone, but not HP-induced atrophic gastritis, increases the risk of gastric lymphoma: a case-control study in Japan. Ann Hematol. 2019;98(8):1981–1987. doi:10.1007/s00277-019-03721-y
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.