")
Back to Journals » Journal of Blood Medicine » Volume 13
Assessment of Blood Transfusion Utilization and Patient Outcomes at Yekatit-12 Hospital, Addis Ababa, Ethiopia
Authors Tewabe H , Mitiku A, Worku H
Received 21 December 2021
Accepted for publication 16 March 2022
Published 29 March 2022 Volume 2022:13 Pages 171—180
DOI https://doi.org/10.2147/JBM.S355178
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Haymanot Tewabe,1 Asaye Mitiku,2 Habtamu Worku3
1Department of Medical Laboratory Sciences, College of Health Science, Debre Markos University, Debre Markos, Ethiopia; 2Department of Medical Laboratory Sciences, College of Health Science, Dilla University, Dilla, Ethiopia; 3Department of Medical Laboratory Sciences, ECUSTA Health Science College, Addis Ababa, Ethiopia
Correspondence: Haymanot Tewabe, Email [email protected]
Background: The goal of blood transfusion is to provide a safe, sufficient, and timely supply of blood components to the recipients by ensuring that donation is safe and no harm to the recipient. So the current study was aimed to assess blood transfusion utilization and its outcome in patients at Yekatit-12 Hospital, Addis Ababa, Ethiopia.
Methods: A cross-sectional study was conducted from May 01 to July 30, 2021, on 616 individuals who have requested blood transfusion at Yekatit-12 Hospital, Addis Ababa, Ethiopia. Information on blood and blood component utilization was collected by using a checklist. Finally, data were analyzed using SPSS version 21.0, and those variables in which P-value is less than 0.05 were considered statistically clinically significant.
Results: A total of 1540 cross-match units were requested for 616 (53.2% male) patients with a mean age of 43 years. Out of 1540 cross-matched blood units, 1498 units of blood were transfused for 615 individuals with a mean of 2.43 units. The most widely used blood component was whole blood 694 (46.3%) and 1252 (83.6%) of the blood unit were “RH” positive. From a total of 68 (11.1%) none improved reported cases, 48 (10.5%) were those transfused with whole blood transfusion. The proportion of improvement after transfusion according to the service ranged from 83.3.0% to 100% and no post-transfusion reactions were reported. A significant improvement was seen in the hematological profile (hemoglobin, red blood cells, hematocrit, platelets, and white blood cells) findings of the transfused individuals after blood unit transfusion (P < 0.05).
Conclusion: The overall utilization rate and improvement status after transfusion were high even if the utilization rate has some limitations. The overall ratios of cross-match to transfusion ratio, transfusion probability, and transfusion index were 1.03, 99.8%, and 0.97, respectively.
Keywords: blood transfusion, utilization, outcome, Yekatit-12 Hospital, Ethiopia
Background
Blood transfusion is a procedure in which whole blood or parts of blood are put into a patient’s bloodstream through a vein to compensate for any type of blood loss or to treat anemia.1 As recent WHO and different national blood bank reports indicated, the rational use of blood has increased and it needs evidence-based patient blood transfusion management and transfusion medicine practice.2 Many clinical data indicate transfusion of blood components is the most common medical procedure in health institutes because the demand for safe blood transfusion is increasing with the increment of a blood disorder.1 On the other hand; if blood transfusion is misused, it may expose recipients to undesirable risks, which causes additional costs for the health system and waste a scarce resource.3
As Many findings indicated, blood transfusion in the clinical area has significant importance and its therapeutic benefit was achieved by taking and implementing evidence-based activities through continuous review and evaluation of demographic and clinical characteristics, clinical response of transfusion recipients, and appropriate clinical utilization of blood and blood products.2
Patient Blood Management (PBM) takes an individualized, multidisciplinary approach to the management of a patient’s blood after transfusion of blood components, through the development of a management plan to optimize a patient’s blood, minimize blood loss, and optimize tolerance of anemia.4 Although blood transfusion order is a common practice in most health care institutes, no clear data is indicated on the utilization and outcomes of blood transfusion. So the assessment of utilization and outcomes of blood transfusion are vital things to provide a rational and evidence-based, case-specific practical framework to avoid unnecessary expenses imposed on patients and institutions, and thereby increases the availability of safe blood for those who are in real need. Thus this study aimed to assess transfusion utilization and patient outcomes at Yekatit-12 Hospital, Addis Ababa, Ethiopia; August 2021.
Materials and Methods
Study Area and Setting
A cross-sectional study was conducted from May 01 to July 30, 2021, at Yekatit-12 Hospital which is found in Addis Ababa; the capital city of Ethiopia under the Addis Ababa Health Bureau; to assess the utilization of blood and blood components.
Source Population
The study population was all patients who have transfused blood and blood components at Yekatit-12 Hospital during the study period.
Study Population
The study population transfused individuals and those who have full records, of blood, transfused, units of blood, the reason for transfusion, a component of transfused, CBC results before and after transfusion, and outcomes of transfusion based on WHO guidelines.
Inclusion and Exclusion Criteria
Inclusion Criteria
The study population transfused individuals and those who have full record of blood transfused, unit of blood, the reason for transfusion, the component of transfused, CBC result before and after transfusion, and outcomes of transfusion based on WHO guidelines Yekatit-12 Hospital from September 01, 2019, to May 20, 2021.
Exclusion Criteria
Recipients with incomplete records based on WHO guideline.
Sample Size Calculation and Sampling Method
Sample Size Calculation
All transfused individuals during the study period and fulfilling our inclusion criteria were included. 3 months of prospective data were collected from the records of transfused patients in all wards of Yekatit 12 Hospital from May 01, 2021, to the end of July 2021. The total number of patients who have transfused during the study period and fulfilled the inclusion criteria was 616.
Sampling Method
A simple random cross-sectional study was conducted from May 01, 2021, to July 30 2021 on transfused individuals at Yekatit-12 Hospital, Addis Ababa, Ethiopia.
Data Collection Procedure
The data was collected by using a checklist which was developed following a thorough review of the literature from different sources and including information related to the socio-demographic condition and medical status. The checklist contains sections for assessing demographics, blood transfusion-related information, and associated factors. The questions and statements are grouped and arranged according to the particular objectives that are aimed to address. Records regarding the reason for transfusion, unit of blood requested, type of blood group requested, type of blood component requested, a unit of blood cross-matched, units of blood utilized after cross-match, and outcomes of recipients after transfusion were collected by reviewing the recipient’s cards, and laboratory blood bank logbooks by using structured pretested check-list. Details including gender, age, a hematological profile of the patient, the number of units that were expired (outdated) before utilization, type and amount of blood components transfused, the health professional who ordered the transfusion, the department from which the request was issued and patient improvement status was noted. Transfused patients with the absence of clinical symptoms, with improvement in hematological profile after transfusion and/or reduced length of stay in the hospital were defined as showing better improvement.
Quality Assurance
The data were collected using a checklist after orientation has given to all data collectors regarding the procedures to be followed during the data collection by hematology experts. In addition, the collected data were reviewed and checked for completeness and consistency daily by the PI and two supervisors.
Data Analysis and Interpretation
Data was cleared, edited, checked for completeness manually, and entered to Software Package for the Social Science (SPSS) for version 20.0 for Windows® (SPSS Inc., Chicago, IL, USA for analysis. After organizing and cleaning the data, frequencies and percentages were calculated for all variables that are related to the objectives of the study. The extent of blood prescribed, utilized, and transfusion outcome was checked. The level of statistical significance was set at a 95% confidence interval. A P-value of less than 0.05 was considered statistically clinically significant. Finally, the result is presented by using tables and narrative forms.
Operational Definitions
- Recipients card: Patient cards that have blood transfusion records.
- Prescribed blood: Unit of blood requested by the physician for transfusion.
- Donated Blood: Units of blood utilized by the patient/ recipients.
- Returned Blood: Blood returned to the lab after cross-matching.
- Missed Blood: Blood was not donated by different factors.
- Moreover, the following transfusion utilization and outcome-related operational definitions were used as a guideline for this study.5,6
- Cross-match to transfusion ratio (C/T ratio) = number of units blood cross-matched to the number of units of blood transfused and a ratio of C/T less than or equal to 2.5 is considered as indicative of significant/efficient blood usage.
- Transfusion probability (TP) = calculated by the number of patients transfused divided by the number of patients cross-matched and then multiplied by 100. A TP value of greater than or equal to 30% was considered an indication of efficient blood usage.
- Transfusion index (TI) = defined by a ratio of the number of blood units transfused to the number of patients cross-matched and a TI value of greater than or equal to 0.5 or was considered as an indication of significant blood utilization.
Ethical Considerations
The study was conducted after ethical approval was obtained from the Research and Ethics Institutional Review Board of ECUSTA Health Science Institute. An official permission letter was submitted to the Addis Ababa Health Bureau and Yekatit-12 Hospital. The informed written consent was obtained for participants with ages of greater than 18 years old and informed written assent was also obtained from each participant with the age of fewer than 18 years from their parents or guardians based on Helsinki declaration or protocol before the actual data collection.
Result
A total of 1540 blood units were requested for 616 study subjects. From a total of 616 transfused patients, 328 (53.2%) were males and the rest 288 (46.8%) were females. The median age of the study subjects was 43 years, with the highest proportion (43.5%) being in the age group 18–35 years. All total 1540 blood units requested for cross-matching were cross-matched in the laboratory and 1498 blood units were transfused with a mean of unit 2.43. From a total of 1498 blood units transfused, 709 (47.3%) of the blood transfused was blood group O and 1252 (83.6%) of the blood was Rh-positive. From a total of 616 subjects, 110 (17.9%) of the patients were given four units of blood, 196 (31.8%) of the patients were given three units of blood, 160 (26.0%) of the patients were given two units of blood and the rest 150 (24.4%) of the patients were given one unit of blood. Additionally from 1540; 1127 (73.15%) of the blood transfusions were requested or authorized by specialist doctors and the rest was requested by general practitioners and specialized nurses (Table 1).
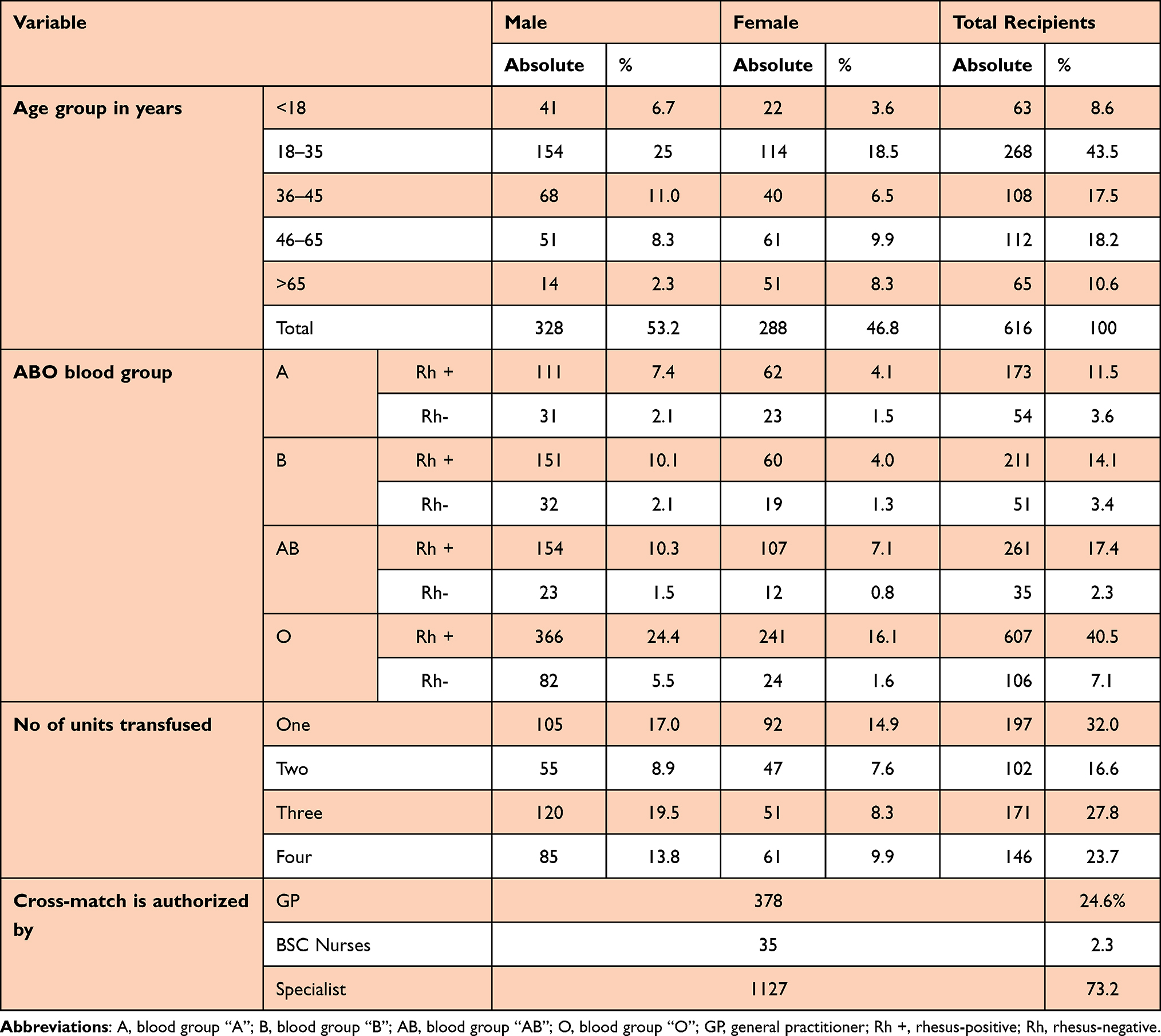 |
Table 1 Demographic Characteristics of Transfused Patients with Different Blood Components at Yekatit-12 Specialized Hospital; Addis Ababa, Ethiopia, from May 01 to July 30, 2021 |
According to this study found the most widely used blood unit component was the whole blood unit which accounted for 990 (66.1%), followed by packed red cell volume which was 208 (13.9%), and then plasma only which was 155 (10.3%), platelets only was 82 (5.5%) and more than one component was 63 (4.2) (Table 2).
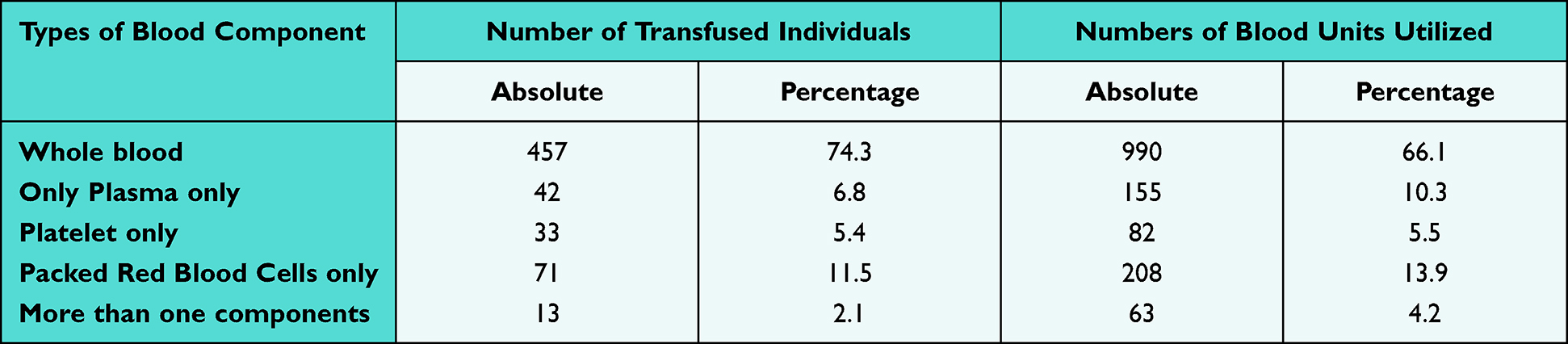 |
Table 2 Types of Blood Components Transfused with Blood from Patients Admitted in Yekatit-12 Specialized Hospital; Addis Ababa, Ethiopia, from May 01 to July 30, 2021 |
As the study findings indicated, two and more than two blood components are transfused for a single patient (like whole blood and plasma, whole blood and platelet, whole blood and PRC, and platelet and PRC, whole blood, Plasma & platelet, and whole blood, plasma and PRC) even if whole blood is the most utilized blood component more than one unit for a single individual (98.75%). In the current study, the blood component transfusion utilization, and outcome pattern at the department level was also assessed and the findings indicated that the majority of the individuals transfused were from medical wards which accounted for 239 (38.8%) and the lowest 17 (2.8%) in the maternity ward. A total of 467 (31.2%) units of blood are utilized by the medical ward; of which 231 (49.5%) were whole blood components. Furthermore, as the finding indicated, the utilization of more than one blood unit for a single person was high in this ward relative to others which accounts for 358 (27.5%) out of 1301 blood units utilized more than one unit, followed by the emergency ward which is 329 (25.3%) (Table 3).
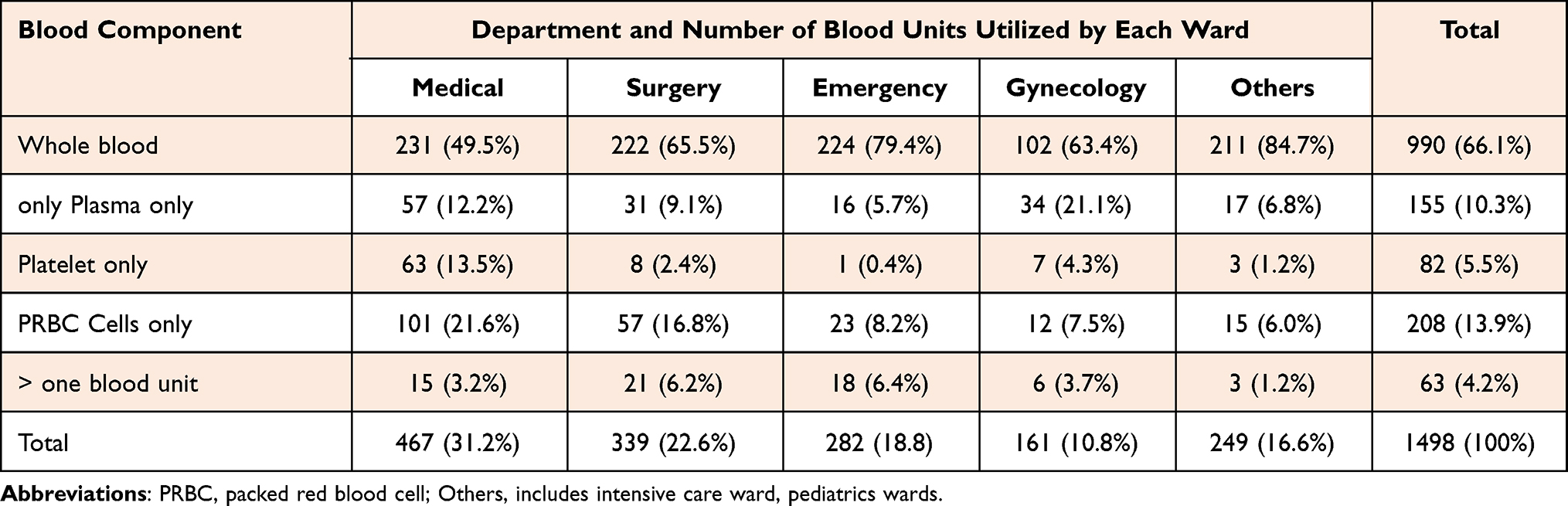 |
Table 3 Distribution of Blood and Blood Component Utilization by Different Departments at Yekatit-12 Specialized Hospital; Addis Ababa, Ethiopia, May 01 to July 30, 2021 |
Selected Hematological Parameters Both in Case of Pre-Transfusion and Post-Transfusion
In the current study, the pre-transfusion and post-transfusion hematological parameter results (hemoglobin, hematocrit, PLT, RBC index, RBC, and WBC) of transfused individuals were measured. The finding of the laboratory results for those individuals indicates better improvement in all blood parameters (Table 4). Additionally, the findings of the current research indicated a significant change in post-transfusion blood cell parameters (hemoglobin, hematocrit, PLT, RBC index, RBC, and WBC) were seen compared with the laboratory results of the pre-transfused hematological findings of the individuals (P value < 0.05).
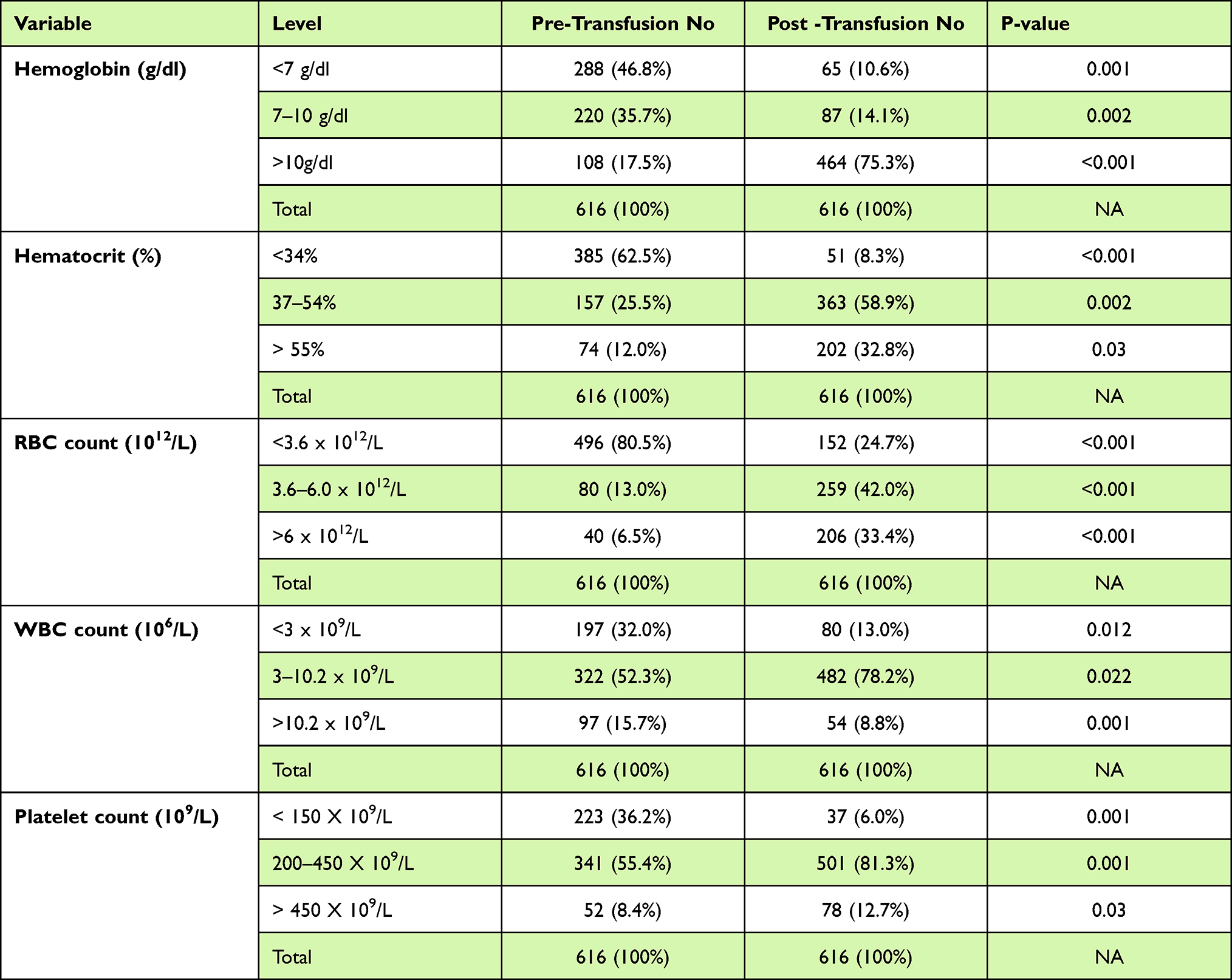 |
Table 4 Selected Hematological Parameters Before and After Whole Blood and Blood Component Transfusion at Yekatit-12 Specialized Hospital; Addis Ababa, Ethiopia, May 01 to July 30, 2021 |
Patient’s Response After Transfusion
Out of a total of 616 transfusion episodes during the study period; 525 (85.2%) of the patients showed better improvement after transfusion, 68 (11.1%) of the patients did not show improvement after transfusion and the rest 23 (3.7%) had no report regarding their response after transfusion. From a total of 457 individuals transfused with whole blood components; 396 (86.6%) cases were improved after transfusion. Out of the total, 68 (11.1%), non-improved cases; 48 (70.6%) were individuals who have transfused with whole blood components; and the rest 20 (29.4%) individuals were patients transfused with other blood component transfusions (Table 5).
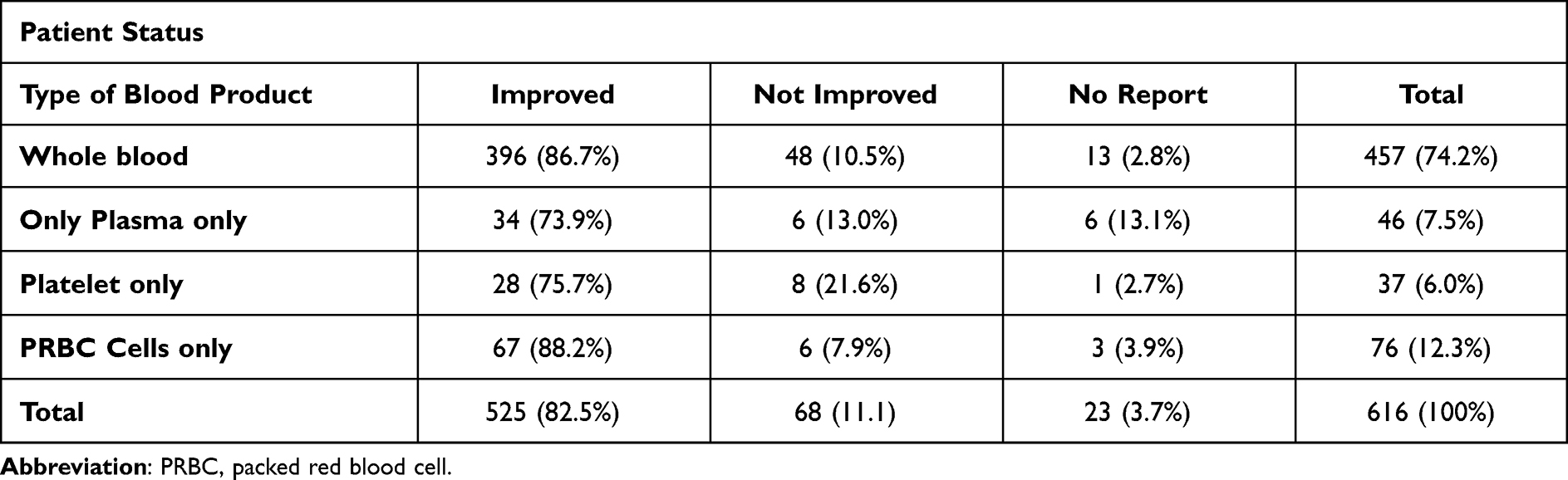 |
Table 5 Patient Improvement Status After Blood Transfusion at Yekatit-12 Specialized Hospital; Addis Ababa, Ethiopia, May 01 to July 30, 2021 (N =616) |
According to the current study finding, the improvement status in all departments was better, which were 210 (87.9%) out of 239 patients transfused in a medical ward, 152 (92.1%) out of 165 transfused patients from the surgical ward, and 79 (74.5%) out of 106 transfused patients in the emergency ward (Table 6).
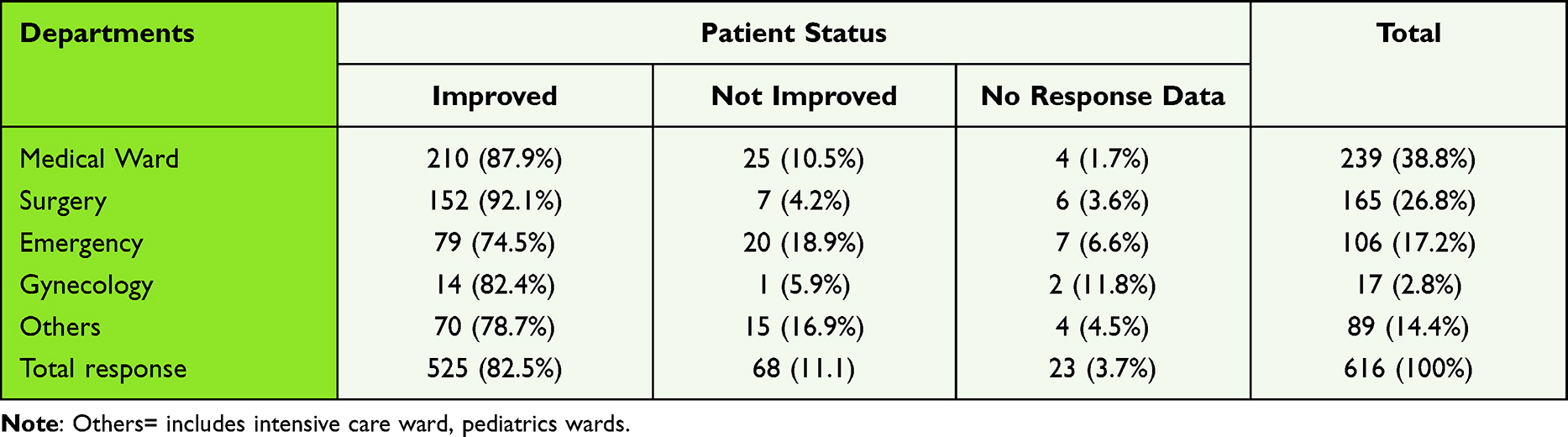 |
Table 6 Patient Improvement Status Regarding Different Departments at Yekatit-12 Specialized Hospital; Addis Ababa, Ethiopia, May 01 to July 30, 2021 (N=616) |
A total of 1540 cross-matched blood units; 1498 blood units were transfused; for 615 patients and the overall ratios of C/T, %T, and TI index were 1.03, 99.8%, and 0.97, respectively (Table 7).
 |
Table 7 Overall Blood Utilization Among Patients Transfused at Yekatit-12 Specialized Hospital; Addis Ababa, Ethiopia, May 01 to July 30, 2021 (N=616) |
As the finding of this study indicated; a significant association was seen between the hematological (hemoglobin, hematocrit, red blood cell, platelet, and white blood cells) parameters of pre-transfused results with that of post transfused result (P-value <0.05)(Table 4).
Discussions
In the current study, out of a total of 616 transfused patients, 328 (53.2%) were males and the mean age of the patients was 43 with a higher percentage in the age range 18–35 which accounts for 268 (43.5%) and this finding was similar with a study finding conducted in Gondar,7 Nigeria8 and the age group was somewhat higher with a study conducted in Jimma, Ethiopia.9 A total of 1540 blood units were requested for 616 patients from different wards in Yekatit-12 Hospital from May 01 to July 30, 2021, of which 1498 (93.7%) blood units were transfused for each patient with a mean of 2.43 blood units which is relatively in line with the finding of different studies conducted in Gondar Hospital, Northwest Ethiopia,7 higher relative to a study conducted in Jimma, Ethiopia,10 Southern Nigeria,8 Saudi Arabia11 and lower than with a cross-sectional study conducted in Ethiopia.12 From a total of 1498 blood units utilized; 990 (66.1%) were whole blood components, 709 (47.3%) of the blood transfused was blood group O type and 1252 (83.6%) of the blood was Rh-positive which is similar to the study conducted in Jimma, Ethiopia,9,10 Southern Nigeria.8
Among 1498 blood units transfused for 615 patients, 713 (47.6%) were blood group “O”, 227 (15.2%) were blood type “A”, 262 (17.5%) were blood type “B” and the rest 296 (19.8%) were blood type AB. In addition from a total of 1498 transfused blood units, most of the blood units; 1252 (83.6%) were RH positive and the rest 246 (16.4%) blood units were RH negative (Table 1). This finding was in line with the findings of the study conducted at Tikur Anbessa Specialised Hospital, Ethiopia,12 an institution-based cross-sectional study conducted in 2018 at Jimma, Ethiopia,10 a cross-sectional study conducted at Gondar Hospital, Ethiopia,7 year hospital-based study conducted in Black Lion Specialized Hospital, Ethiopia13 and a study conducted in.14
In our study the overall ratios of cross-match to transfusion ratio (C/T), transfusion probability (%T), and transfusion index (TI) were 1.03, 99.8%, and 0.97, respectively (Table 4); which indicates better utilization of blood units at different wards of Yekatit-12 Referral Hospital (C/T < 2.5%, T >30% and TI > 0.5). Similar to the current study findings; a study conducted in Jimma, Ethiopia,10 in Gondar, Ethiopia,7 in teaching hospitals of India,15 and a study conducted in Northern India16 were reported better utilization of blood units. However, the current study indicated a better utilization rate relative to a study conducted in Nigeria,14 a cross-sectional study in Rajouri,15 and a study conducted in the blood bank of Usmanu Danfodiyo University Teaching Hospital (UDUTH), Nigeria.14 In addition, the finding of the transfusion probability of the current study was indicated significant blood utilization relative to the finding of the study conducted in large tertiary hospitals in Ethiopia.12
As the findings of this study indicated; out of 615 patients, 419 (68.1%) individuals have utilized two or more than two blood units. Of which 102 (16.6%) individuals were transfused with two blood units, 171 (27.8%) individuals were transfused with three blood units, and the rest 146 (23.7%) individuals were transfused with four blood units (Table 1) and a nearly similar finding was reported by the finding of the study conducted in black lion hospital, Ethiopia [25].
Out of 615 transfused individuals; most of the patients were from the medical ward which accounts for 239 (38.9%), followed by the surgical ward which is 165 (26.8%) (Table 6), and this finding was relatively in line with the finding of a study conducted by.10 Whole blood was the abundantly transfused blood component (55.9% in a medical ward, 65.5% in the surgical ward, 79.2% in an emergency ward, 63.4% in gynecology wards, and 84.7% in other words) (Table 3) which is in line with studies finding conducted in Ethiopia,12 in Gondar, Ethiopia,7 and BLSH, Ethiopia.13
In the current study; a significant association was seen between the hematological (hemoglobin, hematocrit, red blood cell, platelet, and white blood cells) parameters of pre-transfused results with that of post transfused result (P-value <0.05) (Table 4) which is in line with the study conducted in India,17 in Italy18 and a study conducted in BLSH, Ethiopia.13 The overall transfusion rate of this study was 97.3% which is higher than a study conducted in India which reports 90.0%,19 retrospective study conducted in India which reports 62.6%,20 a study conducted in Jimma, Ethiopia which reports 82.1%,10 a study conducted in Gondar, Ethiopia which reports 47%7 and nearly similar with a study finding conducted in Nigeria which reports 94.42%.14 However, in the current study, the utilization of blood components rather than whole blood was minimal, which is less than 12.5%. The main reason for this may be the backward tradition of preparation of blood components based on the requirement of the patient. This was due to the use of whole blood as a sole component for transfusion in resource-limited areas making whole blood is seldom used as a component for blood transfusion rather than its therapeutic products.
Conclusion
Out of 616 individuals requested for cross-match with a mean age of 43 years, 53.2% were males; 1498 blood units were transfused for 615 individuals with an overall average transfused blood unit of 2.43. In the current study, the most utilized blood type was blood group O (47.6%), and RH type was RH positive (83.6%). The most utilized blood component was the whole blood component which accounts for 55.9% in a medical ward, 65.5% in the surgical ward, 79.2% in an emergency ward, 63.4% in gynecology wards, and 84.7% in other wards.
In the current study; from 615 transfused individuals, 68.1% individuals have utilized two or more blood units (16.6% individuals have utilized two blood units, 27.8% individuals have utilized two blood units three blood units, and 23.7% individuals have utilized two blood units four blood units). Also in our finding; a significant improvement was seen in hematological parameters (hemoglobin, hematocrit, red blood cell, platelet, and white blood cells) after transfusion (P-value <0.05). The overall C/T, %T, and TI were 1.03, 99.8%, and 0.97, respectively; which indicates better utilization of blood units (C/T < 2.5%, T >30% and TI > 0.5). The overall prevalence rate of improvement status after transfusion was greater than 73.9 and the overall prevalence rate of non-improvement status after transfusion was 11.11%. The study also showed that there were no post-transfusion reactions during the study period.
Recommendations
According to our findings, we would like to recommend transfusing separated blood components will be more advantageous than transfusing whole blood to reduce the shortage and waste of blood. Training on blood component usage for those engaged in the service is mandatory to use this precious product economically. Finally, regular auditing of blood and blood component utilization could improve the transfusion service and alleviate an increased demand for blood and blood components.
Abbreviations
BLSH, Black Lion Specialized Hospital; CDC, Center of Disease Control Center; CTR or C/T, cross-match to transfusion ratio; ECUSTA, Ethiopian Catholic University Institute; HBV, hepatitis B virus; HCV, hepatitis C virus; Hgb, haemoglobin; HIV, human immunodeficiency virus; NBB, National Blood Bank; PBM, patient blood management; PLT, platelet; PRBC, packed red blood cell; RBC, red blood cell; SPSS, Software Package for the Social Science; WBC, white blood cell; WHO, World Health Organization.
Acknowledgment
We like to say thanks to the ECUSTA Health Science Institute, and the Department of Medical Laboratory Science for granting us to do the research. Our deepest gratitude and heartfelt thanks go to the Addis Ababa health bureau and management members of Yekatit-12 Hospital for their permission to do this research. Additionally, we would like to address our heart full thanks to all health professionals of Yekatit-12 Hospital who help us in fulfilling the checklist and sample analysis. Study participants are also highly acknowledged.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fuller BM, Gajera M, Schorr C, et al. Transfusion of packed red blood cells is not associated with improved central venous oxygen saturation or organ function in patients with septic shock. J Emerg Med. 2012;43(4):593–598. doi:10.1016/j.jemermed.2012.01.038
2. Duchesne JC, Hunt JP, Wahl G, et al. Review of current blood transfusions strategies in a mature level I trauma center: were we wrong for the last 60 years? J Trauma. 2008;65(2):272–278. doi:10.1097/TA.0b013e31817e5166
3. Solow RM. Blood and Thunder. Doubleday; 1971.
4. Thomson A, Farmer S, Hofmann A, Isbister J, Shander A. Patient blood management–a new paradigm for transfusion medicine? ISBT Sci Series. 2009;4(n2):423–435. doi:10.1111/j.1751-2824.2009.01251.x
5. Khoshrang H, Madani AH, Roshan ZA, Ramezanzadeh MS. Survey on blood ordering and utilisation patterns in elective urological surgery. Blood Transf. 2013;11(1):123. doi:10.2450/2012.0025-12
6. Boral L, Henry J. The type and screen: a safe alternative and supplement in selected surgical procedures. Transfusion. 1977;17(2):163–168. doi:10.1046/j.1537-2995.1977.17277151923.x
7. Belayneh T, Messele G, Abdissa Z, Tegene BJ. Blood requisition and utilization practice in surgical patients at University of Gondar Hospital, northwest Ethiopia. J Blood transf. 2013;2013. doi:10.1155/2013/758910
8. Okoroiwu HU, Okafor IM. Demographic characteristics of blood and blood components transfusion recipients and pattern of blood utilization in a tertiary health institution in southern Nigeria. BMC Hematol. 2018;18(1):1–6.
9. Getachew A, Cheneke W, Asres Y, Bekele S, Kebede EJ. Assessment of coverage and quality of selected clinical chemistry tests among medical Laboratories of Health Facilities in Jimma zone, South West Ethiopia. J Trop Med. 2019;2019. doi:10.1155/2019/5954313
10. Feyisa T, Tesfaye Kiya G, Maleko WAJ. Assessment of recipients’ characteristics, transfusion appropriateness, and utilization pattern of blood and blood products in Jimma Medical Center, Jimma, Ethiopia. PLoS One. 2021;16(4):e0250623. doi:10.1371/journal.pone.0250623
11. Alkhaldy HY, AlShahrani BS, Alkhaldi AM, et al. Patterns of blood products utilization at a tertiary care center in the Southern Region of Saudi Arabia. J Appl Hematol. 2021;12(1):6.
12. Zewdie K, Genetu A, Mekonnen Y, Worku T, Sahlu A, Gulilalt D. Efficiency of blood utilization in elective surgical patients. BMC Health Serv Res. 2019;19(1):1–7.
13. Tamene M, Tsegaye A, Birhanu A, Taye B, Birhaneselassie M. Assessment of transfusion utilization and patient outcomes at the largest referral and university hospital in Addis Ababa, Ethiopia. ISBT Science Series. 2016;11(1):7–13.
14. Musa AU, Ndakotsu MA, Hassan -A-A, Kilishi A, Kwaifa IK. Pattern of blood transfusion request and utilization at a Nigerian University Teaching Hospital. Sahel Med J. 2014;17(1):19.
15. Kumari SJ. Blood transfusion practices in a tertiary care center in Northern India. J Lab Phy. 2017;9(2):71.
16. Kaur D, Kandwal M. Blood utilization and quality indicators–Trend at a superspeciality hospital in Northern India. Hematol Transfus Int J. 2016;2(3):00037. doi:10.1183/23120541.00037-2016
17. Chauhan S, Rishi B, Tanwar P, et al. Therapeutic lessons from transfusion in pregnancy-effect on hematological parameters and coagulation profile. Am J Blood Res. 2021;11(3):303.
18. Lippi G, Banfi GJ, Medicine L. Blood transfusions in athletes. Old dogmas, new tricks. Clin Chem Lab Med. 2006;44(12):1395–1402. doi:10.1515/CCLM.2006.262
19. Tiwari AK, Ratan A, Arora D, et al. Audit of clinical use of red blood cells in a tertiary care setting: an algorithmic approach! Global J Transf Med. 2017;2(2):109.
20. Richa S, Chetna J. An audit of appropriate use of blood components in tertiary care hospital. Int J Med Sci Educ. 2015;2(3).
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.