")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Aspects of cognitive performance relating to Theory of Mind (ToM) among people diagnosed with Post-Traumatic Stress Disorder (PTSD)
Authors Altunbas FD, Onen Unsalver B , Yasar AB
Received 6 May 2019
Accepted for publication 28 June 2019
Published 17 July 2019 Volume 2019:15 Pages 2015—2025
DOI https://doi.org/10.2147/NDT.S214595
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Fatma Dilara Altunbas,1 Baris Onen Unsalver,1 Alisan Burak Yasar2
1Uskudar University, Department of Psychology, Istanbul, Turkey; 2Marmara University Hospital, Department of Psychiatry, Istanbul, Turkey
Objective: This study investigated Theory of Mind (ToM) abilities as measured by a hinting task and the Reading the Mind in the Eyes Test (RMET) in individuals diagnosed with post-traumatic strees disorder (PTSD) in relation to different types of childhood trauma and compared to a healthy control group.
Method: RMET, a Clinician Administered PTSD Scale (CAPS), a Beck Depression Inventory (BDI), a Childhood Trauma Questionnaire (CTQ), a hinting task, and a socio-demographic questionnaire were administered to PTSD (n=30) patients and healthy controls (n=30).
Results: There was a significant difference in ToM performance between healthy participants and the PTSD group (p<0.001). A significant correlation was found between trauma types and ToM performance (p<0.01). The diagnosis of PTSD and the severity of PTSD symptoms showed significant correlations with ToM performance (p<0.01). In comparison with the healthy control group, the PTSD group demonstrated lower performance on both ToM tasks. Regardless of the PTSD diagnosis, those people who had a history of childhood trauma had slowed reaction times in response to photographs representing emotionally salient mental states and demonstrated difficulties in the identification of irony/hints in the context of the administered assessment task.
Conclusion: The findings of the present study suggest that a diagnosis of PTSD and a history of different types of trauma have an effect on ToM performance. PTSD seems to lead to deterioration in ToM capacities. This may mean that the experience of childhood adversity may lead to long-lasting damage to social cognition. The current study is helpful in that it contributes to a better understanding of the pathogenesis of PTSD; moreover, it will be beneficial in the development of new treatment options. Our research findings suggest that we must concentrate not only on traumatic events during the treatment process of PTSD follow-up and treatment; we must also target deficiencies in cognitive and emotional capabilities.
Keywords: PTSD, Theory of Mind, ToM, trauma, trauma types
Introduction
Theory of mind (ToM) is the capacity to understand other people’s mental states, their beliefs, intentions, desires, and knowledge. This ability is important for social interactions and communication.1 The concept of ToM was first used in 1978 by Woodruff and Primack, and a wide variety of tasks, methods, and theories on this topic have been accumulating in the literature since that time.2 Good communication skills are important for good social interactions and for being successful in life; ToM abilities comprise being aware of other people’s emotional and cognitive states, so it, therefore, has a crucial role in social interaction and effective communication.3 Theory of mind abilities is associated with social emotional capability and social competence.4 Deficits in ToM may result in problems in social-emotional functioning.
Development of ToM starts from early infancy and extends into adolescence.5,6 Children observe their environment and they gain ToM skills through experience; in this way, they can predict the intentions, beliefs, and desires of others.7 Theory-theory by Adam Morton (1980) asserts that differentiating between real situations and mental states is possible if one has the ability to compare previously observed and learned multiple mental models simultaneously.8
Theory of mind functioning becomes more complex as the child grows up. As ToM develops, children become aware of others’ intentions and begin to understand that people may manipulate their own behaviors based on their purposes. ToM ability is crucial for empathy and necessary for social interaction.9 ToM abilities are as follows: First-order ToM (the ability to identify what somebody else is thinking), second-order ToM (representing the ability of the person to make a prediction of what someone else thinks about the thoughts of a third party), understanding of the metaphor, understanding of the irony, understanding of faux pas (behaving in a wrong way or saying something impolite that leads to an awkward situation in society), and language processing. Therefore, it can be said that social cognition is a product of ToM abilities.
There is no consensus on which tests to use when measuring ToM. Earlier measurements of ToM included various false-belief tasks.10 However, the observation that these measurements were not reliable enough for measuring certain social-cognitive deficits seen in older children and adolescents led to the development of more sensitive tests such as the Reading the Mind in the Eyes Test (RMET) and Strange Stories.11,12 After a lengthy development process, researchers came up with a variety of measurement tools such as the Levels of Emotional Awareness Scale (LEAS), the Awkward Moments Test, and the Movie for the Assessment of Social Cognition (MASC).13–15 Hinting Task is one of the most-used tests in the purpose of assessing ToM abilities.16 The test includes 10 brief stories, which have 2 characters, and at the end of each story, one of the characters drops a moderately clear hint.17 The aim of these tests was to determine ToM abilities such as understanding of emotion, perspective taking, understanding the interpretive nature of mind, attribution of intention, and explanation of behavior with reference to beliefs, knowledge, and desires.18
Post-traumatic stress disorder (PTSD) is a mental health problem that some people develop after experiencing or witnessing a life-threatening event, such as combat, a natural disaster, a car accident, or sexual assault. Two types of trauma can be described according to the duration of exposure. If the traumatic exposure duration is brief (eg, a car accident), it is classified as Type I and if the traumatic exposure is prolonged and repeated (eg, sexual abuse), it is classified as Type II.19 Even though both types of traumas may result in psychopathology, Type II traumas are more commonly associated with life-long psychopathology.20–24 Childhood traumatic events are generally Type II traumas. The prolonged and repeated nature of Type II traumas of childhood would be expected to be associated with deleterious consequences for brain maturation through psychophysiological changes such as prolonged cortisol secretion and a hyperadrenergic state.25
Childhood traumas may affect the development of ToM abilities. Those who inflict the traumas may not be behaving in an abusive or neglectful manner toward the child all the time. Therefore, the child may not have a uniform model of the person, which would be expected to damage the predictive abilities of the child about the intentions, beliefs, and desires of others. The psychophysiological effects of trauma on the developing brain may hamper learning and further development of ToM skills. Maturation of processing capabilities and resources required for ToM abilities may be disrupted.26 Childhood trauma, either in the form of abuse or neglect, may disrupt the learning process (as described in the introduction) required for the development of ToM.27 A study of 47 subjects who had schizophrenia or schizoaffective disorder diagnosis demonstrated that history of exposure to adverse childhood events had a considerable effect on the functioning of certain brain regions (such as the posterior cingulate cortex, precuneus, dorsomedial prefrontal cortex, and temporoparietal junction) during the performance of a ToM task.28
Several studies have suggested that childhood traumas may have a significant role on the functioning of social cognition.29 In an earlier study, 16 Bosnian refugees with war-related PTSD had lower scores on the RMET in comparison to 16 non-PTSD refugees and 50 non-PTSD Danish people.30 In a study by Nietlisbach et al (2010), empathic abilities of PTSD patients (n=16) were evaluated with several tasks such as RMET, empathic resonance test, and faux pas test in comparison to healthy controls (n=16).31 PTSD group had lower RMET scores but the differences were not significant (p=0.14). Shenk et al found that maltreated female adolescents who had low levels of intellectual functioning were less accurate on recognizing facial affect in comparison to non-maltreated controls. In that study, The Dynamic Affect Recognition and Evaluation (DARE) task was used for the assessment of affect recognition ability.32 Nazarov et al (2015) found that women with childhood-abuse-related PTSD had decreased ability to discriminate affective prosody which is essential for social cognition.33
In a study in which 31 women diagnosed with PTSD and 20 healthy women were compared on the basis of their ToM task performances, it was found that women exposed to childhood sexual abuse had lower ToM performance; this was especially the case for ToM abilities required for the interpretation of family interactions.34 This is an important finding indicating the presence of probable misinterpretations in current relationships that might have disruptive consequences for social functioning. Germine and his colleagues (2015) assessed the effects of childhood experiences on functioning of social cognition in adulthood and found that adverse childhood memories partially affected ToM performance.35 In a study of 58 outpatients with psychotic disorders, Mrizak et al (2016) found that a history of childhood trauma was significantly correlated with worsened performance on an intention-inferencing task.36 In contrast, in a study by van Schie et al (2017), emotionally abused and neglected adolescents did not show decreased performance on the RMET.37 They suggested that this could be the result of using different strategies to overcome the difficulties in understanding emotions. The impairments in social cognition may only become observable in more complex or stressful situations than the test conditions.34
The available literature implies that a history of childhood traumatic experiences may result in limited ToM skills, which in turn may give rise to social interaction problems. Therefore, the main focus of the present study was to assess the cognitive performance relating to ToM among people diagnosed with PTSD in comparison to healthy controls. The secondary aim of the study was to investigate the impact of different types of childhood traumatic experience on ToM performance and to determine whether the severity of PTSD symptoms regardless of current PTSD diagnosis had an impact on current ToM performance.
Materials and methods
Sample
The study was conducted with 60 participants and included 30 people diagnosed with childhood trauma-related (type-II traumas) PTSD and 30 healthy controls. The study inclusion criteria for the PTSD group participants were: 1) having an age between 18 and 65 years; 2) being literate; 3) having no organic brain damage; 4) having not consumed medicine that might influence brain function for the last month; and 5) not having a diagnosis of substance abuse. The inclusion criteria for the healthy control group were: 1) being between 18 and 65 years of age; 2) being literate; 3) not having organic brain damage; 4) not having a history of psychiatric treatment; and 5) not having a diagnosis of substance abuse.
This study was approved by the ethical committee of Uskudar University. The study conforms with the ethical principles of Helsinki Declaration for medical research with human subjects. Each patient gave written informed consent for the use of their medical data in the study.
Measurements
Diagnosis of PTSD was confirmed via the Structured Clinical Interview for DSM-IV (SCID).38,39 The SCID is a semi-structured interview administered by a clinician and was developed for the purpose of making a diagnosis of PTSD based on DSM-IV-TR criteria. Post-traumatic stress disorder symptom severity was assessed using the Clinician-Administered PTSD Scale (CAPS). Childhood trauma history was measured with the Childhood Trauma Questionnaire (CTQ). The Reading the Mind in the Eyes Test (RMET) and hinting task were also administered to estimate ToM capabilities.
A sociodemographic questionnaire was used to obtain personal information from participants, and was developed by researchers to collect information on the participants’ age, sex, and education levels. Through the questionnaire, information about participants’ and their families’ mental health history, medical health history, and socioeconomic status were gathered.
CTQ is a 28-item self-report retrospective inventory whose purpose is to measure childhood or adolescent abuse and neglect. It is straightforward and easy to use. The examinee responds to 28 simple questions on a 5-point Likert scale ranging from “Never True” to “Very Often True”.40 Turkish version of the scale is validated by Şar et al.41 CTQ includes 5 sub-scales, which are physical abuse, emotional abuse, physical neglect, emotional neglect, and sexual abuse. Physical abuse refers to bodily aggression toward a child by an older person that might result in injury. Emotional abuse refers to verbal assault direct to a child by an older person that might lead to the feeling of unworthiness and threatened. Physical neglect refers to the inability of satisfying a child’s basic needs such as shelter, food, and safety. Emotional neglect refers to failing to provide basic psychological and emotional needs such as love, support, and belonging for the child. Sexual abuse refers to sexual contact or conducts with a child by an older person through threatening or explicit coercion.42
The Clinican-Administered Posttraumatic Stress Disorder Scale (CAPS) includes 30 questions administered by a trained clinician to assess for PTSD symptoms, including the frequency and severity of a patient’s symptoms. The score of CAPS varies between 0 and 136 based on the severity of PTSD symptoms. The CAPS was developed by Blake and his colleagues and is an in-person clinical assessment for the measurement of post-traumatic stress disorder (PTSD).43 The Turkish version of the assessment was validated by Aker et al.44
The RMET measures the ability of a person to attribute mental states to others from their eyes.11 Turkish validation of the test was made by Yıldırım and his colleagues. According to the study, the Turkish version of RMET was found reliable in a healthy population.45 The test is applied via the presentation of 36 images with four emotion terms. The participant must make a choice between these four emotion terms. Administration of the test requires approximately 10 mins.
The Hinting Task that is used in the study includes 10 short stories. At the end of each story, the protagonist emphasizes his/her intention implicitly. Participants are asked to determine the protagonist’s intention and it is expected that the participant uses ToM capabilities during the task. For each correct answer, 2 points are given.46
Statistical analysis
All statistical analyses were performed using SPSS 21.0. Descriptive statistical findings were described. We aimed to investigate whether ToM performance was “higher” or “lower” in participants with a PTSD diagnosis as compared to healthy controls. This paper used the Mann–Whitney U test in consideration of the following three factors: a) two independent groups were being compared, b) the data collected does not follow a normal distribution, and c) the obtained nominal variables were to be compared with one another.
A chi-square analysis was used to compare discrete variables (sex, marital status, educational background, family mental health history, and family medical health history). Correlation between PTSD symptoms and ToM performance, and trauma types and ToM performance, were analyzed with the Spearman correlation test. Statistical significance was set at p<0.05.
Results
Participants
The study was conducted with 60 participants, of which 19 were male and 41 were female. In addition, all participants with PTSD reported moderate-to-severe histories of childhood trauma on the CTQ. Clinical and demographic characteristics of the sample are summarized in Table 1.
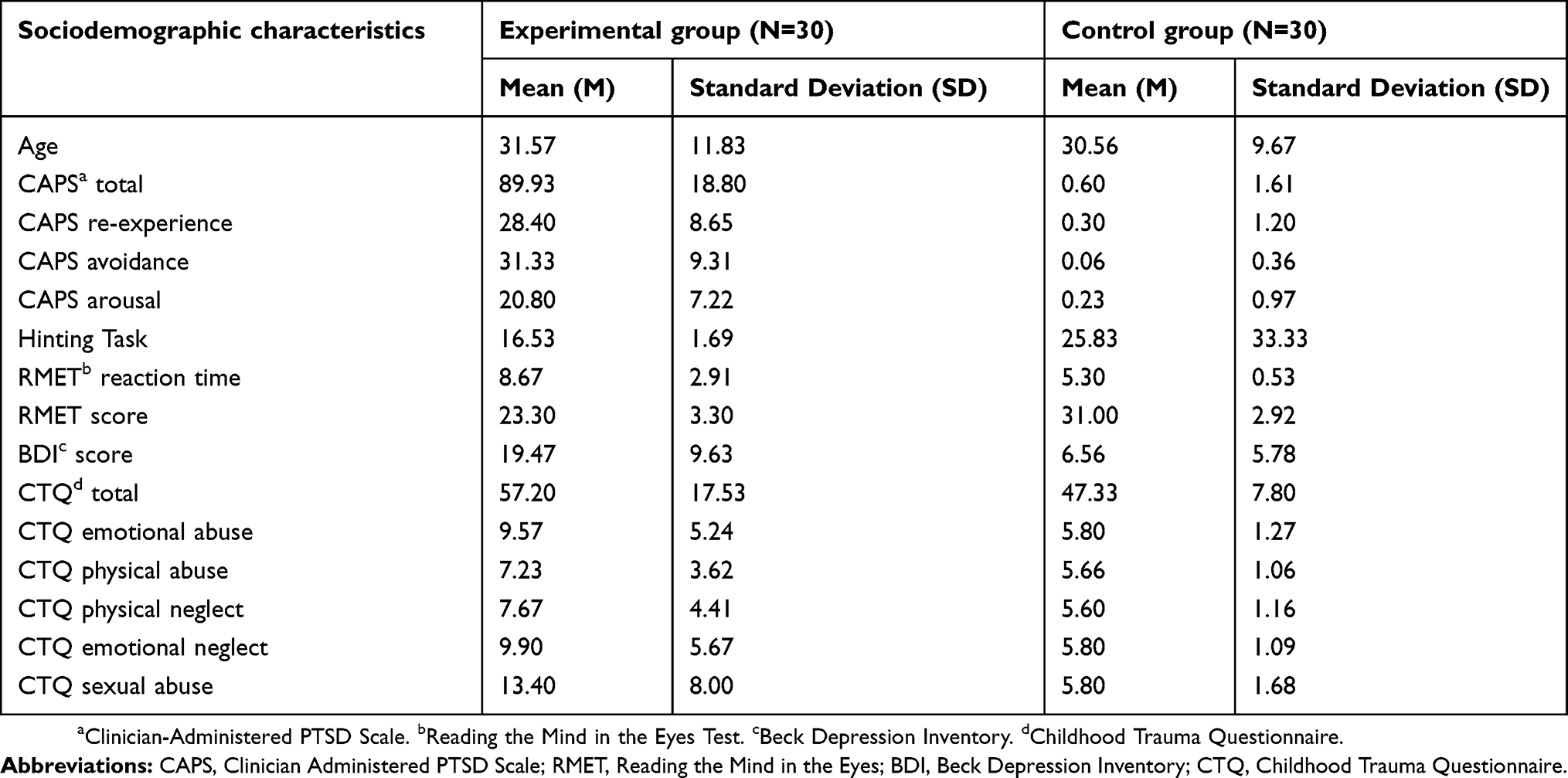 |
Table 1 Clinical and demographic characteristics of study sample |
The analyses were not controlled for education levels because the education levels were not defined in terms of years but as the last school finished such as primary school, college, or master’s degree. According to the chi-square analysis, the groups were not significantly different in terms of education levels (p=0.069, chi-square value=7.105). The results of the ToM tests could have been affected by sex and age differences. However, there were not any significant differences between the PTSD and the control group in terms of sex (p=0.78) and age (p=0.91).
Group comparisons for performance on ToM measures and CTQ scores
Comparisons of the PTSD and the control group on RMET and Hinting Task performances and the CTQ scores are summarized in Table 2.
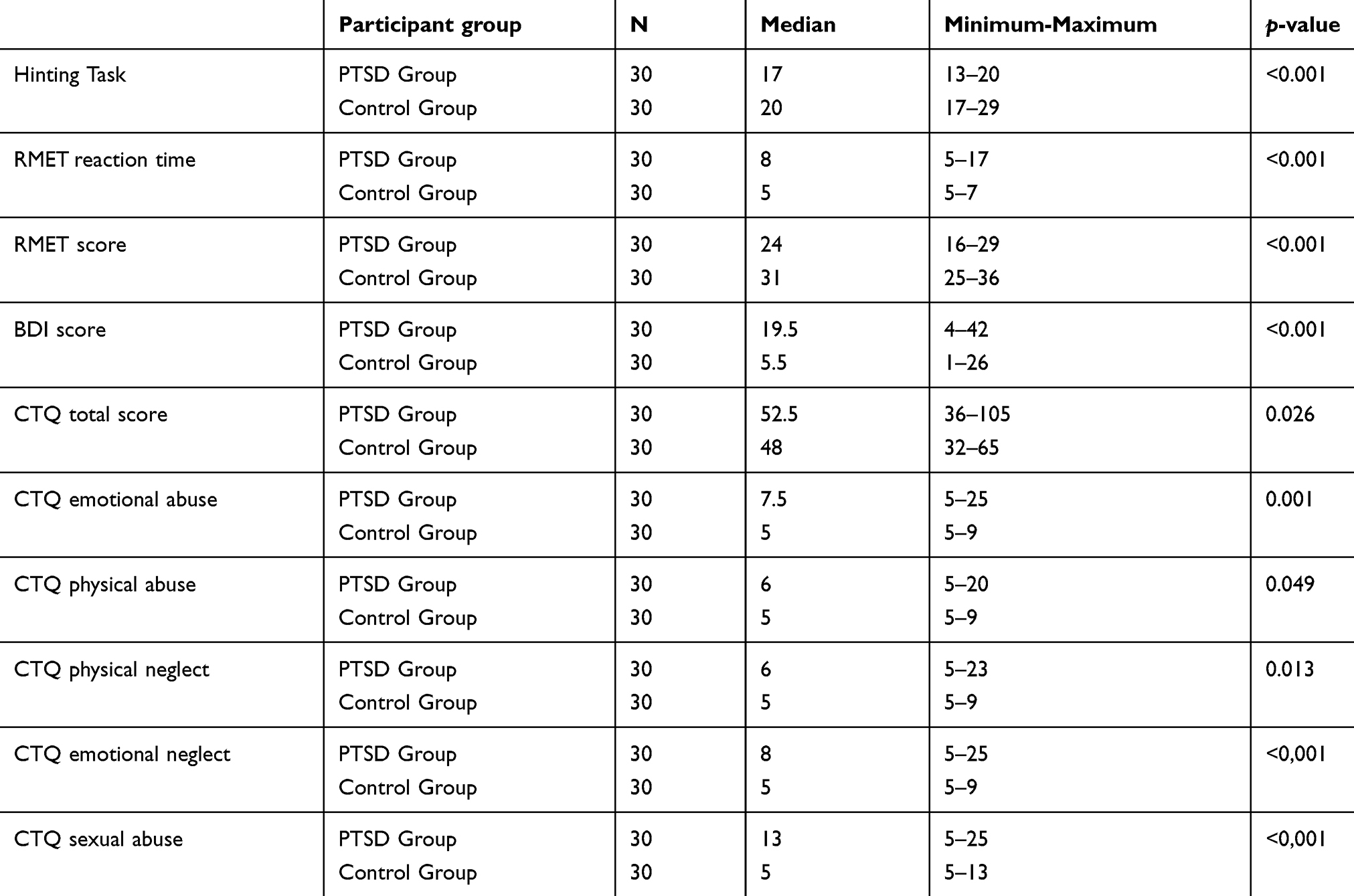 |
Table 2 Comparison of the PTSD and control group on ToM tasks and childhood trauma types |
RMET performance
Relative to controls, the PTSD group who had experienced childhood trauma had difficulties in identifying emotions/mental states of others from their eyes (p<0.001). The average RMET score was 24 points (16–29) for the PTSD group, whereas the average score for the control group was 31 points (25–36).
Reaction times for RMET pictures were recorded for each participant. The results of the Mann–Whitney U test showed that the PTSD group displayed significantly slower reactions in response to photographs (p<0.001). The average reaction time for the RMET among PTSD group participants was 8 (5–17) mins, and the average reaction time of the control group was 5 (5–7) mins.
Hinting task performance
According to the Mann–Whitney U test analysis and relative to the control group, the PTSD group demonstrated worse performance with regard to noticing the irony/hint in stories. The average score for this task in the experimental group was 17 (13–20) and the average score of the control group was 20 (17–29). The difference between the two groups was significant (p<0.001).
Childhood trauma questionnaire scores
The PTSD group displayed significant differences from the control group on the total CTQ score (p=0.026), being emotionally abused (p=0.001), being physically abused (p=0.049), being physically neglected (p=0.013), being emotionally neglected (p<0.001), and being sexually abused (p<0.001).
Relation between ToM tasks and childhood trauma type scores
The Spearman correlation analysis was conducted to determine the relationship between childhood-trauma-type scores and ToM task performances of the whole sample (n=60) regardless of the diagnosis of PTSD. We found significant associations between ToM performance and childhood trauma type scores (see Table 3).
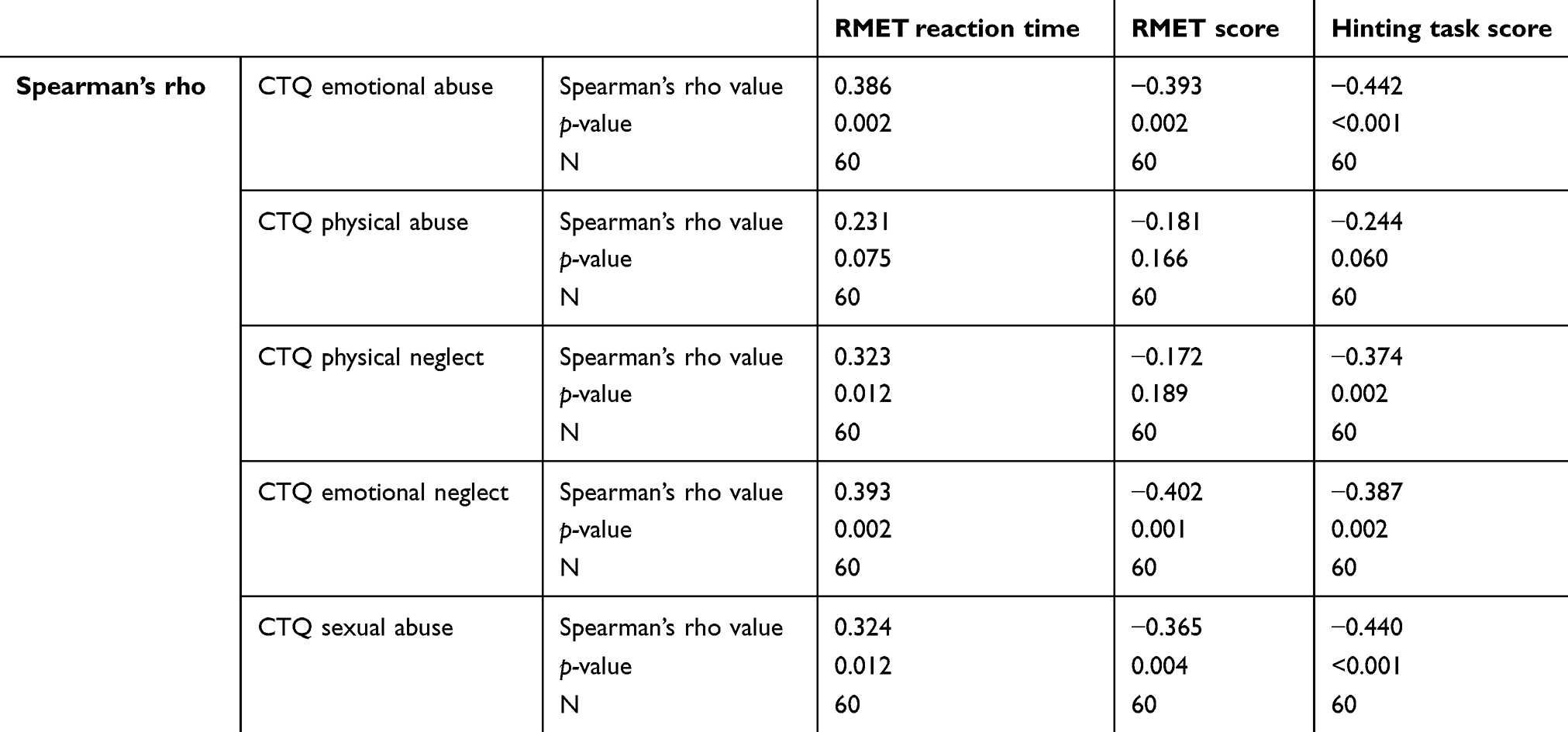 |
Table 3 Correlation analyses between CTQ scores and ToM tasks scores |
Being emotionally abused
There was a moderate, negative, and significant correlation between being emotionally abused and RMET scores (p=0.002). There was a moderate, positive, and significant correlation between being emotionally abused and the reaction time to RMET images (p=0.002). There was also a moderate, negative, and significant correlation between being emotionally abused and hinting task performance (p<0.001).
Being physically neglected
There was a moderate, positive, and significant correlation between being physically neglected and reaction time to RMET images (p=0.002). There was a moderate, negative, and significant correlation between being physically neglected and hinting task performance (p=0.003). There was no significant correlation between RMET scores and being physically neglected (p=0.189).
Being emotionally neglected
There was a moderate, negative, and significant correlation between RMET scores and being emotionally neglected (p=0.001). A moderate, positive, and significant correlation emerged between being emotionally neglected and reaction time to RMET images (p=0.002). There was a moderate, negative, and significant correlation between being emotionally neglected and hinting task performance (p<0.001).
Being sexually abused
There was a moderate, positive, and significant correlation between being sexually abused and reaction time to RMET images (p=0.012). There was a moderate, negative, and significant correlation between being sexually abused and RMET scores (p=0.004). There was a moderate, negative, and significant correlation between being sexually abused and hinting task performance (p<0.001).
Relationship of CTQ subscales
A Spearman correlation analysis was also applied for determining the relationship between CTQ sub-scales. According to the analysis, there was a moderate, positive, and significant relationship between physical abuse and emotional abuse (p<0.01). Also, there was a moderate, positive, and significant relationship between physical neglect and emotional abuse (p<0.001); moreover, a moderate, positive, significant correlation was determined between physical neglect and emotional neglect (p<0.05). Additionally, there was a moderate, positive, and significant correlation between sexual abuse, physical abuse, emotional abuse, and emotional neglect (p<0.001).
Relation between ToM tasks and PTSD symptom scores
The Spearman correlation analysis was conducted to determine the relationship between ToM task performances and PTSD symptom scores of the whole sample regardless of the diagnosis of PTSD. We found significant associations between ToM performance and PTSD symptom scores in our sample (see Table 4).
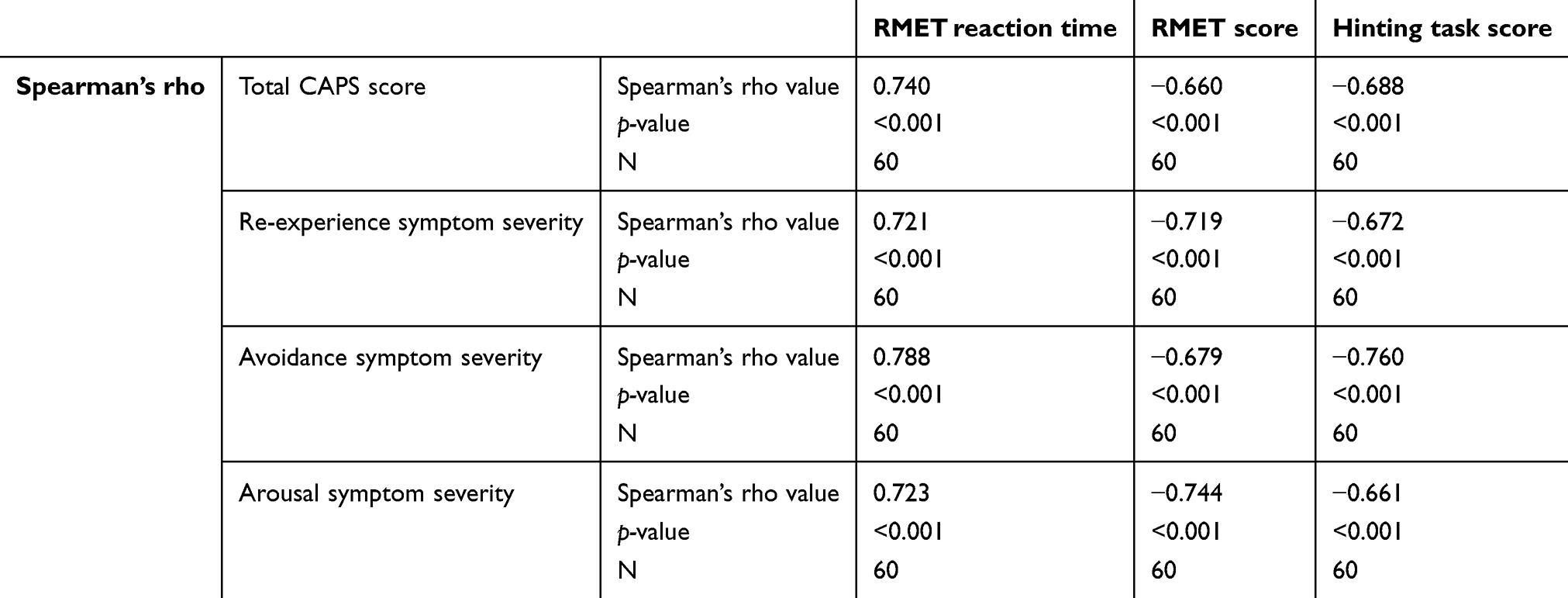 |
Table 4 Correlation analyses between CAPS scores and the ToM tasks scores |
Total CAPS score
There was a moderate, negative, and significant correlation between total CAPS scores and RMET scores (p<0.001), and total CAPS scores and hinting task scores (p<0.001). Furthermore, it was found that there was a strong, positive, and significant correlation between total CAPS scores and reaction time to RMET images (p<0.001).
Re-experiencing of symptom score
There was a moderate, negative, and significant correlation between RMET scores and re-experiencing of symptom severity (p<0.001), hinting task scores and re-experiencing of symptom severity (p<0.001). A moderate, positive, and significant correlation between RMET reaction time and re-experiencing symptom severity was found (p<0.001).
Avoidance symptom score
There was a moderate, negative, and significant correlation between RMET scores and avoidance symptom severity (p<0.001), hinting task scores and avoidance symptom severity (p<0.001). A moderate, positive, and significant correlation between RMET reaction time and avoidance symptom severity was found (p<0.001).
Arousal symptom score
There was a moderate, negative, and significant correlation between RMET score and arousal symptom severity (p<0.001), hinting task score and arousal symptom severity (p<0.001). In addition to that, a moderate, positive, and significant correlation between RMET reaction time and arousal symptom severity was found (p<0.001).
Discussion
This study investigated ToM abilities as measured by the RMET and hinting task in individuals diagnosed with PTSD in relation to different childhood trauma types and in comparison to a healthy control group. We found that a history of emotional neglect, physical neglect, emotional abuse, and sexual abuse showed a significant and negative correlation with ToM task performance. In comparison with the healthy control group, the PTSD group demonstrated lower performance on both ToM tasks. Regardless of the PTSD diagnosis, those people who had a history of childhood trauma had slowed reactions in response to photographs representing emotionally salient mental states, and they demonstrated difficulties in the identification of irony/hints in the context. This may mean that experience of childhood adversity might have led to long-lasting damage to social cognition. Consistent with the available literature, our findings suggest that being exposed to childhood traumas (emotional neglect, physical neglect, emotional abuse, and sexual abuse) affects ToM performance in a negative way.
The psychosocial difficulties that people with PTSD encounter may be related to deficits in social cognition. Neurocognitive problems such as mental defeat, negative appraisal of emotions, perceived negative responses of others, or cognitive distortions may arise in people with PTSD.47,48 Lysaker et al conducted a study to compare the metacognitive capacities in patients with PTSD, HIV(+), and schizophrenia. The study revealed that the PTSD group experienced difficulties in emotion identification and had metacognitive deficits associated with subjective distress, avoidance or numbing, and hyperarousal symptoms.49 Lanius et al revealed that in comparison to healthy controls, individuals with PTSD displayed more behavioral and neuro-biological problems that affected emotional self-awareness, emotion regulation, social emotional processing, and self-referential processing.50 In a meta-analysis of social cognition performance in social phobia, post-traumatic stress disorder, and other anxiety disorders it was found that PTSD patients showed impairments in mentalizing abilities and emotion recognition.51 However, this study included only 6 studies on PTSD. Mazza et al (2012) studied 35 veterans who had been exposed to terrorist attacks and subsequently diagnosed with PTSD. In comparison with the healthy group, the PTSD group had lower scores on emotion recognition tasks and experienced emotional numbness.52 Our results showed a much stronger correlation between PTSD symptom severities with ToM than childhood trauma alone. We found that the ToM performance of participants with PTSD was impaired in comparison with the healthy control group. The severity of PTSD symptoms was one of the determinants affecting the functioning of ToM capabilities. People who experienced the severe form of re-experience, avoidance, and arousal symptoms showed worse performance with respect to understanding the mental states of other people and identifying the hint/irony in dialogues. Furthermore, the severity of PTSD symptoms affected reaction time with regard to the identification of RMET images. This might mean that PTSD may be associated with deficits in social cognitive functioning. Moreover, if the severity of PTSD increases, impairment of ToM performance might increase as well. As a result of ToM impairment that accompanies PTSD, people with a PTSD diagnosis might experience social interaction problems, lower academic performance, and communication problems. The PTSD group had difficulties in interpreting scenes depicting kinship interactions. They also demonstrated slowed reactions in response to photographs depicting emotionally salient mental states and had difficulty identifying the irony/hints in a given context.
Nazarov and his colleagues argued that PTSD causes damage to brain areas associated with ToM abilities and functioning.34 In their study, Nazarov et al found that study participants diagnosed with PTSD experienced communication problems with their family members and had longer reaction times for the recognition of complex mental states from emotionally salient facial/eye expressions (as opposed to healthy participants). They also experienced difficulties in noticing hints/ironies in dialogues. In our sample, ToM functioning was directly affected by a diagnosis of current PTSD, the severity of PTSD, and its symptoms. Different trauma types, a PTSD diagnosis, and PTSD symptoms had an impact on ToM performance and socio-cognitive abilities; participants exposed to one or more different type of traumas and diagnosed with PTSD experienced difficulties with understanding/predicting of others’ intentions, beliefs, behaviors, wishes, emotions, and hints/ironies. In light of our results and the existing literature, it would be interesting to investigate how people with histories of abuse (but without PTSD symptoms) would perform in ToM tasks.
This research suggests that certain cognitive practices and ToM tasks can be incorporated into the treatment process of clients diagnosed with PTSD for the purpose of increasing ToM abilities. The present study implies that patients diagnosed with PTSD have problems in identifying the mental states of other people and experience difficulties in noticing hints/ironies in speech. This means that they might have trouble communicating with people, experience problems in academic life, and have difficulties in social interaction. Our finding is compatible with what Hiatt and Trafton (2010) emphasize with ST; that is, empathetic abilities have a key role in the functionality of ToM.7 Therefore, ToM abilities can be damaged as a result of PTSD and this situation might lead to problems with social interaction. Furthermore, as Moran (2013) has noted, ToM becomes more complex with age.53 Participants diagnosed with PTSD are more likely to make faux pas because of their dysfunctional ToM skills. To overcome this, “reading the mind” practices may be recommended for these patients. Therapy disciplines whose aim is to increase the ability to self-express and understand the mental states of others would be beneficial. Cognitive restructuring psychotherapy techniques and cognitive rehabilitation techniques could be useful in the treatment process of PTSD clients. Play-acting or other such experimental roles could also be helpful in such instances. These acting experiences would be different to other forms of experience; such activity might then lead to improvement in both empathy and ToM skills.54 Additionally, certain simulation techniques and technological tools could be used for practicing emotion identification. Techniques that increase emotional awareness in the patient and in other people must be a treatment priority. Group therapies can also be beneficial in accelerating the healing process.
Our modest sample size is one of the limitations of this study. Clinician-administered tasks were carried out by the same researcher who was not blind to the diagnosis of participants. This might have resulted in bias in the interpretation of the results of the tasks. The participants were examined and tested only once. Had they been examined and tested again at a separate point in time (eg, 6 months later) and if the secondary results were consistent with the primary ones, then our suggestion that a diagnosis of PTSD and/or a history of different types of trauma have an effect on ToM performance in comparison with healthy participants would be more powerful. We used RMET and the hinting task to examine ToM functions; future studies should include additional ToM tasks. Childhood trauma was measured retrospectively; nevertheless, the reliability of retrospective measurements of childhood trauma has been demonstrated.55 Not everyone who goes through trauma develops PTSD. Therefore, it could also be a possibility that those individuals who had lower ToM abilities at the time of the trauma were more prone to develop PTSD afterward.
Conclusions
Investigation of the relationship between ToM and various psychiatric disorders has gained attention in the last two decades. While most studies on ToM focus on autistic spectrum disorders or schizophrenia, research on PTSD has been increasing. Most research has focused on dysfunctional memory encoding or a deregulated hypothalamic-hypophyseal axis for understanding the pathophysiology of PTSD. This study is helpful in that it contributes to a better understanding of the pathogenesis of PTSD; moreover, it will be useful in the development of new treatment options for PTSD. Our research findings suggest that in addition to concentrating on traumatic events, the treatment and follow-up process for PTSD must also target deficiencies in cognitive and emotional capabilities.
Ethics approval and informed consent
This study was approved by the ethical committee of Uskudar University. The study conforms with the ethical principles of Helsinki Declaration for medical research with human subjects. Each patient gave written informed consent for the use of their medical data in the study.
Data availability
This manuscript is prepared from some of the findings of the master’s thesis of the first author. Data are in Turkish language. If needed, the data can be provided by the corresponding upon request by email.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Meijering B, van Rijn H, Taatgen NA, Verbrugge R. What eye movements can tell about theory of mind in a strategic game. PLoS One. 2012;7(9):e45961. doi:10.1371/journal.pone.0045961
2. Tager-Flusberg H, Sullivan K. A componential view of theory of mind: evidence from Williams syndrome. Cognition. 2000;76(1):59–90.
3. Vollm BA, Taylor AN, Richardson P, et al. Neuronal correlates of theory of mind and empathy: a functional magnetic resonance imaging study in a nonverbal task. Neuroimage. 2006;29(1):90–98. doi:10.1016/j.neuroimage.2005.07.022
4. Caputi M, Lecce S, Pagnin A, Banerjee R. Longitudinal effects of theory of mind on later peer relations: the role of prosocial behavior. Dev Psychol. 2012;48(1):257–270. doi:10.1037/a0025402
5. Slaughter V. Theory of mind in infants and young children: a review. Australian Psychologist. 2015;50(3):169–172. doi:10.1111/ap.12080
6. Blijd-Hoogewys EM, van Geert PL. Non-linearities in theory-of-mind development. Front Psychol. 2016;7:1970.
7. Laura M, Hiatt JGT, editor A cognitive model of theory of mind.
8. Morton A. Frames of Mind: Constraints on the Common-sense Conception of the Mental. New York (NY): Oxford University Press; 1980:174.
9. Nietlisbach Gabriela MA. Social cognition and interpersonal impairments in trauma survivors with PTSD. J Aggression Maltreatment Trauma. 2009;18(4):382–402. doi:10.1080/10926770902881489
10. Baron-Cohen S, Leslie AM, Frith U. Does the autistic child have a “theory of mind”? Cognition. 1985;21(1):37–46.
11. Baron-Cohen S, Wheelwright S, Hill J, Raste Y, The PI. “Reading the mind in the eyes” Test revised version: a study with normal adults, and adults with asperger syndrome or high-functioning autism. J Child Psychol Psychiatry. 2001;42(2):241–251.
12. Happe FG. An advanced test of theory of mind: understanding of story characters’ thoughts and feelings by able autistic, mentally handicapped, and normal children and adults. J Autism Dev Disord. 1994;24(2):129–154.
13. Lane RD, Quinlan DM, Schwartz GE, Walker PA, Zeitlin SB. The levels of emotional awareness scale: a cognitive-developmental measure of emotion. J Pers Assess. 1990;55(1–2):124–134. doi:10.1080/00223891.1990.9674052
14. Heavey L, Phillips W, Baron-Cohen S, Rutter M. The awkward moments test: a naturalistic measure of social understanding in autism. J Autism Dev Disord. 2000;30(3):225–236.
15. Dziobek I, Fleck S, Kalbe E, et al. Introducing MASC: a movie for the assessment of social cognition. J Autism Dev Disord. 2006;36(5):623–636. doi:10.1007/s10803-006-0107-0
16. Corcoran R, Mercer G, Frith CD. Schizophrenia, symptomatology and social inference: investigating theory of mind in people with schizophrenia. Schizophr Res. 1995;17:5–13.
17. Gil D, Fernández-Modamio M, Bengochea R, Arrieta M. Adaptation of the hinting task theory of the mind test to Spanish. Revista De Psiquiatría Y Salud Mental (English Edition). 2012;5(2):79–88. doi:10.1016/j.rpsmen.2011.11.002
18. Devine RT, Hughes C. Measuring theory of mind across middle childhood: reliability and validity of the silent films and strange stories tasks. J Exp Child Psychol. 2016;149:23–40. doi:10.1016/j.jecp.2015.07.011
19. Terr LC. Childhood traumas: an outline and overview. FOCUS. 2003;1(3):322–334. doi:10.1176/foc.1.3.322
20. Galea S, Tracy M, Norris F, Coffey SF. Financial and social circumstances and the incidence and course of PTSD in Mississippi during the first two years after Hurricane Katrina. J Trauma Stress. 2008;21(4):357–368. doi:10.1002/jts.20355
21. Hobfoll SE, Canetti-Nisim D, Johnson RJ, Palmieri PA, Varley JD, Galea S. The association of exposure, risk, and resiliency factors with PTSD among Jews and Arabs exposed to repeated acts of terrorism in Israel. J Trauma Stress. 2008;21(1):9–21. doi:10.1002/jts.20307
22. Cerda M, Tracy M, Galea S. A prospective population based study of changes in alcohol use and binge drinking after a mass traumatic event. Drug Alcohol Depend. 2011;115(1–2):1–8. doi:10.1016/j.drugalcdep.2010.09.011
23. McLaughlin KA, Berglund P, Gruber MJ, Kessler RC, Sampson NA, Zaslavsky AM. Recovery from PTSD following Hurricane Katrina. Depress Anxiety. 2011;28(6):439–446. doi:10.1002/da.20790
24. Cerda M, Paczkowski M, Galea S, Nemethy K, Pean C, Desvarieux M. Psychopathology in the aftermath of the Haiti earthquake: a population-based study of posttraumatic stress disorder and major depression. Depress Anxiety. 2013;30(5):413–424. doi:10.1002/da.22007
25. De Bellis MD, Zisk A. The biological effects of childhood trauma. Child Adolesc Psychiatr Clin N Am. 2014;23(2):185–222, vii. doi:10.1016/j.chc.2014.01.002
26. Leslie A, Friedman O, German T. Core mechanisms in ‘theory of mind’. Trends Cogn Sci. 2004;8(12):528–533. doi:10.1016/j.tics.2004.10.001
27. Fonagy P, Gergely G, Target M. The parent-infant dyad and the construction of the subjective self. J Child Psychol Psychiatry. 2007;48(3–4):288–328. doi:10.1111/j.1469-7610.2007.01727.x
28. Quide Y, Ong XH, Mohnke S, et al. Childhood trauma-related alterations in brain function during a Theory-of-Mind task in schizophrenia. Schizophr Res. 2017;189:162–168. doi:10.1016/j.schres.2017.02.012
29. Vasterling JJ, Brewin CR. Neuropsychology of PTSD: Biological, Cognitive, and Clinical Perspectives.1st. New York (NY): The Guilford Press; 2005.
30. Schmidt JZ, Zacharie R. PTSD and Impaired eye expression recognition: a preliminary study. J Loss Trauma. 2009;14:46–56. doi:10.1080/15325020802537096
31. Nietlisbach G, Maercker A, Rössler W, Haker H. Are empathic abilities impaired in posttraumatic stress disorder? Psychol Rep. 2010;106:832–844. doi:10.2466/PR0.106.3.832-844
32. Shenk CE, Putnam FW, Noll JG. Predicting the accuracy of facial affect recognition: the interaction of child maltreatment and intellectual functioning. J Exp Child Psychol. 2013;114:229–242. doi:10.1016/j.jecp.2012.08.007
33. Nazarov A, Frewen P, Oremus C, Schellenberg EG, McKinnon MC, Lanius R. Comprehension of affective prosody in women with post-traumatic stress disorder related to childhood abuse. Acta Psychiatr Scand. 2015;131:342–349. doi:10.1111/acps.12364
34. Nazarov A, Frewen P, Parlar M, et al. Theory of mind performance in women with posttraumatic stress disorder related to childhood abuse. Acta Psychiatr Scand. 2014;129(3):193–201. doi:10.1111/acps.12142
35. Germine L, Dunn EC, McLaughlin KA, Smoller JW. Childhood adversity is associated with adult theory of mind and social affiliation, but not face processing. PLoS One. 2015;10(6):e0129612. doi:10.1371/journal.pone.0129612
36. Mrizak J, Trabelsi R, Arous A, Aissa A, Ben Ammar H, El Hechmi Z. The relationship between childhood trauma and theory of mind in schizophrenia. European Psychiatry. 2016;33:S306.
37. van Schie CC, van Harmelen AL, Hauber K, Boon A, Crone EA, Elzinga BM. The neural correlates of childhood maltreatment and the ability to understand mental states of others. Eur J Psychotraumatol. 2017;8(1):1272788. doi:10.1080/20008198.2016.1272788
38. First MBSR, Gibbon M, Williams JBW. Structured Clinical Interview for DSM-IV Axis I Disorder, Clinican Version (SCID-CV). Washington (DC): American Psychiatric Press Inc; 1997.
39. AÖ Ç, Yıldız M, Köroğlu E. “DSM-IV Eksen I Bozuklukları (SCID-I) Için Yapılandırılmış Klinik Görüşme” Klinik Versiyon. Ankara: Hekimler Yayın Birliği; 1999.
40. Bernstein DP, Ahluvalia T, Pogge D, Handelsman L. Validity of the childhood trauma questionnaire in an adolescent psychiatric population. J Am Acad Child Adolesc Psychiatry. 1997;36(3):340–348. doi:10.1097/00004583-199703000-00012
41. ÖE ŞV, Eda İ. Validity and reliability of the Turkish version of childhood trauma questionnaire. Turkiye Klinikleri J Med Sci. 2012;32(4):1054–1063. doi:10.5336/medsci.2011-26947
42. Grassi-Oliveira R, Cogo-Moreira H, Salum G, et al. Childhood Trauma Questionnaire (CTQ) in Brazilian samples of different age groups: findings from confirmatory factor analysis. Plos ONE. 2014;9(1):e87118. doi:10.1371/journal.pone.0087118
43. Blake DD, Weathers FW, Nagy LM, et al. The development of a clinician-administered PTSD scale. J Trauma Stress. 1995;8(1):75–90.
44. Aker T, Özeren M, Başoğlu M, Kaptanoğlu C, Erol A, Buran B. Clinician-Administered Post-Traumatic Stress Disorder Scale (CAPS): a validity and reliability study. Turk Psikiyatri Derg. 1999;10(4):286–293.
45. Yıldırım EA, Kaşar M, Güdük M, Ateş E, Küçükparlak İ, Özalmete EO. Investigating reliability of reading mind in the eyes test in a Turkish population. Turk Psikiyatri Derg. 2011;22(3):177–186.
46. Sayin A, Oral N, Utku C, Baysak E, Candansayar S. Theory of mind in obsessive-compulsive disorder: comparison with healthy controls. Eur Psychiatry. 2010;25(2):116–122. doi:10.1016/j.eurpsy.2009.09.002
47. Dunmore E, Clark DM, Ehlers A. Cognitive factors involved in the onset and maintenance of posttraumatic stress disorder (PTSD) after physical or sexual assault. Behav Res Ther. 1999;37(9):809–829.
48. Daniels JK, Frewen P, McKinnon MC, Lanius RA. Default mode alterations in posttraumatic stress disorder related to early-life trauma: a developmental perspective. J Psychiatry Neurosci. 2011;36(1):56–59. doi:10.1503/jpn.100050
49. Lysaker PH, Dimaggio G, Wickett-Curtis A, et al. Deficits in metacognitive capacity are related to subjective distress and heightened levels of hyperarousal symptoms in adults with posttraumatic stress disorder. J Trauma Dissociation. 2015;16(4):384–398. doi:10.1080/15299732.2015.1005331
50. Lanius RA, Bluhm RL, Frewen PA. How understanding the neurobiology of complex post-traumatic stress disorder can inform clinical practice: a social cognitive and affective neuroscience approach. Acta Psychiatr Scand. 2011;124(5):331–348. doi:10.1111/j.1600-0447.2011.01755.x
51. Plana I, Lavoie MA, Battaglia M, Achim AM. A meta-analysis and scoping review of social cognition performance in social phobia, posttraumatic stress disorder and other anxiety disorders. J Anxiety Disord. 2014;28(2):169–177. doi:10.1016/j.janxdis.2013.09.005
52. Mazza M, Giusti L, Albanese A, Mariano M, Pino MC, Roncone R. Social cognition disorders in military police officers affected by posttraumatic stress disorder after the attack of An-Nasiriyah in Iraq 2006. Psychiatry Res. 2012;198(2):248–252. doi:10.1016/j.psychres.2011.11.027
53. Moran JM. Lifespan development: the effects of typical aging on theory of mind. Behav Brain Res. 2013;237:32–40. doi:10.1016/j.bbr.2012.09.020
54. Goldstein TR, Winner E. Enhancing empathy and theory of mind. Journal Cognit Dev. 2012;13(1):19–37. doi:10.1080/15248372.2011.573514
55. Tonmyr L, Draca J, Crain J, MacMillan HL. Measurement of emotional/psychological child maltreatment: a review. Child Abuse & Neglect. 2011;35(10):767–782. doi:10.1016/j.chiabu.2011.04.011
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.