")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Assessment of Patient Safety Culture Among Doctors, Nurses, and Midwives in a Public Hospital in Afghanistan
Authors Jabarkhil AQ , Tabatabaee SS, Jamali J, Moghri J
Received 18 November 2020
Accepted for publication 4 February 2021
Published 19 March 2021 Volume 2021:14 Pages 1211—1217
DOI https://doi.org/10.2147/RMHP.S292193
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Abdul Qahir Jabarkhil,1,2 Seyed Saeed Tabatabaee,1 Jamshid Jamali,1 Javad Moghri1
1Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran; 2MoPH, Estiqlal Hospital, Kabul, Afghanistan
Correspondence: Javad Moghri
Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
Email [email protected]
Introduction: The first step to improve the safety of patients in hospitals is to evaluate safety culture. Therefore, the patient safety culture in doctors, nurses and midwives should be reviewed regularly. The aim of the study was to determine the current state of patient safety culture among physicians, nurses and midwives at the Estiqlal Hospital in Kabul to promote an effective safety culture.
Methods: This cross-sectional descriptive study was conducted from January to March 2020 among doctors, nurses, and midwives at the Esteqlal Specialized Hospital in Kabul. In that study, the data were collected through a survey of hospital. Among the 267 employees invited to participate, 267 (100%) completed the surveys. Descriptive statistics have been used to adjust frequency distribution tables and inferential statistics to identify differences in variable relationships. The independent sample T-test and one-way ‘ANOVA ‘ were used to check variations between groups, and SPSS version 25 was used for data analysis.
Results: The findings of this study have shown that organizational learning and non-punitive response to errors have had the highest and lowest scores. Eight out of 12 dimensions of patient safety culture scored lower. Four dimensions of patient safety culture scored the highest. Overall, patient safety culture dimensions were low and poor (44%). This means the patient safety culture at the hospital was poor.
Conclusion: The safety culture of the patients at the hospital was inappropriate, particularly in the eight dimensions of the patient safety culture, immediate intervention was necessary. The study emphasizes the creation of a desirable organizational climate, the need for staff involvement in various levels of decision-making, the creation of a culture of error reporting and recognizing the causing factors, and promoting a patient safety culture.
Keywords: patient safety, patient safety culture, medical error, HSOPSC questionnaire
Introduction
One of the most obvious human rights is the right to be safe from hazards and harm when receiving health care. According to the World Health Organization (WHO), quality of care is the delivery of health services to individuals, populations, and patients that enhances the desired outcome.1 Safety in the diagnosis and treatment of patients is one of the priorities of the healthcare system and one of the key elements of the quality of medical services. It means preventing any harm to the patient while providing medical services. The World Health Organisation estimates that because of unsafe medical procedures, millions of patients are victims of accidents and deaths. These harms may include surgery, wrong technique, post-operative complications, misdiagnosis (late diagnosis and non-diagnosis), infections, and bedsores. Approximately two-thirds of adverse events and related disabilities caused by medical mistakes occur in low- and middle-income countries. It is estimated that out of 421 million hospitalizations worldwide every year, about 42.7 million are at risk, with about two-thirds of all events occurring in low- and middle-income countries.2 Every year, a significant number of patients are injured or die as a result of unsafe and inadequate health care. The costs of the wounded and their families are estimated at millions of American dollars. In 2017, under the heading “Making healthcare safer”, the WHO estimated that about 1 in 10 hospitalized patients were injured and that at least 50% of cases were preventable.3 The Institute of Medicine (IOM) released a report in 1999 that “In the United States, between 44,000 and 98,000 people die every year in hospital due to preventable medical errors “. Martin Makary and Michael Daniel at Johns Hopkins University published a report in BMJ 2016, and mentioned the report. “The medical error is the third most commonly reported cause of death in the United States”. The cost of these errors in American hospitals is estimated to be between US$17 and US$19 billion annually. This unsafe health care resulted in “14% of permanent disabilities, 16% of moderate disabilities, 30% of minimum disabilities, and 8% of unexplained incidents”. Studies have also shown that, in all cases of adverse accidents, the patient requires a further nine days to be hospitalized. These unsafe events involved “34% medical errors, 19% diagnostic errors, 18% obstetrical errors, and 9% neonatal procedures”.4 According to the World Health Organization report in 2018 for developing countries (Africa and Eastern Mediterranean), “one-third of patients died from unsafe health care”. In developing countries, about two out of ten patients will be wounded in the hospital. It is also known that procedures and areas of activity are most likely to lead to adverse outcomes: Therapeutic errors (34%), surgical procedure (27%), obstetrics errors (18%), neonatal procedure (8%), and anesthesia (0.5%).5 However, in many countries, the fear of reporting mistakes is manifested in the culture of health care, hindering progress, learning to improve, and preventing mistakes. Across Europe, medical mistakes and health-related events occur in approximately 8–12% of hospitals. It showed that 15% of hospital costs in Europe are attributable to the treatment of safety-related adverse events. Furthermore, adverse events consume almost 15% of total health spending in OECD countries.6 Every year, in Low- and Middle-Income Countries (LMICs), 5.7 to 8.4 million deaths are attributed to poor-quality health care services, accounting for 15% of all deaths. Annually, unsafe medical practices cause around 134 million adverse events in LMICs, of which 2.6 million are lethal.7 In Canada, one in 18 hospital visits leads to avoidable harm. These incidents generate an additional 2.75 billion dollars in health care treatment costs every year.8 The social and economic impact of patient harm leads to losses of trillions of US dollars worldwide.9 The global focus on increasing the number of services, and the financial mechanisms which provide them need to be complemented by sustained attention to safety.10 The extent, types, and causes of errors, adverse events, and near misses are essential for developing and implementing patient safety policies, strategies, and plans. Therefore, the implementation of reporting and learning systems for events should receive a particular priority among other interventions to ensure patient safety. The reporting environment should be free from blame and punishment to encourage health professionals to report and learn from events and provide opportunities for patients, their families, and their careers to report on their experiences. Other needs to improve patient safety include increased resources to train local personnel, enhancing research capacity, and training of non-physician personnel to create interdisciplinary patient safety teams. A safety culture requires the leadership, commitment, and involvement of personnel at all levels, especially frontline personnel. There is a need for healthcare organizations to assess patient safety culture. Areas of patient safety requiring attention and recognizing the strengths and weaknesses of the hospital’s current safety culture. Prior to intervening in a change in a hospital’s safety culture, it is necessary to assess the current state of the safety culture. Assessing the current state of the patient safety culture makes it possible for the hospital to recognize its strengths and weaknesses. Although many instruments for assessing patient safety culture exist, and one of the most common is the “HSOPSC” questionnaire. That has been developed by the US Agency for Health Care Research and Quality (AHRQ). It is widely used for both institutional and national level measurements.
HSOPSC measures patient safety culture in Afghanistan’s hospital in order to support teamwork and collaboration to improve patient safety. There are no measurement devices for patient safety in Afghanistan’s national language. Afghanistan is also part of the international community and has similar health problems as most countries. Therefore, we used the HSOPSC tools to Raise staff awareness about patient safety and assess the current status of patient safety culture.
The Afghan Ministry of Public Health has made patient safety an absolute priority in response to the increase in medical errors. Patient safety culture surveys have not yet been conducted in public hospitals in Afghanistan, and there are no valid or reliable investigational tools for this purpose. Therefore, to assess the HSOPSC tool in Afghanistan public hospital in addition to constructing an optimal model to assess the level of safety culture in this setting and to benchmark the data against other international studies. The results of such a study will enable hospital staff and management to better understand the nuances of patient safety culture and will be some best practices for other public hospitals. The development of a safety culture can prevent adverse events or promptly correct mistakes before harm is caused to the patients.
Methods
This cross-sectional descriptive study was conducted from January to March 2020 among doctors, nurses, and midwives at the Esteqlal Specialized Hospital in Kabul. Estiqlal Hospital is one of the public hospitals with 400 beds and serves approximately 113,416 patients annually.
In that study, the data were collected through a survey of hospital. “HSOPC” Dari translated questionnaire was distributed to 267 hospital staff consisting of doctors, nurses, and midwife. Participants were volunteers who had submitted a written informed consent. Most respondents had direct contact with patients. All answers were confidential and no response was shared with the local management or anyone else. Hospital managers were asked to collect the completed questionnaires a week after distribution. Among the 267 employees invited to participate, 267 (100%) completed the surveys. Ethical approval was granted by the Research Ethics Committee of Mashhad University of Medicine (IR.MUMS.REC.1398.270), and Research department of Public Health Ministry, Afghanistan. Participants were made aware of the purpose, benefits, and importance of the survey and their rights to participate voluntarily. Data were collected through a questionnaire that included sociodemographic characteristics and the Survey of Patient Safety Culture in Hospitals. Socio-demographic and individual characteristics include age, sex, education, hours worked per week, unit, position, work experience within the current unit, and type of employee. The HSOPSC was translated into Dari by three members who are experienced in health research and survey design. Then, the validity was evaluated by an expert researcher who looked at the translation. The reviewers provided suggestions for improving the quality of the translation and making it easier to understand its purpose. The latest version of the tool was modified accordingly and was then re-tested on 10 physicians in hospital. The reliability of the translated instrument was assessed using Cronbach α which revealed an acceptable value of “0.80”. The translated questionnaire was distributed to all doctors, nurses and midwives at the hospital. All answers were confidential and none was shared with hospital management teams or anyone else. After answering the questions, SPSS version 25 was used for data analysis.
Data Analysis
Descriptive statistics were used to summarize demographic data, patient safety culture dimension/element ratings, and safety results (patient safety grade, the number of reported events). The HSOPSC questionnaire consists of both positive and negative items. The HSOPSC consists of three key elements: population information, 42 elements, and the 12-dimensional measurement scale, as well as two other questions on the overall patient safety grading and the number of events reported in the last 12 months. The items were coded using a 5-point Likert scale ranging from “strongly disagree” to “never”. The mean percent positive response was used to report the results. The positive responses for each item were defined as the percentage of strongly agree and agree (always and most of the time) responses for direct -worded items and strongly disagree and disagree (never and rarely) for reverse worded items. Additionally, the average percentage of positive responses for each level was defined as the average of the percentage of positive responses for the dimension items. The last score was ranked in three levels: high (over 75% of positive responses), medium (50% to 75% of positive responses), and low (under 50% of positive responses). Quantitative data was reported as a mean and standard deviation. The analysis used a 95% confidence interval and 0.05 significance levels. Paired sample t-tests, Pearson correlation test, and ‘ANOV’ were used to compare means. Data analysed on SPSS version 25.
Result
Characteristics of Demographic
Demographic characteristics of participants show that 47.5% of men and 52.4% of women. Concerning the education level, 41.2% bachelor’s degrees, 40.5% MD, 14.2% specialist, and 4.1% had master’s degrees. The majority of respondents reported having less than 15 years of experience working at their current hospital and unit. Most staff worked 40 to 59 hours a week (65.9%). There are significant differences between the 12-dimensional patient safety culture and gender. It means that women share more information than men. There is a significant difference between married person and the dimension of “ non-punitive response to errors”. This means that married persons are less likely to be punished for their mistakes unmarried persons.
There is significant difference between the dimension of “ Frequency of events reporting “ and level of education. This means that masters are less likely to report incidents than others.
Table 1 presents demographics based on the HSPOSC questionnaire.
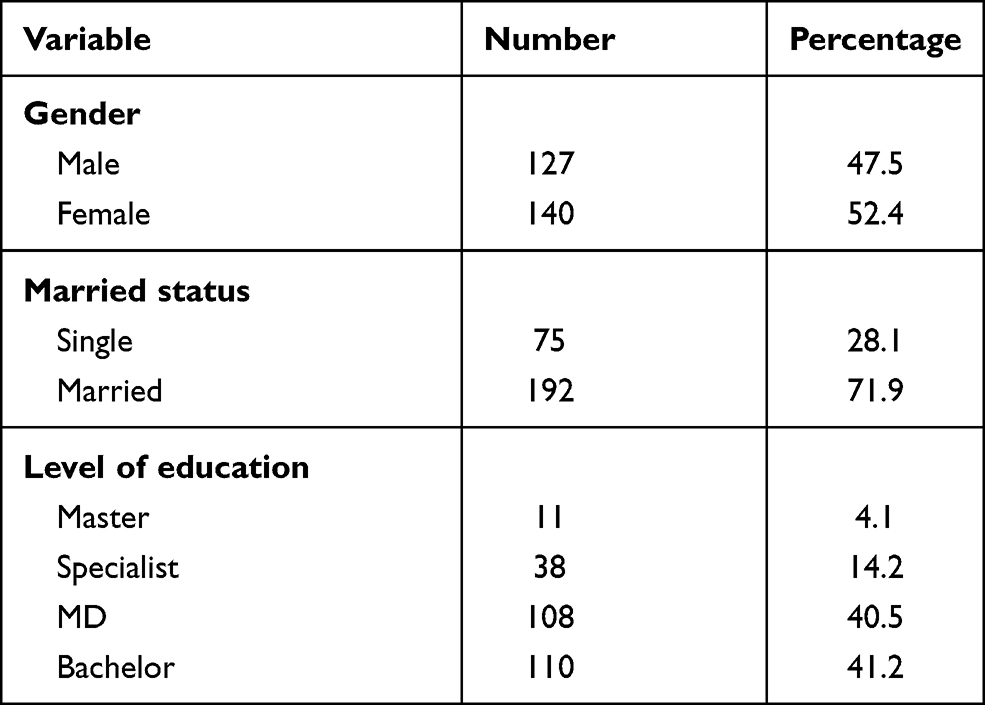 |
Table 1 Demographic Characteristics at the Estiqlal Public Hospital, Kabul, Afghanistan (n=267) |
Patient Safety Culture Dimensions
In this study, dimensions with a mean percentage of positive responses were considered at three levels: High (above 75% of positive responses), medium (50% to 75% of positive responses) and low (below 50% of positive responses). The level of safety culture in non-punitive response to errors (10.8%), communication openness (25.5%), staffing (26.6%), frequency of events reporting (34%), handoffs and transitions (40.6%), feedback and communication about the error (42.8%), supervisor/manager expectations and promoting safety actions (43.8%), overall perceptions of safety (47,6%) were low level. Management support for patient safety (55%), teamwork within units (62.4%), teamwork across units (71.2%), and Organizational learning-continuous improvement (75%) at the medium level. The lowest positive response rate was a nonpunitive response to errors, and the highest positive response rate was in continuous organization’s learning improvement. Overall, the average positive response to the 12 dimensions of patient safety culture was 44%, which showed a poor level of safety culture in the hospital. There is significant difference between the dimension of “ Frequency of events reporting “ and the job category. This meant that midwives were less likely to report events than physicians and nurses. Table 2 presents patient safety culture based on the HSPOSC questionnaire:
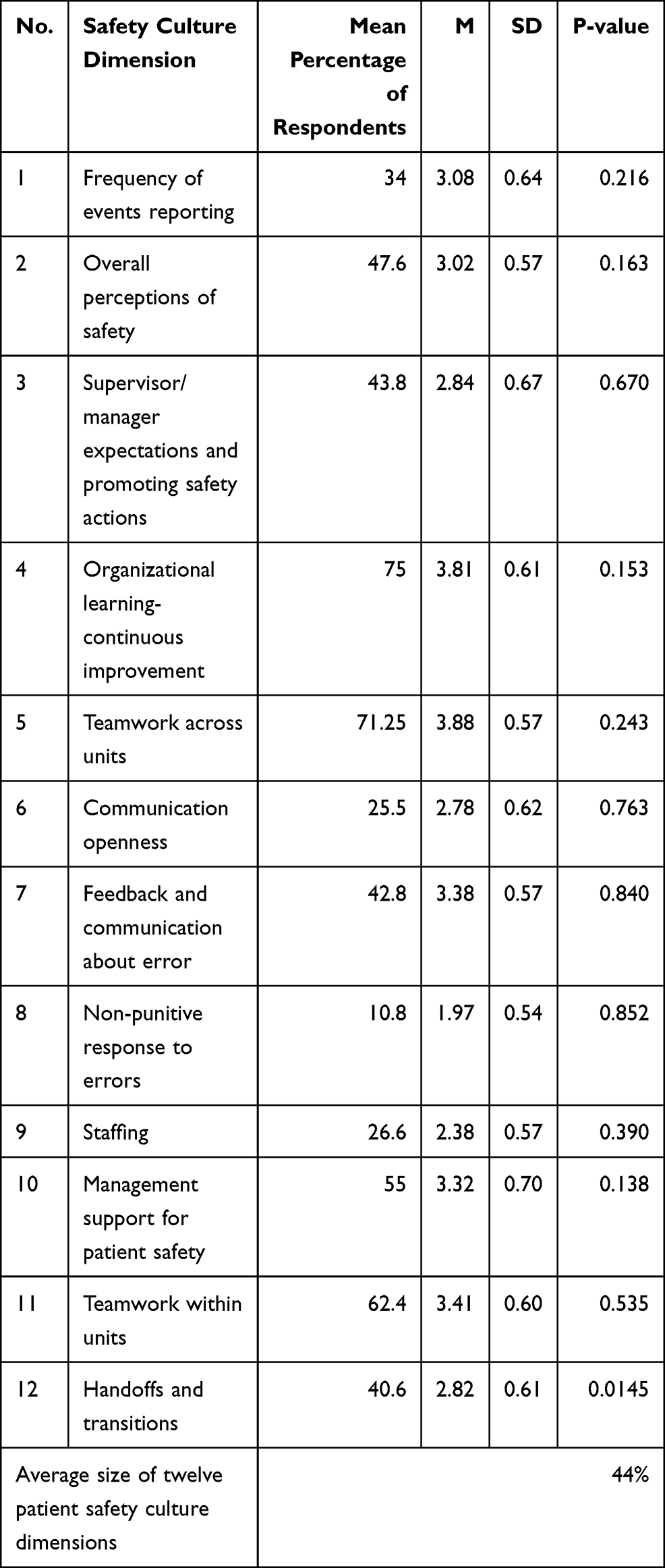 |
Table 2 Average Percentage of Positive Responses Across All 12 Dimensions of Safety Culture Survey at the Estiqlal Public Hospital, Kabul, Afghanistan (n=267) and (M =Mean, SD= Standard Deviation, the Independent Sample t-test and One-Way “ANOVA” Were Used to Check Variations Between Groups, Significant at P ≤ 0.05, “Agree” and “Strongly Agree” are Positive Responses, “Strongly Disagree” and “Disagree” are Positive Responses, nd “Most of the Times” and “Always” are Positive Responses) |
Regarding the “number of reported events”, the findings showed that midwives and nurses reported less medical error than others. Fewer reports were given in the new-born service. This means that reporting of medical errors in the hospital is poor, and the main reason is the fear of punishment from the manager. Table 3 presents Percentage of events report in the last 12 months.
 |
Table 3 Percentage of Events Report in the Last 12 Months at the Estiqlal Public Hospital, Kabul, Afghanistan (n=267) |
In this study, the percentage of hospital staff evaluated the patient safety level. This means that the hospital is in a poor condition and this is a significant statistic for hospitals. Table 4 shows responses to the patient safety grade dimension:
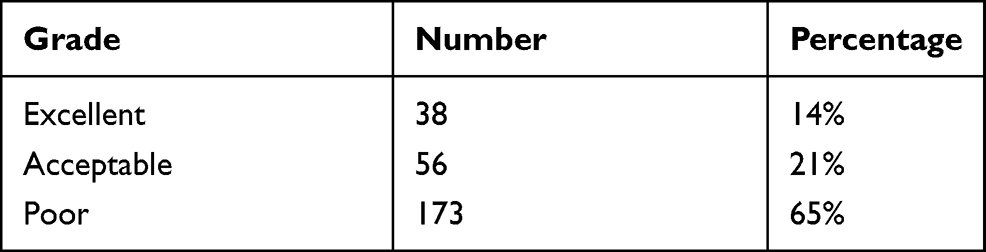 |
Table 4 Responses to the Patient Safety Grade Dimension at the Estiqlal Public Hospital, Kabul, Afghanistan (n=267): Patient Safety Grade |
Discussion
This study assessed the current state of patient safety culture in Esteqlal Hospital using the HSOPSC tool. The current study showed that the overall positive response was poor in all aspects of HSOPSC in the hospital, and that some areas need improvement immediately. The assessment and promotion of a safety culture are recognized as a necessary step to improve patient safety. Overall, the mean positive response rate was 44% which is almost similar to the study implemented in Ethiopia11 but is lower than the Netherlands,12 Palestine,13 and Taiwan.14 This clarification of variation may focus on differences in organizational behavior and management across countries. These countries may have better management values, commitments, leadership, hospital staff relations, economic development and national cultural difference. This means we can learn from hospitals that have a more developed safety culture. In this study, the highest score for organizational learning (75%) and the lowest score for nonpunitive error response (10.8%) were identified. It is interesting to note that “Organizational learning-continuous improvement” the only dimension that scores higher (75%) than the AHRQ data (73%).15 This study showed “teamwork across the unit” and “teamwork within unit” dimensions were the area of highest average positive response rate after organizational learning. This shows that respondents are positive in supporting each other, working together as a team, and act to improve patient safety. This result is nearly compatible with the results of studies carried out in Iran,16 and Netherlands. It is estimated that the “staffing” dimension is low (26.6%), and significantly below the AHRQ (54%). The shortage of qualified personnel is a challenge for the hospital, and there is evidence of its impact on health outcomes. As a result, managers should take appropriate steps to allocate and distribute resources. Meanwhile, staff is a common concern for patient safety in many countries. This study found that 66% of respondents worked more than 40 hours a week. Continuous work causes fatigue in employees, increasing the likelihood of medical errors and side effects on patient safety. Another area of concern is “non-punitive response to error” which has the lowest percentage (10.8%) of positive response among the 12 dimensions of patient safety culture in this study. Most hospital staff believe that their errors are kept against them and are kept in their personal file. Although a significant number of respondents believe that medical error is followed by punitive measures, approximately half of them reported at least one incident in the last 12 months. It is important that the hospital create an environment that encourages the culture and reporting of errors without fear of punishment, to restore patient safety. The mean positive response rate was (10.8%) which is almost similar to the study conducted at the ICU in Brazil (14%), and Saudi Arabia.17–19 The dimension of “Handoffs and transition of care” is at a low-level (40.6%). The main aim of the patient is to transfer and share the patient’s clinical information when transferring responsibility to other employees. The lack of information raises the risk of treatment and ultimately the safety of patients Inadequate staffing, lack of knowledge, communication errors and lack of awareness are the main causes of risk when patients are transferred to hospital.20 The dimensions of “Management support and learning” is at the medium level (55%). Hospital staff believes that hospital management does not create an enabling work environment that enhances patient safety. Their errors are recorded in the personnel files “Frequency of events reporting”. Similar findings were found in studies in Jima, Northern Ethiopia, Tunisia, and Oman.21–23 In this study, only 33.8% of hospital respondents reported at least one event in their hospital in the last year. This is lower than reported by hospitals in Amhara, where two-thirds of health care workers reported at least one event in the Jima region, SNNP hospitals in Ethiopia, Saudi Arabia and Iran.24–26 Our study showed that almost every aspect of a patient safety culture is needed to make improvements. In this study, the hospital was in a poor condition.
Conclusion
The result of the present study showed that the state of patient safety culture in most of the dimensions are not appropriate from the perspective of physicians, nurses, and midwives, which can be due to the culture of punishment, unfair distribution of nurses, and midwives in the hospital unit. In this study, the highest score for organizational learning and the lowest score for non-punitive response to event error were detected. Our study identified most areas that needed to be improved, including increased staffing and resources. Creating a positive safety culture for patients is unavoidable by taking steps that support all aspects of the safety culture. It will be important to invest time and resources in training staff, not blaming anyone, and to encourage a culture of reporting errors among co-workers. This can be achieved through regular and joint training sessions for doctors, midwives and nurses. Additional effort is needed to establish an effective and a positive safety culture in all parts of the hospital. Evidence can help governmental health decision-makers and hospital administrators understand the challenges surrounding the issue of hospital patient safety culture and develop strategies to improve it. There is a suggestion to research, patient safety culture in other public and private hospitals in the future.
Limitation
The study focused on the hospital patient safety culture, with a focus on doctors, nurses and midwives, who make up approximately 75% of Estiqlal hospital staff. Further studies are required to obtain a more comprehensive picture of the patient safety culture taking into account other categories of staff in the hospital.
Ethics Approval and Consent to Participate
The study was approved by the Research Ethics Committee of Mashhad University of Medicine. (IR.MUMS.REC.1398.270), (http://research.mums.ac.ir) and research department of Ministry of Health, Afghanistan before the process of data collection commenced. Participants were given oral and written information on the study, including details on the confidentiality of the data processing. Participants were informed of the voluntary nature of their participation, including the possibility of termination at any time. Written informed consent was obtained from each participant before the participation. Meanwhile, this study was conducted in accordance with the declaration of Helsinki.
Acknowledgments
The author would like to thank the doctors, nurses and midwives at Estiqlal Hospital for their help and participation in the study. I am grateful to the MoPH, the hospital director, and the Mashhad University of Medical Sciencestrainers for supporting the study. I also appreciated Dr. Fatema Kokabi, Dr. Arif Oryakhil, and Dr. Masoda Faizi for their assistance with the editing article.
Author Contributions
Author considered the idea, designed the study, analysed the data, and wrote the article.
Meanwhile, all authors contribution to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Javad Moghri, Seyed Saeed Tabatabaee, and Jamshid Jamali report grants from Mashhad University of Medical Sciences (MUMS). The authors report no other conflicts of interest in this work.
References
1. WHO. Maternal new-born-child adolescent health and gaining/quality of care 2020. Available from: https://www.who.int/teams/maternal-newborn-child-adolescent.health.and.ageing/quality.of.care.
2. Bardossy AC, Zervos J, Zervos M. Preventing hospital-acquired infections in low-income and middle-income countries. Infectious Dis Clin North America. 2016;30:805–818. doi:10.1016/j.idc.2016.04.006
3. WHO patient safety: “Making health care safer”; 2017. Available from: https://www.who.int/teams/integrated-health-services/patient-safety.
4. Dzau V, Ginsburg GS, Finkelman E, Balatbat C, Flott K, Jessica P. Precision medicine a Global Action Plan for Impact. World innovation summit for health; Report of the WISH Precision Medicine Forum 2016. Available from: https://www.wish.org.qa/wp-content/uploads. Accessed February 5, 2021.
5. Precision medicine a Global Action Plan for Impact. World innovation summit for health; 2016. Available from: https://www.wish.org.qa/wp-content/uploads.
6. WHO. Patient safety in developing and transitional countries new insights from africa and the eastern mediterranean health. Available from: https://apps.who.int/iris/handle.
7. OECD. Better policies for better live, patient safety; 2019. Available from: http://www.oecd.org/health/patient-safety.
8. A commentary article about the implementation and advancement of the Patient Safety Friendly Hospital Initiative (PSFHI) in the Eastern Mediterranean Region; 2019. Avaliable from: http://www.ihf-fih.org.
9. Canadian Patient Safety institute (CPSI): awareness of the patient safety crisis in Canada; 2019. Availabel from: http://www.patientsafetyinstitute.ca.
10. WHO. Calls for urgent action to reduce patient harm in healthcare; 2019. Avaliable from: https://www.who.int/news/item.
11. Johnston B, Lou-Meda R, Mendez S. Teaching patient safety in global health. lessons from the Duke global health patient safety AQ8 fellowship. BMJ. 2019
12. Mekonnen A, McLachlan A, Brien J-A, Mekonnen D, Abay Z. Hospital survey on patient safety culture in Ethiopian public hospitals. PubMed. 2017
13. Wagner S, Sorra H. Assessing patient safety culture in hospitals across countries. Int J Qual Health Care. 2013;25:213–221. doi:10.1093/intqhc/mzt024
14. Hamdan S. Assessment of patient safety culture in Palestinian public hospitals. Care. 2013.
15. Chen C, Hung-Hui L. Measuring patient safety culture in Taiwan using the hospital survey on patient safety culture (HSOPSC). BMC Health Services Research. 2010;10. doi:10.1186/1472-6963-10-152
16. Famolaro Y, Burns F, Liu. Hospital survey on patient safety culture user comparative database report; 2016. Available from: https://psnet.ahrq.gov/issue/hospital.
17. Aderaye G, Zumla AI, Onyebujoh PC, Zwijnenberg NC, Hendriks M, Hoogervorst-Schilp J. Healthcare professionals’ views on the feedback of a patient safety culture assessment. Springer Nature Switzerland AG. 2016.
18. Santiago TH, Turrini RN. Organizational culture and climate for patient safety in Intensive Care Units. SCIELO Brazilian scientific journals. Revista Da Escola De 480 Enfermagem Da U S P. 2015;49:123–130. doi:10.1590/S0080-623420150000700018
19. El-Jardali F, Sheikh F, Garcia NA, Jamal D, Abdo A. Patient safety culture in a large teaching hospital in Riyadh baseline assessment, comparative analysis, and opportunities for improvement. BMC Health Services Research. 2014;14. doi:10.1186/1472-6963-14-122
20. Minuzzi AP, Salum NC, Locks MOH Assessment of patient safety culture in intensive care from the health team’s perspective; 2016. Available from: https://www.scielo.br/scielo.php?lng=en.
21. Habibzadeh F, Imanipour M, Mohammad Aliha J, Mehran A. Effect of applying checklist on quality of intra-hospital transport of intensive care patients. Iranian Journal of Cardiovascular Nursing. 2014.
22. Wami SD, Demssie AF, Wassie MM, Ahmed AN. Patient safety culture and associated factors: a quantitative and qualitative study of healthcare workers’ view in Jimma zone Hospitals, Southwest Ethiopia. BMC Health Services Res. 2016;16. doi:10.1186/s12913-016-1757-z
23. Al-Mandhari A, Al-Zakwani I, Al-Kindi M, Tawilah J, Atsu SS, Al-Adawi S. Patient safety culture assessment in Oman. Oman Med J. 2014;29:264–270. doi:10.5001/omj.2014.70
24. Ejajo T, Arega A, Batebo B. Measuring the current patient safety culture in public general hospitals of Southern Nations Nationalities and Peoples Region (SNNPR), Ethiopia. J Environ Public Health. 2017. doi:10.1155/2017/6373595
25. Al-Ahmadi TA. Measuring patient safety culture in Riyadh’s hospitals: a comparison between public and private hospitals. J Egypt Public Health Assoc. 2009;84:479–500.
26. Bahadori M, Izadi AR, Ravangard R, Hosseini SM. Confirmatory factor analysis of patient safety culture in an Iranian Hospital. Patient Safety & Quality Improvement Journal. 2016.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.