")
Back to Journals » Infection and Drug Resistance » Volume 13
Increased Antimicrobial Resistance among Sputum Pathogens from Patients with Hyperglycemia
Authors Yi H , Huang J , Guo L, Zhang Q, Qu J, Zhou M
Received 25 December 2019
Accepted for publication 23 April 2020
Published 11 June 2020 Volume 2020:13 Pages 1723—1733
DOI https://doi.org/10.2147/IDR.S243732
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Huahua Yi,1,2,* Jingwen Huang,1,2,* Lingxi Guo,1,2 Qiurui Zhang,1,2 Jieming Qu,1,2 Min Zhou1,2
1Department of Respiratory and Critical Care Medicine, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2Institute of Respiratory Diseases, Shanghai Jiaotong University School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Min Zhou; Jieming Qu
Department of Respiratory and Critical Care Medicine, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, 197 Ruijin Er Road, Shanghai 200025, People’s Republic of China
Email [email protected]; [email protected]
Background: Glucose management is of great significance. Infection and hyperglycemia are a vicious circle. This study was conducted to describe distribution and antimicrobial resistance of bacteria isolated from patients with normoglycemia, hyperglycemia, or diabetes on admission.
Methods: A retrospective study was conducted in a teaching hospital from January 2015 to March 2017. Bacteria were identified by the Vitek 2 automated system and antimicrobial susceptibility determined.
Results: A total of 1,163 patients were included: 582 with normoglycemia, 292 with hyperglycemia and 289 with diabetes. Enterobacter, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterococcus faecium were the main species isolated from these patients, with 1,616 unduplicated isolates from sputum samples. Patients with hyperglycemia were more prone to carry more than one species, and the rate of multidrug-resistant K. pneumoniae and methicillin-resistant S. aureus was higher in this group. K. pneumoniae from hyperglycemia patients demonstrated increased resistance to carbapenems, especially imipenem (p=0.002) and meropenem (p=0.003), than those isolated from patients with normoglycemia or diabetes. No significance was detected for K. pneumoniae, A. baumannii, or P. aeruginosa between nondiabetes and diabetes patients. In addition, hyperglycemia patients had a higher rate of ICU admission (p= 0.035) and a lower survival rate (p< 0.001).
Conclusion: Patients with hyperglycemia were more prone to carry bacteria, especially multidrug-resistant K. pneumoniae and methicillin-resistant S. aureus. Assessing glucose on admission is of great significance in predicting bacterial carriage and antimicrobial resistance.
Keywords: antimicrobial resistance, K. pneumoniae, S. aureus, hyperglycemia, diabetes
Introduction
The prevalence of diabetes is increasing and becoming the leading cause of morbidity and mortality among noncommunicable diseases worldwide.1,2 In China, the prevalence of diabetes is 11.6% and for prediabetes 50.1% among adults.3 It has been accepted that diabetes is an attributable risk factor of ischemic heart disease and stroke, which killed 12.9 million people worldwide in 2010.4 Not only considered a major risk factor of noncommunicable diseases, diabetes was also a risk factor of infections and worsening outcomes of infectious diseases,5,6 as indicated in community-acquired pneumonia.5 Length of hospital stay and mortality increase among diabetics, particularly among those with poor glycemic control, compared with nondiabetics.6 Glucose management is of great importance in clinical practice.7 Hyperglycemia on admission hinders outcomes of hospitalized patients and increases the risk of mortality.6,7
Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter spp. are the leading pathogens in hospital infections.8 Bacterial resistance to antibiotics has become an urgent global threat, especially the emergence of multidrug resistance, extensive drug resistance, and even pandrug resistance.9 The emergence of antimicrobial resistance (AMR) put the public into panic, because currently available antibiotics may not be effective in treating infections caused by these microorganisms.10 Morbidity, mortality, and length of hospital stay attributable to AMR reported are increasing.11,12 Compared to infection caused by antibiotic-susceptible organisms, higher medical expense and length of stay are also attributable to antibiotic resistance.12,13 Microorganisms resistant to antibiotics are now a considerable challenge for the global health-care system.14
However, opinions from previous studies on whether diabetes increases the risk of AMR among hospitalized patients are divergent.14,15 Tian et al14 found a higher rate of AMR among diabetes patients who had been diagnosed with liver abscess, while another study demonstrated that the rate of carbapenem-resistant K. pneumoniae was lower among diabetes than nondiabetes patients.15 However, little is known about resistance rates of bacteria isolated from patients with normoglycemia or hyperglycemia on admission. Herein, we conducted a retrospective study with the aim of describing the distribution of bacteria from patients with normoglycemia, hyperglycemia, or diabetes and assessing the antimicrobial susceptibility of bacteria isolated from sputum, thus adding direct evidence to this field.
Methods
Study Design
A retrospective study was conducted among adult Han Chinese patients hospitalized in Ruijin Hospital, a tertiary hospital in Shanghai, China. All patients had positive results on sputum bacteria identification from January 2015 to March 2017. Information on pathogens isolated from sputum and pathogens from other samples, such as blood and pus, was collected. Duplicated isolates from nonsterile body fluid from the same patient were excluded. Clinical information, including demographic data and clinical microbiology results, was collected by searching medical records. Written informed consent was obtained from the patients or first-degree relatives. The study was approved by the Ruijin Hospital Ethics Committee, Shanghai Jiao Tong University School of Medicine.
Data Collection
All information for patients included was searched through charts. Lung diseases referred to chronic pulmonary lung disease, pulmonary bronchitis, and bronchiectasis. Cardiovascular diseases were a history of brain infraction, myocardial infarction, or other ischemic heart and brain diseases. Diabetes diagnosis were fasting plasma glucose ≥7 mmol/L, 2-hour plasma glucose ≥11.1 mmol/L during an oral glucose-tolerance test (OGTT), random plasma glucose ≥11.1 mmol/L with classic symptoms of hyperglycemia, or HbA1c ≥6.5%.16 Patients included were divided into two groups according to history of diabetes, and those without diabetes were then subdivided into two groups: normal (fasting plasma glucose<6.1 mmol/L or 2-hour plasma glucose <7.8 mmol/L on OGTT without diagnosed diabetes) or increased glucose (fasting plasma glucose ≥6.1 mmol/L or 2-hour plasma glucose ≥7.8mmol/L on OGTT without diabetes history) on admission. Plasma glucose was tested with an automated system (Advia 1650; Bayer) using the glucose oxidase method.
Isolate Identification and Antimicrobial-Susceptibility Testing
All isolates were identified by matrix-assisted laser desorption ionization time-of-flight mass spectrometry (BioMérieux, Marcy-l’Étoile, France). Antimicrobial-susceptibility testing was determined with Kirby–Bauer disk diffusion and E-tests according to Clinical and Laboratory Standards Institute criteria. Extended-spectrum β-lactamase (ESBL) production was identified by clavulanic acid synergy. Escherichia coli ATCC 25922, P. aeruginosa ATCC 27853, S. aureus ATCC 29213, Staphylococcus pneumoniae ATCC 49619, Enterococcus faecalis ATCC 29212, and Haemophilus influenzae ATCC 49247 were used for quality control.
Statistical Analysis
All statistical analysis was conducted with SAS 9.4 (SAS Institute, USA). Data are described as medians (IQR) for continuous variables and number (percentage) for categorical variables. ANOVA was conducted for continuous variables when calculations were normally distributed and equal in variance analysis, and if not, then changed to nonparametric statistics. Fisher’s exact test or χ2 was used for categorical variables. Comparison was made between diabetes and nondiabetes patients or patients with normoglycemia or hyperglycemia on admission. Two-tailed p<0.05 was considered statistically significant.
Results
Demographic Features
A total of 1,163 patients were included: 582 with normoglycemia, 292 with hyperglycemia, and 289 with diabetes. There were 178 females in the normoglycemia group (30.6%), 83 in the hyperglycemia group (28.4%) and 100 in the diabetes group (34.6%), and no significance was detected by sex in the three groups. As demonstrated in Table 1, patients with diabetes were older than those normal or with hyperglycemia (68, IQR 60–78; 66, IQR 54.5–77; and 65, IQR 55–76, respectively). Average BMI was 22 (IQR 19.4–24.2) kg/m2 in the normoglycemia group, 23.2 (IQR 20.2–25.7) kg/m2 in the hyperglycemia group, and 24 (IQR 21.2–26.8) kg/m2 in diabetics, 33.9% of normoglycemia patients had hypertension, while this was 40.1% among the hyperglycemia patients and 58.5% among the diabetics. For cardiovascular diseases, it was 18.9% for patients with normoglycemia, 19.5% for those with hyperglycemia, and 36.0% for diabetes. No significance was detected for smoking, glucocorticoid usage, prior hospitalization, or antibiotic exposure among the three groups.
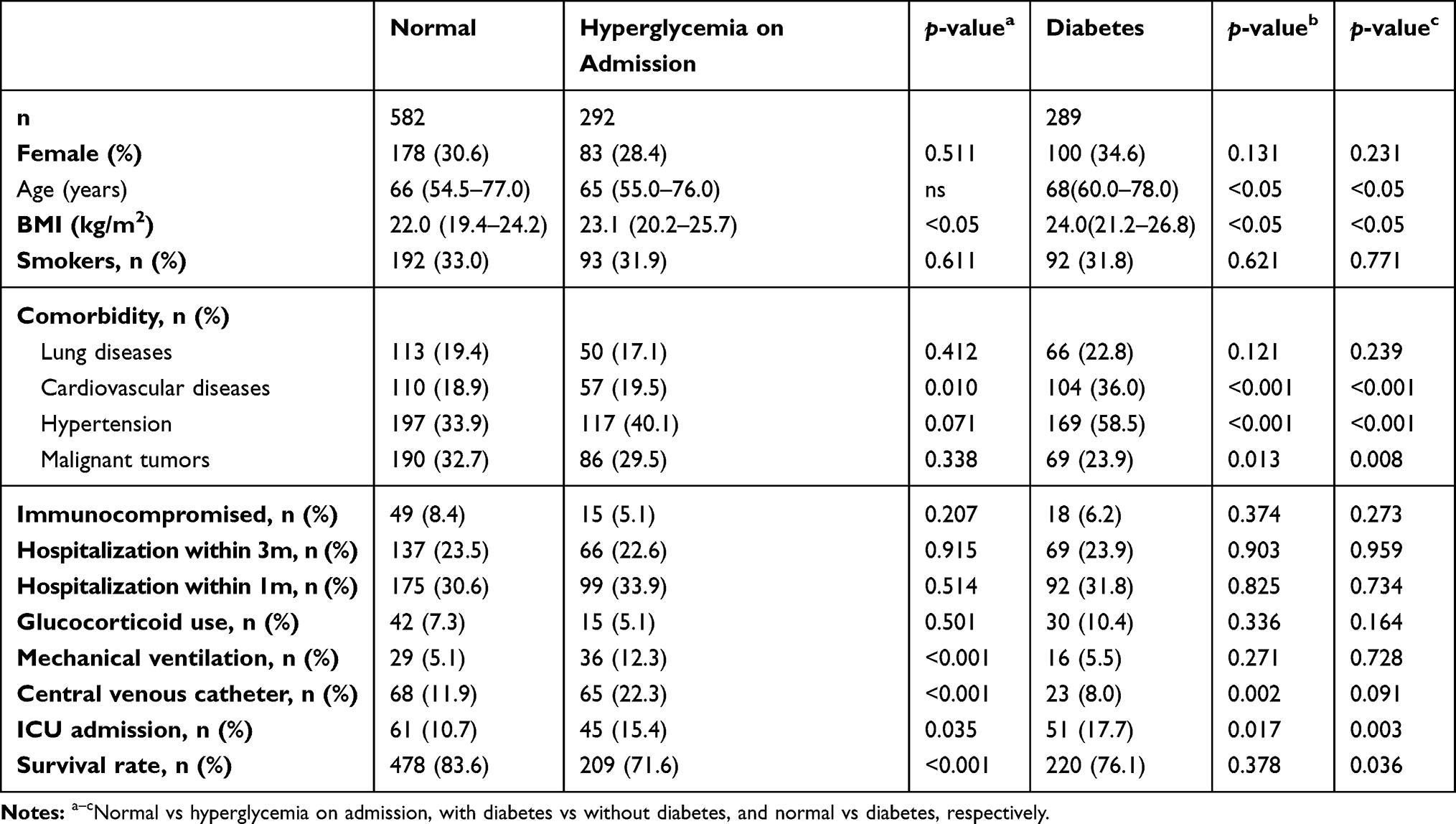 |
Table 1 Demographics of Patients among the three groups |
In terms of treatment and prognosis, incubation of a central venous catheter was more commonly detected in patients with hyperglycemia than those with normoglycemia or diabetes (22.3% vs 11.9% vs 8.0%), and patients with hyperglycemia had a higher rate of mechanical ventilation than those with normoglycemia or diabetics. For further investigation, ICU admission and survival rate were also analyzed. We found that ICU admission was much more prevalent in diabetics than patients with hyperglycemia or normoglycemia (17.7% vs 15.4% vs 10.7%), and the lowest survival rate was seen among patients with hyperglycemia on admission (71.6%).
Bacterial Distribution
A total of 2,167 pathogens were isolated from the patients: 1,616 nonduplicate bacteria identified from sputum samples and 551 bacteria from nonsputum samples (Table 2). For sputum and nonsputum samples, Gram-negative bacilli were the commonest pathogens isolated, comprising Enterobacteriaceae, A. baumannii, and P. aeruginosa, while S. aureus had the greatest proportion among Gram-positive cocci. The highest detection rate for Enterobacteriaceae (39.3%) was in diabetics, while the highest proportion for A. baumannii (21.6%) and S. aureus (25.5%) was found in patients with hyperglycemia, though no significance was detected for the last two species between patients with or without diabetes. In addition, K. pneumoniae was the dominant pathogen among Enterobacteriaceae for all three groups. In terms of the number of bacteria isolated from each patient, we found that 74.6% of patients with increased glucose tended to carry more than one isolate, followed by diabetes patients (68.3%).
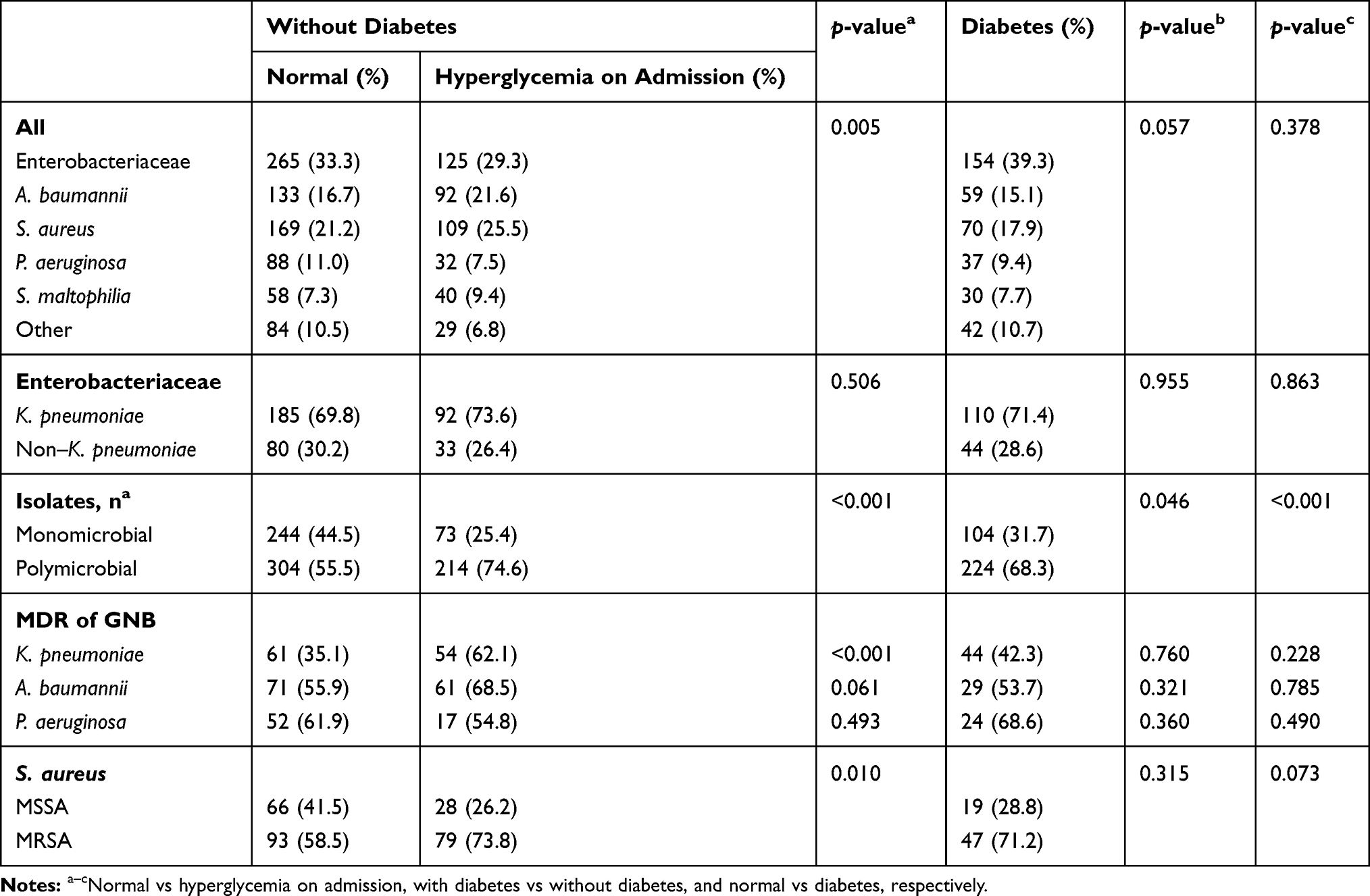 |
Table 2 Isolate Distribution Among the Three Groups |
For antimicrobial-susceptibility testing, the rate of multidrug-resistant K. pneumoniae (MDR-KP) was highest among those with hyperglycemia on admission and higher than the normal glucose group (62.1% vs 35.1%, p<0.001). Percentages for MDR A. baumannii (MDR- AB) and MDR P. aeruginosa (MDR-PA) were quite high among all patients, regardless of glucose level on admission or diabetes status, though no statistical significance was demonstrated for MDR-AB or MDR-PA among the three groups. Similarly to the trend for MDR-KP, methicillin-resistant S. aureus (MRSA) had the highest proportion among patients with hyperglycemia (73.8%), followed by diabetics (71.2%).
Antimicrobial Susceptibility of Bacteria from Sputum
K. pneumoniae, S. aureus, A. baumannii, and P. aeruginosa were the commonest bacteria isolated in the present study, and antimicrobial-susceptibility results for these species isolated from sputum are described in detail. As shown in Table 2, K. pneumoniae was the commonest pathogen detected among Enterobacteriaceae. We conducted further research on the susceptibility of K. pneumoniae from sputum samples to obtain deeper insight, as depicted in Table 3 and 20% of K. pneumoniae was found to produce ESBL. Compared to K. pneumoniae from patients with normal glucose, resistance to cephems, monobactams, quinolones, aminoglycosides, and carbapenems of K. pneumoniae from patients with hyperglycemia on admission was increased. 35.6% of K. pneumoniae from patients with increased glucose was resistant to imipenem and 35.9% not susceptible to meropenem, both significantly higher than those with normal glucose (p=0.002 and p=0.003, respectively). The overall rate of K. pneumoniae resistance to ertapenem was higher than for meropenem and imipenem, though no statistical significance was reached among the three groups. For tigecycline, the last available treatment for carbapenem-resistant K. pneumoniae, no significance was detected between patients with or without diabetes and patients with normal or increased glucose. The resistance rate of K. pneumoniae from patients with increased glucose was 5.8%, not significantly higher than any other patients. In terms of the resistance rate of all agents tested, no statistical significance was demonstrated among patients with different glucose metabolism status.
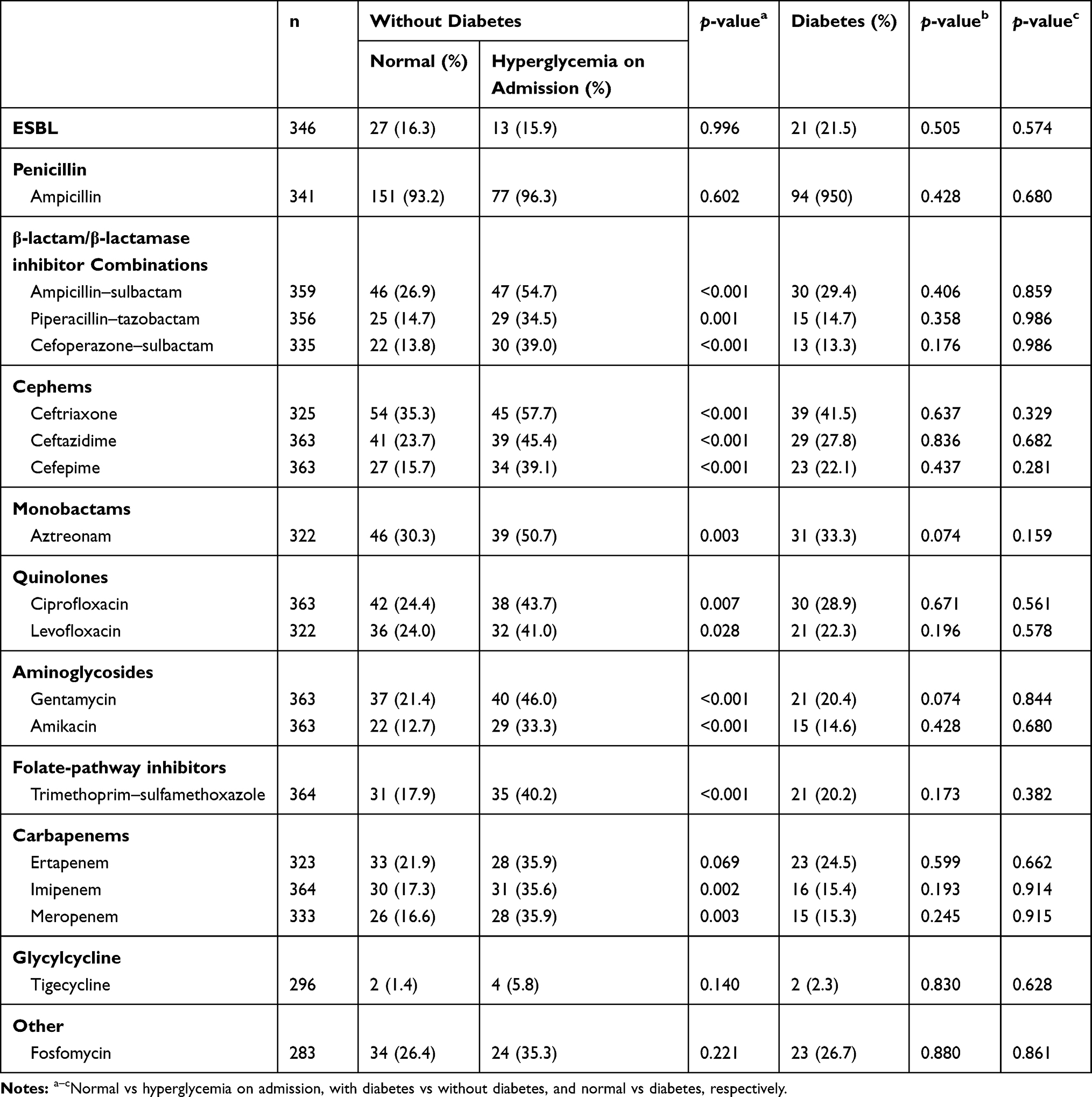 |
Table 3 Antibiotic-Resistance Rate of K. pneumoniae Isolated from Sputum |
A. baumannii was the second commonest pathogen in the current study, and the resistance rate was generally high for these isolates (Table 4). For antimicrobial agents tested except levofloxacin, tigecycline, and aminoglycosides, the highest resistance level was seen among patients with hyperglycemia on admission, followed by patients with normal glucose and without diabetes, while A. baumannii isolates from diabetes patients showed the lowest resistance rate (Table 4). A. baumannii isolated from patients with diabetes showed statistically lower resistance to ampicillin–sulbactam than those from nondiabetics (p=0.010).
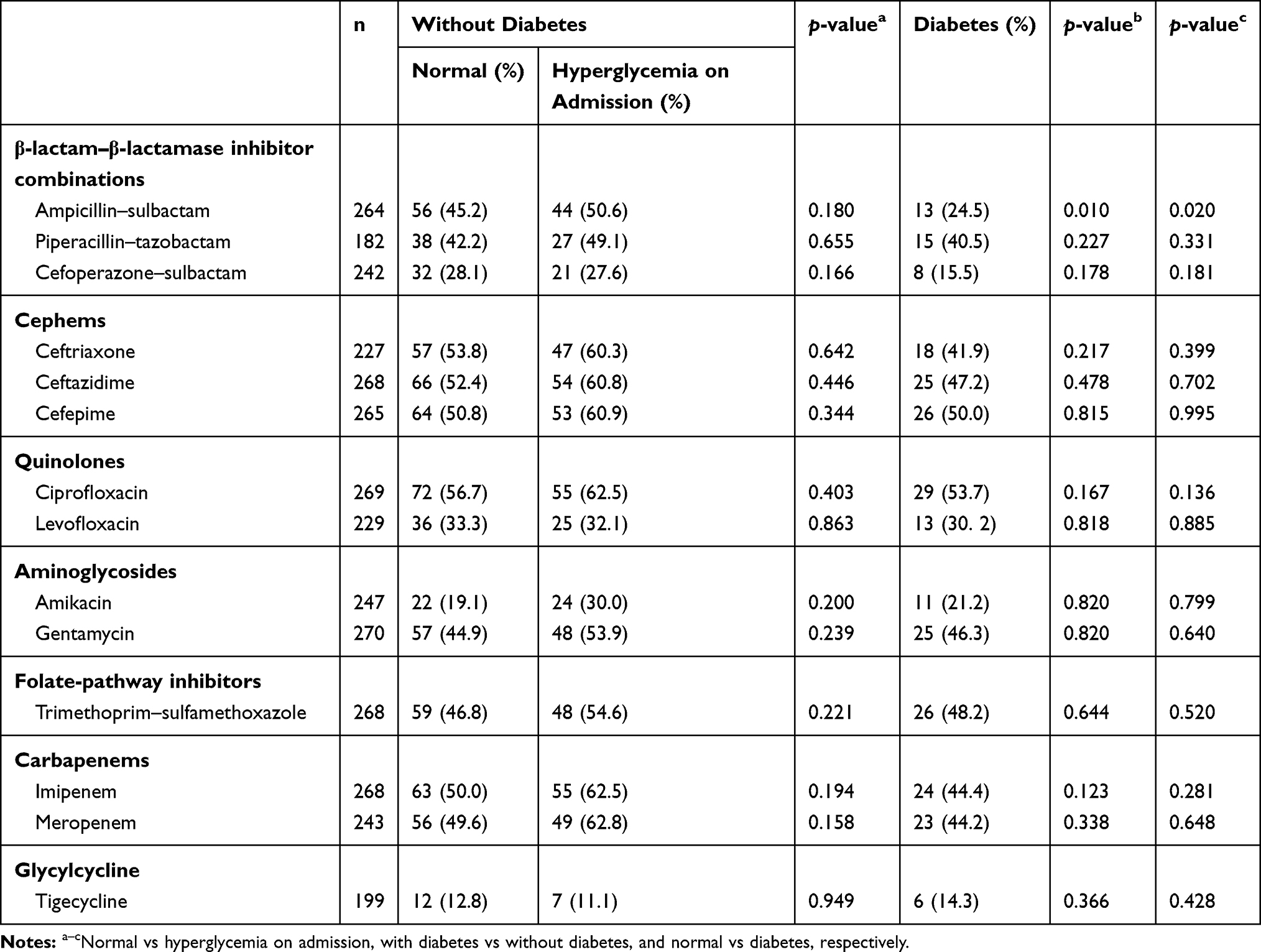 |
Table 4 Antibiotic-Resistance Rate of A. baumannii Isolated from Sputum |
For P. aeruginosa, resistance varied, as patients had different glucose status (Table 5). Nonsusceptibility rates of fosfomycin and carbapenems were higher than other agents. The highest resistance to imipenem was seen among P. aeruginosa isolated from patients with diabetes (34.3%), while for meropenem this was seen among P. aeruginosa isolations from patients with normal glucose (32.1%). No significance was demonstrated for any of the agents tested among the three groups.
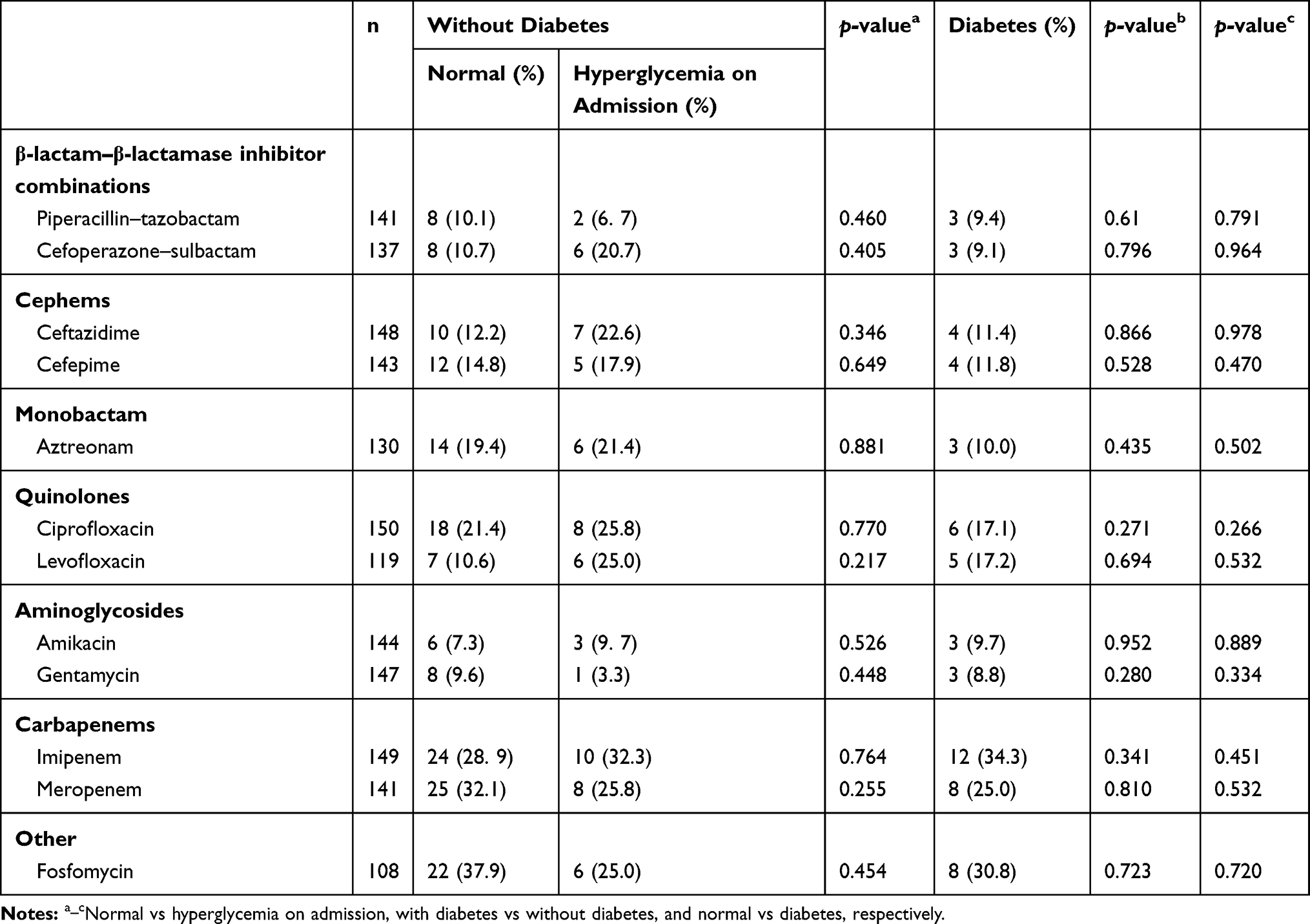 |
Table 5 Antibiotic-Resistance Rate of P. aeruginosa Isolated from Sputum |
S. aureus was the predominant species among Gram-positive cocci, among which MRSA occupied two-thirds and methicillin-susceptible S. aureus (MSSA) about a third (219 vs 112, Table 6). For all tested antimicrobial agents, the resistance rate of MRSA was much higher than MSSA. MSSA from diabetes patients tended to show higher resistance to levofloxacin than from patients without diabetes (p=0.006). No significance was reached for MRSA among those with different glucose status in terms of drug resistance. None of these isolates was detected to be resistant to vancomycin, linezolid, or teicoplanin.
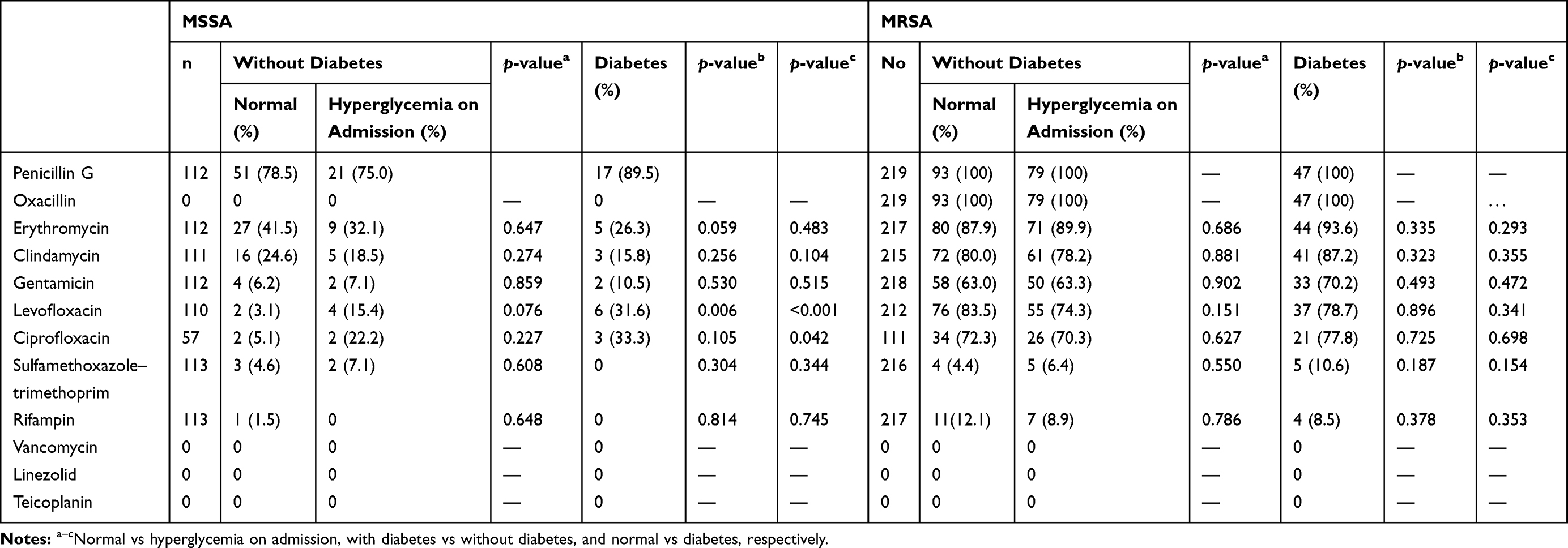 |
Table 6 Antibiotic-Resistance rate of S. aureus Isolated from Sputum |
Discussion
AMR is a threatening crisis all over the world, and poses a great challenge to humans worldwide. Increased AMR demands profound knowledge about epidemiology and potential risk factors in this field so that we can take better control. It has been accepted that prior exposure to antimicrobial agents, residence in health-care facilities, and ICU admission are the risk factors of increased occurrence of AMR.
With significantly increasing prevalence in the past few decades, diabetes affected about 463 million people worldwide in 2019.17 Diabetes is always considered a risk factor during infection. Glucose control is of great importance in clinical practice. Hyperglycemia is associated with worsening outcomes and is a risk factor of in-hospital mortality.7 This is the first study that we know of to focus mainly on the relationship between AMR and glucose level on admission. We found that AMR depended on glucose level on admission. Patients with hyperglycemia were more likely to carry more than one bacterium, much higher than those with normal glucose, and the same trend was also detected in patients with diabetes compared to non-diabetes. What is more, MDR-KP was much more prevalent in patients with hyperglycemia on admission, and the highest rate of MRSA was also detected in patients with hyperglycemia.
In terms of common species of bacteria, Enterobacteriaceae, A. baumannii, P. aeruginosa, and S. aureus — common pathogens causing infections in clinical practice — were also the commonest pathogens detected in the current study. In addition, the distribution of these bacteria was significantly different between those isolated from patients with or without hyperglycemia on admission. Enterobacteriaceae made up the highest proportion among all isolates, and K. pneumoniae was the major pathogen among Enterobacteriaceae for all patients, regardless of glucose-metabolism status. There was no significance detected for the distribution of bacteria isolated from patients with or without diabetes nor for the number of patients carrying more than one isolate between the two groups. All this indicated that hyperglycemia on admission played a much more important role in bacteria distribution and AMR, and this is the first study to provide evidence for the link between AMR and glucose metabolism.
K. pneumoniae was the most commonly detected species among Enterobacteriaceae. At the same time, resistance to most antimicrobials, including imipenem and meropenem, was highest in the hyperglycemia group. Carbapenems serve as last-line antibiotics to treat bacteria that are not susceptible to broad-spectrum antibiotics.18 In mainland China, K. pneumoniae resistance to meropenem and imipenem has increased from 2.6% to 13.4% and 2.4% to 10.5%, respectively.19 In this study, we found that the rate of K. pneumoniae resistance to carbapenems detected among hyperglycemia was higher than the general rate reported in mainland China from 2005 to 2014,19 highlighting the importance of assessing glucose levels on admission and checking the carriage of K. pneumoniae. It was comforting to find that resistance to tigecycline in K. pneumoniae isolates was low, and no significance was reached for the three groups in our study, so tigecycline can be an alternative to deal with infection caused by carbapenem-resistant K. pneumoniae.20 Less exposure to tigecycline may be the potential explanation, but this should be further explored within well-designed research.
For A. baumannii and P. aeruginosa, the two other common kinds of pathogen isolated from sputum in the current study, MDR for all groups was high and no statistical significance was detected for most drugs. The highest rate of carbapenem-resistant A. baumanni was detected among A. baumanni isolated from hyperglycemia patients, and it was much higher than that of P. aeruginosa and K. pneumoniae, which was also a huge threat to inpatients.21 The high-level resistance in A. baumannii was consistent with the reported national average level,19 indicating that broad-spectrum resistance in A. baumannii is emerging, as in a previous study.22 Sputum P. aeruginosa in our study demonstrated a higher resistance rate than the reported epidemiology,19 and the highest rate was always seen among hyperglycemia patients. Structural lung diseases, such as chronic obstructive pulmonary diseases or bronchiectasis, are risks for P. aeruginosa colonization,23 and nearly 20% of patients were comorbid with chronic lung diseases in the present study.
In our study, MRSA had a higher percentage among patients with hyperglycemia or diabetes than normoglycemic individuals. Methicillin resistance in the current study was also higher than that reported throughout our country.19 It has been found that nasal carriage of S. aureus is higher among diabetics.24 An increased risk of community-acquired S. aureus bacteremia has been reported among diabetes patients, especially among those with long duration, poor glycemic control, and diabetes complications.24 What is more, hyperglycemia increases the risks of respiratory infections caused by S. aureus,6,25 and hyperglycemia-induced bacterial growth can be inhibited via modification of glucose flux into the airway epithelium being modified by metformin.26
The phenomenon of resistance rates for K. pneumoniae and S. aureus being higher than the average level throughout our country may be accounted for by the fact that among first-class hospitals, patients’ conditions are always severe in ours. The total number of antimicrobial-susceptibile isolates for each drug varied in this retrospective clinical study, but our findings provide an important indication that patients are at high risk of carrying antibiotic-resistant bacteria, particularly those with hyperglycemia on admission, thus calling for special attention and initial microorganism screening among them. In addition, patients with hyperglycemia had a higher rate of mechanical ventilation and central venous catheter incubation along with increased AMR. Patients with hyperglycemia or diabetes showed a higher rate of ICU admission and in-hospital mortality. The causality linking high antibiotic resistance and worse outcomes among hyperglycemia or diabetes patients should be further explored in prospective studies.
There are several limitations in the current study. Firstly, it was a retrospective study and focused on microorganism resistance in a nosocomial context, which did not distinguish colonization from infection. Bacteria were identified by the Vitek 2 automated system, as mentioned in the Methods section. It would have been valuable if bacterial isolates were identified by 16sRNA and minimum inhibitory concentration determined by agar dilution or broth microdilution. In addition, ESBL was not deeply discussed. Finally, this was a single-center study conducted only in our hospital. Well-designed multicenter studies are needed to delineate the prevalence of AMR among hyperglycemic or diabetic inpatients and the potential link between AMR of bacterial and in-hospital mortality.
In conclusion, the current study provides comprehensive information about bacterial distribution and resistance rates among sputum isolates, including K. pneumoniae and S. aureus, for hyperglycemia or previously diagnosed diabetes patients. The findings are of utmost importance in clinical calls for focused efforts to distinguish patients with hyperglycemia on admission or previous diagnosis of diabetes from those with normoglycemia, for they are prone to carrying resistant bacteria.
Acknowledgments
The abstract of this paper — "Increased antimicrobial resistance among sputum pathogens from patients with hyperglycemia: a retrospective study from a hospital in Shanghai" — was presented at the American Thorax Society Conference (2019) as a poster presentation with interim findings.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The study was supported by the National Key R&D Program of China (2017YFC1309701 and 2017YFC1309700), National Natural Science Foundation of China (81570029), Shanghai Key Discipline for Respiratory Diseases (2017ZZ02014), and innovative research teams of high-level local universities in Shanghai.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
2. Group IDFDA. Update of mortality attributable to diabetes for the IDF Diabetes Atlas: estimates for the year 2013. Diabetes Res Clin Pract. 2015;109(3):461–465. doi:10.1016/j.diabres.2015.05.037
3. Xu Y, Wang L, He J, et al. Prevalence and control of diabetes in Chinese adults. JAMA. 2013;310(9):948–959. doi:10.1001/jama.2013.168118
4. Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010 a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):27. doi:10.1016/S0140-6736(12)61689-4
5. Lepper PM, Ott S, Nuesch E, et al. Serum glucose levels for predicting death in patients admitted to hospital for community acquired pneumonia: prospective cohort study. BMJ. 2012;344:e3397. doi:10.1136/bmj.e3397
6. Baker EH, Janaway CH, Philips BJ, et al. Hyperglycaemia is associated with poor outcomes in patients admitted to hospital with acute exacerbations of chronic obstructive pulmonary disease. Thorax. 2006;61(4):284–289. doi:10.1136/thx.2005.051029
7. Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, AE K. Hyperglycemia an independent marker of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab. 2002;87(3):5. doi:10.1210/jcem.87.3.8341
8. Santajit S, Indrawattana N. Mechanisms of antimicrobial resistance in ESKAPE pathogens. Biomed Res Int. 2016;2016:2475067. doi:10.1155/2016/2475067
9. Gajdacs M. The concept of an ideal antibiotic: implications for drug design. Molecules. 2019;24:5. doi:10.3390/molecules24050892
10. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
11. Barrasa-Villar JI, Aibar-Remón C, Prieto-Andrés P, et al. Impact on morbidity, mortality, and length of stay of hospital-acquired infections by resistant microorganisms. Clin Infect Dis. 2017;65(4):644–652. doi:10.1093/cid/cix411
12. Neidell MJ, Cohen B, Furuya Y, et al. Costs of healthcare- and community-associated infections with antimicrobial-resistant versus antimicrobial-susceptible organisms. Clin Infect Dis. 2012;55(6):807–815. doi:10.1093/cid/cis552
13. Mauldin PD, Salgado CD, Hansen IS, et al. Attributable hospital cost and length of stay associated with health care-associated infections caused by antibiotic-resistant gram-negative bacteria. Antimicrob Agents Chemother. 2010;54(1):109–115. doi:10.1128/AAC.01041-09
14. Tian LT, Yao K, Zhang XY, et al. Liver abscesses in adult patients with and without diabetes mellitus: an analysis of the clinical characteristics, features of the causative pathogens, outcomes and predictors of fatality: a report based on a large population, retrospective study in China. Clin Microbiol Infect. 2012;18(9):E314–30. doi:10.1111/j.1469-0691.2012.03912.x
15. Tian L, Tan R, Chen Y, et al. Epidemiology of Klebsiella pneumoniae bloodstream infections in a teaching hospital: factors related to the carbapenem resistance and patient mortality. Antimicrob Resist Infect Control. 2016;5:48. doi:10.1186/s13756-016-0145-0
16. American Diabetes A2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2018. Diabetes Care. 2018;41(Suppl 1):S13–S27.
17. http://www.diabetesatlas.org.
18. Gupta N, Limbago BM, Patel JB, et al. Carbapenem-resistant Enterobacteriaceae: epidemiology and prevention. Clin Infect Dis. 2011;53(1):60–67. doi:10.1093/cid/cir202
19. Hu FP, Guo Y, Zhu DM, et al. Resistance trends among clinical isolates in China reported from CHINET surveillance of bacterial resistance, 2005-2014. Clin Microbiol Infect. 2016;22(Suppl 1):S9–14. doi:10.1016/j.cmi.2016.01.001
20. Tzouvelekis LS, Markogiannakis A, Psichogiou M, et al. Carbapenemases in Klebsiella pneumoniae and other Enterobacteriaceae: an evolving crisis of global dimensions. Clin Microbiol Rev. 2012;25(4):682–707. doi:10.1128/CMR.05035-11
21. Pogue JM, Mann T, Barber KE, Carbapenem-resistant KSK. Acinetobacter baumannii epidemiology, surveillance and management. Expert Rev Anti Infect Ther. 2013;11((4:383–393. doi:10.1586/eri.13.14
22. Potron A, Poirel L, Nordmann P. Emerging broad-spectrum resistance in Pseudomonas aeruginosa and Acinetobacter baumannii: mechanisms and epidemiology. Int J Antimicrob Agents. 2015;45(6):568–585. doi:10.1016/j.ijantimicag.2015.03.001
23. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27–72.
24. Smit J, Søgaard M, Schønheyder HC, Nielsen H, Frøslev T, RW T. Diabetes and risk of community-acquired Staphylococcus aureus bacteremia A population-based case-control study. Eur J Endocrinol. 2016;174(5):9. doi:10.1530/EJE-16-0023
25. Philips BJ, Redman J, Brennan A, et al. Glucose in bronchial aspirates increases the risk of respiratory MRSA in intubated patients. Thorax. 2005;60(9):761–764. doi:10.1136/thx.2004.035766
26. Garnett JP, Baker EH, Naik S, et al. Metformin reduces airway glucose permeability and hyperglycaemia-induced Staphylococcus aureus load independently of effects on blood glucose. Thorax. 2013;68(9):835–845. doi:10.1136/thoraxjnl-2012-203178
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.