")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
A Social Return on Investment Analysis of Improving the Management of Chronic Obstructive Pulmonary Disease Within the Spanish National Healthcare System
Authors Merino M , Martín Lorenzo T , Maravilla-Herrera P, Ancochea J , Gómez Sáenz JT, Hass N , Molina J , Peces-Barba G, Trapero-Bertran M , Trigueros Carrero JA , Hidalgo-Vega Á
Received 22 February 2022
Accepted for publication 2 June 2022
Published 21 June 2022 Volume 2022:17 Pages 1431—1442
DOI https://doi.org/10.2147/COPD.S361700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Min Zhang
María Merino,1 Teresa Martín Lorenzo,1 Paulina Maravilla-Herrera,1 Julio Ancochea,2– 4 José Tomás Gómez Sáenz,5 Nicole Hass,6 Jesús Molina,7 Germán Peces-Barba,8 Marta Trapero-Bertran,9 Juan Antonio Trigueros Carrero,10 Álvaro Hidalgo-Vega11
1Health Outcomes Research, Weber, Madrid, Spain; 2Pulmonology Service, La Princesa University Hospital - IIS-Princesa, Madrid, Spain; 3Faculty of Medicine, Universidad Autónoma de Madrid, Madrid, Spain; 4Respiratory Diseases Networking Biomedical Research Centre - CIBERES, Carlos III Institute of Health - ISCIII, Madrid, Spain; 5Nájera Health Centre, Nájera, La Rioja, Spain; 6Chronic Obstructive Pulmonary Disease Patient and Family Association - APEPOC, Pontevedra, Spain; 7Francia Health Centre, Fuenlabrada, Madrid, Spain; 8Pulmonology Service, Fundación Jiménez Díaz University Hospital, Madrid, Spain; 9Basic Sciences Department, University Institute for Patient Care, Universitat Internacional de Catalunya, Barcelona, Spain; 10Menasalbas Health Centre, Mensalbas, Toledo, Spain; 11Department of Economic Analysis and Finances, Universidad de Castilla-La Mancha, Toledo, Spain
Correspondence: María Merino, Health Outcomes Research, Weber, Calle Moreto 17, 5° Dcha, Madrid, 28014, Spain, Tel +34 91 639 38 24, Fax +34 91 634 6643, Email [email protected]
Purpose: To define a set of proposals that would improve the current management of chronic obstructive pulmonary disease (COPD) within the Spanish National Healthcare System (SNHS) from a comprehensive multidisciplinary perspective and to assess the impact of its implementation from clinical, healthcare, economic, and social perspectives.
Patients and Methods: A group of 20 stakeholders related to COPD (healthcare professionals, patients, and informal caregivers, among others) participated in an online Delphi process to agree on a set of 15 proposals that would improve the current management of COPD within the SNHS in four areas: diagnosis, risk stratification, management of exacerbations, and management of stable COPD. A one-year forecast-type social return on investment (SROI) analysis was used to estimate the impact that implementing the set of proposals would have in relation to the investment required. A sensitivity analysis was used to test the strength of the model when varying assumption-based data-points.
Results: The hypothetical implementation of the complete set of 15 proposals would require a € 668 million investment and would generate a € 2079 million social impact concerning savings for the SNHS and quality of life improvements for patients and their informal caregivers, among others. Accordingly, for every euro invested in the set of proposals, a social return of € 3.11 would be generated (€ 2.71 in the worst-case scenario and € 3.62 in the best-case scenario) of both tangible (32.56%) and intangible nature (67.44%).
Conclusion: Altogether, implementing this set of 15 proposals would generate a positive social impact, threefold the required investment. The results may inform decisions relative to healthcare policy and practice regarding COPD management within the SNHS, further contributing to reduce the large burden of COPD.
Keywords: disease management, chronic disease, respiratory disease, economic evaluation, social impact, Spain
Introduction
Chronic obstructive pulmonary disease (COPD), a preventable and treatable disease, is characterized by persistent respiratory symptoms (ie, dyspnea, cough, and/or sputum production) as a result of airway and/or alveolar abnormalities associated with a critical exposure to noxious particles or gases, generally tobacco smoke.1 COPD is one of the most prevalent conditions worldwide. In Europe, the prevalence of COPD has been estimated at 12.4% (95% CI: 10.8–14.0%), and in southern Europe (including Spain) at 10.8% (95% CI: 7.8–13.8%) among adults on or over 40 years old.2 In Spain, the prevalence of COPD has been estimated within these ranges at 11.8% among adults on or over 40 years old (ie, 3,206,921 when applied to the Spanish population of adults on or over 40 years old on 1 July 2020).3,4 This represents an increase from previous estimates in 2006–2007 (10.2%).5 Moreover, underdiagnosis of COPD has been estimated at 74.7% according to data collected from 2017 to 2019,4 increasing with respect to previous reports according to data collected from 2006 to 2007 (73.1%).5
The 2019 Global Burden of Disease Study identified COPD as one of the leading causes of morbidity and mortality worldwide.6 In western Europe (including Spain), COPD accounts for 3.41% of all disability-adjusted life years (DALYs), and 4.97% of all deaths.7 Similarly, in Spain, COPD accounts for 4.03% of all DALYs and 7.29% of all deaths, ranking sixth and third among other conditions, respectively.8,9 Accordingly, as observed with other highly prevalent chronic diseases, COPD poses a substantial economic and social burden1,10 which has been estimated at €1547 million in Spain, including direct healthcare costs and non-healthcare costs associated with professional and/or informal caregiving, and indirect costs associated with labor productivity losses.10,11 This burden is expected to increase along with prevalence, given the continued exposure to risk factors (eg, tobacco smoke) and population ageing.1 Moreover, high rates of underdiagnosis will continue to generate unnecessary burden as COPD is considered a treatable disease.4
Recent consensus studies have analyzed the current status of COPD management in Spain, and multiple stakeholders agree there is much room for improvement.11–14 Overall, studies highlight the need to reduce the high rates of underdiagnosis; to promote training and compliance with clinical guidelines; to guarantee access to respiratory rehabilitation; to provide patients, caregivers, and society with information and training on COPD and healthy lifestyle habits; to ensure patients and caregivers receive a comprehensive management of biopsychosocial factors; to improve assistance continuity through and adequate coordination between healthcare professionals, primary care, and specialized care; to implement and enhance home assistance; and to design coordinated and shared global strategies among stakeholders associated with COPD management, among others.11–13 However, only one of these studies used a multistakeholder perspective and COPD-relevant profiles such as pharmacists, internal medicine specialists, respiratory physical therapists, social workers, or informal caregivers were not accounted for.11
Interventions based on the needs described by multiple stakeholders may have a multidimensional impact. Moreover, given the budget and/or resource limitations of the Spanish National Health System (SNHS), putting the impact of such interventions into perspective using the investment required to implement them may allow for more efficient decision-making in this regard.15 The multiple impacts that such interventions would have relative to the investment required to implement them may be ideally assessed using the social return on investment method (SROI).15–17 This method takes into account a more extended concept of value, expressed in monetary terms, incorporating both positive and negative social, economic, and environmental costs and benefits associated with multiple stakeholders.18 To measure a more comprehensive concept of value, different valuation methods have been developed to translate social value to monetized value (eg., people’s willingness to pay or spending preferences).19 Despite the subjectivity associated with some of these methods, valuing intangible aspects without a market price is essential to expose social returns, usually associated with patient and caregiver needs, which would otherwise remain unaccounted for. Previous experiences have been used to guide decisions relative to healthcare interventions,18,20–23 including interventions on chronic diseases overall,24 heart failure,25 psoriasis,26 multiple sclerosis,27 rheumatoid arthritis,28 or haemophilia A,29 among others. To date, no other study has used the SROI method to assess the impact of any healthcare intervention specifically designed for COPD. Therefore, this study aimed to establish a set of proposals that would improve COPD management in the SNHS from a comprehensive multistakeholder perspective and to estimate, from a clinical, healthcare, economic, and social perspective, the impact it would generate if it were to be implemented.
Materials and Methods
The SROI framework includes 6 stages which have been used to develop and report the present study. A detailed description of the SROI method has been provided elsewhere.16 In brief, a one-year forecast-type SROI analysis was carried out to estimate the impact that a set of proposals to improve COPD management within the SNHS would have, with respect to the required investment. A forecast-type SROI analysis warrants a reduced time frame to limit variability and increase accuracy. Results are presented for the set of proposals as a whole and within key areas of analysis.
The analysis was based on data gathered from a Delphi process with stakeholders related to COPD in Spain, the scientific literature, the Spanish National Institute of Statistics and the Ministry of Health, official bulletins of the Spanish Autonomous Communities regarding the median rates of health services, and market prices. Prices were updated according to the corresponding Consumer Price Index to 2019 euros. Sensible assumptions were made whenever essential data points for the SROI analysis were lacking or uncertain, such as those presenting a large variability.
This study was exempt from approval by an institutional or ethical review board given its observational nature. Notwithstanding, the procedures used in the present study were in compliance with the Declaration of Helsinki 1975/83.
Stage 1. Establishing Scope and Identifying Key Stakeholders
A set of 15 priority proposals to improve the management of COPD within the SNHS was determined using a Project Advisory Committee (PAC) and a Multidisciplinary Expert Committee (MEC). The PAC, included two nationally renowned pulmonologists, three nationally renowned primary care physicians, a renowned health economist, and a renowned representative of the Asociación de Pacientes con EPOC (APEPOC, one of the largest COPD patient associations in Spain), was gathered to establish the areas of analysis in which specific proposals would be allocated and to confirm the stakeholder profiles related to COPD in Spain that would constitute the MEC. The MEC, which included the members of the PAC as well as three hospital managers, another pulmonologist, an internal medicine specialist, a case management nurse, a respiratory nurse, a hospital pharmacist, a primary care pharmacist, a respiratory physical therapist, a social worker, a patient with COPD, and an informal caregiver of a patient with COPD, was gathered to agree on the set of 15 top-rated proposals within the key areas of analysis identified by the PAC. To do so, a three-round online Delphi process using three individual and anonymous questionnaires was carried out. The first questionnaire was sent to each member of the MEC to collect proposals that would improve the current management of COPD within the key areas of analysis. Thereafter, a second questionnaire was sent to each member of the MEC for them to rate individual proposals on a scale of 0 (not important) to 10 (very important) regarding their capacity to improve how COPD is currently managed. Finally, the average score of each proposal was estimated, and a third questionnaire including the 15 top-scoring proposals was sent to each member of the MEC for them to rate each proposal on a scale of 0 (no positive impact) to 10 (large positive impact) regarding their capacity to have an impact on particular aspects of patients’ and caregivers’ lives.
To reduce the scope of proposals to specific activities and identify which stakeholders might contribute to and/or be influenced by such activities, a review of the scientific and grey literature was carried out for each proposal.
Stage 2. Building an Impact Map: Identifying and Valuing Inputs, in Relationship with Activities and Outcomes
The inputs (ie, resources) to implement the activities comprising each proposal were established and linked to specific stakeholders. Thereafter, the number of resources was multiplied by their unit prices to determine their cost. Unit prices were selected following a conservative approach by which the highest unit price was used to avoid underestimating costs. The time patients and informal caregivers spend on activities was not monetized as they are the main beneficiaries of such activities, according to the current convention on the SROI method. Thereafter, the investments of individual proposals were added to obtain the total investment.

Stage 3. Identifying and Valuing Outcomes
For the activities within each proposal, a series of outcomes were identified and linked to the stakeholders involved. For each outcome, an indicator of the amount of outcome-associated change that would occur (ie, number of patients that would improve their knowledge about the disease) was established and monetized by applying a financial value to such change (ie, minimum annual contribution for a COPD patient association). Outcomes can be defined according to their attributes as positive or negative, and tangible or intangible. The latter (ie, those without a market value) were monetized using revealed-preference methods through financial proxies. This is, inferring valuations from the prices of market-traded goods which most closely resembled the intangible outcome (eg, average annual expenditure on games and hobbies per person to value improvements in leisure life or perceived health status). Financial values and proxies of outcomes were selected following a conservative approach by which the lowest values were used to avoid overestimating the value of outcomes.
Besides data gathered from the scientific literature, this analysis was based on information gathered from the Delphi process with the members of the MEC, and patients with COPD and their caregivers through an online Focus Group.

Stage 4. Establishing the Impact
To avoid over-claiming, outcomes were individually adjusted by subtracting the following adjustment factors: 1) the proportion of the outcome that would have still been achieved had the activity had not taken place (deadweight), 2) that would be due to the contribution of other activities (attribution), and that would displace other outcomes (displacement) from their total value. Given the one-year timeframe, the drop-off adjustment factor did not apply. Thereafter, the impacts of individual proposals were added to obtain the total impact.

Stage 5. Calculating the SROI
The SROI ratio was obtained by dividing the net impact that the hypothetical implementation of the set of proposals would generate by the total investment needed. A positive SROI ratio (ie, greater than 1) indicates a greater total impact relative to the total investment required.
For the complete set of proposals:

Stage 6. Reporting the Results
The final stage of the SROI process requires communicating the results to stakeholders, essential to allow identified unmet needs regarding the management of COPD in Spain to be more closely met. Accordingly, the results of the SROI analysis were shared with the members of the PAC, and their feedback was included to obtain a validated final version of the SROI analysis.
Sensitivity Analysis
A sensitivity analysis was performed to determine the effect of varying assumption-based data-points on the SROI ratio. It included a reference scenario, a best-case scenario (using a value that would result in a smaller investment and/or greater outcome), and a worst-case scenario (using a value that would result in a greater investment and/or smaller outcome). Refer to Supplementary Materials for a detailed list of the assumptions varied according to the three sensitivity analysis scenarios.
Results
We present a set of 15 top-rated proposals that would improve the current management of COPD within the SNHS according to the following areas of analysis: diagnosis, risk stratification, management of exacerbations, and management of stable COPD (Table 1). Proposal 3 on informing patients and families about the disease and its treatments has been used as an example to depict the results. For a detailed analysis of each proposal, refer to Supplementary Materials.
 |
Table 1 Proposals to Improve Chronic Obstructive Pulmonary Disease Management Within the Spanish National Healthcare System According to Areas of Analysis |
A total investment of €668 million would be required to implement the complete set of 15 proposals to improve COPD management within the SNHS. The group of proposals for the management of exacerbations would account for the greatest part of the investment (55.22%), followed by the management of stable COPD area (22.92%), and the risk stratification area (21.37%). Within the management of exacerbations area, the proposal that would account for the largest proportion of the investment would be Proposal 8 on ensuring continuity of care after an exacerbation in coordination with primary care (44.29%), followed by Proposal 9 on the availability of adequate resources for exacerbations that require hospitalization (29.01%), and Proposal 7 on training therapeutic adherence in patients (25.03%). Moreover, within the area of stable COPD management, the largest proportion of the investment would be attributed to Proposal 11 on implementing a smoking cessation plan for smokers with COPD (80.68%). In addition, within the area of risk stratification, the largest proportion of the investment would be attributed to Proposal 3 on providing information to patients and families about the disease and its treatments (47.72%) and Proposal 4 on agreeing COPD treatment and management with patients and caregivers (43.73%) (Table 2).
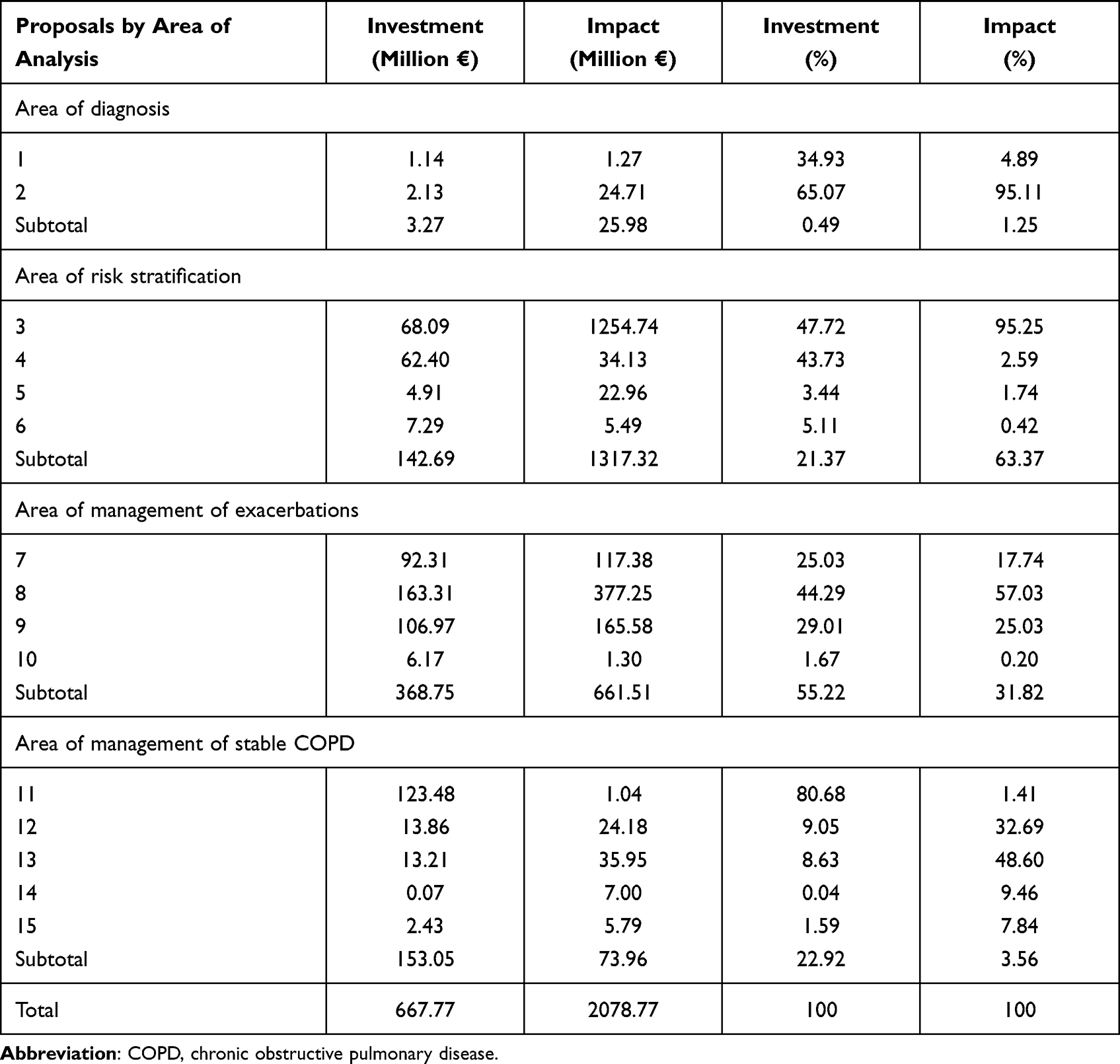 |
Table 2 Investment and Impact for Each Proposal, Area of Analysis, and the Complete Set of Proposals; and Proportion of the Area of Analysis for Each Proposal and of the Complete Set of Proposals for Each Area of Analysis (€2019) |
Focusing on the example, the investment required to implement Proposal 3 on providing information to low-risk patients and their families about the disease and its treatments included the cost of the design, creation, and dissemination of a leaflet with key information on COPD and its treatments. The contents of this leaflet would be developed by a group of experts on COPD and validated by primary care and specialized care scientific societies. The investment further included one nursing consultation to deliver and explain the contents of the leaflet. Subsequent annual investments would have to be made to update and communicate the information on the leaflet (Table 3 of Supplementary Materials).
Moreover, the total investment would have €2079 million social impact. The implementation of the group of proposals within the area of risk stratification would generate the greatest part of the impact (63.37%), followed by management of exacerbations (31.82%). Within the area of risk stratification, the proposal that would account for the greatest part of the impact would be Proposal 3 on providing information to patients and families about the disease and its treatments (95.25%). Moreover, within the management of exacerbations area, Proposal 8 on ensuring continuity of care after an exacerbation in coordination with primary care would account for the greatest part of the impact (57.03%), followed by Proposal 9 on the availability of adequate resources for exacerbations that require hospitalization (25.03%), and Proposal 7 on training therapeutic adherence in patients (17.74%) (Table 2).
Following the example, the implementation of the activities included in Proposal 3 would generate a positive impact on the SNHS and nursing professionals associated with reductions in healthcare resources and workload, respectively. Workload reductions for nursing professionals would be related to improved health outcomes, largely compensating for the annual consultation to inform patients and their families. Moreover, low-risk patients and their caregivers would improve their health literacy (except for those with an adequate level of health literacy which were included as a deadweight) and increase their satisfaction with the SNHS (except for those already satisfied with the SNHS which were included as deadweight). However, patients would reduce their working hours, and caregivers would increase their workload associated with the need to attend the nursing consultation. Part of the impact associated with the improvement in health literacy would be attributed to Proposal 4 on agreeing with patients and caregivers on the treatment and management of COPD (Table 18 of Supplementary Materials).
The SROI ratio resulting from the implementation of the complete set of proposals was estimated at 3.11:1, that is, for every euro invested in the hypothetical implementation of the 15 proposals as a whole a social return of €3.11 would be generated. The largest SROI ratio was obtained in the area of risk stratification (9.23:1), followed by diagnosis (7.93:1), management of exacerbations (1.79:1), and management of stable COPD (0.48:1) (Table 3). Regarding the typology of the social return, 67.4% (€2.10) was associated with intangible returns (eg, improved satisfaction with the SNHS or health literacy, among others), while 32.6% (€1.01) was associated with tangible returns (eg, reduced number of hospitalizations or referrals to specialized care, among others). Most of the generated social return would be of intangible nature, especially within the area of risk stratification (97.2%), followed by the areas of stable and exacerbated COPD management (18.2% and 16.2%). Contrarily, most of the social return within the area of diagnosis would be of tangible nature (99.9%) (Figure 1).
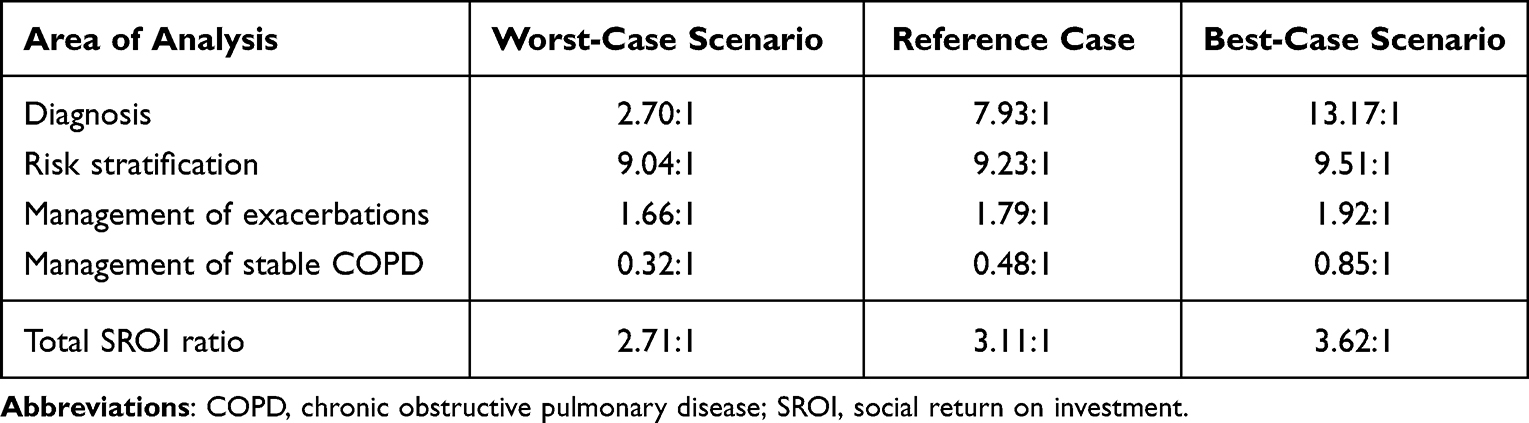 |
Table 3 Social Return on Investment Ratio and Sensitivity Analysis According to Areas of Analysis |
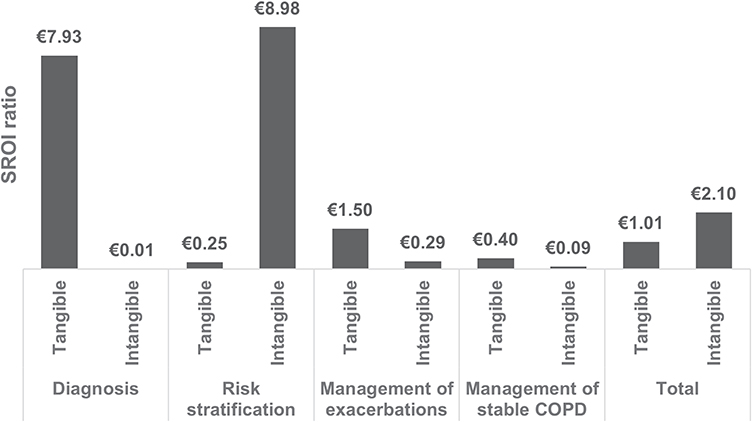 |
Figure 1 Social return on investment ratio according to areas of analysis and return typology. Abbreviations: COPD, chronic obstructive pulmonary disease; SROI, social return on investment. |
The total SROI ratio could vary between €2.71 in the worst-case scenario and €3.62 in the best-case scenario, according to the results of the sensitivity analysis, which could increase the social return up to 16% or reduce it by 13%. However, a much larger variability was observed within the areas of diagnosis and management of stable COPD (Table 3).
Discussion
The implementation of the complete set of 15 proposals would generate a €3.11 (€2.71 - €3.62) social return for every euro invested. In addition, the estimated total investment of €668 million accounts for only 0.9% of the annual healthcare budget in Spain,30 which may seem low for a disease affecting 11.8% of the Spanish population on or over 40 years old.4 The 15 proposals were defined by multiple key stakeholders associated with COPD in Spain to improve how the SNHS currently manages COPD, related to diagnosis, risk stratification, management of exacerbations, and management of stable COPD. Overall, these proposals are coordinated with recently identified needs regarding current management of COPD in Spain (eg, to provide primary care professionals with training on COPD and spirometry; to provide patients and their families with information on COPD and its treatments, and promote joint agreements; and to improve coordination between primary and specialized care, among others)11–13 and confirm there is still much room for improvement.14 However, these studies identified additional proposals to improve COPD management in Spain that have not been included in the present SROI analysis (eg, providing pulmonary rehabilitation, enhancing vaccination, or implementing telemedicine, among others).12,13 This may be attributed to differences in the scope of the studies, the areas considered, and/or the configuration of the multidisciplinary group of experts used to identify proposals. While the proposals of the present study aimed to improve COPD management within the SNHS in 4 areas of analysis and included patients and caregivers among key stakeholders, previous studies included the private sector, up to 16 areas of analysis, and did not include either patients or caregivers.12,13 Nevertheless, the set of 15 top-rated proposals were obtained from over 600 that were initially identified.
This is the first study to use the SROI method to assess the multidimensional impact of a comprehensive approach to improve how the SNHS currently manages COPD. Accordingly, comparisons with the scientific literature are difficult. Nevertheless, a recent study using the SROI method to estimate the impact of a series of interventions to improve heart failure management (ie, another prevalent and chronic condition) in the SNHS generated a social return of €3.52, similar to that reported for COPD in the present study.25
Focusing on areas of analysis, the largest SROI ratios were obtained in the areas of risk stratification and diagnosis. Within the area of diagnosis, most of the social return was of tangible nature and associated with Proposal 2 on training primary care professionals on COPD. More specifically, the social return for this proposal was attributed to reductions in healthcare costs related to the inappropriate use of inhaled corticosteroids. The latter generates higher COPD management costs with respect to an appropriate use31 and may benefit from an educational program for primary care based on clinical practice guidelines.32
On the contrary, within the area of risk stratification, most of the social return was of intangible nature and associated with Proposal 3 on informing patients and their families about the disease and its treatments. This proposal generated the largest social return among all proposals (60.36%), irrespective of the area of analysis and the investment required for its implementation, attributed to improvements in the patients’ health literacy and a greater satisfaction of patients and their families with the SNHS. The prevalence of COPD patients with an inadequate health literacy in Spain has been estimated at 58%, a quality which, if deficient, has been associated with unfavorable patient reported outcomes regarding dyspnea, wellbeing and daily life, and health-related quality of life; a higher risk of having comorbidities, need of caregiving, anxiety and depression, admissions or visits to the emergency department, and mortality.33,34
A negative SROI ratio (ie, lower than 1) was obtained in the area of stable COPD management as the investment was greater than the social return. This was associated with the large investment required to implement a smoking cessation plan for smokers with COPD, based on the financial coverage of pharmacological treatments for smoking cessation and a proactive telephone follow-up, relative to the low success rate of the intervention over routine clinical practice (ie, brief advice by the physician and printed self-help documentation). Nevertheless, this intervention has been reported to be cost-saving after 10 years.35 Moreover, the most effective preventive intervention against COPD is smoking cessation,11 which should be a priority given that over 30% of the Spanish population under 65 years old smoke on a daily basis.36 Despite the negative SROI ratio in the area of stable COPD management, Proposal 14 on the development of a pharmacological and non-pharmacological palliative care plan for end-stage patients within this area resulted in a very large social return relative to the small investment required to develop and disseminate a clinical practice guideline on the matter. A recently published update of the Spanish COPD clinical practice guideline includes a section on palliative care of patients with COPD, which may lead to a significant social impact.37
Recently, Spain participated in an international task force to develop evidence-based quality standards for the management of diagnosed or undiagnosed patients with COPD meeting modifiable high-risk criteria for exacerbations and subject to management optimization. In brief, these quality standards span the entire spectrum of COPD disease management including subject identification, comprehensive evaluation, follow-up, and non-pharmacological and pharmacological interventions, underpinned by some of the needs identified in the present study.38 This is of special relevance considering that the largest proportion of the total investment would be used to implement proposals within the management of exacerbations area (55%).
The results of this study may be used to guide decisions on the management of COPD within the SNHS, as efficiency in healthcare management is constantly pursued. However, a series of limitations should be accounted for when interpreting the results. First of all, a forecast-type SROI analysis provides an estimate of the impact associated with the implementation of the complete set of 15 proposals. While an evaluative SROI analysis based on real-world evidence may provide a more realistic foundation for decision-making, this forecast-type SROI analysis may be used to identify specific and relevant data to monitor in a future evaluative SROI analysis.16,39 Second, using a one-year time horizon may not reveal long-term cost-effective and/or cost-saving interventions. Alternatively, a long-term SROI analysis may provide a better basis for decision-making (eg, prioritizing smoking cessation programs with a large initial investment that may be cost-effective and/or cost-saving after 10 years of their implementation). Despite this limitation, the present study captures immediate impacts, of special interest to public finance decision-makers which usually operate from a short-term perspective.40 In addition, forecasting the comprehensive impact of investing in a large set of proposals implies a considerable degree of variability which warrants a shorter timeframe to increase accuracy.
Third, unlike unit prices of tangible outcomes, the use of financial proxies to value intangible outcomes is not as objective and may introduce a certain degree of bias. This bias and its impact on the results were reduced by selecting proxies which most closely resembled intangible outcomes and using the lowest value among those available to avoid overestimating the value of intangible outcomes, respectively. Moreover, altogether, the tangible part of the SROI ratio was greater than one. Therefore, intangible impacts would only contribute to increase the ratio. Similarly, the use of assumptions for data points that are lacking or uncertain may further introduce bias. Despite the latter, even in the worst-case scenario, the results of the sensitivity analysis showed a positive SROI ratio. Other sources of bias may lie in the methods used for analysis or the arrangement of the MEC. A different configuration of the MEC may have resulted in a different set of proposals.
Finally, the results of the SROI analysis further depend on the specific setting of the intervention, the SNHS in this study. Therefore, applying the results of the present study to other settings should be done with caution. The valuation of public health interventions in other countries using the SROI method generated a great variability of ratios, which appear to decrease with increased specificity of interventions.18,20,21 Accordingly, interventions in other countries which aim to achieve common standards of practice may yield comparable results.1
Notwithstanding, the SROI method introduces a broader concept of value compared to traditional economic evaluation frameworks. Accordingly, the present study accounted for the perspectives of multiple stakeholders including patients and caregivers, used financial proxies to monetize complex outcomes such as improvements in health-related quality of life, and captured both positive and negative impacts in one single ratio. Moreover, the SROI framework shows the entire spectrum of the so-called “theory of change” for each stakeholder, that is, the way the investment on specific activities leads to every impact.18
Conclusion
This study presents a comprehensive set of proposals that would improve how the SNHS currently manages COPD. Their implementation through specific activities would generate a positive social return, despite the investment required to complete them which was roughly one-third of the total social return. Proposal 3 on informing low-risk patients and their families about COPD would be the main contributor to the total social return, irrespective of the area of analysis and the investment required for its implementation. This proposal generated a 100% intangible social return, highlighting the importance of considering aspects such as patient satisfaction with the SNHS in decision-making. However, results by areas of analysis and/or proposals should not be interpreted independently, but as part of a wider strategy to improve the comprehensive management of COPD in Spain. These results may be used to inform decisions relative to healthcare policy and practice regarding COPD management within the SNHS, further contributing to reduce the large burden of COPD. Nevertheless, strategies that help reduce investments and maximize outcomes should continue to be explored.
Abbreviations
APEPOC, Asociación de Pacientes con EPOC; COPD, chronic obstructive pulmonary disease; DALYs, disability-adjusted life years; MEC, Multidisciplinary Expert Committee; PAC, Project Advisory Committee; SNHS, Spanish National Health System; SROI, social return on investment.
Acknowledgments
The authors would like to thank the members of the Multidisciplinary Expert Committee, the Asociación de Pacientes con EPOC (APEPOC), and the patients and informal caregivers who participated in the Delphi process and the Focus Group, for their valuable contribution to the present study.
Disclosure
This study was funded by Chiesi and GSK. MM, TML, and PMH are employees of Weber, an independent company that received non-binding fees from Chiesi and GSK to carry out this study. JA, JTGS, NH, JM, GPB, MTB, and JATC received consulting fees as members of the advisory board. The authors report no other potential conflicts of interest in relation to this work. Data from this study were presented at Virtual ISPOR Europe 2021 and at the 2021 Congress of the Spanish Society of Primary Care Physicians (43 Congreso Nacional SEMERGEN Zaragoza 2021).
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2021 report).; 2021.
2. Blanco I, Diego I, Bueno P, et al. Geographical distribution of COPD prevalence in Europe, estimated by an inverse distance weighting interpolation technique. Int J Chron Obstruct Pulmon Dis. 2017;13:57–67. doi:10.2147/COPD.S150853
3. Instituto Nacional de Estadística. Cifras de población. Provisionales a 1 de julio de 2020. Población residente por fecha, sexo y edad [National Institute of Statistics. Population data. Provisional on 1 july 2020. Population residing by date, sex, and age]. INE; 2020. Available from: https://www.ine.es/jaxiT3/Datos.htm?t=31304.
4. Soriano JB, Alfageme I, Miravitlles M, et al. Prevalence and determinants of COPD in Spain: EPISCAN II. Arch Bronconeumol. 2020. doi:10.1016/j.arbres.2020.07.024
5. Miravitlles M, Soriano JB, Garcia-Rio F, et al. Prevalence of COPD in Spain: impact of undiagnosed COPD on quality of life and daily life activities. Thorax. 2009;64(10):863–868. doi:10.1136/thx.2009.115725
6. Institute for Health Metrics and Evaluation. Chronic obstructive pulmonary disease. Level 3 cause; 2019. Available from: http://www.healthdata.org/results/gbd_summaries/2019/chronic-obstructive-pulmonary-disease-level-3-cause.
7. Global Burden of Disease Collaborative Network. Global burden of disease study 2019 (GBD 2019) results. Western Europe. Institute for Health Metrics and Evaluation; 2019. Available from: http://ghdx.healthdata.org/gbd-results-tool.
8. Global Burden of Disease Collaborative Network. Global burden of disease study 2019 (GBD 2019) results. Spain. Institute for Health Metrics and Evaluation; 2019. Available from: http://ghdx.healthdata.org/gbd-results-tool.
9. Country profile: Spain. Institute for Health Metrics and Evaluation; 2019. Available from: http://www.healthdata.org/spain.
10. Merino M, Villoro R, Hidalgo-Vega Á, Carmona C. Social economic costs of COPD in Extremadura (Spain): an observational study. Int J Chron Obstruct Pulmon Dis. 2018;13:2501–2514. doi:10.2147/COPD.S167357
11. Bouza E, Alvar A, Almagro P, et al. Chronic obstructive pulmonary disease (COPD) in Spain and the different aspects of its social impact: a multidisciplinary opinion document. Rev Esp Quimioter. 2020;33(1):49–67. doi:10.37201/req/2064.2019
12. Arriero‐Marín JM, Orozco‐Beltrán D, Carratalá‐Munuera C, et al. A modified Delphi consensus study to identify improvement proposals for COPD management amongst clinicians and administrators in Spain. Int J Clin Pract. 2021;75(5). doi:10.1111/ijcp.13934
13. Ancochea J, Aguilar J, de Lucas P, et al. La epoc en España: reflexión sobre la situación actual y propuesta de soluciones 2021 [COPD in Spain: thoughts on the current situation and proposals on solutions 2021]. EIDON. 2020;54:151–187. Spanish. doi:10.13184/eidon.54.2020.151-187
14. Ancochea J, Soriano JB. COPD in Spain at the start of a new decade. Arch Bronconeumol. 2021;57(1):1–2. doi:10.1016/j.arbres.2020.01.025
15. Yates BT, Marra M. Social Return On Investment (SROI): problems, solutions … and is SROI a good investment? Eval Program Plann. 2017;64:136–144. doi:10.1016/j.evalprogplan.2016.11.009
16. Nicholls J, Lawlor E, Neitzert E, Goodspeed T. A guide to social return on investment. 2nd ed. The SROI network. accounting for value; 2012. Available from: http://www.socialvalueuk.org/app/uploads/2016/03/The%20Guide%20to%20Social%20Return%20on%20Investment%202015.pdf.
17. Nicholls J. Social return on investment—development and convergence. Eval Program Plann. 2017;64:127–135. doi:10.1016/j.evalprogplan.2016.11.011
18. Banke-Thomas AO, Madaj B, Charles A, van den Broek N. Social Return on Investment (SROI) methodology to account for value for money of public health interventions: a systematic review. BMC Public Health. 2015;15(1):582–595. doi:10.1186/s12889-015-1935-7
19. Nielsen JG, Lueg R, Liempd DV. Challenges and boundaries in implementing social return on investment: an inquiry into its situational appropriateness. Nonprofit Manag Leadersh. 2020;1–23. doi:10.1002/nml.21439
20. Masters R, Anwar E, Collins B, Cookson R, Capewell S. Return on investment of public health interventions: a systematic review. J Epidemiol Community Health. 2017;71(8):827–834. doi:10.1136/jech-2016-208141
21. Gosselin V, Boccanfuso D, Laberge S. Social return on investment (SROI) method to evaluate physical activity and sport interventions: a systematic review. Int J Behav Nutr Phys Act. 2020;17(1):26. doi:10.1186/s12966-020-00931-w
22. Ashton K, Schröder-Bäck P, Clemens T, Dyakova M, Stielke A, Bellis MA. The social value of investing in public health across the life course: a systematic scoping review. BMC Public Health. 2020;20(1):597. doi:10.1186/s12889-020-08685-7
23. Hutchinson CL, Berndt A, Forsythe D, Gilbert-Hunt S, George S, Ratcliffe J. Valuing the impact of health and social care programs using social return on investment analysis: how have academics advanced the methodology? A systematic review. BMJ Open. 2019;9(8):e029789. doi:10.1136/bmjopen-2019-029789
24. Jones C, Hartfiel N, Brocklehurst P, Lynch M, Edwards RT. Social return on investment analysis of the health precinct community hub for chronic conditions. Int J Environ Res Public Health. 2020;17(14):5249. doi:10.3390/ijerph17145249
25. Merino M, Jiménez M, Manito N, et al. The social return on investment of a new approach to heart failure in the Spanish National Health System. ESC Heart Fail. 2020;7(1):130–137. doi:10.1002/ehf2.12535
26. Carretero G, Moreno D, González Domínguez A, et al. Multidisciplinary approach to psoriasis in the Spanish National Health System: a social return on investment study. Glob Reg Health Technol Assess. 2020;7(1):50–56. doi:10.33393/grhta.2020.2146
27. Moral Torres E, Fernández Fernández Ó, Carrascal Rueda P, et al. Social value of a set of proposals for the ideal approach of multiple sclerosis within the Spanish National Health System: a social return on investment study. BMC Health Serv Res. 2020;20(1):1–16. doi:10.1186/s12913-020-4946-8
28. Merino M, Ivanova Y, Martín Lorenzo T, Hidalgo-Vega Á. Improving rheumatoid arthritis management within the Spanish National Health System: a social return on investment study. Clin Exp Rheumatol. 2022;40:104–111. doi:10.55563/clinexprheumatol/mh38sy
29. Soto I, Mateo J, García-Diego DA, et al. The impact of improving haemophilia A management within the Spanish National Healthcare System: a social return on investment analysis. BMC Health Serv Res. 2022;22(1):115. doi:10.1186/s12913-021-07447-4
30. Ministerio de Sanidad, Consumo y Bienestar Social. Estadística de gasto sanitario público 2019. Principales resultados [Public health expenditure statistics 2019. Main results]; 2021. Spanish.
31. de Miguel-Díez J, Carrasco-Garrido P, Rejas-Gutierrez J, et al. Inappropriate overuse of inhaled corticosteroids for COPD patients: impact on health costs and health status. Lung. 2011;189(3):199–206. doi:10.1007/s00408-011-9289-0
32. Ulrik CS, Hansen EF, Jensen MS, et al. Management of COPD in general practice in Denmark – participating in an educational program substantially improves adherence to guidelines. Int J Chron Obstruct Pulmon Dis. 2010;5:73–79. doi:10.2147/copd.s9102
33. Puente-Maestu L, Calle M, Rodríguez-Hermosa JL, et al. Health literacy and health outcomes in chronic obstructive pulmonary disease. Respir Med. 2016;115:78–82. doi:10.1016/j.rmed.2016.04.016
34. Amado CA, Pérez-García C, Fernández BT, Agüero-Calvo J, Muñoz-Cacho P, Golpe R. Information needs in COPD after an educational programme: influence in exacerbations and admissions. Int J Chron Obstruct Pulmon Dis. 2020;15:2663–2671. doi:10.2147/COPD.S275002
35. Trapero‐Bertran M, Muñoz C, Coyle K, et al. Cost‐effectiveness of alternative smoking cessation scenarios in Spain: results from the EQUIPTMOD. Addict Abingdon Engl. 2018;113(Suppl 1):65–75. doi:10.1111/add.14090
36. Observatorio Español de las Drogas y las Adicciones. Encuesta sobre alcohol y otras drogas en España, EDADES 2019/20. [Survey on alcohol and other drugs in Spain, EDADES 2019/20]. Ministerio de Sanidad. Delegación del Gobierno para el Plan Nacional sobre Drogas. 2021. Spanish.
37. Lopez-Campos JL, Almagro P, Gómez JT, et al. Actualización de la Guía Española de la EPOC (GesEPOC): comorbilidades, automanejo y cuidados paliativos [Update on the Spanish COPD guideline (GesEPOC): comorbidities, self-care, and palliative care]. Arch Bronconeumol. 2021:S0300289621002167. Spanish. doi:10.1016/j.arbres.2021.08.002
38. Pullen R, Miravitlles M, Sharma A, et al. CONQUEST quality standards: for the collaboration on quality improvement initiative for achieving excellence in standards of COPD care. Int J Chron Obstruct Pulmon Dis. 2021;16:2301–2322. doi:10.2147/COPD.S313498
39. Banke-Thomas A. What about the issues in using social return on investment as an evaluation tool? Eval J Australas. 2018;18(1):64–68. doi:10.1177/1035719X17753984
40. Pokhrel S. Return on investment (ROI) modelling in public health: strengths and limitations. Eur J Public Health. 2015;25(6):908–909. doi:10.1093/eurpub/ckv136
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.