")
Back to Journals » Advances in Medical Education and Practice » Volume 9
Are we on the right track? Answers from a national survey of Thai graduates’ perceptions during the transition to the 6-year PharmD program
Authors Suttajit S , Suwannaprom P , Supapaan T, Eakanunkul S, Tangkiatkumjai M, Kongkaew C , Anderson C , Wongpoowarak P
Received 4 May 2018
Accepted for publication 16 July 2018
Published 27 September 2018 Volume 2018:9 Pages 713—722
DOI https://doi.org/10.2147/AMEP.S173014
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Siritree Suttajit,1 Puckwipa Suwannaprom,1 Teeraporn Supapaan,2 Suntara Eakanunkul,3 Mayuree Tangkiatkumjai,4 Chuenjid Kongkaew,5 Claire Anderson,6 Payom Wongpoowarak7
1Department of Pharmaceutical Care, Faculty of Pharmacy, Chiang Mai University, Chiang Mai, Thailand; 2Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Ubon Ratchathani University, Ubon Ratchathani, Thailand; 3Department of Pharmaceutical Sciences, Faculty of Pharmacy, Chiang Mai University, Chiang Mai, Thailand; 4Department of Clinical Pharmacy, Faculty of Pharmacy, Srinakharinwirot University, Nakhon Nayok, Thailand; 5Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Naresuan University, Phitsanulok, Thailand; 6Division of Pharmacy Practice and Policy, School of Pharmacy, University of Nottingham, Nottingham, UK; 7Department of Clinical Pharmacy, Faculty of Pharmaceutical Sciences, Prince of Songkla University, Songkhla, Thailand
Purpose: To serve the higher demands of pharmaceutical services, pharmacy education in Thailand has shifted from 5-year BPharm program to 6-year PharmD program with two specialization tracks: pharmaceutical care (PC) and industrial pharmacy (IP). This study aimed to compare the perceptions regarding professional competencies, pharmacy profession, and planned workplace between graduates with 5-year BPharm and 6-year PharmD and between those with PC and IP specialty.
Methods: A cross-sectional national survey using a paper–pencil self-administered questionnaire was distributed to all new graduates attending the pharmacy licensure examination in March 2015.
Results: Of all 1,937 questionnaires distributed, 1,744 were returned and completed (90% response rate). Pharmacy graduates rated highest on their competencies in professional ethics, followed by PC services and system management. They rated low confidence in medication selection procurement and pharmaceutical industry competencies. The 6-year PharmD graduates showed higher confidence in ethics and professional pride than the 5-year BPharm graduates. Graduates with PC specialty rated higher perceived competency in PC, system management, primary care, and consumer protection domains, while the IP graduates were superior in IP and medication selection and procurement domains, and most graduates (PC and IP) intended to work mainly in a hospital or a community pharmacy. Hospital was preferred for the PC graduates, and the IP graduates were more likely to work in pharmaceutical industry, regulation and consumer protection, sales and marketing, and academia.
Conclusion: With some gaps still to be filled, the transition from 5-year BPharm to 6-year PharmD program with specialty tracks gave extra confidence to graduates in their specialty competencies and professional pride, leading to differences in preferred workplace. The findings of this study reflect that Thai pharmacy education continues to adjust to the needs of the society and the changing health care environments. Longitudinal monitoring to observe this transition is needed for both curriculum adjustment and competency of the graduates.
Keywords: attitude, pharmacy education, PharmD curriculum, competency, transition, Thailand
Introduction
Health care systems around the world have continuously transformed to serve the changing needs of societies, and countries were encouraged to constantly develop the pharmaceutical workforce to serve these changes.1 In the United States, pharmacy education has shifted to offer PharmD degree as the only entry-level degree, while pharmacy education in South Korea has expanded from 4 to 6 years in response to a new law enacted that requires all prescriptions filled at a pharmacy by pharmacists.2,3
Similarly, a demand for high-quality health care services in Thailand requires pharmacists to have better clinical skills to be a part of the health care team, especially in the hospital setting,4 as well as in the community setting where newly endorsed Good Pharmacy Practice (GPP) regulation require an on-duty pharmacist in all new community pharmacies that are opened after June 2014.5,6 In addition, health care reform and the universal coverage scheme result in increased health care service utilization.7 Thus, pharmacists have expanded their responsibilities for ensuring rational drug use, developing medication systems to guarantee effective medication use under policy constraints,8 and conducting proactive health promotion services for primary health care delivery. With the diverse roles and huge responsibilities of Thai pharmacists along pharmaceutical supply chains,4,9,10 it is very challenging to develop a pharmacy curriculum to meet with all the needs.
Thai pharmacy education has transitioned from having two entry-level degrees – a 5-year Bachelor of Pharmacy (BPharm) (with three main tracks: pharmaceutical care [PC], pharmaceutical sciences, and social and administrative pharmacy) and a traditional 6-year Doctor of Pharmacy (PharmD) (PC) program – to a single national 6-year PharmD program (including PC and industrial pharmacy [IP] tracks).4,11 The Pharmacy Council of Thailand mandated that in 2014, marking the 100th year of pharmacy education in Thailand, all Thai entry-level pharmacy curricular will be only a 6-year PharmD program. It is believed that this shift will prepare pharmacy graduates with competencies as a specialist not a generalist to serve the demands of the job market.4,12
In general, the structure of the curriculum comprises the first year for general education, the second year for basic sciences and preclinical courses, the third year for core professional courses, the fourth and fifth years for professional specialty courses, and the sixth year for professional clerkships.13 There are two specialty tracks, namely IP and PC. However, three groups of courses are normally applied for both tracks, but in different proportions. The courses in IP group are product oriented and prepare students for competencies in formulation, quality control, medicinal chemistry, and manufacturing. The PC courses are patient oriented and intended to train students in patient care, while courses in social and administrative pharmacy focus in system management and pharmaceutical public health.4,13
It is necessary to observe whether the Thai pharmacy education transition from a 5-year BPharm program to a 6-year PharmD program with specialty tracks will meet the needs of the country’s health care environments. Chanakit et al11 conducted a qualitative research on the perceptions of stakeholders on the transition to all PharmD programs in Thailand. The majority of stakeholders in the PC area agreed that the transition was a step-up for the profession from being generalists to specialists. PharmD graduates were able to provide high-quality patient care and work with other health care professionals. However, some employers were concerned that the PC competencies were seemingly matched with tertiary hospital settings, but did not meet the needs of primary care and community care settings.11 Regarding the IP track, employers reported that the graduates lacked research skills required for pharmaceutical product development.11
Previous research has mainly focused on societal perspective on the curricular transition,11,14 and there has been limited research exploring the perspective of the graduates themselves. A previous study that observed self-reported competency across Thai pharmacy education programs was limited to a subgroup of graduates from a public university who enrolled in the public service program of the Ministry of Public Health,15 and thus, the reported competencies were more likely to focus on the area of PC only while this research aimed to survey both PC and IP.
The objectives of this research were to compare perceptions regarding professional competencies, pharmacy profession, and planned workplace between the 5-year BPharm and the 6-year PharmD graduates and among graduates with PC track and IP track. This research was the first national survey conducted after pharmacy students completed the program by 2014 academic year, which was when the first year of all 6-year PharmD program was mandated. After 2015, there were only 6-year PharmD graduates. The findings reflect a transition of pharmacy education and serve as an input for reconstruction and advancement of pharmacy education in response to the shift of roles and responsibilities of pharmacy practices.
Materials and methods
Study design and target population
This study was a cross-sectional national survey, distributed during the academic year 2014 national pharmacy licensure examination (March 2015) at all 12 test centers around Thailand. Respondents were pharmacy graduates who registered for the examination (n=1,937), representing graduates from 17 universities all around the country in the academic year 2014.
Questionnaire development
Data were collected through a paper–pencil self-administered questionnaire, which composed of four parts. Part 1 assessed participants’ gender, university, grade point average (GPA), study plan (5-year or 6-year program), specialty tracks (PC or IP), and planned workplace. Part 2 asked participants about their perceived professional core competency assessed by six domains (35 items); for example, domain 1 assessed professional ethics (three items), domain 2 PC services (seven items), and so on. The six domains (35 items) of professional core competencies are shown in Table 1. Respondents were asked to rate their level of confidence in performing tasks according to Thai pharmacy professional core competency framework, announced by the Pharmacy Council of Thailand in 2012.15,16 Part 3 assessed self-perception of eight soft-skills (eg, apply knowledge and skills in real-world practice, life-long learning, English skill), developed from a previous study.17 Part 4 assessed their perception of pharmacy profession and curriculum (eg, contribution of pharmacy profession toward patients’ health, 6-year program worth for future career) (Table 2). Parts 2–4 were assessed by a 5-point Likert-type scale, where score 5=strongly agree and 1=strongly disagree.
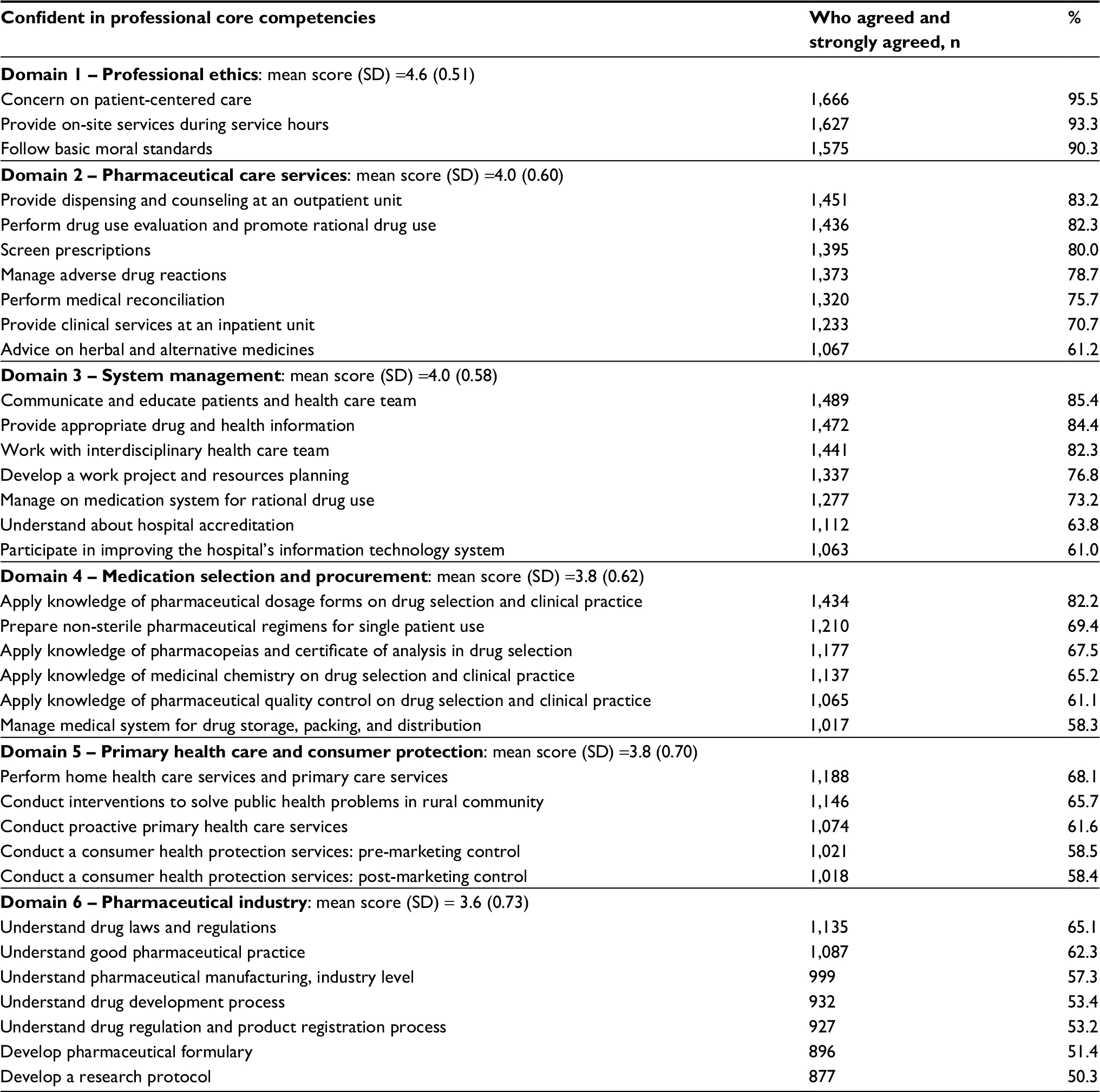 | Table 1 Perceived professional core competencies (six domains) of Thai pharmacy graduates (N=1,744) |
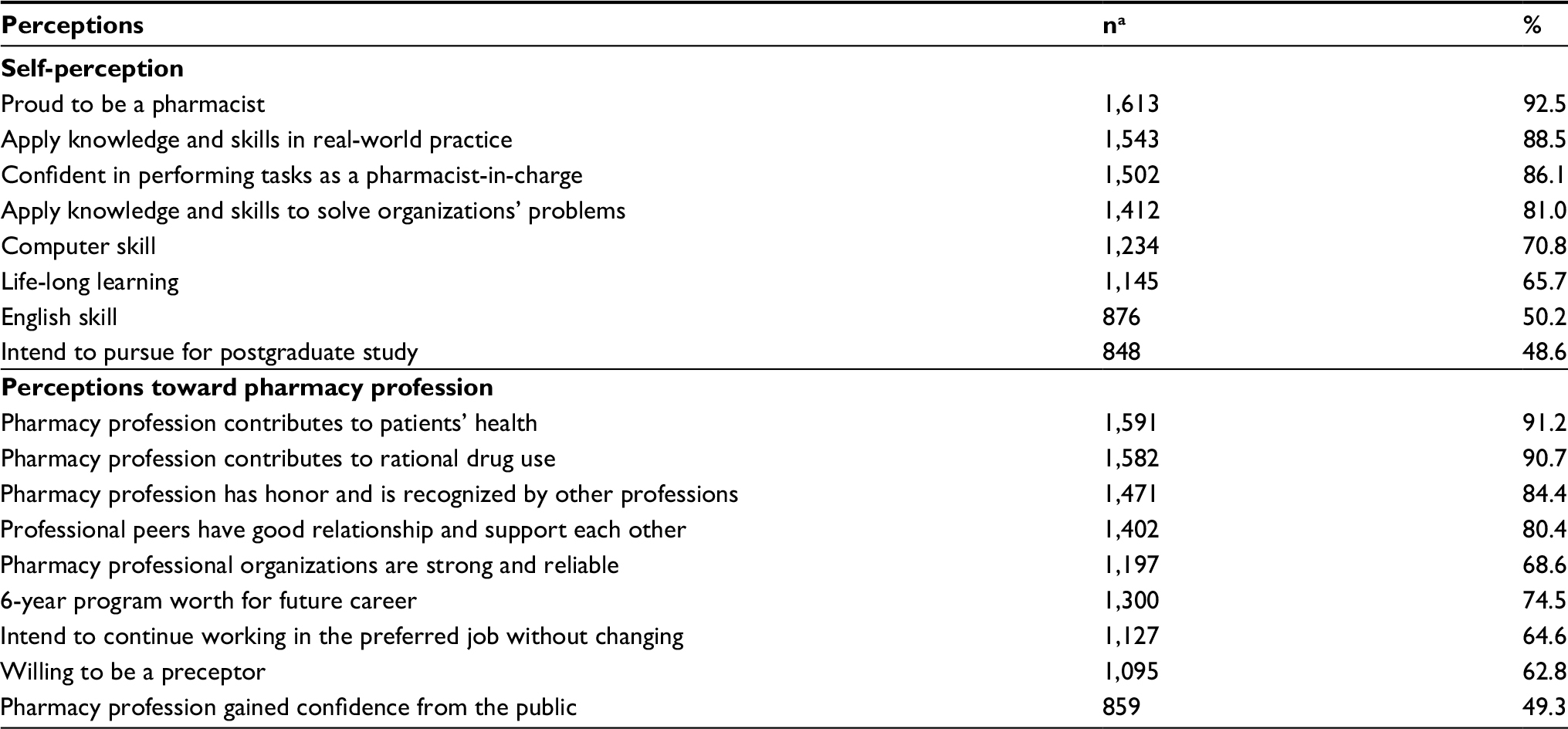 | Table 2 Respondent self-perception and perceptions toward pharmacy profession (N=1,744) Note: aThose answered 4 (agree) and 5 (strongly agree) in 5-point Likert scale. |
The questionnaire was reviewed for content validity by three faculty staff with more than 10 years of teaching experiences from three different pharmacy schools. After the questionnaire was revised with respect to received recommendations, it was pretested by the fifth year PharmD students from a public university who completed all course requirements and were qualified to take professional clerkship rotations. The overall internal consistency of 35-item perceived professional competency was 0.960, assessed by Cronbach’s alpha coefficient. Using factor analysis to discover patterns of relationship between the 35 items, perceived professional competencies could be grouped into six domains, including professional ethics, system management, medication selection and procurement, PC, primary health care and consumer protection, and pharmaceutical industry. The internal consistency for each factor was 0.766, 0.893, 0.876, 0.918, 0.913, and 0.925, respectively.
Data collection
The researchers introduced the research protocol to the Pharmacy Council of Thailand, the Pharmacy Education Consortium of Thailand, and asked the dean of every pharmacy school for cooperation to distribute the survey. During the period when the participants prepared for the objective structured practical examination, the research team introduced the project and informed that the participation would be anonymous and voluntary before leaving the room. The completion and returning of the questionnaire were implied to be informed consent. Those who were willing to participate filled out the questionnaire and put it in a designated box. It took about 15 minutes to complete the questionnaire.
Statistical analysis
Data were entered and analyzed by SPSS/Win version.17.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics was used. For the 35-item professional competency, principal component analysis with varimax rotation and eigenvalue ≥1.0 was used for data reduction (Table S1). To compare between 5-year BPharm and 6-year PharmD graduates, and among graduates with PC track and IP track on their perceptions toward their competency, pharmacy profession and preferred workplace, perceptions on the 5-point Likert scale were grouped into two groups, score 4–5 = confidence and score 1–3 = diffident. Multivariable logistic regression was later used to control the effects of gender, GPA, and types of university (public or private). Assumptions of multiple logistic regression were met. Statistical significance was set at a P-value of 0.05.
Ethics approval
The study protocol was approved by the institutional review board of Ubon Ratchathani University on July 26, 2013. The research team followed the protocol to ensure the participants’ risk protection. All participation was anonymous and voluntary. Data were stored within the researchers’ encrypted, password-protected computers in a locked office. Only the researchers could access the data. No incentive was provided for participation.
Results
Respondent characteristics
Of all 1,937 questionnaires distributed, 1,778 were returned, in which 34 responses were incomplete. Only 1,744 were used in data analysis (90% response rate). Respondent characteristics are presented in Table 3. The majority was female with 6-year PharmD degree in PC track.
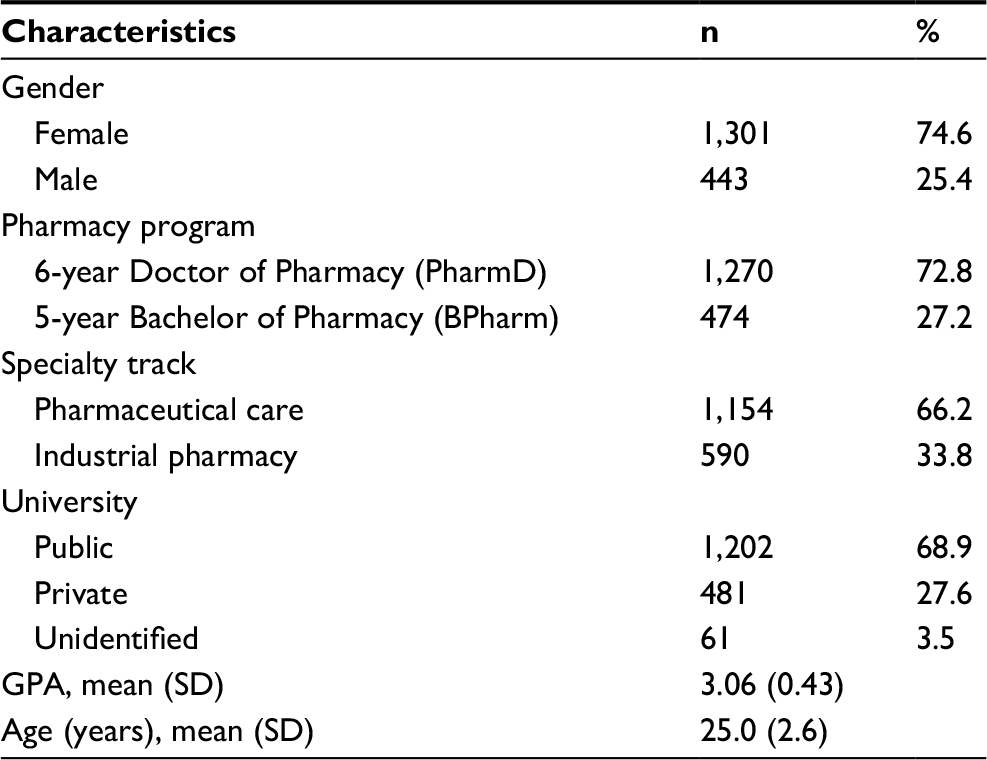 | Table 3 Respondent characteristics (n=1,744) Abbreviation: GPA, grade point average. |
Perceived professional core competency
Respondents were asked to rate their level of confidence in performing tasks required as pharmacy core professional competencies, and factor analysis categorized the 35 items into six domains (Table 1). The respondents rated their competency regarding professional ethics the highest, followed by providing PC for individual patient and system management. Confidence in performing competencies related to medication selection and procurement was low as well as for primary health care and consumer protection. The competency regarding pharmaceutical industry was rated the lowest (Table 1), which might be due to the smaller proportion of graduates from IP track.
Self-perception and perceptions toward pharmacy profession
Apart from the professional core competency, the results reflected high professional pride in these graduates (Table 2). They were proud to be a pharmacist and confident in acting as a pharmacist-in-charge and strongly believed that the pharmacy profession contributes to public wellness. However, the graduates perceived that the pharmacy profession did not gain much recognition from the public. In graduates’ view, it is worth holding a 6-year PharmD degree, but only half of them intended to pursue further study, and they lacked confidence in some core competencies like life-long learning skill and English skills (Table 2).
Planned workplace
The majority of the graduates planned to work as a hospital pharmacist or a community pharmacist. A medical representative for a pharmaceutical company and an industrial pharmacist were less popular, but still a higher choice than being a university lecturer or a regulator for consumer health protection (Table 4).
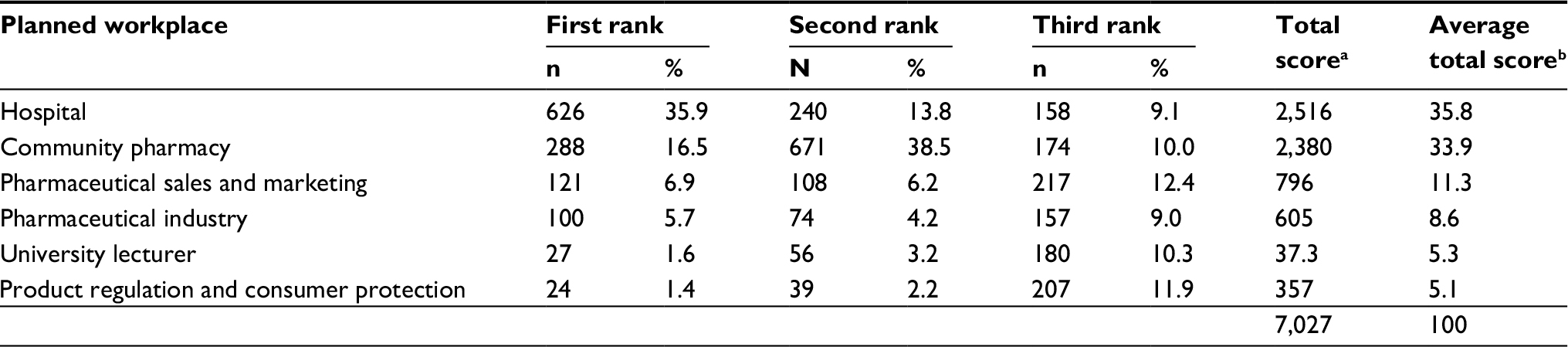 | Table 4 Graduates’ planned workplace Notes: aTotal score = (n of first rank × 3) + (n of second rank × 2) + (n of third rank × 1). bAverage total score = total score × 100/sum of total score. |
Five-year BPharm program vs 6-year PharmD program
Table 5 highlights the differences in pharmacy graduates during the transition from the 5-year BPharm to the 6-year PharmD program with two specialty tracks. Comparing perceived professional competency between the programs, it was found that the 6-year PharmD tended to be more confident than the 5-year BPharm graduates, but the only significant difference observed was the professional ethics domain. The 6-year PharmD graduates also showed higher pride in the pharmacy profession and valued a year longer in a 6-year program. In addition, the 6-year PharmD graduates’ preference to work in pharmaceutical industry was significantly greater than the BPharm graduates (Table 5).
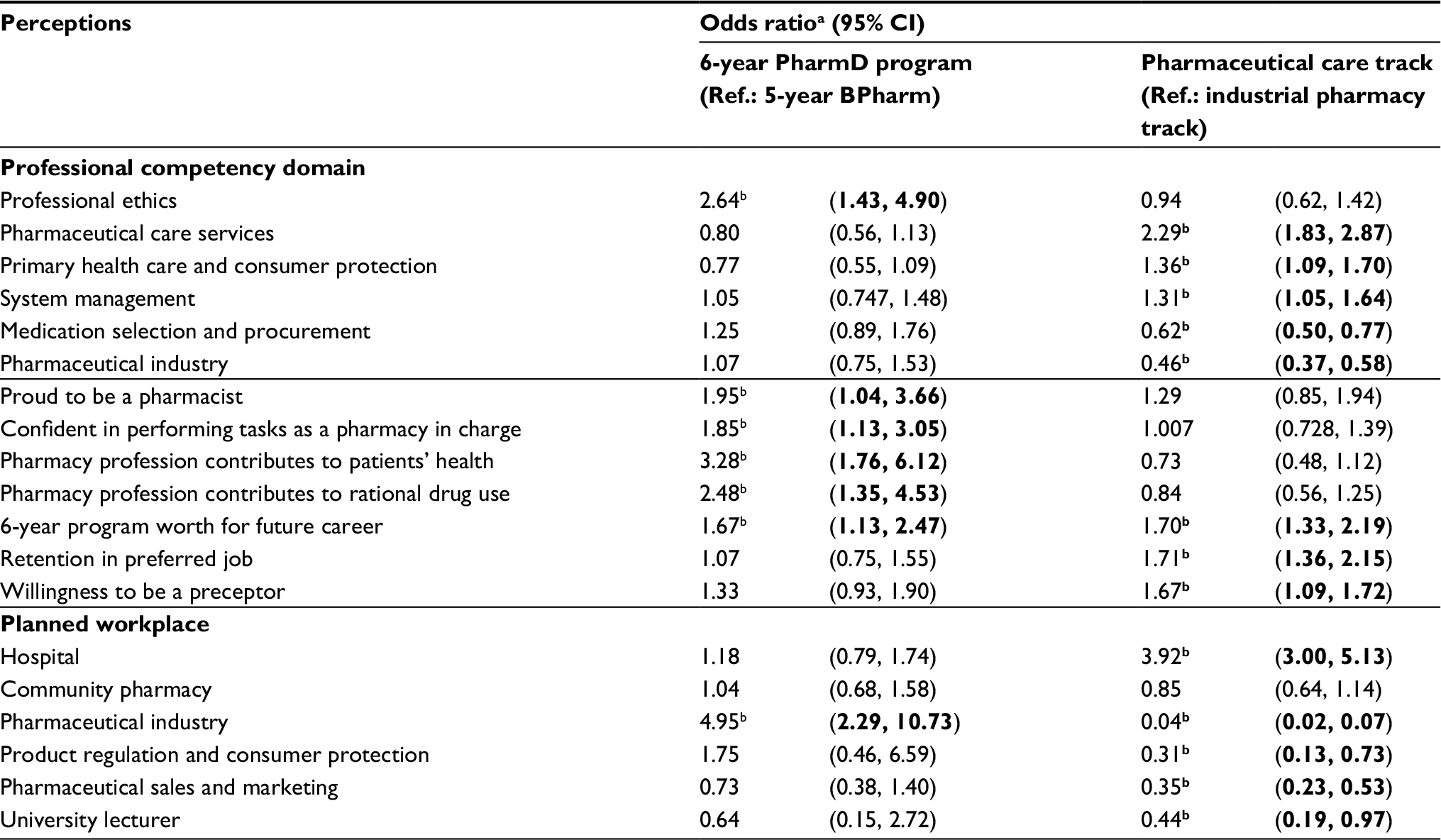 | Table 5 Differences in perceptions and planned workplace of graduates from 5-year BPharm to 6-year PharmD program with specialty tracks Notes: aAdjusted for gender, GPA, academic program (5-year BPharm or 6-year PharmD), specialty track (pharmaceutical care or industrial pharmacy), type of university (public or private). bStatistically significant at P<0.05. All bold odds ratio’s are statistically significant. Abbreviation: GPA, grade point average. |
While differences in professional core competency were not explicit between the two programs, specialty tracks did reflect the differences. The graduates in different specialty tracks were confident in different domains of professional core competency and also preferred different workplace. The graduates of the PC track had significantly higher confidence perceived competency in the domains of PC services, system management, primary care, and consumer protection. Thus, they were more likely to plan to work in a hospital than those of the IP track. The graduates of the PC track also valued the 6-year program more and had higher commitment to retain their preferred job and be a preceptor in the future (Table 5).
On the other hand, the graduates with IP specialty had significantly higher perceived competency in two domains: medication selection and procurement and IP activities. They strongly preferred to work in a pharmaceutical manufacturing company than those of another track (OR 25.64, 95% CI 13.51, 50.0). They also planned to work in the area of product regulation and consumer protection, sales and marketing for a pharmaceutical company, and in pharmacy education more than the graduates from PC track. However, a community pharmacy was a preferred workplace for all graduates regardless of the area of specialty (Table 5).
Discussion
This study was the first national survey of perceived professional competency among Thai pharmacy graduates during the transition from having two entry-level degrees (5-year BPharm and a traditional 6-year PharmD) to a single national 6-year PharmD curriculum. The main objectives of expanding the pharmacy curriculum were to advance pharmacy competency from a generalist to a specialist and to meet the demands of the current job market. To produce a specialist, a curricular structure of a 6-year PharmD program has increased credits for professional courses and clerkships. To meet the demand of the job market, the 6-year PharmD program offers three specialty tracks, including PC, IP, and consumer health protection (the latter was launched in 2013, and there are no graduates from this track yet).4,13
Transition from 5-year BPharm to 6-year PharmD program
The findings of this study revealed that the transition from 5-year BPharm to 6-year PharmD program with specialty tracks increased the confidence of the graduates (Table 5). Two key findings are as follows: 1) 6-year PharmD program boosted graduates’ professional pride while retaining their confidence in performing basic professional tasks; and 2) having the specialty tracks formed confidence in the specific domain of professional competency for the graduates and led to different preferences in job selection.
From a generalist to a specialist
For the first key finding, although graduates from the 5-year and 6-year programs were not significantly different in their confidence in performing professional tasks, the 6-year PharmD graduates showed significantly higher confidence in domains related to professional ethics and greater professional pride than the 5-year BPharm graduates. This might be due to PharmD students spending more time working in real-world practice, both during their clinical years in school and an additional year of experiential learning through 6–7 professional clerkships. Nemire and Meyer supported the notion that experiential education allows students to develop foundation skills (eg, professionalism and ethics), which are essential for being pharmacists.18,19 Pharmacy schools have had the opportunity to introduce earlier exposure to pharmacy practice. Although there was no significant difference in professional competency between the 5-year BPharm and 6-year PharmD graduates, it should be noted that the time of survey being conducted during the national licensing examination might lead to the similar range of confidence in all graduates since they needed to prepare themselves to meet the same minimal standard of professional core competency established by the Pharmacy Council of Thailand.
For the second key finding, the results supported that the expansion of pharmacy curriculum has increased superiority of competencies among the students with respect to their different specialties. The graduates specializing in PC had higher perceived competency in the domains of PC services, system management, primary care, and consumer protection. The graduates who specialized in IP had higher perceived competency in medication selection and procurement and IP. The previous research conducted with employers and pharmacists supported the transition to the 6-year PharmD program since it equipped newly graduated pharmacists with specialized competencies, and the graduates were more ready to work.11,14 Development of specialization is a global trend for pharmacy to continue to become more patient oriented and enhance professional recognition. Pharmacy education in Europe also developed a core set of competencies for specialization for pharmacist who would become an expert in one particular skill or area such as hospital pharmacy or community pharmacy.20
Workforce–competency mismatching
In an overview, the transition to PharmD program might be successful in increasing their competencies. However, the one big question that needed to be answered was how the 6-year PharmD program would fulfill many expectations required by law under one single pharmacy license.4 The results of the present study show that although 34% of the students graduated with IP track, <10% preferred to work for pharmaceutical manufacturing companies. The majority planned to work in a community pharmacy or a hospital instead. This may mean that they may not be as competent as their PC track colleagues to do this work, although it may also reflect individual preferences for workplace choice. In 2013, 32% of the pharmacy graduates enrolled to work for the public services, which was mainly in hospital settings, and these graduates achieved their BPharm with pharmaceutical science background.15 This raises an alarm regarding a mismatch between the graduates and their work competencies resulting from the single pharmacy license in Thailand. During this transition of the pharmacy curriculum, without the reform in licensing process, employers may need to reconsider and be more selective in their recruitment and training process. Although holding a single pharmacy license as their seniors, these new PharmD graduates have different specialties. Understanding the characteristics and competencies of these graduates can help employers to put the right person in the right job, which may lead to better performance and better outcomes to patients and society. For example, hospitals can assign the new PharmD pharmacist specialized in IP track to take care of the medication selection and procurement or the extemporaneous preparation, instead of assigning them into the clinical services.
Gaps to be filled
Another concern mentioned in previous studies that the 6-year PharmD program was effective in preparing students in clinical care for tertiary hospital settings, but not ready for other tasks, such as providing primary care and community care.14 Similarly, employers reported a need for additional competencies for those working in local pharmaceutical manufacturing settings.11 The findings of this survey, representing the graduates’ view on their competencies, were concordant with the previous work.15 The graduates rated their highest level of confidence in providing PC services for an individual patient. They rated themselves lower for competencies in primary health care and consumer protection and pharmaceutical industry. Similar findings were observed among employers in hospitals, they remarked that pharmacy education should include and integrate the subjects of health promotion and public health in pharmacy curriculum.14
The curriculum urgently needs adjusting to fulfill the demands on pharmacists’ tasks regarding primary care, community care, health system management, and medication system management. Designing a curriculum for strengthening these competencies is very challenging for Thai pharmacy educators because there is no roadmap to follow, unlike the traditional 6-year PharmD program, which is similar to the US PharmD program that focuses on patient care or PC competencies. The movement of the 6-year PharmD program in Thailand was originated in the area of clinical pharmacy under the support of the US–Thai consortium, which has supported the training of Thai academic workforce in the US universities, since 1993.4
Tasks regarding primary care, community care, health system management, and medication system management required the integration of different kinds of knowledge, ranging from pharmaceutics, pharmacotherapy, public health, organization and management, and other applied fields. To design this kind of program, further curriculum reform is required, where educators need to carefully think about the core philosophy and design for holistic connections of courses.21,22 Findings from this study support the need for the integration of knowledge as those graduates who completed the IP track reported higher perceived competency in medication selection and procurement domains than those who completed the PC track, which may be because of their superior product-oriented knowledge. In a survey of pharmacy graduates enrolled in the public services program, the graduates with a specialty in IP also reported higher level of competency in consumer health protection (including regulatory affairs on health products), which required integration of product- and patient-oriented knowledge.15
The results of this study could be used in pharmacy health workforce planning. However, some limitations are noted. First, this was a self-assessment by the graduates, not an actual evaluation on task performing or professional performance. However, it was the best available choice for the baseline situation as there were no other comparative assessments.15,17 The alternative might be scores from the national licensing examination, which mainly focus on professional core competency and do not cover other perspective of graduates’ perceptions and core competencies such as communication and lifelong learning. Second, the survey was conducted during the national licensing examination. It is possible that parts of the perceived competency were from the studying and tutoring for the examination, not solely from the training program. Nevertheless, the results act as a reflection for the real baseline competency of the entry-level pharmacy workforce. Further study might consider a cohort study to follow these 6-year PharmD graduates who are employed in various settings and compare them with their peers who graduated from the 5-year BPharm degree. This further study would provide a better picture of whether or not specialization in the 6-year PharmD program is producing better workforces.
Conclusion
The findings of this study reflect that Thai pharmacy education continues to adjust to the needs of society and the changing health care environments. Longitudinal monitoring to observe this transition is needed for both curriculum adjustment and competency of the graduates.
Acknowledgments
The authors wish to thank various people for their contributions to the study; the pharmacy graduates for their participation; The Pharmacy Council of Thailand, the Pharmacy License Examination Center, all the 12 test centers, all 19 Faculty of Pharmacy, and the Pharmacy Education Consortium of Thailand for their coordination in data collection; Dr Nithima Sumpradit for her support regarding the work in pharmacy workforce development. Special thanks to Associate Professor Petcharat Pongcharoensuk, who, although no longer with us, continues to inspire by her works in the area of pharmacy education and workforce.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
International Pharmaceutical Federation (FIP). Global vision for education and workforce; 2016. Available from: http://www.fip.org/files/fip/PharmacyEducation/2016_report/2016-11-Education-workforce-global-vision.pdf. Accessed October 1, 2017. | ||
Kim E, Ghimire S. Career perspectives of future graduates of the newly implemented 6-year pharmacy educational system in South Korea. Am J Pharm Educ. 2013;77(2):37. | ||
Cho HK. Challenges and opportunities posed by a new prescription law in South Korea. Am J Health Syst Pharm. 2002;59(18):1780–1782. | ||
Pongcharoensuk P, Prakongpan S. Centennial pharmacy education in Thailand. J Asian Assoc School Pharm. 2012;1(1):8–15. | ||
Wuttipanich T, Kitisopee T. Economic impact assessment on good pharmacy practice regulation in Thai community pharmacy. Thai J Pharm Sci. 2015;39(3):119–126. | ||
Bureau of Drug Control Ministry of Public Health [homepage on the Internet]. Good pharmacy practice; 2014. Available from: http://www.fda.moph.go.th/sites/Drug/SitePages/GPPPage.aspx. Accessed October 1, 2017. | ||
Limwattananon S, Tangcharoensathien V, Tisayaticom K, Boonyapaisarncharoen T, Prakongsai P. Why has the Universal Coverage Scheme in Thailand achieved a pro-poor public subsidy for health care? BMC Public Health. 2012;12(Suppl 1):S6. | ||
Tangcharoensathien V, Mills A, Palu T. Accelerating health equity: the key role of universal health coverage in the Sustainable Development Goals. BMC Med. 2015;13:101. | ||
The Royal Thai Government Gazette. The Pharmacy Professions Act of 1994; 1994. Available from: https://www.pharmacycouncil.org/share/file/file_48.pdf. Accessed October 1, 2017. | ||
Suwannaprom P, Suttajit S, Eakanunkul S, Chanakit T. A Competency Framework for the Next Decade Thai Pharmacist (2017–2026) (Draft). Bangkok: The Pharmacy Education Consortium of Thailand and The Pharmacy Council of Thailand; 2017. | ||
Chanakit T, Low BY, Wongpoowarak P, Moolasarn S, Anderson C. Does a transition in education equate to a transition in practice? Thai stakeholder’s perceptions of the introduction of the Doctor of Pharmacy programme. BMC Med Educ. 2015;15:205. | ||
The Royal Thai Government Gazette Vol 125 SPN. The Pharmacy Council of Thailand’s regulation about accredited pharmacy degree; 2008. Available from: www.pharmacycouncil.org/share/file/file_269.pdf. Accessed January 15, 2018. | ||
Chanakit T, Low BY, Wongpoowarak P, Moolasarn S, Anderson C. A survey of pharmacy education in Thailand. Am J Pharm Educ. 2014;78(9):161. | ||
Chanakit T, Low BY, Wongpoowarak P, Moolasarn S, Anderson C. Hospital pharmacists’ perceptions of the suitability of doctor of pharmacy graduates in hospital settings in Thailand. BMC Med Educ. 2015; 15:181. | ||
Sumpradit N, Suttajit S, Hunnangkul S, Wisaijohn T, Putthasri W. Comparison of self-reported professional competency across pharmacy education programs: a survey of Thai pharmacy graduates enrolled in the public service program. Adv Med Educ Pract. 2014;5:347–357. | ||
The Pharmacy Council of Thailand. Pharmacy Council Announcement No. 18/2012. Professional core competency of Doctor of Pharamacy Program 2012. Available from: https://goo.gl/evU3fy. Accessed January 15, 2018. | ||
Sitaruno S, La-Ongkaew S, Malison N. Satisfaction toward the Doctor of Pharmacy (Pharm D.) graduates and Pharm.D. program: perspective of graduates, employers, colleagues and patients. Thai J Hosp Pharm. 2013;23(2):75–85. | ||
The Curriculum SIG Writing Group. A curriculum committee toolkit for addressing the 2013 CAPE Outcomes. Available from: https://www.aacp.org/sites/default/files/2017-10/CurriculumSIGCAPEPaperFinalNov2014.pdf. Accessed April 18, 2018. | ||
Nemire RE, Meyer SM. Educating students for practice: educational outcomes and community experience. Am J Pharm Educ. 2006;70(1):20. | ||
International Pharmaceutical Federation (FIP). Advanced Practice and Specialisation in Pharmacy: Global Report. The Hague, the Netherlands: International Pharmaceutical Federation; 2015. | ||
Husband AK, Todd A, Fulton J. Integrating science and practice in pharmacy curricula. Am J Pharm Educ. 2014;78(3):63. | ||
Katajavuori N, Hakkarainen K, Kuosa T, Airaksinen M, Hirvonen J, Holm Y. Curriculum reform in Finnish pharmacy education. Am J Pharm Educ. 2009;73(8):151. |
Supplementary material
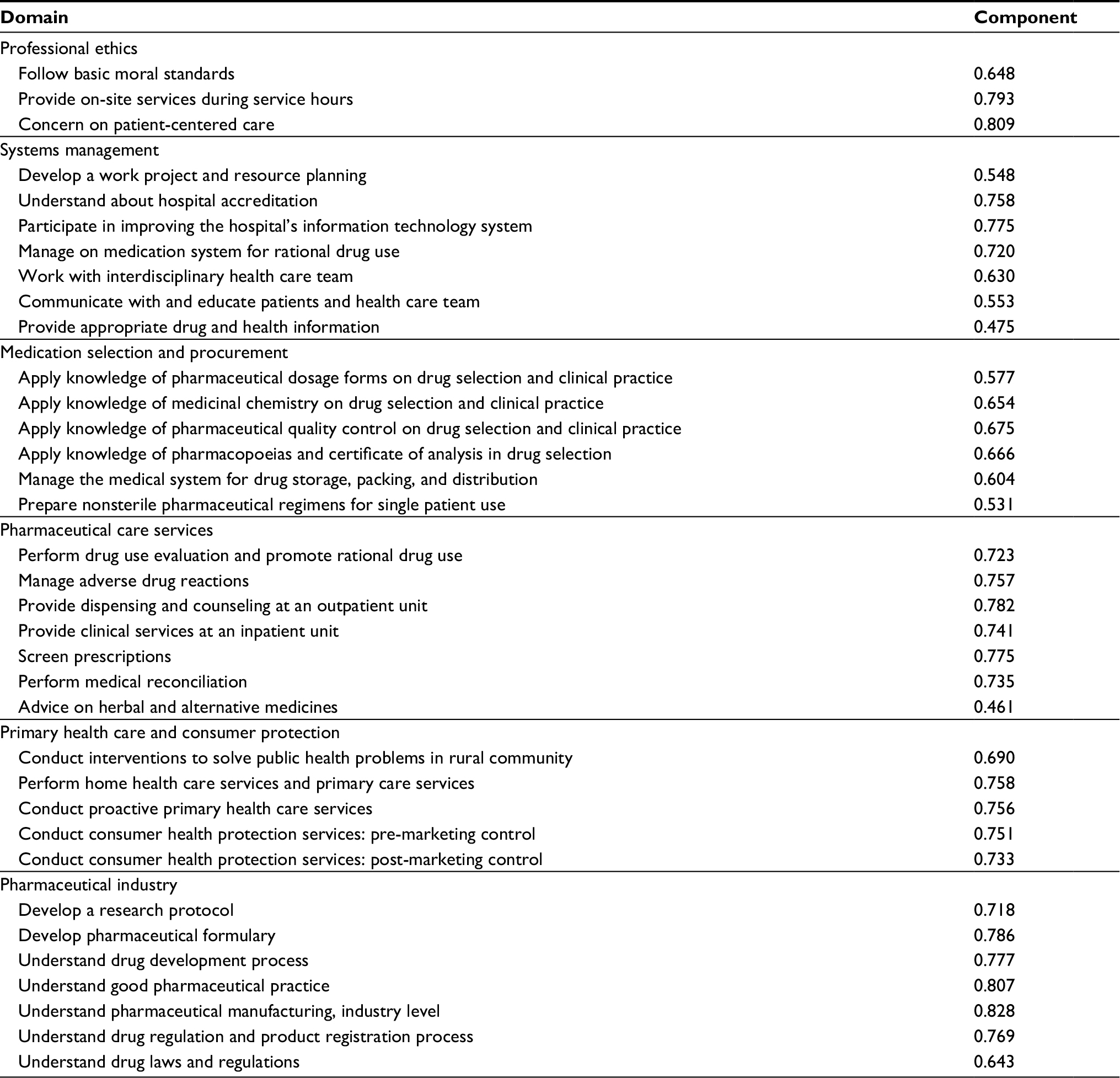 | Table S1 Factor analysis for Thai pharmacy core professional competencies Notes: Extraction method: principal component analysis. Rotation method: varimax with Kaiser normalization. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.