")
Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 14
Assessment of Anti-VEGFs in Treating Diabetic Macular Edema in Alfaisal Eye Center, Khartoum, Sudan, 2019
Authors Ahmedalgabri RHM , Omer T, Zarroug F, Elkhawad AO, Noma M
Received 14 September 2021
Accepted for publication 8 March 2022
Published 5 April 2022 Volume 2022:14 Pages 37—47
DOI https://doi.org/10.2147/CPAA.S338926
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Video abstract presented by Rayan Hamza Mohammed Ahmedalgabri.
Views: 339
Rayan Hamza Mohammed Ahmedalgabri,1 Tarig Omer,2 Fatima Zarroug,3 Abdullah Omer Elkhawad,1 Mounkaila Noma4
1Department of Pharmacology, University of Medical Science and Technology, Riyadh, Khartoum, Sudan; 2Vitreo Retinal Department, Alfaisal Eye Centre, Riyadh, Khartoum, Sudan; 3Department of Diabetes Education, Ahfad University for Women, Omdurman, Khartoum, Sudan; 4Department of Research Methodology and Biostatistics, University of Medical Science and Technology, Riyadh, Khartoum, Sudan
Correspondence: Rayan Hamza Mohammed Ahmedalgabri, Tel +249 918394529, Email [email protected]
Background: Anti-vascular endothelial growth factor (anti-VEGF) medicines have revolutionized DME and DR treatment. Despite the worldwide use of anti-VEGFs, their use remains limited in Sudan. This study aimed to assess the impact of anti-VEGF (ranibizumab and bevacizumab) injections in patients with diabetic macular oedema in Khartoum, Sudan.
Methods: An analytical comparative cross-sectional study was implemented in Alfaisal referral eye centre. A Standard questionnaire was used to collect the variables related to the research objectives. Thirty-four patients were recruited; 16 patients under ranibizumab (Lucentis) and 18 under bevacizumab (Avastin). Data were analyzed through SPSS 23, best-corrected visual acuity (BCVA) and central retinal thickness (CRT) measurements were considered as main outcomes to evaluate the treatment effectiveness.
Results: Among the 34 participants, 64.7% were males and 35.3% were females, with an average age of 62 years and 13 years of long standing diabetes. A total of 54 eyes received an average of 2.3 injections in an average of 7 months’ period. The mean BCVA before and after treatment for both drugs respectively 0.19 min and 0.21 min was statistically correlated (p = 0.000). For patients under Lucentis, the mean BCVA before and after medication was 0.20 min– 0.24 min and 0.19– 0.19 min for those who used Avastin. The mean central retinal thickness (CRT), before and after treatment for both drugs, was 492.22μm– 422.89μm, respectively, with a significant correlation (p = 0.003). For patients under Lucentis, the mean CRT decreased from 536.30 μm to 425.19 μm; it dropped from 453.16μm to 421.18μm for patients under Avastin. About 79.4% (27/34) of the participants reported that injections were not affordable and 14.7% (5/34) complained from shortage of one dose, regardless of which type of treatment. Glycaemia control, duration of treatment, type and frequency of injections used were found to be the most contributing factors to the effectiveness of anti-VEGF medications.
Conclusion: Both anti-VEGF medications are effective in treating DME, Lucentis showed better improvements in BCVA and macular thickness than Avastin. Policymakers in Sudan require urgent alternative strategies to increase access to these medications.
Keywords: ranibizumab, bevacizumab, anti-VEGFs, diabetes mellitus, diabetic retinopathy, diabetic macular edema
Introduction
Diabetes related retinopathy is the most common microvascular complication of diabetes mellitus and considered as leading cause of visual impairment or blindness.
The global prevalence of diabetes related retinopathy (DR) is 27.0%; varying from 3.8% in the US to 17.2% in Sudan.1–3 Diabetic macular edema (DME), Another important categorization of DR, occurs across all DR severity levels of non-proliferative diabetic retinopathy (NPDR) and proliferative diabetic retinopathy (PDR). It represents the most common cause of vision loss in patients with DR. The pathology of accumulation of fluid within the central portion of the retina can occur in isolation without other signs of microangiopathy in the fundus; therefore, it is sometimes classified as a separate entity. DME and DR are tightly connected; hence, their pharmacological therapy affects both manifestations in an interchangeable manner.4
VA test and optic comprehensive tomography (OCT) measurements are the most used modalities for monitoring treatment responses in DR patients.4
Anti-VEGFs injections become the 1st line therapy for DR; they work against the vascular endothelial growth factors in the retina to control the growth of abnormal blood vessels from the choroid which is the main pathological problem of DR.4,5 The three anti-VEGF medicines used in DR and DME are Eylea® (aflibercept), Lucentis® (ranibizumab) and Avastin® (Bevacizumab); in Sudan the two last are the ones available. Corticosteroids represent a fundamental alternative for treating DR5 but most often as a second choice level. The indication of steroids may be considered in patients who have a history of a major cardiovascular event as clinical trials confirmed that anti-VEGFs are contraindicated to those patients. Steroids can also be used in non-responders to anti-VEGF or in patients who are not willing to come for monthly injections.5,6 Focal-Grid Laser treatment, an effective treatment option in the past, is not anymore used in standard care in the era of anti-VEGF injections.6 However, the International Council of Ophthalmology (ICO) stated that Focal laser is indicated for DME and DR if intraocular injections of anti-VEGF agents are not available or it can be applied earlier to areas of persistent retinal thickening in eyes unresponsive to anti-VEGF treatment, in intermediate and low-resource settings, and this has been the usual practice in Sudan.7,8
This study aimed to evaluate the outcomes of anti-VEGFs injection in Sudanese patients of diabetic macular edema and to find the most contributing factors to this outcome. As well as, assessing the accessibility of patients to these injections.
Materials and Methods
An analytical facility based cross-sectional study was implemented in Alfaisal referral eye centre from December 2019 to March 2020; this referral eye centre with four retinal ophthalmologists administers in monthly average of 50 anti-VEGF injections to patients with various retinal conditions. A written permission was obtained from institutional review committee of the University of Medical Sciences and Technology and a well verbal informed consent was obtained from the health professionals and all of the patients who were interviewed.
All patients with diabetic related retinopathy who presented to the clinic were included and other types of retinopathies were excluded. 34 patients were recruited with 16 patients under Lucentis® (Ranibizumab) and 18 under Avastin® (Bevacizumab). A standardized pretested questionnaire was used to collect data from patients who were treated with the two anti-VEGFs concerned. The data collected include the characteristics of the patients, their visual acuity (BCVA) and central retinal thickness (CRT), information on additional treatment (Laser) was also recorded. The patients were also interviewed regarding their improvement post treatment as well as the availability and affordability of the treatment.
Pre and post treatment measures of BCVA and CRT, which are referred to baseline and most recent measurements, were extracted from medical files. Both BCVA and CRT were considered to be the main outcomes that evaluate treatment effectiveness. Visual acuity was measured with Snellen chart BCVA and then converted into its decimal equivalents in minutes for statistical purposes. Central retinal thickness (precisely of the fovea in the macula) was obtained by a Heidelberg OCT which gives a cross-sectional imaging of the retina, that directly measures optical reflectivity in the z-plane (depth of the retina), with high-axial resolution (10–14 µm).
Data were computerized in Epi Info 7 and analysed through SPSS 23. Descriptive statistics were performed to summarize the collected data, chi square tests were used to test associations between categorical variables and correlation analysis estimated the associations between numerical variables. Changes on visual acuity before and after treatment were tested through paired t-test. Multinomial regression was performed to establish the relationship between vision outcomes and a set of predictors for BCVA and for OCT measurements. All the performed statistical tests were considered significant when p <0.05.
Results
Characteristics of the Study Participants
The participants were predominantly males (64.7%, 22/34), females were 35.3% (12/34). Their age ranged from 40 to 91 years with a median of 62 years. Professionally more than half (52.9%, 18/34) of the participants were working, 26.5% (9/34) were not working and 20.6% (7/34) were retired.
All the patients were diagnosed with type 2 diabetes, which they were experiencing for 3 to 40 years with a median duration of their condition of 13 years. Their glycaemia control (HA1C) ranged from 5.8 mg to 11.0 mg with a median of 8.0 mg. Of the 34 participants, co-morbidities were absent in 17.7% (6/34) and presents in 82.3% (28/34) with 56% (19/34) suffering from hypertension alone or associated to another disease.
Participants Under Treatment
The participants, all are diabetic retinopathy patients, more than half (53.0%, 18/34) were using Avastin®, 38.2% (13/34) had Lucentis® and 8.8% (3/34) shifted from Avastin to Lucentis. For standardizing the treatment scheme of the participants, the pharmacological treatment of the participants was regrouped in two groups Avastin and Lucentis. The average of their treatment duration regardless of the drug type was found to be seven months.
From the 34 participants in this study the total number of affected eyes, which received the treatment was found to be 54 eyes. The number of anti-VEGF injections varied across the eyes. It ranged from 1 to 6 injections for the right eye with average of 2.4 injections±1.4 and from 1 to 5 for the left eye with a mean injection of 2.2±1.4 (Figure 1). Figure 1 also displayed that the median number of injection was the same 2 injections for the right eye regardless the type of pharmacological treatment. However, in the left eye, the median number of injection was lower (1 injection per eye) for Lucentis and the median number of injection for Avastin was 2. In the overall, the average number of injections received in the 54 eyes was 2.3 injections (95% [CI: 1.9–2.7]).
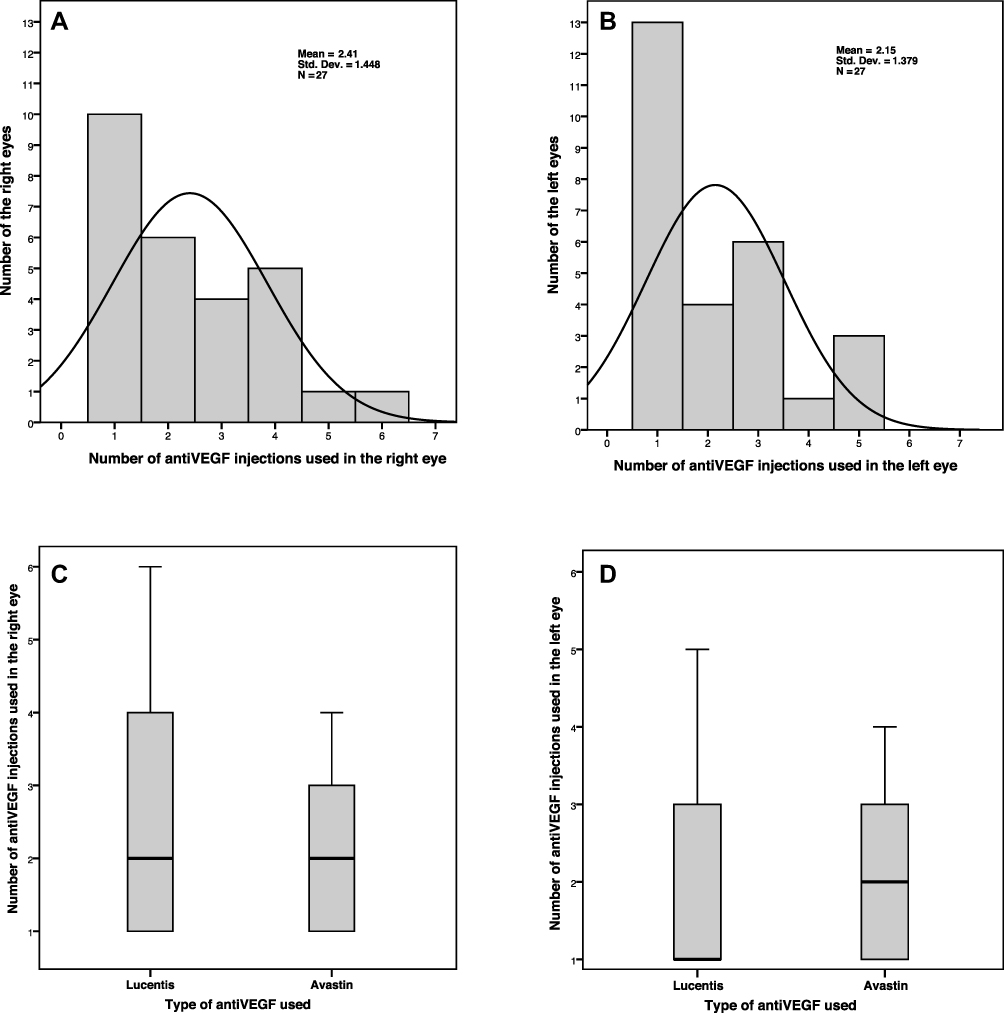 |
Figure 1 Frequency of injections received per eye and median number of injections per pharmacological treatment. (A) Number of anti-VEGFs injections used by the right eyes of patients. (B) Number of anti-VEGFs injections used by the left eyes of patients. (C) Median number of injections for each drug across the right eyes. (D) Median number of injections for each drug across the left eyes. |
Regarding the side effects and safety related the pharmacological treatment, 94.2% (32/34) of the participants had minor side effects, serious side effects were recorded in 2.9% (1/34) of the participants and one (2.9%) participant experienced both minor and severe side effect. Of the 16 participants treated with Lucentis, none presented a severe side effect. Of 18 participants who received Avastin injections, 88.8% (16/18) experienced no serious side effects, they were 5.6% (1/18) who presented with serious side effects and 5.6% who experienced both minor and serious side effects.
Laser Treatment Used by the Study Participants
The need of additional laser treatment was investigated in the study population, 55.9% (19/34) of the participants underwent additional laser intervention whereas the remaining 44.1% (15/34) did not need it. The proportion in need of laser intervention was higher (61.1%, 11/18) in the group under Avastin, whereas 50% (8/16) of those using Lucentis received laser. However, there was no statistically significant association (Pearson chi-square=0.424, p=0.515) between the type of pharmacological treatment and the need of laser intervention.
For those who were in need of laser intervention, the timing for receiving the therapy before or after the pharmacological treatment in respectively 42.1% (8/19), and 15.8% (3/19) of the participants received Laser intervention before and after (both) their respective pharmacological treatment. Table 1, revealed that there was no statistically significant association (Likelihood Ratio=1.957, p=0.376) between the type of pharmacological treatment and the time of the Laser intervention.
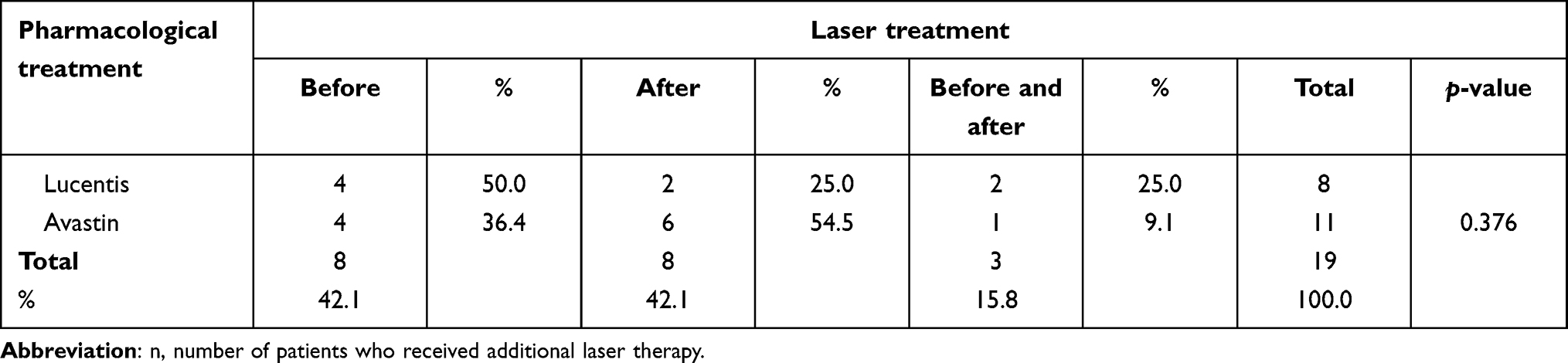 |
Table 1 Time of Laser Administered by Type of Pharmacological Treatment in the Study Population (n=19) |
Of the 11 participants who had Laser intervention after pharmacological treatment (8 after and 3 before and after) as displayed by Table 1, there were 36.4% (4/11) under Lucentis and 63.6% (7/11) under Avastin. The majority (54.5%, 6/11) of them had to receive the laser therapy because the pharmacological treatment failed to maintain their vision and 45.5% (5/11) for stabilizing their retinopathy; however, there was no statistically significant association (Fisher’s Exact Test= 0.652, p=0.652) between the pharmacological treatment and the reasons for administering Laser therapy after pharmacological.
Effectiveness of the Pharmacological Treatment
Comparison of BCVA Before and After Pharmacological Treatment
The BCVA of each eye was first measured using the Snellen chart then it was converted into its decimal equivalents.
The details in Table 2 showed that the mean BCVA for all eyes before treatment was 0.19 min (95% [CI: 0.12–0.26]); it increased to 0.21 min (95% [CI: 0.07 −0.36]) after treatment; this mean varied from 0.19 min ± 0.18 for Avastin to 0.24 min ± 0.17 for Lucentis.
 |
Table 2 Comparison Between Visual Acuity in Decimal Equivalent Before and After Treatment by Type of Anti-VEGFs Used |
Despite the higher mean observed in the group of patients who used Lucentis, indicated that Lucentis improved BCVA better than Avastin, the paired t-test which confirmed the changes in visual acuity before and after treatment revealed these changes were not statistically significant.
A correlation analysis was performed to assess the strength of association between visual acuity changes before and after treatment. The changes in BCVA of the right eyes were statistically significant (p=0.000) and the association was found to be strong before and after treatment (0.802). On the other hand, the changes in the BCVA of the left eyes had an intermediate association (R2=0.635) before and after treatment; nonetheless these changes were statistically significant (p=0.000).
Comparison of OCT Measurements Before and After Pharmacological Treatment
Regarding the OCT measurements, the mean for both drugs before treatment was 492.22 µm ±167.98 then improved to 422.89 µm ±169.70 after treatment; this mean varied from 421.18 µm ±174.12 for Avastin to 425.19 µm ±171.54 for Lucentis. As detailed in Table 3
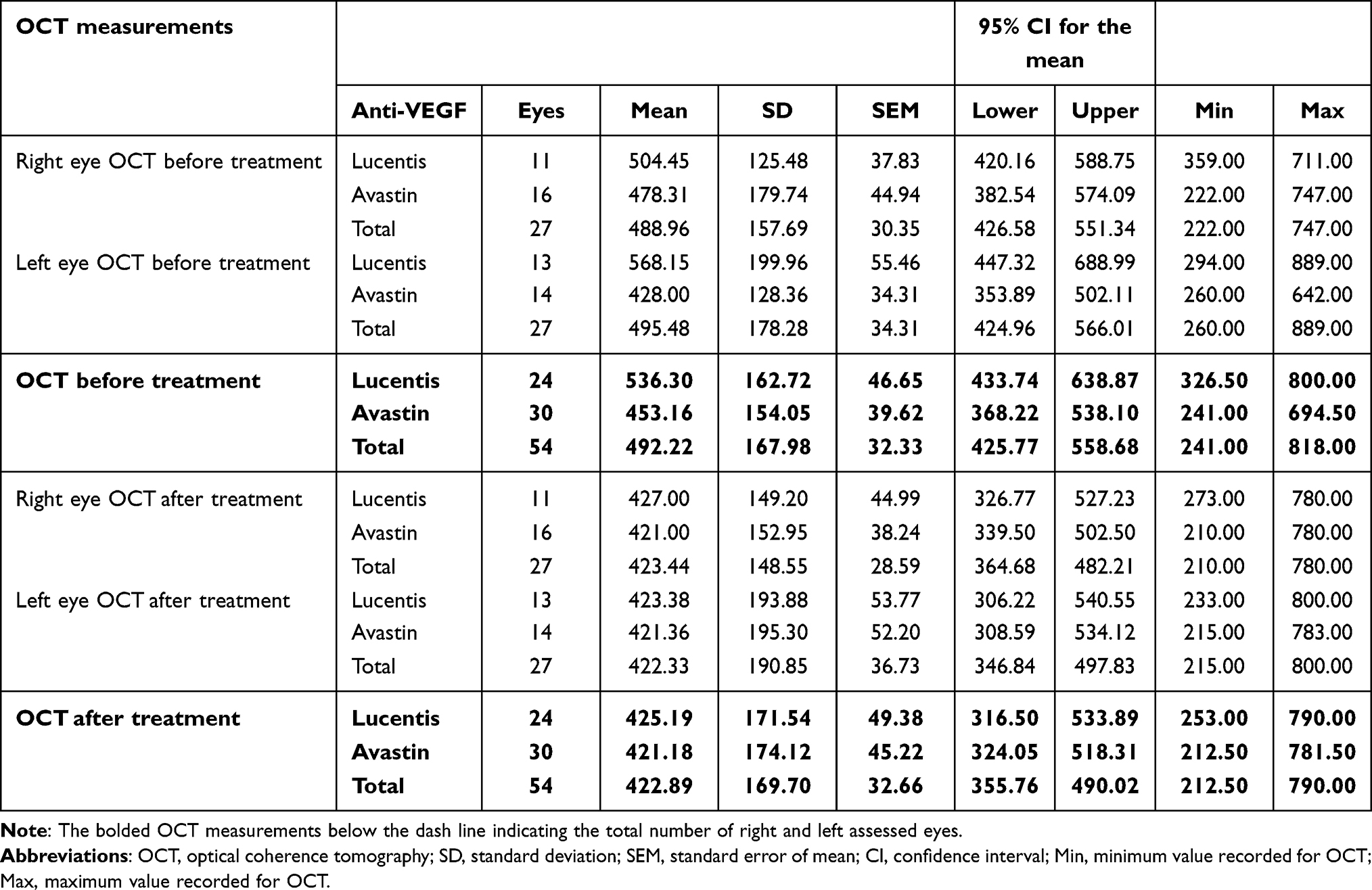 |
Table 3 Comparison of OCT Measurements in nm Across the 2 Types of Anti-VEGFs Used |
Testing the correlation between OCT measurements and the pharmacological treatment revealed a statistically significant differences in the thickness of the eyes before and after treatment with respectively R2 =0.552 for right eyes and 0.557 for left eyes with a p-value of respectively of 0.003. This association was statistically confirmed by the results a paired samples t-test, which revealed a significant paired differences.
Satisfaction of Patients Towards Pharmacological Treatment
Of the 34 patients who were asked about their status following treatment, half reported that they were improved and half did not, with a no statistically significant difference (p= 0.634) between improvement of the type of Anti-VEGF and the satisfaction of the participants.
Of the 54 eyes treated with Anti-VEGF injections, 51.9% (28/54) had a mean best corrected visual acuity in decimal equivalent of 0.318 min± 0.172 in the improved eyes; the mean BCVA was lower (0.103 min ±0.079) in the eyes without improvement post treatment (48.1%, 26/54). On the contrary, the mean central retinal thickness of 367.430 µm ± 121.583 in the group of the participants who reported an improvement following treatment increased to 482.615 µm ± 197.081 in those who did not have an improvement as revealed by Table 4.
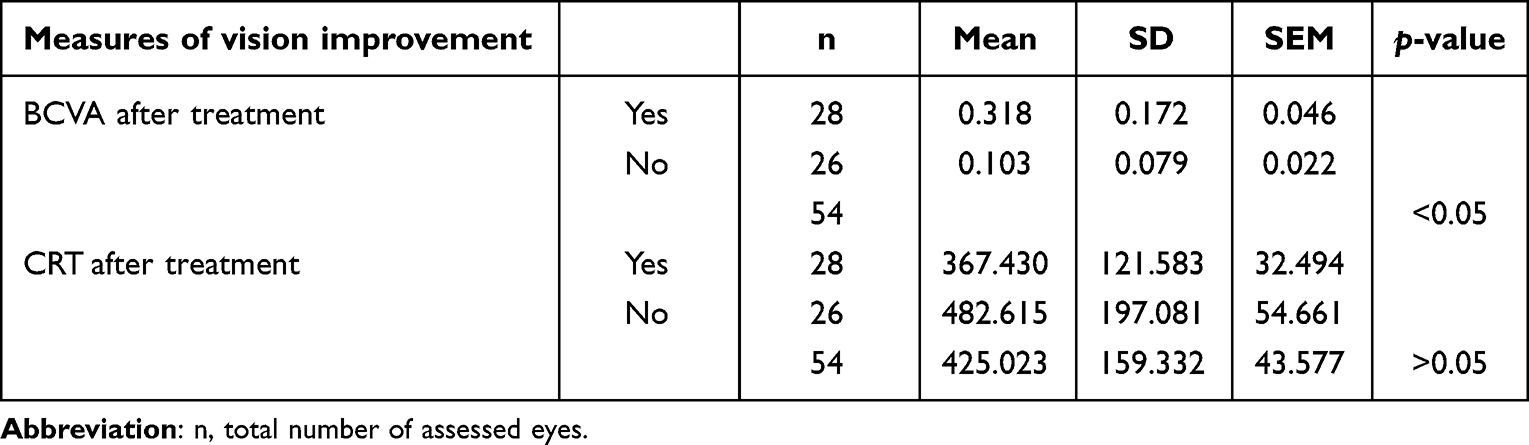 |
Table 4 Satisfaction of Patients by Vision Improvement Through Ophthalmological Measures (n=54) |
Compliance to Prescribed Pharmacological Treatment
The compliance of the participants was measured through two questions: (i) Having regular follow up visits and (ii) Taking the medications according to the timetable prescribed. So participants were labelled as compliant when the two above questions were answered “Yes”. 91.2% (31/34) of the participants were compliant and the remaining 8.8% (3/34) were non-compliant.
Of the 3 participants who were not compliant, 66.7% (2/3) surprisingly reported that their vision improved while only 48.8% (15/31) of the participants who were compliant declared that their vision improved following the received treatment; however, this difference was not statistically significant (p = 0.5). According to the treatment received, 66.7% (2/3) of the non-compliant patients were under Avastin and 33.3 (1/3) were under Lucentis. The complaints were 51.6% (16/31) under Avastin and 48.4% (15/31) were under Lucentis. Despite, the higher proportion under Avastin in the two groups of compliance, a no statistically significant association (p =0.545) was found between compliance and reported improvement.
Availability and Affordability of the Pharmacological Treatment from the Perspectives of Patients
Availability of Pharmacological Treatment
Of the 34 participants, 14.7% reported shortage of one dose of injection which was not experienced by 85.3.%. Fisher’s Exact Test revealed no statistically significant association between availability of medications and types of anti-VEGFs with a p-value of 0.2.
Affordability of Pharmacological Treatment
The affordability of the treatment was assessed through three main questions related to socioeconomic status of the participants, the financial access to the medicine and how participants coped to get the treatment. Socioeconomic classification showed that most of the participants (73.5% 25/34) were in the average socioeconomic group, 23.4% (8/34) had a low socioeconomic status and the remaining 2.9% (1/34) fell in the high socioeconomic group. The financial access to the medication was measured through two questions, participants were asked (i) if the injection was affordable to them and (ii) if they have ever missed a dose because of its cost. Only 20.6% (7/34) of the participants reported that the injections were affordable to them. Nonetheless, 67.6% (23/34) had never missed any dose because of its cost.
Likelihood ratio test revealed a no statistically significant association (p=0.069) between missed dose because of high cost, reported affordability of the injections and the different types of anti-VEGFs used. Coping mechanism of the participants to get their medications is displayed on Table 5.
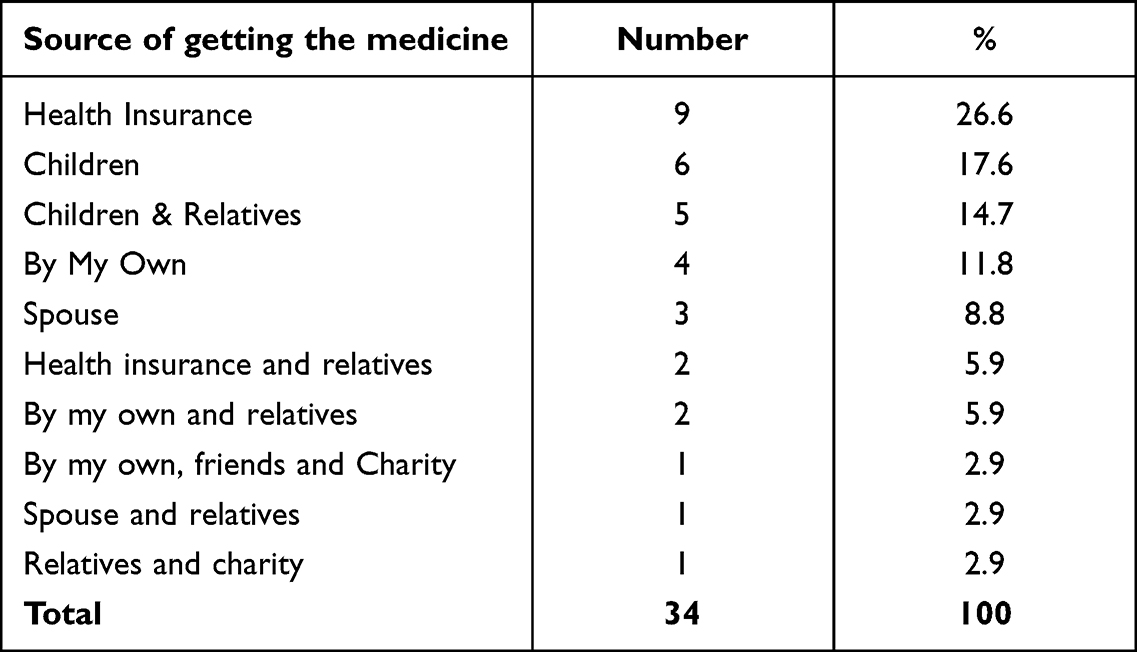 |
Table 5 How Participants Coped to Get the Treatment |
Impact of Pharmacological Treatment on Diabetic Macular Edema
Assessment of Pharmacological Treatment on Visual Acuity Measured in Decimal Equivalent
The visual acuity of participants measured in Snellen and converted in decimal equivalent in minute, was regrouped in three categories: the near normal vision (0.33–0.66 min), moderate low vision (0.16–0.25 min) and ≤ severe low vision (0.01–0.100). The near normal vision was considered as the reference group in the multinomial model for predicting the impact of pharmacological treatment based on eight explanatory variables which were namely type of anti-VEGF, frequency of the injections used, age of the participant, duration of the diabetes mellitus, level glycaemia control (HA1C), comorbidities, affordability of the medications and treatment duration. Then the odds ratio (OR) was estimated for each of the eight variables as the average of both eyes; the same principle was applied to the calculation of the confidence intervals for the OR.
In the overall, within the eight predictors, the glycaemia control and the type of anti-VEGFs used had the highest contribution on the change of visual acuity.
Assessment of Pharmacological Treatment on Optical Coherence Tomography Measures
The retinal thickness was assessed through Optical Coherence Tomography (OCT) measures which was broke in three groups ≤250–449 µm (64.8%, 35/54), 450–699 µm (25.9%) and ≥700 µm (9.3%). A multinomial regression was performed to establish the relationship between central retinal thickness (outcome variable with reference group ≤250–449 µm) and four predictors. The duration of treatment and frequency of injections used were found to be the most contributors to the decrease in central retinal thickness.
Discussion
Anti-VEGFs has become the 1st line in retinopathy therapeutic practice, whereas laser photocoagulation intervention has gradually decreased in favour of these injections, this study aims at evaluating the intravitreal anti-VEGFs therapy in the management of DME and the efficiency of these drugs in reducing the macular thickness and maintaining the visual acuity, the need for laser intervention due to medical failure and it also assesses the affordability and availability of these intravitreal injections in the Sudanese market. The study included 34 patients (54 eyes) with diabetic retinopathy specifically DME, (53.0%, 18/34) were under Avastin (Bevacizumab), 47% (16/34) were under Lucentis (Ranibizumab). Regardless of the type of treatment used, the average number of injections received in the 54 eyes was found to be 2.3 injections (95% [CI: 1.9–2.7]), which is lower than a frequency of 3.4 injections per year recorded by another study in 2018,9 this low number of injections received to the Sudanese patients can be due to use of adjunctive laser therapy or the high cost of the injections which can constrain receiving more frequent injections.
Regarding the side effect and safety related to the anti-VEGFs treatment, majority of the participants 94.2% (32/34) had minor side effects after injection administered and 5.85 (2/34) reported that they had serious side effects in term of eye infection after injection, interestingly all of them were under Avastin (Bevacizumab) treatment.
55.9% (19/34) of the participants were having adjunctive laser therapy, however there was no statistically significant association (Pearson chi-square=0.424, p=0.515) between the type of pharmacological treatment and the need of laser intervention. Of the 19 participants who had laser, 11 patients had their laser sessions after the anti-VEGFs course of injections and it was found that (54.5%, 6/11) had to take the laser because the pharmacological treatment failed to maintain their vision and 45.5% (5/11) took it for stabilizing their retinopathy. No published data was found to assess the quantity of the need of laser therapy due to pharmacological treatment failure.
The effectiveness of anti-VEGFs treatment was evaluated by measuring the differences in mean visual acuity changes and central retinal thickness measurements before and after treatment, also the personal satisfaction of the individuals was assessed. The mean best corrected visual acuity (BCVA) for both drugs before treatment was 0.19 min (95% [CI: 0.12–0.26]) it increased to 0.21 min (95% [CI: 0.07 −0.36]) after treatment with a significant correlation test (p=0.000). When comparing the BCVA across the 2 types of anti-VEGFs used, the group of patients who used Lucentis has a higher mean after treatment, which suggest that Lucentis improved VA better than Avastin. The average of BCVA before and after treatment (0.20 −0.24 min) (19 −19 min) for Lucentis and Avastin respectively. But this difference was not statistically significant (p ˃0.05), in comparison to another published Sudanese study10 the pre and post treatment mean vision with Lucentis was (0.20–0.30) and (0.18–0.37) with Avastin.
The mean of central retinal thickness (CRT) of both drugs was = 492.22 (95% [CI. 428.86–555.58]) before treatment, it dropped to 422.89 (95% [CI. 358.88–486.89]) after treatment. The paired t-test correlation revealed a statistically significant differences in the retinal thickness of the eyes before and after treatment p-value 0.003. When comparing the CRT measurements across the 2 types of anti-VEGFs used, it was found that Lucentis succeed to decrease the mean retinal thickness from (536.30 to 425.19) and Avastin managed to decrease it from (453.16 to 421.18), although the group of patients who used Avastin recorded lower mean, Lucentis gave the better improvement in CRT pre and post treatment. The lower results of Avastin could be due to the better base line retinal thickness in this group of participants, but however, this difference in means between the two drugs is not statistically significant (p ˃0.05). In another study10 the pre and post treatment thickness was (403.6 to293.6) and (389.3 to 276.1) for Lucentis and Avastin respectively.
Availability of these treatments was found to be fluctuant in the Sudanese market, 14.7% (5/34) of the participants complained that they have experienced shortage of one dose, regardless of which type of treatment. When assessing the affordability of these medications it was found that despite the fact that the majority of the participants (73.5% 25/34) have an average socioeconomic status, 79.4% (27/34) of the participants reported that both types of injections are not affordable to them, although the published data11–13 states the Avastin (Bevacizumab) is cost effective compared to other anti-VEGFs injections. Also 34.2% (11/34) reported that they miss or delay at least one dose because of its high cost, this agrees with a European study14 stated that anti-VEGFs injections have high rising cost and this affects the ability of the health providers to provide care for their patients.
The diminished Availability and the problem of the unaffordable high cost of these injections are of the main constraints limiting its widespread usage in Sudan and have a direct negative clinical impact on DME patients, considering that about 36% of the its population are below the poverty line with 25% of them live in extreme poverty.15 The authorities and policymakers in Sudan require alternative solutions and mitigations plans to overcome these constraints.
The limitation to this research is that it’s a one facility based study, which brought us to have a sample size not capturing the whole country. However, it enabled us to come with the above regression model.
The multinomial regression model found that, the glycaemia control and type of anti-VEGFs used were the highest contributors to the change of visual acuity. And the frequency of injections used and duration of treatment were the most contributors to the decrease in central retinal thickness.
In summary, both anti-VEGFs medications are effective in treating eyes of patients of DME, correlation analysis showed a significant difference in both types of treatments based on mean visual acuity and central retinal thickness measurements. Lucentis (Ranibizumab) showed preferable improvement in visual acuity and retinal thickness than Avastin (Bevacizumab).
Glycaemia control, duration of treatment, type and frequency of injections used are the most contributing factors to the effectiveness of anti-VEGFs medications.
Availability of these treatments is fluctuant in the Sudanese market and the majority of the population cannot afford it. This contributes more to the limitation of these medicines in the country and challenges the health care givers to deliver the patients a good sustained form of medical service.
Abbreviations
Anti-VEGFs, anti-vascular endothelial growth factors; BCVA, best corrected visual acuity; CCGs, clinical commissioning groups; DM, diabetes mellitus; DME, diabetic macular oedema; DR, diabetic retinopathy; DRCR.net, Diabetic Retinopathy Clinical Research Network; EURETINA, European Society of Retina Specialists; FA, fluorescein angiography; FTH, foveal thickness; ICERs, incremental cost-effectiveness ratios; ICO, International Council of Ophthalmology; NPDR, non proliferative diabetic retinopathy; OCT, optic comprehensive tomography; PDR, proliferative diabetic retinopathy; QALY, quality-adjusted life-year; VA, visual acuity.
Data Sharing Statement
To support data sharing all the data used in the frame work of this research will be available upon request made to the 1st corresponding author.
Ethical Approval and Consent to Participate
SUMASRI institutional review board of the University of Medical Science and Technology reviewed the research proposal and a written authorization of implementing the research was granted from the University. Request of ethical approval was submitted to the Ministry of Health and due to the lockdown related to COVID-19 pandemic and the socio-political instabilities in the country; verbal informed consent process was approved by the Ministry of Health, hospital administration and treating medical doctors to access patients’ medical records. As well as patients provided their full consent to participate in the study. However, various attempts were conducted to obtain written consent from Ministry of Health of Khartoum state, the last attempt was on 15/2/2022. The Ministry of Health declared taking note of the research has already implemented. These statements were written of the basis of the declaration of honor of all the authors. The confidentiality of all study participants was insured through the use of anonymous research tools and the data collected for them will not be used for any other purpose other than the research objectives.
Acknowledgments
We would like to acknowledge Alfaisal Eye Centre for allowing us to conduct this study at their clinic and for allowing us to access all the needed medical records, also we thank all the patients who participated in this study for their cooperation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Rayan Hamza Mohammed Ahmedalgabri bore all the cost related to the study in the frame work of her thesis for the Master of Clinical Pharmacology from the University of Medical Science and Technology.
Disclosure
The authors declared no conflicts of interest for this work.
References
1. Thomas RL, Ng SM. Risks and prevalence of diabetic retinopathy in children and young people with type 1 diabetes mellitus. J Diabetes Clin Res. 2020;2(2):68–74.
2. Varma R, Bressler NM, Doan QV. Prevalence of and risk factors for diabetic macular edema in the United States. JAMA Ophthalmol. 2014;132(11):1334–1340. doi:10.1001/jamaophthalmol.2014.2854
3. Elmahdi EM, Kaballo AM, Mukhtar EA. Features of non-insulin-dependent diabetes mellitus (NIDDM) in the Sudan. Diabetes Res Clin Pract. 1991;11(1):59–63. doi:10.1016/0168-8227(91)90142-Z
4. Chew EY, Davis MD, Danis RP. The effects of medical management on the progression of diabetic retinopathy in persons with type 2 diabetes: the Action to Control Cardiovascular Risk in Diabetes (ACCORD) eye study. Ophthalmology. 2014;121(12):2443–2451. doi:10.1016/j.ophtha.2014.07.019
5. Meduri A, Oliverio GW, Trombetta L, Giordano M, Inferrera L, Trombetta CJ. Optical coherence tomography predictors of favorable functional response in naïve diabetic macular edema eyes treated with dexamethasone implants as a first-line agent. J Ophthalmol. 2021;2021:6639418. doi:10.1155/2021/6639418
6. Schmidt-Erfurth U, Garcia-Arumi J, Bandello F, et al. Guidelines for the management of diabetic macular edema by the European Society of Retina Specialists (EURETINA). Ophthalmologica. 2017;237(4):185–222. doi:10.1159/000458539
7. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352:837–853. doi:10.1016/S0140-6736(98)07019-6
8. Wong TY, Sun J, Kawasaki R, et al.Guidelines on diabetic eye care: the International Council of Ophthalmology recommendations for screening, follow-up, referral, and treatment based on resource settings. Ophthalmology. 2018;125. doi:10.1016/j.ophtha.2018.04.007
9. Holekamp NM, Campbell J, Almony A, et al. Vision outcomes following anti-vascular endothelial growth factor treatment of diabetic macular edema in clinical practice. Am J Ophthalmol. 2018;191:83–91. doi:10.1016/j.ajo.2018.04.010
10. El Awad SM, Elrahman NM, Ahmad MI, et al.Comparison of anti VEGF and laser photocoagulation in Diabetic Macular Edema (DME). EC Ophthalmol. 2020;11(4):19–24.
11. Dakin HA, Wordsworth S, Rogers CA, et al. Cost-effectiveness of ranibizumab and bevacizumab for age-related macular degeneration: 2-year findings from the IVAN randomised trial. BMJ Open. 2014;4:e005094. doi:10.1136/bmjopen-2014-005094
12. Heier JS, Bressler NM, Avery RL, et al. Comparison of aflibercept, bevacizumab, and ranibizumab for treatment of diabetic macular edema: extrapolation of data to clinical practice. JAMA Ophthalmol. 2016;134(1):95–99. doi:10.1001/jamaophthalmol.2015.4110
13. Ross EL, Hutton DW, Stein JD, Bressler NM, Jampol LM, Glassman AR; Diabetic Retinopathy Clinical Research Network. Cost-effectiveness of aflibercept, bevacizumab, and ranibizumab for diabetic macular edema treatment: analysis from the diabetic retinopathy clinical research network comparative effectiveness trial. JAMA Ophthalmol. 2016;134(8):888–896. doi:10.1001/jamaophthalmol.2016.1669
14. Hollingworth W, Jones T, Reeves BC, et al. A longitudinal study to assess the frequency and cost of antivascular endothelial therapy, and inequalities in access, in England between 2005 and 2015. BMJ Open. 2017;7:e018289. doi:10.1136/bmjopen-2017-018289
15. UNICEF Sudan. Policy, evidence & social protection; 2022. Available from: https://www.unicef.org/sudan/policy-evidence-social-protection.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.