")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 11
Assessment of sleep quality and its predictors among patients with diabetes in Jazan, Saudi Arabia
Authors Darraj A , Mahfouz MS , Alsabaani A , Sani M, Alameer A
Received 29 June 2018
Accepted for publication 18 July 2018
Published 25 September 2018 Volume 2018:11 Pages 523—531
DOI https://doi.org/10.2147/DMSO.S178674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ming-Hui Zou
Abdulaziz Darraj,1 Mohamed Salih Mahfouz,2 Abdullah Alsabaani,3 Mubarack Sani,2 Anwar Alameer1
1Jazan Health Affairs, Ministry of Health, Jazan, Saudi Arabia; 2Family and Community Medicine Department, College of Medicine, Jazan University, Jazan, Saudi Arabia; 3Family and Community Medicine Department, College of Medicine, King Khalid University, Abha, Saudi Arabia
Background: Poor sleep quality is common among patients with diabetes. It is associated with negative physical, psychological, and functional consequences. However, the implicated risk factors of poor sleep quality remain uncertain.
Objectives: This study aimed to determine the prevalence of poor sleep quality among patients with diabetes and to investigate the factors associated with the poor sleep quality.
Patients and methods: An analytical cross-sectional study of 307 diabetic patients in Jazan, Saudi Arabia was conducted in 2018. A multistage cluster random sampling was used to select the study participants. Sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI). Data on patient’s characteristics were gathered via patients’ interviews, and medical data were collected based on the patients’ files. Logistic regression analysis was used to identify the predictors of poor sleep quality.
Results: The mean score of PSQI was 5.29±2.73. The prevalence of poor sleep quality was 55.4% (95% CI 49.7–60.8). Sociodemographic and clinical factors were significantly associated with poor sleep quality, such as being elderly, female, illiterate, smoker, complications of diabetes, comorbidity, or psychological symptoms. However, female gender was the strongest predictor of reporting poor quality of sleep, OR= 3.69, 95% CI 1.65–8.28 (P<0.001).
Conclusion: Poor sleep quality among diabetic patients is a prevalent health problem. Many factors can affect sleep quality. Health care providers may consider routine screening for and address sleep problems among diabetic patients.
Keywords: poor sleep quality, prevalence, risk factors, diabetes mellitus, Saudi Arabia
Introduction
Diabetes is a critical public health problem. Globally, over the past few decades, the magnitude of diabetes among adults aged ≥18 years has risen dramatically, with the number of patients with diabetes in 2014 reaching 422 million. The middle- and low-income countries in particular are under the greatest threat and according to the 2016 WHO report,1 these countries are also expected to experience the greatest increase in the prevalence of diabetes over the next few years. Locally, the prevalence of diabetes in Saudi Arabia was assessed to be 25.4% among people aged between 20 and 79 years.2,3
Until the mid-20th century, sleep was thought of as a dormant part of our daily lives, however, this turned out to be inaccurate because our brains are active during sleep.4 Sleep is a complex, very organized condition that is fundamental to life.5 It is an essential biological process that maintains physical, mental, and emotional health.6 Sleep quality is defined as one’s perception that they fall asleep easily, for an adequate duration of time so as to wake up feeling rested, and can make it through the day without facing excessive daytime sleepiness.7
Poor sleep quality is a prevalent health problem among patients with diabetes. It is estimated that 53.4% of diabetic patients experience a poor quality of sleep compared to 29% in general population.8 Concerns over poor sleep quality among patients with diabetes have increased in recent years, but the implicated risk factors of poor sleep quality remain uncertain. Different factors that may affect the sleep quality of patients with diabetes have been suggested by many studies, including sociodemographic, clinical, and diabetes-related factors, such as duration of diabetes, diabetic complications, presence of comorbidity,9 uncontrolled glycosylated hemoglobin,10 abnormal body mass index (BMI),11 insulin use,12 and psychological factors.13
The effects of unhealthy sleep pattern on the body are numerous and widely varied, spanning different body systems. Accumulated evidence shows that, disturbed sleep is an important factor associated with the impairment of the entire spectrum of mental abilities, ranging from simple to more complicated mental functions,14 which can lead to deficits in alertness and cognitive performance,15 and occurrence of accidents.16 Moreover, many adverse physiological effects can occur due to this disturbance, including high blood pressure, impairment of glucose control, and an increase in the body inflammation process.17,18 In addition, management of poor sleep quality in patients with diabetes is important as it has been recognized as one of the causes that can lead to several complications experienced by diabetic patients. It is related with negative physical, mental, and functional consequences.19 Poor quality of sleep has been found to be a crucial factor for bad glycemic control,20 moreover, it can lead to many complications, such as cardiovascular diseases,21 neuropathy,22 retinopathy,23 nephropathy,24 and psychological distress.25
Therefore, it is critical to investigate the risk factors associated with poor sleep quality among patients with diabetes to improve their quality of sleep. The purpose of this research study was to determine the prevalence of poor sleep quality among patients with diabetes and to investigate the factors that affect their sleep.
Patients and methods
Design, setting, and participants
This is an analytical cross-sectional study that was conducted on patients with diabetes, at primary health care centers (PHCCs) in Jazan during the period from October 2017 to April 2018. The study included participants aged ≥18 years, who were diagnosed with diabetes for at least 1 year. Patients with known psychiatric disorders, on sleeping pills, who are pregnant, or working night shifts were excluded.
Sampling procedure
Sample size was calculated using Swanson and Cohen method,26 according to the following parameters: 73% estimated prevalence in the population,12 0.05 margin of error, and 95% CI. The calculated sample size was 302 subjects adjusted to be 332 to account for 10% nonresponse rate. A multistage cluster random sampling technique was followed to select eight PHCCs. A random sample was selected from each primary health care center proportionally.
Data collection and study instruments
The data collection tools included sociodemographic characteristics, clinical-related variables, and a sleep quality assessment questionnaire. The patients were interviewed by a trained physician in order to collect the data. Sociodemographic section gathered information about age, gender, occupation, marital status, education level, personal habits, and physical activity. The clinically related variable section comprises information about diabetes duration, complications (retinopathy, nephropathy, neuropathy, or cardiovascular), comorbidity (hypertension, bronchial asthma, chronic obstructive pulmonary disease, gastroesophageal reflux disease), medications, HbA1c, BMI, and psychological factors. The study utilized three standardized and validated tools, namely global physical activity questionnaire (GPAQ), depression, anxiety, and stress scale (DASS), and Pittsburgh Sleep Quality Index (PSQI).
PSQI
PSQI is a standardized subjective tool to assess sleep quality over the past month. It consists of seven component scales: sleep disturbances, sleep duration, sleep latency, sleep efficiency, use of sleep medication, daytime dysfunction, and sleep quality. Each component is scored from 0 to 3. The seven component scores are summed up to yield a global PSQI score ranging from 0 to 21. A subject with an overall PSQI score >5 is considered to have poor sleep quality.27 A validated Arabic version of PSQI was utilized.28
GPAQ
GPAQ is a tool that was developed by WHO to assess the physical activity, and it measures physical activity in three domains: activities at work, transportation, and leisure. If the total physical activity metabolic equivalent minutes per week is >600, the subject is classified as physically active.29
DASS
DASS is a standardized and validated instrument. It includes three self-reported scales with seven items for each scale, that are intended to evaluate the psychological states of depression, anxiety, and stress. The 4-point severity scale is used to rate the degree to which the participant has experienced each item. Scores for each emotional state are calculated by adding the scores for the relevant items.30
Data management and statistical analysis
Data entry and analysis were achieved using the Statistical Package for Social Sciences version 23 for Windows (IBM Corporation, Armonk, NY, USA). The data analysis includes both descriptive and inferential statistics. The descriptive statistics were calculated in the form of frequency counts and percentages. For the quantitative variables, mean and SD were used. Sleep quality status was the dependent variable of the study, and various sociodemographic and clinical variables were considered as independent variables. The chi-squared test was used to test the statistical significance of associations. Univariate logistic regression analysis was performed to evaluate the association between various independent variables and sleep quality. To estimate the effect of explanatory variables on the sleep quality, the multivariate logistic regression analysis was performed. P-value <0.05 was considered statistically significant.
Ethical considerations
The study was approved by the Ethics Committee of King Khalid University, Saudi Arabia (approved number: REC#20180142). Each participant was provided with detailed information about the research and was assured of confidentiality. Written informed consent was obtained, and participants were aware of their right to participate or withdraw from the study at any time.
Results
Sociodemographic and clinical characteristics
A total of 307 participants were included in the analysis, giving a response rate of 92.5%. According to Table 1, the mean age was 53.8±12.3 years, with almost an equal distribution of gender in the sample, with 48% being females. Approximately 80% were married and one-third were illiterate. Among the study participants, 21.2% were smokers, 18.2% were khat users, and 62.2% were physically inactive. Diabetic complications were exhibited by 48.5% of participants, while comorbidity was present in 58%. Twenty-eight percent were using insulin. Fifty-nine percent were considered uncontrolled based on them having a HbA1c >7%. Two-thirds of the participants had been classified as overweight or obese. Abnormal scores of depression, anxiety, and stress were 24.4%, 45%, and 27.7%, respectively.
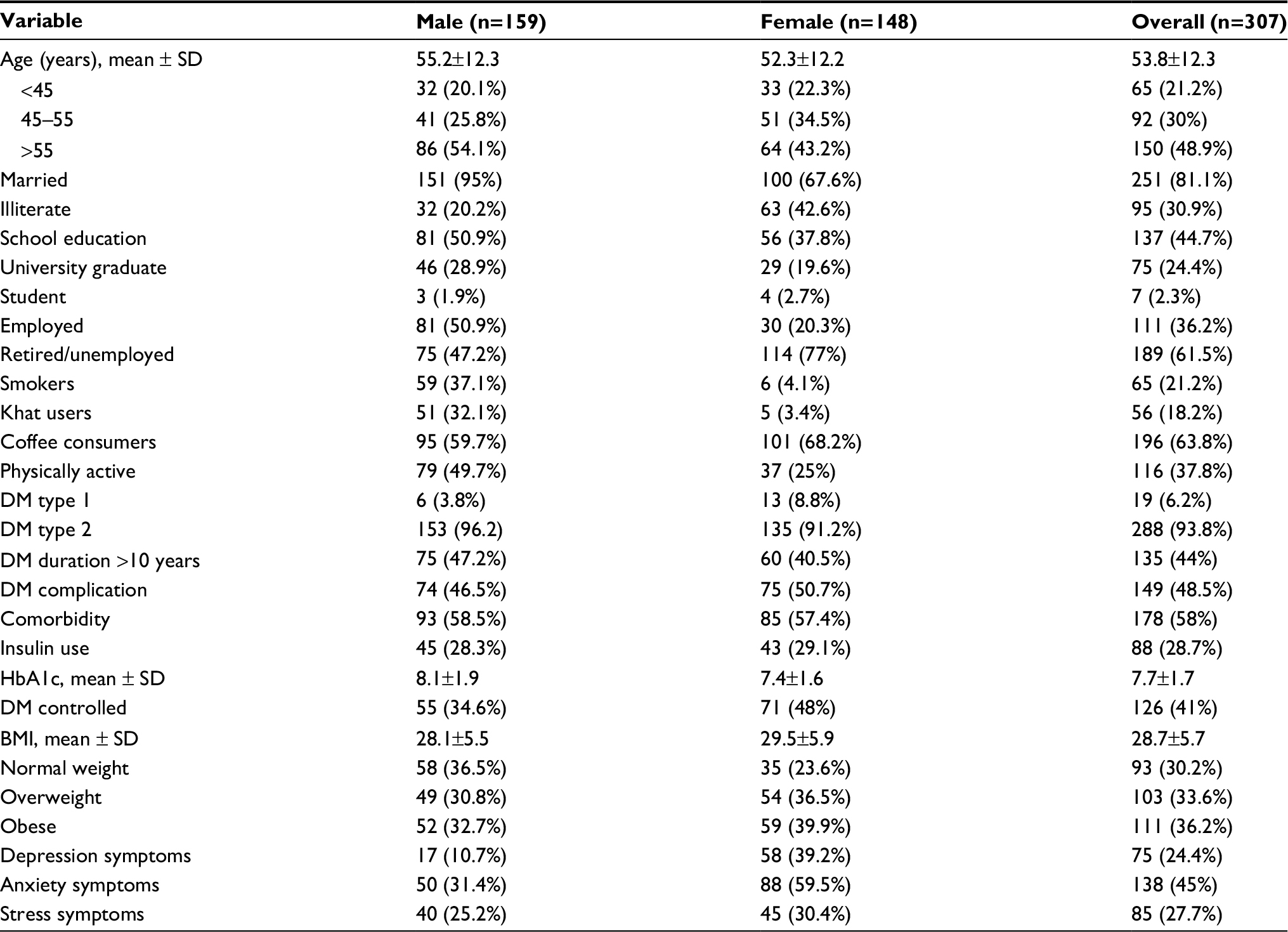 | Table 1 Sociodemographic and clinical characteristics of participants by gender Abbreviations: BMI, body mass index; DM, diabetes mellitus. |
Sleep quality among study participants
The PSQI was used to assess the participants’ sleep quality status. The mean score was 5.29±2.73. Based on the respective criteria, 170 participants (55.4%) had a poor sleep quality with a cutoff point of PSQI score >5.27 Table 2 displays the association between the patients’ sociodemographic characteristics and poor sleep quality. Forty percent of participants aged <45 years had poor sleep quality, and this percentage increased to 55.4% and 62% in the higher age categories of 45–55 and >55 years, respectively (P=0.012). The majority (66.9%) of females reported poor sleep quality, while this was in the minority for males (44.7%) (P<0.001). Poor sleep quality was higher (78.9%) among the illiterate, compared to educated patients (P<0.001). Compared to those who were employed, poor sleep quality was reported by majority (59.7%) of unemployed participants (P=0.043). In addition, poor sleep quality was more prevalent among smokers (P=0.005), khat users (P<0.001), and participants who were physically inactive (P=0.004). The associations between both marital status and sleep quality and coffee consumption and sleep quality were not statistically significant (P=0.154 and P=0.56, respectively).
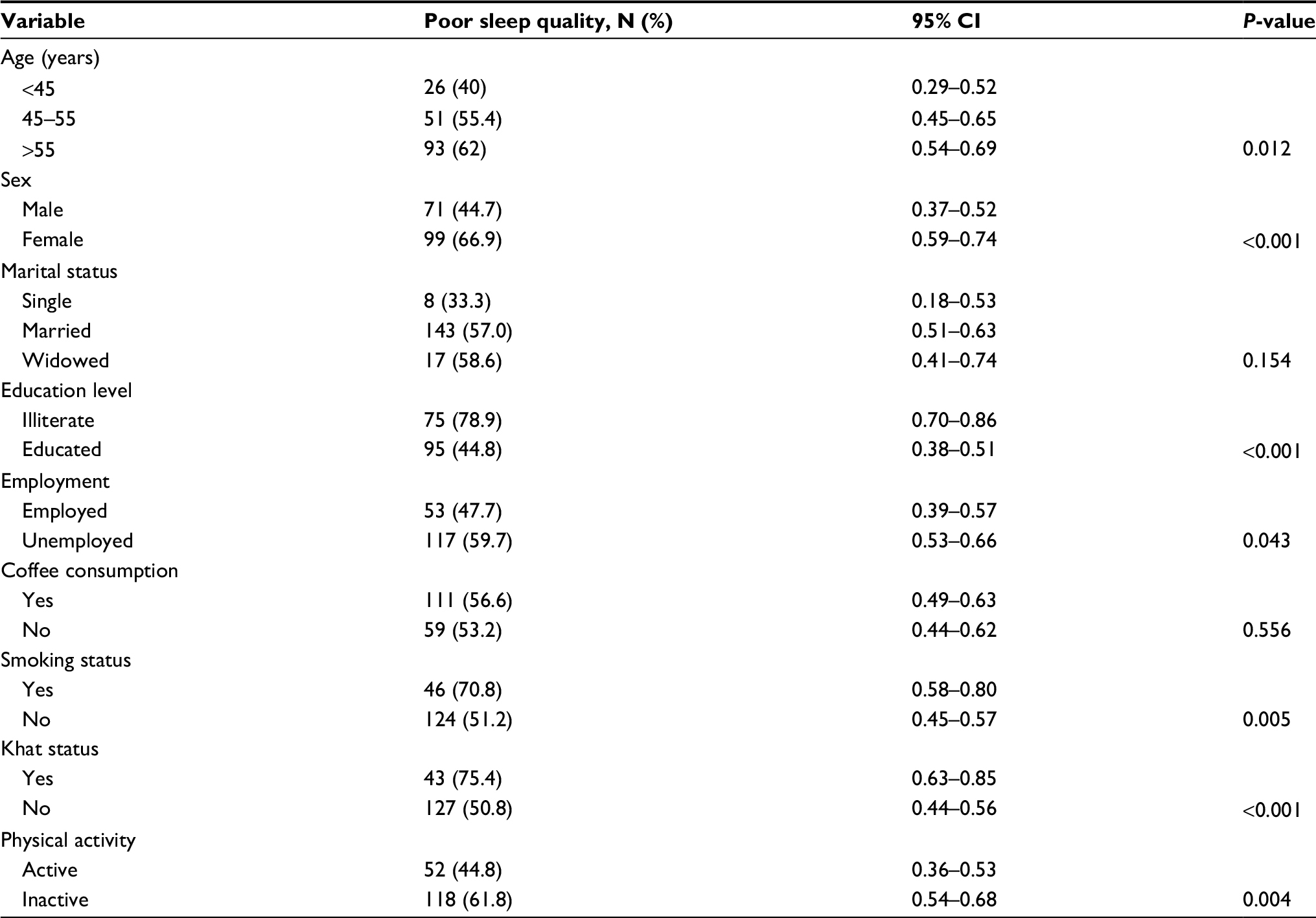 | Table 2 Sleep quality among the participants according to sociodemographic variables |
Table 3 shows the associations between the patients’ clinical characteristics and poor sleep quality. Poor sleep quality was more prevalent among participants who had diabetes for a longer duration (P<0.001), had diabetes complications (P<0.001), had a comorbidity (P<0.001), were being treated with insulin (P=0.036), had uncontrolled diabetes (HbA1c >7%) (P<0.001), had psychological symptoms (P<0.001), and had an abnormal BMI. The percentages of poor sleep quality among overweight and obese participants were 61.2% and 64.9%, respectively, compared to 38% of the participants whose weight was normal (P<0.001). However, there was no statistically significant association between diabetes type and poor sleep quality (P=0.804).
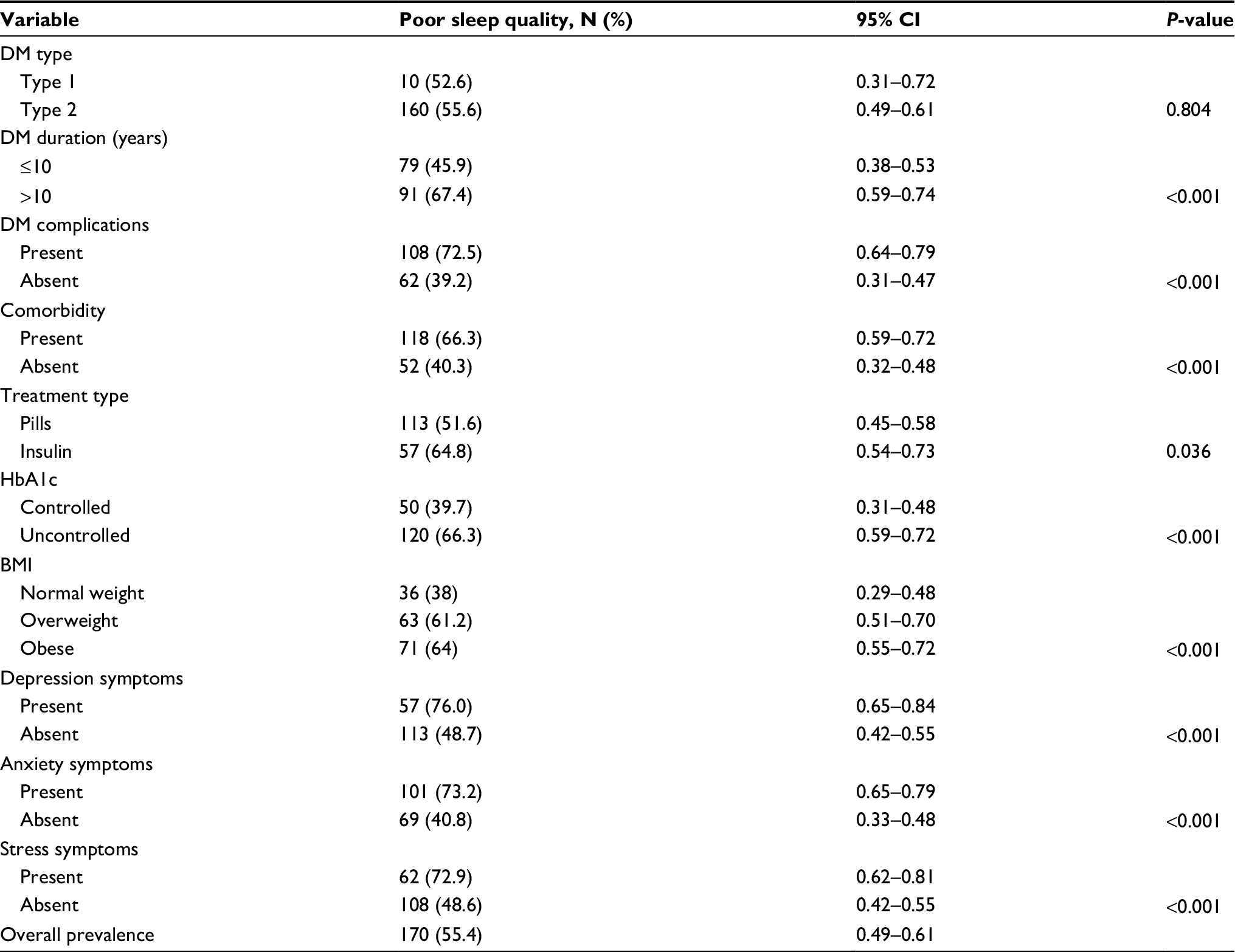 | Table 3 Sleep quality among the participants according to clinical variables Note: P-value <0.05. Abbreviations: BMI, body mass index; DM, diabetes mellitus. |
Predictors of poor sleep quality
Table 4 shows the results of the univariate and multivariate logistic regression analyses. The univariate analysis at 95% CI shows that the statistically significant predictors of poor sleep quality were: being elderly (particularly aged >55 years), female, illiterate, unemployed, smoker, khat user, physically inactive, overweight or obese, on insulin treatment, having diabetes for >10 years, having diabetes complications, having comorbid conditions, uncontrolled diabetes, and psychiatric symptoms. The full model comprising all of the predictors in the multivariate logistic regression analysis was statistically significant (P<0.001). Only eight independent variables made a statistically significant contribution to the model, namely female, illiterate, smoker, khat user, diabetes mellitus (DM) complications, comorbidity, overweight or obese, and anxiety. The strongest predictor of reporting poor sleep quality was the female gender, with this gender being 3.69 times more likely to report poor sleep quality than the male gender. ORfemale vs male =3.69 (95% CI 1.651–8.276; P<0.001).
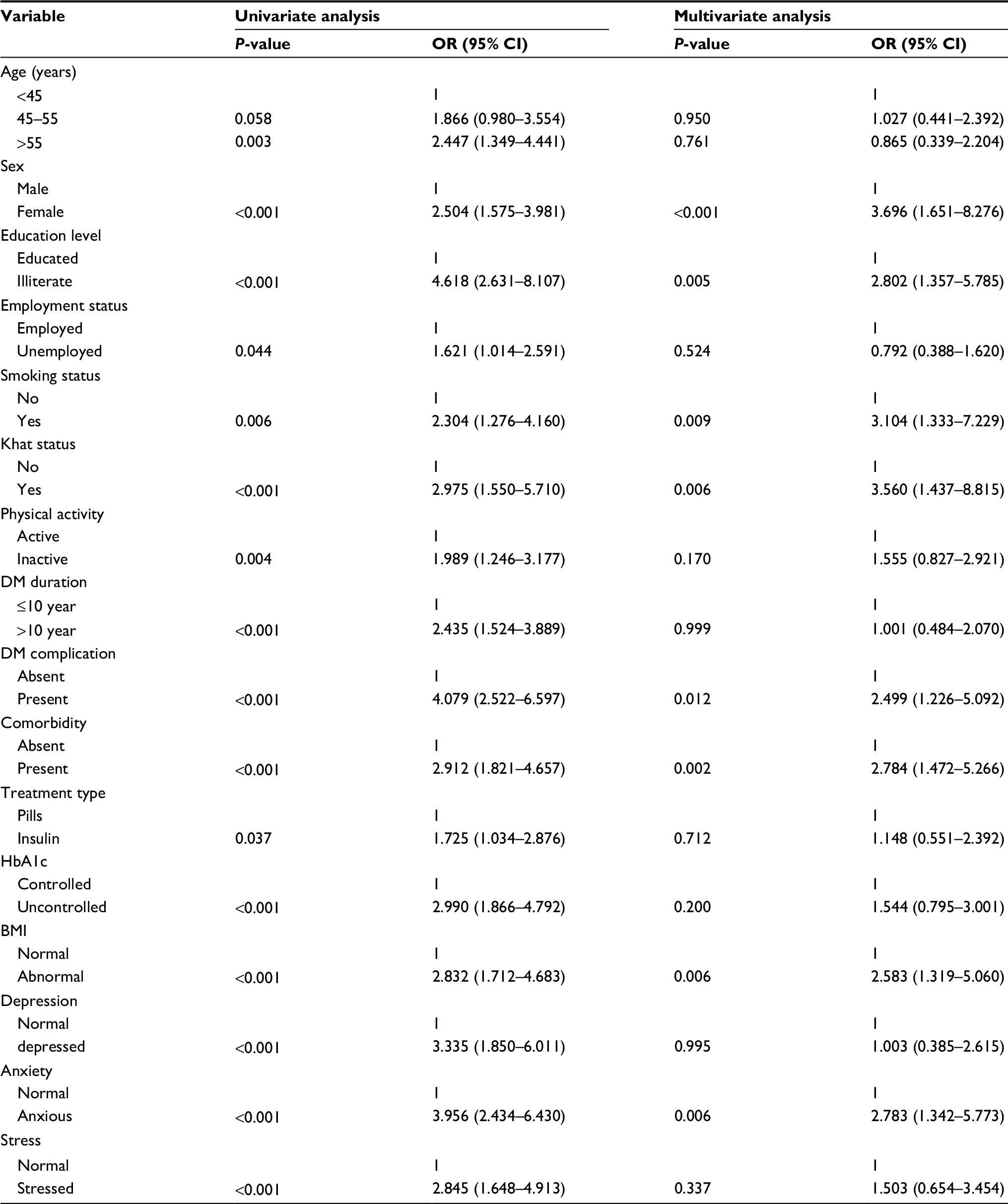 | Table 4 Results of logistic regression analysis between patient characteristics and poor sleep quality Note: The categories of the predictive variables that received odds ratios of 1.00 are reference categories. Abbreviations: BMI, body mass index; DM, diabetes mellitus. |
Discussion
In this study, poor sleep quality was present in more than half of the participants (55.4%). This prevalence is similar to the studies conducted by Cunha et al and Luyster et al.31,32 Some studies have shown a higher prevalence, such as those by Yücel et al and Colbay et al;33,34 however, these studies targeted diabetic patients in tertiary or referral hospitals, thus the risk of poor sleep quality for such patients seems to be higher. The present study shows that there is a higher prevalence of poor sleep quality among patients who are older, female, illiterate, or unemployed. This is consistent with the studies of Lou et al, Nefs et al, and Alqurayn et al.9,11,13 Regarding age and poor sleep quality, age-related sleep changes could explain the association, as age increases, sleep becomes less efficient.35 Female subjects in this study have some unfavorable sociodemographic and clinical characteristics compared with male subjects, such as higher BMI, less physical activity, and more diabetes complications. In addition, being illiterate may decrease the level of awareness regarding diabetes and its consequences, and increase the probability of poor sleep quality. The current study did not find a statistically significant relationship between coffee consumption and sleep quality. In fact, evidence of the effect of caffeinated drinks on the nature of sleep does exist; however, this effect is temporary, and drinking caffeinated beverages 6 hours prior to bed-time does not affect sleep, as shown by Drake et al.36 In the current study, the majority of participants who drank caffeinated beverages usually did so in the morning or afternoon. However, the effect of caffeine at bed-time, which was set at 10:30 pm for the current study, should be eliminated. In the current study, most of the smokers, khat users, and physically inactive participants reported poor sleep quality. This is consistent with studies by Nefs et al and Alqurayn et al.11,13 Another study that found no significant association between sleep quality and smoking was the one conducted by Alshenghiti et al.37 In fact, the effect of smoking on sleep quality has been established by many studies. These studies confirm the impact of smoking on sleep, such as sleep architecture disturbance.38 The use of khat also has a big effect on sleep quality,39 which mainly increase the sleep latency and decrease the efficiency of sleep.40 Regarding physical activity, interestingly, an interventional study was conducted during 2011 to assess the effects of four months of increased physical activity on sleep quality among diabetic patients. This study found a greater improvement in sleep quality in the intervention group compared to the control group.41 In the current study, no significant association was found between DM type (type 1 or type 2) and sleep quality. This finding is consistent with studies conducted by Nefs et al and Denic-Roberts et al.11,42 Poor sleep quality was more prevalent among participants who had diabetes for a longer duration, particularly, >10 years, DM complications, comorbidities, uncontrolled diabetes, and an abnormal BMI, as well as those using insulin treatment. This finding is in line with the majority of studies, including studies by, Cunha et al, Yücel et al, and Colbay et al.31,33,34 In addition, poor sleep quality was higher among patients with psychiatric symptoms, such as depression, anxiety, and stress. This finding is consistent with findings presented in studies by Luyster et al, Denic-Roberts et al, and Yücel et al.32,33,42 This study has some limitations. First, the sleep quality was subjectively assessed using the PSQI. Apart from its acceptance as a standardized tool, it is not an objective measure like polysomnography. Second, a cross-sectional design can only suggest an association. Finally, the study lacks a healthy, nondiabetic control group to assess direct comparison.
Conclusion
Poor sleep quality among diabetic patients is a prevalent health problem. Several factors can affect sleep quality. Based on the study findings, it is important for health care providers to detect and manage sleep problems in patients with diabetes as a part of their routine management, especially in patients who are female, illiterate, having diabetes for >10 years, having at least one diabetes complication, or comorbid condition, in order to prevent the effects of poor sleep quality.
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
Acknowledgments
We would like to thank all of the study participants and the research team who participated in the study for their excellent cooperation. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization. Global Report on Diabetes. Geneva: World Health Organization; 2016. Available from: http://apps.who.int/iris/bitstream/10665/204871/1/9789241565257_eng.pdf. Accessed February 18, 2018. | ||
Al-Rubeaan K, Al-Manaa HA, Khoja TA, et al. Epidemiology of abnormal glucose metabolism in a country facing its epidemic: SAUDI-DM study. J Diabetes. 2015;7(5):622–632. | ||
Alqurashi KA, Aljabri KS, Bokhari SA. Prevalence of diabetes mellitus in a Saudi community. Ann Saudi Med. 2011;31(1):19–23. | ||
Bae CJ, Schaefer NF. Normal human sleep. In: Carney PR, Berry RB, Geyer JD, editors. Clinical Sleep Disorders, 18th ed. Philadelphia: Lippincott, Williams & Wilkins; 2005:29–37. | ||
Roehrs T. Sleep physiology and pathophysiology. Clin Cornerstone. 2000;2(5):1–12. | ||
Altevogt BM, Colten HR, editors. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem. Washington, DC: National Academies Press; 2006. | ||
Krystal AD, Edinger JD. Measuring sleep quality. Sleep Med. 2008;9(Suppl 1):S10–S17. | ||
Sokwalla SM, Joshi MD, Amayo EO, et al. Quality of sleep and risk for obstructive sleep apnoea in ambulant individuals with type 2 diabetes mellitus at a tertiary referral hospital in Kenya: a cross-sectional, comparative study. BMC Endocr Disord. 2017;17(1):7. | ||
Lou P, Qin Y, Zhang P, et al. Association of sleep quality and quality of life in type 2 diabetes mellitus: a cross-sectional study in China. Diabetes Res Clin Pract. 2015;107(1):69–76. | ||
Knutson KL, Ryden AM, Mander BA, van Cauter E. Role of sleep duration and quality in the risk and severity of type 2 diabetes mellitus. Arch Intern Med. 2006;166(16):1768–1774. | ||
Nefs G, Donga E, van Someren E, et al. Subjective sleep impairment in adults with type 1 or type 2 diabetes: Results from Diabetes MILES – The Netherlands. Diabetes Res Clin Pract. 2015;109(3):466–475. | ||
Suhaym AA, Assiri H, Alhazzani A, et al. Impact of diabetes on sleep disorders and sleep quality (p4. 286). Neurology. 2016; 86(Suppl 16):4–286. | ||
Alqurayn A, Abdrabalnabi A, Aljasim M, et al. Sleep quality assessment in Saudi patients with type 2 diabetes from National Guard Primary Healthcare Centers: a cross-sectional study. Int J Med Res Prof. 2017;3(5):328–334. | ||
Balkin TJ, Rupp T, Picchioni D, Wesensten NJ. Sleep loss and sleepiness: current issues. Chest. 2008;134(3):653–660. | ||
Strøm-Tejsen P, Zukowska D, Wargocki P, Wyon DP. The effects of bedroom air quality on sleep and next-day performance. Indoor Air. 2016;26(5):679–686. | ||
Filtness AJ, Armstrong KA, Watson A, Smith SS. Sleep-related vehicle crashes on low speed roads. Accid Anal Prev. 2017;99(Pt A):279–286. | ||
Alvarez GG, Ayas NT. The impact of daily sleep duration on health: a review of the literature. Prog Cardiovasc Nurs. 2004;19(2):56–59. | ||
Irwin MR, Wang M, Ribeiro D, et al. Sleep loss activates cellular inflammatory signaling. Biol Psychiatry. 2008;64(6):538–540. | ||
Chasens ER, Sereika SM, Burke LE, Strollo PJ, Korytkowski M. Sleep, health-related quality of life, and functional outcomes in adults with diabetes. Appl Nurs Res. 2014;27(4):237–241. | ||
Tang Y, Meng L, Li D, et al. Interaction of sleep quality and sleep duration on glycemic control in patients with type 2 diabetes mellitus. Chin Med J. 2014;127(20):3543–3547. | ||
Osonoi Y, Mita T, Osonoi T, Saito M, et al. Poor sleep quality is associated with increased arterial stiffness in Japanese patients with type 2 diabetes mellitus. BMC Endocr Disord. 2015;15(1):29. | ||
Zhang J, Zhang L, Guo L. The relationship between sleep quality and diabetic autonomic neuropathy in elder patients with type 2 diabetes mellitus. Zhonghua Nei Ke Za Zhi. 2016;55(3):196–201. | ||
Jee D, Keum N, Kang S, Arroyo JG. Sleep and diabetic retinopathy. Acta Ophthalmol. 2017;95(1):41–47. | ||
Ohkuma T, Fujii H, Iwase M, et al. Association between sleep duration and urinary albumin excretion in patients with type 2 diabetes: the Fukuoka diabetes registry. PLoS One. 2013;8(11):e78968. | ||
Seligowski AV, Pless Kaiser AP, Niles BL, et al. Sleep quality as a potential mediator between psychological distress and diabetes quality of life in veterans with type 2 diabetes. J Clin Psychol. 2013;69(10):1121–1131. | ||
Swanson W, Cohen J. Color vision. Ophthalmol Clin North Am. 2003;16(2):179–203. | ||
Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. | ||
Almadi T. The Role of Work Stress in the Development of Metabolic Syndrome Among Jordanians [PhD thesis]. NSW: University of Sydney; 2014. | ||
Armstrong T, Bull F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J Public Health. 2006;14(2):66–70. | ||
Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335–343. | ||
Cunha MC, Zanetti ML, Hass VJ. Sleep quality in type 2 diabetics. Rev Lat Am Enfermagem. 2008;16(5):850–855. | ||
Luyster FS, Dunbar-Jacob J. Sleep quality and quality of life in adults with type 2 diabetes. Diabetes Educ. 2011;37(3):347–355. | ||
Yücel S¸Ç, Güler EK, Ak I. Investigation of sleep quality, quality of life, anxiety and depression in patients with diabetes mellitus. Int J Diabetes Dev Ctries. 2015;35(1):39–46. | ||
Colbay G, Cetin M, Colbay M, Berker D, Guler S. Type 2 diabetes affects sleep quality by disrupting the respiratory function. J Diabetes. 2015;7(5):664–671. | ||
Fetveit A. Late-life insomnia: a review. Geriatr Gerontol Int. 2009;9(3):220–234. | ||
Drake C, Roehrs T, Shambroom J, Roth T. Caffeine effects on sleep taken 0, 3, or 6 hours before going to bed. J Clin Sleep Med. 2013;9(11):1195. | ||
Alshenghiti AM, Alsadran FF, Alzahrani RA, et al. Sleep quality among type 2 Saudi diabetics. Med J Cairo Univ. 2016:167–171. | ||
Zhang L, Samet J, Caffo B, Punjabi NM. Cigarette smoking and nocturnal sleep architecture. Am J Epidemiol. 2006;164(6):529–537. | ||
Nakajima M, Dokam A, Kasim AN, et al. Habitual khat and concurrent khat and tobacco use are associated with subjective sleep quality. Prev Chronic Dis. 2014;11:E86. | ||
Lemma S, Patel SV, Tarekegn YA, et al. The epidemiology of sleep quality, sleep patterns, consumption of caffeinated beverages, and khat use among Ethiopian college students. Sleep Disord. 2012;2012:1–11. | ||
Fritz T, Caidahl K, Osler M, et al. Effects of Nordic walking on health-related quality of life in overweight individuals with type 2 diabetes mellitus, impaired or normal glucose tolerance. Diabet Med. 2011;28(11):1362–1372. | ||
Denic-Roberts H, Costacou T, Orchard TJ. Subjective sleep disturbances and glycemic control in adults with long-standing type 1 diabetes. Diabetes Res Clin Pract. 2016;119:1–2. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.