")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Protocol Implementation for Normothermia in Surgery Settings in Italy: Budget-Impact Analysis
Authors Monzani R , Barbera G, Restelli U, Galeone C, Petrini F
Received 16 June 2020
Accepted for publication 1 October 2020
Published 30 October 2020 Volume 2020:13 Pages 2347—2356
DOI https://doi.org/10.2147/RMHP.S267923
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Roberta Monzani,1 Giovanna Barbera,2 Umberto Restelli,3,4 Carlotta Galeone,5 Flavia Petrini6
1Day Hospital Chirurgico, IRCCS Humanitas Research Hospital Rozzano, Rozzano, Italy; 2Independent researcher, Milan, Italy; 3Centre for Health Economics, Social and Health Care Management Carlo Cattaneo University, Castellanza, Italy; 4School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa; 5Bicocca Applied Statistics Center (B-ASC), Università degli Studi di Milano-Bicocca, Milan, Italy; 6Anestesia, Rianimazione e Terapia Intensiva, Università Gabriele d’Annunzio — ASL 2 Abruzzo, Chieti, Italy
Correspondence: Carlotta Galeone
Bicocca Applied Statistics Center (B-ASC), Università degli Studi di Milano-Bicocca, 8 Via Bicocca Degli Arcimboldi, Milan 20126, Italy
Tel +39 02 6448 5823
Email [email protected]
Introduction: Hypothermia is a well-known risk of the perioperative period and considered a preventable effect of anesthesia care. Nevertheless, it is not fully controlled, causing a number of adverse outcomes following surgical operations and thus increasing length of stay in hospital and treatment costs. The aim of this study was to assess the budget impact (BI) of the implementation of proactive strategies to prevent inadvertent perioperative hypothermia (IPH) in surgical patients in Italy, as recommended by international guidelines and by a good clinical practice (GCP) guideline of the Italian Society of Anesthesia, Analgesia, Reanimation, and Intensive Care.
Methods: BI was calculated over a 3-year period from the perspective of the Italian National Health Service (NHS). Model inputs were extracted from national literature when available and otherwise from international sources. The reference analytic model was based on the cost-effectiveness analysis of the National Institute for Health and Care Excellence clinical guidance 65. Estimates were based on assessments made about current malpractice in Italy and on a hypothesis of how future practice might change by implementing the GCP. Model output included overall BI results, variations in the number of warmed patients, medical-device average costs and use of mix.
Results: The base-case estimate quantified a decrease of 35% in extra days of hospital stay due to IPH and a net BI of –€ 60.92 million.
Conclusion: Increasing protocol adoption for preventing IPH would lead to both clinical advantages and significant savings for the NHS. Its large diffusion in Italian hospitals is thus desirable.
Keywords: budget-impact analysis, active-warming systems, inadvertent perioperative hypothermia, Italy, perioperative warming
Introduction
Perioperative hypothermia is defined as central body temperature (CBT) <36°C1 during and after surgery. It is a common event, occurring 20%–70%2,3 of the time. Mild hypothermia (defined as CBT 34°C–36°C4) is the most frequent scenario.5 Inadvertent perioperative hypothermia (IPH) is mainly a result of anesthesia-induced redistribution of body heat that occurs within the first hour after anesthesia induction. Anesthetic agents impair the body’s ability to control and conserve heat by inhibiting vasoconstriction and shivering.5
No significant differences have been observed in general and locoregional anesthesia: both end up causing the same result through different actions. Under normal circumstances, the body controls its temperature with very tight tolerance, the core being 2°C–4°C warmer than the periphery. General anesthesia affects central thermoregulation by impairing peripheral vasoconstriction and the mechanisms of thermogenesis. After induction, a 1°C decrease occurs within 30 minutes, caused by redistribution,6 as anesthesia causes vasodilatation, which allows the core’s warmer blood to flow freely through the cooler body periphery. As blood circulates, it cools before returning to the heart, thus reducing core temperature. This decline in temperature is known as redistribution temperature drop. Hypothermia is very common during locoregional anesthesia, as this impairs central thermoregulatory control. It has been observed that the combined use of these techniques leads to a piling up of mechanisms that results in more profound hypothermia, especially in elderly people.7
IPH is not only uncomfortable for the surgical patient but may also affect patient outcomes and treatment costs. By affecting drug metabolism, PH is associated with prolonged recovery from anesthesia, including the need to prolong the stay in postanesthesia care unit (recovery room).8 It is also associated with an increased number of morbid cardiac events (MCEs),9 greater intraoperative blood loss,10 thermal discomfort,11 and increased post-operative wound-infection rates.8 Each of these adverse events increases the expenditure of the National Health Service (NHS), and some can affect a patient’s long-term quality of life.
IPH is both common and preventable. Without perioperative warming, the majority of patients will become at least slightly hypothermic (CBT < 36°C). Measuring CBT, maintaining normothermia, and actively warming patients undergoing surgery is crucial for the prevention of IPH and thus to reduce the number of adverse health outcomes associated with IPH. Notwithstanding its importance, temperature monitoring and active patient warming is not currently a standardized clinical practice in Europe. In this context, a survey conducted on 8,083 surgical procedures found that patient temperature was monitored in 19.4% of interventions and 38.5% of patients had actively been warmed, mainly through forced-air systems.12
In consideration of the evidence of positive clinical effects resulting from IPH prevention, many European societies, public authorities, and agencies — following the guidance published by the World Health Organization13,14 — recommend maintaining patient normothermia throughout the whole perioperative period. For our purpose, we referred to the National Institute for Health and Care Excellence (NICE) clinical guideline published in 2008 and updated in 2016,15 a checklist recommended by the Italian NHS,16 and to a specific good clinical practice (GCP) guideline published by the Italian Society of Anesthesia, Analgesia, Reanimation, and Intensive Care (Società Italiana di Anestesia, Analgesia, Rianimazione, e Terapia Intensiva [SIAARTI]) in 2017.17
A reduction in use of health-care resources could be achieved by decreasing the incidence of IPH and thus the incidence of related adverse events. The present study describes a budget impact (BI) model that estimates results of the introduction and diffusion of appropriate protocols aiming to detect this phenomenon and maintain normothermia in the perioperative period in surgical patients. Following the NICE guideline18 and the SIAARTI GCP,17 the protocol includes measurement of CBT, maintaining normothermia, and actively warming patients undergoing surgery. BI analyses estimate changes in the budget-holders’ resource use for populations that are eligible for the protocol, once this is implemented in current practice in the management of surgical patients. Ultimately, the model allows us to address the issue of affordability of systematic implementation of the protocol for the Italian NHS, and thus represents a useful instrument for health-care budget-holders to investigate and predict how maintaining perioperative normothermia may affect expenditure or budgets for health systems.
Methods
A BI analysis was performed to estimate the financial impact of the introduction of a protocol for monitoring and maintaining perioperative normothermia in Italy compared to the current treatment mix adopted in surgical settings. The aim was to compare the total costs of the current scenario (ie, where IPH-prevention protocols are scarcely adopted) and a future scenario (ie, where IPH-prevention protocols are largely adopted). The perspective of the analysis was of a third-party payer, the NHS, and estimates were conducted over a 3-year time horizon. The model was constructed according to the principles of good practice for BI analysis from the International Society for Pharmacoeconomics and Outcomes Research,19 and was developed using Microsoft Excel.
Budget-Impact Model
The BI model was based on the cost-effectiveness analysis of the full NICE guideline on this issue — management of IPH in adults18 — which used a decision-tree model to estimate the impact of various clinical strategies to prevent IPH on the incidence of each adverse health consequence. The economic model was designed to assess the reduction in resource use that can be achieved by lessening IPH and thus decreasing the incidence of complications associated with IPH.18 In the BI model, two of these clinical consequences were considered — MCEs and surgical site infections (SSIs) — that according to a recent Cochrane systematic review1 can be considered most relevant in both clinical and economic terms. In addition, according to the NICE economic model, as mild PH lengthens postoperative recovery and results in unplanned intensive care unit (ICU) patient admission, the expected increase in hospital length of stay (LOS) and postanesthesia care unit length of recovery for hypothermic20 patients has been calculated and compared to the normothermic ones. This information, though not available on Italian databases, was considered applicable to the Italian context according to expert opinion. The BI model provides estimates of the national cost impact arising from implementation of the appropriate perioperative care for normothermia in Italy. These estimates are based on assumptions made on current practice in Italy and hypotheses of how current practice might change following the implementation of the SIAARTI GCP.17 Univariate sensitivity analysis was performed to assess the robustness of the results from the base case.
Assumptions
Baseline risk of hypothermia estimated by the NICE was based on a cohort with average anesthesia duration >60 minutes. At the same time, the baseline risk of hypothermia applied to the analysis was estimated for patients with American Society of Anesthesiologists (ASA) risk grade I under general anesthesia. The probability of a patient experiencing a specific consequence was assumed to be independent of their probability of experiencing a different one, and the hospital LOS impact each of them had was assumed to be the same, regardless of whether the event occurred in a hypothermic or normothermic patient. Finally, the analysis assumed that the LOS attributable to each adverse consequence was additive. The BI model adopted the same assumptions as the economic model constructed by the NICE. These assumptions were considered generalizable to health-care settings of other high-income countries, and were also deemed valid for the Italian context on the basis of SIAARTI experts.
Eligible Population
The SIAARTI GCP17 guideline recommended monitoring and actively warming adult patients undergoing surgery in general or regional anesthesia, or a combination of the two, for longer than 30 minutes. As adult surgical patients are at risk of developing IPH at any stage of the perioperative pathway, monitoring and warming should affect the whole perioperative period (preoperative, intraoperative, and postoperative).Surgical operations lasting >30 minutes performed on adult patients (age>18 years), both under general and locoregional anesthesia, were the target of the BI model. The number of surgical interventions performed on the adult population in a year was not available from institutional sources in Italy. This was thus estimated on the basis of 2016 hospital-discharge data published by the Italian Ministry of Health,21 with reference to the national number of discharges in both ordinary and daytime regimes and grouped according to clinical code aggregates of interventions. This initial estimate was gauged to consider possible interventions not performed as the primary intervention (+10%, based on expert opinion), interventions performed on the pediatric population (−4%),22 and interventions lasting <30 minutes (−15%).23 Total operations carried out in 1 year in Italy was estimated to number about 3.7 million, while the number of target interventions for the present BI model was approximately 3 million (Figure 1).
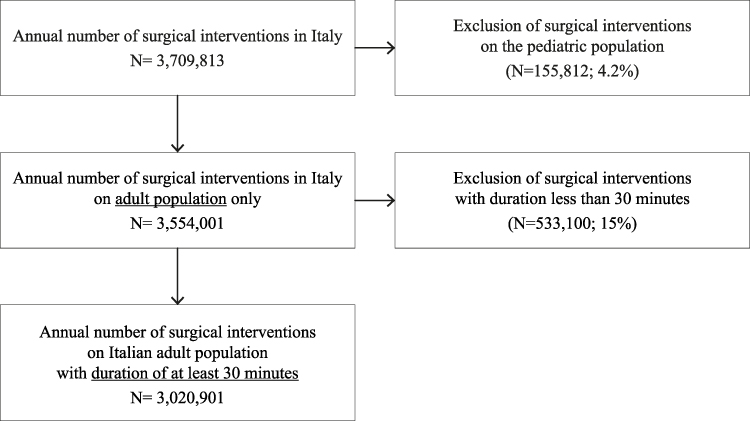 |
Figure 1 Target population. |
Epidemiological Inputs
The BI model considered SSIs and MCEs adverse IPH consequences, both having an impact on hospital LOS for a surgical patient. For each adverse event, the model required inputs of baseline risk in normothermic patients, relative risk (RR) in the hypothermic patient group, and extra LOS associated with postoperative complications. If available, data inputs for Italy were taken from national literature or institutional reports. Otherwise, they were taken from the NICE Guideline.18 All model parameters adopted (Table 1) were validated by expert opinions. Baseline risk for SSIs in Italy were extrapolated from a report of the SSI Surveillance Service published in 2014.22 A total of 355 surgical wards collected data between 2009 and 2011. In sum, 60,460 operations across eleven surgical categories were observed and 1,628 SSIs reported. This corresponds to an incidence of 2.6%, which was applied as the baseline risk of SSIs in normothermic patients.
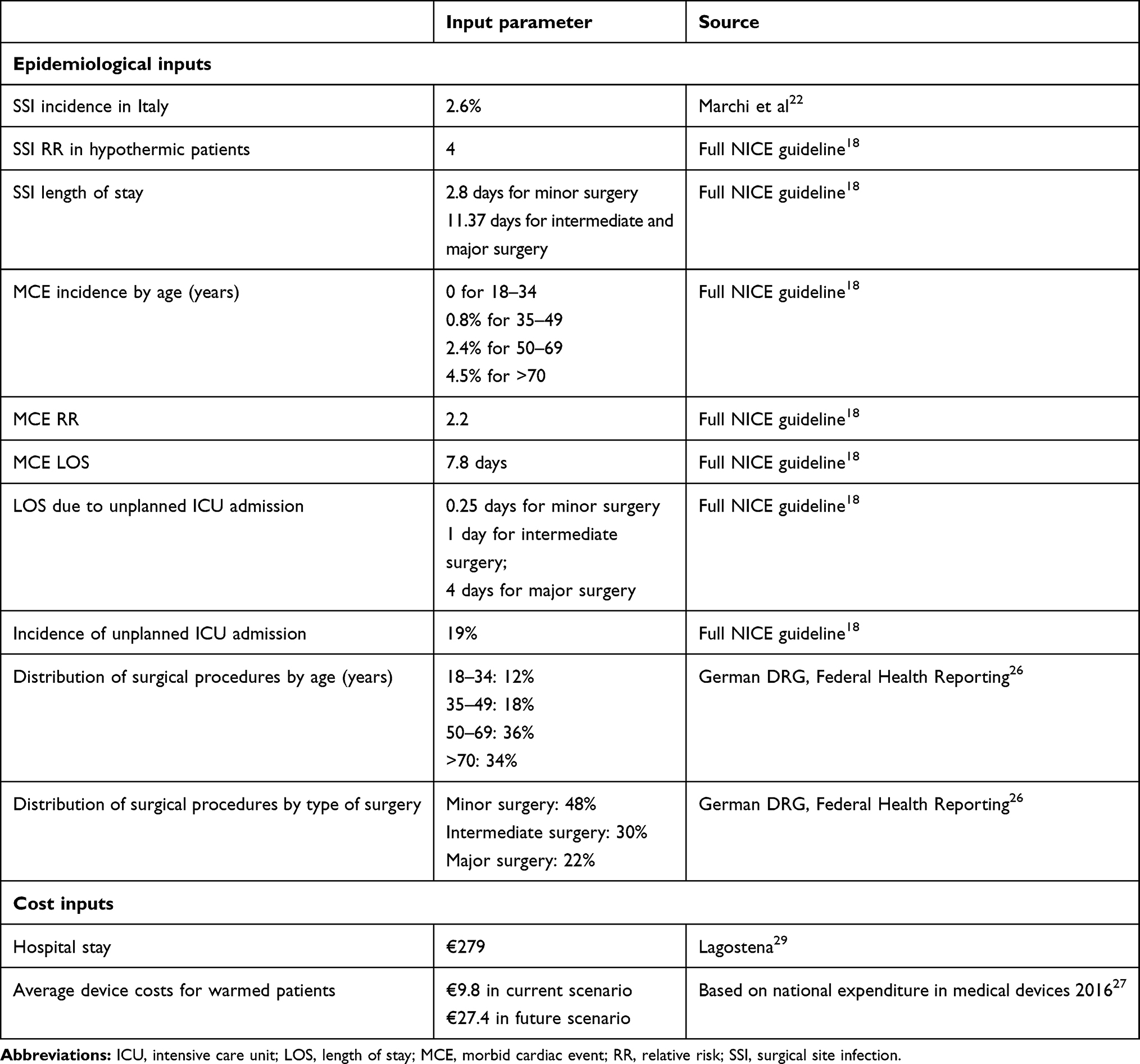 |
Table 1 Epidemiological and cost model input parameters |
As a result of a detailed literature review, the NICE clinical guideline18 found an RR for SSI in the hypothermic patient group of 4 (95% CI 1.6–10.2). The guideline assumed that the average extra LOS in hypothermic patients receiving intermediate and major surgery was equal to the average increased LOS reported by Coello et al24 of 11.37 days. For minor-surgery patients, the NICE group considered the extra LOS for a superficial SSI reported by Coello et al of 2.8 days (95% CI 2.2–3.5).18 Based on the results of a cohort study published in 2001 by Polanczyk et al,25 the NICE guideline identified the baseline risk of MCEs for the normothermic patient group. All risk rates are summarized in Table 1. Hospital-episode statistics referring to the UK were considered to identify the extra LOS in hospitals associated with each type of event: the average extra LOS for an MCE was 7.8 hospital days. The estimated RR of an MCE in the IPH-patient group was 2.2 (95% CI 1.1–4.7).
Mild-hypothermia effects cover a broad range of complications, including bloodloss, increased transfusion rates, and reduced metabolism of most drugs. Consequently, IPH lengthens postoperative recovery and results in unplanned patient ICU admission. As baseline for the duration of hospital stay, the NICE guideline considered 0.25 days for minor surgery, 1 day for intermediate surgery, and 4 days for major surgery, an estimated increase of 19% (95% CI 7%–31%) in total LOS.18 This LOS lengthening was applied to all hypothermic patients in the model.Since there were no Italian data available, the distribution of patients by age and type of surgery from Germany was adopted in the model,26 since the German setting was considered adequately comparable to Italy on the basis of SIAARTI experts involved (Table 1).
Current Scenario
The number of medical devices used in current practice was estimated by analyzing data published on national expenditure on medical devices in 2016 by the Italian Ministry of Health.27 Expenditure attributable to all medical devices generally used in clinical settings to maintain normothermia was considered: xboth active-warming systems that transfer heat to the patient (usually forced-air systems and conductive blankets or mattresses) and passive insulation systems that decrease heat loss, but will not add any benefit in maintenance of perioperative normothermia (usually insulation blankets).28 In addition, expenditure for warming-fluid devices and probes for CBT monitoring was included. The estimated share of patients yearly warmed in Italy reached 32%. The proportion of medical devices for patient warming in the current Italian scenario, estimated from Italian Ministry of Health 2016 data,27 is reported in Figure 2. The incidence estimate of PH in the current scenario was calculated by weighting the incidence of IPH associated with the use of each warming system (or alternatively, no use of device), as reported in the NICE guideline (Chapter 1318 — “Cost-effective analysis”) by the usage share of the same medical devices.
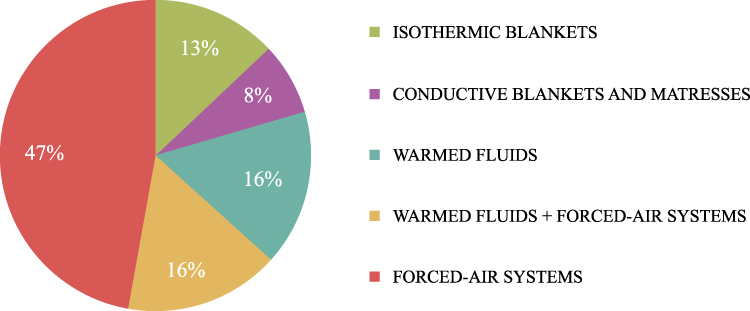 |
Figure 2 Medical devices for patient warming in the current Italian scenario. |
Future Scenario
The GCP guideline published by SIAARTI17 recommends warming patients intraoperatively from induction of anesthesia using a forced-air device when anesthesia lasts >30 minutes or they are at higher risk of IPH, and suggests the use of a resistive heating mattress or blanket if a forced-air warming device is not suitable. Reflecting this recommendation, current practice is expected to change gradually following the implementation of the guideline, and3 years from now, the share of warmed patients should reach 85%. At the same time, with protocol implementation, CBT is systematically measured and patients mainly warmed through forced-air systems. Medical device–usage proportions are 86% forced-air and 14% resistive heating devices. Warmed fluids are suppose to be used for all major surgery interventions and half the intermediate surgery ones. In the first and second year following protocol implementation, the proportion of warmed patients gradually increases to 50% and then to 70%.
Costs
Direct costs of medical devices for monitoring CBT and maintaining normothermia and of hospital stay in surgical ward were considered, as the model focuses on prolongation of hospital LOS for a hypothermic patient. Hospital-stay costs were estimated based on data published in standard hospital cost studies conducted by the Italian Health Network for the sharing of standard costs, indicators, and results of health activities. The available data refer to Galliera Hospital in Genoa29 and show the total average production cost incurred by the hospital for all patients discharged from the General Surgery Department during 2015. The cost was indexed at 2019 money values in accordance with the rate of change in hospital-service prices, as estimated by the corresponding subindex of the Italian price index for the whole society by the National Institute for Statistics,30 and was €279 per patient per day. This included physician, nurse, and other staff costs, drugs, medical devices, and a share of general hospital costs. Costs of lab tests, X-rays, surgical procedures, and operating room were not considered in this cost of hospital–stay assessment. Average medical device costs were estimated as the weighted average of prices of tenders assigned in Italy in 2016, inflated to 2019 prices, and weighted by the corresponding volumes purchased. The assessed average cost for medical devices considered in the current scenario was €9.8, referring to the 32% share of interventions with patient warming. In the future scenario, the average cost for medical devices in implementation of the protocol on 85% of interventions increased to €27.4. This cost included probes for monitoring CBT and active-warming systems, as previously indicated.
Results
Starting from the target population (Figure 1), the model assessed resource and BI associated with diffusion of the protocol for preventing IPH, calculated as the difference in population-resource use and costs, respectively, between current and future scenarios. In the future scenario the number of patients undergoing surgery with application of the protocol increased from 966,000 in the current scenario to 2.5 million (Table 2). Implementing the protocol resulted in additional costs due to increased use of forced-air warming systems and inductive-heating mattresses and blankets. From the combination of raised number of warmed patients and exclusive use of active-warming systems, medical device expenditure increased €60.89 million (from €9.5 million in the current scenario to €70.3 in the future one). The model estimated consistent benefits and savings from this protocol’s implementation: fewer patients becoming hypothermic during surgery, and consequently a substantial reduction in costs arising from the management of adverse events caused by IPH. Combining the results of increased LOS for a hypothermic patient with the amount of hypothermic patients for the number of national procedures per year, the model estimated a total of 436,000 full days of hospital stay due to IPH could be prevented. This result impacted in reduction of costs by almost €121.8 million and simultaneously increasing the quality of life of patients who avoided the consequences of IPH. As shown in Figure 3, the overall BI on the NHS arising from increased expenditure for combined medical devices and lower costs due to a decrease in IPH incidence was estimated at net savings of almost €60.92 million in the third year of protocol implementation.
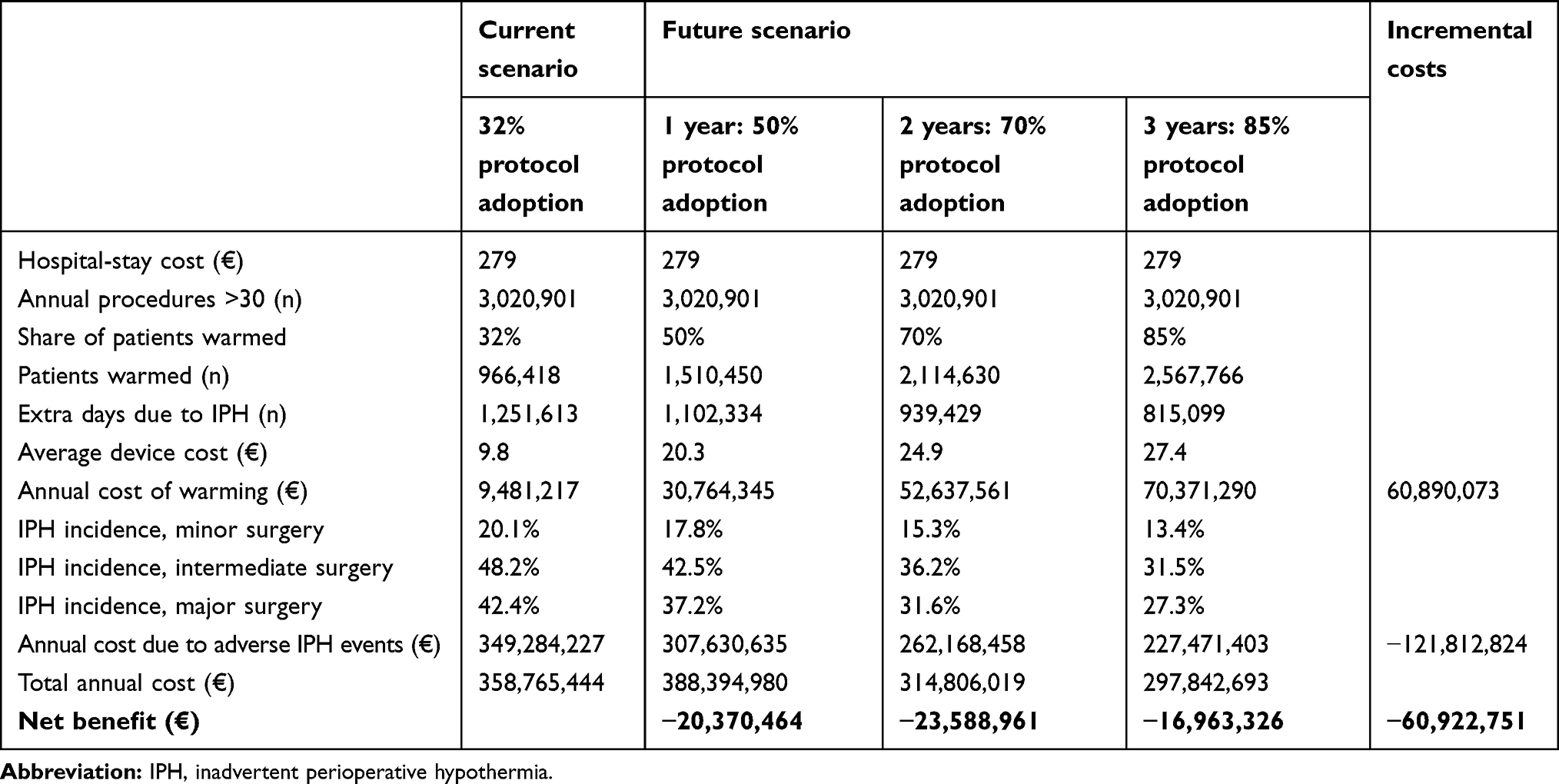 |
Table 2 Budget Impact Model Results |
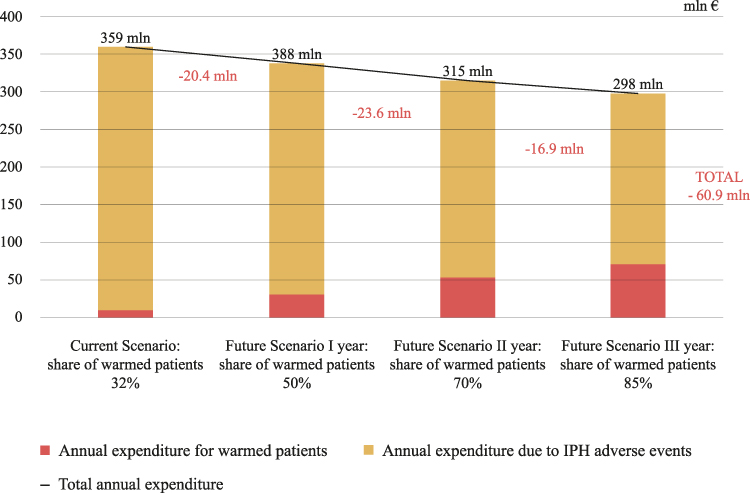 |
Figure 3 Estimated annual total and incremental budget impact for each year of the time frame for warming patients intraoperatively in Italy. |
Sensitivity Analysis
One-way sensitivity analyses were performed by changing base-case parameters of the model, and shown in a tornado diagram (Figure 4). A range of variability equal to 20% of the central value was considered, assuming this as a reasonably wide range, for the reference population. Cost of medical devices in current and future scenarios and cost of hospital stay in surgical wards varied within ±20%. Incidence of accidental hypothermia range was ±20%. The results of the sensitivity analysis showed that all input variables reacted to changes in net benefit directly (Figure 4), with the exception of device costs in the future scenario and incidence of IPH, for which a cost increment was associated with a decrease in potential savings. Other conditions being equal, the analysis showed a greater sensitivity of net benefit to cost of hospitalization and incidence of IPH (the variation was more than proportional).
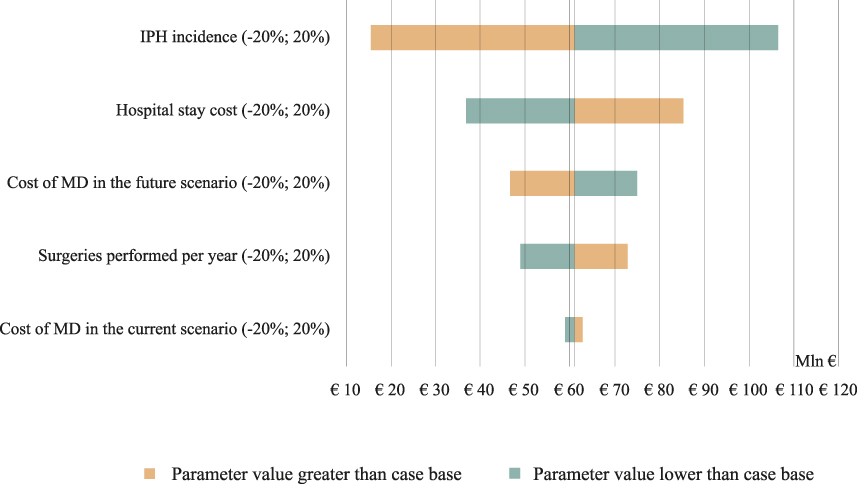 |
Figure 4 Tornado diagram for sensitivity analyses. Central value: base-case budget-impact savings of €60.9 million. |
Discussion
This study provides estimates of the impact on national cost of the implementation of the SIAARTI GCP guidance on preventing IPH in Italy. The present BI model found relevant savings for the Italian NHS. To our knowledge, this is the first evidence in an Italian context, and to date, few similar studies on the estimation of cost reductions due to effectiveness of thermal care–bundle implementation in preventing IPH have been published.31,32 A recent Australian pharmacoeconomic study estimated important savings in IPH prevention to the health system consistent to our results.32
Several original items were computed in the present analysis, eg, estimated number of surgical interventions performed in Italy each year — an information not immediately available from public data — and an estimate of usage share of medical devices for normothermia maintenance in surgical settings in Italy. These data on the real-life utilization of medical devices, based on the institutional database,27 allowed us to perform a realistic assessment of current practice in the present scenario and could be useful to health-care budget-holders to understand the impact of protocol implementation on their budget, on the population’s healt,h and on health-care resources during the same period.
Our BI analyses found that protocol implementation for preventing IPH in surgery settings in Italy caused important additional costs, due to the increased number of patients needing warming devices (from 32% of patients undergoing surgery in the current scenario to 85% in the future scenario) and to a change in the mix of medical devices for patient warming to be adopted in future scenarios. In fact, in the future scenario the adoption of a consistent increment in proportion of the most efficacious medical devices in preventing IPH (ie, the active-warming systems) was expected, as recommended by the SIAARTI GCP guidance.17 These, however, are generally more expensive than passive devices. The BI model estimated an important increase in cost for medical devices (an increment of more than sevenfold the total cost in the current scenario), but at the same time, this model estimated crucial savings for the Italian NHS. In fact, by implementing the IPH-prevention protocol in the future scenario, the model estimated a considerable reduction in costs from adverse events caused by hypothermia, given the smaller number of patients expected to become hypothermic during surgery. LOS was estimated to decrease by 35% (from 1.25 million in the current scenario to 815,000 in the future one), with saved resources amounting to almost €122 million. Finally, the BI model estimated a net benefit of IPH prevention to the Italian NHS of €60.62 million. This result highlights that protocol implementation not only guarantees an improvement in clinical patient care and consequently in quality of life of patients after surgery, but it is also a sustainable strategy for NHS savings. Sensitivity analyses showed that model conclusions were robust with respect to the variability of input parameters, and cost reductions emerged in all cases considered. Preventing IPH-protocol implementation is crucial to reduce SSIs, ie, the most common health care–associated infections,33–35 and their incidence reduction should be a main goal for health-care budget-holders (also to fight increasing antibiotic resistance). This would also lead to an improvement in hospital-productivity indices, such as bed- rotation index or number of hospital discharges.
This study has some limitations. Hypothermia-risk assumptions were based on a cohort with a mean duration of anesthesia >60 minutes, and this may have led to overestimation of risk of hypothermia receivwith shorter procedures. Also, the baseline risk of hypothermia estimated for patients with ASA risk grade I treated under general anesthesia may have underestimated the risk in patients with higher ASA risk grades or those having combined regional and general anesthesia. Model implementation considered epidemiological inputs not strictly referring to the Italian population, due to a lack of national data. However, data from other high-income European Union countries were considered adequate for the Italian clinical context by expert opinion. In the model, only two adverse events associated with IPH were considered (ie, MCEs and SSIs), since according to recent evidence these complications can be considered the most relevant in both clinical and economic terms.1 Moreover, we assumed that patients were warmed intraoperatively only, despite the NICE guideline18 recommending warming patients throughout the entire perioperative pathway. Including other consequences due to IPH and considering prewarming in the BI model would probably increase the estimation of net savings for the NHS in the future scenario.
The present BI model considered direct health costs only. Moreover, the LOS costs considered in the present model are an underestimate of the real ones, in consideration of possible extra costs due to return to operating rooms, additional lab tests, or diagnostic tests due to complications. On the other hand, the adoption of new active-warming systems may impact on total cost of health-care personnel, due to training time and additional energy consumption associated with increasing use of warming systems. None of these costs was considered, due to the absence of specific data.
Conclusion
Based on BI analysis, the introduction and implementation of perioperative normothermia best care, as recommended by international guidelines and the SIAARTI GCP guideline, would result in both clinical and economic advantages for the Italian NHS. The model estimated relevant savings for hospitals. It is thus advantageous from the economic and clinical point of view for the SIAARTI GCP guidelineon perioperative normothermia to be widely adopted in Italian hospitals. In consideration of our favorable findings, further studies from other European countries are awaited.
Acknowledgments
We thank Dr Emiliano Tizi and all SIAARTI for scientific support, Dr Laura Benedan for editorial assistance, and Dr Maddalena Iannantuoni for graphical support. This research did not receive any grants from funding agencies in the public, commercial, or not-for-profit sector.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Madrid E, Urrútia G, Roqué I Figuls M, et al. Active body surface warming systems for preventing complications caused by inadvertent perioperative hypothermia in adults. Cochrane Database Syst Rev. 2016;4:CD009016. doi:10.1002/14651858.CD009016.pub2
2. Ruetzler K, Kurz A. Consequences of perioperative hypothermia. Handb Clin Neurol. 2018;157:687–697. doi:10.1016/B978-0-444-64074-1.00041-0
3. Alfonsi P, Bekka S, Aegerter P, Farag E; SFAR Research Network investigators. Prevalence of hypothermia on admission to recovery room remains high despite a large use of forced-air warming devices: findings of a non-randomized observational multicenter and pragmatic study on perioperative hypothermia prevalence in France. PLoS One. 2019;14(12):e0226038. doi:10.1371/journal.pone.0226038
4. Bindu B, Bindra A, Rath G. Temperature management under general anesthesia: compulsion or option. J Anaesthesiol Clin Pharmacol. 2017;33(3):306–316. doi:10.4103/joacp.JOACP_334_16
5. Mahoney CB, Odom J. Maintaining intraoperative normothermia: a meta-analysis of outcomes with costs. AANA J. 1999;67(2):155–163.
6. Sun Z, Honar H, Sessler DI, et al. Intraoperative core temperature patterns, transfusion requirement, and hospital duration in patients warmed with forced air. Anesthesiology. 2015;122(2):276–285. doi:10.1097/ALN.0000000000000551
7. Leslie K, Sessler DI, Bjorksten AR, Moayeri A. Mild hypothermia alters propofol pharmacokinetics and increases the duration of action of atracurium. Anesth Analg. 1995;80(5):1007–1014. doi:10.1097/00000539-199505000-00027
8. Lenhardt R, Marker E, Goll V, et al. Mild intraoperative hypothermia prolongs postanesthetic recovery. Anesthesiology. 1997;87(6):1318–1323. doi:10.1097/00000542-199712000-00009
9. Frank SM, Fleisher LA, Breslow MJ, et al. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events: a randomized clinical trial. JAMA. 1997;277(14):1127–1134. doi:10.1001/jama.1997.03540380041029
10. Rajagopalan S, Mascha E, Na J, Sessler DI. The effects of mild perioperative hypothermia on blood loss and transfusion requirement. Anesthesiology. 2008;108(1):71–77. doi:10.1097/01.anes.0000296719.73450.52
11. Kurz A, Sessler DI, Lenhardt R. Perioperative normothermia to reduce the incidence of surgical-wound infection and shorten hospitalization. Study of Wound Infection and Temperature Group. N Engl J Med. 1996;334(19):1209–1215. doi:10.1056/NEJM199605093-341901
12. Torossian A. Survey on intraoperative temperature management in Europe. Eur J Anaesthesiol. 2007;24(8):668–675. doi:10.1017/S0265021507000191
13. World Health Organization. Global guidelines for the prevention of surgical site infection; 2016. Available from: https://apps.who.int/iris/bitstream/handle/10665/250680/9789241549882-eng.pdf?sequence=8.
14. Allegranzi B, Zayed B, Bischoff P, et al. New WHO recommendations on intraoperative and postoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis. 2016;16(12):e288–e303. doi:10.1016/S1473-3099(16)30402-9
15. National Institute for Health and Care Excellence. Hypothermia. Prevention and management in adults having surgery (CG65) clinical guideline. 23 April 2008. Last updated December 2016. Available from: http://nice.Org.Uk/guidance/cg65.
16. Italian Ministry of Health. Operating room safety manual: recommendations and checklist; 2009. Available from: http://www.salute.gov.it/imgs/C_17_pubblicazioni_1119_allegato.pdf.
17. Di Marco P, Canneti A Normotermia perioperatoria. Buone pratiche cliniche SIAARTI; 2017. Available from: http://www.siaarti.it/SiteAssets/Ricerca/buone-pratiche-cliniche-siaarti-normotermia-perioperatoria/Buone%20Pratiche%20Cliniche%20SIAARTI%20-%20Normotermia%20perioperatoria.pdf.
18. National Institute for Health and Care Excellence. The management of inadvertent perioperative hypothermia in adults. April 2008. Full guideline Last updated December 2016. Available from: https://www.nice.org.uk/guidance/cg65/evidence/full-guideline-pdf-196802751.
19. Sullivan SD, Mauskof JA, Augustovski F, et al. Budget impact analysis principles of good practice: report of the ISPOR 2012 budget impact analysis good practice II task force. Value Health. 2014;17(1):5–14. doi:10.1016/j.jval.2013.08.2291
20. Casati A, Fanelli G, Ricci A, et al. Shortening the discharging time after total hip replacement under combined spinal/epidural anesthesia by actively warming the patient during surgery. Minerva Anestesiol. 1999;65:507–514.
21. [dataset] Italian ministry of health hospital discharge report sdo tables; 2016. Available from: http://www.salute.gov.it/portale/documentazione/p6_2_8_3_1.jsp?lingua=italiano&id=28.
22. Marchi M, Pan A, Gagliotti C, et al. The Italian national surgical site infection surveillance programme and its positive impact, 2009 to 2011. Eur Surveill. 2014;19(21):20815. doi:10.2807/1560-7917.ES2014.19.21.20815
23. Buttazzi R, Ricciardi A, Gagliotti C, Moro ML Surgical site infection surveillance in Italy. Orthopedic interventions 2014. Non Orthopedic interventions 2015. Regional health and social agency of Emilia-Romagna Published December 2016 Available from: https://assr.regione.emilia-romagna.it/pubblicazioni/rapporti-documenti/report_snich_2014-2015.
24. Coello R, Charlett A, Wilson J, Ward V, Pearson A, Borriello P. Adverse impact of surgical site infections in English hospitals. J Hosp Infect. 2005;60(2):93–103. doi:10.1016/j.jhin.2004.10.019
25. Polanczyk CA, Marcantonio E, Goldman L, et al. Impact of age on perioperative complications and length of stay in patients undergoing noncardiac surgery. Ann Intern Med. 2001;134(8):637–643. doi:10.7326/0003-4819-134-8-200104170-00008
26. Federal health reporting service (GBE). Available from: http://www.gbe-bund.de/gbe10/trecherche.prc_them_rech?tk=14501&tk2=18651&p_uid=gast&p_aid=60121836&p_sprache=E&cnt_ut=1&ut=18651.
27. [dataset] Italian Ministry of Health National expences in medical devices 2016 – appendix; 2017. Available from: http://www.dati.salute.gov.it/dati/dettaglioDataset.jsp?menu=dati&idPag=91.
28. Sessler DI. Perioperative thermoregulation and heat balance. Lancet. 2016;387(10038):2655–2664. doi:10.1016/S0140-6736(15)00981-2
29. Lagostena A, L’esperienza Della SC. Chirurgia generale ed Epatobiliopancreatica. In Convegno: la sostenibilità dei sistemi sanitari, Ospedale di Bolzano, 1 giugno 2016. Available from: http://www.sabes.it/it/archivio-news.asp?aktuelles_action=300&aktuelles_image_id=848844.
30. [dataset] National Istitute of Statistics: I.Stat Nic – annual average from 2016 onwards (base 2015). Available from: http://dati.istat.it/.
31. National Institute for Health and Care Excellence. Resource impact report: hypothermia: prevention and management in people having surgery (CG65). Available from: https://www.nice.org.uk/guidance/cg65/resources/resource-impact-report-pdf-2731292749.
32. Ralph N, Gow J, Conway A, et al. Costs of inadvertent perioperative hypothermia in Australia: a cost-of-illness study. Collegian. 2020;27(4):345–351. doi:10.1016/j.colegn.2019.10.003
33. European Centre for Disease Prevention and Control. Annual epidemiological report 2016 – surgical site infections. Stockholm: ECDC. Available from: https://ecdc.europa.eu/sites/portal/files/documents/AER-HCAI-SSI.pdf.
34. European Centre for Disease Prevention and Control. Point prevalence survey of healthcare-associated infections and antimicrobial use in European acute care hospitals. Stockholm: ECDC; 2013. Available from: http://ecdc.europa.eu/en/publications/Publications/healthcare-associated-infections-antimicrobial-usePPS.pdf.
35. Suetens C, Latour K, Kärki T, et al. Prevalence of healthcare-associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: results from two European point prevalence surveys, 2016 to 2017. Eurosurveillance. 2018;23:1800516. doi:10.2807/1560-7917.ES.2018.23.46.1800516
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.