")
Back to Journals » Patient Preference and Adherence » Volume 15
Association Between Caregivers’ Family Management and Quality of Life in Children with Chronic Disease in Southern Thailand
Authors Sutthisompohn S , Kusol K
Received 2 July 2021
Accepted for publication 7 September 2021
Published 22 September 2021 Volume 2021:15 Pages 2165—2174
DOI https://doi.org/10.2147/PPA.S327553
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Video abstract presented by Sirikran Sutthisompohn.
Views: 353
Sirikran Sutthisompohn, Kiatkamjorn Kusol
School of Nursing, Walailak University, Nakhon Si Thammarat, Thailand
Correspondence: Kiatkamjorn Kusol
School of Nursing, Walailak University, 222 Thaiburi, Thasala District, Nakhon Si Thammarat, Thailand
Tel +66 81-979-6565
Email [email protected]
Purpose: Caring for children with chronic diseases, caregivers have to manage their child’s daily life to prevent complications and improve their quality of life. This study investigated family management of children with chronic diseases, quality of life of children, and correlation between family management of caregivers and quality of life of children as perceived by the caregivers.
Patients and Methods: This cross-sectional study collected data from 200 pairs of caregivers and children with asthma, anemia, and thalassemia aged 5 to 12 years after receiving treatment and follow-up in the pediatric outpatient department of the tertiary hospital, June to November 2020. Research instruments comprised a Family Management Measure (FaMM) and the Pediatric Quality of Life Inventory (PedsQL 4.0). Data were analyzed using descriptive and Spearman rank correlation coefficient statistics.
Results: The caregivers of children obtained a mean score on family management of 166.88 (S.D.= 11.32). The quality of life of children with chronic illness had a mean score of 66.59 (S.D.= 18.63). Correlation analysis revealed that easy family management of the caregivers had a positive correlation with the quality of life of children with chronic diseases. On the contrary, difficulty in family management negatively correlated with the quality of life of the children.
Conclusion: Most caregivers could have easy family management in caring for the children. In summary, easy family management will allow children with chronic illness to receive decent care from their caregivers, contributing to improved quality of life.
Keywords: family management, quality of life, chronic illness, children, caregiver
Introduction
Over the past few decades, the number of children diagnosed with chronic diseases has been rising every year1 due to advanced medical treatment translating into the increased survival rates and saving lives of children with chronic illness from lethal threats more effectively than in the past.2 In Asia, China has witnessed many children with chronic diseases hospitalized due to several conditions, including chronic kidney diseases, diabetes, and Rheumatic disease.3 A similar trend In Thailand and the standard conditions leading to hospitalization are hematology abnormality, respiratory disease, heart disease, cancer, etc. Furthermore, the mortality rates of the children suffering from chronic diseases are the highest; males aged 5–14 years tended to experience it more than females.4 When children fall ill due to the long-term and unpredictable symptoms of the diseases, they also lack practical thinking and decision-making in caring for themselves because of immature growth and development. Thus, caregivers will have to care for their children with chronic diseases with specific goals in mind not only to prevent complications or mortality rates but also to encourage their quality of life.2,5 Such responsibility undoubtedly has ripple impacts on the physical and mental well-being of both the caregivers and the children.3,6
The Family Management Style Framework (FMSF), which widely adopted by Knafl, Deatrick, and Havill (2012), extends its scope over various dimensions: it addresses the extent of perception, needs, thought, and beliefs which caregivers have regarding daily routines in response to chronic conditions of children to see whether it leads to easy or difficult family management based on six aspects: Child’s daily life, Condition management ability, Condition management effort, Family life difficulty, view of condition impact and Parental mutuality based on the Family Management Measure. For result interpretation, high total scores in three aspects, including Child’s daily life, Condition management ability, and Parental mutuality, denote effortless family management style. In contrast, high scores in the three other areas, including Condition management effort, Family life difficulty, and view of condition impact, denote complex family management style.7
Research on the FMSF revealed that caregivers of children with chronic diseases exhibit inconsistent and discontinuous family management as indicated by high mean scores in some parts of family management.3,8–12 However, it also depends on the diversity of factors influencing family management, as uncovered in the study in Duangdech, Patoomwan, Pookboonmee, Orathai, and Rehm (2017) investigating family management for children with cerebral palsy in Thailand. Findings suggested that family hardiness and severity were the factors involved in family management and affected children’s health conditions.13 Similarly, Sutthisompohn et al demonstrated that asthma severity had a positive correlation and was a predictive factor of family management.10 Moreover, the age of the caregivers, number of medicines used, education, income, and family functioning also had some effects on family management for children.3,14,15
Four components, more specifically, their characteristics, determine whether family management of the caregivers will be easy or difficult: attributes of the illness, person, family, and environment.7 The quality of life of chronic diseases in children is one of the crucial goals for treatment. It involves caregivers’ preference of happiness, enabling children with chronic conditions to carry out their daily routines the same way children at their age commonly do. First, physical functioning is concerned with perceiving an ability to exercise, cope with pain and fatigue. The second is emotional functioning which is fear, sadness, anger, anxiety, and sleep. The last two include social and school functioning: the perception of relationships with others and difficulties in learning, memorizing, working on, completing assignments, and being absent from school to receive continual treatments typical among children with chronic diseases. The PedsQL 4.0 can be employed to assess these perceptions.16
Previous studies demonstrated that children with chronic diseases usually undergo substandard life quality due to limitations caused by the disease-generated symptoms and health conditions.5,17,18 A systematic review by Hall et al found that factors generating impacts on the quality of life of children comprise child’s age, caregivers’ knowledge, duration of illness, recurrence of diseases, ability to control symptoms, and the number of hospitalization.1 Besides, some studies uncovered that easy family management affects the quality of life in children with chronic diseases.3,19–21 Therefore, family management of children may influence the quality of life of children with chronic illnesses.
Previous studies found that each family of children with chronic diseases adopted different management methods depending on the factors related to family management ability.3,10,13–15 In this study, the researchers believe that caregivers’ family management may affect the quality of life of the children as perceived by their caregivers. Thus, the researchers appreciate the importance of researching family management and the quality of life of children with chronic diseases in Southern Thailand. And the correlation between family management carried out by caregivers with chronic diseases according to the FMSF by Knafl et al7 covers six aspects and quality of life four elements of perception focused on physical, emotional, social, and school functioning. The most common chronic diseases in children follow-up in the pediatric outpatient department of the Maharaj Nakhon Si Thammarat Hospital, including asthma and thalassemia, and anemia among children aged 5–12 years. It’s aimed to serve as a guideline for promoting caregivers’ family management so that the caregivers give efficiently aligned with the treatment goals, mitigating the severity of the illnesses, preventing complications, and promoting the quality of life of children at their age deserve.
Patients and Methods
Study Design, Setting, and Sample
In the cross-sectional study, the sample was among 200 pairs of caregivers and their children with chronic diseases (asthma, anemia, and thalassemia) aged 5 to 12 years and followed up in a pediatric outpatient department, Maharaj Nakhon Si Thammarat Hospital, Thailand, over the period between June to November 2020. G*Power 3.1 with the level of power set at 0.95 and effect size set at 0.30 were employed to calculate the number of research samples.22 Sample grouping was conducted using proportional sampling with children suffering from three types of chronic diseases who came to receive treatment at Maharaj Nakhon Si Thammarat Hospital most frequently from October 2018 to September 2019: asthma, anemia, and thalassemia. After that, purposive sampling was employed to select a group of caregiver research samples based on the inclusion criteria: aged 18 years or older, responsible for managing, caring, and making treatment decisions and, live in the same households with the selected children with asthma, anemia, thalassemia aged 5 to 12 years and have suffered from the conditions longer than three months. Both the caregivers and children consented to participate in this research. We were in a good state of mind and communication in Thai.
Questionnaire
Research instruments were detailed as follows:
1) A questionnaire on demographic data of caregivers: elicited data on age, relationship, status, education, occupation, income, and experience in caring for children with chronic diseases, and general data of the children including gender, age, age at which the first disease manifestation occurred, the number of times to the hospital for treatment, and the chronic diseases.
2) The FaMM investigating six aspects based on the framework proposed by Knafl et al, 2012, back-translated in 5 parts by Wattana, Jintrawet, and Lamchang and one factor by the researcher. The questionnaire consisted of 53 items assessed using five rating scales ranging from 1 score representing “strongly disagree” to 5 scores representing “strongly agree.” Score interpretation of easy family management involved a total score derived from 5 items on the management of a child’s daily life, 12 items on condition management ability, and 8 items on parental mutuality, which altogether yielded 25–125 scores. The score range of 87.50 to 125.00 signified easy family management. Turning to the problematic family management, scores in this aspect derived from 4 items on Condition management effort, 14 items on family life difficulty, and 10 items on condition impact. The score range of 84 to 140 signified complex family management.23
3) The PedsQL 4.0: There are 2 issues for 5–7 and 8–12 years old. The questionnaire consists of 23 items covering four aspects, including physical, emotional, social, and school functioning, rated by Likert’s scale five scores interpreted according to the perception of caregivers and children ranging from 0–4 scores in each item (0=100, 1=75, 2=50, 3=25, 4=0). High scores denote an excellent quality of life for children.16
Reliability and Validity
Content Validity
The PedsQL 4.0 had its content validity checked and the Item Content Validity Index (CVI) calculated, yielding the value of 0.88. The FaMM, whose five aspects were back-translated by Wattana et al, was supported by Family Assessment Device (FAD) and Eyberg Child Behavior Inventory (ECBI) and calculated using Pearson’s correlation coefficients statistical significance.23
Back Translation
The FaMM consisted of 8 items, granted permission from the tool owner, translated from English into Thai, back-translated from Thai into English by the specialized and experts in the two languages. Next, the researchers conducted an accurate cross-check of the translated content with the original Thai version and decided what to modify.
Reliability
As a try-out, the researcher administered the FaMM, and PedsQL 4.0 to 15 children with chronic diseases followed up in the pediatric outpatient department at the hospital. The reliability value was determined using Cronbach’s alpha coefficient. The six aspects comprised 1) Child’s daily life 2) Condition management ability 3) Condition management effort 4) Family life difficulty 5) Condition impact and 6) Parental mutuality, each of which had a Cronbach’s alpha of 0.92, 0.80, 0.81, 0.85, 0.89, and 0.93 respectively. For the PedsQL 4.0, with the caregivers’ accounts, the reliability was 0.89, and for the children with chronic diseases, the reliability was 0.92.
Statistics
Demographic data, caregivers’ family management, and quality of life were analyzed using descriptive statistics comprising frequency distributions, percentage, mean, standard deviation. Association between the caregivers’ family management and quality of life were analyzed using the Kolmogorov–Smirnov test demonstrating difference from a normal distribution, so the association was analyzed using the Spearman rank correlation coefficient statistics, determining statistical significance at 0.05.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. All procedures performed in studies involving human participants followed the ethical standards of the Ethical Institutional Consideration. This study received approval from Ethics Committee on Human Research at Walailak University on April 21, 2020. (WUEC-20-092-01) and Ethics Committee on Research of Maharaj Nakhon Si Thammarat Hospital on May 25, 2020 (WU-EC-NS-2-191-63) as required by the process before data collection. Inform consent; Researchers obtained from all individual participants included in the study.
Results
Demographic Data of Caregivers
Among the 200 caregivers, the majority, at 78.5% (n= 157) were mothers of children, 59% (n= 118) aged 21–40 years, 76.5% (n= 153) married, 41% (n= 82) graduating with secondary education, 31.5% (n= 63) making living employment. In terms of household incomes, 40% (n= 80) earned less than 10,000 Thai baht, and most of the caregivers at 62% (n= 124) had gained previous experience in caring for children with chronic diseases (Table 1).
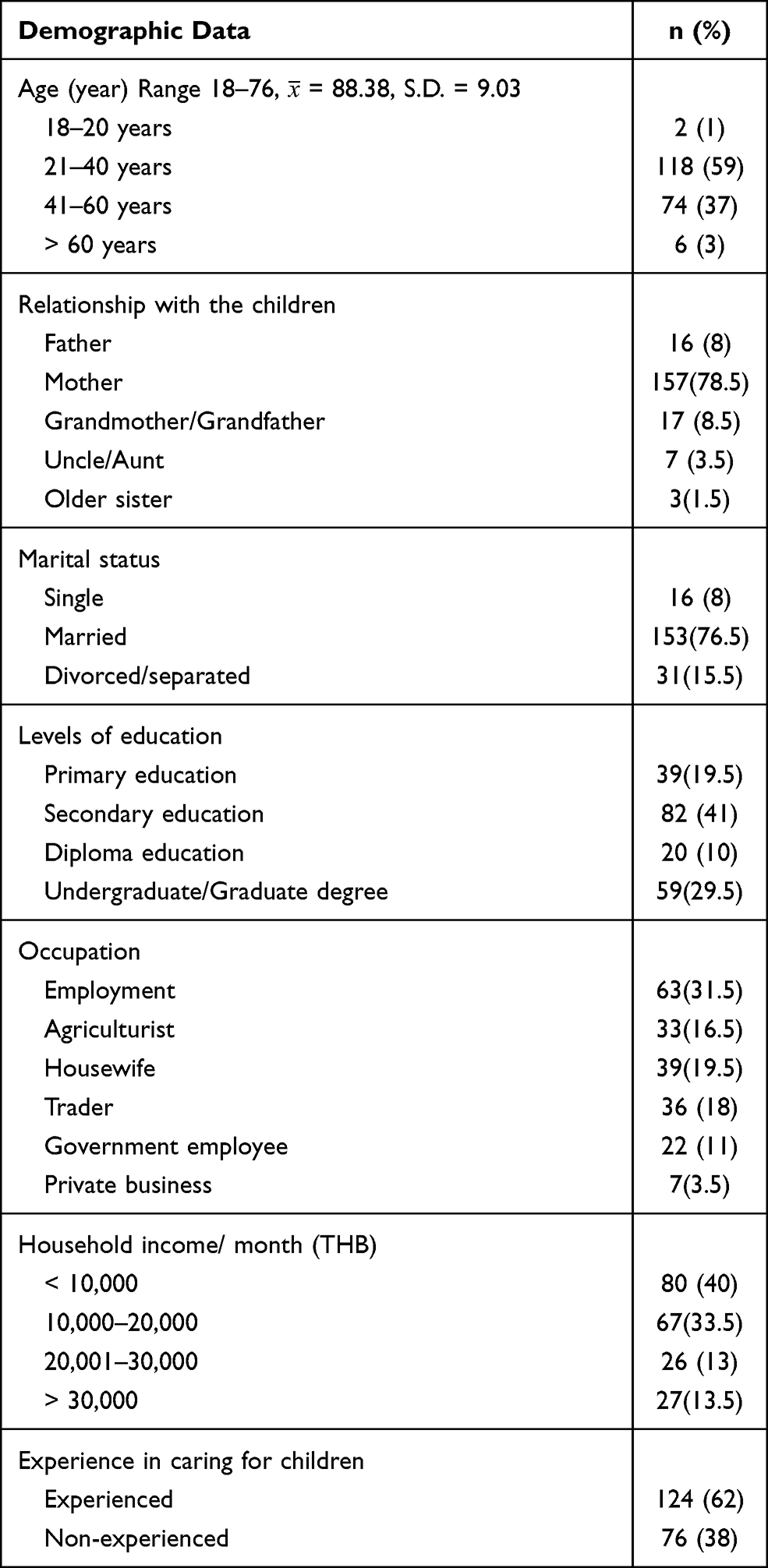 |
Table 1 Demographic Data of Caregivers (n = 200) |
Demographic Data of Children with Chronic Disease
Among the 200 children with chronic diseases, 58% (n= 116) were male, 42% (n= 84) were female, 52% (n= 104) aged 5–7 years, 41% (n= 82) manifesting the illness for the first time younger than one year, 38% (n= 76) received treatment at the hospital 1 to 3 times/year. Half of the children with chronic diseases, at 50.5% (n= 101) had asthma (Table 2).
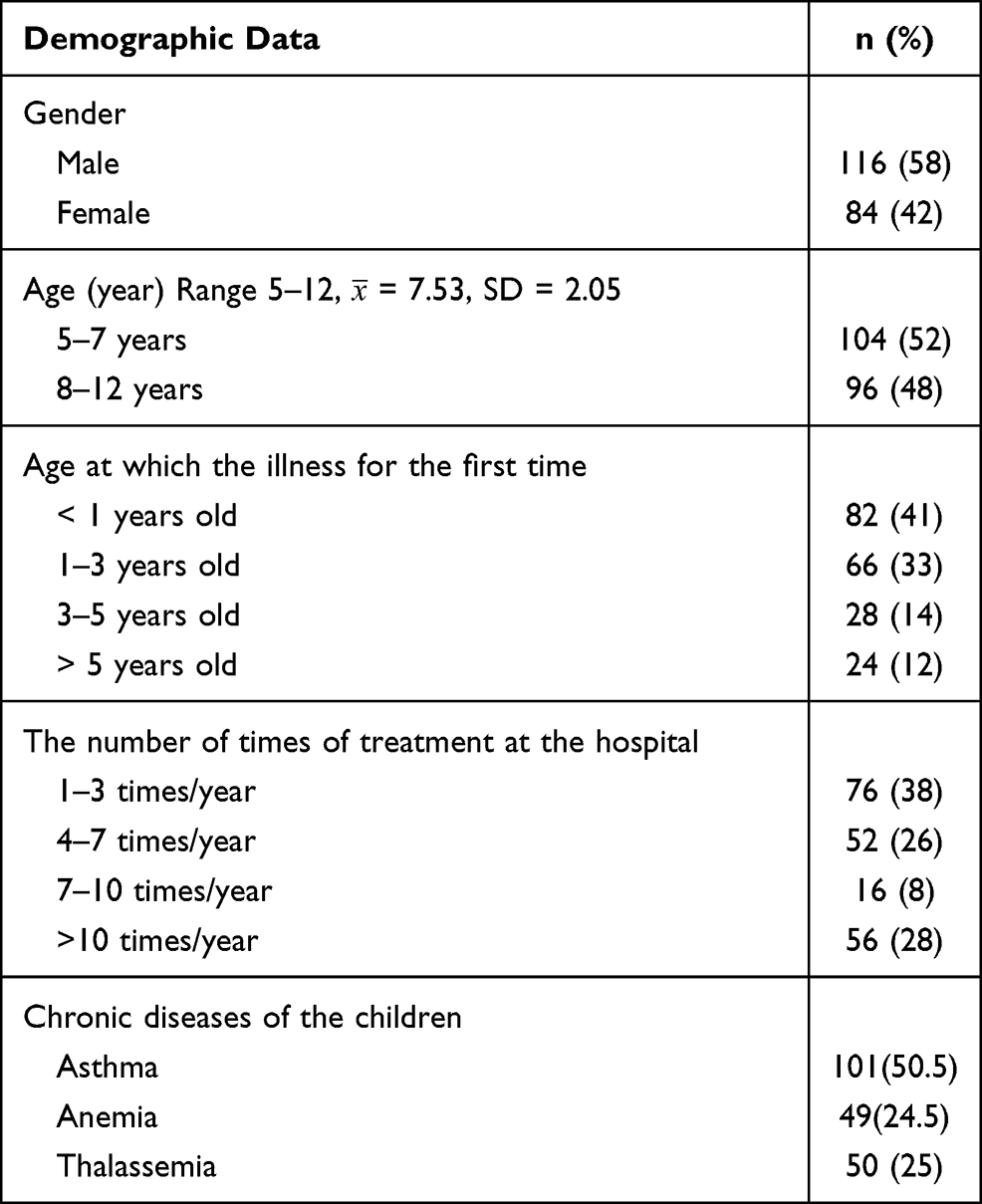 |
Table 2 Demographic Data of Children with Chronic Disease (n= 200) |
Family Management of Caregiver
The 200 caregivers obtained a mean score of 166.88 out of 256 on family management, 98.71 scores on easy, and 68.18 on difficulty family management: the scores were high on easy and were low on difficulty reveal that the caregivers of chronic illness children had the easy family management. When categorized by the diseases, caregivers tended to the children who obtained mean scores on family management thalassemia, anemia, and asthma ( = 169.28, 168.27, and 165.03).
= 169.28, 168.27, and 165.03).
When categorized based on easy aspects, children with asthma scored the maximum ( = 99.87), followed by anemia (
= 99.87), followed by anemia ( = 99.61). Furthermore, the caregivers with asthma received the top mean score on the child’s daily life and condition management ability aspects (
= 99.61). Furthermore, the caregivers with asthma received the top mean score on the child’s daily life and condition management ability aspects ( =19.96, and 47.23), respectively. However, those caring for the children with anemia scored the top (
=19.96, and 47.23), respectively. However, those caring for the children with anemia scored the top ( = 33.35) on family management in parental mutuality. On the other hand, turning to difficult family management, the caregivers of children with thalassemia received the top mean score (
= 33.35) on family management in parental mutuality. On the other hand, turning to difficult family management, the caregivers of children with thalassemia received the top mean score ( = 73.82), followed by anemia (
= 73.82), followed by anemia ( = 68.65) (Table 3).
= 68.65) (Table 3).
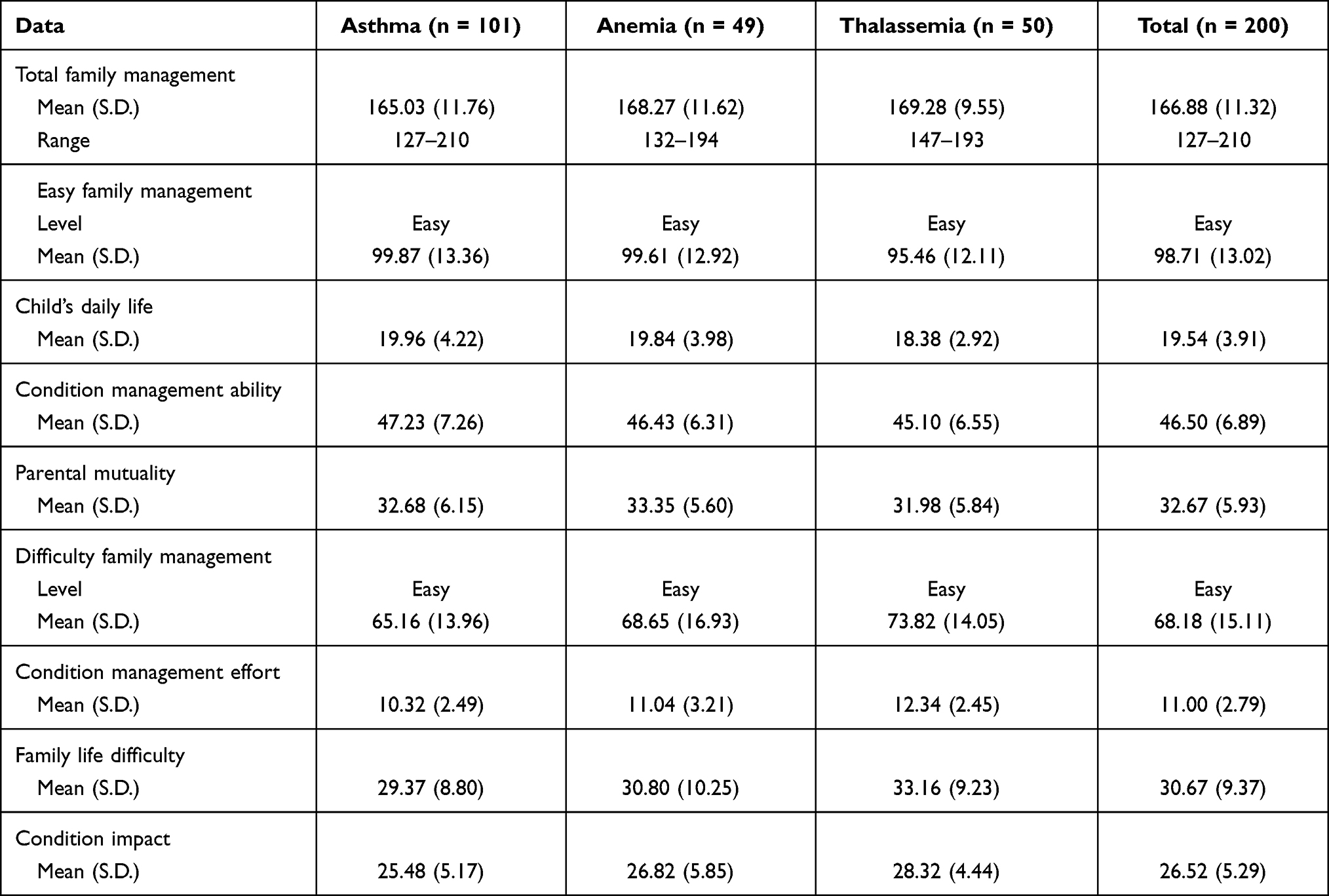 |
Table 3 Level, Mean Scores, and Standard Deviation of Family Management in Caregivers |
Quality of Life in the Children with Chronic Diseases
Quality of life perceived by caregivers yielded the mean score of 66.59 and 81.45 based on the children. It found that the caregivers with all types of chronic diseases gave a higher score on the quality of life to psychosocial than physical functioning. But the mean score on physical was higher than psychosocial functioning from the perception of children. When categorized by types of diseases, the children with asthma were found with the maximum mean scores on quality of life—based on the perception of both the caregivers and children (Caregivers = 67.91, and children = 83.39), followed by the pairs dealing with anemia (Caregivers = 67.35 and children = 82.36) (Table 4).
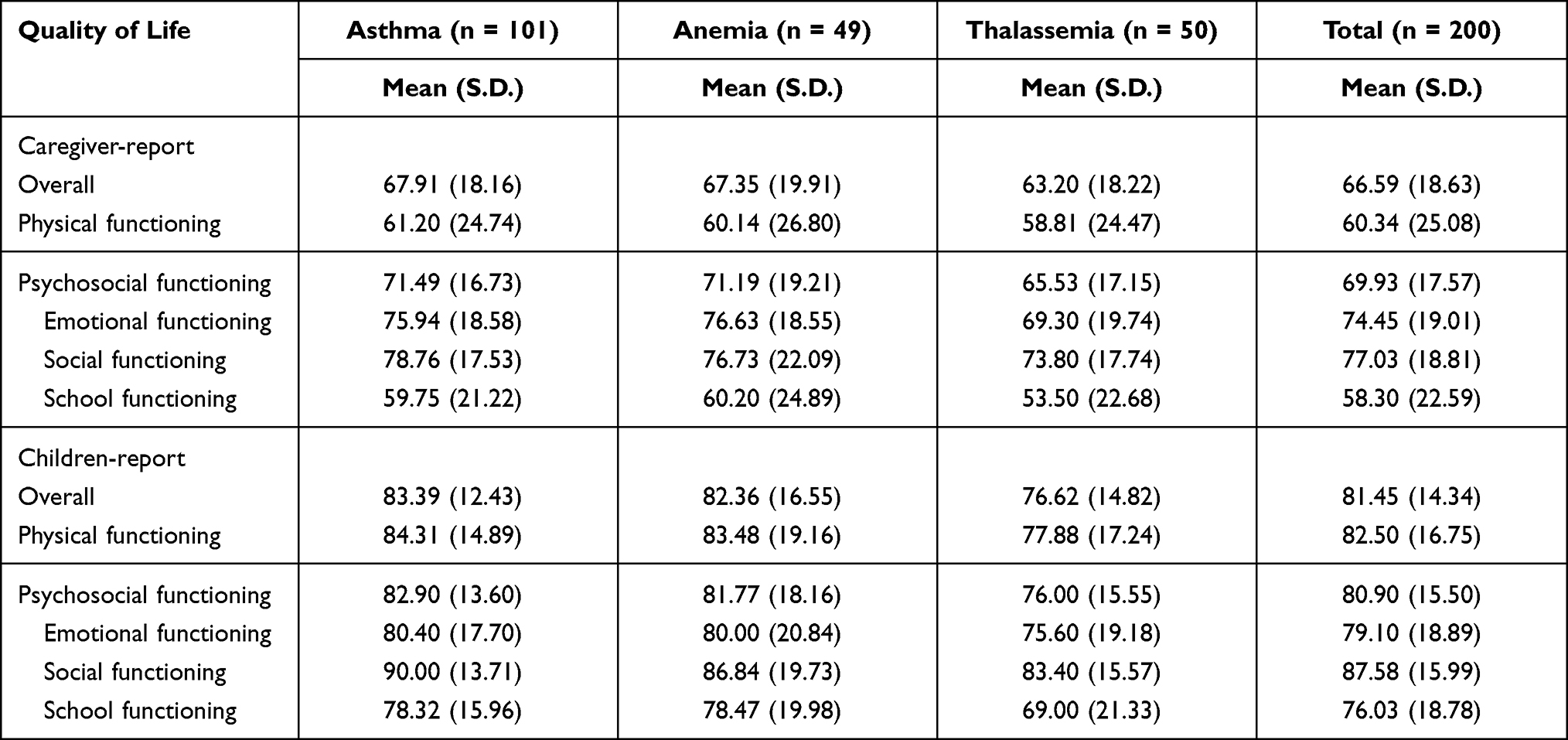 |
Table 4 Mean Scores and Standard Deviation of Quality of Life as Perceived by Caregivers and Children |
The Relationship Between Caregivers’ Family Management and Quality of Life in Children
Correlation between family management of the caregivers and the quality of life of the children perceived by a caregiver was analyzed using the Spearman rank correlation. Results suggested that easy family management positively correlated with the overall quality of life with statistical significance (r= 0.22, p< 0.01). Looking into each aspect, it was found that easy family management had a positive correlation with quality of life in psychosocial (r= 0.25, p< 0.01), emotional (r= 0.24, p< 0.01), and social functioning (r= 0.23, p< 0.01). On the other hand, it negatively correlated difficult family management and overall quality of life (r= −0.26, p< 0.01). Going by aspects, difficult family management had a negative correlation with the quality of life in physical (r= −0.15, p< 0.05) psychosocial (r= −0.29, p< 0.01) emotional (r= −0.36, p< 0.01) and social functioning (r= −0.24, p< 0.01) (Table 5).
 |
Table 5 Correlation Coefficient Statistics Between Family Management and Quality of Life (n = 200) |
Discussion
Family Management of Caregivers
The family management of caregivers in children with chronic diseases demonstrated that the caregivers averaged 166.88 on the six aspects. The mean score on easy family management was 98.71, while difficult family management yielded 68.18, resulting in the interpretation that the caregivers had easy family management. In more detail, most of them, at 78.5%, were mothers demoting biological relation. Fifty-nine percent of the caregivers were aged 21–40 years divided into early and mid-adults, and 41% completed secondary education. Therefore, the caregivers were presumably more capable of making decisions and caring for children than younger or older adults.10,14,15
Moreover, the caregivers had gained some experience caring for children with chronic diseases. The caregivers were aware of children with chronic illnesses for an extended period. In this regard, the children may exhibit persistent or severe symptoms enabling them to live their lives quite similar to other children at their age. It was consistent with the study by Jones, Whitehead, and Crowe (2016), reporting that caregivers with previous experience in caring for children with chronic diseases during the time with no relapses or stable condition had more confidence and ability to care for children than within an emergency period.24 Besides, the children within the 5–12 age characterized by improved rational thinking and partial self-care abilities, so they could care for themselves without relying on others entirely.
In contrast, some caregivers were divorced or separated, resulting in enormous responsibility for singlehandedly care for the children. Being deprived of no assistance caused exhaustion and stress. The caregivers worked full-time, resulting in insufficient time to care for the children to their most total ability. Some caregivers needed to take some time off from their jobs, meaning reduced incomes since their children required treatment at the hospital. The study also uncovered that they earned less than 10,000 THB per month. It was consistent with numerous previous studies on factors influencing family management for children with chronic disease suggesting that role in a family, age, educational levels of caregivers, stable occupations providing sufficient incomes, age of children, and the period in which the diseases were active, less severity of the disease and social support were all the factors determining whether caregivers of children would have easy or difficult family management.3,10,12,14,15,25
Categorized by diseases, the caregivers obtained similar family management, namely thalassemia, anemia, and asthma. However, organized by aspects, the caregivers of children with asthma obtained the maximum mean scores on easy family management, followed by those caring for the children with anemia and thalassemia. Furthermore, the caregivers of children with asthma who scored received the maximum mean scores on the child’s daily life and condition management ability. However, in parental mutuality, those caring for the children with anemia obtained the highest mean scores. In complex family management, the caregivers of children with thalassemia received the highest mean score, followed by those caring for the children with anemia and asthma. Consistent with the study by Mendes et al, families of children with asthma experienced management of difficulties in family life on a lower level than families of children with diabetes and epilepsy.12 For example, asthma naturally causes inflammation in the respiratory system, so the management is primarily centered on medication or inhalers to keep the symptoms under control or prevent a relapse. Environmental management to avoid any stimulants is also focused on it. The disease’s prognostic trend seems to be better as age increases.26 However, thalassemia is a condition of an abnormal blood system that needs to receive a blood transfusion and checkup to detect strange blood, mainly suffering from iron overload.21 The caregivers cannot be managed procedures by themselves but need to be treated by health care providers. Caregivers of children with thalassemia showed lower mean family management scores than the children with asthma.
Quality of Life in the Children with Chronic Diseases
According to the overall caregiver accounts, the quality of life of children with chronic diseases in this study suggested that the quality of life obtained a lower mean score than that based on the children’s accounts. At the same time, reports of the caregivers gave a higher mean score to quality of life in psychosocial functioning than physical functioning, versions of the children assigned a higher mean score to the physical functioning than the psychosocial functioning. Furthermore, children with chronic diseases scored the highest on quality of life in social functioning but the lowest in school functioning. It can explain that even though children with chronic illnesses can go to school, study hard, perform in class and do homework, frequent school absence for doctor’s appointments or treatment at a hospital during the relapse period also occurs.17,27 It’s similar in this study; some children with chronic disease needed to visit the hospital for treatment more frequently than ten times a year. Turing to quality of life in physical functioning, caregivers and children were aware of performing a daily routine such as walking, running, exercising, etc. In emotional functioning, both caregivers and children were slightly concerned. It indicates that the caregivers may not genuinely understand the needs of the children with chronic disease causing them to feel afraid of and concerned about their unpredictable conditions. They also expected their children to have the same quality of life as others their age do. Therefore, the caregivers acknowledge that the quality of life of children with chronic diseases was lower than that perceived by the children, and perception in each aspect was different.1
Data suggested that the children with asthma obtained the highest mean score, followed by anemia and thalassemia. The quality of life of children based on the caregivers found that the children with anemia received the highest mean in emotional functioning and school functioning. Based on the children’s accounts, those with similar anemia obtained the highest mean quality of life scores in school functioning. This finding indicated that both the children with asthma and their caregivers perceive happiness in life and live the same as or quite similar to the other chronic disease children at the same age the most compared to children with other diseases. It may be because asthma does not characteristically have complex disease progression or severe complications resulting in less frequent hospital visits. This finding harmonized with that by Mendes et al.12
Nonetheless, in case of an asthmatic attack or severe uncontrollable symptoms, exercise-induced bronchospasm decreases children’s physical activities with asthma.28 Children need to administer an inhaler, oxygen, etc. Children with asthma could also experience a lower quality of life.17,29 Still, children with thalassemia suffering from low hemoglobin in the blood system will annually need more than six times per year blood transfusion,21 in worse cases, some of whom have to do the splenectomy or experience complications: transfusion allergic reaction, hepatitis, delayed growth, and malnutrition. In addition, children with these diseases may need to be hospitalized for an extended period, causing them to have a lower quality of life than those with asthma.27,31
Correlation of Caregiver’s Family Management and Quality of Life of Chronic Illness Children
The easy family management comprises a child’s daily life, condition management ability, and parental mutuality exhibited a positive correlation in the low level with the quality of life of the children with chronic diseases. It was consistent with the findings of the study by Sheng et al, putting forward that the caregivers with easy family management provided quality of life to children with a chronic disease.3 This can explain that 157 caregivers were mothers related to chronic disease children by heredity, satisfaction in caring for their chronic disease child, and perception that they are not a burden. They understand and acknowledge illnesses of children with a chronic disease whose disease progression lasts for an extended period because they have had the chronic disease since the age below one year. Also, 62% of the caregivers had gained previous experiences caring for other children with chronic illnesses. Cumulative expertise contributes significantly to the confidence they have in caring for children with chronic conditions more effectively.24
However, 5–12 years-old children with chronic diseases have developmentally, to some degree, achieved the physical strength and capacity to care for themselves without entirely depending on their caregivers.30 The difference in each chronic disease may also be the result of the different family management. Hence, the caregivers or other family members could assume their daily routines and efficiently sought particular treatments and cared for children with chronic diseases. They administered medications or inhalers for asthma required in the treatment plan;10 Providing disease-specific diets or refraining from giving iron-rich food to those with thalassemia, taking the children to blood transfusion appointments, and consistently keeping track of laboratory results. Moreover, the caregivers in this study have been assisted by health care providers and accessed the health care service system with specific units to manage their child’s conditions. Children with chronic diseases might not exhibit any relapses or complications, meaning they could go through quite identical daily routines compared to other children at their age and 38% of them visited the hospital for treatment only 1–3 times a year. With this, the caregivers acknowledged that the children had a good quality of life. It was apparent that the caregiver and the chronic-disease children, other determinants came into play, affecting easy family management. As a result, the correlation between easy family management and the quality of life was low level. Going by aspect, data revealed that easy family management had a positive correlation with psychosocial functioning, emotional functioning, and social functioning, which was consistent with the study by Zhang et al, Im et al and Chusri et al uncovering that caregivers’ easy family management was related to a more stable emotional condition of the children: less frustration, irritability, adequate sleep, sociability and ability to play with their peers.15,19,21
Meanwhile, complex family management comprises a condition management effort, family life difficulty, and view of condition impact exhibited a negative correlation in the low level with the overall quality of life. It can explain that the caregivers acknowledged that the chronic diseases their children experienced complicated the family due to the diseases’ unpredictability. Additionally, this study indicated that 28% of the children with chronic diseases visited the hospital more than ten times annually. As a result, they experienced a substandard quality of life. In each aspect, it was evident that complex family management negatively correlated on a low level with the quality of life. The condition in which caregivers had difficult control significantly and negatively impacted the quality of life of children with chronic diseases. The children might need persistent hospital visits for treatment, have their physical movement limited, making them unable to exercise strength or follow daily routines, experience fatigue, pain, anxiety, and fear of the procedures incurring crying, tantrum, unsociability, or no interaction with others resulting in behavioral regression.27,29,31
Conclusion
This study has demonstrated that caregivers of children with all types of chronic diseases experience easy family management. Those caring for children with asthma have the most accessible family management. In contrast, those caring for children with thalassemia have the most challenging family management. Despite being identically categorized as chronic diseases, the progression of different diseases forges distinct family management approaches. Based on the caregivers’ accounts, the children’s quality of life is lower than that reported by the children with chronic diseases. The children with asthma have the best life quality, followed by those with anemia and thalassemia—easy family management results in improved life quality of children with chronic diseases. Therefore, the healthcare providers should pay attention to family management, create a family promotion, and optimize the administration regarding its quality, comprehensibility, and specificity for each type of chronic disease so that children suffering from diverse chronic conditions have access to a quality life.
Data Sharing Statement
Additional data are not available.
Acknowledgments
The authors wish to thank Kathleen Knafl for permitting to use of FaMM. I would also like to congratulate Mapi Research Trust Organization for allowing to use of PedsQL 4.0. My gratitude goes to the Research Institute for Health Sciences and the Excellence Center of Nursing Institute, Walailak University, to give me invaluable support. The assistance and cooperation provided by Maharaj Nakhon Si Thammarat Hospital and research participants were greatly appreciated.
Author Contributions
Both authors made a significant contribution during conception, study design, execution, data acquisition, analysis, interpretation, drafting, revising, and critically reviewing the article, and gave final approval of the version to be published. In addition, the authors agreed to the journal that the article was submitted to and to be accountable for all aspects of the work.
Funding
This work was supported financially by the Research Institute for Health Science (WU-IRG-63-021) and the Excellence Center of Nursing Institute, Walailak University. However, the University and Excellence Center had no role in designing, collecting, analyzing, and writing the manuscript.
Disclosure
The authors report no conflicts of interest for this work or regarding the publication of this paper.
References
1. Hall CA, Donza C, McGinn S, et al. Health-related quality of life in children with chronic illness compared to parents: a systematic review. Pediatr Phys Ther. 2019;31(4):315–322. doi:10.1097/PEP.0000000000000638
2. Piran P, Khademi Z, Tayari N, Mansouri N. Caregiving burden of children with chronic diseases. Electron Physician. 2017;9(9):5380–5387. doi:10.19082/5380
3. Sheng N, Ma J, Ding W, Zhang Y. Family management affecting transition readiness and quality of life of Chinese children and young people with chronic diseases. J Child Health Care. 2018;22(3):470–485. doi:10.1177/1367493517753712
4. Strategy and Planning Division, Ministry of Public Health. Public Health Statistics A.D. 2019. Nonthaburi: Ministry of Public Health; 2020.
5. Odgers HL, Tong A, Lopez-Vargas P, et al. Research priority setting in childhood chronic disease: a systematic review. Arch Dis Child. 2018;103(10):942–951. doi:10.1136/archdischild-2017-314631
6. Cohn LN, Pechlivanoglou P, Lee Y, et al. Health outcomes of parents of children with chronic illness: a systematic review and meta-analysis. J Pediatr. 2020;218:166–177.e2. doi:10.1016/j.jpeds.2019.10.068
7. Knafl KA, Deatrick JA, Havill NL. Continued development of the family management style framework. J Fam Nurs. 2012;18(1):11–34. doi:10.1177/1074840711427294
8. Chusri O, Deoisres W, van Riper M. The style of management in families having a child with thalassemia. SDU Res J. 2016;9(3):111–125.
9. Kim I, Ekas NV, Hock R. Associations between child behavior problems, family management, and depressive symptoms for mothers of children with an autism spectrum disorder. Res Autism Spectr Disord. 2016;26:80–90. doi:10.1016/j.rasd.2016.03.009
10. Sutthisompohn S, Lamchang S, Jintrawet U. Factors predicting family management among caregivers of children with asthma. Nurs J. 2020;47(4):27–38.
11. Kim DH, Im YJ. The influence of family management style on psychosocial problems of childhood cancer survivors in Korea. Eur J Oncol Nurs. 2015;19(2):107–112. doi:10.1016/j.ejon.2014.10.010
12. Mendes TPGP, Crespo CAM, Austin JK. Family cohesion and adaptation in pediatric chronic conditions: the missing link of the family’s condition management. J Child Fam Stud. 2016;25(9):2820–2831. doi:10.1007/s10826-016-0447-0
13. Duangdech W, Patoomwan A, Pookboonmee R, Orathai P, Rehm RS. A causal model of the health status of children with cerebral palsy. PRIJNR. 2017;21(4):291–304.
14. Close S, Sadler L, Grey M. In the dark: challenges of caring for sons with Klinefelter syndrome. J Pediatr Nurs. 2016;31(1):11–20. doi:10.1016/j.pedn.2015.05.002
15. Zhang Y, Wei M, Shen N, Zhang Y. Identifying factors related to family management during the coping process of families with chronic childhood conditions: a multi-site study. J Pediatr Nurs. 2015;30(1):160–173. doi:10.1016/j.pedn.2014.10.002
16. Varni JW. Scaling and Scoring of the Pediatric Quality of Life Inventory™ PedsQLTM. Lyon: Mapi Research Trust; 2013:7–8.
17. Kouzegaran S, Samimi P, Ahanchian H, Khoshkhui M, Behmanesh F. Quality of life in children with asthma versus healthy children. Open Access Maced J Med Sci. 2018;6(8):1413–1418. doi:10.3889/oamjms.2018.287
18. Liu X, Han Q. Risk factors on health-related quality of life in children with epilepsy. Clin Pediatr (Phila). 2015;54(14):1334–1338. doi:10.1177/0009922815580405
19. Im Y, Cho Y, Kim D. Family management style as a mediator between parenting stress and quality of life of children with epilepsy. J Pediatr Nurs. 2019;45:e73–e78. doi:10.1016/j.pedn.2018.12.007
20. Mendes TP, Crespo CA, Austin JK. The psychological costs of comparisons: parents’ social comparison moderates the links between family management of epilepsy and children’s outcomes. Epilepsy Behav. 2017;75:42–49. doi:10.1016/j.yebeh.2017.07.017
21. Chusri O, Deoisres W, van Riper M. Influencing of family management in families with thalassemic children on health-related quality of life and family functioning: SEM approach. Walailak J Sci Tech. 2017;16(1):27–38. doi:10.48048/wjst.2019.3653
22. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
23. Wattana S, Jintrawet U, Lamchang S. Factors Related to Family Management in Families Having Children with Congenital Heart Disease [Master’s Thesis Pediatric Nursing]. Chiang Mai: Chiang Mai University; 2018.
24. Jones V, Whitehead L, Crowe MT. Self-efficacy in managing the chronic respiratory disease: parents’ experiences. Contemp Nurse. 2016;52(2–3):341–351. doi:10.1080/10376178.2016.1213647
25. Yusuk P, Sananreangsak S, Teerarungsikul N. Factors related to maternal management for children with thalassemia. JOPN. 2019;11(1):151–162.
26. AlOtaibi E, AlAteeq M. Knowledge, and practice of parents and guardians about childhood asthma at King Abdulaziz Medical City for National Guard, Riyadh, Saudi Arabia. Risk Manag Healthc Policy. 2018;11:67–75. doi:10.2147/RMHP.S143829
27. Mettananda S, Pathiraja H, Peiris R, et al. Health-related quality of life among children with transfusion-dependent β-thalassemia major and hemoglobin E β-thalassemia in Sri Lanka: a case-control study. Health Qual Life Outcomes. 2019;17(1):137. doi:10.1186/s12955-019-1207-9
28. Van der Kamp MR, Thio BJ, Tabak M, Hermens HJ, Driessen J, Van der Palen J. Does exercise-induced bronchoconstriction affect physical activity patterns in asthmatic children. J Child Health Care. 2020;24(4):577–588. doi:10.1177/1367493519881257
29. Ibrahim NK, Alhainiah M, Khayat M, Abulaban O, Almaghrabi S, Felmban O. Quality of life of asthmatic children and their caregivers. Pak J Med Sci. 2019;35(2):521–526. doi:10.12669/pjms.35.2.686
30. Souto DO, Cruz TKF, Fontes PLB, Batista RC, Haase VG. Motor imagery development in children: changes in speed and accuracy with increasing age. Front Pediatr. 2020;8:100. doi:10.3389/fped.2020.00100
31. Mikael NA, Al-Allawi NA. Factors affecting quality of life in children and adolescents with thalassemia in Iraqi Kurdistan. Saudi Med J. 2018;39(8):799–807. doi:10.15537/smj.2018.8.23315
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.