")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Assessment of Type II Diabetes Patients’ Caregivers’ Burnout Level: A Cross-Sectional Study in Taif, Saudi Arabia
Authors Alsaedi YE, Almalki AA , Alqurashi RD, Altwairqi RS, Almalki DM, Alshehri KM, Alamri AA , Alswat KA
Received 6 January 2022
Accepted for publication 26 March 2022
Published 8 April 2022 Volume 2022:15 Pages 1091—1099
DOI https://doi.org/10.2147/DMSO.S357340
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Yousef E Alsaedi,1 Asim A Almalki,2 Rakan D Alqurashi,2 Rami S Altwairqi,3 Daifallah M Almalki,3 Khalid M Alshehri,3 Abdullah A Alamri,4 Khaled A Alswat5
1Public Health Department, Madinah Health Cluster, Madinah, Saudi Arabia; 2School of Medicine, Taif University, Taif, Saudi Arabia; 3Diabetes and Endocrine Specialist Center, Prince Mansour Military Hospital, Taif, Saudi Arabia; 4Endocrinology Department, Alhada Armed Forces Hospital, Taif, Saudi Arabia; 5Department of Medicine, School of Medicine, Taif University, Taif, Saudi Arabia
Correspondence: Yousef E Alsaedi, Public Health Department, Madinah Health Cluster, P.O. Box 8592, Madinah, 42391, Saudi Arabia, Tel +966597181795, Email [email protected]
Background: Diabetes mellitus type II (T2D) is a chronic condition that requires significant change in the family behavior and is associated with psychosocial conflicts for both patients and their family environment. The aim of this study is to assess burnout among relatives caring for patients with T2D.
Methods: This cross-sectional study with random sampling was conducted on 501 caregivers of patients with T2D between April and September 2021 at Prince Mansour armed forces hospital in Taif city, Saudi Arabia. Data collection tool was a modified version of the caregiver stress self-assessment questionnaire. Data analysis was then carried out using t-test and chi-square test (SPSS v20).
Results: The mean patient age was 64.4+12.0 years, female predominant with longstanding T2D. Metformin was the most prescribed T2D medication. The caregivers’ mean age was 34.9+12.4 years, male predominant, and around 45% of them report low level of education and income; 63.9% of the caregivers report little to no stress. Compared with caregivers with mild/moderate stress and moderate/severe stress, caregivers with little to no stress were more likely to be younger in age (P < 0.001), male (P = 0.464), single (P = 0.035), patient’s offspring (P = 0.490), caring for T2D patients with younger age (P = 0.058) and shorter T2D duration (P = 0.074), patients who were less likely to use a wheelchair (P = 0.008), patients who were less likely to be prescribed a complex insulin regimen and with better glycemic control parameters (both P > 0.05), and patients with higher HDL level (P = 0.037).
Conclusion: There were no correlations between the caregivers’ levels of stress and the T2D patients’ HbA1c levels. There was a significant positive correlation between a caregiver’s stress score and the caregiver’s age. Future studies are needed to assess other caregivers’ parameters and their relation to metabolic control of T2D patients.
Keywords: diabetes, burnout, caregiver
Introduction
Diabetes mellitus type II (T2D) is a chronic condition that requires significant change in the family behavior. According to the International Diabetes Federation Atlas, the worldwide prevalence of diabetes mellitus (DM) in adults was 9.3% in 2019 and is expected to increase to 10.2% and 10.9% in 2030 and 2045 respectively. The number of people with DM worldwide in 2019 was 463 million and is expected to increase to as much as 700 million in 2045.1 In Al Nozha et al. 2004, the overall prevalence of DM in Saudi Arabia among Saudis aged 30 years and older is 24% which represents a 10 times increase when compared with 2.5% in 1982.2,3 In 2014 Al-Rubeaan et al. showed that DM prevalence in Saudi Arabia was 25.4% for those aged ≥30 years and this percentage decreased to 11.9% when we consider the full age spectrum.4 This alarming trend of DM in Saudi Arabia over the last 3 decades has created an enormous burden on the healthcare system.5
Adherence to a diabetes management plan is associated with psychosocial conflicts for both patients and their family environment.6 When there was appropriate family behavior supporting a patient’s diabetes regimen, there was more satisfaction with the illness adaptation and less intervention to the planned regimen due to emotional problems.7 Given that chronic disease affects the quality of life of patients and family caregivers, the World Health Organization has stated that health care for chronic conditions should focus on the patients and their families.8,9
There are few studies that have assessed the quality of life of family caregivers of patients with DM and those that have examined this issue have insisted on taking the account of clinicians regarding a caregiver’s position.10–12 In a study done to assess the quality of life of family caregivers of patients with T2D, they found that family caregivers of patients with DM seemed to be at risk of depression and poor quality of life.13 This burnout will increase in cases of DM-related foot ulcers and hemodialysis.14,15
The term “ burnout ” was used firstly in aviation (in 1940) to describe a point at which the jet engines stop working. This term then translated to a meaning a heavy, monotonous and frustrating job, in which the person works harder and harder on a daily basis, with no satisfaction, until it seems that any action does not make any difference.16
In the light of these findings, we conducted this study to assess the burnout level among relatives caring for patients with T2D, bearing in mind other caregivers’ factors such as gender, age, financial status, educational level, marital status, and patients’ factors such as age, gender, duration of diabetes, and their relation to metabolic parameters.
Method
This cross-sectional study took place between April and September 2021 at Prince Mansour armed forces hospital in Taif city, Saudi Arabia and included Saudi patients with T2D and their caregivers attending the diabetes clinics for a regular follow-up visit. Random sampling included adult subjects caring for patients with T2D who agreed to take part in the study. We excluded caregivers who had been diagnosed with any psychiatric illness or having independent T2D themselves, as for the patients we excluded those who were younger than 18 years old or having the diagnosis of type 1 diabetes or gestational diabetes. If the participant reported a monthly income of 5000 SR or less, then we considered him/her to have a low income while those who reported a monthly income of 15,000 SR or more were considered to have a high income.
Ethical approval was obtained after fulfilling all the ethical requirements by the research ethical committee of the Armed Forces Hospitals before starting the data collection, approval No. 19/2/78/359 issued at 12/5/2019. All participants provided informed consent, in accordance with the Declaration of Helsinki.
Patients’ vital signs and body mass index (BMI) were recorded on the day of the interview. The data collection process was divided into two phases, the first phase included gathering data through a questionnaire which had two main parts, the first part was concerned with the sociodemographic data of the caregiver that includes caregiver’s age, gender, education, income, and relationship to the patient. The second part had 20 questions assessing the level of stress of the caregiver using the modified version of the caregiver stress self-assessment questionnaire by Dr. Steven Zarit, which is valid as a reliable tool for measuring the burden of caregivers. The questionnaire has 20 questions, each question is scored according to the response as 0: never, 1: rarely, 2: sometimes, 3: quite frequently and 4: nearly always, where the minimum score is zero and the maximum possible score is 80. Then the caregivers were stratified according to their score into four categories as following: 0–20: little to no stress, 21–40: mild to moderate stress, 41–60: moderate to severe stress, 61–80: severe stress.17
The second phase included gathering of the patients’ most recent biochemical and clinical data by the researchers through the patients’ electronic files using the medical record numbers which were provided by the caregivers upon filling the questionnaire.
After gathering the data, they were entered and coded using Microsoft Excel and then exported and analysed using the Statistical Package for the Social Sciences (SPSS) version 20 IBM (Armonk, New York, United States). At-test was used for continuous variables comparison and Chi-square test was used for assessment of categorical variables relationships.
Results
A total of 501 patients with T2D and their caregivers were included in the study (Table 1). The patients’ mean age was 64.4+12.0 years, female predominant with longstanding T2D, with an average BMI in the obesity range. Metformin was the most prescribed T2D medication followed by glargine insulin and sulfonylurea. Statins were the most prescribed cardiovascular medications followed by ACE inhibitors/ARB blockers and aspirin. The mean fasting glucose reading and HbA1c level were in the uncontrolled range while the mean fasting lipid profiles were at goal. The mean serum creatinine and urine microalbuminuria were normal.
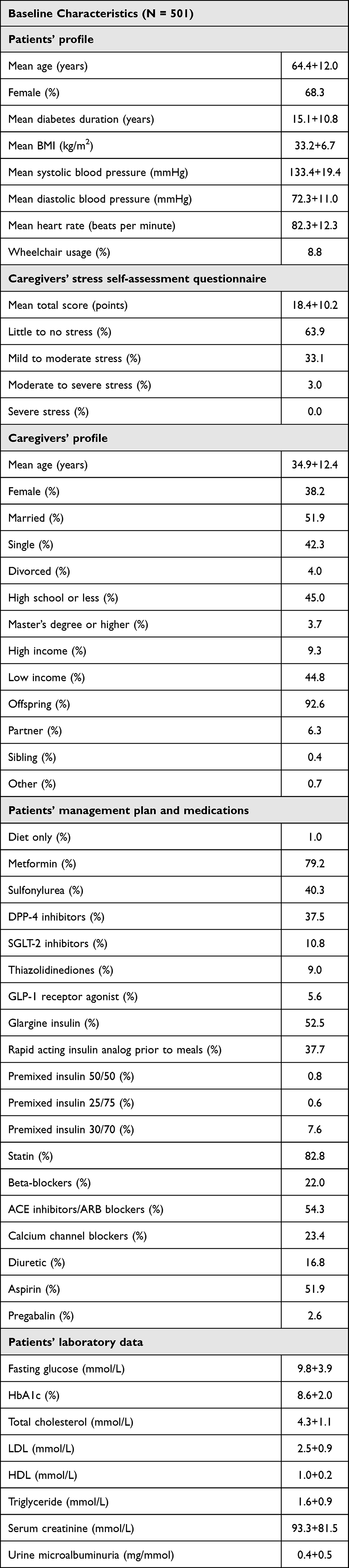 |
Table 1 Baseline Characteristics of the Whole Cohort |
The caregivers’ mean age was 34.9+12.4 years, male predominant, half of them were married, and around 45% of them report low level of education and income. Majority of the caregivers were patients’ offspring, and they report little to no stress.
Altogether 63.9% of the caregivers report little to no stress while the rest have mild/moderate and moderate/severe stress, but none have severe stress (Table 2). Compared with caregivers with mild/moderate stress and moderate/severe stress, caregivers with little to no stress were more likely to be younger in age (P <0.001), male (P = 0.464), single (P = 0.035), have Bachelor degree (P = 0.504), patient’s offspring (P = 0.490), caring for T2D patients with younger age (P = 0.058), shorter T2D duration (P = 0.074), patients who were less likely to use a wheelchair (P = 0.008), patients who were less likely to be prescribed a complex insulin regimen (P >0.05), patients with better glycemic control parameters (P >0.05), and patients with higher HDL level (P = 0.037).
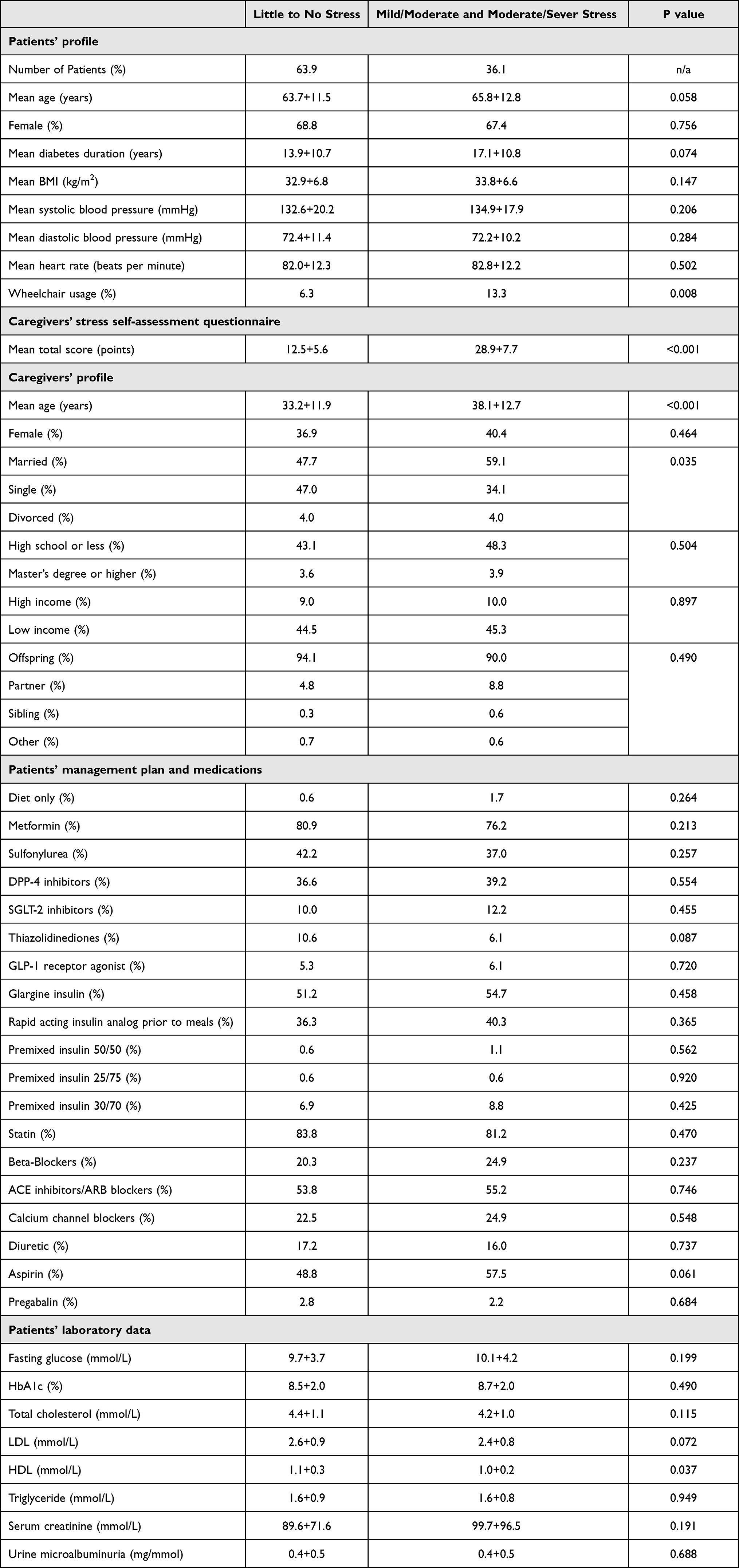 |
Table 2 Baseline Characteristics Based on the Caregiver’s Stress Self-Assessment Questionnaire Score |
No significant correlations were found between the caregiver’s level of stress and the patient’s HbA1c level when we evaluated the mean HbA1c level across each of the caregiver’s stress categories separately (Figure 1). While a non-significant positive correlation noted between the caregiver’s age and caregiver’s stress categories (Figure 2).
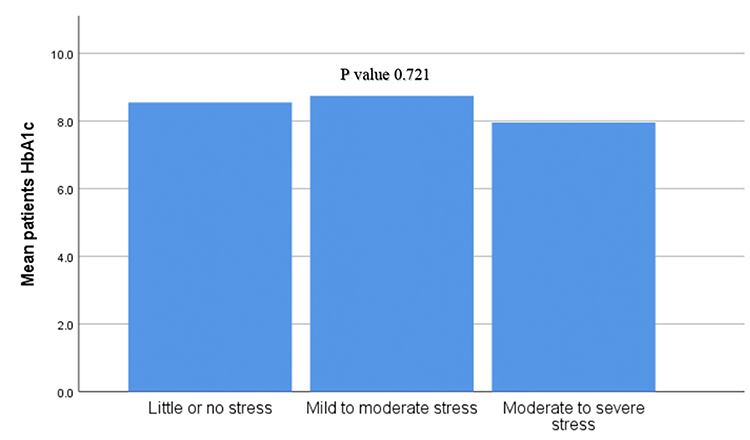 |
Figure 1 Mean patient’s HbA1c level according to the degree of the caregiver’s stress |
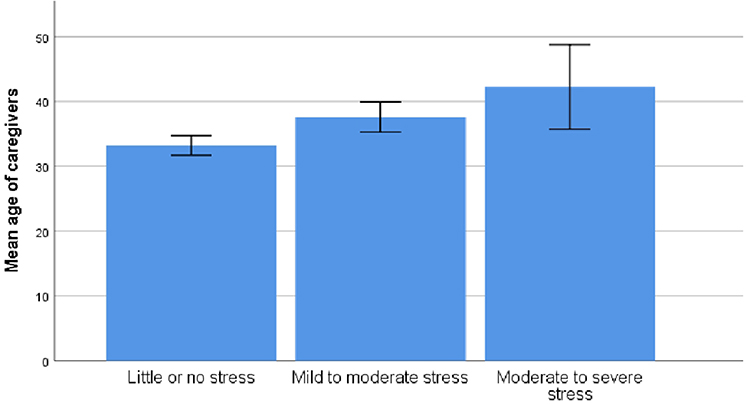 |
Figure 2 Mean age of the caregivers and the degree of the caregivers’ stress. |
Adjusting for the caregiver gender, caregiver education, caregiver marital status, caregiver monthly income, caregiver relation to the patient, patient age, and patient gender showed significant positive partial correlation between total caregiver’s stress score and the caregiver’s age (r = 0.170, P = 0.001). Also, adjusting for caregiver age, caregiver gender, caregiver education, caregiver marital status, caregiver monthly income, caregiver relation to the patient, patient age, patient gender, duration of diabetes, and patient BMI showed non-significant positive partial correlation between the total caregiver’s stress score and both patient’s fasting glucose reading (r = 0.073, P = 0.226) and patient’s HbA1c level (r = 0.103, P = 0.143).
Discussion
A recent study showed that DM may affect a caregiver’s personal and social life.18 Our study showed that 36.1% of the caregivers report mild/moderate and moderate/severe stress. A recent study also showed that only 18.4% of T2D patients’ caregivers report high level of strain.19 The observed difference likely related to the screening tool difference along with the caregiver age in our study. Another study showed that 42% of the caregivers had little to no stress and the difference observed may be related to the caregiver’s relation to patients as 92.6% of our study caregivers were patient’s offspring compared with 40%.20
A recent study showed that caregiver’s educational level inversely correlated with the caring burden level.21 Our study showed that half of the caregivers have a college degree and report a low income. This is similar to the findings of another recent study.22 Also, most of our study caregivers were younger males and this is opposite to what been reported in a recent review article which likely reflects a cultural difference between the countries.23 Also, female caregivers were non-significantly more likely to report mild/moderate/severe stress in our study and this concurred with other study findings.24,25
Our study showed non-significant higher HbA1c and fasting glucose along with higher percentage of high school degree or less in the mild/moderate/severe stress groups which concurs with a recent study finding that showed lower medications adherence along with higher HbA1c in the stress and low education groups.26,27 Despite being on a complex regimen, caregivers with mild/moderate/severe stress had non-significant worse glycemic control for the T2D patient and that may possibly be due to ineffective training and teaching for the caregivers as shown in a recent study.28
Our study showed that caregivers who care for T2D patients who use a wheelchair are more likely to report mild/moderate/severe stress. A recent study showed patients’ wheelchair usage increases the psychological burden for the caregivers.29 Also, we showed a non-significant positive correlation between the caregivers’ age and caregivers’ stress which was also reported in a recent study.30
Our study strength includes novelty and a lack of local data in this topic along with the comprehensive medications and biochemical data. Our weakness includes single center data collection, lack of the comorbid conditions data, dependency level, data about the caregiving hours and number of caregivers.
Conclusion
Most of the T2D patients’ caregivers report little to no stress and those were significantly more likely to be male, single, and younger in age compared with those with mild/moderate and moderate/severe stress. Adjusting for possible confounders showed a significant positive correlation between caregiver’s stress score and the caregiver’s age. Future studies are needed to assess other caregivers’ parameters and their relation to metabolic control of T2D patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project was supported by the Taif University Research Support Project Number (TURSP-2020/37), Taif University, Taif, Saudi Arabia.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. International Diabetes Federation. IDF Diabetes Atlas.
2. Al-Nozha MM, Al-Maatouq MA, Al-Mazrou YY, Al-Harthi SS. Diabetes mellitus in Saudi Arabia. Saudi Med J. 2004;25(11):45.
3. Alzaid A. Diabetes: a tale of two cultures. Br J Diabetes Vascular Dis. 2012;12(2):343.
4. Al-Rubeaan K, Al-Manaa H, Khoja T, et al. The Saudi abnormal glucose metabolism and diabetes impact study (Saudi-DM). Ann Saudi Med. 2014;34(6):465–475.
5. Abdulaziz Al Dawish M. Diabetes mellitus in Saudi Arabia: a review of the recent literature. Curr Diabetes Rev. 2016;12(4):359–368.
6. Trief PM, Ploutz-Snyder R, Britton KD, Weinstock RS. The relationship between marital quality and adherence to the diabetes care regimen. Ann Behavioral Med. 2004;27(3):148–154.
7. Trief PM, Grant W, Elbert K, Weinstock RS. Family environment, glycemic control, and the psychosocial adaptation of adults with diabetes. Diabetes Care. 1998;21(2):241–245.
8. World Health Organization. Innovative Care for Chronic Conditions: Building Blocks for Action: Global Report. 2002. Geneva: World Health Organization; 2015. https://www.who.int/chp/knowledge/publications/icccglobalreport.pdf.
9. Lim JW, Zebrack B. Caring for family members with chronic physical illness: a critical review of caregiver literature. Health Qual Life Outcomes. 2004;2(1):1–9.
10. Awadalla AW, Ohaeri JU, Al-Awadi SA, Tawfiq AM. Diabetes mellitus patients’ family caregivers’ subjective quality of life. J Natl Med Assoc. 2006;98(5):727.
11. Awadalla AW, Ohaeri JU, Tawfiq AM, Al-Awadi SA. Subjective quality of life of outpatients with diabetes: comparison with family caregivers’ impressions and control group. J Natl Med Assoc. 2006;98(5):737.
12. Brod M. Pilot study-quality of life issues in patients with diabetes and lower extremity ulcers: patients and care givers. Quality Life Res. 1998;7(4):365–372.
13. Anaforoğlu İ, Ramazanoğulları İ, Algün E, Kutanis R. Depression, anxiety, and quality of life of family caregivers of patients with type 2 diabetes. Med Principles Practice. 2012;21(4):360–365.
14. Nabuurs-Franssen MH, Huijberts MS, Kruseman AN, Willems J, Schaper NC. Health-related quality of life of diabetic foot ulcer patients and their caregivers. Diabetologia. 2005;48(9):1906–1910.
15. Lee VY, Seah WY, Kang AW, Khoo EY, Mooppil N, Griva K. Managing multiple chronic conditions in Singapore–exploring the perspectives and experiences of family caregivers of patients with diabetes and end stage renal disease on haemodialysis. Psychol Health. 2016;31(10):1220–1236.
16. Schröder JP. Wege aus dem Burnout: möglichkeiten der nachhaltigen Veränderung. Cornelsen. 2006;1:32.
17. Yap P. Validity and reliability of the Zarit Burden Interview in assessing caregiving burden. Ann Acad Med Singapore. 2010;39:758–763.
18. Li J, Cesari M, Del Campo N, et al. Impact of diabetes on caregiver stress in patients with Alzheimer’s disease: data from the ICTUS study. Int Psychogeriatrics. 2018;30(8):1109–1117.
19. King A, Ringel JB, Safford MM, et al. Association Between Caregiver Strain and Self-Care Among Caregivers with Diabetes. JAMA network open. 2021;4(2):e2036676.
20. Van Loon AM. The Australian concept of Faith Community. Parish Nursing. 1999;11:287–295.
21. Mirhosseini S, Bazghaleh M, Basirinezhad MH, Abbasi A, Ebrahimi H. Health-related quality of life and caregiver’s burden in patients with chronic diseases: a cross-sectional study. Family Med Primary Care Rev. 2021;23(1):29–35.
22. Kristaningrum ND, Ramadhani DA, Yati Sri Hayati S. Correlation between the burden of family caregivers and health status of people with diabetes mellitus. J Public Health Res. 2021;10(2):343.
23. Sharma N, Chakrabarti S, Grover S. Gender differences in caregiving among family-caregivers of people with mental illnesses. World j Psychiatry. 2016;6(1):7.
24. Torimoto-Sasai Y, Igarashi A, Wada T, Ogata Y, Yamamoto-Mitani N. Female family caregivers face a higher risk of hypertension and lowered estimated glomerular filtration rates: a cross-sectional, comparative study. BMC Public Health. 2015;15(1):1.
25. Del-Pino-Casado R, Frias-Osuna A, Palomino-Moral PA, Ramon Martinez-Riera J. Gender differences regarding informal caregivers of older people. J Nurs Scholarsh. 2012;44(4):349–357.
26. Beck JK, Zhang Y, Shay CM, et al. Diabetes knowledge in young adults: associations with hemoglobin A1C. Families Sys Health. 2015;33(1):28.
27. Johnson MD, Anderson JR, Walker A, Wilcox A, Lewis VL, Robbins DC. Common dyadic coping is indirectly related to dietary and exercise adherence via patient and partner diabetes efficacy. J Family Psychol. 2013;27(5):722.
28. Ross SA, Tildesley HD, Ashkenas J. Barriers to effective insulin treatment: the persistence of poor glycemic control in type 2 diabetes. Curr Med Res Opin. 2011;27(sup3):13–20.
29. Rushton PW, Labbé D, Demers L, Miller WC, Mortenson WB, Kirby RL. Understanding the burden experienced by caregivers of older adults who use a powered wheelchair: a cross-sectional study. Gerontology and Geriatric Medicine. 2017;3:2333721417703736.
30. Shen S, Wan Y, Xie Y, Chen Z, Li F. Care Stress Experienced by Caregivers of Elderly Individuals with Disabilities and the Coping Strategies Utilized: a Survey Study in the City of Nanjing, China. J Fam Issues. 2019;40(10):1396–1414.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.