")
Back to Journals » Advances in Medical Education and Practice » Volume 12
Assessment of Student Perspectives on Improving Wellness in Medical School: Qualitative Results from a Cross-Sectional Survey of Medical Students in Florida
Authors Butcher MR, Thompson KM , Williams MK, Cooke BK, Merlo LJ
Received 10 June 2021
Accepted for publication 28 August 2021
Published 21 September 2021 Volume 2021:12 Pages 1067—1079
DOI https://doi.org/10.2147/AMEP.S323332
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Monica R Butcher, Kathryn M Thompson, Michelle K Williams, Brian K Cooke, Lisa J Merlo
University of Florida College of Medicine, Gainesville, FL, 32611, USA
Correspondence: Lisa J Merlo
University of Florida College of Medicine, PO Box 100256, 1149 Newell Dr, Gainesville, FL, 32611, USA
Tel +1 352 294 4900
Email [email protected]
Purpose: Helping medical students maintain wellbeing has become an important concern, as many medical students report a decline in their mental health during the course of their training. To improve students’ wellbeing, some schools have implemented wellness programs into their curricula. While there is growing research about the effectiveness of these programs, little is known about what medical students themselves desire to support their wellbeing. This study aimed to assess medical student perspectives regarding the most effective ways to promote wellness during medical school.
Participants and Methods: To address this gap in the literature, a survey was administered to medical students at the nine medical schools in the state of Florida. Participants included 864 medical students, whose anonymous responses were analyzed descriptively as well as qualitatively to determine major themes.
Results: Students provided novel suggestions and recommendations, including ideas for curricular additions and changes, cultural changes within schools, promoting positive behaviors and extracurricular activities, and providing resources for students.
Conclusion: Based on the participants’ responses, it is evident that wellness is an important issue to medical students and, given the variety of suggestions, schools should strongly consider what wellness changes to implement and whether participation in them should be mandatory. The results of this study will be a resource to medical schools and educators who are considering curricular changes to address medical student wellbeing.
Keywords: curriculum, health promotion, mental health, medical education, medical student wellbeing
A Letter to the Editor has been published for this article.
A Response to Letter has been published for this article.
Introduction
An important aspect of medical education is supporting the wellbeing of the student body, a subject that has been emphasized more in recent years. Despite increased institutional efforts to promote wellness, more than 80% of medical students report some form of psychological distress.1 In fact, rates of psychological distress2 including depression,3,4 burnout,4 anxiety,5 and a low mental quality of life1,3,6,7 are higher in medical students than same-age peers. Studies have shown that approximately one half of all medical students screen positive for depressive symptoms3,4,6 and about one in four meet a clinical diagnosis for depression.5,8–10 Furthermore, the prevalence of suicidal ideation in medical school is 11.1%.11 Burnout, a state characterized by a triad of depersonalization, lack of personal accomplishment, and emotional exhaustion, affects approximately half of medical students.3,4,6,7
Yet, studies have shown that newly-matriculating medical students have similar or better emotional functioning compared to same-age college graduates in other fields.12,13 This suggests that medical education is, in part, responsible for poor medical student mental health. In fact, studies have shown that psychological distress increases during medical school, with the peak year differing based on the type of distress studied (ie, depressive symptoms versus self-reported stress levels).6,13–15 Female medical students are at increased risk for worsened mental and physical health compared to male peers, with several studies indicating worse emotional health2,5,6,13,14,16,17 and physical health18,19 profiles among women. In addition, although students generally enter medical school with a coping reservoir, stressors related to academic performance and the time demands of medical school may deplete this internal resource.20
Although medical student distress is widespread and relatively common, many students still do not seek mental health care. In fact, in a study of depressed medical students, only 22% of these students were receiving mental health counseling services.8 Major barriers for seeking care are time,8,21 perceived lack of confidentiality,8,21 and overcoming stigma.8,21,22 Vankar et al23 found that 29% of the medical students from their sample in India reported they would feel less intelligent if they sought help for depression, 28% believed it would be risky to admit depression to a counselor or mentor, and 35% feared that other students would gossip if the others knew they were depressed. As a result, students may prefer access to less stigmatized resources to support their mental health and wellbeing.
Previous studies have demonstrated preliminary support for integrating comprehensive mental health programming (ie, a multipronged approach offering prevention, support, and clinical services) within the medical school21 or implementing a “wellness program” to support student health and wellbeing.24 Such initiatives may directly or indirectly impact student health and wellness, as one study showed that student perception of whether their school had a system to help students cope with stress was independently associated with decreased suicidal ideation, student perceived stress, and number of poor mental health days.14 In addition, various interventions aimed at managing student stress have been studied,25,26 including the implementation of a pass/fail grading system,7,10,27 mindfulness training,25,28–32 and curricular changes.10,33 However, these interventions vary significantly in terms of the amount of time and resources required, and there is limited information available regarding what resources, supports, and programs the students themselves would prefer. This study aimed to assess medical student perspectives regarding the most effective ways to promote wellness during medical school. To our knowledge, this is the first multicenter study using qualitative research strategies to assess student desires regarding medical school policies and programs to improve student wellbeing.
Materials and Methods
Procedure
All study procedures were in accordance with the Declaration of Helsinki regarding research ethics. Data for this study were drawn from the results of a cross-sectional anonymous survey investigating medical student wellness in the State of Florida that was administered in spring of 2014. The research was supported by the Florida Council of Medical School Deans and received primary approval from the University of Florida (UF) Institutional Review Board. Secondary approval was granted by the Lake Erie College of Osteopathic Medicine (LECOM) IRB. Ethical approval was waived by the IRBs at Florida International University (FIU), University of Miami (UM), Nova Southeastern University (NSU), University of South Florida (USF), University of Central Florida (UCF), Florida State University (FSU), and Florida Atlantic University (FAU). The study included all public (FAU, FIU, FSU, UCF, UF, USF), and private (LECOM, NSU, UM), new (FAU: 2011, FIU: 2006, FSU: 2000, LECOM: 2004, UCF: 2006, and established (NSU: 1981, UF: 1956, UM: 1952, USF: 1971), university-based (UF, UM, USF) and community-based (FAU, FIU, FSU, LECOM, NSU), allopathic (FAU, FIU, FSU, UCF, UF, UM, USF) and osteopathic (LECOM, NSU) medical schools within the state. According to school report and/or publicly available information, at the time of the study, the schools varied in size and diversity of the student body (ie, FSU = 481 students, 46% female, 17% underrepresented minority [URM]; LECOM = 744 students, 42% female, 10% URM; NSU = 984 students, 39% female, 17% URM; UF = 537 students, 44% female, 25% URM; USF = 625 students, 45% female, 11% URM). Some schools allowed students to select multiple categories when reporting demographics and did not provide %URM statistics (ie, FAU = 188 students, 54% female, 67% White, 5% Black/African American, 13% Asian, 15% Hispanic/Latino, 5% other; FIU = 373 students, 45% female, 41% White, 8% Black/African American, 18% Asian, 32% Hispanic/Latino, 6% other; UCF = 359 students, 50% female, 57% White, 5% Black/African American, 24% Asian, 13% Hispanic/Latino, 7% other; UM = 809 students, 49% female, 54% White, 6% Black/African American, 23% Asian, 13% Hispanic/Latino, 7% other).
All currently enrolled medical students from each school were eligible to participate. They were invited by student leaders to complete an anonymous Online Survey administered through Survey Monkey. Invitations were sent via email and/or in-class announcements. Students were told that they could complete the survey on their own time and that the survey would take about 30 minutes to complete. In order to ensure anonymity, the requirement for written informed consent was waived in favor of including a research description (which contained the primary elements of a consent document) on the first page of the Online Survey. Students were required to confirm their understanding of the research study, the anonymous nature of their responses, and their desire to participate before advancing to the actual survey items. Anonymity was further preserved by requesting that students not name their schools or provide any other identifiers in free response items. They received no compensation for participation.
Measure
A 98-item research questionnaire was developed for the parent study in consultation with key stakeholders (eg, medical school deans, administrators of the state physician health program, and medical students) who provided feedback on early drafts to revise content and ensure clarity. It included both fixed choice and free response questions that covered the following: physical and psychological health (current and prior to medical school), level of stress, level of competitiveness in the school, bullying, substance use, spirituality, utilization of resources, coping strategies, and suggestions for curricular improvement. Some findings have been previously reported.34 The current study explores student responses to two free response questions: 1)“What could medical schools do to improve medical student health and wellness?” and 2)“If you were to design a student wellness program for your medical school, what would it include and not include?”
Participants
Participants in the parent study were 1139 medical students representing all 9 medical schools in Florida. At the time of the study, the total number of medical students matriculating in the State of Florida was ~5100. However, because students were invited to participate by peer leaders at their institutions, we were unable to verify what percentage of those students actually received invitations to participate. The current research includes data from the 864 students (76% of the total sample of survey respondents) who completed the survey in its entirety, including responding to the two free response items assessing student recommendations to improve wellness. As seen in Table 1, this sample was 57% female. A plurality of the participants were first year students (34%), and they reported a variety of living situations. No other demographic variables were assessed in order to protect the anonymity of the students and their medical schools.
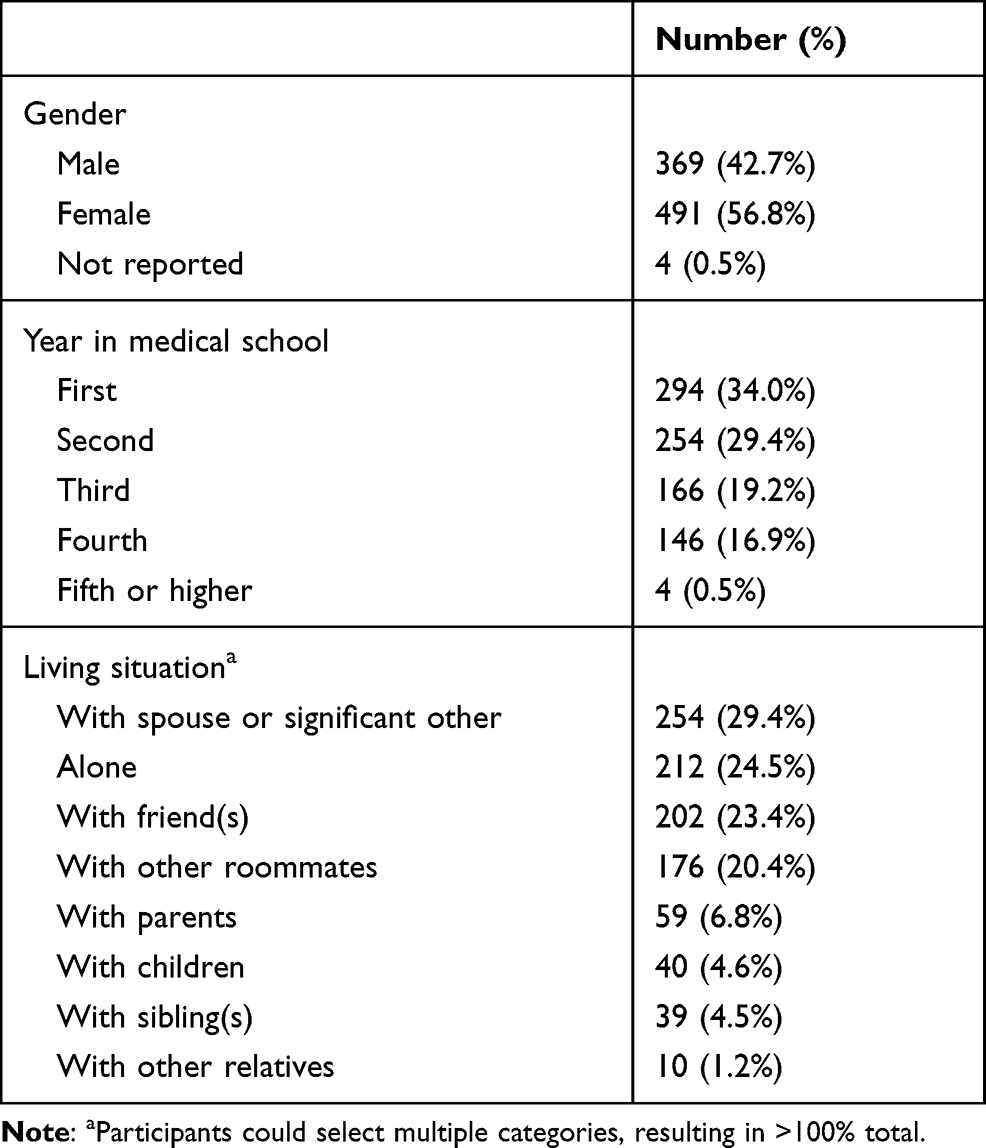 |
Table 1 Characteristics of Study Participants |
Data Analysis
Descriptive statistics were calculated using SPSS v.20. Following procedures for thematic analysis outlined by Braun and Clarke,35 qualitative data were reviewed by the first and final author independently, using an inductive approach to generate codes at the semantic level. Agreement on the final list of codes was reached through discussion. The second and final author jointly coded approximately 10% of responses to achieve inter-rater reliability. Then, the second author coded the remaining items. In the event of uncertainty, the code was assigned in consultation with the final author. Codes were sorted into themes jointly by the second and final author. Prevalence of each theme (and subtheme) were determined by counting the number of respondents who mentioned the theme in their response(s). Representative quotations for each theme were selected by the first, third, and final author in order to enrich the description of each theme.
Results
Regarding ways to improve medical student health and wellness, 128 students (14.8% of respondents) indicated that they had no suggestions or failed to provide a response. However, 736 students (85.2% of respondents) provided suggestions regarding changes and/or additions to their existing curricula, and/or resources that they believed would better support students. Results are listed by theme, with representative quotations for each. Table 2 lists the number of comments from students for each theme and underlying topic.
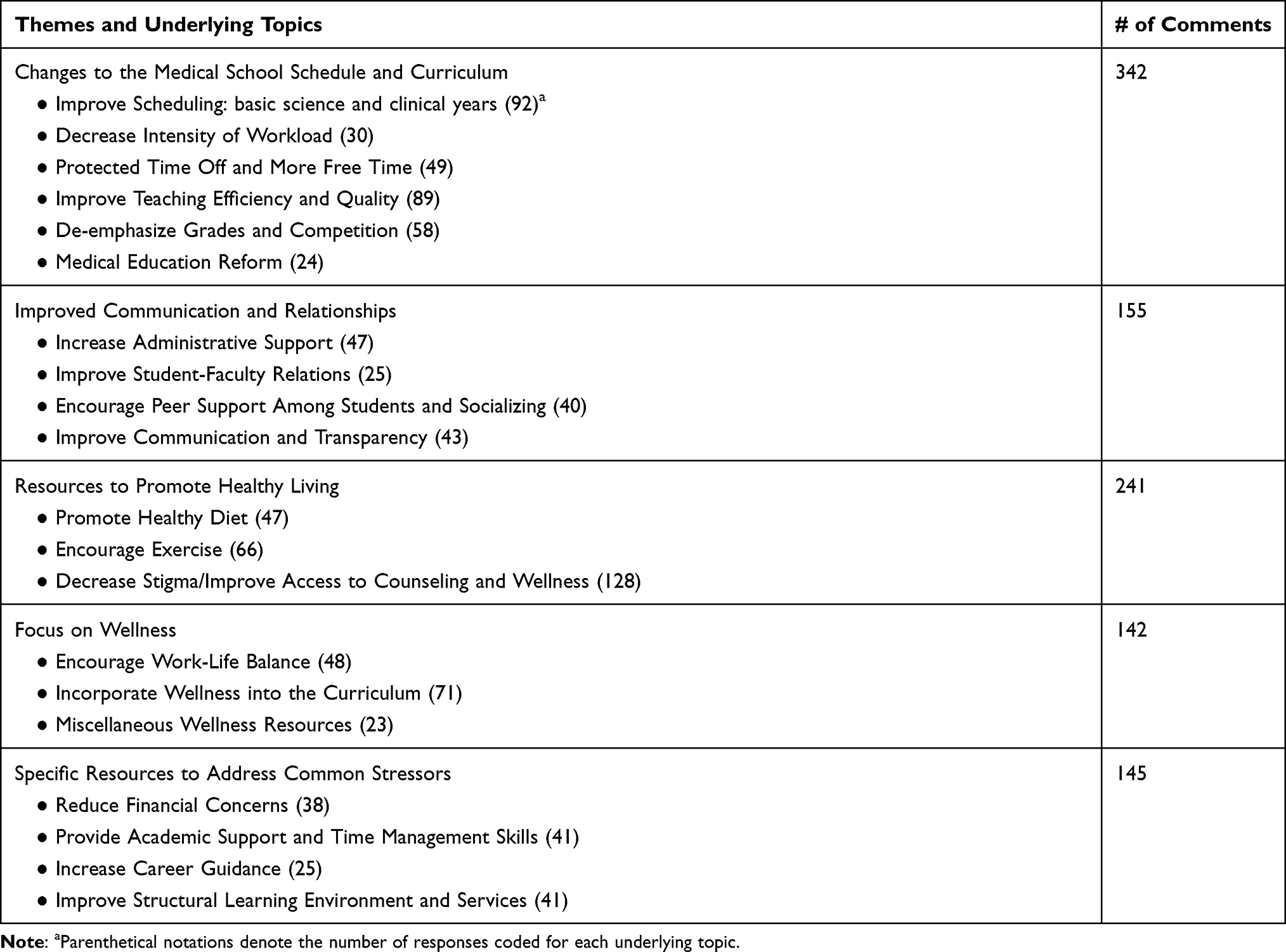 |
Table 2 Number of Comments for Each Theme Related to How Medical Schools Could Improve Medical Student Health and Wellness |
Changes to the Medical School Schedule and Curriculum
Improve Scheduling (in Basic Science and Clinical Years)
Students suggested changes to improve the scheduling of classes by increasing flexibility and consistency. Specifically, students in their basic science years recommended minimizing mandatory activities (eg, “Make all classes optional … Optional classes definitely allow students to use their time more effectively for more important things”) or limiting the hours during which mandatory activities would be scheduled (eg, “[Schedule] fewer hours of lecture in a day (such as going from 8–12 or 1) or give us an extra day off in a week (like Wed), so we have more time to study”). Some even recommended having scheduled study time (eg, “In my experience, having independent study time has been extremely beneficial in balancing academic and lifestyle demands”) and flexibility built in (eg, “[Schools can help by] allowing students to have more control over their schedules”). Further, students recommended consistency of scheduling as a high priority (eg, “Don’t make the stress worse with unpredictable scheduling”). For students in their clinical years, frustrations with scheduling pertained to extensive work hours, with many students believing that schools should work to shorten the time students spend on the wards (eg, “Let medical students go home at a decent hour during their 3rd year of medical school”), including implementation of a work hour limitation eg,
[Enforce] duty hour limitations for students. Several times, medical students in third year were working for longer hours than interns, with no regard to the former’s duty hour limitations.
Considering the amount of time spent on the wards, students believed that there was not adequate time to study for examinations (eg, “Give more study time in third year. As in built into your schedule rather than the two hours between getting home and sleeping”).
Decrease Intensity of Workload
Medical students noted that the variable intensity of their programs also detracted from wellbeing. Some students suggested that one way to balance the workload was to make schooling longer with a “slower pace of class and/or a longer academic year.” Other students suggested maintaining the length of time in school but balancing the workload better within that time frame to eliminate the stresses of having multiple examinations in one day eg,
Do a better job of scheduling when tests are … we tend [to] have tests pile up upon each other so that we have to pick our battles and decide to study for 1 test and not the other,
or alternating between extremes in terms of required work. As one student suggested,
Consider workload in relation to students’ ability to balance a healthy lifestyle in the creation of the curriculum. Some modules are a joke and the students have way too much free time, on the flip side doing anatomy in 8 weeks makes it basically impossible to succeed in the course and maintain a healthy lifestyle.
Protected Time off and More Free Time
Students further requested that schools provide them with occasional breaks from academic and/or clinical responsibilities (eg, “Implement legitimate breaks every few weeks– weekends off, break days between blocks”). Those in the basic science years specifically requested days off after large examinations to recuperate [eg, “A few more 3-day weekends for students to decompress (AFTER exams, not before)”]. However, students suggested that having any free days would be a welcome change allowing them occasional opportunities to decompress (eg, “Schedule free days … random days where we can just have the whole day to not worry about school”), engage in self-care (eg, “Build in more opportunities for personal health days so that students may visit physicians, dentists, and mental health professionals”), and manage personal needs eg,
Offer more days, especially during third year, for students to catch up on reading and perform necessary tasks for their everyday life that they don’t have the time to do.
Improve Teaching Efficiency and Quality
In order to address some of the above concerns, students suggested streamlining the curriculum to remove material or experiences they viewed as unnecessary to their education eg,
The time taken to give us extra information about topics that are extraneous to our medical education should be used for our own personal time to catch up on work, stay healthy, do research … something beneficial.
In particular, students perceived little benefit from completing required assignments eg,
Make sure that the only homework is studying. Some medical schools assign written homework assignments that come across as busy work and I feel that they come in the way of my adequate studying.
Regarding content, students requested that the curriculum be more focused on development of clinical proficiency eg,
Take some of the pointless details out of the curriculum. There are tons of things being taught to us that have no clinical relevance, but have been tested on the USMLE (so we have to learn them)
or preparation for the Step exams used in the United States to grant medical licensure (eg, “Start teaching us what they’re supposed to be teaching us to do well on board exams”). Further, some students reported that their professors created a poor learning environment due to lack of pedagogical skills (eg, “Medical schools could put much more emphasis on good teaching skills, rather than using experts in their fields”).
De-Emphasize Grades and Competition
Students requested removal of academic rankings and graded systems from medical education (eg, “Get rid of ranking systems which force competition between peers”) in order to reduce within-class rivalry (eg, “Foster a non-competitive atmosphere among students”), and introduce more collaborative learning opportunities (eg, “Encourage collaboration and not so much competition”). Students predicted that making the curriculum pass/fail would reduce their stress levels and complement the learning process (eg, “Moving to a pass/fail system would take the edge off the stress and would allow students to focus more on learning the material than just getting the grade”).
Medical Education Reform
Some students felt that improving medical student health and wellness could best be achieved by completely overhauling the medical education system eg,
I think it’s more of a medical education issue as opposed to medical school improvements. I think the whole system really needs a revision and serious consideration.
For example, some believed that the current structure overemphasizes high stakes exams (eg, “Less emphasis on Step 1 scores for residency admission”), and creates unnecessary stress due to the relatively low number of available residency positions (eg, “Increase the amount of residency positions available for US graduates”). Some students suggested incorporating more of the medical school curriculum during undergraduate training (eg, “We could learn a lot more in undergrad that is specific for medicine so that we have less to learn in medical school itself”).
Improved Communication and Relationships
More Supportive Administration
Students expressed some frustration with medical school administrators, recommending against “threaten[ing] your students with the consequences of failure … I wish they were on our side to help, not to punish.” Students commented that the environment of medical school could be improved upon to be more supportive and friendlier (eg, “[Schools could work to] produce an environment of support that fosters the student, not one that further breaks them down”). They suggested that administrators should “accommodate their students as much as possible. This would depend on the specific school and the concerns students have there.” Additionally, they requested that administrators “remember that we are adults and are choosing to be here - quit treating us like children who you think you have to babysit.” Students also noted that the rigidity of rules could be decreased eg,
[The administration] could show more flexibility and be more willing to work with students with scheduling and career planning instead of enforcing arbitrarily created rules.
Finally, students requested that schools be as organized as possible and work to lessen logistical problems (eg, “Do their best to minimize the many ‘small’ administrative, technology, and scheduling errors and frustrations. We have enough to deal with already”).
Improve Student–Faculty Relations
Strain in the student–faculty relationship was a concern to some medical students who wanted their schools to “encourage a supportive environment between classmates and faculty.” They suggested that medical schools could work to discourage medical student mistreatment and “ensure residents and faculty are invested and interested in teaching medical students.” Students commented that faculty would benefit students by having “more reasonable expectations for [student] workload” and by “understand[ing] time constraints.”
Encourage Peer Support and Socializing Among Students
Medical students emphasized the importance of peer support during medical school, stating that it was imperative to improve class community eg,
Class unity is an important factor in stress levels … knowing that there are a hundred others in your same shoes, or a hundred others that would be there for you if you needed it is important to the health and wellness of medical students.
Participants proposed that schools could achieve this goal by actively working to limit negative behaviors (eg, “Teach students to respect and be cordial to one another … [Have students] avoid trying to bully, humiliate and hurt each other”), as well as by providing students with “more structured times to share their struggles and experiences with other students.” Specifically, students recommended implementing “better medical student support groups (without faculty involvement).” Others suggested that schools could facilitate student interaction outside of the classroom (eg, “[Schools could] provide the students with more opportunities to socialize”), perhaps by providing resources on campus (eg, “ping pong room/dedicated rec room for medical students,” a “free arts and crafts center, [or] offer other fun activities at low or no cost that don’t involve studying”).
Improve Communication and Transparency
Communication between all persons involved in medical education could be improved in order to enhance medical student health and wellness (eg, “Improve communication among staff members and between staff and students”). Students were concerned about the administration and faculty listening to their needs. These students suggested that the administration and faculty “be open to student feedback and be willing to make changes based upon that feedback if it is appropriate.” Students also expressed a desire for medical schools to communicate educational goals more explicitly. It was recommended that schools provide “clear, concise expectations with clear and concise material given to reach those expectations” in order to reduce student stress. Students reported feeling uncertain about their performance and suggested that schools would show “transparency in [the] educational and evaluation process[es].” One student commented, “I believe that a great deal of stress comes from the unknown.”
Resources to Promote Healthy Living
Promote Healthy Diet
Medical students requested that schools assist students in accessing more nutritious foods in a number of ways, including providing education services (eg, “[Schools could] include programs about nutrition and making healthy, non- time-consuming meals”) and offering healthy eating options on campus eg,
[Provide] places to eat cheap, healthy foods … I have gone 10 hours without eating because I was too tired to prepare food in the morning, and couldn’t eat an expensive, unappetizing, unhealthy meal when I was trying to get through enough material before I left campus.
Students further recommended that schools make the healthy food available at more times of the day [eg, “Better access to affordable and healthy food, at better hours (eg, while studying)”] and consider nutrition when offering food to students [eg, “Provide healthy meals for all free-food events (student organizations, too)”].
Encourage Exercise
Students suggested that schools could improve health and wellness by encouraging physical fitness with accessible and inexpensive exercise options. Specific suggestions included providing access to gym facilities (eg, “Either have a gym on campus, or offer free gym memberships at a nearby gym”), fitness classes (eg, “Offer group exercise/yoga specifically for medical students”), or other physical activities (eg, “Implement easily accessible medical student-only exercise activities”). Some even suggested that schools could promote physical health by requiring students to have access to exercise facilities (eg, “Have mandatory gym sign ups”).
Decrease Stigma/Improve Access to Counseling and Wellness
Students requested that schools improve access to mental health counseling that was accessible, free, and confidential (eg, “School should provide FREE mental health advisors who ensure privacy”). While many schools already offer counseling resources, students described limited access due to counselor availability (eg, “Provide more access to therapy. Our school’s therapist is booked so tight”) and practical barriers (eg, “scheduling and cost are the largest barriers to receiving these services”). In addition, students felt that schools could more effectively advertise the health and wellness services available (eg, “Remind us repeatedly about the wellness services available and how to access them”). Other suggestions included requiring all students to attend sessions with a counselor as a preventative measure (eg, “Enforce regular one-on-one meetings with wellness counselors so that students who are struggling are caught BEFORE they go under rather than after”) and to decrease concerns about stigma (eg, “Provide an environment where students feel comfortable talking to someone about mental health issues” and “[Have] more conversation and education to destigmatize mental health”).
Focus on Wellness
Encourage Work-Life Balance
Students suggested that medical schools foster an atmosphere that supports and encourages wellness (eg, “Just advertising the importance of health and wellness on a regular basis that also includes staff and faculty would be good”). Suggestions included “provid[ing] seminars and lunch meetings devoted to health and wellness” and “actively encourag[ing] and facilitat[ing] participation by all students in health and wellness improvement.” Students recommended offering wellness promotion activities (eg, “Hold regular programming consisting of activities to help students relax and unwind”), such as “meditation or yoga classes on campus, [which would] make it easier to have access to stress reduction techniques.” Students further suggested that schools could
be more encouraging and considerate of the fact that medical students are also people. We have lives and interests outside of medicine and that should always be remembered.
In addition, considering the impact of medical school on relationships, students suggested education that would “Prepare students for managing friendships and romantic partnerships during medical school.” In general, students seemed to feel that balance could be more easily achieved if schools incorporated extracurricular activities into the curriculum by “creating avenues to involve medical student extracurricular passions within curricula.” Two students even recommended that schools enforce “mandatory free time.”
Incorporate Wellness into the Curriculum
Many students suggested introducing mandatory wellness programs (eg, “Teach meditation and stress-relieving tools without having [students] individually seek education in these areas”). Specifically, they suggested that schools could “provide a 1 hour course on de-stressing, focusing on actual techniques we would use or allowing us to use that time to just do leisurely activities.” Others recommended “wellness-based small group discussion sessions built into the med school curriculum,” and “mandatory short courses that cover medical student health and awareness topics.” Many students recommended that schools “incorporate relaxing activities into the class schedule,” explaining that, “Instead of just having resources available, we could have those resources brought to us, and built into our schedule.” Finally, students recommended that instead of having time blocked out to use wellness resources, schools could initiate mandatory wellness check-ups (eg, “Require regular meetings with advisors that asked about the student’s health and wellbeing”).
Miscellaneous Wellness Resources
Medical students recommended that schools offer more miscellaneous wellness resources such as, “more relaxation services like massage and aromatherapy” and to “bring in pets for therapy days at the school.” In addition, some students expressed their desires for pet walking and care services (especially during high-stress periods like exam weeks), couples therapy, more activities involving significant others, and free dietician services.
Specific Resources to Address Common Stressors
Reduce Financial Concerns
Students suggested that efforts to reduce financial concerns would promote increased wellness. Specifically, students expressed interest in having schools help them “reduce the amount of debt we are accruing. I am not talking about cheaper loans; I am talking about lowering the cost” in addition to requesting lower out-of-pocket costs (eg, “Provide more scholarships, streamline education to make the tuition more reasonable”). Many students requested access to financial advising (eg, “Give us better counseling on our finances” and “Include classes and lunch discussions on time management and financial burden”).
Provide Academic Support and Time Management Skills
Respondents requested that additional academic support services be made available to all students, not only those struggling with school. Specifically, they suggested that medical schools “teach time management skills before classes” and provide “more help with studying (strategies, study groups, etc.).” Students also reported feeling they “would benefit from learning styles workshops, which would help them study more effectively and efficiently, freeing up more time for relaxation and exercise.” Finally, students mentioned that schools could lend more support for board studying and often suggested “USMLE Step 1 prep courses.”
Increase Career Guidance
Career planning was also noted as an area schools could improve upon. Medical schools could provide students with “more time scheduled into the curriculum for career counseling, career development.” Many students called for mentorship relationships to be established among medical students and faculty (eg, “a stronger physician/faculty mentor and career advising program” and “Provide better guidance, mentorships, and planning for students”). Additionally, students felt schools could assist specialty decision-making by “giving med students more time to experience different specialties so it is less stressful trying to pick your future career.”
Improve Structural Learning Environment and Services
Students also commented on their desire for comfortable learning/relaxation spaces (eg, “Students need tranquil environments with natural light, free or inexpensive coffee, and healthy free food” and “Offer massage chairs, nap rooms, leisure areas that are on the medical school campus”). One frequent response was the desire to have a gym added to the medical school building or one within walking distance (eg, “Put a small med student gym in one of the buildings” and “provide a dedicated gym space with machines and locker room shower that would allow us to conveniently workout and cleanup”). In addition to improvements to the structural learning environment, students recommended adding services, such as “hir[ing] instructors for yoga sessions/exercise classes/etc.”
Suggestions for Designing a Student Wellness Program
On the item assessing student perspectives on what a medical school wellness program should entail, 324 students (28.4% of the total sample) responded. Of these, 59 students (18.2% of respondents) indicated that they had no suggestions and 265 students (81.8% of respondents) offered ideas for a student wellness program. Students responded with the type of content they would like to see implemented into a wellness program and/or the modality by which they would like to see the wellness program carried out, and responses generally reflected the same themes as the previous question. Table 3 lists the number of comments from students for each content theme and modality theme.
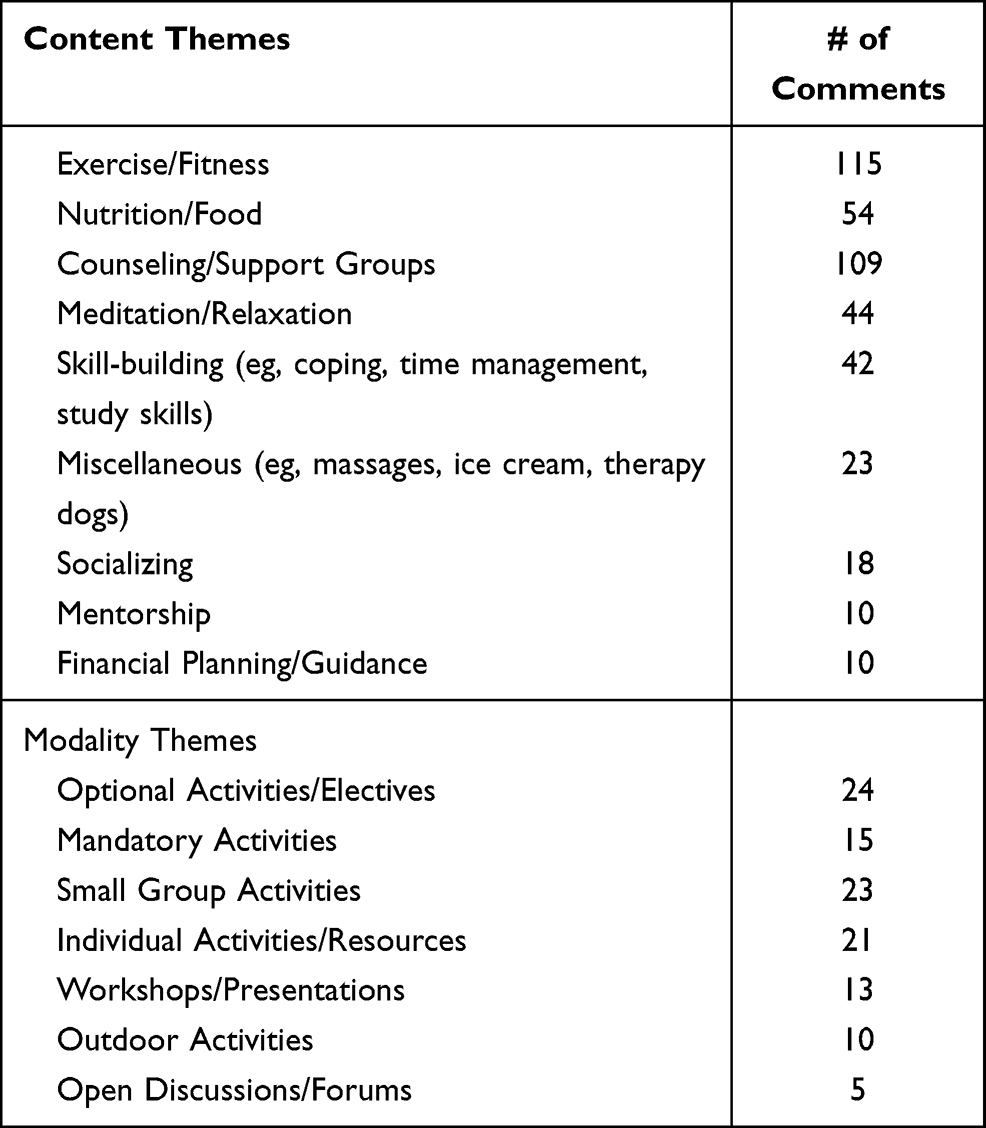 |
Table 3 Number of Comments for Each Theme Related to Student Suggestions for a Medical School Wellness Program |
Implementing more opportunities for exercise/fitness and counseling/support groups gathered the highest response rate from medical students. Many of the responses supporting exercise/fitness cited more fitness and yoga classes on campus and free or discounted gym access. Responses regarding counseling/support groups suggested offering various student support groups to talk about stressors, and free and confidential counseling services on campus, with many suggesting mandatory individual sessions at least once per semester. Other ideas included access to dieticians and healthier foods, meditation and relaxation classes, tutors or counselors to aid with studying and time management, access to massage therapists and visits from therapy dogs, non-academic class socials to create class unity, mentorship from both medical students in later years of training and practicing physicians, and financial planning classes and resources.
The modality by which medical students thought wellness program initiatives should be implemented yielded varying responses. Many students suggested optional activities/electives (eg, “Anything forced will be viewed as a waste of time or unnecessary by many people” and “[don’t include] mandatory sessions that imitate lectures students already receive for many hours of the day”), though there was also support for mandatory participation in select activities, particularly related to checking in on student wellbeing (eg, “Mandatory visit to a psychologist/psychiatrist at least once a semester in 1st/2nd year”). Indeed, several students suggested small group meetings to discuss stressors and how to balance the demands of medical school (eg, “Regular (monthly) student support groups” and “It would include confidential small group meetings in which we would discuss highs and lows in our lives and check in with one another”); and others recommended individual meetings (eg, “I think the biggest thing would be to regularly schedule periodic 1-on-1 meetings with all students to see how they’re doing” and “Have advisors meet up with students early on in the year to give students individualized info on how to study and stay positive”). Other responses suggested workshops/presentations on stress management and mental health/wellness, with emphasis on creating work-life balance (eg, “Sessions on coping strategies” and “Include some workshops on maintaining a life/school balance”). Finally, some students recommended including outdoor activities like hikes or picnics that promote being out in nature and hosting open forums where students could bring up any issues for discussion.
Discussion
Research has shown that many medical students believe that resources devoted to their wellness are lacking.36 Student feedback is invaluable to institutions attempting improvements, and it has been used in other studies as a way to test the effectiveness of newly implemented wellness programs.24,37 The current results address a gap in the literature by soliciting student recommendations regarding changes to the medical school experience that might promote better health and wellness among medical students. Although a small literature base documents student feedback on existing programs, this study took a different approach by asking students what they would suggest going forward to support student wellbeing. Given the significant cost of implementing changes to the curriculum, providing additional resources, and/or making other improvements to the medical school experience, this information may be particularly valuable to medical schools that are in the planning stages of wellness program development, allowing them to avoid investing resources in less-valued interventions and/or missing opportunities to implement highly desired changes.
A key finding of the present study was that student perspectives were consistent with the Stanford Model of Professional Fulfillment,38 which conceptualizes wellbeing/fulfillment as being significantly influenced by institutional factors, rather than primarily individual factors. The model describes 3 key components: 1) culture of wellness, which refers to the supportiveness of the learning/work environment; 2) efficiency of practice, which refers to policies and procedures that make it easier or more difficult to complete work; and 3) personal resilience, which refers to individual efforts at self-care. It emphasizes the fact that personal resilience is only one component of wellbeing, which cannot make up for sustained exposure to negative culture and inefficient processes. Student responses reflected this insight, with the majority of students suggesting changes to the structure and culture of medical school, rather than implementation of additional student-directed “wellness” programming.
With regard to culture, students recommended improving communication with students, and promoting increased respect and support from peers and faculty. Specifically, students suggested that strong mentoring programs could help them feel more supported. Mentoring programs in medical school have been related to high or improved academic performance for students, as well as facilitating the development of a student-faculty relationship that supports student personal and professional growth.39–41,45–48 Students also suggested decreasing stigma toward mental healthcare, and increasing access to counseling. Anecdotally, our student-directed events aimed at combatting stigma (eg, panels involving graduating students and faculty members sharing their own mental health struggles and recovery) have been among the best-attended and most appreciated initiatives we have implemented. Finally, students recommended minimizing aspects of the curriculum that seem unnecessary/excessive, while encouraging recreational and social activities to promote better work/life balance. This is consistent with a recent study showing that implementing the combination of a mindfulness course, social events, pass/fail grading, and reduced contact hours in preclinical years led to lower rates of severe depression, stress, and anxiety among medical students.10
Recommendations related to efficiency of process primarily included requests to streamline and improve curricular scheduling, as well as to emphasize quality of teaching. Some students suggested that medical schools should be reformed to place less emphasis on Step 1 scores. Although this may have seemed like a radical suggestion just a few years ago, the USMLE is scheduled to move to pass/fail grading on the Step exams beginning in 2022. This change is supported by a study which found that using Step 1 scores to rank residency applicants is not evidence-based, as scores were not correlated with reliable measures of medical student or resident clinical skills.41 Students also requested that their schools implement a pass-fail grading system, which has been shown to improve mental quality of life and decrease perceived stress and burnout7,27–30,39–42 without producing a significant change in scores on Step 1 and 2 exams or post-residency specialty board certification exams.21
With regard to suggestions associated with improving personal resilience, some of the student recommendations have demonstrated effectiveness in previous studies. For example, students recommended implementing a wellness program into the existing curriculum. Various studies have documented the benefits of such an intervention, particularly when the program focuses on development of mindfulness and other aspects of stress reduction.30,43–45 We have recently obtained particularly positive student feedback by implementing mandatory wellness content that is directly tied to clinical skill development.46 Students also outlined ways to improve physical wellness, such as through integrating yoga or other exercise programs into the curriculum, which previous studies have credited for improving medical student wellbeing.47–49
When asked specifically about designing a “wellness program,” student responses were more consistent with the individually focused personal resilience initiatives that have typically been implemented to support wellbeing (eg, access to fitness classes/equipment, counseling, nutrition). One remaining logistical challenge is determining which elements of a wellness program should be made mandatory or voluntary, as students have conflicting beliefs regarding this issue. The question highlights the students’ difficulty choosing personal health over work responsibilities, which is a significant challenge for many practicing physicians as well.50,51 Extrapolating from the low rates of help-seeking among medical students experiencing psychological distress, it is likely that many students who would benefit from wellness programs would choose not to participate if attendance were voluntary. Indeed, students participating in our elective course on mindfulness and mind-body medicine raised similar concerns when asked about ways to better disseminate the course content to their peers.45
On the other hand, making wellness programs mandatory for all students might contravene their desire for more protected time-off and independent study time outside of required school activities. One option may be to build in protected time for student wellness efforts into the curriculum, with some flexibility regarding programming/resources from which students can choose what would be most beneficial to them. Some studies have used medical students’ brainstorming responses to categorize clusters of self-care activities to better understand and improve self-care.49 Future research should explore the perceived benefit of mandatory versus optional participation in wellness activities. In addition, future studies should examine whether teaching medical students to prioritize wellness during medical school results in sustained adherence to healthy behaviors throughout their careers. While many institutions have already made changes to improve medical student wellbeing, studies suggest that further changes to the healthcare environment and culture need to be made.50
Limitations
Some limitations to this study should be noted. All participants were students enrolled in medical school within the state of Florida, so it is possible that results would not generalize to students in other states. However, it is noteworthy that the sample included students from public and private, allopathic and osteopathic, university- and community-based, and new and established medical schools. Second, the data were obtained only from students who chose to participate in the study and completed the open-ended questions. It is unknown how views of students who chose not to participate may differ from those included in the study. Despite this, the results reflect the views of a significant number of students and are worthy of attention in their own right. Relatedly, the overrepresentation of first-year students in the sample (ie, 34%) may have skewed the results toward comments regarding early experiences in medical school (ie, during primarily classroom-based learning). Finally, due to concerns about anonymity, it was not possible to assess student recommendations based on their age, race, or the school they attended, which may have helped to contextualize student responses. Future research should examine demographic differences in student recommendations to determine whether different wellness initiatives may be perceived as beneficial for students with different backgrounds and needs.
Conclusion
Promoting and supporting medical student wellness is vital to the development of a healthy physician workforce. Though medical schools have increased attention to this topic in recent years, it is important to consider student-identified needs and desires when developing wellness initiatives in order to maximize the impact. Results of this study outline a variety of targets for intervention, including novel suggestions that had not been reported in the literature previously. Medical schools may use these recommendations to guide efforts to improve their curricular structure, support services, and/or program offerings in order to encourage wellbeing among their students. Though financial and logistical challenges to implementing some recommendations exist, the results provide insight into avenues for future exploration in the development of medical student wellness initiatives. Further, many of the suggestions from the students in this study would be inexpensive to implement and may significantly improve medical student wellbeing.
Acknowledgments
This project was funded by the Professionals Resource Network, Inc., an integral arm of the Florida Medical Association. The authors wish to thank the medical students who participated in this study, and the Florida Council of Medical School Deans, Florida Medical Association, and Florida Osteopathic Medical Association for their support of the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dyrbye LN, Harper W, Durning SJ, et al. Patterns of distress in US medical students. Med Teach. 2011;33(10):834–839. doi:10.3109/0142159X.2010.531158
2. Dyrbye LN, Thomas MR, Shanafelt TD. Systematic review of depression, anxiety, and other indicators of psychological distress among U.S. and Canadian medical students. Acad Med. 2006;81(4):354–373. doi:10.1097/00001888-200604000-00009
3. Dyrbye LN, Thomas MR, Eacker A, et al. Race, ethnicity, and medical student well-being in the United States. Arch Intern Med. 2007;167(19):2103–2109. doi:10.1001/archinte.167.19.2103
4. Dyrbye LN, West CP, Satele D, et al. Burnout among U.S. medical students, residents, and early career physicians relative to the general U.S. population. Acad Med. 2014;89(3):443–451. doi:10.1097/ACM.0000000000000134
5. Ghodasara SL, Davidson MA, Reich MS, Savoie CV, Rodgers SM. Assessing student mental health at the Vanderbilt university school of medicine. Acad Med. 2011;86(1):116–121. doi:10.1097/ACM.0b013e3181ffb056
6. Dyrbye LN, Thomas MR, Huntington JL, et al. Personal life events and medical student burnout: a Multicenter Study. Acad Med. 2006;81(4):374–384. doi:10.1097/00001888-200604000-00010
7. Reed DA, Shanafelt TD, Satele DW, et al. Relationship of pass/fail grading and curriculum structure with well-being among preclinical medical students: a Multi-Institutional Study. Acad Med. 2011;86(11):1367–1373. doi:10.1097/ACM.0b013e3182305d81
8. Givens JL, Tjia J. Depressed medical students’ use of mental health services and barriers to use. Acad Med. 2002;77(9):918–921. doi:10.1097/00001888-200209000-00024
9. Mosley TH
10. Slavin SJ, Schindler DL, Chibnall JT. Medical student mental health 3.0: improving student wellness through curricular changes. Acad Med. 2014;89(4):573–577. doi:10.1097/ACM.0000000000000166
11. Rotenstein LS, Ramos MA, Torre M, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and meta-analysis. JAMA. 2016;316(21):2214–2236. doi:10.1001/jama.2016.17324
12. Brazeau CM, Shanafelt T, Durning SJ, et al. Distress among matriculating medical students relative to the general population. Acad Med. 2014;89(11):1520–1525. doi:10.1097/ACM.0000000000000482
13. Rosal MC, Ockene IS, Ockene JK, Barrett SV, Ma Y, Hebert JR. A longitudinal study of students’ depression at one medical school. Acad Med. 1997;72(6):542–546. doi:10.1097/00001888-199706000-00022
14. Compton MT, Carrera J, Frank E. Stress and depressive symptoms/dysphoria among US medical students: results from a large, nationally representative survey. J Nerv Ment Dis. 2008;196(12):891–897. doi:10.1097/NMD.0b013e3181924d03
15. Santen SA, Holt DB, Kemp JD, Hemphill RR. Burnout in medical students: examining the prevalence and associated factors. South Med J. 2010;103(8):758–763. doi:10.1097/SMJ.0b013e3181e6d6d4
16. Linn BS, Zeppa R. Stress in junior medical students: relationship to personality and performance. J Med Educ. 1984;59(1):7–12.
17. Toews JA, Lockyer JM, Dobson DJ, et al. Analysis of stress levels among medical students, residents, and graduate students at four Canadian schools of medicine. Acad Med. 1997;72(11):997–1002. doi:10.1097/00001888-199711000-00019
18. Lins L, Carvalho FM, Menezes MS, Porto-Silva L, Damasceno H. Health-related quality of life of students from a private medical school in Brazil. Int J Med Educ. 2015;6:149–154. doi:10.5116/ijme.563a.5dec
19. Pagnin D, de Queiroz V. Comparison of quality of life between medical students and young general populations. Educ Health (Abingdon). 2015;28(3):209–212. doi:10.4103/1357-6283.178599
20. Dunn LB, Iglewicz A, Moutier C. A conceptual model of medical student well-being: promoting resilience and preventing burnout. Acad Psychiatry. 2008;32(1):44–53. doi:10.1176/appi.ap.32.1.44
21. Wasson LT, Cusmano A, Meli L, et al. Association between learning environment interventions and medical student well-being: a systematic review. JAMA. 2016;316(21):2237–2252. doi:10.1001/jama.2016.17573
22. Worley LL. Our fallen peers: a mandate for change. Acad Psychiatry. 2008;32(1):8–12. doi:10.1176/appi.ap.32.1.8
23. Vankar JR, Prabhakaran A, Sharma H. Depression and stigma in medical students at a private medical college. Indian J Psychol Med. 2014;36(3):246–254. doi:10.4103/0253-7176.135372
24. Drolet BC, Rodgers S. A comprehensive medical student wellness program–design and implementation at Vanderbilt school of medicine. Acad Med. 2010;85(1):103–110. doi:10.1097/ACM.0b013e3181c46963
25. Shapiro SL, Schwartz GE, Bonner G. Effects of mindfulness-based stress reduction on medical and premedical students. J Behav Med. 1998;21(6):581–599. doi:10.1023/A:1018700829825
26. Shiralkar MT, Harris TB, Eddins-Folensbee FF, Coverdale JH. A systematic review of stress-management programs for medical students. Acad Psychiatry. 2013;37(3):158–164. doi:10.1176/appi.ap.12010003
27. Bloodgood RA, Short JG, Jackson JM, Martindale JR. A change to pass/fail grading in the first two years at one medical school results in improved psychological well-being. Acad Med. 2009;84(5):655–662. doi:10.1097/ACM.0b013e31819f6d78
28. de Vibe M, Solhaug I, Tyssen R, et al. Mindfulness training for stress management: a Randomised Controlled Study of medical and psychology students. BMC Med Educ. 2013;13(1):107. doi:10.1186/1472-6920-13-107
29. Finkelstein C, Brownstein A, Scott C, Lan YL. Anxiety and stress reduction in medical education: an intervention. Med Educ. 2007;41(3):258–264. doi:10.1111/j.1365-2929.2007.02685.x
30. Rosenzweig S, Reibel DK, Greeson JM, Brainard GC, Hojat M. Mindfulness-based stress reduction lowers psychological distress in medical students. Teach Learn Med. 2003;15(2):88–92. doi:10.1207/S15328015TLM1502_03
31. Saunders PA, Tractenberg RE, Chaterji R, et al. Promoting self-awareness and reflection through an experiential mind-body skills course for first year medical students. Med Teach. 2007;29(8):778–784. doi:10.1080/01421590701509647
32. Warnecke E, Quinn S, Ogden K, Towle N, Nelson MR. A randomised controlled trial of the effects of mindfulness practice on medical student stress levels. Med Educ. 2011;45(4):381–388. doi:10.1111/j.1365-2923.2010.03877.x
33. Keissling C, Schubert B, Scheffner D, Burger W. First year medical students’ perceptions of stress and support: a comparison between reformed and traditional track curricula. Med Educ. 2004;38(5):504–509. doi:10.1046/j.1365-2929.2004.01816.x
34. Merlo LJ, Curran JS, Watson R. Gender differences in substance use and psychiatric distress among medical students: a comprehensive statewide evaluation. Subst Abus. 2017;38(4):401–406. doi:10.1080/08897077.2017.1355871
35. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
36. Frank E, Hedgecock J, Elon LK. Personal health promotion at US medical schools: a Quantitative Study and qualitative description of deans’ and students’ perceptions. BMC Med Educ. 2004;4(1):29. doi:10.1186/1472-6920-4-29
37. Dyrbye LN, Shanafelt TD. Commentary: medical student distress: a call to action. Acad Med. 2011;86(7):801–803. doi:10.1097/ACM.0b013e31821da481
38. Bohman B, Dyrbye L, Sinskey C. Physician well-being: the reciprocity of practice efficiency, culture of wellness, and personal resilience. NEJM Catal. 2017;3:4.
39. Frei E, Stamm M, Buddeberg-Fischer B. Mentoring programs for medical students–a review of the PubMed literature 2000–2008. BMC Med Educ. 2010;10(1):32. doi:10.1186/1472-6920-10-32
40. Dimitriadis K, von der Borch P, Stormann S, et al. Characteristics of mentoring relationships formed by medical students and faculty. Med Educ Online. 2012;17(1):17242. doi:10.3402/meo.v17i0.17242
41. McGaghie WC, Cohen ER, Wayne DB. Are United States medical licensing exam step 1 and 2 scores valid measures for postgraduate medical residency selection decisions? Acad Med. 2011;86(1):48–52. doi:10.1097/ACM.0b013e3181ffacdb
42. Rohe DE, Barrier PA, Clark MM, Cook DA, Vickers KS, Decker PA. The benefits of pass-fail grading on stress, mood, and group cohesion in medical students. Mayo Clin Proc. 2006;81(11):1443–1448. doi:10.4065/81.11.1443
43. Dobkin PL, Hutchinson TA. Teaching mindfulness in medical school: where are we now and where are we going? Med Educ. 2013;47(8):768–779. doi:10.1111/medu.12200
44. Dobkin PL, Balass S. Multiple influences contribute to medical students’ well-being and identity formation. Med Educ. 2014;48(4):340–342. doi:10.1111/medu.12409
45. Williams MK, Estores IM, Merlo LJ. Promoting resilience in medicine: the effects of a mind-body medicine elective to improve medical student well-being. Glob Adv Health Med. 2020;9:2164956120927367. doi:10.1177/2164956120927367
46. Dede B, Merlo LJ, Smith KB. CBT in the ATL: cognitive restructuring techniques to improve the well-being of medical students and their future patients [Abstract].
47. Bitonte RA, DeSanto DJ
48. Morris A, Do D, Gottlieb-Smith R, et al. Impact of a fitness intervention on medical students. South Med J. 2012;105(12):630–634. doi:10.1097/SMJ.0b013e318273a766
49. Simard A-A, Henry M. Impact of a short yoga intervention on medical students’ health: a Pilot Study. Med Teach. 2009;31(10):950–952. doi:10.3109/01421590902874063
50. George S, Hanson J, Jackson JL. Physician, heal thyself: a Qualitative Study of physician health behaviors. Acad Psychiatry. 2014;38(1):19–25. doi:10.1007/s40596-013-0014-6
51. Smith F, Goldacre MJ, Lambert TW. Working as a doctor when acutely ill: comments made by doctors responding to United Kingdom surveys. JRSM Open. 2016;7(4):2054270416635035.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.