Back to Journals » Journal of Healthcare Leadership » Volume 18
A Once-in-a-Generation Transformation at an Academic Public Hospital During Federal Funding Uncertainty
Authors Spellberg B, Coffey CE Jr, Bickley L, Ross W, Kaiser LR, Yee HF Jr
Received 10 January 2026
Accepted for publication 22 March 2026
Published 26 March 2026 Volume 2026:18 595146
DOI https://doi.org/10.2147/JHL.S595146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Zhanming Liang
Brad Spellberg,1,2 Charles E Coffey Jr,1,2 Liz Bickley,3 Warren Ross,3 Larry R Kaiser,4 Hal F Yee Jr5
1Hospital Administration, the Los Angeles General Medical Center, Los Angeles, CA, USA; 2Department of Medicine, University of Southern California, Los Angeles, CA, USA; 3Korn-Ferry, Inc, Los Angeles, CA, USA; 4The College of Physicians of Philadelphia, Philadelphia, PA, USA; 5Department of Medicine, University of California, San Francisco, CA, USA
Correspondence: Brad Spellberg, Los Angeles General Medical Center, 2051 Marengo Street, Los Angeles, CA, 90033, USA, Email [email protected]
Abstract: Fiscal and regulatory pressures on public hospitals and academic medical centers (AMC) will likely worsen in coming years, given looming changes to Medicaid and federal research funding. Recently, such pressures threatened to disrupt the 140-year affiliation between the Los Angeles General Medical Center (LA General) and the University of Southern California (USC). We sought to describe lessons learned during a two-year restructuring of this relationship, and to describe the impact of this transformation on patient care. Hospital-wide mortality metrics were extracted from the Vizient Clinical Database and Leapfrog hospital safety scores were retrieved from public releases. Citing increasing fiscal pressure, in March of 2023, USC noticed LA County that it was terminating the existing $170 million per year medical school affiliation agreement (MSAA) that funded > 90% of the clinical staffing at LA General. In response, LA General began a national hiring campaign to ensure sufficient staffing irrespective of the outcome of ongoing negotiations. In 21 months, LA General hired 273 physicians, dentists, and allied health professionals across all 19 clinical departments. Meantime, LA General and USC evolved a shared understanding that a blended model of employment best served both organizations. Such a dramatic transformation of workforce in such a short period of time raised concerns about risks to patients. We therefore monitored hospital-wide mortality rate and Leapfrog patient safety scores during the hiring process. However, hospital-wide observed and observed/expected mortality rates significantly declined the quarter after hiring began, and Leapfrog safety scores rose during the hiring period. Public hospitals and AMCs can strengthen their relationships despite ongoing fiscal and regulatory pressures via intentional organization restructuring and cultural transformation. Such transformational efforts may be all the more important at a time of great flux and uncertainty in government funding for clinical care and academic research.
Keywords: public hospitals, academic medical centers, staffing, culture change, quality improvement, patient safety
Introduction
From July 2023 through March 2025, a dramatic transformation occurred at the Los Angeles General Medical Center (LA General), one of the largest public hospitals in the US. In 21 months, LA General hired 273 doctors, dentists, advanced practice providers, and technical specialists as County government employees, replacing University contractors. This unprecedented pace of hiring enabled the hospital to fundamentally transform its culture while allowing its academic affiliate, the University of Southern California (USC), to improve its fiscal sustainability. Here we consider key lessons learned from this transformation, including approaches taken to recruitment and culture change, and outcomes achieved. These lessons may be particularly important in light of recent challenges regarding federal funding of Medicaid and academic research in the US.
Methods
As part of normal hospital operations, LA General regularly collects hospital-wide aggregated observed, expected, and observed/expected index mortality data from the Vizient Clinical Data Base, and receives hospital safety scores biannually from Leapfrog. Expected mortality was calculated by the Vizient database using proprietary algorithms, based on age and the total sum of ICD-10-CMs and procedural CPT codes captured for the patients. We assessed changes in these outcomes before and after hospital staffing changes via control charts, using standard methodologies.1 A statistically significant shift occurs when any datapoint crosses the upper or lower control limit, or 2 of 3 datapoints are in between the 95th percentile lines and upper or lower control limits. Per 45 Code of Federal Regulations Part 46, this study does not constitute human subjects research as there was no intervention or interaction with patients and no information was individually identifiable as no patient records were accessed.
Background for the Transformation
LA General and USC have been affiliated since 1885. Together, they jointly sponsor one of the largest graduate medical education (GME) training institutions in the US, with more than 1000 post-graduate physician and dentist trainees annually. Historically, nearly all attending staff at LA General were employed by the County of Los Angeles but had faculty appointments at USC. Due to a County fiscal crisis in 1987, >90% (~420/460) of the attending full time equivalent (FTE) staff at LA General switched to USC employment, funded by the LA County-USC Medical School Affiliation Agreement (MSAA). Since that time, University employed faculty split their clinical effort between LA General and the University Medical Center.
Between 2020 and 2022, due to growing concerns about on-site availability and quality of care supervision from some attendings, County hired approximately 60 physicians to replace University-contracted faculty in the LA General Departments of Anesthesia and Medicine. Subsequently in March of 2023, University and County leadership met to discuss ongoing fiscal, managerial, and compliance issues related to the MSAA. The County indicated a need for a cohort of physician and dental faculty who would be present full-time and embedded within the culture of LA General, to improve the quality and safety of patient care and resident supervision. In turn, the University indicated a need for more funding if they were required to provide facility-dedicated, full-time staffing. The University issued a notice of termination of the MSAA, triggering a difficult renegotiation for a new contract, during which the future staffing for the hospital became uncertain.
In response, the LA County Board of Supervisors passed a measure instructing and authorizing LA General to hire clinicians across all 19 clinical departments to ensure that irrespective of the outcome of negotiations, staffing at this critical, safety-net hospital would not be compromised at the end of the negotiation period.
The daunting task to potentially replace all 360 remaining University-employed FTE faculty at LA General began in July of 2023. The County contracted with one of the largest medical staffing firms in the US, Korn Ferry, to assist with recruitment of top tier talent.
Fortunately, negotiations on a new LA County-USC MSAA continued even while hiring was occurring. During these negotiations, the parties agreed that USC would provide faculty appointments to the attending staff the County hired, and in return the University would have input in selecting those faculty. The result was a more collaborative process in which the two parties recognized that a blended model would most likely optimize patient care, trainee supervision, and financial value to both the County and University. In this new, blended model, a majority of attending faculty (~380 FTEs, 80%) would be employed by the County, while a substantial minority (~100 FTEs, 20%) would remain University-employed.
The Hiring Process
Qualities Emphasized in Hiring
Throughout the hiring process, regular and direct engagement between Korn Ferry’s team and LA General leadership, including the Chief Medical Officer (CMO) and Associate CMO, was critical to candidate identification and selection. This collaborative process led to a mission statement explaining to prospective candidates the rationale behind this hiring initiative and why it was fundamental to the quality of care provided at the largest safety net hospital in the western US. A major focus of this mission statement was the concept that a once-in-a-generation transformation was underway at LA General, with a goal of improving quality, safety, and efficiency of care, while enhancing trainee supervision. We specifically and overtly messaged the desire to hire mission-driven individuals committed to serving the underserved and who wanted to help create and facilitate a new culture within this large, public, safety-net hospital.
One of the requirements for our vetting process was an understanding of the unique needs of a public hospital system. LA General is the largest level 1 trauma center in the US west of Texas, and has one of only 3 burn units in Los Angeles County. It offers complex quaternary care of virtually all types, with the exception of organ transplants. Approximately 80% of LA General’s patients are funded by Medicaid or are self-pay; less than 5% have commercial insurance. Primary care patients are assigned to LA General via a capitation model. Thus, our focus is on population-based managed care, proactively addressing health within the community to avoid emergency room visits, while simultaneously serving as the lodestone of the safety net, serving as the largest Level 1 Trauma Center and providing highly technically sophisticated emergency and inpatient care for the 10 million residents of the most populous County in the US.
We met multiple outstanding physician candidates who expressed a desire to build out subspecialized care models with the intent to bring in new patients from all over world to compete with the “top” programs in the US. While we enjoyed meeting those individuals, they were not the correct fit for our mission, purpose, or culture. Rather, we focused on hiring physicians who wished to participate as part of a robust team of experts whose mission was to provide the best care possible, at the highest quality and level of technical expertise, to the most Los Angelinos possible, with the fixed resources available. In short, our focus was on excelling in the fundamentals of population-based healthcare, while still providing extremely advanced emergency, intensive, and subspecialty care.
Our clear and firm focus on hiring individuals based on alignment with our mission and purpose proved to be very successful. Of the people we hired, none indicated that money was a substantive factor in their choice to join LA General; indeed, many took pay cuts. The common theme of our hires was the desire to provide outstanding care as part of a team that had a mission and purpose beyond their own needs—to be “part of something larger than myself”. One physician leader distilled their desire to join this cultural transformation thusly, “I want to play for a championship caliber team”.
Another common theme among the proceduralists and surgeons interviewed was amazement that their productivity would not be assessed based on work relative value units (wRVUs), and that clinicians would not be rewarded for doing more procedures on people simply to generate more wRVUs. On numerous occasions we heard variations of the question, “So, I would no longer have to do questionably necessary procedures on people to increase my RVUs?” Indeed, we answered, “Not only do you not have to, we do not want you to!” This was an important source of job satisfaction for prospective hires and underscored not only the unique healthcare system under which LA General operates, but the generally under-appreciated dark side of the fee-for-service health system that predominates elsewhere in the US.
Specialty Focus of Hiring
After extensive discussion, the County and University came to a shared realization that there was no advantage to University-employment for faculty who would be spending all of their time at the County hospital. The County recognized the advantages of having such individuals serve as the core of cultural transformation at LA General. For the University, there was no advantage to bearing the cost of salaries for such individuals, since they would have limited to no availability to generate additional variable revenue by working at the USC private health system across the street. Thus, full-time employment with the County made the most sense for such individuals going forward.
In contrast, for specific types of care with significant academic subspecialization (eg, Surgical Specialties, Dermatology, Pathology), the County did not have the need for a full-time position. For such subspecialized areas, it made both economic and clinical sense for the County to contract that work to University-employed physicians. This was particularly true for some specific clinical Departments in which University leadership had demonstrated a consistent track record of true partnership and a recognition of the importance of the affiliated relationship for both parties (eg, Surgery, Orthopedic Surgery, Dermatology, Neurosurgery, Emergency Medicine). For the University, the advantage of maintaining a contracted employment model was that such individuals could participate part-time in the teaching and complex patient care at the County hospital, while still generating wRVUs and covering the majority of their compensation at the private University health system.
Cultural Transformation
Previously, the incentives for providers and management were mis-aligned within the MSAA. Contracted physicians needed to generate the majority of their compensation via work at the USC private health system. As a result, there was little collaboration between these individuals and staff at LA General, and it was very difficult for them to participate in hospital-wide quality and safety initiatives. Changing the employment model, and the subsequent hiring of 273 clinicians by the County, facilitated the realignment and culture change that all parties needed.
In parallel, LA General physician leadership recognized that it was critical to establish a new cultural framework while onboarding such a large, new workforce. During hiring, LA General leadership dialogued with candidates about the type of workplace environment they wanted to be part of. In February of 2024, LA General began holding quarterly town halls for County-employed attending staff, with both in person and virtual attendance options. Those who had been hired but had not yet started their employment were included.
Extensive staff dialogue leading up to the inaugural town hall had resulted in 10 proposed foundational principles behind LA General’s cultural transformation (See Supplemental Materials). After discussion, the attendees agreed that these points would not be viewed as platitudes, but would rather serve as our True North—our guiding principles for how we would interact with one another. Multiple participants expressed gratitude at the opportunity to have a voice in our transformation, in contrast with their prior work experience. We continue to hold these town halls on a quarterly basis to enable sustainment of this cultural transformation.
The culture change was palpable immediately, even during the rolling onboarding process for new staff. Nurses, social workers, clerks, administrators, and clinical staff across the hospital commented on how engaged and collaborative the new hires were. These comments were and still are being made regularly in meetings with executives, at the hospital’s weekly all-employee virtual town hall, and as casual comments made while walking down the hallways. We have even had patients and family members write letters to hospital leadership expressing surprise and gratitude at the degree of teamwork they witnessed between physicians of different specialties, specifically noting that they had not experienced this type of teamwork at other hospitals.
Healthcare Performance
A predominant concern was the potential for patient harm to result from chaos and confusion triggered by such a substantial staff turnover over such a short time. We therefore monitored hospital mortality rates and patient safety scores before and after the intervention as balancing measures to assess impact on hospital care.
During the 21-month period of staff hiring, hospital observed mortality significantly declined (Figure 1). Expected mortality remained stable (Figure 1), such that Observed over Expected (O/E) Index Mortality fell significantly to its lowest level (Figure 1). There was no concurrent significant change in number of hospital discharges per quarter.
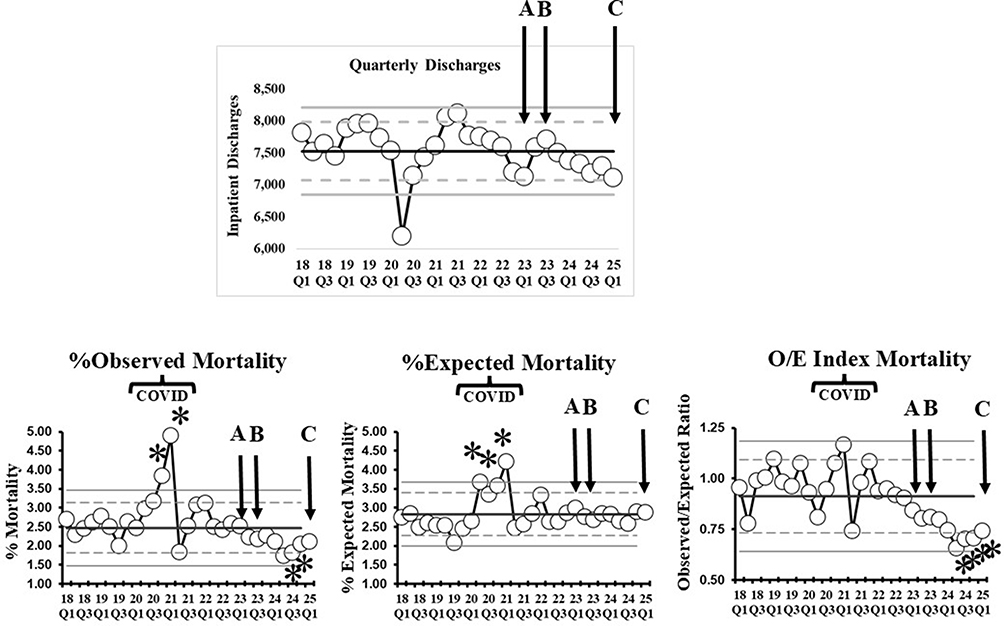 |
Figure 1 Mortality Rate by Quarter at LA General. Source: Author’s own analysis, with data taken from the Vizient Clinical Database (https://www.vizientinc.com/Member-login). Control charts demonstrate quarterly, hospital-wide, LA General Observed, Expected, and O/E (Observed/Expected) Index Mortality. Brackets denote unusual mortality rates due to the COVID-19 pandemic. Arrows labeled A indicate the quarter in which USC noticed County it was terminating the affiliation agreement to trigger renegotiation. Arrows labeled B indicate the quarter in which the County began its aggressive hiring. Arrows labeled C indicate the quarter that County hiring ended. Negotiations for a new affiliation agreement continued from the period of Arrow A through Arrow C. Control lines include the mean (central solid line), 95th percentiles (dashed lines), and upper and lower control limits (highest and lowest solid lines). *A statistically significant shift occurs when any datapoint crosses the upper or lower control limit, or 2 of 3 datapoints are in between the 95th percentile lines and upper or lower control limits. |
To assess patient safety beyond mortality, we tracked the Medical Center’s Leapfrog safety grades. Leapfrog is an independent organization that provides aggregated patient safety grades to acute care hospitals in the US. They combine publicly reported data regarding rates of hospital acquired infection, pressure ulcers, falls with injury, retained foreign bodies, post-operative complications, and other metrics, to provide safety grades for participating hospitals. These grades are released twice annually, in the spring and fall. During the years preceding the hiring period, LA General consistently achieved a C grade from Leapfrog, with a brief period of a D grade (Figure 2). During the first six months of the hiring period, the hospital achieved a B grade for the first time since 2016. During the remaining period, the hospital achieved and maintained an A grade for the first time in its history (Figure 2).
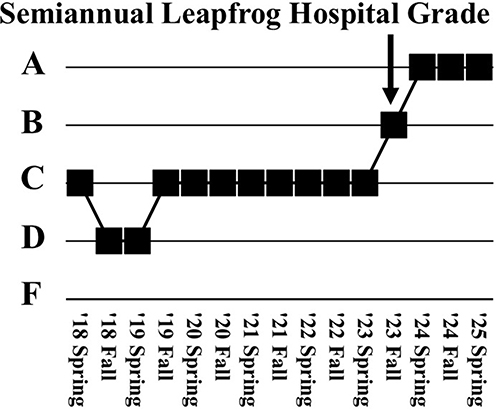 |
Figure 2 Leapfrog Patient Safety Grades for LA General Since 2018. Source: Author’s own analysis. Leapfrog releases updated safety grades twice annually, in the Spring and Fall. The scores encompass a variety of patient safety indicators, such as hospital acquired infection rates, pressure ulcers, falls with injury, retained foreign bodies, etc. The arrow demonstrates the quarter in which County hiring began to replace contracted workforce. |
Thus, after the staffing intervention, not only was there no increase in mortality or fall in safety scores, LA General achieved significant improvement in hospital-wide mortality and safety scores. As these data are observational in nature, we cannot demonstrate causality of these outcomes changes resulting from the staffing change. Nevertheless, the primary point was to exclude patient harm, and we found no evidence of harm resulting from the staffing change.
Conclusions
Many of the leading public safety net hospitals in the US have undergone substantial restructuring of their financial and administrative relationships with their University affiliates in recent years.2–4 Several factors have predominantly driven such restructuring. The continuing challenge of providing high quality inpatient care along with more stringent requirements regarding supervision of post-graduate resident physicians, and increasingly complex payor billing rules, all demand substantially enhanced attending physician presence and involvement. Meanwhile, University health systems are under increasing financial pressure due to competition with private health systems,5 pressure on extramural grant funding,6,7 and narrowing financial margins generated by medical schools.8 The aggregate effect has forced Universities to find increased funding to recruit and retain faculty members who provide services at affiliated hospitals.
As a result, staffing models have evolved at public hospitals, ranging from virtually all physicians and dentists employed by the University academic affiliate(s) (for example, Zuckerberg San Francisco General Hospital and Trauma Center), to the large majority employed by the public hospital (for example, Harbor-UCLA Medical Center), to hybrid models in between. LA General has now experienced the full spectrum of these models.
We believe that the LA General experience illustrates the importance of several fundamental management principles.
First, historical norms should not guide how an institution’s workforce is organized. Rather, the institution’s needs and priorities should be the guiding force. If the workforce structure is mal-aligned, then the staffing model should be changed.
Second, the culture of an organization can be dramatically transformed via an intentional effort, which includes input from frontline staff of desired changes, a purposeful selection of personnel who are aligned with the new culture, and demonstration by leadership that the principles upon which transformation is based upon are not platitudes, but actually True North guiding principles.
Third, to get “the right people in the right seat on the bus”,9 alignment with the mission of the organization takes precedence over compensation. Money was not the primary motivator of the people who joined us. We made clear who we were, why we existed, and what our mission was up front. That clear message enabled us to recruit people specifically aligned with that mission and purpose.
Korn Ferry’s recruitment support was instrumental in achieving the outcomes of LA General’s workforce transformation. By leveraging a deep understanding of the healthcare labor market and employing innovative strategies, and working closely with hospital leadership, Korn Ferry not only helped to fill the roles but also ensured that each hire aligned with LA General’s mission and cultural vision. The rapid implementation of recruitment processes, combined with tailored sourcing strategies and white-glove support, enabled LA General to maintain continuity in patient care while simultaneously transforming its organizational culture. This partnership underscored the importance of strategic recruitment in driving both operational excellence and long-term cultural change, serving as a critical factor in the hospital’s success.
Finally, while academic mission and patient care are sometimes at odds with one another, they share critically important common ground. Medical schools require access to patients for teaching and research. In turn, the availability of faculty appointments for attending staff, the presence of trainees, and availability of other scholarly support (eg, medical library access, Institutional Review Boards, grants and contracts office) helps affiliated medical centers recruit and retain top clinical talent. Nevertheless, for academic medical centers, scholarly work cannot be prioritized over patient care and education. The key is balance, to maximize the overlap where the academic and clinical milieus are in alignment and support each other, while minimizing detracting conflict. We believe a blended employment model facilitated achieving that balance at LA General and USC.
Although LA General has a distinct payor mix and mission compared to many other hospitals, we believe our experience can inform others who wish to undergo their own transformation, for the betterment of the patients and communities they serve, their workforce, and their trainees. Such transformational efforts may be all the more important at a time of great flux and uncertainty in federal funding for clinical care and academic research.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Carey RG, Lloyd RC. Measuring Quality Improvement in Healthcare. Milwaukee: Quality Press; 2001.
2. Administrator d. Parkland-UT Southwestern divide threatens patient care. The Dallas Morning News. Available from: https://www.dallasnews.com/news/investigations/2013/02/10/parkland-ut-southwestern-divide-threatens-patient-care/.
3. Chang D. Jackson approves UM agreement. The Miami Herald. Available from: https://www.miamiherald.com/news/local/community/miami-dade/article1964525.html/.
4. Friedman E. The Boston City hospital: a tale of three cities. Massachussetts Medical Society. Available from: https://www.massmed.org/About/MMS-Leadership/History/The-Boston-City-Hospital--A-Tale-of-Three-Cities/.
5. Levin E, Malani R, Odden A, Schulz J. Ensuring the financial sustainability of academic medical centers. McKinsey and Company. Available from: https://www.mckinsey.com/industries/healthcare/our-insights/ensuring-the-financial-sustainability-of-academic-medical-centers#/.
6. Sekar K. National institutes of health (NIH) funding: FY1996-FY2025. Congressional Research Service. Available from: https://crsreports.congress.gov/product/pdf/R/R43341#:~:text=Excluding%20ARPA%2DH%2C%20the%20inflation,peak%20level%20%2D2.7%25.
7. Kozlov M, Exclusive MS. NIH to terminate hundreds of active research grants. Nature. 2025;639(8054):281–7. doi:10.1038/d41586-025-00703-1
8. Bannow T. Hospitals have been financially propping up medical schools, but now it’s squeezing their bottom lines. STAT. Available from: https://www.statnews.com/2022/04/14/hospitals-medical-schools-financial-relationship-tension-squeezing-bottom-line/.
9. Collins J. Good to Great: Why Some Companies Make the Leap. and Others Don’t. Harper Business; 2001.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Systematic Literature Review of Safety Culture in Hemodialysis Settings
Albreiki S, Alqaryuti A, Alameri T, Aljneibi A, Simsekler MCE, Anwar S, Lentine KL
Journal of Multidisciplinary Healthcare 2023, 16:1011-1022
Published Date: 11 April 2023
Tracing Missing Surgical Specimens: A Quality Improvement Strategy for Adverse Events Based on Root Cause Analysis
Huang LL, Yang JH, Hong WW, Wang BL, Chen HF
Risk Management and Healthcare Policy 2025, 18:2139-2150
Published Date: 27 June 2025