")
Back to Journals » Patient Preference and Adherence » Volume 8
Assessment of selected quality fields of nursing care in neurosurgical wards: a prospective study of 530 people – multicenter studies
Authors Ślusarz R, Biercewicz M, Barczykowska E, Haor B , Głowacka M
Received 9 May 2014
Accepted for publication 24 June 2014
Published 21 August 2014 Volume 2014:8 Pages 1113—1121
DOI https://doi.org/10.2147/PPA.S67437
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Robert Ślusarz,1 Monika Biercewicz,2 Ewa Barczykowska,3 Beata Haor,4 Mariola Głowacka5
1Neurological and Neurosurgical Nursing Department, Collegium Medicum, Nicolaus Copernicus University, Bydgoszcz, 2Clinic of Geriatrics, 3Nursing Department, Collegium Medicum, Nicolaus Copernicus University, Torun, 4Faculty of Health Science, University of Humanities and Economics in Wloclawek, Wloclawek, 5Institute of Health Sciences, State School of Higher Professional Education in Plock, Plock, Poland
Background: One of the elements influencing the assessment of nursing care quality is the assessment of the nurse’s functions that determine the nurse’s particular tasks. The aim of this work was to assess selected tasks involved in the nurse’s caring function, which influence nursing care quality on neurosurgical wards, on the basis of patients’ and nursing staff’s opinions.
Materials and methods: The research was carried out on neurosurgical wards in Poland on a group of 455 patients and 75 nurses. In order to assess nursing care quality, an author’s original questionnaire (Questionnaire – Patient Satisfaction) was used.
Results: Statistically significant differences concerned particular groups (both patients and nurses) in the assessment of selected issues: providing information about performed activities and operations (P=0.000 and P=0.040), respecting personal dignity and assuring discretion during the operations (P=0.000 and P=0.001), speed of response to patient’s requests (P=0.000 and P=0.000), time availability of nurses for the patient (P=0.000 and P=0.000), providing information about further self-care at home (P=0.032, P=0.008), and nurses’ attitude (kindness, courtesy, tenderness, care) to patients (patient’s assessment only P=0.000).
Conclusion: Selected tasks in the field of the caring function of nurses were assessed differently by particular groups. There were no statistically significant differences in the assessment of particular tasks in the opinions of patients and nurses, which means that both examined groups similarly assessed tasks involved in the nurse’s caring function, which influence nursing care quality.
Keywords: care quality, caring function, nurse, neurosurgery
A Letter to the Editor has been received and published for this article.
Introduction
It is very difficult to define the term “quality”, especially with respect to medical care. Treatment results alone should not be the only criterion when quality is discussed, because the whole treatment process and overall atmosphere in which health services are provided are equally important as the outcome.
In recent years in Poland, quality in health care has been getting more and more important, due to changes in the health care system, progress in medicine, and the development of new technologies. Although one of the measurable and very important results of introducing quality-improvement programs is obtaining International Organization for Standardization accreditation, the most important reason for which quality must be improved every day is ensuring professional care at the highest level, adjusted to patients’ needs and desires.
Potential beneficiaries of medical services (patients) contribute to the contemporary market of those services through expressing their opinions and expectations. This makes health care providers adjust their services to patients’ needs, which seems to be a must in modern times.1 This situation, related to a holistic approach toward patients, which prevails among medical professionals, raised patients’ awareness of responsibilities of health care institutions.
The term “medical service quality” first appeared at the beginning of the twentieth century in the US.2–6 It is defined in many ways, eg, “quality in medical service means satisfactory ways to meet patients’ needs and expectations with a low usage of resources”, or “the degree of perfection of actions with relation to the knowledge level and technology development”, or “the extent to which medical services for individual patients, as well as for the population, being in accordance with current knowledge, increase the possibility of achieving desired medical results”.7 Despite the problems with finding one definition, a growth of scientific interest in this phenomenon is being observed.
In the literature, there are many articles related to care quality; however, it is difficult to find an article concerning care quality in neurosurgery. Therefore, this field should be investigated by researchers, and might result in introducing measurement methods in all medical services.
Health services (procedures) provided by neurosurgical wards should be analyzed along with the following aspects: the time devoted to the patient, patience, doctors’ knowledge about the patient’s medical history, respecting personal dignity, kindness, understanding patients and their families, and ward regulations.1,8,9 These aspects are particularly important on neurosurgical wards, where disturbances of the patient’s cognitive processes, mobility, and consciousness determine the whole therapeutic process and quality of health services.
There are four functions of nursing suggested by World Health Organization experts, thanks to which the main roles and tasks of nursing care can be determined. Among those functions, there is a caring function, considered as one of the leading functions when it comes to the job of a nurse. A classic definition of a caring function of a nurse involves complex tasks referring to: 1) helping, accompanying, assisting, and supporting a patient in finding the solution for their health problems, 2) the recognition of the patient’s need for care, 3) helping to solve the problems of biological, psychological, and social nature that may occur as the result of the individual patient’s reaction to the methods of diagnosis, treatment, or rehabilitation, 4) supporting a patient facing current or potential health problems, and helping them to accept to live with an illness or physical or mental impairment. The range of the tasks of caring function results from the common definition of care accepted by the International Council of Nurses, which defines “care” as to be of assistance for an unhealthy or healthy person in doing the activities that serve to keep him/her in a healthy condition, to recover, or to ensure a peaceful death: all of the things that a person would be able to do on his/her own, if he/she had indispensable energy, will, or knowledge.10 The care function also involves time availability for the patients, providing information about nursing procedures, respecting patients’ dignity, and ensuring discretion during operations, etc. Undoubtedly, the chosen areas of nurses’ activity resulting from the care function have an influence on care quality.
A recent project done in 12 countries of Europe (RN4Cast [Registered Nurse Forecasting]) referred to the issue of patients’ safety, satisfaction, and the quality of care in the assessment of nurses and patients. The aim of the study was to find out whether a proper organization of hospital care (the increase of employment and improvement of nurses’ work environment) can influence the quality of care of a patient and the stability of employment in European countries. It was concluded that a deficit in care quality occurs in every country. It was also assumed that the improvement of the working environment in hospitals may be a relatively inexpensive strategy to improve the safety and quality of hospital care and to increase patients’ satisfaction.11
One of the latest findings (May 2014), also in the framework of RN4Cast project, referred to the assessment of the difference in the number of patients per nurse, nurses’ qualifications, and the death rate among hospital patients who had undergone surgical procedures in nine of 12 European countries. It was concluded that increased level of employment of nurses and higher levels of nurse education can considerably lower the death rate of surgical patients in European hospitals. The reduction of nursing staff and the low level of education can worsen the quality of care and can have an adverse effect on patient results.12
The aim of this study was to assess the selected areas of nursing care in neurosurgical wards of Kujawy and Pomorze Voivodeship on the basis of the opinions of patients and nursing staff. Selected roles of the caring function of a nurse were assessed, such as informing patients about performed activities and operations, respecting personal dignity and ensuring discretion during the operations, speed of reaction to patient requests, time availability of nurses for the patient, providing information about further self-care at home, and nurses’ attitude (kindness, courtesy, tenderness, and care) to patients. The detailed aims of the study were presented as the following research problems:
- How do patients assess the selected tasks of caring function that influence care quality?
- Are there any differences between patients’ assessment and nurses’ self-assessment of selected occupational tasks influencing care quality?
Materials and methods
Study design
The results presented in this article are from a multicenter medical service-quality project executed by four university medical centers in Poland: 1) the Neurological and Neurosurgical Nursing Department, Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University in Toruń, 2) the Department of Neurological and Psychiatric Nursing, Medical University of Gdansk, 3) the Department of Neuroscience, Wrocław Medical University, and 4) the Department of Nursing Development, Medical University of Lublin. Currently (2010–2013), the research is being carried out within the scope of statutory activity of the Neurological and Neurosurgical Nursing Department of Collegium Medicum, Nicolaus Copernicus University in Toruń.
Data collection
The data for analysis were gathered in a research project carried out in five neurosurgical wards of Kujawy and Pomorze Voivodeship: the Neurosurgery and Neurotraumatology Department of University Hospital 2 in Bydgoszcz, the Neurosurgery Clinic of University Hospital 1 in Bydgoszcz, the Neurosurgery and Head Surgery Clinic of the Tenth Military Clinical Hospital in Bydgoszcz, the Neurosurgery Department of the Regional Specialist Hospital in Grudziądz, and the Neurosurgery Department of the Provincial Hospital in Włocławek.
For the purpose of this study, the aforementioned wards were marked as I, II, III, IV, and V, respectively, where I, II, and III are the units of clinical hospitals in Bydgoszcz and IV and V are the units of specialist hospitals outside Bydgoszcz. The research involved 455 patients hospitalized in the aforementioned wards and 75 nurses (male and female) employed in these wards. The sociodemographic characteristics of both groups are presented in Table 1.
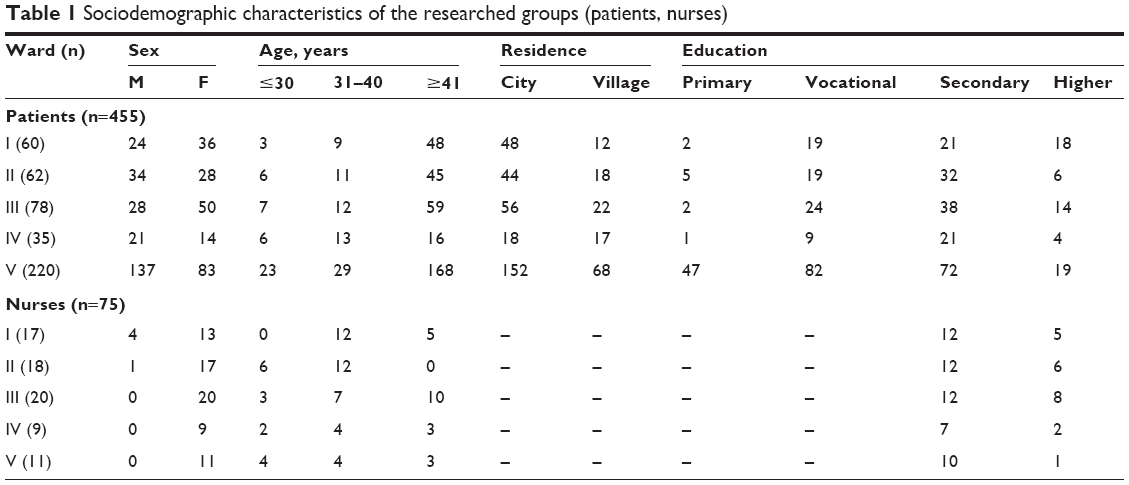 | Table 1 Sociodemographic characteristics of the researched groups (patients, nurses) |
Instrument
The research was conducted by means of a diagnostic survey with the use of a questionnaire answered by the patients on the day of discharge from hospital (ward) after the treatment was completed. The respondents’ answers to the questionnaire questions reflected their opinions. The questionnaire forms were available from the nursing station; the respondents were asked to complete and return them to a special box.
In the study, the anonymous Questionnaire – Patient Satisfaction (QPS) was used (Table 2). A similarly constructed questionnaire was answered by group one (patients) and group two (nurses), in order to collect responses to the same or similar questions from the two independent groups. The questionnaire was prepared on the basis of standard methods and tools used for the assessment of the quality of service and care. The assumptions of ServQual and ServPerf13–15 appeared to be useful, because of their assessment of the service quality with the distinction of its main attributes. The other materials used were: Newcastle Satisfaction with Nursing Scale,16,17 the Patient Satisfaction with Nursing Care Quality Questionnaire,18,19 and a questionnaire of patient’s satisfaction proposed by Lenartowicz.20 QPS is a tool for a subjective assessment of a particular issue, with no universal answer key. The numeric value assigned to each question reflects the patient’s subjective judgment, defined as either good or bad. To assess the particular questions in the QPS, a Likert scale was used, where points 1 and 2 reflected negative statements, point 3 neutral judgment, and points 4 and 5 positive statements. The respondents could mark their opinions from 5 (very good) to 1 (very bad).
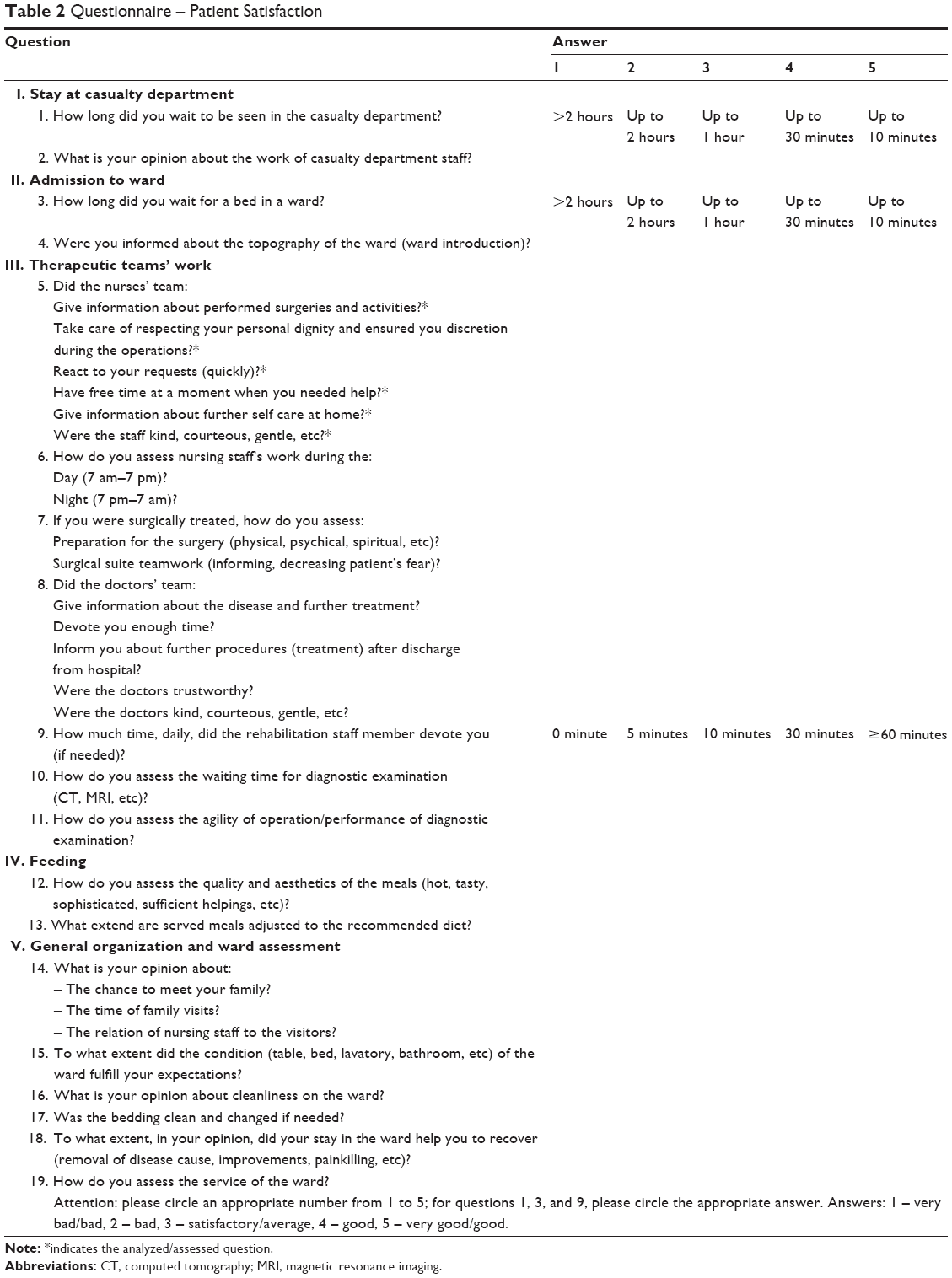 | Table 2 Questionnaire – Patient Satisfaction |
The QPS satisfies psychometric criteria in terms of reliability (internal consistency, Cronbach’s α=0.96) and validity (correlation coefficients ranged between 0.79 and 1.00), and may be applied for evaluation of the level of patient satisfaction with nursing care in hospital neurosurgical wards. The QPS consists of 19 questions, covering five areas that have an influence on medical service quality: area I, stay at casualty department (two questions); area II, ward admission (two questions); area III, therapeutic teamwork (seven questions); area IV, feeding (two questions); and area V, general organization and assessment of the ward (six questions) (Table 2). The opinions of patients and nurses about selected aspects of therapeutic teams’ work were analyzed in the study (area III, six questions marked with asterisks) (Table 2).
Ethical approval
To conduct the study, the consent of the Bioethics Commission at Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University in Toruń was obtained (KB42/2010).
Statistical analysis
Analysis was performed using Statistica 6.0. In a statistical analysis arithmetic mean and standard deviation were used. A statistical rank test – the Kruskal–Wallis H-test – which compares variable distributions in K >2 groups and does not assume distribution normalcy, was also used in the study. When the two groups were compared, the Mann–Whitney U-test was used. This test assesses the differences of one feature between two populations (groups). A significance level of P≤0.05 was accepted.
Results
The participants in the research were hospitalized patients and nurses employed in five different neurosurgical wards in Kuyavian–Pomeranian Voivodeship in Poland. Three of these were neurosurgical wards of clinical hospitals in Bydgoszcz, and two others were neurological wards of specialist hospitals located outside Bydgoszcz in the province. All of those are accredited wards, offering a wide range of neurosurgical treatment options. They also have proper diagnostic and medical facilities. Due to the regionalization rule, most of their patients are from this region; however, if there is a necessity, some patients beyond the region can also be admitted. The amount of nursing staff employed in ward I was 18, in ward II 22, ward III 31, ward IV 11, and ward V 16. The number of beds in particular wards was as follows: ward I, 26 beds; ward II, 45; ward III, 50; ward IV, 23; and ward V, 22 beds. The annual number of hospitalized patients in particular wards was comparable, and reached about 1,100. This amount also resulted from the contract agreement for the provision of medical services. The difference in the number of people taking part in the research resulted from the fact that participation in the research – completing a questionnaire – was voluntary.
Giving information about performer operations and activities
In the patients’ opinions, the best result was achieved by nurses from ward I (average 4.85) while the worst result was achieved by nurses from ward V (average 4.19); the difference here was statistically significant (P=0.000). The nurses’ opinions differed from the patients’ assessment, ie, the highest score (average 4.85) was achieved by nurses from ward III and the lowest (average 4.33) by nurses from ward II (P=0.040). Statistical analysis of both groups’ (patients and nurses) assessment of performed operations and activities showed no statistically significant differences between the groups (P=0.147) (average scores in each group: patients, 4.38; nurses, 4.61) (Table 3).
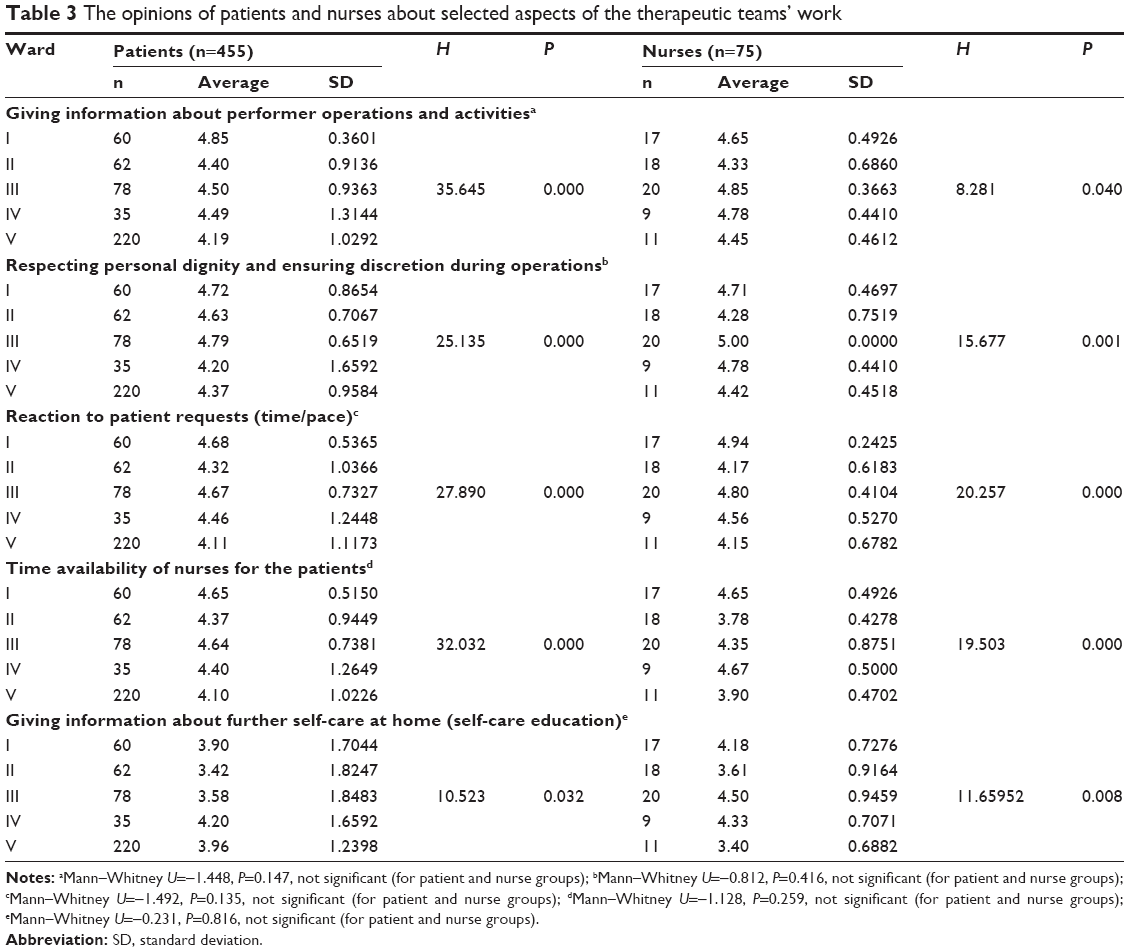 | Table 3 The opinions of patients and nurses about selected aspects of the therapeutic teams’ work |
Respecting personal dignity and ensuring discretion during operations
According to patient assessment, the best result was achieved by nurses from ward III (average 4.79), while the worst result was achieved by nurses from ward IV (average 4.20); the difference here was statistically significant (P=0.000). According to the nurses’ assessment, the highest score (average 5.00) was achieved by nurses from ward III, and the lowest (average 4.28) by nurses from ward II (P=0.001). Statistical analysis of both groups’ (patients and nurses) opinions about respecting personal dignity and ensuring discretion during surgery showed no statistically significant differences (P=0.416) (average scores for groups: patients, 4.51; nurses, 4.63) (Table 3).
Reaction to patients’ requests (time/pace)
According to patient assessment, the best result was achieved by nurses from ward I (average 4.68), while the worst result was achieved by nurses from ward V (average 4.11); the difference here was statistically significant (P=0.000). The nurses’ assessment of nurses was similar: the highest score (average 4.94) was achieved by nurses from ward I, and the lowest score (average 4.15) by nurses from ward V (P=0.000). No statistically significant difference was found between opinions of both groups (patients and nurses) about the speed of reaction to patients’ requests (P=0.135) (average scores for groups: patients, 4.44; nurses, 4.52) (Table 3).
Time availability of nurses for the patients
According to patients, the best result was achieved by nurses from ward I (average 4.65), while the worst was by nurses from ward V (average 4.10); the difference here was statistically significant (P=0.000). The nurses’ assessment of particular wards was different, ie, the highest score (average 4.67) was achieved by nurses from ward IV, and the lowest (average 3.78) by nurses from ward II (P=0.000). No statistically significant difference was found between opinions of both groups (patients and nurses) about time availability of nurses for patients (P=0.259) (average scores for groups: patients, 4.43; nurses, 4.27) (Table 3).
Giving information about further self-care at home (self-care education)
According to patients, the best result was achieved by nurses from ward IV (average 4.20), and the worst by nurses from ward II (average 3.42); the difference here was statistically significant (P=0.032). The nurses’ assessment of particular wards was different, ie, the highest score was achieved by nurses from ward III (average 4.50), and the lowest score (average 3.40) by nurses from ward V (P=0.008). No statistically significant difference was found between opinions of both groups (patients and nurses) about giving information about further self-care at home (P=0.816) (average score for groups: patients, 3.83; nurses, 4.00) (Table 3).
Relation (kindness, courtesy, gentleness, care) of nurses to patients (patients’ opinions)
In the opinion of patients, the best result was achieved by nurses from ward I (average 4.77), and the worst by nurses from ward V (average 4.34); the difference here was statistically significant (P=0.0001). Also, a statistically significant difference (P=0.000) was found between opinions expressed by patients of wards I–III and IV/V (average score in wards I–III was 4.70, and in wards IV and V 4.36) (Table 4).
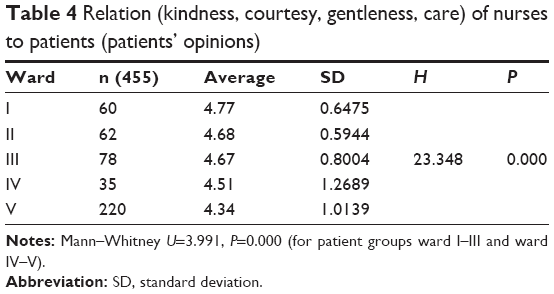 | Table 4 Relation (kindness, courtesy, gentleness, care) of nurses to patients (patients’ opinions) |
Discussion
Polish researchers emphasize the importance of medical and nursing care, which involves not only nursing, therapeutic, and technical procedures, but also interpersonal communication, nurses’ and doctors’ knowledge, and their ability to make decisions. Medical staff, especially nurses, must be aware that their attitude and behavior influence patient’s first impressions, and consequently have an impact on the hospitalized patient’s comfort.21,22
Due to the lack of standardized tools for assessment of care quality and satisfaction in Poland, the current study was based on the authors’ original questionnaire – the QPS. In the majority of research conducted in Poland, the measurement and assessment of patients’ satisfaction with nursing care in hospitals have been performed using authors’ original questionnaires designed for the purpose of a given study or institution.23–25 Between 2010 and 2012, a psychometric validation of the Newcastle Satisfaction with Nursing Scale (NSNS)16,26 was performed in order to adapt it to Polish conditions, but the results were ambiguous and difficult to compare. The authors reported that the level of experience related to nursing care and satisfaction with this care in Polish hospitals assessed with the NSNS varied from satisfactory to very good. Most tools used in Poland for assessment of patients’ satisfaction and care quality have not been verified statistically, and thus their validity and reliability have not been established. Consequently, it is difficult to interpret the results.
Although there are many assessment tools, their structure and assessment areas are similar. The results of the majority of studies indicate that patients are satisfied with the quality of care. Thorne et al27 reported 70%–80% of positive opinions concerning neurosurgical care, but indicated some administrative flaws. Terada et al28 argued that intensive postoperative care on neurosurgical wards had no impact on the overall satisfaction of patients with hospital care. Wasilewski,22 who conducted his study on a neurosurgical ward, proved that psychosocial care related to social support is crucial. Other studies among patients hospitalized for lumbar discopathy indicate the importance of meeting patients’ religious and spiritual needs.29 The results of Graczyk’s study30 showed that patients hospitalized for cervical and lumbar discopathy positively assessed nursing care. Similar assessment of patients’ satisfaction was performed by Sierpińska and Dzirba31: 87% of respondents assessed nurses’ kindness as very good, speed of reaction to patients’ requests was assessed as very good by 78%–83% of the patients, providing information about nursing procedures and postoperative regimens was assessed as very good by 70%, and assistance with maintaining body hygiene was assessed as very good by 76% of the respondents. Similar results were also obtained by Wyrzykowska,32 who performed her study on neurosurgical wards: 53% of patients assessed nursing care as good, 43% as good, 3% as satisfactory, and 1% as bad. Providing information about the purpose and form of nursing procedures was assessed positively by 78% of patients. Also, opinions about nurses’ attitude and level of professionalism were highly positive: 84% positively assessed level of professionalism, and more than 78% of patients appreciated nurses’ kindness and understanding.
Assessment of satisfaction with nursing was performed by Kropornicka et al29 among patients hospitalized for lumbar discopathy. A high percentage of positive responses (over 90%) was obtained for conditions at the hospital, opportunity to meet religious and spiritual needs, and opportunity for contact with close relatives. Overall atmosphere on the ward and attitude of nurses were also assessed very positively. Patients negatively assessed communication with nurses, opportunity to express anxiety and worries about their health, information provided by nurses in the scope of self-care at home (53% of patients were not provided with this information), and healthy lifestyle (36% were not informed); 54% of patients confirmed that nurses did not encourage them to express their thoughts and feelings about their health or anxiety caused by symptoms of their disease.
Palese et al33 studied 1,565 surgical patients from six European countries, and concluded that satisfaction with nursing care was high and ranged between satisfied and very satisfied.
The obtained results show that nurses’ work is assessed on good/very good levels by patients. The research carried out by the Collaborating Centre for Development of Quality and Safety in Health Systems34 showed that all aspects of nurses’ assessment reached nearly 90% positive scores. For patients, the most important aspects are kindness and proper attitude toward them, professional skills, and efficiency in performing surgery operations.
This analysis proves that in contrast to results achieved outside our country,27 the lowest score for nurses was achieved in the area of self-care education, while the highest score was achieved for staff’s kindness. In many publications, this aspect of care is taken into account, because it happens very often that for a patient the presence of a nurse or a doctor and contact with them are much more important than technical operations performed by the staff.32 It was not always possible to comment on the results of the current study in the context of other authors’ results, due to the diversity of tools and methods.
Conclusion
The selected tasks from the area of nurses’ care function, influencing care quality, were assessed in different ways by different groups. Almost all assessed tasks in both groups achieved more than good scores. The highest score, in patients’ opinions, was achieved by the following tasks: respecting personal dignity and ensuring discretion during surgery, speed of reaction for patient requests, and time availability of nurses for the patient. According to nurses’ opinion, the most important tasks were the following: respecting personal dignity and ensuring discretion during surgery, providing information about performed operations and activities, and speed of reaction for patient’s requests.
No statistical differences were found between the groups’ assessments of selected occupational tasks that influence care quality, since both the patients and nurses similarly assessed all these tasks.
Acknowledgments
The authors are grateful to Janice L Hinkle, PhD, RN, CNRN, School of Nursing, Catholic University of America, for assistance and valuable suggestions. This study was supported by the Clinical Nursing Department, Collegium Medicum, Nicolaus Copernicus University (grant 523/2011).
Disclosure
The authors report no conflicts of interest in this work.
References
Małecka B, Marcinkowski JT. [Patient satisfaction as a factor designing modern market of medical services]. Probl Hig Epidemiol. 2007;88:17–19. Polish. | ||
Krapp M. Quality assurance in research and development: an insoluble dilemma? Fresenius J Anal Chem. 2001;371:704–713. | ||
Clarkson P, Challis D. Quality assurance practices in care management: a perspective from the United Kingdom. Care Manag J. 2003;4:142–151. | ||
Stausberg J, Nonnemacher M, Weiland D, Antony G, Neuhäuser M. Management of data quality – development of a computer-mediated guideline. Stud Health Technol Inform. 2006;124:477–482. | ||
Pharow P, Blobel BG, Savastano M. The aspects of safety in future care settings. Stud Health Technol Inform. 2007;127:276–287. | ||
Eckert H, Resch KL. [Quality management – quo vadis? Perspectives for quality management in hospitals]. Z Arztl Fortbild Qualitatssich. 2003;97:219–226. German. | ||
Wójcik M. [Ambulatory cardiac care in the opinion of patients]. 2008. Available from: http://www.statsoft.pl/czytelnia/medyczne/Abulatoryjna_opieka.pdf. Polish. Accessed July 28, 2014. | ||
Prot K, Pałyska M, Anczewska M, Indulska A, Raduj J. Patient satisfaction with community-based psychiatric care. Post Psychiatr Neurol. 2005;14:299–304. | ||
Wroński K, Bocian R. Why national health services establishments should analyse their patient’s satisfaction with the medical services offered? Pieleg Chir i Angiolog. 2009;4:127–130. | ||
Ślusarska B, Zarzycka D, Zahradniczek K. Fundamentals of Nursing. Vol 1. Lublin, Poland: Czelej; 2004. | ||
Aiken LH, Sermeus W, Van den Heede K, et al. Patient safety, satisfaction, and quality of hospital care: cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ. 2012;344:e1717. | ||
Aiken LH, Sloane DM, Bruyneel L, et al. Nurse staffing and education and hospital mortality in nine European countries: a retrospective observational study. Lancet. 2014;383:1824–1830. | ||
Beverly B. The application of SERVQUAL in a district nursing service. 2001. Available from: http://www.jcn.co.uk/journal/05-2001/general/344-the-application-of-servqual-in-a-district-nursing-service. Accessed July 28, 2014. | ||
Parasuraman A, Zeithaml VA, Berry LL. Alternative scales for measuring service quality: a comparative assessment based on psychometric and diagnostic criteria. J Retailing. 1994;70:201–230. | ||
Parasuraman A, Zeithmal VA, Berry L. Conceptual model of service quality and its implications for future research. J Mark. 1985;49:41–50. | ||
Gutysz-Wojnicka A, Dyk D. The adaptation of the Polish version of the Newcastle Satisfaction with Nursing Scale (NSNS). Nurs Top. 2007;2:133–138. | ||
Thomas LH, McColl E, Priest J, Bond S, Boys RJ. Newcastle Satisfaction with Nursing Scale: an instrument for quality assessments of nursing care. Qual Health Care. 1996;5:67–72. | ||
Ksykiewicz-Dorota A, Sierpińska L, Gorczyca R, Rogala-Pawelczyk G. Polish version of Patient Satisfaction with Nursing Care Quality Questionnaire (PSNCQQ). Prog Health Sci. 2011;1:51–56. | ||
Laschinger HS, McGillis Hall L, Pedersen Ch, Almost J. A psychometric analysis of the patient satisfaction with nursing care quality questionnaire: an actionable approach to measuring patient satisfaction. J Nurs Care Qual. 2005;20:220–230. | ||
Lenartowicz H. Quality Management in Nursing. Warsaw: CEM; 1998. | ||
Smolińska A, Marciniak M, Ślusarz R, Królikowska A, Jabłońska R, Książkiewicz B. Satisfaction level of health service on the neurological ward. Udar Mózgu. 2008;10:70–82. | ||
Wasilewski P. A subjective assessment of selected aspects of hospital’s stay satisfaction in surgical departments. Pielęg Chir Angiolog. 2008;3:81–86. | ||
Gaweł G, Twarduś K, Kin-Dąbrowska J, Pyć L. Quality of nursing’s care at cardiologic department. Problemy Pielęgniarstwa. 2008;16:339–342. | ||
Juszczak K, Jaracz K. Quality of nursing care in current research – review literature. Pol Rev Health Sci. 2008;17:321–326. | ||
Żakowska A, Zera A, Krupienicz A. The quality of nursing care in the opinion of patients who have undergone urological and orthopedic anaesthetized by subarachnoid. Przegląd Urologiczny. 2009;55:39–44. | ||
Gutysz-Wojnicka A, Dyk D, Cudak E, Ozga D. Measuring patient satisfaction with the Polish version of the Newcastle Satisfaction with Nursing Scale. Scand J Caring Sci. 2013;27:311–318. | ||
Thorne L, Ellamushi H, Mtandari S, McEvoy AW, Powel Ml, Kitchen ND. Auditing patient experience and satisfaction with neurosurgical care: results of a questionnaire survey. Br J Neurosurg. 2002;16:243–255. | ||
Terada Y, Inoue S, Tanaka Y, Kawaguchi M, Hirai K, Furuya H. The impact of postoperative intensive care on outcomes in elective neurosurgical patients in good physical condition: a single centre propensity case-matched study. Can J Anaesth. 2010;57:1089–1094. | ||
Kropornicka B, Baczewska B, Turowski K. The satisfaction of patients from nursing care during hospitalisation because of lumbar disc disease. 2003. Available from: http://www.neurocentrum.pl/biblioteka/styl_zycia/tom2/spistresci.php. Accessed July 28, 2014. | ||
Garczyk D. Patient’s satisfaction as an expression of quality of nursery care in persons treated surgically due to spinal discopathy in cervical or lumbar vertebral segment. J Neurol Neurosurg Nurs. 2013;2:48–56. | ||
Sierpińska L, Dzirba A. The level of patient satisfaction with nursing care in hospital wards. Pielęg Chir Angiolog. 2011;1:18–22. | ||
Wyrzykowska M. Assessment of nursing care in patients’ opinion. Pielęg Chir Angiolog. 2007;1:3–10. | ||
Palese A, Tomietto M, Suhonen R, et al. Surgical patient satisfaction as an outcome of nurses’ caring behaviors: a descriptive and correlational study in six European countries. J Nurs Scholarsh. 2011;43:341–350. | ||
Cieślik P. Medical personnel in the eyes of patients. Służba Zdrowia. 2001;15:5–8. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.