")
Back to Journals » Journal of Asthma and Allergy » Volume 13
Assessment of Chronic Respiratory Health Symptoms and Associated Factors Among Flour Mill Factory Workers in Addis Ababa, Ethiopia, 2019: A Cross-Sectional Study
Authors Alemseged EA , Takele AK, Zele Y , Abaya SW, Kiros KG, Mehari M , Bezabh YA , Atsbaha AH , Awoke TY , Goyteom MH
Received 30 July 2020
Accepted for publication 18 September 2020
Published 14 October 2020 Volume 2020:13 Pages 483—492
DOI https://doi.org/10.2147/JAA.S273820
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Embay Amare Alemseged,1 Abera Kumie Takele,2,* Yifokire Zele,2,* Samson Wakuma Abaya,2,* Kbrom Gmechu Kiros,3,* Medhin Mehari,1,* Yonas Angaw Bezabh,1,* Abadi Hailay Atsbaha,1,* Tegegnework Yitayew Awoke,4,* Mekonnen Haftom Goyteom3 **
1Department of Public Health, School of Medicine and Health Sciences, Adigrat University, Adigrat, Ethiopia; 2Department of Preventive Medicine, School of Public Health, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 3Department of Nursing, School of Medicine and Health Sciences, Adigrat University, Adigrat, Ethiopia; 4Food, Medicine, and Health Care Authority, Addis Ababa City Administration, Addis Ababa, Ethiopia
*These authors contributed equally to this work
Correspondence: Embay Amare Alemseged Email [email protected]
Background: Flour mill workers are at high risk of developing respiratory symptoms due to exposure to flour dust in their working environment. Exposure to flour dust linked with the development of chronic respiratory disorders. However, very little evidence has been available on the respiratory symptoms of exposed workers in large-scale flour mill factories. Therefore, the aim of this study was to assess chronic respiratory health symptoms and associated factors among flour mill workers in Addis Ababa, Ethiopia.
Methods: Cross-sectional study was conducted among a sample of 424 randomly selected workers from Addis Ababa flour mill factories. Respiratory health symptoms were assessed using an American Thoracic Society standard questionnaire customized with local context. Data were checked for completeness and Epi-Info V. 7.2 and SPSS V.21 statistical software were used for data entry and analysis, respectively. Multivariable logistic regression model was used to identify variables associated with chronic respiratory health symptoms. Variables that had significant association were identified based on adjusted odds ratio (AOR) with 95% confidence interval (CI) and p < 0.05. Data were presented using tables, texts and figures.
Results: The prevalence of chronic respiratory health symptoms among flour mill factory workers was 58.3% (95% CI: 53.7– 63.4). Chronic respiratory health symptoms were significantly associated with age group (AOR=1.95, 95% CI; 1.17– 2.79 and AOR=12.3, 95% CI; 4.39– 34.6), monthly income (AOR=1.68, 95% CI; 1– 2.79), work experience (AOR=2.58, 95% CI; 1– 6.62), past dust exposure (AOR=1.86, 95% CI; 1.08– 3.2) and utilization of respiratory protective equipment (AOR=2.29, 95% CI; 1.27– 4.13).
Conclusion and Recommendation: Chronic respiratory health symptoms were highly prevalent among flour mill factory workers. Supportive supervision and cooperation between Ministry of Labour and Social Affairs, flour mill managers and workers are needed to reduce exposure and improve working environment.
Keywords: flour dust, flour mill worker, prevalence, Addis Ababa, Ethiopia
Introduction
Dust is a small, dry solid particle that ranges from one to a hundred micrometers in diameter size and formed by natural forces or human-made processes (like crushing, grinding, milling, drilling, and sweeping). Dusts are classified into organic and inorganic. Inorganic dust comes from non-living things and organic dust comes from living things.1 Flour dust is complex organic dust of finely ground particles arising from the milling of cereals or pulses.2 The respiratory symptoms have been documented in employees exposed to a variety of dust in small and large-scale industries, which generate dust during their production process. The diseases of the respiratory system caused by occupational dust are influenced by the type of dust, dose, duration of exposure, and genetic factors. Exposure to flour dust is one of the most common causes of allergic rhinitis, chronic respiratory disorders, including asthma and occupational airway diseases. In many industries such as flour mills and bakeries, the dust generated during cleaning, grinding, packaging, and transport is released in the atmosphere and can be inhaled.3 In low- and middle-income countries, occupational respiratory health symptoms and diseases are at high burden. Due to increasing investments, high unemployment rates; due to this, workers are more likely to continue working even when having poor health status and old machines, which produced excessive dust to work environment is still used for production purposes. Work-related respiratory symptoms are broadly abundant in low-income regions of Africa, including Ethiopia.4
Flour mill workers are at risk of developing chronic respiratory health effects due to exposure in their working environment.5 Chronic respiratory diseases account for about 10.7% of all non-communicable diseases (NCD).6 Occupational respiratory illnesses account for up to 30% of all recorded work-related disorders, with up to 50% prevalence among workers in high-risk sectors such as mining, construction, and dust-generating works.7 In Ethiopia, the total death of NCDs was estimated to account for 691,000 individuals (30%), with chronic respiratory diseases 3%.6 Dusty environment and unfavorable climatic conditions are significant occupational hazards in flour factories that influence workers’ health.8 Previous studies showed that flour dust exposure causes respiratory symptoms such as chest pain, phlegm, wheezing, cough, shortness of breath in flour mill workers.9,10
Over 50 million workers engaged in different medium and large-scale manufacturing industry in Ethiopia, about 55,000 workers are engaged in flour mill factories.11 In most flour milling factories, the attention of most workers is mainly on adverse outcomes. As long as there are no severe accidents immediately, occupational safety and health policies and practices are not carried out adequately. To the investigators' knowledge, no study is conducted in large-scale flour mill factories (where the work setup, production capacity, and numbers of workers were different from the local grain mill) to assess respiratory symptoms and associated factors among workers. Therefore, the objective of the study was to assess chronic respiratory symptoms and associated factors among flour mill factory workers in Addis Ababa, Ethiopia.
Methods and Materials
Study Setting, Design, and Population
The study area was conducted in two large-scale factories of Addis Ababa (Kaliti and Fafa food complex share companies). Addis Ababa is the capital city of Ethiopia that geographically lays 9°1′48″N latitude and 38°44′24″E line of longitude. It covers an area of 540 square kilometers (54,000 hectares), with a total population of 3,147,000.12 The city has ten sub-cities and 116 districts. A cross-sectional study design was conducted among 424 randomly selected workers from March 10-May 25 2019.
Sample Size Determination and Sampling Technique
The sample size was determined using single population proportion formula with the following assumptions: prevalence of respiratory symptoms= 54.3%, (add ref) d: Margin of error = 5%, at 95% confidence interval = 1.96 it becomes 381 by adding 10% for non-response rate; the final sample size becomes 424. Akaki Kaliti sub-city was selected because it has a large number of medium and large scales manufacturing industries and a large number of the population in this sub-city is engaged in industrial activities. From the selected sub-city, two flour mill factories were selected based on their number of workers engaged and production rate capacity. The sample of study participants from both flour mill factories was proportionally allocated. A simple random sampling technique was used to select study subjects from each department.
Data Collection Tool and Procedure
The tool was adapted from American Thoracic Society (ATS). The tool was divided into four sections: socio-demographic characteristics, behavioral characteristics, work-related characteristics, and environmental factors. After granting a written consent face-to-face interview was performed by the trained data collectors. An observational checklist was used to assess the working condition (includes housing condition, ventilation, type of machine and site visit at the work area was made to observe whether the study participants utilize the appropriate personal protective devices or not, type of operation the study participant covered).
Data Quality Assurance
A standardized questionnaire modified from ATS was used to assure data quality. Prior to data collection, training was given to the data collectors and supervisors in order to fill the questionnaire appropriately and to reduce bias. Additionally, the questionnaire was translated from English to Amharic and back-translated to English using the standard procedure to assure its validity. Each data collector has checked the questionnaires frequently for completeness and consistency. The supervisors also have checked all the filled questionnaires on daily basis. The principal investigator has cautiously observed and followed the overall activities of the data collection.
Data Analysis
Descriptive statistics were used to describe the study populations using frequency distribution, measures of central tendency, and dispersion that was displayed using tables, texts and figures. Binary logistic regression was used to see an association between independent variables and chronic respiratory symptoms. Variables significant at p < 0.2 were included in the multivariable logistic regression analysis. Statistical significance was declared at P value <0.05.
Operational Definitions
Chronic respiratory symptoms: - development of one or more of the chronic symptoms of a cough, cough with sputum, breathlessness, nose irritation, wheezing, chest illness, and sneezing, which lasts at least three months in one year.13
Chronic Cough:-Experience of a cough for most days of the week (≥4 days) for at least three months in one year.13
Duration of exposure: is defined as the working hours of workers in the factory per day.
Dust: consisting of particles in the environment that originates from several sources such as flour dust.
Duration of employment: is defined as current workers’ experience in the factory.
Previous exposure history: - workers experience in the dusty environment before the current working position.14
Cough with sputum production: - It is sputum expectoration on most days of the week (5 days) for at least three consecutive months in one year.13
Chronic Breathlessness: - Is defined as discomfort or difficulty breathing in different activities like walking up a slight hill, when undressing, walking at own pace.15
Chronic wheezing: -a condition of causing a wheezy or whistling sound heard during inhalation or exhalation (at least three months in a year).13
Chronic chest pain: - In the past year, chest pain that kept off work.14
Current smokers:-Workers who were smoking at the time of the study or a person who smokes cigarettes every day or some days.16
Pieces of cloths: Any item of clothing made up of textile/leather can be worn by the workers to cover their nose/mouth to protect the entry of flour dust particles.
Local exhaust ventilation: is the removal of airborne contaminants, close to their source of generation or release, before they can spread and reach the worker’s breathing zone.1
Ethical Consideration
This study was conducted in accordance with Helsinki declaration. Addis Ababa University ethical review board approved the study. Issues of rights, privacy, and confidentiality were ensured during data collection period. Participants had the right to participate or not and to withdraw at any time when they feel discomfort.
Results
Socio-Demographic Characteristics of Respondents
A total of 424 flour mill workers were selected from the two large-scale flour mill factories to participate in the study with a response rate of 97.9%.
Out of 415 respondents, 276 (66.5%) were males, and 203 (48.9%) were found between the age group of 26–45 with the mean (±SD) age of 29.67 (±8.52) years. Three hundred (72.3%) of the participants were Orthodox followers, and 208 (50.1%) of the study participants were single. Regarding educational level, 164 (39.5%) of the respondents attended grades 9–12. The mean (±SD) monthly income (ETB) of respondents was 2326.03 (±1268.17) (Table 1).
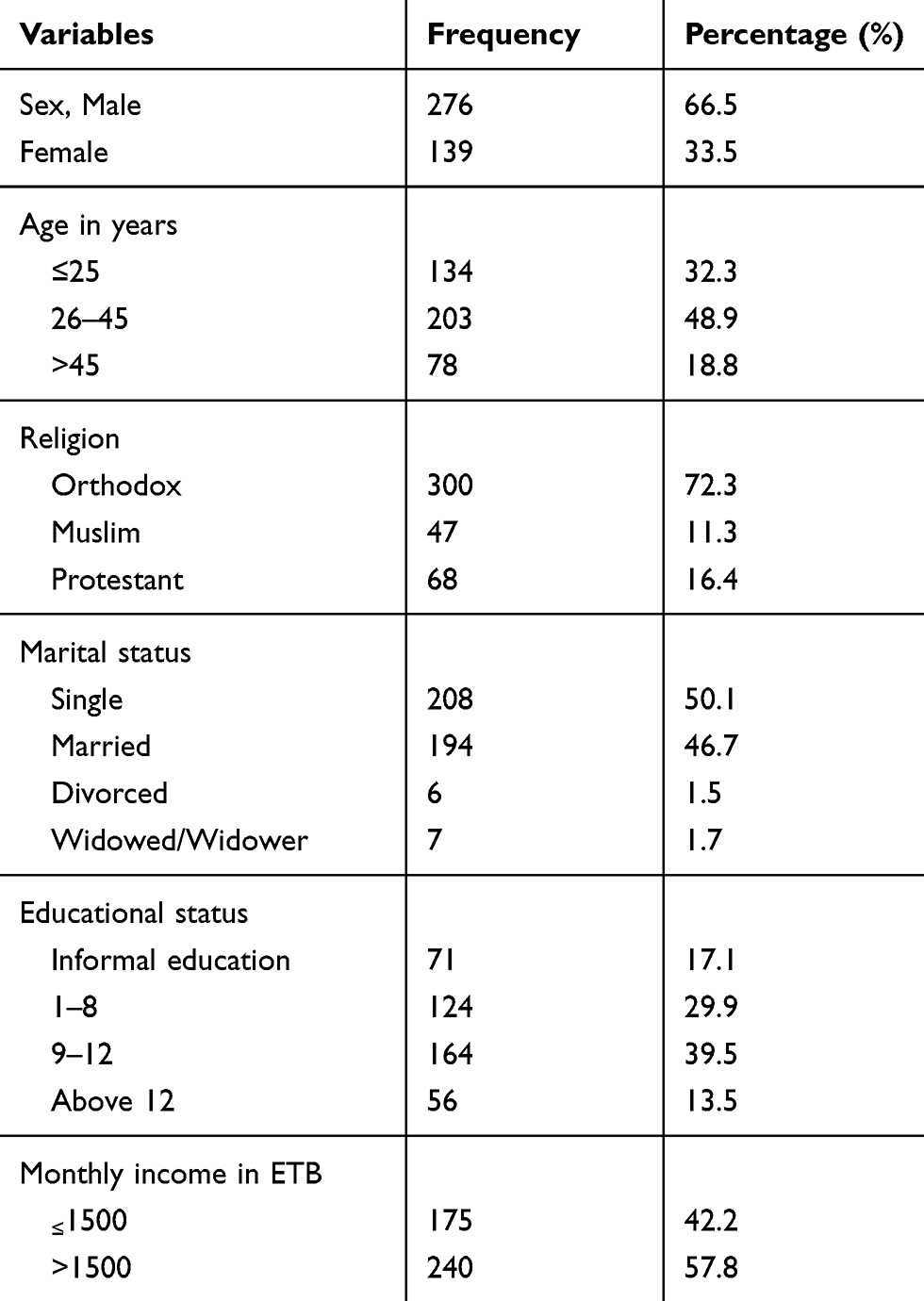 |
Table 1 Socio-Demographic Characteristics of Flour Mill Factory Workers in Addis Ababa, Ethiopia, 2019 |
Work-Related Characteristics of Flour Mill Workers
Out of 415 respondents, 331 (79.8%) of the respondents had less than ten years (≤10 years) work experience in flour milling factory, and the majority (92%) of the study participants worked below eight hours (≤8 hours) per a day. Three hundred ninety-four (94.9%) of the respondents worked above five days (>5) per week, and 126 (30.4%) flour mill workers had a past occupational history in dusty areas before they were employed in this flour milling factory. Regarding the previous history of respiratory diseases, which is confirmed by a physician, Sixty-two (14.9%) of the respondents had a history of respiratory illnesses; out of them, 49 (79%) of the respondents were males. Study participants who had: asthma 15 (24.2%), chronic bronchitis 19 (30.6%), emphysema 21 (33.9%), and TB 7 (11.3%) were found (Table 2).
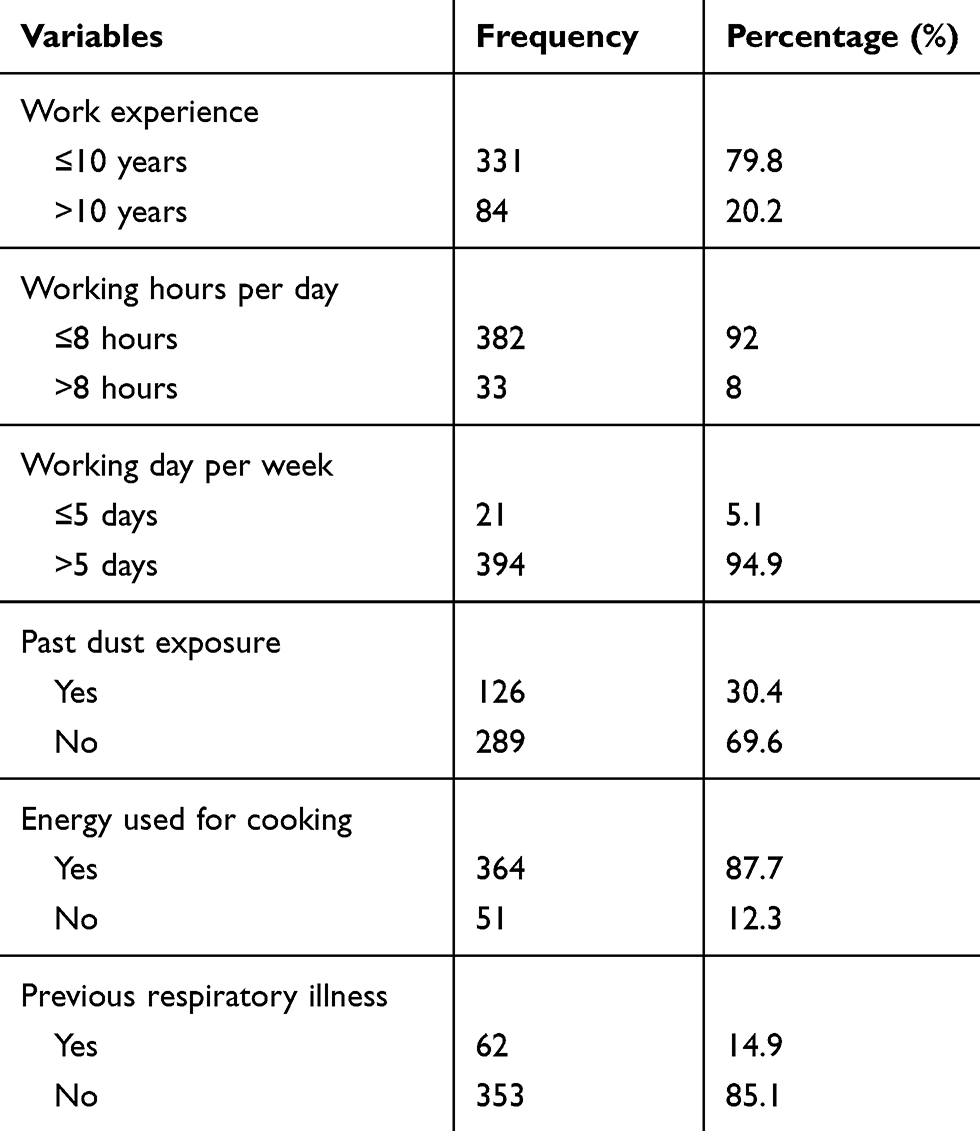 |
Table 2 Workplace Factors of the Flour Mill Factory Workers in Addis Ababa, Ethiopia, 2019 |
Regarding the type of fuel used for cooking as a primary source, 364 (87.7%) of the participants prepared food at home. Of these 364, one hundred eighty-five (50.8%) of participants used biomass (including wood, coal, and gas), and 179 (49.2%) participants used electricity as a primary source. Out of 415, one hundred fifty-two (36.6%) of the respondent were worked in the production department; the rest respondent worked in packing (22.2%), loading and unloading (15.2%), machine operator (14.7%) and cleaning (11.3%) departments.
Individual/Behavioral Characteristics of Flour Mill Workers
Out of 415 respondents, 93 (22.4%) of respondents were used pieces of cloth as personal protective equipment. But none of them reported using proper respiratory protective devices. Regarding the smoking behavior of individuals, only 23 (5.5%) study participants had a history of cigarette smoking, of the 23 ever smokers, 7(30.4%) of the respondents were current smokers. Regarding occupational safety training, 123 (29.6%) respondents taken the training, and 129 (31.1%) of the participant were supervised by professionals on occupational health and safety issues. One hundred forty-one (47.2%) of the reasons mentioned by the respondents for none use of PPE was not available in the workplace (Figure 1).
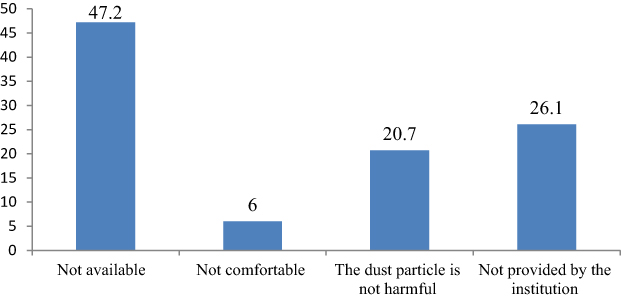 |
Figure 1 Reason for not using personal protective devices among flour mill factory workers in, Addis Ababa; Ethiopia, 2019. One hundred forty-one (47.2%) of the reasons mentioned by the respondents for not using of PPE was not available in the workplace. Whereas the rest of the participants were said not provided by the institution (26.1%), the dust particle is not harmful (20.7), and not comfortable to use (6%). |
Prevalence of Chronic Respiratory Health Symptoms Among Flour Mill Workers
The overall prevalence of chronic respiratory health symptoms among flour mill workers was 242 (58.3%), (95% CI; 53.7–63.4) with the prevalence of cough 114 (27.5%), phlegm 97 (23.4%), wheezing 85 (20.5%), nose irritation 109 (26.3%), sneezing 141 (34%), shortness of breath 116 (28%) and chest pain 59 (14.2%). The prevalence of chronic respiratory health symptoms among males was 159 (65.7%), and the prevalence of chronic respiratory health symptoms among production (milling) workers was 102 (42.12%). The prevalence of chronic respiratory health symptoms among the age of 26–45 was 117 (48.3%), and the prevalence of chronic respiratory health symptoms among married participants was 132 (54.5%). The prevalence of chronic respiratory health symptoms among participants who did not take training and did not use personal protective devices was 71.9% and 81.8%, respectively (Table 3).
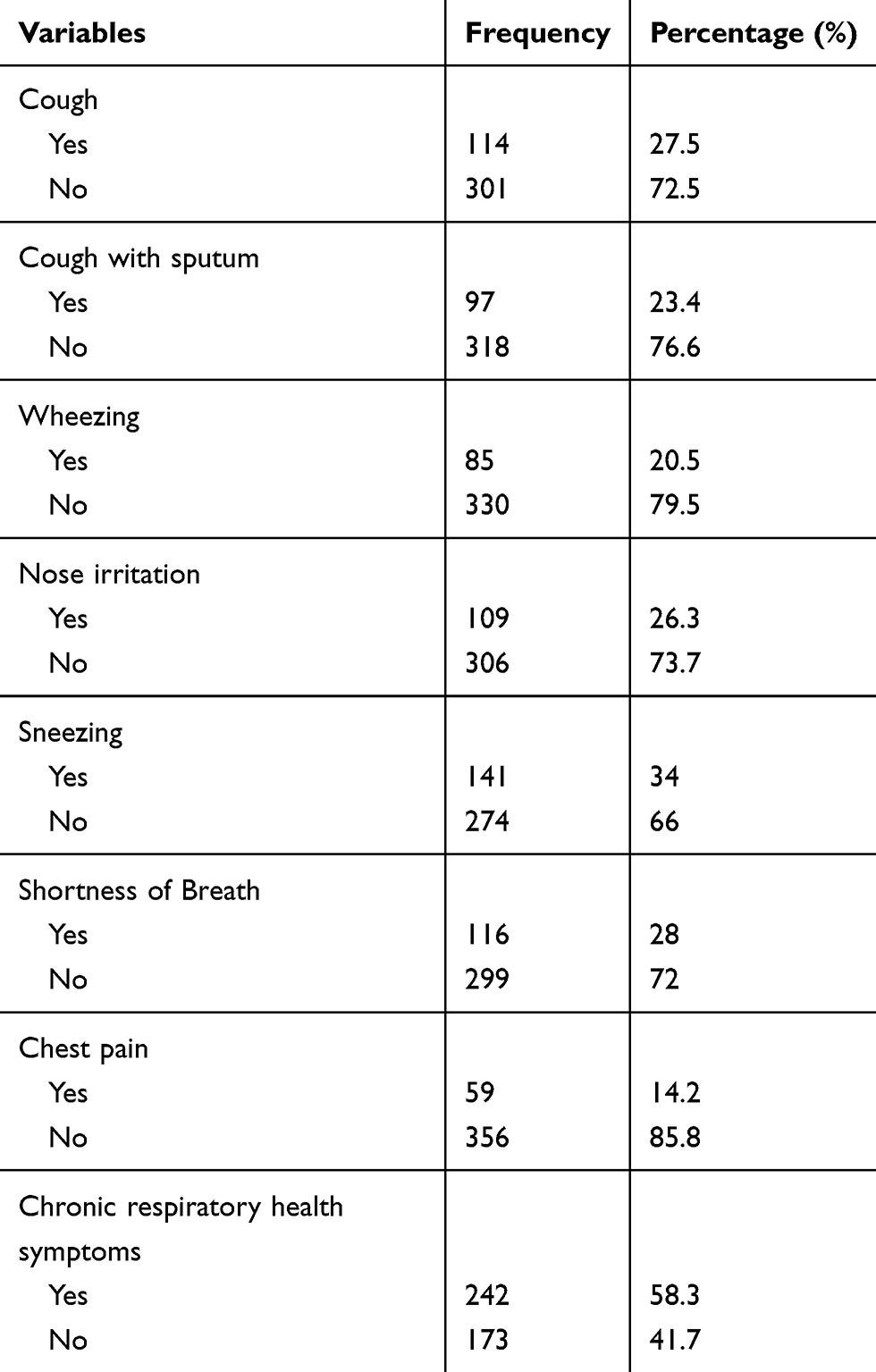 |
Table 3 Prevalence of Respiratory Health Symptoms Among Flour Mill Factory Workers in Addis Ababa, Ethiopia, 2019 |
Factors Associated with Chronic Respiratory Symptoms Among Flour Mill Workers
Age was significantly associated with chronic respiratory health symptoms among flour mill factory workers. The odds of developing chronic respiratory health symptoms among workers with the age of 26–45 (AOR=1.95, 95%CL; 1.17–3.24) and >45 (AOR=12.33, 95%CL; 4.39–34.64) years were 1.95 and 12.33 times significantly higher than workers with the age of ≤25 years, respectively.
The average monthly income was significantly associated with chronic respiratory health symptoms among flour mill workers. The odds of developing chronic respiratory health symptoms among workers with a monthly income of ≤1500 ETB (AOR=1.68, 95%CL; 1–2.79) were 1.68 times significantly higher than workers with a monthly income of >1500 ETB.
History of dust exposure was significantly associated with chronic respiratory health symptoms among flour mill factory workers. The odds of developing chronic respiratory health symptoms were 1.86 times significantly higher among workers who had worked in a dusty job before engaging in these factories than workers not worked in a dusty work environment before (AOR=1.86, 95% CL; 1.08–3.21).
Employees used pieces of cloths instead of respirator/dust mask as PPE was significantly associated with chronic respiratory health symptoms among flour mill factory workers. Flour mill workers who used pieces of cloths had 56% less likely to develop chronic respiratory symptoms (AOR = 0.44, 95% CI; 0.26–0.84) than workers who did not use pieces of cloths.
The work experience of flour mill workers was significantly associated with the development of chronic respiratory health symptoms. The odds of developing chronic respiratory symptom(s) were 2.58 times substantially higher among workers who had work experience of >10 years (AOR=2.58, 95%CL; 1.-6.62) than workers who had work experience of ≤10 years (Table 4)
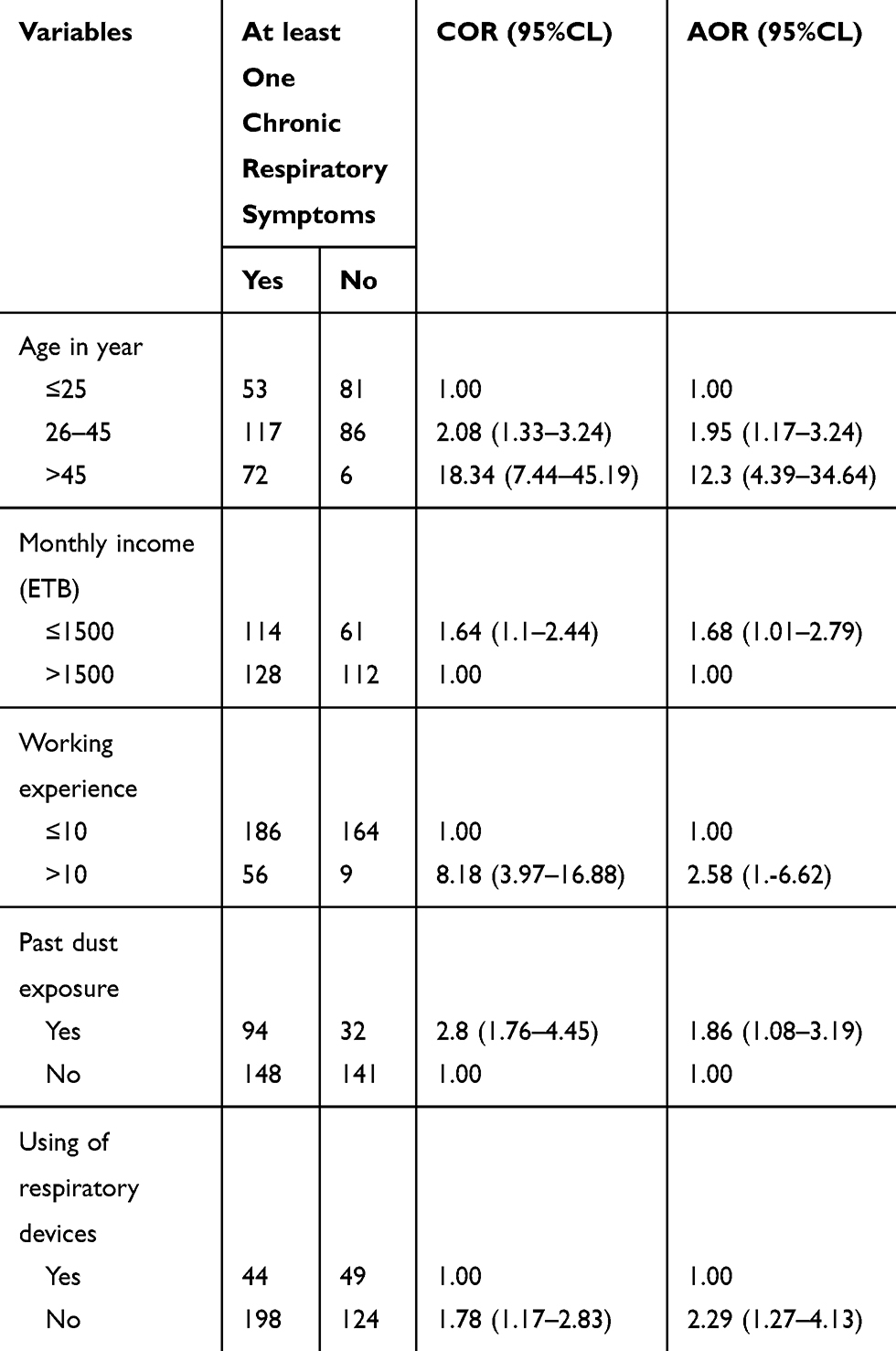 |
Table 4 Factors Associated with Chronic Respiratory Health Symptoms Among Flour Mill Factory Workers in Addis Ababa, Ethiopia, 2019 |
Environmental Factors on Flour Mill Workers
The study’s observational findings indicated that flour dust was accumulated on the walls, ceiling, floors, and machines of different working areas. Especially very high dust accumulated in the flour mill and packing department of flour mills as fine organic flour dust gets airborne in the indoor environment of the flour mills. Due to this, workers easily inhaled heavy dose of flour dust. The reason for high dust was due to a lack of dust absorber or local exhaust ventilation. The workplaces of flour mills were very congested, and above six machines were found in one room and perform different activities each. There were no employees who were using proper personal protective mask/respirator. The organizations were provided pieces of cloths that were tied on the neck of workers to protect the entry of flour dust particles. But most of them did not use even those pieces of cloth due to a lack of sufficient supply. Most of them did not use the provided piece of clothes since some of them believed it reduces performance, some of them said it is not comfortable, and the other reason was inefficient for protecting the dust particles. Most of the females were used the provided piece of cloth in the workplace. Even though the organization did not provide PPE, females also used their own cloths for protecting themselves from flour dust.
The nature of the house was very old, and the floors were made up of woods, and it easily accumulates the dust. The state of natural and mechanical ventilation, design of the machine, and high production rate had an impact on dust exposure. Individual behavior was observed; the standing position of some workers was very close to the machines and worked different working activities. The type of sack (bag) used for packing also had an impact (the dust was higher when they used old sack (bag) than new sack), which produces a massive amount of dust concentration. As a result, they are continuously exposed to a heavy concentration of flour dust.
Flour mill workers have similar exposure levels in each department, but some of the workers were performing their duty in standing position, which is very close to the machines, some of the workers perform additional activities, so it increases the exposure for the dust. Flour dust was found in any corners of the working place even outside the rooms, which perform different activities. The workplace area is very congested, has poor ventilation, and used a very old machine, which increases dust concentration. Flour dust exposure within the different departments of this study varied considerably between flour mill factories based on the current study, which was assessed by observational checklist and the standard questionnaires. Flour mill workers who were working in the production (milling) section were highly exposed to flour dust than the other departments. On the other hand, flour mill workers who engaged in machine operating were less exposed to flour dust comparing to the other departments.
Discussion
The result of the current study showed that the overall prevalence of chronic respiratory health symptoms among flour mill factory workers was 58.3% (95% CL; 53.7–63.4). This study was in line with a study done in Ethiopia, Hawassa, among flour mill factory workers with a prevalence of (56.6%).17 But comparatively higher than the previous study conducted in the UK, the prevalence of respiratory symptoms among flour millers was 22%.18 This difference could be due to the variation in the definition of the outcome variable18 used only the development of upper respiratory tract, allergy, cough, and nose irritation. While this study used the development of cough, cough with sputum, sneezing, nose irritation, wheezing, shortness of breath, and chest pain. Another reason could be that no one used any respiratory protective devices, and only (22.4%) workers used pieces of cloth in this study. The observed difference could be explained by the study setting in which the study was done, and the sample size of the current study was large. The finding of this study revealed that the prevalence of chronic respiratory symptoms such as cough (27.5%), cough with sputum (23.4%), wheezing (20.5%), nose irritation (26.3%), sneezing (34%), shortness of breath (28%) and chest pain (14.2%) was in line with the study done in Hawassa among flour mill workers.17 But comparatively lower than the study done in North West Ethiopia, in Kola Diba town with cough (42.1%), wheezing (35.7%), sneezing (64.9%), and chest pain (17.5%).19 The difference might be due to the type of factory. Since the study was done in Kola Diba was conducted in local flour mill workers. Still, this study was done in large-scale industry which uses advanced machine than that of the local flour mill, so the local flour mill has more dust than current study and in local flour milling manual working is common. Still, in this study, most of the activities were covered mechanically. In addition, the difference could be due to the local/place where Kola Diba is located on the rural side compared to this study area, and the workers may lack awareness. The present study suggested that the prevalence of cough (27.5%) was consistent with the previous study conducted in Addis Ababa among local flour milling workers (27.7%), but the prevalence of this study was higher than the previous study where cough with sputum (11.1%), wheezing (14.3%), shortness of breath (14.8%) and no chest tightness was observed.20 The observed difference might be due to the small sample size in the previous study and conducted only on male workers. The high production rate in the current study also the other reason for the high prevalence of chronic respiratory symptoms.
This study suggested that age of flour mill workers was significantly associated with chronic respiratory symptoms (age group, 26–45 years) (AOR=1.95, 95% CL; 1.17–3.24) and >45 years (AOR=12.33, 95% CL; 4.39–34.64) which was consistent with the previous study conducted in Egypt among flour mill workers in 2013 (p<0.05).11 The difference between the age group might be due to the variation in the appropriate utilization of nose/mouth mask, ie, the young people may wear it properly while the old people may have a misconception on the nose/mouth mask utilization. Another reason could be as age increases individual immunity decrease. However, age is not significantly associated with the previous study conducted in Ethiopia, Hawassa, among flour mill factory workers.17
This study suggested that the monthly income of the participants was significantly associated with the development of chronic respiratory health symptoms among flour mill workers with a monthly income of ≤1500 (ETB) (AOR =1.68, 95% CL; 1.01–2.79). This finding indicated that workers with a monthly income of ≤1500 were 1.68 times more likely than workers with a monthly income of >1500 ETB to develop chronic respiratory health symptoms. This study was similar to the study conducted in Finland among the low socio-economic status population, which indicated that a population with low income develops chronic respiratory symptoms than with high-income populations.21 This finding may be due to those workers with a monthly income of less than 1500 ETB works extra time to get a bonus or an additional fee. This should be because exposures to flour dust for a long time (hours) enhanced dust accumulation in the respiratory system; thus, workers can develop chronic respiratory symptoms.
The current study found that workers with previous dust exposure were significantly associated with the development of chronic respiratory health symptoms than workers with no past dust exposure (AOR=1.86, 95% CL; 1.08–3.21). This study is similar to the study done in Tanzania among the sunflower oil industry, which stated that previous dusty jobs are three times more likely to have difficulty breathing and breathlessness as the respiratory health symptoms than free from the previous dusty job.22 This evidence can be explained by the fact that workers with previous exposure ignore to use personal protective equipment because they think they adapt the dust. This statistical significance could be because the workers might have previously worked in dusty jobs identified to cause the respiratory problem, so this may lead to the aforementioned respiratory tissue physiologic change in later life and exacerbate the occurrence of respiratory symptoms.
Our study found that there was a statistically significant association between chronic respiratory symptoms and the duration of employment. Workers with work experience >10 years were significantly associated with the development of chronic respiratory symptoms (AOR=2.58, 95% CL; 1.00–6.62). This finding was in line with the study done in Ethiopia and Egypt (Duration of employment was found to be an important factor that influenced the prevalence of respiratory symptoms among flour mill workers (p=0.0027)).10,17 This could be due to increased dust accumulation in the respiratory system, long-term exposure leading to airway limitation, and workers with high work experience who may not use PPE due to ignorance.
This study revealed that respiratory protective device utilization was significantly associated with the development of chronic respiratory health symptoms. Workers who did use pieces of cloths to cover their nose and mouth while at work were 56% less likely to develop chronic respiratory health symptoms than workers who did not use pieces of cloths (AOR = 2.29 95% CI; 1.27–4.13). Respiratory protective equipment utilization behavior of the flour mill factory workers was very low. Even majority of workers agreed on the importance of RPE using for preventing themselves from flour dust particles, but the factories did not supply RPE for workers and which is similar with the result of the study done in Hawassa, India and Nigeria flour milling factory workers13,17,23. This is maybe due to the lack of standardized respiratory protective devices used in those factories because no one was used any respiratory protective device rather than pieces of cloth, and the equipment was not classified according to the quality of protection. Yet the usage of pieces of cloths in this study was (22.4%), which is lower than the study done in Tanzania (55.8%).22 This difference may be due to a lack of awareness on the utilization of personal protective equipment while at work and lack of occupational health and safety training in the present study.
Statistically, a significant association was detected between the presence of respiratory symptoms and the work section. Workers in milling (AOR=3.24, 95% CL; 1.54–6.82) and packing (AOR=2.42 95% CL; 1.06–5.49) sections were more likely to develop chronic respiratory symptoms than workers in machine operating sections. This finding was inconsistent with the previous study conducted in Ethiopia, Hawassa city, which reported that mixing workers had a high prevalence of chronic respiratory symptom than milling section17 but in line with the study done in Iraq and Egypt, which reported that packing and milling departments had high chronic respiratory symptoms than other departments.10,24 This could be due to differences in working conditions such as ventilation type, machine type, number of machines present in one room, and use of the personal protective device. Another reason could be participants who were working in packing and milling had direct contact with the fine products of flour, which can be easily inhaled.
Limitation of the Study
Respondents recall bias, and interviewers’ bias was possibly introduced while interviewing the study participants. Since this study used a cross-sectional study design, no conclusive remarks can be drawn on causal-outcome associations between flour dust exposure and adverse respiratory health effects in such studies. So it is good if the personal dust exposure level is added to know individual exposure by using measuring personal dust exposure.
Conclusions and Recommendations
The overall prevalence of chronic respiratory health symptoms among flour mill factory workers was high. Respiratory symptoms were found to be more common among older age, low monthly income, with past dust exposure, milling and packing work section, long work experience (>10 years), and not using respiratory protective devices workers. Most flour mill workers were unaware of the effect of exposure to flour dust. An unhealthy condition in the workplace environment was observed, and none of the workers used respiratory protective devices.
Regular supervision of a flour mill factory is needed. They should issue detailed regulations that can be legally binding and should monitor to ensure the implementation of these regulations.
In the long run, it is recommended to apply engineering control to reduce dust concentration at the workplace, ie, local exhaust ventilation or dust absorber, modification of the old machine, or better to change by new machine and the workplace should be designed with easy to clean floor. It is advisable to apply the administrative control method, ie, policy and producers should be posted and practice accordingly, job rotation of workers, occupational health and safety training should regularly give, giving Incentives or any reward is better for those who have good work practices which minimize exposure. Managers should ensure continuity and effective inspection and maintenance programs. It is recommended to provide standard and adequate respiratory protective devices and better to encourage the workers to utilize it.
Workers should keep workplace hygiene and should properly wear respiratory protective equipment supplied by the institution. They should apply policy and producers which are posted in the workplace and better to develop good working practice. Further study is advised to use a longitudinal study for investigating personal dust exposure level, chronic respiratory symptoms, and lung function changes among flour mill workers.
Abbreviations
AOR, adjusted odds ratio; ATS, American Thoracic Society; CI, confidence interval; COPD, chronic obstructive pulmonary disease; COR, crude odds ratio; Epi Info, Epidemiological Information package; ETB, Ethiopian Birr; ILO, International Labor Organization; NCDs, non-communicable diseases; OR, odds ratio; PPEs, personal protective equipments; RPE, respiratory protective equipment; SD, standard deviation; SPSS, Statistical Package for Social Sciences; TB, tuberculosis; WHO, World Health Organization.
Data Sharing Statement
The dataset used and analyzed during this study are available from the corresponding authors on reasonable request.
Ethics Approval and Consent to Participate
Ethical clearance and approval was taken from Addis Ababa University ethical review committee. Permission letter was obtained from flour mill factories managing director for requesting facilitation to conduct a research study. The study participants who fulfilled the criteria for the study and agreed to participate were given written consent and signed before data collection started. Issues of rights, privacy, and confidentiality were ensured during data collection period. Participants had the right to participate or not and to withdraw at any time when they feel discomfort. The study participant did not get a direct benefit like money but they become a beneficiary in the future from the study.
Acknowledgment
Above all, I would like to thank the Almighty God for his unreserved and unconditional love and Kindness and for keeping me in health and strength to complete this thesis work. I also extend my grateful thanks to the management of flour mill factories, all data collectors, supervisor and study participants for their cooperation during data collection. I would like to thank Addis Ababa University School of Public Health. Last but not the least, my sincere gratitude goes to my beloved families and friends for continuous encouragement and moral support during the thesis work.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
Addis Ababa University. “The funder has no role in study design, data collection and analysis, decision to publish, preparation of the manuscript”.
Disclosure
All authors declared that they have no competing interests for this work.
References
1. Goelzer B. Hazard Prevention and Control in the Work Environment: Airborne Dust. Geneva: World Health Organization; 1999.
2. WORKSAFE. Workplace exposure standards and biological exposure indices on flour dust, November 2019. [Cited 2020 May 20]. https://worksafe.govt.nz/topic-and-industry/work-related-health/monitoring/exposure-standards-and-biological-exposure-indices/
3. Bagheri Hosseinabadi M, Krozhdeh J, Khanjani N, Zamani A, Ranjbar M, Mohammadian M. Relationship between lung function and flour dust in flour factory workers. Int J Community Med Res. 2013;2(2):138–146.
4. Kakouei H, Mari OH. Exposure to Inhalable Flour Dust and Respiratory Symptom of Workers in a Flour Mill in Iran. 2005.
5. Esterhuizen T, Hnizdo E, Rees D. Occurrence and causes of occupational asthma in South Africa – results from SORDSA’s occupational asthma registry, 1997–1999. S Afr Med J. 2001;91(6):509–513.
6. World Health Organization. Global Status Report on Non-Communicable Diseases. Geneva, Switzerland: World Health Organization; 2014.
7. Mariammal T, Amutha A, Sornaraj R. Work related respiratory symptoms and pulmonary function tests observed among construction and sanitary workers of Thoothukudi. Int J Pharmtech Res. 2012;4(3):1266–1273.
8. Subbarao P, Mandhane PJ, Sears MR. Asthma: epidemiology, etiology and risk factors. Cmaj. 2009;181(9):E181–E90. doi:10.1503/cmaj.080612
9. Ige O, Awoyemi B. Respiratory symptoms and ventilatory function of the bakery worker in Ibadan, Nigeria. West Afr J Med. 2002;21(4):316–318.
10. Mohammadien HA, Hussein MT, El-Sokkary RT. Effects of exposure to flour dust on respiratory symptoms and pulmonary function of mill workers. Egypt J Chest Dis Tuberc. 2013;62(4):745–753. doi:10.1016/j.ejcdt.2013.09.007
11. Growth N. Transformation Plan II (2015/16-2019/20). Vol I the Main Text Addis Ababa. 2016.
12. Adugna A. Demography and Health Organization Population Data Sources wwwEthio. 2007:34–52.
13. Ghosh T, Gangopadhyay S, Das B. Prevalence of respiratory symptoms and disorders among rice mill workers in India. Environ Health Prev Med. 2014;19(3):226–233. doi:10.1007/s12199-014-0384-8
14. Asfaw S, Enquselassie F, Tefera Y, Gizaw M, Wakuma S, Woldemariam M. Determinants of chronic respiratory symptoms among pharmaceutical factory workers. J Trop Med. 2018;2018.
15. Stenton C. The MRC breathlessness scale. Occup Med (Chic Ill). 2008;58(3):226–227. doi:10.1093/occmed/kqm162
16. Ryan H, Trosclair A, Gfroerer J. Adult current smoking: differences in definitions and prevalence estimates—NHIS and NSDUH, 2008. J Environ Public Health. 2012;2012.
17. Ashuro Z. Comparative Cross Sectional Study on Chronic Respiratory Symptoms, Pulmonary Function, and Associated Factors Among Flour and Pepsi Factory Workers in Hawassa City. Southern Ethiopia: Addis Ababa Universty; 2018.
18. Smith T, Parker G, Hussain T. Respiratory symptoms and wheat flour exposure: a study of flour millers. Occup Med (Chic Ill). 2000;50(1):25–29. doi:10.1093/occmed/50.1.25
19. Demamu S, Ayele F, Tilahun L, Fekadu S, Teklehaimanot W, Dawit Y. Epidemiologic survey of respiratory symptoms among workers of small grain mills and others. Ethiop J Health Dev. 1998;12(3).
20. Demeke D. Assessment of Respiratory Symptoms and Pulmonary Functions Among Workers of Flour Mills. Addis Ababa, Ethiopia: Addis Ababa University; 2017.
21. Kanervisto M, Vasankari T, Laitinen T, Heliövaara M, Jousilahti P, Saarelainen S. Low socioeconomic status is associated with chronic obstructive airway diseases. Respir Med. 2011;105(8):1140–1146.
22. Buliga V, Rongo LM, Mamuya SH. Dust exposure and respiratory health symptoms among workers in small scale sunflower oil industry in Singida, Tanzania. Int J Res. 2017.
23. Iyogun K, Lateef SA, Ana GR. Lung function of grain millers exposed to grain dust and diesel exhaust in two food markets in Ibadan Metropolis, Nigeria. Saf Health Work. 2019;10(1):47–53. doi:10.1016/j.shaw.2018.01.002
24. Ajeel NA, Al-Yassen AK. Work-related allergic disorders among flour mill workers. Med J Basrah Univ. 2007;25(1):29–32. doi:10.33762/mjbu.2007.48127
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.