")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Assessment of Serum Vitamin B12 and Folate Levels and Macrocytosis in Patients with Type 2 Diabetes Mellitus on Metformin Attending Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia: A Cross-Sectional Study
Authors Wale Tesega W , Genet S , Natesan G , Tarekegn G , Girma F, Chalchisa D, Belay Y, Geto Z , Asmamaw Dejenie T
Received 12 February 2021
Accepted for publication 9 April 2021
Published 3 May 2021 Volume 2021:14 Pages 2011—2018
DOI https://doi.org/10.2147/DMSO.S306433
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Wondwossen Wale Tesega, 1 Solomon Genet, 2 Gnanasekaran Natesan, 2 Getahun Tarekegn, 2 Fitsum Girma, 3 Dinkinesh Chalchisa, 3 Yohannes Belay, 3 Zeleke Geto, 4 Tadesse Asmamaw Dejenie 5
1Department of Biomedical Sciences, School of Medicine, College of Health Sciences, Arbaminch University, Arba Minch, Ethiopia; 2Department of Medical Biochemistry, School of Medicine, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 3National Reference Laboratory for Immunohematology, Ethiopian Public Health Institute, Addis Ababa, Ethiopia; 4Department of Biomedical Science, College of Medicine and Health Science, Wollo University, Dessie, Ethiopia; 5Department of Biochemistry, School of Medicine, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Correspondence: Tadesse Asmamaw Dejenie Tel +251 90-904-5760
Email [email protected]
Background: Metformin is the first-line drug in the treatment of type 2 diabetes mellitus. Monitoring vitamin B 12 deficiency associated with long-term and high-dose therapy is not a common practice in many clinical settings in Ethiopia.
Objective: The study aimed to measure levels of serum vitamin B 12 and folate and to assess the macrocytic status of type 2 diabetes mellitus patients on metformin.
Methods: A cross-sectional study was conducted on 80 type 2 diabetes mellitus patients who had been on metformin for 5 months or more at the diabetic clinic of Tikur Anbessa Specialized Teaching Hospital. Serum vitamin B 12 and folate levels were quantified by chemiluminescent immunoassays. Mean corpuscular volume was determined by complete blood count. Differences in vitamin B 12 and folate levels and mean corpuscular volume between different groups were assessed using Kruskal–Wallis H and Mann–Whitney U tests.
Results: Vitamin B 12 and folate deficiency were documented in 5% and 23.8% of participants, respectively, and 6.2% of patients were macrocytic. Levels of vitamin B 12 and folate in patients who had been on metformin > 1,500 mg/day ≥ 4 years were significantly lower those who had been on metformin 1,000– 1,500 mg/day and < 1,000 mg/day < 4 years, respectively.
Conclusion: Low serum vitamin B 12 and folate levels and macrocytosis were found to be associated with prolonged metformin treatment.
Keywords: macrocytosis, metformin, type 2 diabetes mellitus, vitamin B 12, folate
Background
Metformin has been used widely in the treatment of type 2 diabetes for decades.1,2 The exact mechanism of metformin action has only been partially explored and remains controversial. However, it has been found that the glucose-lowering effect of metformin is mainly due to the inhibition of hepatic glucose output.
Various guidelines advocate the use of metformin as the first-line glucose-lowering agent concurrently with lifestyle-modification approaches if there are no contraindications like renal and hepatic dysfunction.3,4,4 For example, the American Diabetes Association and American Association of Clinical Endocrinologists recommend the use of metformin as first-line treatment for type 2 diabetes mellitus and prediabetes to prevent progression of the disease. It has been reported that metformin is a pharmacological cause of vitamin B deficiencies in patients with type 2 diabetes mellitus which leads to long-term deleterious neurological and hematological effects.5–7
Vitamin B12 is a water-soluble vitamin that plays a fundamental role in DNA synthesis, optimal hemopoiesis, and neurological function. In the human body, vitamin B12 is converted enzymatically into its two coenzyme forms, methylcobalamin and adenosylcobalamin.8–10 Through its active forms, vitamin B12 exerts its physiological effects through mediating important enzymatic pathways that help keep the body’s nerve and blood cells healthy and helps to make DNA, the genetic material in all cells. The clinical picture of vitamin B12 deficiency is hence predominantly of features of hematological and neurocognitive dysfunction.8
In the mitochondria, for example, propionyl-CoA is enzymatically carboxylated to methylmalonyl-CoA, which is then reversibly isomerized to succinyl-CoA by the B12-dependent enzyme methylmalonyl-CoA mutase. As such, deficiency in vitamin B12 blocks the production of succinyl-CoA and leads to elevated methylmalonic acid, which induces neuron destabilization and consequential neurological deficits.11,12 In the cytoplasm, the methylation of homocysteine to produce methionine uses 5-methyltetrahydrofolate as the methyl donor in a reaction catalyzed by methionine synthase that requires methylcobalamin.10,12 Therefore, vitamin B12 deficiency leads to a condition known as folate trap (functional folate deficiency), where free folate is trapped in the form of methyltetrahydrofolate. Therefore, deficiency in any form of vitamin B12 and folate ultimately affect methionine metabolism to the point where homocysteine can no longer remethylate back to methionine, causing hyperhomocysteinemia.13,14
Many studies have reported that higher doses and prolonged duration of metformin treatment induce vitamin B12 deficiency and consequential complications in type 2 diabetes mellitus patients.5,7,15 This effect is most often seen after the patient has received long-term treatment (ie, ≥6 months) and high doses (ie, >1 g/day) of metformin.7,16
Different proposed mechanisms explain metformin-induced vitamin B12 deficiency among patients with type 2 diabetes mellitus: alterations in small-bowel motility activating bacterial overgrowth, competitive inhibition or inactivation of vitamin B12 absorption, alterations in intrinsic factor (IF) levels, and interaction with the cubulin endocytic receptor.6 Metformin has also been shown to prevent calcium-dependent absorption of the vitamin B12–IF complex at the terminal ileum.17
Even though metformin is a cornerstone in the treatment of type 2 diabetes, many reports and the package insert of metformin advise patients using high doses for a long time to have routine serum vitamin B12 measurements done every 2–3 years besides the hematological assessments recommended to be done on annual basis.18 However, screening type 2 diabetes mellitus patients using high doses for a long time to monitor metformin’s side effects like vitamin B12 deficiency is not a common clinical practice in many clinical settings in Ethiopia. Therefore, this study aimed to measure levels of serum vitamin B12 and folate and assess the macrocytic status of type 2 diabetes mellitus patients on metformin.
Methods
Between October and December 2019, a total of 80 patients with type 2 diabetes mellitus who fulfilled the American Diabetes Association criteria (reported of the expert committee on the diagnosis and classification of diabetes mellitus, 1997), aged 35 to 79 years and who had been on metformin for 5 months and above, were recruited for this cross-sectional study using a convenient sampling method. All patients were from the Diabetic Clinic of Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia.
Exclusion Criteria
Patients with thyroid disease, liver disease, pernicious anemia, active cancer, end-stage renal disease, chronic pancreatitis, Helicobacter pylori infection, or HIV, having undergone gastrectomy or ileal resection, documented diagnosed reason for vitamin B12 malabsorption (alcoholism, atrophic gastritis, celiac disease, Crohn’s disease, gastric banding, or bypass), those on oral/intramuscular vitamin B12 supplements, H2-receptor blockers, proton-pump inhibitors, methotrexate, or chloramphenicol, and vegetarians, pregnant women, alcoholics, and smokers were excluded.
Ethics Approval and Informed Consent
The study adhered to Declaration of Helsinki principles. The study protocol was approved by Addis Ababa University Biochemistry Department Ethics and Research Committee (DRERC). Ethics approval (SOM/BCHM/02/2012) was obtained from the departmental research and ethics review committee of the Department of Medical Biochemistry and College of Health Sciences Institutional Review Board (DRERC). Informed consent was obtained from participants before sample collection. Confidentiality and privacy were assured.
Data and Blood Collection
Sociodemographic, clinical, and therapeutic data related to type 2 diabetes mellitus were collected from participants’ medical history charts and interviews using an Amharic-language structured questionnaire administered by experienced nurses. After subjects had been fasted overnight, 6 mL venous blood was collected from each participant and dispensed into blood collecting tubes with serum separator and EDTA (4 mL for serum separation and 2 mL for complete blood counts). The 4 mL blood samples were allowed to retract and were then centrifuged at 3,000 rpm for 10 minutes to obtain serum samples that were kept at −20°C until analysis for vitamin B12 and folate levels. Complete blood countswere done immediately after collection. Laboratory testing was done at the National References Laboratory for Clinical Chemistry, Ethiopian Public Health Institute.
Determination of Serum Vitamin B12, Folate, and MCV
Biochemical tests for serum vitamin B12 and folate were analyzed and determined with a Cobas 6000 immunoassay analyzer. A UniCelDxH 800 analyzer (Beckman Coulter) was used for hematology testing to determine mean corpuscular volume (MCV). Vitamin B12 deficiency was defined as a serum concentration <197 pg/mL and folate deficiency as serum concentration <4.6 ng/mL. Macrocytosis was defined as MCV <96 fL.
Statistical Analysis
After checking the distribution of vitamin B12, folate, MCV, and other variables for normality using histograms, Mann–Whitney U and Kruskal–Wallis H tests for abnormally distributed data, were used to determine differences in medians (vitamin B12, folate, and MCV). Independent t-tests and one-way ANOVA with Welch tests for normally distributed data were used to determine differences in means of age and BMI. Data with normal distribution are presented as means ± SD, while data with abnormal distribution are presented as medians (IQRs). Spearman’s correlation coefficient was used to measure relationships among variables. P<0.05 was considered statistically significant. SPSS 25 was used to perform all analyses.
Results
Mean participant age was 56.35±10.60 years, of whom 64 (80%) were above the aged >56 years, 57.5% female, and 93.8% resided in an urban setting. Mean daily dose of metformin was 1,200±644.35 mg, with 4 (1–20) yearsthe median duration of metformin intake. There were 43.8% and 28.7% of patients using insulin and glibenclamide, respectively, in addition to metformin. Vitamin B12- and folate-deficient patients numbered four (5%) and 19 (23.8%), respectively, while the other five (6.2%) patients had macrocytosis (Table 1).
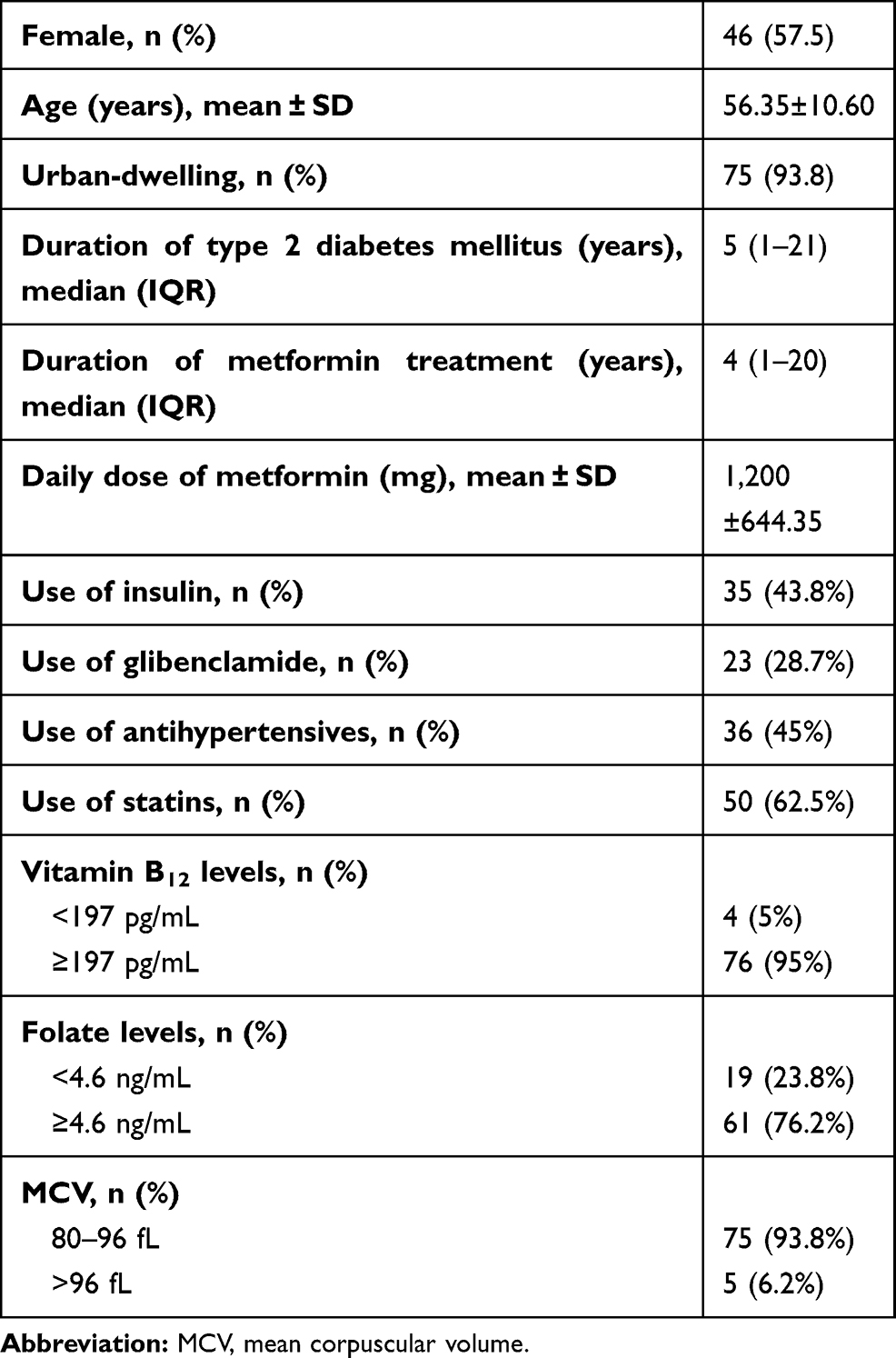 |
Table 1 Demographic and Clinical Characteristics of Participants (n=80) |
In sum, 43 and 16 participants were taking metformin doses <1,000 mg and 1,000–1,500 mg, respectively, but none had developed vitamin B12 deficiency. However, of the 21 who used metformin >1,500 mg, vitamin B12 deficiency was observed in four. This accounted for 5% of 80 participants (Figure 1).
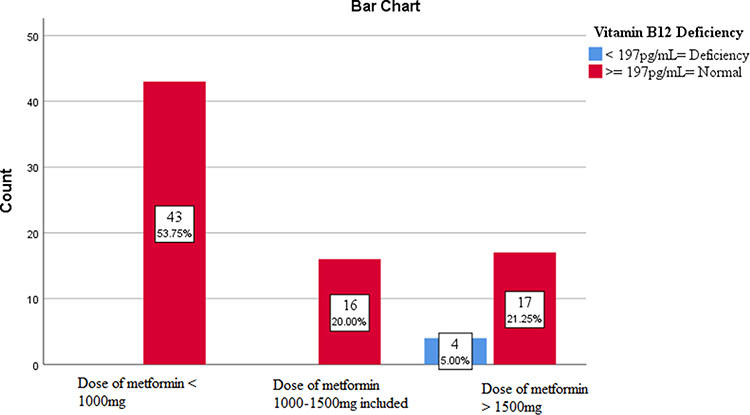 |
Figure 1 Serum vitamin B12 status of selected type 2 diabetes mellitus patients based on daily dose of metformin. |
As depicted in Figure 2, although there were cases of folate deficiency in patients taking metformin <1,000 mg,and 1,000–1,500 mg per day, the highest percentage of folate deficiency was observed in patients on metformin >1,500 mg per day. As the dose increased, the percentage of patients with serum folate levels <4.6 ng/mL increased as well (Figure 2).
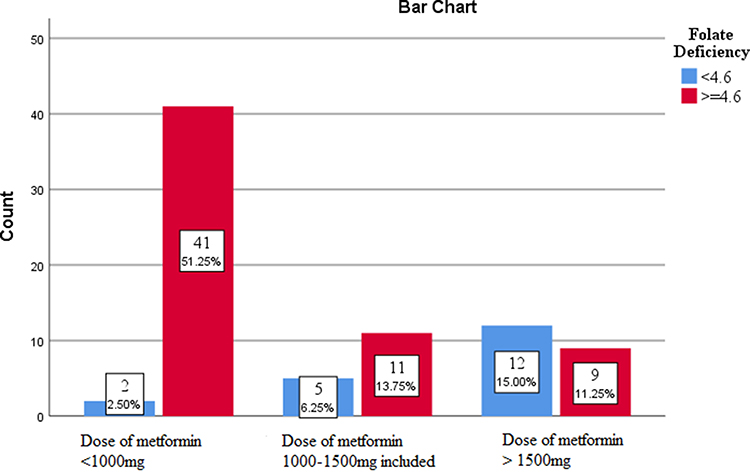 |
Figure 2 Serum folate status of selected type 2 diabetes mellitus patients based on daily dose of metformin. |
Based on metformin intake, patients were divided into two groups: <4 years’ intake and ≥4 years. Four patients who were found to be vitamin B12-deficient had been taking metformin ≥4 years. However, no patients who had been on metformin <4 years experienced vitamin B12 deficiency. Similarly, though there were cases of folate deficiency in patients who had taken metformin <4 years, higher (34.3%) folate deficiency was observed in patients who had been taking metformin ≥4 years (Table 2).
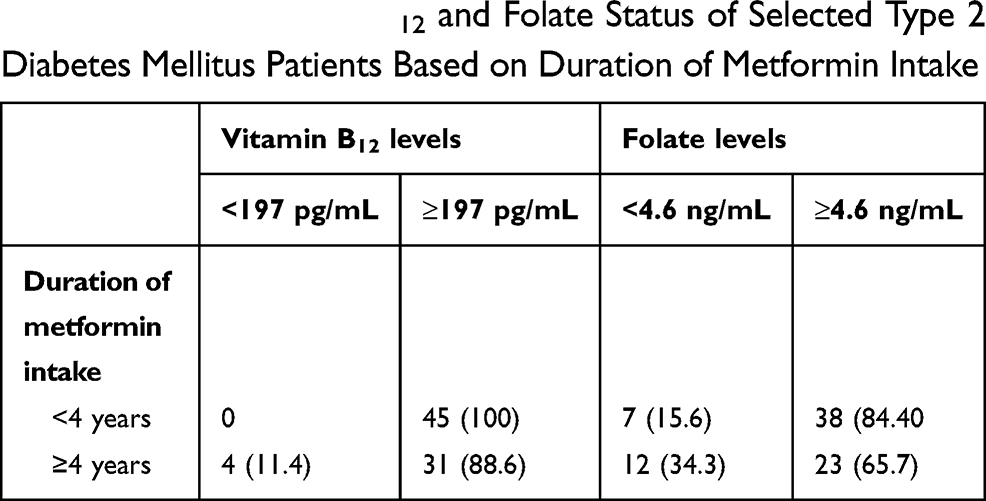 |
Table 2 Serum Vitamin B12 and Folate Status of Selected Type 2 Diabetes Mellitus Patients Based on Duration of Metformin Intake |
Note: Data expressed as n (%)
As shown in Table 3, patients were divided into 3 groups based on daily metformin dose. The median level of vitamin B12 in patients on >1,500 mg/day was significantly lower (P<0.001) than patients on of 1,000–1,500 mg/day and <1,000 mg/day. Those on <1,000 mg/day had the highest median B12. Similarly, median serum folate of patients on >1,500 mg/day was significantly lower than patients on 1,000–1,500 mg/day and <1,000 mg/day (P=0.002). Differences in median MCV with the different daily doses was not statistically significant (P=0.518). Similarly, there was no statistically significant difference in mean BMI or age of patients on different doses (Table 3).
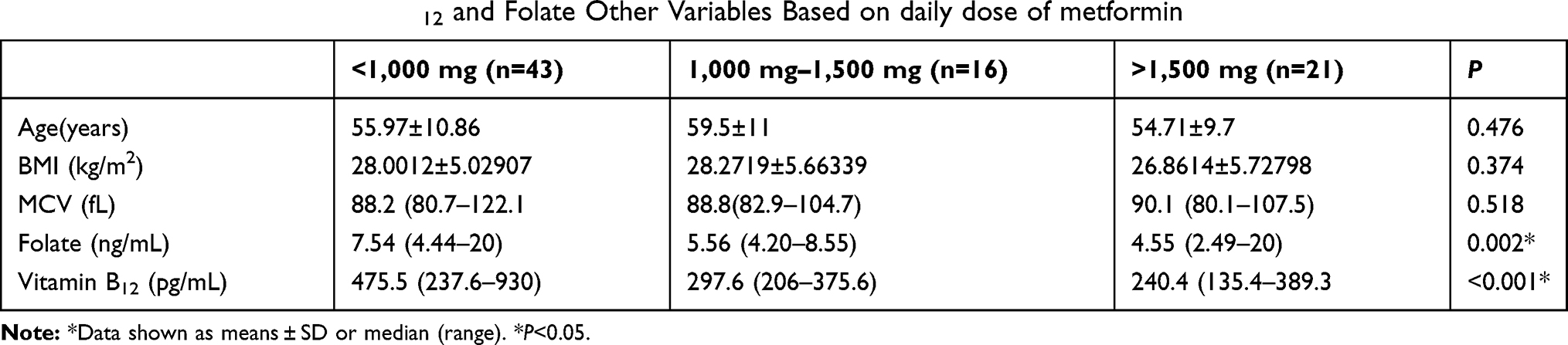 |
Table 3 Serum Levels of Vitamin B12 and Folate Other Variables Based on daily dose of metformin |
Based on duration of metformin intake, patients were again divided into two groups; <4 years and ≥4 years. Patients who had used metformin ≥4 years had significantly lower median vitamin B12 than patients who had used it <4 years (P<0.001). Furthermore, median serum folate of patients who had used metformin <4 years was significantly higher than patients who had used it ≥4 years (P=0 0.01). However, neither MCV (P=0.207) nor BMI (P=0.207) was associated with duration of intake (Table 4).
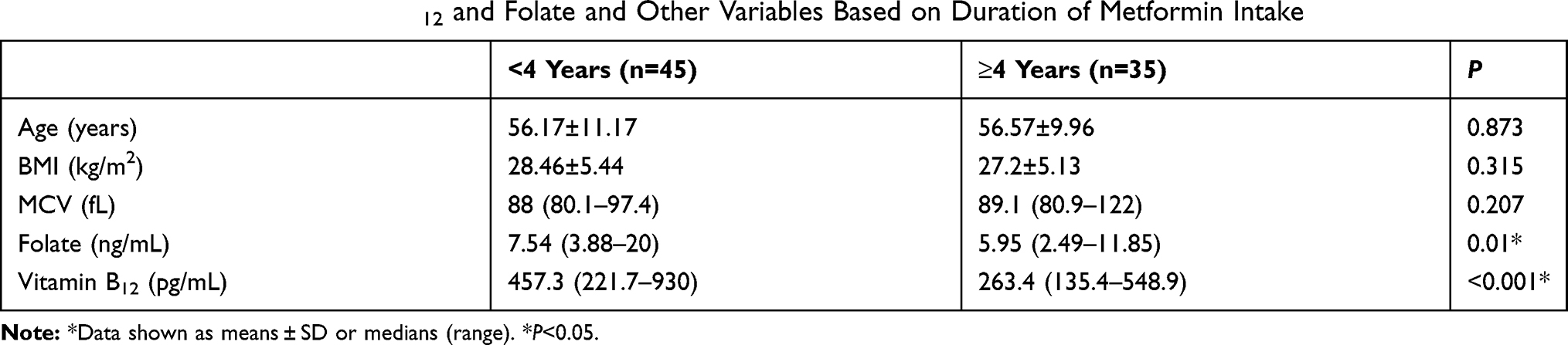 |
Table 4 Serum Levels of Vitamin B12 and Folate and Other Variables Based on Duration of Metformin Intake |
Spearman’s correlation coefficients between variables showed negative correlations between doses (r=−0.324***, P=0.003; r=−0.523***, P=0) and duration (r=−0.313***, P=0.005; r=−0.218***, P=0.052) of use with serum vitamin B12 and folate levels, respectively. MCV values were positively associated with dose and (r=0.036***, P=0.752) and negatively associated with duration of treatment (r=−0.020***, P=0.864).
Discussion
This study was conducted to determine serum vitamin B12 and folate levels and assess macrocytosis in type 2 diabetes mellitus patients on metformin.
Controlled clinical trials of metformin have reported that 7% of patients havesubnormal levels of previously normal serum vitamin B12 without clinical manifestations. As well as the package insert for metformin, research has recommended that patients susceptible to low vitamin B12 should have routine serum vitamin B12 blood tests done every 2–3 years in addition to hematological parameters that are recommended on an annual basis.18 Furthermore, to prevent neurological deterioration rather than treat it once it has begun, it has been suggested that annual monitoring of serum vitamin B12 results in better patient health.5,7,15,16
This study indicated an incidence of vitamin B12 levels below the lower reference limit of 5%, and is thus in concordance with other reports.19–21 This could be due to interference with vitamin B12 absorption from the B12–IF complex as a consequence of prolonged metformin use18 or due to nutritional deficiency.22
The 23.8% incidence of folate deficiency in patients on higher doses and longer metformin use is in line with other studies.15,23 However, comparing the percentage of vitamin B12 and folate deficiencies of this study with the prevalence of vitamin B12 and folate deficiencies in other studies is not straightforward, and several factors should be borne in mind. For example, different techniques are used in determining serum vitamin B12 and folate levels, such as high-performance liquid chromatography vs immunoassay and different cutoff values used for deficiency determination. Furthermore, we did not include type 2 diabetes mellitus patients without metformin intake as a control group, which is among factors that have to be considered when comparing our results and those in the literature.
Many studies have investigated the effect of dose and duration of metformin use on vitamin B12 levels and found that lower of vitamin B12 levels are highly prevalent in patients on higher doses and longer duration of metformin treatment.15,19,23–26 In this study, the smallest value (240 pg/mL) for vitamin B12 was recorded in patients with type 2 diabetes mellitus with daily intake >1,500 mg. This is entirely consistent with previous studies, where lower levels of vitamin B12 were observed in patients on higher doses than control groups.19,25,27 However, this study is inconsistent with Nervo et al,22 where vitamin B12 had no association with the daily dose, but did for duration of use.
In terms of the metformin-treatment duration, as it, lower levels of vitamin B12 in patients on prolonged treatment have been reported by a number of studies.19,24,26 This is entirely consistent with this study, with 457.3 pg/mL vitamin B12 level observed in patients on metformin <4 years and a significant drop to 263.4 pg/mL in those on metformin ≥4 years. However, Chen et al11 did not find any significant association between metformin duration and vitamin B12 deficiency.
Many studies have already concluded that dose and duration of metformin treatment are the most important risk factors of vitamin B12 deficiency in type 2 diabetes mellitus patients. For example, in Ko et al, subjects on metformin >10 years and on >2 g showed about fourfold the risk of vitamin B12 deficiency of those with duration <4 years and on 1 g.25 Similarly, each 1 g daily intake caused a near-threefold increase (OR 2.88, p<0.001) in risk of developing vitamin B12 deficiency. Additionally, metformin treatment ≥3 years more than doubles (OR 2.39, p=0.001) the risk of developing vitamin B12 deficiency according to Ting et al.31 This could explain the lower levels of vitamin B12 in our patients on metformin >4 years and intake >1,500 mg/day than the other group of patients in our study cohort.
The exact pathogenic mechanisms through which high doses of metformin and long duration of treatment cause vitamin B12 deficiency have not been fully elucidated. However, different proposed mechanisms explain metformin-induced vitamin B12 deficiency among patients with type 2 diabetes mellitus: alterations in small-bowel motility, which stimulates bacterial overgrowth and consequential vitamin B12 deficiency, competitive inhibition or inactivation of vitamin B12 absorption, alterations in IF levels, and interaction with the cubulin endocytic receptor, among others.6,10 Metformin has also been shown to inhibit the calcium-dependent absorption of the vitamin B12–IF complex at the terminal ileum. This inhibitory effect is reversed with calcium supplementation.17
According to several cohort and case–control studies, there is a negative causal relationship between dose and duration of metformin treatment and level of vitamin B12.15,23,24,26 This study also revealed a negative cross-sectional relationship between these variables. However, due to its design, it was not quite unequivocal about the direction of causality or relationship, as patients would have had serum vitamin B12 lower than normal even before they had started metformin treatment. Therefore, further carefully designed research is required to be done in Ethiopia to ensure the consistency of our findings with those reported in previous clinical studies.
The folate levels in patients on prolonged and higher dos of metformin in this study are partly consistent with the results reported in other studies.14,23 It has been reported that type 2 diabetes mellitus patients with vitamin B12 deficiency had folate levels decreased from normal.15,23,25 However, our observations could not confirm that low folate levels were due to vitamin B12 deficiency, and how metformin affects folate status has not yet been elucidated. Deficiency in any form of vitamin B12 can be due to different factors, including disease, drug use, and low-vitamin diet, which can lead to a condition known as folate trap (functional folate deficiency), where free folate is trapped in the form of methyltetrahydrofolate.30 This could be a possible reason for type 2 diabetes mellitus patients with vitamin B12 deficiency in our study having serum folate levels below normal. We assessed folate levels in terms of dose and duration of metformin treatment. However, studies on levels of serum folate in relation to dose and duration of metformin treatment are limited and rare. As such, it was difficult to correlate the results of our study, the first of this kind in Ethiopia, with those of previous articles.
The percentage of patients with macrocytosis was in agreement with Ko et al,20 but not with Robert et al27 who did not find any increase in MCV. Studies investigating the association of metformin-related vitamin B12 deficiency with MCV are rare and varied. However, considering the physiological importance of vitamin B12 and folate in the development of red blood cells, probable reasons for the observed higher MCV values in patients on doses of metformin for prolonged duration could be low serum vitamin B12 and folate levels. Though there were few with macrocytosis, this finding should not be ignored, as both vitamin B12 and folate are required substrates for the maturation of blood cells, and deficiencies in them could lead to a classic form of anemia known as megaloblastic anemia.32
In the present study, age did not show any specific pattern as daily dose and was and was insignificantly higher in patients on metformin >4 years. Other studies have shown conflicting results, with some associating age with vitamin B12 deficiency21 while others finding no relationship.17,25 In our study, mean BMI was insignificantly lower in patients on metformin >4 years. In Akinlade et al, patients on metformin for a prolonged duration had mean BMI insignificantly higher than controls.2 On the other hand, in terms of daily dose, BMI did not show a specific pattern of consistency and was not comparable to findings in previous studies. Therefore, a strong unequivocal relationship connecting age, BMI, and metformin-related vitamin B12 deficiency could not be established.
Strengths and Limitations
This first Ethiopian study of this kind has several positive aspects. Firstly, as we assessed the folate levels and macrocytosis in addition to serum vitamin B12 levels, it could serve as a starting point for further investigations. Secondly, it could be used by physicians as a reference to consider the usefulness of monitoring vitamin B12 levels in patients on metformin. This study also has important limitations. Given its cross-sectional design, we were unable to assess time as a factor or hence establish a causal relationship. Age-matched type 2 diabetes mellitus patients not using metformin were not included as a control group. The cohort was also relatively small (80) and there was no age difference among participants. Therefore, to draw clinically significant conclusions, it is recommended that further investigations proceed with larger cohorts, and include biochemical tests for methylmalonic acid and homocysteine levels, considering that these have been identified as better indicators of functional vitamin B12 deficiency than actual serum vitamin B12 level itself.33,34
Conclusion
The findings of this study show that low serum vitamin B12 and folate levels were associated with higher doses and a long duration of metformin treatment. Macrocytosis was also observed in patients on prolonged and high-dose metformin use, but with no statistical significance. Therefore, yearly routine monitoring of serum levels of vitamin B112, folate and hematological parameters like MCV and blood film in type 2 diabetes mellitus patients on higher doses and longer duration of metformin treatment are required to monitor the effect of metformin on levels of vitamin B12 and folate and macrocytosis.
Abbreviations
BMI, body-mass index; DRERC, Departmental Research and Ethics Review Committee; EPHI, Ethiopian Public Health Institute; IF, intrinsic factor; MCV, mean corpuscular volume.
Data Sharing Statement
The data sets used during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors contributed to data analysis, drafting, or revising the article, have agreed on the journal to which the article will be submitted, gave final approval to the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was supported both financially and materially by the Ethiopian Public Health Institution (EPHI) in collaboration with Addis Ababa University.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Ahmed MA, Muntingh G, Rheeder P. Vitamin B12 deficiency in metformin-treated type-2 diabetes patients, prevalence and association with peripheral neuropathy. BMC Pharmacol Toxicol. 2016;17(1):44. doi:10.1186/s40360-016-0088-3
2. Akinlade KS, Agbebaku SO, Rahamon SK, et al. vitamin b12 levels in patients with type 2 diabetes mellitus on metformin. Ann Ib Postgrad Med. 2015;13(2):79–83. doi:10.4314/aipm.v13i2
3. Alharbi TJ, Tourkmani AM, Abdelhay O, et al. The association of metformin use with vitamin B12 deficiency and peripheral neuropathy in Saudi individuals with type 2 diabetes mellitus. PLoS One. 2018;13(10):e0204420. doi:10.1371/journal.pone.0204420
4. American Diabetics Association. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetesd. 2019. Diabetes Care. 2019;42(Supplement1):S90–102. doi:10.2337/dc19-S009.
5. Andrès E, Loukili NH, Noel E, et al. Vitamin B12 (cobalamin) deficiency in elderly patients. J Can Med Assoc. 2004;171(3):251–259. doi:10.1503/cmaj.1031155
6. Aroda VR, Edelstein SL, Goldberg RB, et al. Long-term metformin use and vitamin B12 deficiency in the diabetes prevention program outcomes study. J Clin Endocrinol Metab. 2016;101(4):1754–1761. doi:10.1210/jc.2015-3754
7. Aslinia F, Mazza JJ, Yale SH. Megaloblastic anemia and other causes of macrocytosis. Clin Med Res. 2006;4(3):236–241. doi:10.3121/cmr.4.3.236
8. Bailey RL, Carmel R, Green R, et al. Monitoring of vitamin B-12 nutritional status in the United States by using plasma methylmalonic acid and serum vitamin B-12. Am J Clin Nutr. 2011;94(2):552–561. doi:10.3945/ajcn.111.015222
9. Bauman W, Shaw S, Jayatilleke E, et al. Increased intake of calcium reverses vitamin B12 malabsorption induced by metformin. Diabetes Care. 2000;23(9):1227–1231. doi:10.2337/diacare.23.9.1227
10. Black MM. Effects of Vitamin B12 and folate deficiency on brain development in children. Food Nutr Bull. 2008;29(2_suppl1):S126–31. doi:10.1177/15648265080292S117
11. Chen S, Lansdown AJ, Moat SJ, et al. An observational study of the effect of metformin on B12 status and peripheral neuropathy. Br J Diabetes Vasc Dis. 2012;12(4):189–193. doi:10.1177/1474651412454924
12. Day C. ADA-EASD diabetes guidance: individualised treatment of hyperglycaemia. Br J Diabetes Vasc Dis. 2012;12(3):146–151. doi:10.1177/1474651412450477
13. De Jager J, Kooy A, Lehert P, et al. Long term treatment with metformin in patients with type 2 diabetes and risk of vitamin B-12 deficiency: randomised placebo controlled trial. BMJ. 2010;20:340. doi:10.1136/bmj.c2181
14. Faeh D, Chiolero A, Paccaud F. Homocysteine as a risk factor for cardiovascular disease: should we (still) worry about it? Swiss Med Wkly. 2006;136(47–48):745–756. doi:10.4414/smw.2006.11283
15. Food & Drug Administration. Metformin hydrochloride tablets. Food and Drug Adminstration; 2002.
16. Foretz M, Guigas B, Bertrand L, et al. Metformin: from mechanisms of action to therapies. Cell Metab. 2014;20:953–966. doi:10.1016/j.cmet.2014.09.018
17. Green R, Allen LH, Bjørke-Monsen AL, et al. Vitamin B12 deficiency. Nat Rev Dis Prim. 2017;3(1):1–20. doi:10.1038/nrdp.2017.40
18. Iftikhar R, Kamran SM, Qadir A, et al. Prevalence of vitamin B12 deficiency in patients of type 2 diabetes mellitus on metformin: a case control study from Pakistan. Pan Afr Med J. 2013;16(1). doi:10.11604/pamj.2013.16.67.2800
19. Kalra DK. Homocysteine and cardiovascular disease. Curr Atheroscler Rep. 2004;6(2):101–106. doi:10.1007/s11883-004-0097-3
20. Ko SH, Ko SH, Ahn YB, et al. Association of vitamin B12 deficiency and metformin use in patients with type 2 diabetes. J Korean Med Sci. 2014;29(7):965–972. doi:10.3346/jkms.2014.29.7.965
21. Liu KW, Dai LK, Jean W. Metformin-related vitamin B12 deficiency. Age Ageing. 2006;35(2):200–201. doi:10.1093/ageing/afj042
22. Nervo M, Lubini A, Raimundo FV, et al. Vitamin B12 in metformin-treated diabetic patients: a cross-sectional study in Brazil. Rev Assoc Med Bras. 2011;57(1):46–49. doi:10.1590/s0104-42302011000100015
23. Obeid R, Jung J, Falk J, et al. Serum vitamin B12 not reflecting vitamin B12 status in patients with type 2 diabetes. Biochimie. 2013;95(5):1056–1061. doi:10.1016/j.biochi.2012.10.028
24. Owhin SO, Adaja TM, Fasipe OJ, et al. Prevalence of vitamin B 12 deficiency among metformin-treated type 2 diabetic patients in a tertiary institution, South-South Nigeria. SAGE Open Med. 2019;(7):1–8. doi:10.1177/2050312119853433
25. Pawlak R, Parrott SJ, Raj S, et al. D. How prevalent is vitamin B12 deficiency among vegetarians? Nutr Rev. 2013;71(2):110–117. doi:10.1111/nure.12001
26. Pflipsen MC, Oh RC, Saguil A, et al. The prevalence of vitamin B12 deficiency in patients with type 2 diabetes: a cross-sectional study. J Am Board Fam Med. 2009;22(5):528–534. doi:10.3122/jabfm.2009.05.090044
27. Robert CO, Brown DL. Vitamin B12 deficiency. Am Fam Physician. 2003;67(5):979–986. doi:10.29309/tpmj/18.4438
28. Rush EC, Katre P, Yajnik CS. Vitamin B12: one carbon metabolism, fetal growth and programming for chronic disease. Eur J Clin Nutr. 2014;68(1):2–7. doi:10.1038/ejcn.2013.232
29. Shane B. Folate and vitamin B12, metabolism: overview and interaction with riboflavin, vitamin B6, and polymorphisms. Food Nutr Bull. 2008;29(2_suppl1):S5–16. doi:10.1177/15648265080292s103
30. Song R. Mechanism of metformin: a tale of two sites. Diabetes Care. 2016;39(2):187–189. doi:10.2337/dci15-0013.
31. Ting R, Szeto C, Chan M, et al. Risk factors of vitamin B12 deficiency in patients receiving metformin. Arch Intern Med. 2006;166(18):1975–1979. doi:10.1001/archinte.166.18.1975.
32. Wile DJ, Toth C. Association of metformin, elevated homocysteine, andmethylmalonic acid levels and clinically worsened diabetic peripheral neuropathy. Diabetes Care. 2010;33(1):156–161. doi:10.2337/dc09-0606.
33. Wulffelé MG, Kooy A, Lehert P, et al. Effects of short-term treatment with metformin on serum concentrations of homocysteine, folate and vitamin B12 in type 2 diabetes mellitus: a randomized, placebo-controlled trial. J Intern Med. 2003;254(5):455–463. doi:10.1046/j.1365-2796.2003.01213.x.
34. Zalaket J, Wehbe T, Abou Jaoude E. Vitamin B12 deficiency in diabetic subjects taking metformin: a cross sectional study in a Lebanese cohort. J Nutr Intermed Metab. 2018;11:9–13. doi:10.1016/j.jnim.2017.12.001
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.