")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Assessment of Health Research Capacity in Western Sydney Local Health District (WSLHD): A Study on Medical, Nursing and Allied Health Professionals
Authors Lee SA , Byth K , Gifford JA , Balasubramanian M , Fozzard CA, Skapetis T , Flood VM
Received 12 July 2019
Accepted for publication 10 December 2019
Published 11 February 2020 Volume 2020:13 Pages 153—163
DOI https://doi.org/10.2147/JMDH.S222987
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Sharon A Lee,1,2 Karen Byth,1,2 Janelle A Gifford,2– 5 Madhan Balasubramanian,1,2,6,6 Carolyn A Fozzard,1 Tony Skapetis,6,7 Victoria M Flood1– 3
1Western Sydney Local Health District, Research and Education Network, Westmead, NSW 2145, Australia; 2Faculty of Medicine and Health, Sydney School of Health Sciences, University of Sydney, Sydney, NSW 2141, Australia; 3Charles Perkins Centre, The University of Sydney, Camperdown, NSW 2006, Australia; 4South Western Sydney Local Health District, Liverpool, NSW 2170, Australia; 5Ingham Institute for Applied Medical Research, Liverpool, NSW 2170, Australia; 6Faculty of Medicine and Health, Sydney Dental School, University of Sydney, Sydney, NSW 2005, Australia; 7Division of Oral Health, Western Sydney Local Health District, Westmead, NSW 2145, Australia
Correspondence: Victoria M Flood
Research & Education Network, Westmead Hospital, Corner Hawkesbury & Darcy Road, Westmead, NSW 2145, Australia
Tel +612 8890 9721
Fax +612 8890 8627
Email [email protected]
Background: Research should inform clinical decision-making and evidence-based practice for all health professionals. To build research capacity among all health professionals, there is a need to measure the levels of research capacity and identify the gaps and needs of health-care professionals. The aim of the study was to better understand the research culture and capacity of health professionals (medical, nursing and allied health) in Western Sydney Local Health District, Sydney, Australia.
Methods: A research capacity and culture tool (RCCT) survey was electronically distributed to all health staff in WSLHD. Data were collected between November 2016 and January 2017. Participants were surveyed through a 10-point Likert scale that measured research capacity at the individual, team and organisational levels.
Results: A total of 393 health staff responded to the study: allied health practitioners (46.3%), nursing staff (35.4%) and medical practitioners (18.3%). Females made 76% of the sample, and 54% were aged between 35 and 54 years. Individual responses were different across professions, with an average median score for medical 6.3 (95% CI 5.8– 6.9), allied health 5.3 (95% CI 4.9– 5.7) and nursing 4.5 (95% CI 4.1– 5.0) after adjustment for age and gender. Team responses for medical staff (average median score 5.9 95% CI 5.3– 6.4) were higher than allied health (4.1 95% CI 3.7– 4.6) and nursing (4.3 95% CI 3.8– 4.8), after adjusting for age and gender. However, there were no differences between the three professions for the organisational responses. Allied health and nursing staff were less confident in obtaining research funding, submitting ethics applications, writing for publication and mentoring colleagues about research.
Conclusion: This study demonstrates the individual research capacity for medical, allied health and nursing professionals are different. Research capacity building needs to be individually tailored to the specific needs of each profession. This research will inform future capacity building activities and training for health professionals in a large public health organisation of Sydney, Australia.
Keywords: research capacity, allied health, nursing
Plain Language Summary
Health-care professionals working in organisations such as hospitals are in a unique position to carry out research to benefit service provision as well as their own career development. Research is the foundation of evidence-based guidelines that inform clinical practice and sound decision making for all health-care professionals. However, there may be gaps in the capacity to conduct research across different professions. This study surveyed health-care professionals in a large metropolitan teaching hospital in Sydney, Australia to assess research capacity, enablers and barriers to research. Self-perceived research capacity differed widely across allied health, nursing and medical professionals. Nursing and allied health professionals had reduced confidence in many aspects of research when compared to medical professionals, in particular obtaining research funding, submitting ethics applications, writing for publication and mentoring colleagues about research. The results of this study can be used to tailor workforce planning and education to bridge these gaps and meet the individual needs of each profession..
Introduction
Research is the foundation of evidence-based guidelines that inform clinical practice and sound decision making for all health professionals. The ability of health professionals to utilise, conduct and evaluate research is particularly important. Many countries worldwide have advocated the importance of research capacity building among health-care professionals.1–5
In Australia, research capacity building in health professionals has been a primary focus over the last decade, and in public health organisations is undertaken by a range of professions including allied health, nursing and medical professionals. It is recognised that health settings engaged in research have improved patient outcomes.6 The Australian Government has dedicated over $6 billion of the total health budget for 2019–2020 to support research.7 However, the research capacity of health professionals within public health organisations are varied and some may lack the necessary research experience or may require further support at an organisational level.8 The varied research skill level of different professionals may reflect many aspects such as; undergraduate training, departmental culture, mentor availability or individual interest in research.9–11
Previous studies have reported health professionals who undertake research have improved skill sets, job satisfaction and increased opportunities for career advancements.12–14 Hence building the capacity of staff to undertake research is an important component of health systems. Through research we can improve health outcomes for patients that potentially lead to a healthier community. Presentation of research findings to healthcare policy makers can encourage the implementation of research findings directly impacting clinical care.15 Upskilling and retention of staff are valued attributes to health-care institutions and these attributes attract researchers from elsewhere. Identification of barriers and facilitators within a health-care institution and subsequent workforce training are imperative to build a sustainable research culture within institutions.
A recent systematic review on the evaluation of research capacity development for individuals and organisations by Huber et al concluded that research capacity is maximised when conducted multi-professionally.16 To build research capacity among all health professionals, there is a need to measure the levels of research capacity and identify the gaps and needs of health-care workers.
There are few available tools to measure the research capacity and culture within health-care organisations. Paget et al assessed research capacity in a paediatric hospital population across nursing, medical and allied health professional17 using a self-developed tool that has not yet been validated. However, the research capacity and culture tool (RCCT) is a validated questionnaire that encompasses the individuals, team and organisations research capacity.18 This tool has been widely used to assess research capacity within professions including, dietitians,19 podiatrists,13,20 occupational therapists21 and allied health professionals as a group.8,22,23 To our knowledge, there are not any studies assessing the research capacity in health-care settings of all health disciplines within the same survey using the RCCT.
Therefore, the aim of this study was to describe the research capacity and culture of allied health, nursing and medical staff in a large urban public health organisation within NSW known as Western Sydney Local Health District (WSLHD).
Methods
Data Collection
A survey of all health professionals (allied health, nursing and medical staff) working in WSLHD was conducted between November 2016 to January 2017. WSLHD is a public health organisation that services approximately one million people from culturally and linguistically diverse background, where approximately 7150 health professionals were employed in late 2016 at the time of the survey (approximately 968 allied health staff, 4100 nursing staff and 2079 medical staff).
Study data were collected and managed using REDCap electronic data capture tools hosted at the University of Sydney.24 REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies. All health professional staff across WSLHD including Allied health, nursing and medical professionals were initially approached by an introductory email containing information about the study and a link to the REDCap survey. Reminders to complete the survey were provided in a health newsletter and via email. Data collected included demographic and employment details (such as age, gender, educational qualification, place of work, team role, years of experience), general research information (such as current enrolment in a research program, having research in their role description) and research culture and capacity tool (RCCT).
Research Culture and Capacity Tool (RCCT) Data Items
The research culture and capacity of health professionals were assessed through a battery of 51 items, classified across three domains: individual level (14 items); team level (19 items) and organisational level (18 items), using the previously validated RCCT18. Questions in the RCCT ask participants to self-assess research skills and supports such as writing research protocols, literature review skills, availability of research software and data analysis skills. Respondents were asked to rank their level of agreement to each item or statement ranging from 1 to 10, with 1 being least skill or success and 10 being strong skill or success to that item or statement. In general, respondents were ranking their own skill or success level or assessing the team or organisation support for providing adequate research training and infrastructure. The RCCT also asked respondents to indicate their perceived barriers or motivators to undertaking research.
Data Preparation and Analysis
Online responses were collated from REDCap and exported for statistical analysis to the software IBM SPSS V24 (IBM SPSS, 2017). A minimum dataset was required for inclusion in the analysis; respondents needed to have nominated their profession and completed a minimum of one question with a response between 1 and 10 in the Individual, Team or Organisation questionnaires. If all answers were unsure or left blank respondents were excluded. Health professionals were classified into three groups (allied health, nursing and medical), based on their response to main practicing profession in WSLHD (dentists were classified under the medical category, oral health technicians were classified as allied health professionals). Age groups were collapsed to three categories: less than 35 years, 35–54 years and 55+ years. Educational qualifications were categorised into three categories: undergraduate level, graduate/post-graduate level and higher degree by research (HDR). The place of work was limited to two categories: hospital group (including Westmead, Blacktown, Auburn and Mt Druitt hospitals, and those who worked across multiple hospitals within WSLHD) and health services group (mental health, community health and population health services). Respondents were classified into three broad roles: clinician, management/executive or teaching/research. Years of experience were categorized as either: less than 10 years’, or 10 or more years’ experience. Respondents were also categorized into groups based on a) current enrolment in a research degree and b) a research role in their job description.
The median and interquartile range (IQR), that is lower to upper quartiles were used to summarise skewed variables. Percentages were used for categorical variables. Kruskal–Wallis non-parametric analysis variance was used to test for differences in the distribution of the Individual, Team and Organisational domains across professions. The median score across the items in each domain (Individual, Team and Organisation) was calculated for each participant. The reported “average median score” for each domain refers to the mean across of those individual median scores. We further adjusted for age and gender, then reported where there were differences between the professions for the average median score (p < 0.05). Figures have been used for each domain to illustrate the proportion of each health profession whose median score exceeded successively higher values at each score unit for the median score.
Ethical Considerations
Ethical approval for the study was obtained from the Western Sydney Local Health District Human Research Ethics Committee (Local Reference AU/LNR/16/WMEAD/410 - 4881). Consent was implied with an “opt in” approach via completion of the survey after reading the participant information.
Results
A total of 501 (7%) health professionals from WSLHD responded to the electronic survey, and 393 met our minimum dataset requirements and were included in the final analysis. One hundred and eight (108) of the respondents were excluded, 36 who did not nominate a profession and the remainder failed to enter a response, or provided only “unsure” responses to all items in the survey. When those excluded were compared to those included in the final analysis (the “participants”) no statistically significant differences were found with respect to gender, profession, age or place of work. However, those with a higher research degree or in senior team roles were, however, significantly more likely to meet the inclusion criteria.
Sample Characteristics
The largest proportion of respondents were allied health practitioners (46.3%), followed by nursing (35.4%) and medical professionals (18.3%). Females comprised over three-quarters of the participants (76.1%), and the majority of participants were aged 35–54 years (53.8%). About one-fifth were currently enrolled in a research program (18.0%) and a similar proportion had a HDR qualification (17.3%). Notably, more than a third of medical staff who completed the survey had a HDR qualification, compared to 18.1% among allied health professions and 6.5% among nursing staff. A relatively higher proportion of nursing and allied health staff were currently enrolled in a research degree (21.2% and 17.9%, respectively). More than 60% of participants were clinicians, 16.1% identified roles as management or executive and the remaining 21.2% were currently employed in teaching or research positions. The respondents were mostly experienced health professionals with 72.3% having more than 10 years of experience (see Table 1).
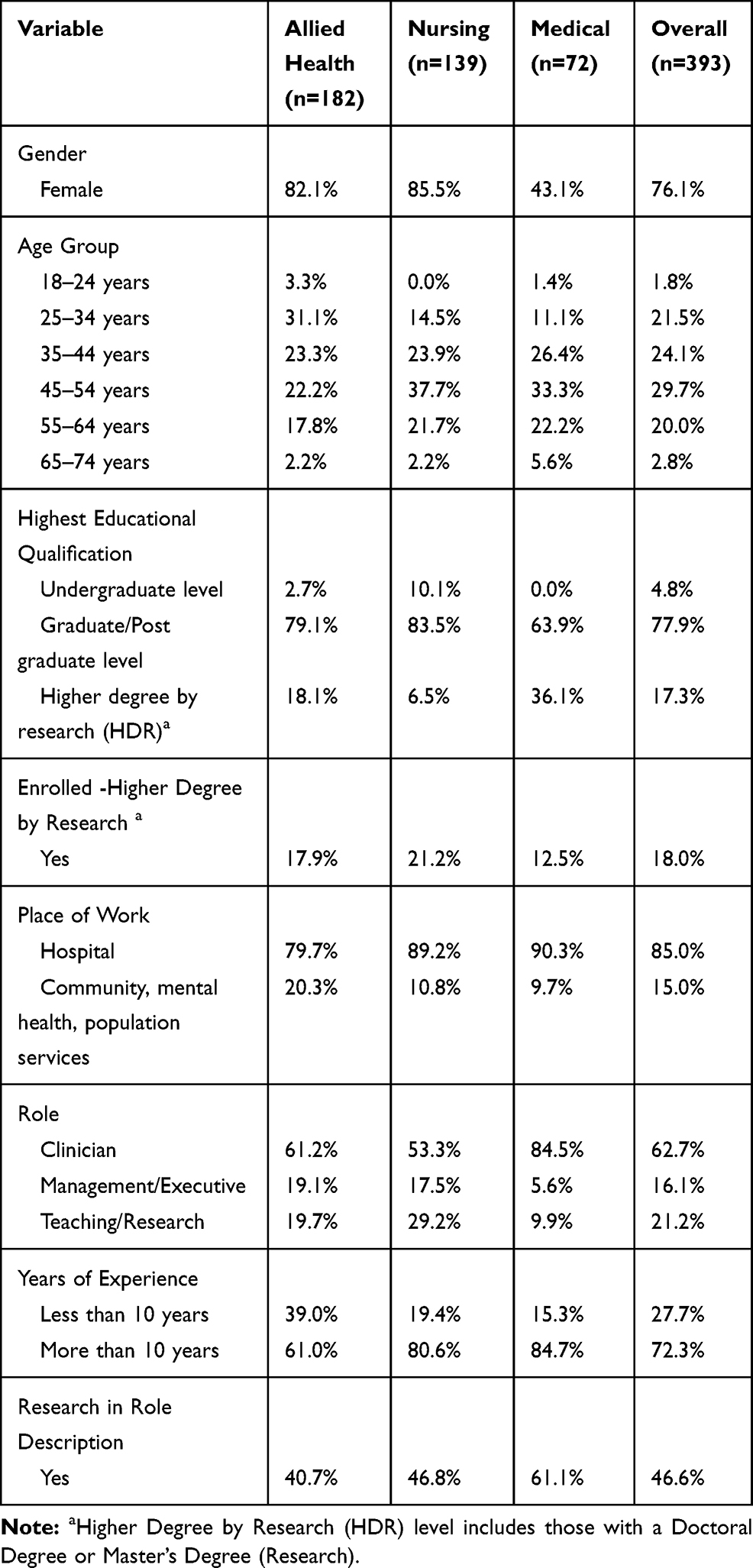 |
Table 1 Sample Characteristics of Participants of the Research Capacity and Culture Tool, by Health Profession |
Research Culture and Capacity Tool (RCCT) Items
The results of all Individual (14 items), Organisational (19 items) and Team (18 items) level RCCT items grouped by health profession (allied health, nursing and medical) are presented in Tables 2–4. At the Individual level (Table 2), there were differences in all responses across the three health professions, except for the items about “designing questionnaires”, “collecting data” and “analysing qualitative data”; for these three items all three groups responded similarly. Allied health and nursing professionals scored lowest on “securing research funding”, “submitting ethics applications”, “writing for publication” and “providing advice to less experienced researchers” at an Individual level, with a median score of four or less.
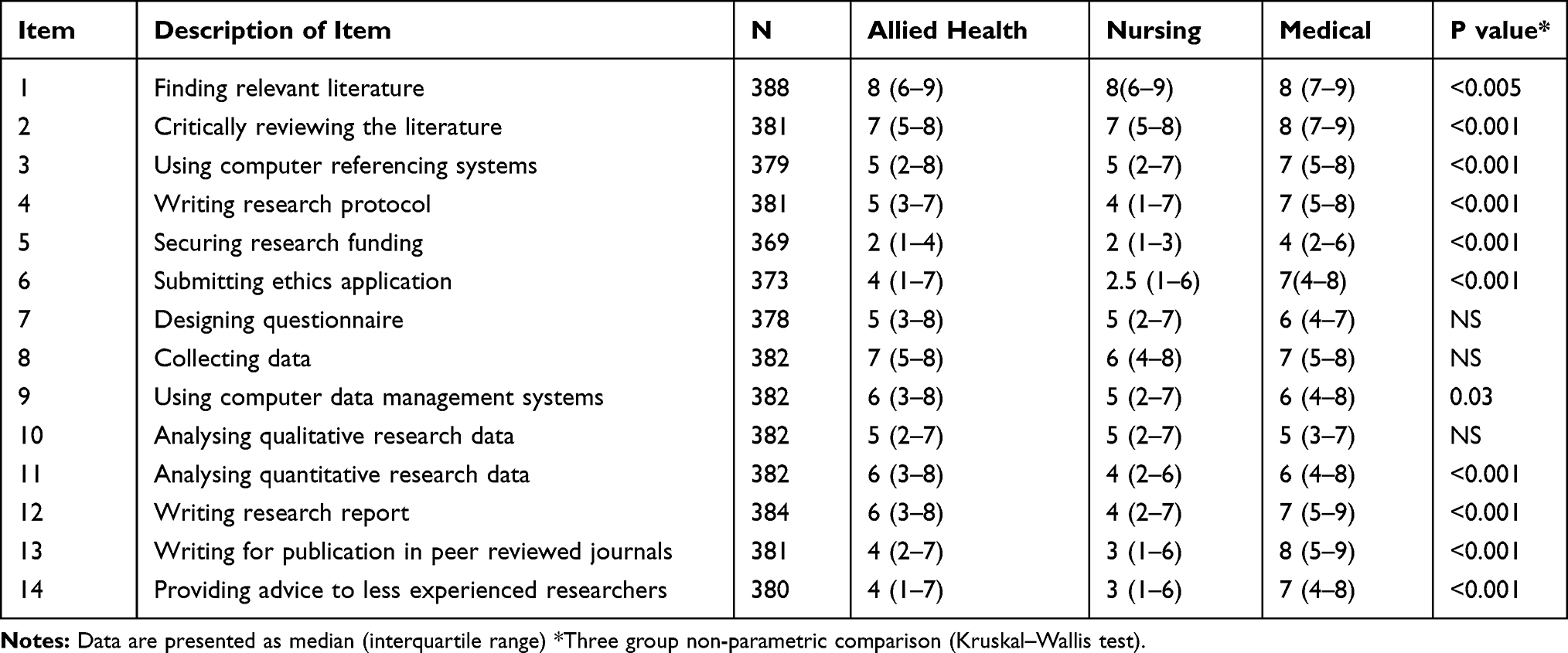 |
Table 2 Individual Domain Responses Ranging from 1 (Low Skill) to 10 (High Skill) |
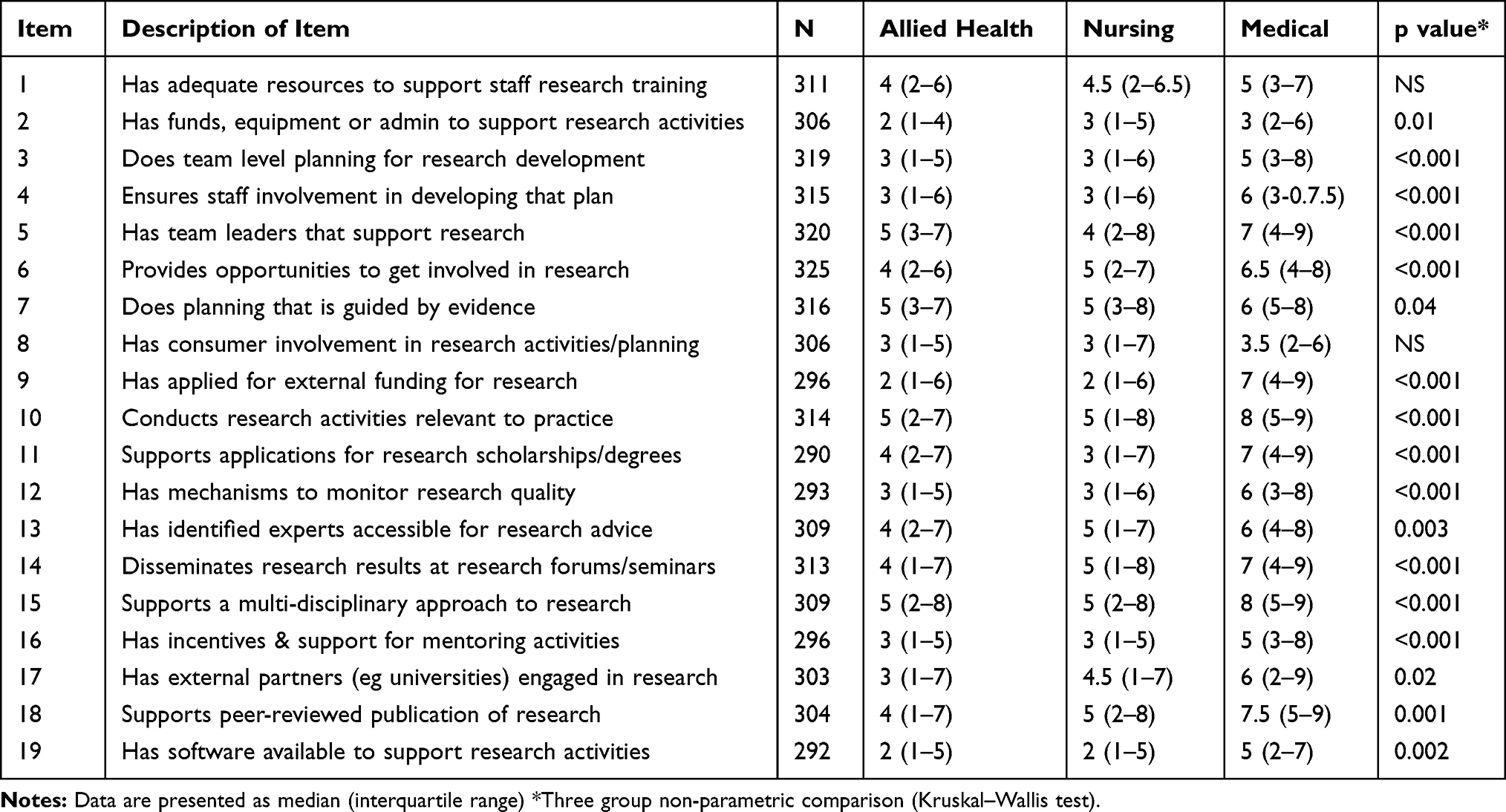 |
Table 3 Team Domain Responses Ranging from 1 (Low Skill) to 10 (High Skill) |
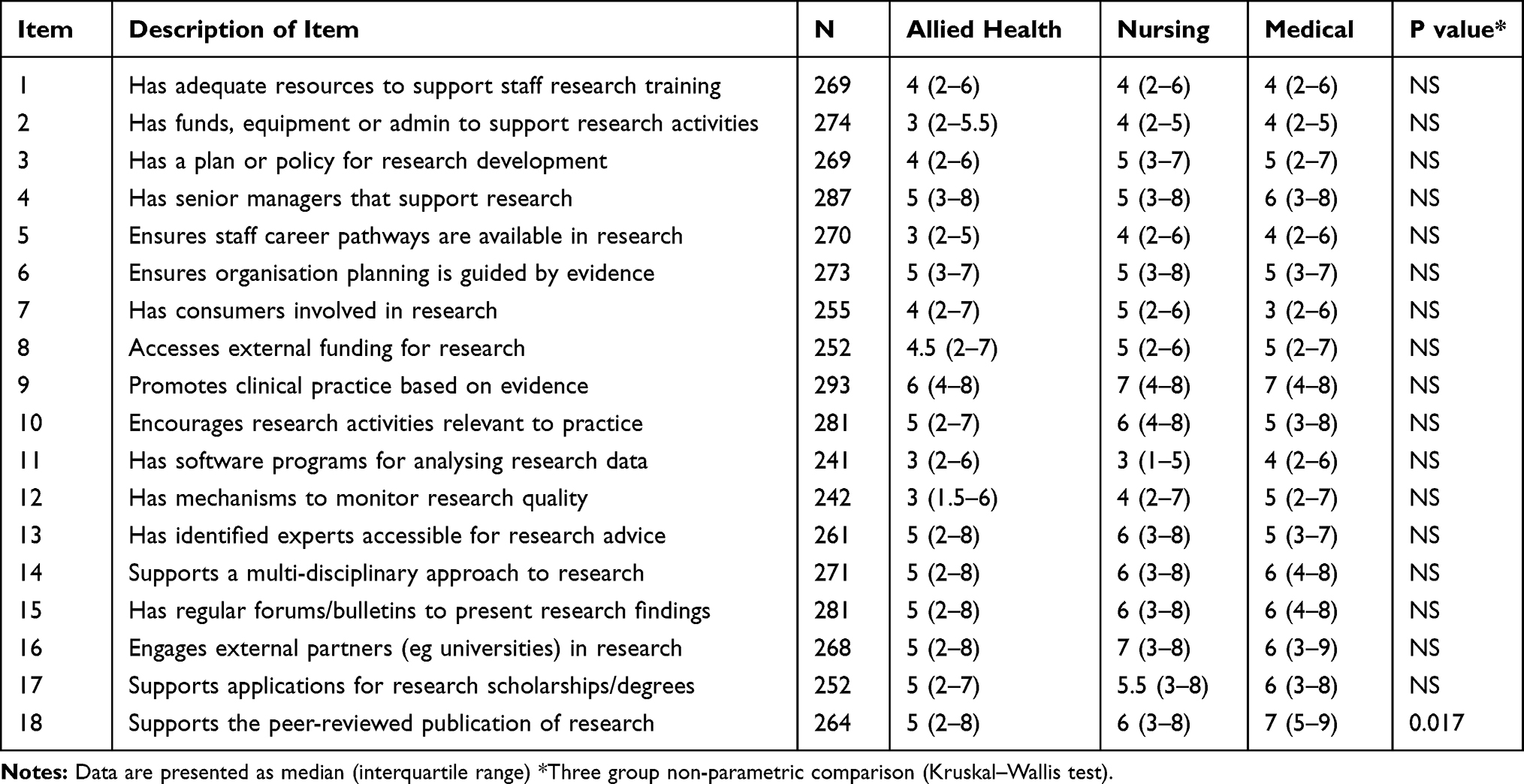 |
Table 4 Organisational Domain Responses Ranging from 1 (Low Skill) to 10 (High Skill) |
With the exception of “adequate resources to support staff research training” and “consumer involvement in research activities and planning”, Team level (Table 3) responses differed significantly by health profession. In the team domains, allied health professionals and nurses scored an average of five or less for all items. Medical professionals scored five or more for all items except for “has funds, equipment or admin to support research activities” and “consumer involvement in research activities/planning”.
In contrast, organisational level (Table 4) responses were generally not significantly different between the three health profession groups, except with respect to “supports the peer reviewed publication of research” where medical staff scored higher (p=0.017).
The Individual domain average median score for the medical professionals was higher at 6.3 (95% CI 5.8–6.9) than that for allied health professionals (5.3 95% CI 4.9–5.7) which in turn was higher than that for nursing (4.5 95% CI 4.1–5.0) (p< 0.001), after adjusting for age and gender (Table 5). After adjustment for age and gender the Team domain average median score among the medical professionals was also higher than that for nursing and allied health professionals who were comparable (medical score 5.9 (95% CI 5.3–6.4), nursing 4.3 (95% CI 3.8–4.8), allied health 4.1 (95% CI 3.7–4.6); p<0.05 for medical score vs nursing and allied health). The Organisational domain demonstrated no significant differences between the professions after adjustment for age and gender (Table 5) Medical 5.1 (95% CI 4.5–5.7), Allied Health 5.0 (95% CI 4.5–5.4) and Nursing 5.3 (95% CI 4.7–5.8).
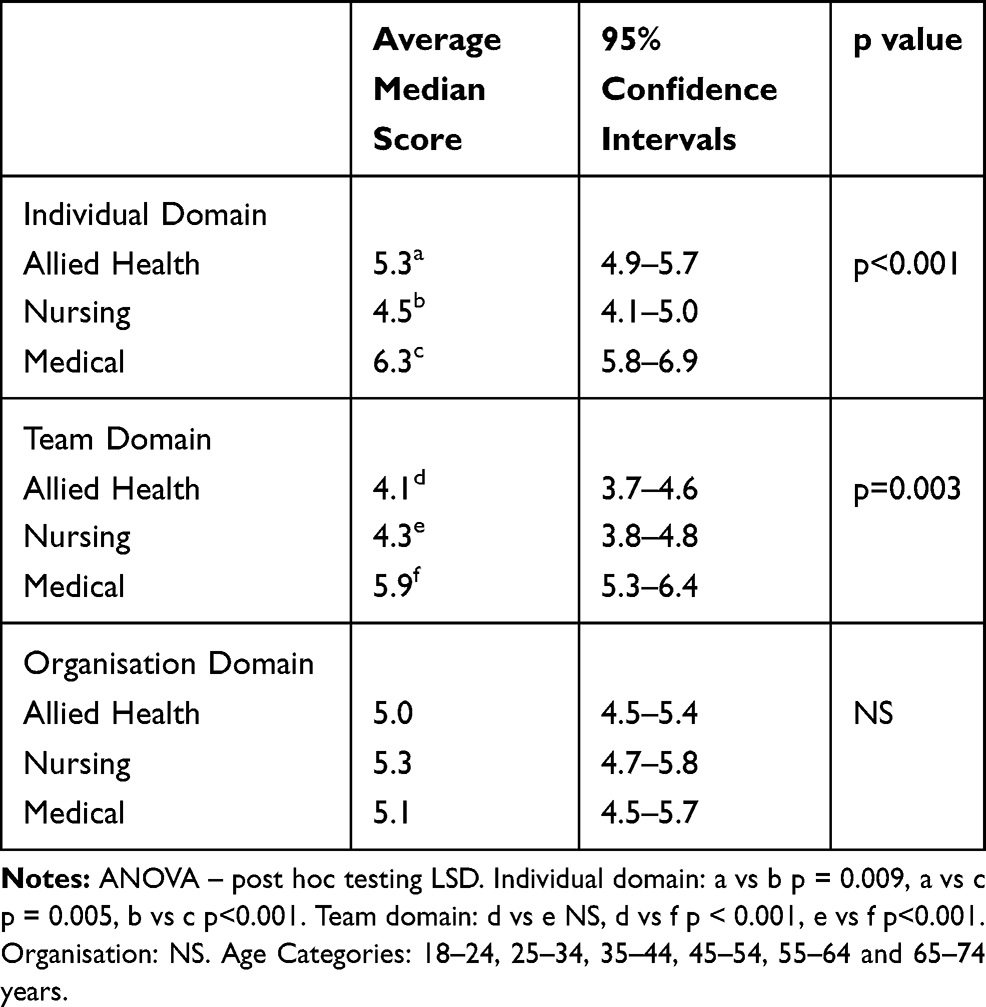 |
Table 5 Average of the Median Score for Each Domain Item by Health Profession, Adjusted for Age and Gender |
When considering the Individual domain scores for each profession (Figure 1), the average median scores for each profession as a group indicated that only 47% of nurses and 60% of allied health scored greater than or equal to five, whereas 78% of medical professionals scored ≥5. The Team domains (Figure 2) demonstrated similar results with 42% of nurses and 40% of allied health professionals with an average median score ≥5 and 70% of medical professionals average median score was ≥5. Whereas this difference was not seen in the Organisational domains (Figure 3) with 64% nurses, 58% allied health and 56% medical professionals with scores ≥5.
 |
Figure 1 Percentage of subjects whose median score for the Individual domain items exceeded the score of 5. (bold line arbitrary cut point). |
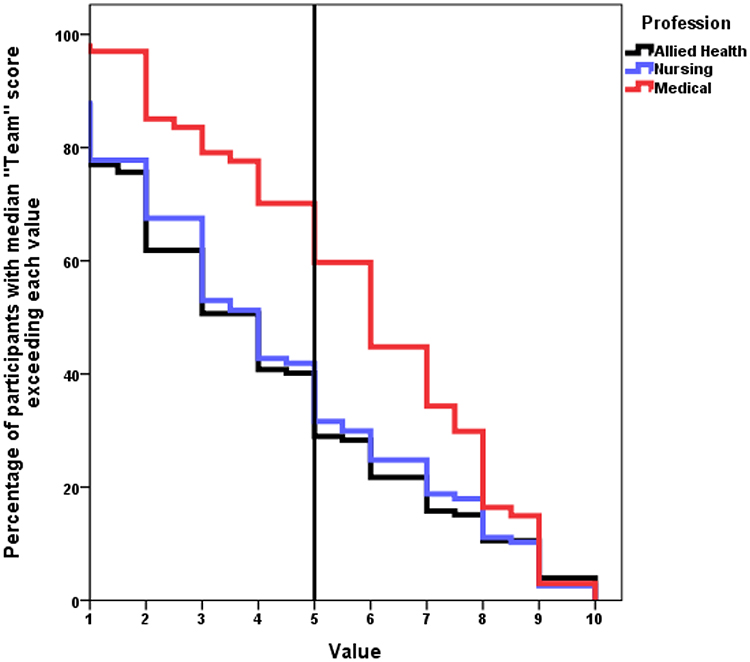 |
Figure 2 Percentage of subjects whose median score for the Team domain items exceeded the score of 5. (bold line arbitrary cut point). |
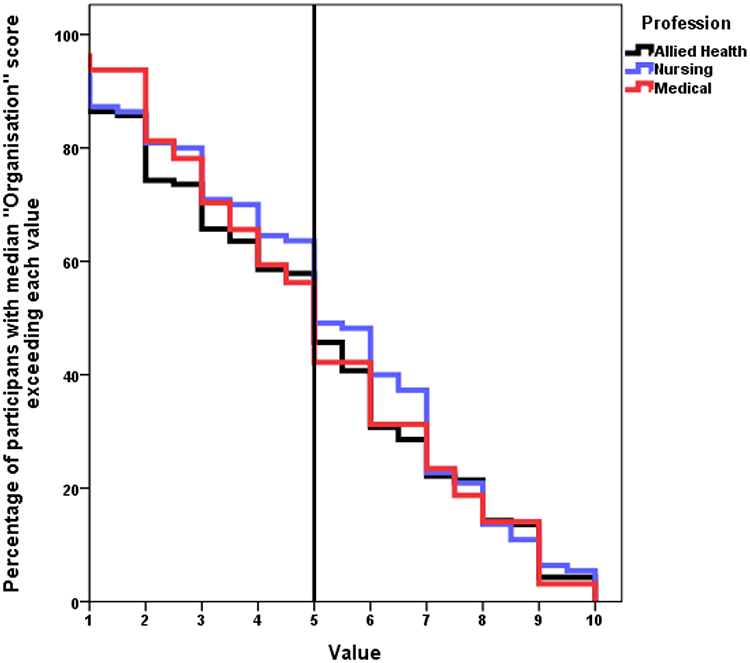 |
Figure 3 Percentage of subjects whose median score for the Organisation domain items exceeded the score of 5. (bold line arbitrary cut point). |
The main barriers to research reported by respondents were: “other work role takes priority” and “lack of time for research”, as well as “lack of funds and skills for research” (Table 6). In contrast the main motivators for research were: “to develop skills”, “increased job satisfaction”, “problem identified that needs changing” and “to keep the brain stimulated” (Table 7).
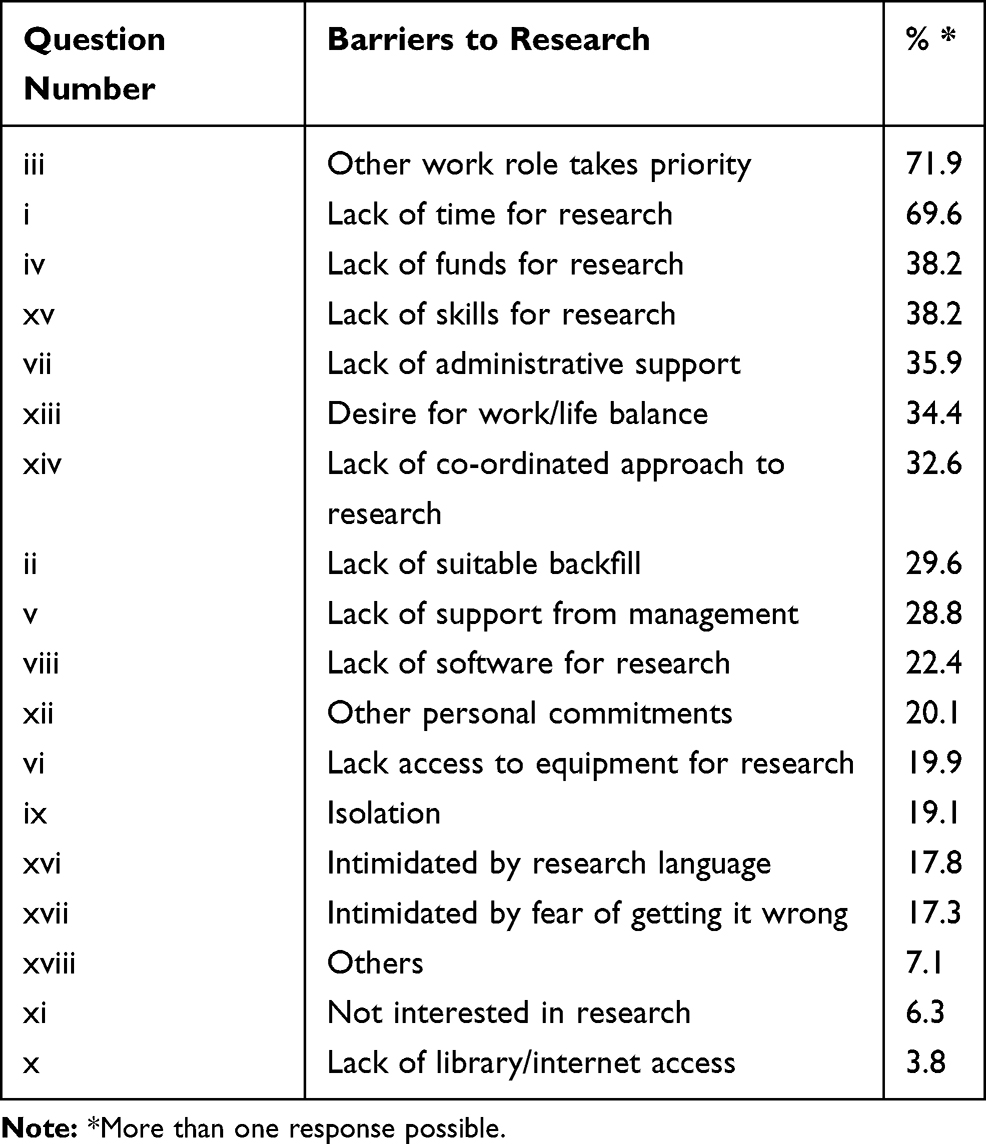 |
Table 6 Barriers to Research (n=393) from the RCCT |
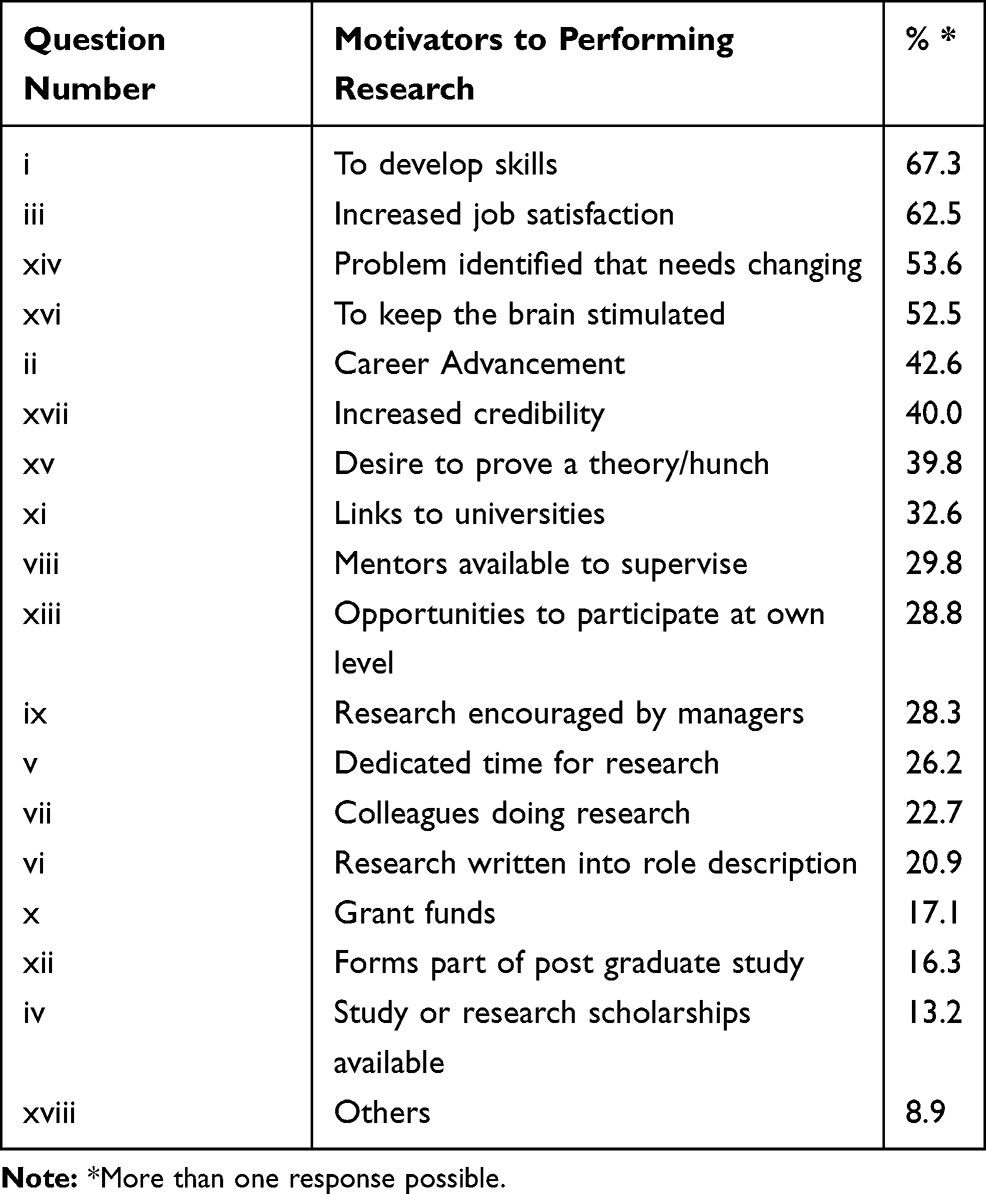 |
Table 7 Motivators to Research (n=393) from the RCCT |
Discussion
This is the first study to define the research capacity and culture across three health profession groups, namely; allied health, nursing and medical within a large public health organisation in Australia. Overall results demonstrated all three professions identified different areas of need at an individual and team level, although all three groups were similar when assessing the organisational research capacity.
This study has highlighted areas of need and will allow workforce planning and training to improve research capacity across all disciplines. WSLHD includes tertiary hospitals, and community centres servicing a diverse population, hence the findings from this study may be broadly applicable to similar public health organisations within Australia. Through engagement with healthcare policy makers and the wider research stakeholders it is hoped that this studies results will contribute to building a sustainable research culture within our institution.
Allied health and nursing professional’s self-assessment of their individual research capacity and culture was low compared with medical professionals, with less than 60% of allied health and less than 50% of nursing respondents scoring greater than five out of ten. In contrast, medical professionals generally had higher scores at an Individual and Team level, which may indicate more confidence in conducting research.
Medical professionals have long been expected to undertake postgraduate studies in research in order for career progression,25 yet this has not been seen in allied health and nursing staff to the same extent until more recently. This may be the reason for the higher current enrolment levels in these professions as nursing and allied health professions having the higher number of current enrolment in higher research degrees 21% and 18% respectively compared to only 13% of medical professions. However, it is possible that these numbers could reflect a bias in the people who chose to participate in the survey. We also note that the survey was delivered in a specific order of Individual, Team and Organisation domains, and we observed a decreasing response rate as the survey progressed. The lowest number of responses for items in each domain were: Individual 369, Team 290 and Organisation 242. This is likely due to survey fatigue, however because the RCCT has been validated utilising all three domains, participants were asked to complete the whole questionnaire with the results analysed accordingly.
Western Sydney Local Health District is a large public health organisation in Sydney, NSW. There have been multiple studies that have utilised the RCCT within professions,13,20,22 however no prior research has directly compared allied health, nursing and medical profession using this tool. Similar to other studies among only allied health professionals8,22,23 our study highlighted the same area of lower skill or success for individuals; writing for publication in peer-reviewed journals, providing advice to less experienced researchers, submission of ethics applications and securing research funding. Interestingly in this study nursing and allied health responses were very similar and markedly different form of medical professionals.
The majority of health professionals in this survey report a “desire to develop skills” and “improve job satisfaction” as the main motivators for individuals to undertake research, similar results have been found in the other studies in allied health professionals only.8,13,23 The barriers to research identified “other work role takes priority” and “lack of time for research” were the most commonly identified issue with lack of funding and lack of skills for research being an issue for a third of respondents. Again, this is what has been identified in previous studies in allied health professionals.8,13,23
One of the limitations of this study was the low response rate with only 7% of staff participating in the survey. None the less validity of a study should not be judged on the response rate alone.26 People who responded might have been more interested in research, which is reflected by the relatively large numbers with either a research degree or currently enrolled in a research degree. Therefore, the responses may be more in line with the views of health professionals who are actively engaged in the research process, and not necessarily those of a wider health professional experience. Whilst this may present some degree of response bias it may also be a closer representation of what the real enablers and barriers are for researchers across the different professions. Survey response rates vary greatly in the available literature from 6% in podiatrist20 increasing to 24% in allied health and nursing,5 through to 54% across the allied health professional group.8 A recent study by Kidd et al highlighted survey response rates to be lower when surveys are administered electronically compared to those on paper.27 Our response rate was low at 7% but interestingly when comparing the responses from allied health professionals in Allison et al8 to the allied health responses from our survey they were very similar. Thus indicating that although our response rate was low results are comparable to what has been found in individual professional groups when tested elsewhere. As this is the first study to compare allied health, nursing and medical we are not able to compare response rates in all of these populations.
The results of this study highlight the need for public health organisations to conduct periodic assessments of research capacity to ascertain the needs of all health-care workers within their institutions. Based on the findings of this study we are initiating further research education opportunities with a focus on nursing and allied health staff within the organisation. There is also potential for interdisciplinary research training across the professions, which has the added benefit of encouraging collaboration between professional groups on future research projects.
Based on the findings from this study, research is required to explore the individual barriers and enablers experienced by each of the different health professions in more detail via qualitative research with research active health professionals.
Conclusion
This study provides evidence of the unique requirements of allied health, nursing and medical professionals in developing research capacity. It is clear that the requirements for each are different and consideration should be given to individualising research capacity improvements or support. These results can be used to develop tailored education and training to better support the needs of each health profession group.
Acknowledgments
The authors would like to thank Ms Timothea Lau for her contributions to the manuscript preparation and formatting. We would also like to acknowledge Ms Joanne Edwards and Dr Roslyn Crampton for their encouragement of nursing and medical staff to participate in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brauer S, Haines T, Bew P. Fostering clinician-led research. Aust J Physiother. 2007;53:143–144. doi:10.1016/S0004-9514(07)70020-X
2. Baumbusch J, Kirkham S, Khan K, et al. Pursuing common agendas: a collaborative model for knowledge translation between research and practice in clinical settings. Res Nurs Health. 2008;31(2):130–140. doi:10.1002/(ISSN)1098-240X
3. Hulcombe J. An approach to building research capacity for health practitioners in a public health environment: an organisational perspective. Aust Health Rev. 2014;38(3):252–258. doi:10.1071/AH13066
4. Misso ML, Ilic D, Haines TP, Hutchinson AM, East CE, HJ T. Development, implementation and evaluation of a clinical research engagement and leadership capacity building program in a large Australian health care service. BMC Med Educ. 2016;16(13):1–9. doi:10.1186/s12909-016-0525-4
5. Luckson M, Duncan F, Rajai A, Haigh C. Exploring the research culture of nurses and allied health professional (AHP’s) in a research-focused and a non-research-focused healthcare organisation in the UK. J Clin Nurs. 2018;27:1462–1476. doi:10.1111/jocn.14264
6. NSW Ministry of Health. NSW Health And Medical Research Strategic Review. Sydney; 2012.
7. NHMRC. Budget outcomes 2019: the Australian Government budget 2019 sets out the economic and fiscal outlook for Australia. Available from: https://www.nhmrc.gov.au/about-us/news-centre/budget-2019-statement.
8. Alison J, Zafiropoulos B, Heard R. Key factors influencing allied health research capacity in a large Australian metropolitan health district. J Multidisciplinary Healthcare. 2017;10:277–291. doi:10.2147/JMDH.S142009
9. Golenko X, Pager S, Holden L. A thematic analysis of the role of the organisation in building allied health research capacity: a senior managers’ perspective. BMC Health Serv Res. 2012;12:276. doi:10.1186/1472-6963-12-276
10. Borkowski D, McKinstry C, Cotchett M, Williams C, Haines T. Research culture in allied health: a systematic review. Aust J Prim Health. 2016;22(4):294–303. doi:10.1071/PY15122
11. Wilkes L, Cummings J, McKay N. Developing a culture to facilitate research capacity building for clinical nurse consultants in generalist paediatric practice. Nurs Res Pract. 2013;2013:709025.
12. Pager S, Holden L, Golenko X. Motivators, enablers, and barriers to building allied health research capacity. J Multidiscip Healthc. 2012;5:53–59. doi:10.2147/JMDH.S27638
13. Lazzarini P, Geraghty J, Kinnear E, Butterworth M, Ward D. Research capacity and culture in podiatry: early observations within Queensland Health. J Foot Ankle Res. 2013;6:1–11. doi:10.1186/1757-1146-6-1
14. Finch E, Cornwell P, Ward E, McPhail S. Factors influencing research engagement: research interest,confidence and experience in an Australian speech-language pathology workforce. BMC Health Serv Res. 2013;13:144. doi:10.1186/1472-6963-13-144
15. Boaz A, Baeza J, Fraser A. Effective implementation of research into practice: an overview of systematic reviews of the health literature. BMC Res Notes. 2011;4:212. doi:10.1186/1756-0500-4-212
16. Huber J, Nepal S, Bauer D, Wessels I, Fischer M, Kiessling C. Tools and instruments for needs assessment, monitoring and evaluation of health research capacity development activities at the individual and organizational level: a systematic review. Health Res Policy Syst. 2015;13(80):1–17. doi:10.1186/s12961-015-0070-3
17. Paget S, Lilischkis K, Morrow A, Caldwell P. Embedding research in clinical practice: differences in attitudes to research participation among clinicians in a tertiary teaching hospital. Intern Med J. 2014;44(1):86–89. doi:10.1111/imj.12330
18. Holden L, Pager S, Golenko X, Ware R. Validation of the research capacity and culture (RCC) tool: measuring RCC at individual, team and organisation levels. Aust J Prim Health. 2012;18:62–67. doi:10.1071/PY10081
19. Howard AJ, Ferguson M, Wilkinson P, Campbell KL. Involvement in research activities and factors influencing research capacity among dietitians. J Human Nutr Dietetics. 2013;26(s1):180–187. doi:10.1111/jhn.2013.26.issue-s1
20. Williams C, Lazzarini P. The research capacity and culture of Australian podiatrists. J Foot Ankle Res. 2015;8(11). doi:10.1186/s13047-015-0066-9
21. Pighills A, Plummer D, Harvey D, Pain T. Positioning occupational therapy as a discipline on the research continuum: results of a cross-sectional survey of research experience. Aust Occup Ther J. 2013;60(4):241–251. doi:10.1111/aot.2013.60.issue-4
22. Williams C, Miyazaki K, Borkowski D, McKinstry C, Cotcher M, Haines T. Research capacity and culture of the Victorian public health allied health workforce is influenced by key research support staff and location. Aust Health Rev. 2015;39:303–311. doi:10.1071/AH14209
23. Borkowski D, McKinstry C, Cotchett M. Research culture in a regional allied health setting. Aust J Prim Health. 2017;23:300–306. doi:10.1071/PY16085
24. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
25. Royal Australasian College of Physicians. Advanced Training programs. 2019. Available from: https://www.racp.edu.au/trainees/advanced-training/advanced-training-programs.
26. Morton SM, Bandara DK, Robinson EM, Carr PE. In the 21st Century, what is an acceptable response rate? Aust N Z J Public Health. 2012;36(2):106–108. doi:10.1111/j.1753-6405.2012.00854.x
27. Kidd JC, Colley S, Dennis S. Surveying allied health professionals within a public health service: what works best, paper or online?. Eval Health Prof. 2019;doi:10.1177/0163278719870568
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.