")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
“Working in the Dark”: Experiences of Frontline Health Workers in Bangladesh During COVID-19 Pandemic
Authors Das Pooja S , Nandonik AJ , Ahmed T , Kabir ZN
Received 9 February 2022
Accepted for publication 23 March 2022
Published 25 April 2022 Volume 2022:15 Pages 869—881
DOI https://doi.org/10.2147/JMDH.S357815
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shangjucta Das Pooja,1 Ahmed Jojan Nandonik,1 Tanvir Ahmed,1 Zarina Nahar Kabir2
1SAJIDA Foundation, OTOBI Center, Dhaka, 1212, Bangladesh; 2Department of Neurobiology, Care Sciences and Society, Karolinska Institute, Huddinge, 141 83, Sweden
Correspondence: Shangjucta Das Pooja, SAJIDA Foundation, OTOBI Centre, 5th Floor, Plot 12, Block CWS(C), Gulshan South Avenue, Dhaka, 1212, Bangladesh, Tel +880 1670733453, Email [email protected]
Introduction: Frontline health workers (FHW) are working relentlessly to combat the COVID-19 pandemic globally. This is particularly challenging for low- and middle-income countries such as Bangladesh because of resource scarcity. Therefore, it is critical to understand the challenges of healthcare providers to help shaping a contextual pandemic response plan address current and future similar crises.
Aim: This study aimed to describe the challenges faced by FHWs in Bangladesh in terms of information on COVID-19, managing patients with COVID-19, and what motivated them to continue providing service during the pandemic.
Methods: This qualitative study explored the experiences of 18 FHWs who were purposely recruited from different health interventions of a development organization in Bangladesh. In-depth interviews and focus group discussions were conducted during July–August 2020 using a semi-structured interview guide. The interviews were transcribed verbatim and content analysis was used to analyze the data which led to four categories.
Results: Four main categories and ten sub-categories emerged from the analysis. Categories derived from the analysis were as follows: i) experiences of the FHWs regarding information on COVID-19: “Working in the dark”, ii) experience of providing care: “Patients are grateful”, iii) impact on personal/family life: “Life is still in lockdown” and iv) motivation to carry on providing care.
Conclusion: FHWs desire a stable information source to prepare themselves for future health care crises. Organizational support is essential for them to overcome physical and mental struggles and keep themselves motivated to continue service provision during pandemics.
Keywords: frontline health workers, COVID-19, pandemic, low- and middle-income countries, Bangladesh
Introduction
Bangladesh has long been considered as a paradox in global health. Despite low spending in health (3.5% of gross domestic product),1 Bangladesh has made remarkable progress in key global health indicators over the last few decades.2 Health indicators such as average life expectancy and coverage of immunization services have considerably improved, infant mortality rate, maternal mortality ratio and total fertility rate declined.3 However, such progress is not uniformly distributed across the country. From a health system viewpoint, there is still considerable disparity in access to healthcare. Such disparity becomes visible when access to healthcare is stratified by various socioeconomic groups and geographic regions. Similar to many low- and middle-income countries (LMICs), Bangladesh has a number of structural causes for this long-standing disparity in health. Among those, lack of human resource for health (HRH) is one of the main concerns.4
Bangladesh suffers from both critical shortage of HRH5 and its unequal distribution especially between rural and urban areas.6 The doctor to population ratio in Bangladesh is 0.6 to 1000 and nurse-midwives to population ratio is 0.4 to 1000 people.7 This is low when compared to World Health Organization (WHO) endorsed desirable doctor–population ratio of 1:1000.8 According to a health facility survey conducted in 2013, more than 25% of physician positions and 22% of nurse positions at upazila (sub-district) health complexes were vacant.9 Poor living conditions, excessive workload, lack of proper equipment, limited career opportunities, insufficient wages and benefits in rural areas are some of the main causes of absenteeism of health care providers in rural areas of Bangladesh.6 In addition, HRH in Bangladesh often has to work within intense resource constraints leading to lack of provision of quality service. This adds to unfavorable work condition which in turn leads to peoples’ dissatisfaction in utilization of health care services. As a result, there is periodic incidence of violence against HRH across the country.10,11
With this backdrop of challenging HRH situation, Bangladesh confirmed its first case of COVID-19 on March 8, 2020 and has been burdened with 1.59 million confirmed cases and more than 28 thousand deaths from COVID-19 as of January 10, 2022.12 COVID-19 has created unprecedented psychosocial and socio-economic instability among people due to the loss of lives and livelihoods.13
A population-based study from Bangladesh reported mental health-related problems such as loneliness (71%), anxiety (64%), depression (38%) and sleep disturbance (73%) during COVID-19 pandemic.14 Health workers in particular face enormous challenges as one of the key frontline workers during the COVID-19 pandemic.15 Globally, the risk of COVID-19 infection was very high among the FHWs compared to the general community.16–18 Studies also found that FHWs who were involved in the care of COVID-19 patients have also been exposed to negative mental health outcomes like anxiety, depression, and insomnia.19,20 Moreover, FHWs have faced different professional and psychosocial challenges while working in COVID-19 dedicated facilities. Less support from family, harsh working environment,21 fear of contaminating family members,22 adaptation with continuously changing guidelines, practice and policies, lack of personal protective equipment (PPE)23 were some of the challenges faced by FHWs throughout this pandemic. In Bangladesh, where the health care system is already burdened with crisis of resource constraints and lack of HRH, the FHWs have to endure tremendous pressure to work endlessly during the COVID-19 pandemic thus placing them at high risk of exposure to the disease.24 So it is critical to understand the challenges of healthcare providers considering their fight from the front during the COVID-19 pandemic.
This study aimed to describe the challenges faced by FHWs in Bangladesh in terms of information on COVID-19, managing patients with COVID-19 and what motivated them to continue providing service during the pandemic.
Materials and Methods
Design
This qualitative descriptive25 study aimed to describe the experiences of FHWs in relation to providing services to patients with COVID-19 during the ongoing pandemic.
Study Setting
This study was conducted on a group of FHWs who were working in different health initiatives of SAJIDA Foundation (SF), one of the leading development organizations in Bangladesh. As part of its health programs, it provides tertiary health care services. The organization converted one of its hospitals, in Narayanganj (27 kilometers from Dhaka), into a hospital dedicated only for patients with COVID-19. SF also set up a hotline service to provide free medical advice to the general public. During the pandemic, SF offered round the clock service to chronically ill patients at home by formal caregivers.
Participants and Sampling
Using purposive sampling method, participants of this descriptive qualitative study were selected from the hospital (physicians and nurses), health information hotline service (physicians) and home care service (formal caregivers with paramedic training) of SAJIDA Foundation (SF), all dedicated to patients of COVID-19. Twenty-three FHWs were approached for interview, among them five declined. Thus, a total of 18 participants were interviewed. Of the 18 participants, 11 were physicians, 5 nurses and 2 formal caregivers. The participants included equal number of men and women (Table 1). 4 `Seven individual interviews (two formal caregivers, one hospital nurse, four physicians) and three focus group discussions (one group of three hospital physicians, one group of four physicians of hotline service, one group of four hospital nurses) were conducted by two of the co-authors (SDP & AJN) who were trained on qualitative data collection.
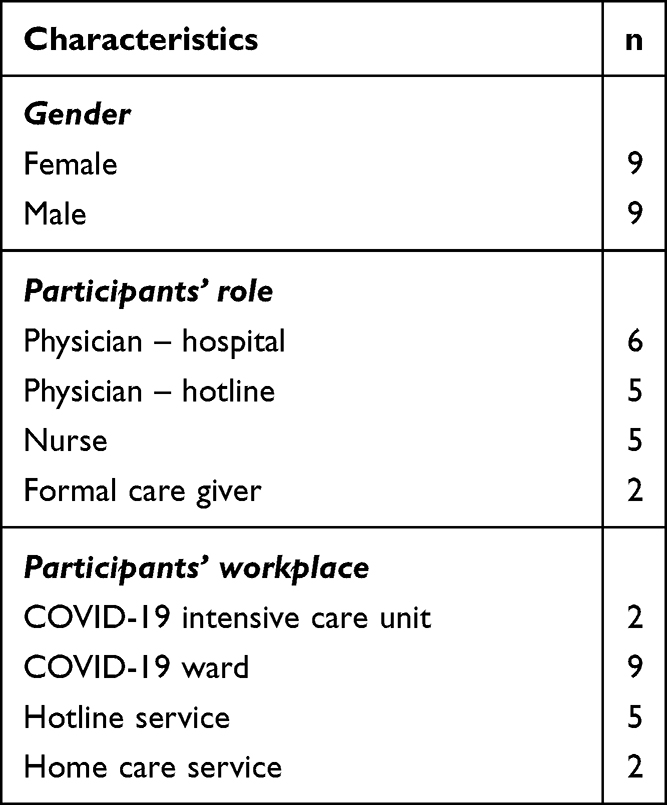 |
Table 1 Characteristics of the Participants |
Data Collection
Using semi-structured interview guide, in-depth interviews and focus group discussions were conducted with the participants during July and August, 2020. The participants were reached through telephone. The interview guide was developed based on relevant literature and discussion within the research team. The interview guide was pre-tested with two FHWs (one physician and one nurse) who were not included in the study. The interviews were conducted via telephone or online communication platform (Microsoft Teams) due to the physical distancing protocols during COVID-19 pandemic. Each individual interview lasted for 40–50 minutes and each focus group discussion lasted for 100–110 minutes. All interviews were audio recorded with permission from the participants. This study was conducted under the purview of SAJIDA Foundation which did not require a formal ethical approval particularly due to the non-invasive nature of the study. Ethical guidelines outlined in the Declaration of Helsinki was followed in the study. Before the initiation of the interview, informed consent was obtained and audio recorded. Participants were informed about the objectives of the study, data confidentiality, anonymity of the study participants, and their right to withdraw from the study at any time. A unique identification number was allocated for each participant, by which, deidentification of the participants was ensured. All data were stored on a password protected cloud storage system which was accessible by the researchers only. No institutional ethical approval was required for this study.
Data Analysis
After all the interviews were transcribed in Bangla, analysis was performed applying inductive approach using content analysis.26 The co-authors read the transcripts multiple times (all transcripts by SDP and AJN, selected few by ZNK and TA) to identify codes. The codes were organized to identify common patterns and grouped as sub-categories and the latter into categories. The analysis followed an iterative process which eventually resulted in four categories. Codes were checked against the transcripts independently by the researchers and through regular team meetings during data analysis, until decision regarding the sub-categories and categories were reached.
The iterative nature of the analysis process helped to identify codes, sub-categories and categories by each of the team members individually and in group. This led to triangulation by researchers at the analysis level. Even the use of different data collection tools, ie, individual interviews and focus group discussions contributed to triangulation of the data.
Results
The data analysis resulted in four categories: Experiences of the FHWs regarding information on COVID-19: “Working in the dark”, Experience of Providing care: “Patients are grateful”, Impact on personal/family life: “Life is still in lockdown” and Motivation to carry on providing care (see Table 2). Findings related to the categories are illustrated by quotes. Key quotes presented in the paper were translated into English. Quotes by specific participants are referred to as “P” and the participant’s number.
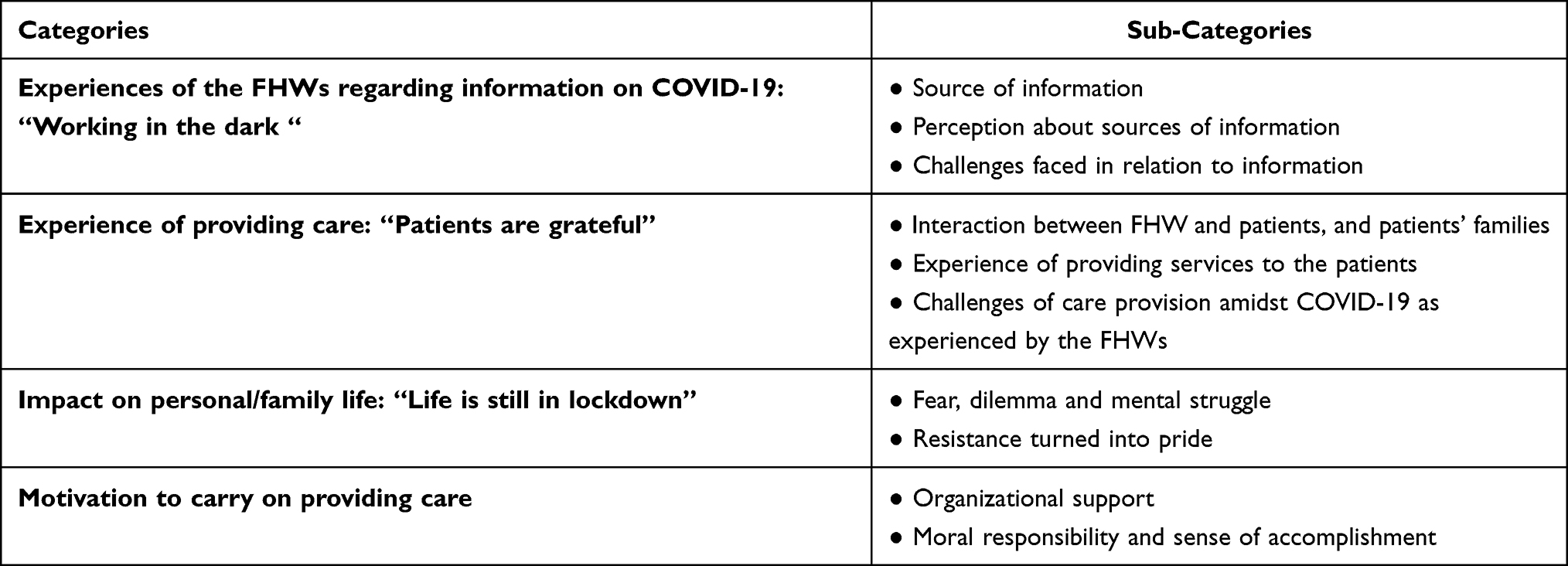 |
Table 2 List of Categories and Sub-Categories |
Experience of the FHWs Regarding Information on COVID-19: “Working in the Dark”
The FHWs were asked about their experience about COVID-19 related information on its preventative measures, and its diagnosis and treatment. While discussing the information sources, they shared their perception in terms of the authenticity and/or quality of these sources. Participants also mentioned challenges they faced in accessing and using the information.
Source of Information
When asked about the information sources almost all participants agreed that in a pandemic it is expected to have information which were haphazard and inaccurate. Training programs organized at the workplace, Television, YouTube and social media, and shared knowledge among colleagues were stated as the main sources of information for the nurses and home caregivers. One of the participants, a nurse, mentioned “Initially I did not know how to wear and remove PPE. Our hospital has provided trainings on this and also informed us about the updates on a regular basis.” (P5, nurse at hospital). On the other hand, institutional guidelines such as from WHO, Government of Bangladesh, Center for Disease Control (CDC) in USA, Institute of Epidemiology, Disease Control and Research (IEDCR) in Bangladesh, National Health Services (NHS)- UK were the main sources of information for the physicians. Some followed ongoing national and international clinical trials, while others relied on suggestions provided by their senior medical experts and leveraged their own clinical observations/experiences as sources of information to guide treatment of patients with COVID-19 (suspected or positive cases). Many physicians combined the suggestions and guidelines collected from various sources as the basis to treat patients. A physician explained, “We have tried to treat our patients by blending WHO guideline and clinical observations made by our expert clinicians and ourselves as junior doctors.” (P2, physician at hospital). All the participants believed continuous scientific research on COVID-19 was required to develop more user friendly and precise guidelines.
Perception on Sources of Information
While participants identified many sources of information on how to prevent and treat COVID-19, they mentioned only few to be reliable. When asked about their preferred sources, physicians referred to the guidelines by the Ministry of Health and Family Welfare (MoHFW) and from WHO as the most reliable ones. In addition, a physician of hotline service, found the national guidelines more relevant to the Bangladeshi context compared to those by WHO. According to the participant, the national guidelines were more contextualized and appropriate taking into the account the existing available resources and logistical support in Bangladesh. A participant described:
It is difficult for everyone to follow the WHO guideline because of the differences in logistical support in different countries. For this reason, each country has their own guideline that is unique. Designated professionals of our country maintain this guideline with utmost care, so I prioritize national guideline in the first place. (P6, physician at hospital).
Sharing knowledge between colleagues was found as a common source of information. P17, one of the nurses, implied that more group discussions, focused meetings and trainings would have disseminated COVID-19 related information better. Some advised to have a centralized information source and recommended establishing a system consisting of information regarding testing facilities, capacity of hospitals dedicated for patients of COVID-19 and updated treatment protocols. One participant expressed,
If we had a website or portal in Bangladesh, the physicians could get access necessary information in one place by logging in. (This would have been particularly important) as sometimes we have found difference between the WHO and national guideline. (P9, physician at hotline service).
Challenges Faced in Relation to Information
When asked about major challenges faced by the participants in relation to information on COVID-19, issues like contradictory information, authenticity of information and continuous changes in guidelines were mentioned the most. Participants felt that information related to COVID-19 was not sufficient and if available it was hard to assess its authenticity. One of the physicians from the hotline service reported that mainstream media was responsible for circulating contradictory information and advocating medicine without evidence. According to the participant:
Media was circulating news that a certain drug will cure Corona with a reference from a specialist physician. A drug cannot be used without clinical trial or prior approval. But the headline on the media was presented in a way that a certain drug will work and its trial has been completed. But later on, it was clarified by our supervisor (specialist himself) that the trial of that specific drug was still ongoing. (P9, physician at hotline service).
Furthermore, physicians provided hotline services reported challenges with referral system caused by lack of adequate information about the existing capacity of hospitals to admit patients and available testing facilities. They would refer the caller to a nearby hospital without being completely sure if the hospital had the capacity to take another patient or if the testing facility was available at that particular time. This created confusion and difficulties for both the physician and the caller.
Considering such disarray, challenges of availability and accessibility of reliable information, one participant mentioned that working in the pandemic felt like “working in the dark.” However, participants also reported to have managed to adapt with the changing guidelines as the guidelines became more uniform overtime and modified their treatment pattern accordingly. As one of the participants mentioned,
I used to give Azithromycin following the national guideline, initially it was like working in the dark as there was a lot of modification going on in drugs and other guidelines keeping the basic things in place. (P10, physician at hotline service).
Experience of Providing Care: “Patients are Grateful”
The FHWs discussed their experiences of providing care from three viewpoints: interaction with patients and their families while providing care, medical management of the patients and challenges they faced while providing care.
Interaction Between FHW and Patients, and Their Families
According to the participants, knowledge of the patients and their family members about COVID-19 influenced the treatment pattern offered by the FHWs. Participants also stated that the care seeking behavior of the patients changed over time as they (patients) became more knowledgeable about COVID-19. Some of the physicians explained that during the early stage of the pandemic, due to fear of death, people were often inclined to opt for hospitalization even at the slightest possibility of COVID-19 infection. However, over time with more awareness, patients were more agreeable about isolating and managing the disease at home. As one of the participants said:
Patients were rushing to hospitals even with slightest symptoms like cough or mild fever thinking that s/he is COVID-19 positive … But people are now aware that being a COVID-19 positive patient does not necessarily mean that s/he will die. People are now staying isolated at home and trying to boost their immunity. (P6, physician at hotline service).
While this was helpful for providing services, sometimes such improved knowledge was coupled with misinformation resulting into taking unprescribed medicines and sometimes without completing the necessary course of medication. One of the physicians shared:
There was a shortage of tests in the beginning, patients could not do the tests even if they were asked to do. Names of certain drugs were circulating and people thought that they would recover by taking these. Many people are in greater danger by self-medicating and without completing the dosage. (P10, physician at hotline service).
FHWs talked about strengthening bond between them and the patients during this stressful time. Participants stated that patients’ trust and confidence in the physicians and nurses increased during this pandemic as they were the only people who were physically available for the patients. Participants from the hotline service added that patients were grateful towards them as well. The participants explained that this was due to the harsh reality of COVID-19 and them (physicians) becoming the sole savior in the eyes of the patients. Such attitude was in contrast to their experiences from the time before the pandemic. As one of the physicians stated,
When I used to work in normal (Non COVID-19) hospitals, behavior of the patients’ attendants then and now is totally different. They are now showing gratefulness towards us. (P2, physician at hospital).
Family members relied solely on them (FHWs) to take care of their dear ones. As one of the nurses mentioned, “Patients also realized that we (FHWs) were the only people who were staying beside them, so they never misbehaved with us.” (P5, nurse at hospital).
Sometimes family members of patients seemed to anticipate and accept the ultimate fate of their dear ones. There were incidents of family members “nowhere to be found” after admitting patients to the hospital. As one of the physicians stated:
The attitude of the majority of the patients’ attendants here [at the hospital] was that they gave up hope about the patient … In many cases, the experience is even more horrible. Family members bade farewell to the patients as they left them at the hospital. (P3, physician at hospital).
Experience of Providing Services to the Patients
Participants working in different health care settings such as home care, hospital dedicated to patients with COVID-19 and hotline services shared their experiences of managing patients. Most of the physicians mentioned that the clinical management was mainly focused on symptomatic treatment that was based on the severity of the symptoms. Formal caregivers providing home care had to complete quarantine before beginning service and often had to explain in detail to the client and his/her family about the preventative practices and safety measures that would be followed at work.
Preventative practices for COVID-19 were relatively new thus, all the participants expressed the physical and mental stress they felt while continuously using personal protective equipment (PPE) such as face masks, gowns and goggles for long hours. Physicians and nurses working at the hospital faced problems with breathing, exhaustion, nausea, stress and headache from wearing PPE every day. One of the physicians stated:
“Initially when I started to use PPE, I used to have shortness of breath while wearing N95 mask for long period, I could not wear more than an hour.” (P2, physician at hospital).
However, gradually most of the participants claimed to have gotten accustomed to PPE and felt that they may benefit from such practice even after COVID-19 comes under control.
Challenges of Care Provision Amidst COVID-19 as Experienced by the FHWs
Participants talked about challenges they faced while providing health care services. One of the major challenges of managing patients with COVID-19 was irrational and unsupported demand for specific prescription by patients and/or their family members due to the influence of their social network and the media. In this connection, one of the physicians mentioned, “There was a demand for a certain drug among patients, they were confused about taking that drug.” (P9, physician at hotline service). The nature of challenges faced by the hotline service physicians were a bit different than the other participants. In absence of face-to-face observation, real time assessment of patients was not possible which had an effect on the treatment pattern. On top of it, difficulties in communicating over phone further contributed to the existing challenges of assessing patients. Providing treatment without seeing the patient physically was a problem to make accurate diagnosis. However, they tried to provide treatment to the patients with patience and sincerity. One of the hotline physicians stated:
As we cannot see the patients over hotline, so we are doing our work based on patient’s statement. For example, when a patient says, he/she is suffering from severe breathlessness we consider him/her as a patient of severe respiratory syndrome. (P8, physician at hotline service).
Participants talked about the sufferings of the patients and FHWs due to the errors of the existing health system in the country. One of the physicians expressed dissatisfaction due to lack of coordination between different tiers of the health system as a result of which the patients had difficulties in accessing health care. For instance, there was no proper information regarding testing facilities, such as its location, availability of testing services, cost, etc. This also affected effective referral in ways such as difficulties in ensuring if the patients visited the facilities they were referred to. Moreover, P6 thought that due to lack of proper isolation practices COVID-19 infection was spreading rapidly which in turn made the prevailing health system vulnerable in terms of human resources for health and medical equipment in the hospital.
Our system was not standing on the base it was supposed to be. Making a good rule of thumb for those in managerial positions and fixing some measures in advance by anticipating what the situation might be at some point; these things were lacking. For example, how many tests should be done every day, how easily can the tests be delivered to the people without any kind of harassment to the people, to maintain isolation properly from the beginning to the end …. Due to not maintaining such isolation properly, Corona spread that way. How many kits and how many doctors need to be provided in those hospitals to deal with it? All of this took a toll. (P6, physician at hotline service).
Impact on Personal and Family Life: “Life is Still in Lockdown”
The participants in the study shared their experiences of how their personal lives were affected due to their role as a FHW during COVID-19 pandemic and how they coped.
Fear, Dilemma and Mental Struggle
Participants who worked at the hospital dedicated for patients of COVID-19 mentioned that initially they were in dilemma about joining the hospital. They were afraid of impending death as the COVID-19 infection was rising across the globe as was its death toll. However, many disregarded their fear out of a sense of commitment for duty, ie, serving the country as well as humanity and looked upon the responsibility of serving during the pandemic as an opportunity. One of the physicians referred to this as a unique learning opportunity, “This situation was new to everyone which created fear and anxiety but we worked with courage. It was a unique experience that will help me in future.” (P2, physician at hospital).
Another participant, a formal caregiver providing home care, mentioned the restrictions imposed by the patient’s family during the pandemic necessitated her to stay away from her family for as long as five months. It was not easy to convince her own family members to accept such a long absence. When others were going back to their normal life over time, P2 described that those who worked in health care service were “still in lockdown”.
I’m connecting to my family over phone when necessary … saying Hi to my parents, asking how they are doing. They were also checking on me, how I was doing …. how I was managing things during COVID-19 spread … I told them not to worry … my husband wasn’t convinced at first that I would be detached for five months, but he accepted later on … (P7, formal caregiver at home care).
Similar view was expressed by another participant,
Things have changed in Bangladesh. People are going back to the normal lifestyle, but we can’t. But those who work in the health sector seems like we are still in lockdown. (P2, physician at hospital).
Participants spoke about their mental stress and struggle during the pandemic. P6, a physician, talked about the void in life for staying away from the family members to maintain physical distancing. Participants maintained regular communication with their family members while staying away from home. Another physician, P10, expressed concern about her career as her examination got postponed due to the pandemic. Depression and stress were prominent due to the restriction of movement and excessive workload. One participant mentioned:
All I can say is, everyone seems a little depressed or frustrated. I can’t move about freely or see my family. Since we are exposed to COVID-19 we have to maintain a lot of things. This is hampering our normal lifestyle as we can’t do things the way we want to. We [physicians] are getting depressed. (P15, physician at hospital).
Guilt of spreading the virus and infection to the family members was another psychological stress that the participants had to deal with on regular basis. As one of the participants mentioned:
The hospital I was working in has arranged a place for me to stay. I went to see my mother during Ramadan. I guess my mother caught COVID-19 from me. I felt guilty. (P4, physician at hospital).
Another participant shared his story of how he had to refrain from seeing his father who was admitted for treatment for COVID-19 in the same hospital where he was working. It was very depressing, yet he had to stay true to his responsibility, guidelines on COVID-19 and his profession.
When my father was sick, he was right in front of me [at the hospital], but he couldn’t see my face and I couldn’t touch him; I was wearing PPE. After 26 days, he saw me, which was a big relief for me. We had to overcome the mental depression we faced. (P14, physician at hospital).
Almost all the participants mentioned that working as a FHW was not liked by the wider community and was perceived to be a stigmatized role. One of the physicians from the hospital dedicated for patients of COVID-19 shared her story about how she was evicted from the dormitory when the authority came to know about her role as a FHW in the COVID-19 pandemic.
To be honest, I hide that information [about joining COVID-19 hospital]. I said I was in a training program at medical college which actually was true. When I started my shift as a medical officer, I received an eviction notice from my hostel. It was a shock for me as I didn’t have anyone else in the city. (P3, physician at hospital).
A Story of “Resistance Turned into Pride”
Most of the participants said that they faced resistance from their families when they decided to work at a hospital that was dedicated for patients of COVID-19. Some had to hide the fact from the family while some faced problems in their marital life. However, over time the family members felt secure as they remained healthy and did not get infected while working with patients of COVID-19. The participants mentioned that they were extra cautious in following preventative practices to keep their family members safe from COVID-19. Thus, over time, the resistance and the fear gradually turned to pride and satisfaction. As one of the participants stated: “Initially, I didn’t let my parents and my father-in-law know about me joining there [COVID-19 hospital]. Only my husband knew, but he was not in favor.” (P3, physician at hospital).
A participant also added, “A lot has changed. I have the support of my mother and my sisters. Now they understand the gravity of the situation, and they feel proud of me.” (P2, physician at hospital).
Motivation to Carry on Providing Care
The study participants talked about their motivation to carry on providing service as an FHW. They mentioned how their organization provided a conducive environment for them, their own sense of moral responsibility and sense of accomplishment which motivated them to carry on providing care during the COVID-19 pandemic.
Organizational Support: “Place of Relief”
Participants appreciated the support they received from their own organization which was not available to many FHWs who were working at other health facilities. For instance, participants talked about the inadequacy of PPE in different Government institutions and expressed gratitude to their own organization for providing adequate PPE and ensuring their safety. P14 also praised their leadership that all categories of staff members were equally respected by the organization. One of the organizational factors for which the participants were very grateful was that their organization made its healthcare facilities available not only for the staff but also for their family members. This was crucial as it was as struggle to get access to healthcare facilities which were flooded with patients. As P14 stated,
Maybe that was the reason that Almighty put me in a COVID-19 unit so that I could serve my father [patient]. If I wasn’t here [working at COVID-19 unit] my father may or may not have received his treatment in a hospital … where else could I take him? It would have been uncertain … After that incident [father getting admitted to the hospital] everyone showed their support. (P14, physician at hospital).
The participants’ organization provided residential facilities for the FHWs during the period they stayed away from their families as a precautionary measure. Participants appreciated the bonding created amongst colleagues which helped them to relieve work-related stress and cope with the mental struggle of staying away from their families. They valued the support from colleagues and the time they spent together. It helped to keep them rejuvenated during this pandemic. P15, talked about playing games and meditating to divert his mind from the everyday struggle.
Moral Responsibility and Sense of Accomplishment: “Call of Duty”
Most of the participants talked about their moral duty as health care professionals to work in a crisis such as a pandemic despite resistance from their families. They mentioned that their commitment to serve humanity motivated them to work in this pandemic. Participants felt that the decision to work in COVID-19 pandemic was the right one. This experience will always be something to remember and share with future generations. One of the participants said:
Am I going to sit at home while others [doctor’s] are fighting the war [pandemic]! … it is not that I’m expecting a medal from the government or my name in the newspaper or any kind of recognition. But in the future, when all this ends … when I’ll have grandchildren, then I’ll tell them that there was a pandemic in 2020, and I served as a frontliner back then. (P14, physician at hospital).
In addition to their sense of moral responsibility, acknowledgement of their service directly by the patients and their family members gave a sense of accomplishment for the participants. This helped the FHWs to endure all the strenuous and stressful work during the pandemic. One of the participants felt that blessings and prayers from patients and their family members were the greatest reward of their professional lives.
I would say that it (attitude of patients’ family members) was different in this COVID-19 situation. Family members of discharged patients used to call us over the phone to show their thankfulness which I cannot express in words! It was a gratifying moment in my life. I received a lot of prayers, and it was a good experience. (P3, physician at hospital).
P13 expressed hope that someday the world will be back to normal and people can move about freely again.
Just like everyone else I desire that every person will recover and the world will heal again. Right now, it feels like we are restrained, and we are not free. I am hoping for that moment when we will be able to walk freely in this world again. (P13, physician at hospital)
Discussion
COVID-19 has unfolded major gaps in responding to emergencies like the COVID-19 pandemic especially in resource-poor health systems like Bangladesh.27 As soon as the first case was identified, limited testing facilities, lack of provision of appropriate management and coordinated effort to implement Infection prevention and control (IPC) related measures resulted into widespread confusion among people and FHWs. Moreover, electronic including social network-based media contributed to this mass confusion.28 As a result, the cases started rising rapidly which further contributed to the surge in demand for frontline health workers to work in hospitals.15 With this backdrop, this study describes the experience of health workers serving at the frontline at the time of COVID-19 pandemic in Bangladesh. Their experience was categorized into four areas: access to and experience of information on COVID-19, experience of providing care, impact on personal and family life, and motivation to carry on providing care. This helped in understanding the challenges of providing healthcare services during COVID-19 in Bangladesh and how these challenges can be addressed to embark on a contextualized response plan for potential pandemics, especially in a resource poor setting.
It was evident from the findings that availability and access to accurate and up to date information played a major role in providing quality healthcare by the FHWs. Previous studies and experience of pandemic have highlighted how access to such relevant and accurate information can increase health care providers’ knowledge and ensure positive attitude towards patients which thereby contribute in shaping the provision of healthcare.29–31 In line with the findings of this study, earlier studies have also pointed out that international guidelines such as from WHO can often be “generic” and “not country-specific”.32 This was the very reason for FHWs to consider national guidelines to be more relevant and effective while providing services. One of the most important characteristics of information sources and guidelines appeared to be its consistent flow. The finding of this study suggests that because of the novel nature of the pandemic and global multidisciplinary studies, new evidence was emerging very frequently, sometimes on daily basis. Due to the continued national priority and effort in considering newer and relevant evidence, these guidelines became more accurate, uniform and effective over time which was extremely helpful in managing patients. Previous studies have reported that health workers desired consistent information and guidance but rapidly changing recommendations can lead to confusion and inconsistencies in service provision.33 Findings from this study shows that there was a lack of a unified platform which could have been very handy for the FHWs to access information when in need and not turn to unstructured internet browsing and/or social media and land on spurious information which could potentially mislead appropriate medical practice.
According to the finding of this study, the major challenge which had a significant impact on management and care provision during the pandemic was knowledge about COVID-19 of the patients and their family members, and that of the family members of the FHWs. As described in the findings, care seekers’ inadequate knowledge about COVID-19 misled them into taking unprescribed medicines and not following isolation protocols. This was a major challenge for the FHWs as well as the hospital authorities to ensure COVID-19 infection risk free environment in the hospital. Similar finding was reported by a study in Ethiopia, which described poor knowledge on COVID-19 led to poor practice towards IPC protocols among the care seekers.34 Working in a COVID-19 unit meant being exposed to COVID-19 patients. Those who came forward to join COVID-19 unit of a hospital were faced with resistance from their family. However, both family members of the patients and FHWs eventually settled in with the fear and misconception regarding the pandemic as COVID-19 related information began to gain clarity over time. This further shows how important information can be to ensure effective service provision during pandemics. Therefore, as described before, a uniform information dissemination platform for everyone to seek updated information from could have improved and eased COVID-19 related service provision by the FHWs.
Role of organization in enabling FHWs to render healthcare amidst pandemics emerged to be vital. One of the major challenges for the FHWs was need for a safe working environment. Working amidst COVID-19 pandemic meant that FHWs were at risk of contracting COVID-19 themselves and eventually infecting their household members. As reported in other studies, our findings show that FHWs faced challenges such as high workload, psychological distress, shortage of adequate PPE and social stigmatization while working during the pandemic.15 In healthcare settings, proper use of PPE and other IPC measures are crucial in preventing the transmission and risk of infection of COVID-19.35 A study among intensive care nurses in Spain reported fear of contagion and infecting family and friends due to lack of logistical support and improper management of PPEs in the workplace.36 The organization where the participants of the current study were selected from ensured adequate supply of PPE, provision of safe residence and mental health counselling and peer to peer communication. The participants of this study were satisfied with the provision of PPE arranged by their organization. In addition, the organization also ensured periodic training specifically designed for the FHWs. This helped the FHWs to keep themselves updated with national guidelines and manage patients accordingly. Other studies have found training on COVID-19 related IPC is strongly associated with better knowledge and practices37 and lack of proper training can hinder IPC measures.38 A study among FHWs in Venezuela recommended improved education and training program for FHWs during COVID-19.39 Critical care nurses in Iran mentioned inadequate training, inappropriate work shifts, poor communication, lack of PPE as professional and organizational challenges during this pandemic.40 Studies have reported that FHWs require mental support to increase productivity and motivation in these challenging times.41 Along with support with continuous training, safe working environment, provision of residential facilities to isolate from family members, organizational support towards the family members by offering them emergency admission in the hospital for COVID-19 especially helped in keeping up the motivation of the FHWs to continue to provide services. A study in Romania suggested that continuous observation from national institutions is needed to provide a better psychological follow-up to the FHWs during COVID-19 pandemic.42 A recent study in UK reports that FHWs are in need of a psychological support system that includes peer, organizational and professional support.43
Limitations
Due to the regulations of maintaining physical distance during the COVID-19 pandemic, all interviews were conducted online. This resulted in missing unspoken cues during the interviews which may have contributed to better interpretation of the data. The small sample size of the study and the fact that the study participants consisted of FHWs working at a single organization, as a result the findings from this study may not be transferrable to experiences of FHWs working in other health care settings.
Conclusion
It is very important to have planned effort to respond to and mitigate impact of pandemics like COVID-19 particularly in a resource poor context like Bangladesh. This study has highlighted challenges faced by the FHWs to ensure effective provision of COVID-19 services and its continuity. Such challenges can be addressed in two ways. A reliable contextualized information channel, preferably stewarded by the government, can help both FHWs to render effective services and the general public to comply with hygiene practices and get better guidance in seeking health care. Secondly, organization(s) play a vital role of in providing necessary training, ensuring occupational safety and even social security to the FHWs. This should be incorporated and treated as the cornerstone of a contextualized response and mitigation plan and related policies for the current and future pandemics. However, for this, dialogue and coordination between government and non-government organizations to understand the demand is of paramount importance.
Abbreviations
CDC, Center for Disease control and Prevention; FHW, frontline health workers; HRH, human resource for health; IEDCR, Institute of Epidemiology, Disease Control and Research; IPC, infection prevention and control; LMIC, low- and middle-income countries; MoHFW, Ministry of Health and Family Welfare; NHS, National health services; PPE, personal protective equipment; SF, SAJIDA Foundation; WHO, World Health Organization.
Acknowledgments
The authors would like to thank all the participants for their involvement in the study, including SAJIDA Foundation hospital authority for their support during data collection.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Islam A, Ahsan GBT. Health System Financing in Bangladesh: a Situation Analysis. Am J Econ Financ Manag. 2015;1(5):494–502.
2. Mannan M. Access to Public Health Facilities in Bangladesh: a Study on Facility Utilisation and Burden of Treatment. Bangladesh Dev Stud. 2013;36(4):25–80.
3. Osman FA. Health Policy, Programmes and System in Bangladesh: achievements and Challenges. South Asian Surv. 2008;15(2):263–288. doi:10.1177/097152310801500206
4. Ahmed SM, Hossain MA, RajaChowdhury AM, Bhuiya AU. The health workforce crisis in Bangladesh: shortage, inappropriate skill-mix and inequitable distribution. Hum Resour Health. 2011;9(1):1–7. doi:10.1186/1478-4491-9-3/TABLES/4
5. Mahmood SAI. Health Systems in Bangladesh | insight Medical Publishing. Heal Syst Policy Res. 2012;1(1):1–4.
6. Darkwa EK, Newman MS, Kawkab M, Chowdhury ME. A qualitative study of factors influencing retention of doctors and nurses at rural healthcare facilities in Bangladesh. BMC Health Serv Res. 2015;15(1):1–12. doi:10.1186/s12913-015-1012-z
7. World Bank. Population density (people per sq. km of land area) - Bangladesh | data. World Bank; 2018. Available from: https://data.worldbank.org/indicator/EN.POP.DNST?locations=BD.
8. WHO. Physicians density (per 1000 population). UNdata; 2011. Available from: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/physicians-density-(per-1000-population).
9. Khan MM, Hotchkiss R. Use of a Balanced Scorecard in strengthening health systems in developing countries: an analysis based on nationally representative Bangladesh Health Facility Survey. Int J Health Plann Manage. 2013;28(2):202–215. doi:10.1002/HPM.2136
10. Hasan I, Hassan Z, Bulbul MI, Joarder T, Chisti MJ. Iceberg of workplace violence in health sector of Bangladesh. BMC Res Notes. 2018;11:702. doi:10.1186/s13104-018-3795-6
11. Hossain MM, Sultana A, Shaha T, Rahman MZ, Hossain Nirob MM, Yasmeen S. Violence against health workforce in Bangladesh: a call for action. Int J Community Med Public Heal. 2018;5(5):2151. doi:10.18203/2394-6040.IJCMPH20181739
12. Bangladesh COVID - Coronavirus Statistics – worldometer. Available from: https://www.worldometers.info/coronavirus/country/bangladesh/.
13. Bodrud-Doza M, Shammi M, Bahlman L, Islam ARMT, Rahman MM. Psychosocial and Socio-Economic Crisis in Bangladesh Due to COVID-19 Pandemic: a Perception-Based Assessment. Front Public Heal. 2020;8:341. doi:10.3389/FPUBH.2020.00341/BIBTEX
14. Das R, Hasan MR, Daria S, Islam MR. Impact of COVID-19 pandemic on mental health among general Bangladeshi population: a cross-sectional study. BMJ Open. 2021;11(4):45. doi:10.1136/bmjopen-2020-045727
15. Razu SR, Yasmin T, Arif TB, et al. Challenges Faced by Healthcare Professionals During the COVID-19 Pandemic: a Qualitative Inquiry From Bangladesh. Front Public Heal. 2021;9:1024. doi:10.3389/fpubh.2021.647315
16. Nguyen LH, Drew DA, Graham MS, et al. Risk of COVID-19 among front-line health-care workers and the general community: a prospective cohort study. Lancet Public Heal. 2020;5(9):e475–e483. doi:10.1016/S2468-2667(20)30164-X
17. Mhango M, Dzobo M, Chitungo I, Dzinamarira T. COVID-19 Risk Factors Among Health Workers: a Rapid Review. Saf Health Work. 2020;11(3):262–265. doi:10.1016/j.shaw.2020.06.001
18. Jin H, Chen Y, Fu Q, Qu Q. Occupational risk factors of contracting COVID-19 among health workers: a systematic review. Work. 2021;69(3):721–734. doi:10.3233/WOR-210477
19. Rossi R, Socci V, Pacitti F, et al. Mental Health Outcomes Among Frontline and Second-Line Health Care Workers During the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Netw Open. 2020;3(5):e2010185–e2010185. doi:10.1001/JAMANETWORKOPEN.2020.10185
20. Lai J, Ma S, Wang Y, et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw Open. 2020;3(3):e203976–e203976. doi:10.1001/JAMANETWORKOPEN.2020.3976
21. Shahbaz S, Ashraf MZ, Zakar R, Fischer F. Psychosocial, emotional and professional challenges faced by female healthcare professionals during the COVID-19 outbreak in Lahore, Pakistan: a qualitative study. BMC Women's Health. 2021;21(1):1–10. doi:10.1186/S12905-021-01344-Y/TABLES/1
22. Ali. Assessment of challenges faced by Health Care Workers caring COVID-19. patients at Level-3 COVID-19 Hospital. J Med Sci Clin Res. 2021;09(4):345. doi:10.18535/jmscr/v9i4.10
23. Ness MM, Saylor J, Di Fusco LA, Evans K. Healthcare providers’ challenges during the coronavirus disease (COVID-19) pandemic: a qualitative approach. Nurs Health Sci. 2021;23(2):389–397. doi:10.1111/NHS.12820
24. Hussain M, Begum T, Batul SA, Tui NN, Islam MN, Hussain B. Healthcare workers during the COVID-19 pandemic: experiences of doctors and nurses in Bangladesh. Int J Health Plann Manage. 2021;36(S1):174–181. doi:10.1002/hpm.3154
25. Sandelowski M. What’s in a name? Qualitative description revisited. Res Nurs Heal. 2010;33(1):77–84. doi:10.1002/nur.20362
26. Patton MQ. Qualitative Research and Evaluation Methods: Theory and Practice. SAGE Publications, Inc; 2015.
27. Islam S, Islam R, Mannan F, Rahman S, Islam T. COVID-19 pandemic: an analysis of the healthcare, social and economic challenges in Bangladesh. Prog Disaster Sci. 2020;8:100135. doi:10.1016/j.pdisas.2020.100135
28. Sayeed Al-Zaman M. Healthcare crisis in Bangladesh during the COVID-19 pandemic. Am J Trop Med Hyg. 2020;103(4):1357–1359. doi:10.4269/ajtmh.20-0826
29. Petrie KJ, Faasse K, Thomas MG. Public Perceptions and. Knowledge of the Ebola Virus, Willingness to Vaccinate, and Likely Behavioral Responses to an Outbreak. Disaster Med Public Health Prep. 2016;10(4):674–680. doi:10.1017/DMP.2016.67
30. Suen LKP, So ZYY, Yeung SKW, Lo KYK, Lam SC. Epidemiological investigation on hand hygiene knowledge and behaviour: a cross-sectional study on gender disparity. BMC Public Health. 2019;19(1):1–14. doi:10.1186/S12889-019-6705-5/TABLES/4
31. Joukar F, Mansour-Ghanaei F, Soati F, Meskinkhoda P. Knowledge levels and attitudes of health care professionals toward patients with hepatitis C infection. World J Gastroenterol. 2012;18(18):2238–2244. doi:10.3748/wjg.v18.i18.2238
32. Souadka A, Essangri H, Benkabbou A, Amrani L, Majbar MA. COVID-19 and Healthcare worker’s families: behind the scenes of frontline response. EClinicalMedicine. 2020;23. doi:10.1016/j.eclinm.2020.100373
33. Billings J, Seif NA, Hegarty S, et al. What support do frontline workers want? A qualitative study of health and social care workers’ experiences and views of psychosocial support during the COVID-19 pandemic. PLoS One. 2021;16(9):e0256454. doi:10.1371/JOURNAL.PONE.0256454
34. Feleke BT, Wale MZ, Yirsaw MT. Knowledge, attitude and preventive practice towards COVID-19 and associated factors among outpatient service visitors at Debre Markos compressive specialized hospital, north-west Ethiopia, 2020. PLoS One. 2021;16(7 July):e0251708. doi:10.1371/journal.pone.0251708
35. Deressa W, Worku A, Abebe W, Gizaw M, Amogne W. Availability and use of personal protective equipment and satisfaction of healthcare professionals during COVID-19 pandemic in Addis Ababa, Ethiopia. Arch Public Heal. 2021;79(1):1–14. doi:10.1186/s13690-021-00668-3
36. Fernández-Castillo RJ, González-Caro M-D-D, Fernández-García E, Porcel-Gálvez AM, Garnacho-Montero J. Intensive care nurses’ experiences during the COVID-19 pandemic: a qualitative study. Nurs Crit Care. 2021;26(5):397–406. doi:10.1111/nicc.12589
37. Nepal R, Sapkota K, Paudel P, et al. Knowledge, attitude and practice regarding COVID-19 among healthcare workers in Chitwan, Nepal. J Chitwan Med Coll. 2020;10(3):98–102.
38. Houghton C, Meskell P, Delaney H, et al. Barriers and facilitators to healthcare workers’ adherence with infection prevention and control (IPC) guidelines for respiratory infectious diseases: a rapid qualitative evidence synthesis. Cochrane Database Syst Rev. 2020;4(4):1–55. doi:10.1002/14651858.CD013582
39. Mendoza Millán DL, Carrión-Nessi FS, Mejía Bernard MD, et al. Knowledge, Attitudes, and Practices Regarding COVID-19 Among Healthcare Workers in Venezuela: an Online Cross-Sectional Survey. Front Public Heal. 2021;9:951. doi:10.3389/FPUBH.2021.633723/BIBTEX
40. Chegini Z, Arab-Zozani M, Rajabi MR, Kakemam E. Experiences of critical care nurses fighting against COVID-19: a qualitative phenomenological study. Nurs Forum. 2021;56(3):571–578. doi:10.1111/nuf.12583
41. Brahmi N, Singh P, Sohal M, Sawhney RS. Psychological trauma among the healthcare professionals dealing with COVID-19. Asian J Psychiatr. 2020;54:102241. doi:10.1016/j.ajp.2020.102241
42. Ungureanu BS, Vladut C, Bende F, et al. Impact of the COVID-19 Pandemic on Health-Related Quality of Life, Anxiety, and Training Among Young Gastroenterologists in Romania. Front Psychol. 2020;11. doi:10.3389/fpsyg.2020.579177
43. Nguyen HB, Nguyen THM, Tran TTT, et al. Knowledge, attitudes, practices, and related factors towards covid-19 prevention among patients at university medical center Ho Chi Minh City, Vietnam. Risk Manag Healthc Policy. 2021;14:2119–2132. doi:10.2147/RMHP.S305959
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.