")
Back to Journals » Infection and Drug Resistance » Volume 11
Appropriate composites of cefoperazone–sulbactam against multidrug-resistant organisms
Authors Lai CC , Chen CC , Lu YC , Lin TP, Chuang YC, Tang HJ
Received 24 May 2018
Accepted for publication 6 July 2018
Published 11 September 2018 Volume 2018:11 Pages 1441—1445
DOI https://doi.org/10.2147/IDR.S175257
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Joachim Wink
Chih-Cheng Lai,1 Chi-Chung Chen,2,3 Ying-Chen Lu,3 Tsuey-Pin Lin,4 Yin-Ching Chuang,2,5 Hung-Jen Tang4,6
1Department of Intensive Care Medicine, Chi Mei Medical Center, Liouying, 2Department of Medical Research, Chi Mei Medical Center, Tainan, 3Department of Food Science, National Chiayi University, Chiayi, 4Department of Health and Nutrition, Chia-Nan University of Pharmacy and Science, 5Department of Internal Medicine, Chi Mei Medical Center, Liouying, 6Department of Medicine, Chi Mei Medical Center, Tainan, Taiwan
Objectives: This study aims to assess the in vitro activity of different cefoperazone–sulbactam ratios against different multidrug-resistant organisms (MDROs).
Materials and methods: Minimum inhibitory concentrations (MICs) and susceptibility rates of cefoperazone, sulbactam and cefoperazone–sulbactam at fixed ratios of 2:1, 1:1 and 1:2 against 344 MDRO clinical isolates, including extended-spectrum β-lactamase (ESBL)-producing Escherichia coli (n=58), ESBL-producing Klebsiella pneumoniae (n=58), carbapenem-resistant Enterobacteriaceae (n=57), carbapenem-resistant Pseudomonas aeruginosa (n=49) and carbapenem-resistant Acinetobacter baumannii (n=122), were measured.
Results: Combined treatment with sulbactam and cefoperazone resulted in decreased MIC50 values across all MDROs, as well as decreases in most MIC90 values, except for carbapenem-resistant Enterobacteriaceae and carbapenem-resistant P. aeruginosa (MIC90 values remained >64 mg/L). Susceptibility rates of treatment with cefoperazone alone against all MDROs were much lower than that of cefoperazone–sulbactam combination (all P<0.05), except in carbapenem-resistant P. aeruginosa. Additionally, the susceptibility rate gradually increased as the ratio of cefoperazone–sulbactam was adjusted from 2:1 to 1:1 and to 1:2 for carbapenem-resistant Enterobacteriaceae, ESBL-producing K. pneumoniae and carbapenem-resistant A. baumannii. There were no significant ratio-dependent changes in susceptibility rates with cefoperazone–sulbactam in carbapenem-resistant P. aeruginosa.
Conclusion: Adding sulbactam enhances cefoperazone activity against most MDROs excluding carbapenem-resistant P. aeruginosa, and the activity of cefoperazone–sulbactam against these MDROs is greatest at a ratio of 1:2, followed by ratios of 1:1 and 2:1.
Keywords: cefoperazone–sulbactam, extended-spectrum β-lactamases, Escherichia coli, Klebsiella pneumoniae, multidrug-resistant organisms
Introduction
β-Lactam antibiotics, which include penicillin, cephalosporin, monobactam and carbapenem, are the most commonly used antibiotics in the world. However, the increased use of β-lactam antibiotics has led to the development of various types of antibiotic resistance, with the production of β-lactamases as one of the primary mechanisms.1 Therefore, β-lactamase inhibitors, such as sulbactam, tazobactam, clavulanic acid, avibactam, relebactam and vaborbactam, have been developed and combined with β-lactam antibiotics to overcome this mechanism.2–5 To date, several β-lactam/β-lactamase inhibitor antibiotics have been shown to exhibit synergistic in vitro activities against multidrug-resistant organisms (MDROs), including amoxicillin–clavulanate, ampicillin–sulbactam, piperacillin–tazobactam, cefoperazone–sulbactam, ceftolozane–tazobactam, ceftazidime–avibactam and meropenem–vaborbactam.6–9 However, the ratio of β-lactam to β-lactamase inhibitor that exerts the greatest inhibitory activity against MDROs is not known, and it is unclear whether the present formula of β-lactam/β-lactamase inhibitor is the best composite. Our previous study9 demonstrated that cefoperazone–sulbactam at a 1:1 ratio had a higher susceptibility rate against MDROs such as extended-spectrum β-lactamase (ESBL)-producing Escherichia coli, carbapenem-resistant E. coli and carbapenem-resistant Acinetobacter baumannii, compared with cefoperazone–sulbactam at a 2:1 ratio. In this study, we hypothesize that a higher ratio of sulbactam in the cefoperazone–sulbactam combined antibiotic may lead to greater in vitro activity against MDROs. Therefore, in this study, we test the efficacy of cefoperazone–sulbactam at ratios of 2:1, 1:1 and 1:2 against MDROs in vitro.
Materials and methods
Collection of clinical isolates
Clinical isolates of ESBL-producing E. coli, ESBL-producing Klebsiella pneumoniae, carbapenem-resistant Enterobacteriaceae, carbapenem-resistant Pseudomonas aeruginosa and carbapenem-resistant A. baumannii were collected during the period of 2008–2015. These isolates were obtained from the Department of Bacteriology at three hospitals including one medical center (1,273 beds), one regional hospital (876 beds) and one district hospital (263 beds). ESBL-producing E. coli and K. pneumoniae isolates were confirmed as previously described.10 Carbapenem resistance is classified as resistance to either imipenem, meropenem, doripenem or ertapenem.
In vitro susceptibility
The minimum inhibitory concentrations (MICs) of the drugs were measured by broth microdilution as described in a previous study.11 Standard powders of cefoperazone and sulbactam were provided by TTY (TTY Biopharm, Taipei, Taiwan), and MIC and susceptibility interpretation criteria were determined according to previous guidelines.10,12 Doubling dilutions of cefoperazone ranged from 0.25 to 64 mg/L, and four different sets of dilutions were tested. The first series of cefoperazone dilutions were tested without added sulbactam. The second, third and fourth series contained cefoperazone combined with sulbactam at a 2:1 ratio (two parts cefoperazone to one part sulbactam), a 1:1 ratio (one part cefoperazone to one part sulbactam) and a 1:2 ratio (one part cefoperazone to two parts sulbactam). Finally, we tested sulbactam without cefoperazone. Susceptibilities of cefoperazone alone and cefoperazone–sulbactam at 2:1, 1:1 and 1:2 ratios were determined using the criterion of MIC of cefoperazone ≤16 mg/L.11 E. coli ATCC 25922 and K. pneumoniae ATCC 700603 were treated as quality control strains.
Statistical analysis
A chi-squared test was used for the analysis, with P-values of <0.05 considered statistically significant.
Results
In this study, a total of 344 MDROs from clinical isolates, including ESBL-producing E. coli (n=58), ESBL-producing K. pneumoniae (n=58), carbapenem-resistant Enterobacteriaceae (n=57), carbapenem-resistant P. aeruginosa (n=49) and carbapenem-resistant A. baumannii (n=122), were enrolled for testing. The MIC values of cefoperazone alone and in combination with sulbactam against ESBL-producing E. coli, ESBL-producing K. pneumoniae, carbapenem-resistant Enterobacteriaceae, carbapenem-resistant P. aeruginosa and carbapenem-resistant A. baumannii are shown in Table 1. Cefoperazone alone showed high MICs against most isolates, with MIC50 and MIC90 >64 mg/L, except ESBL-producing K. pneumoniae (MIC50=64 mg/L). MIC50 values decreased for all of MDROs after the addition of sulbactam, and most MIC90 values decreased, except of carbapenem-resistant Enterobacteriaceae and carbapenem-resistant P. aeruginosa (MIC90 values remained >64 mg/L). We then tested the different combinations of cefoperazone–sulbactam at 2:1, 1:1 and 1:2 ratios. For ESBL-producing E. coli, K. pneumoniae and carbapenem-resistant A. baumannii, MIC50 and MIC90 values decreased as the ratio of cefoperazone–sulbactam changed from 2:1 to 1:1 and to 1:2. For carbapenem-resistant Enterobacteriaceae, only MIC50 values decreased as the ratio of cefoperazone–sulbactam changed from 2:1to 1:1 and to 1:2, with all of MIC90 values >64 mg/L. For carbapenem-resistant P. aeruginosa, no significant change in MIC values was noted for various ratios of cefoperazone–sulbactam combinations.
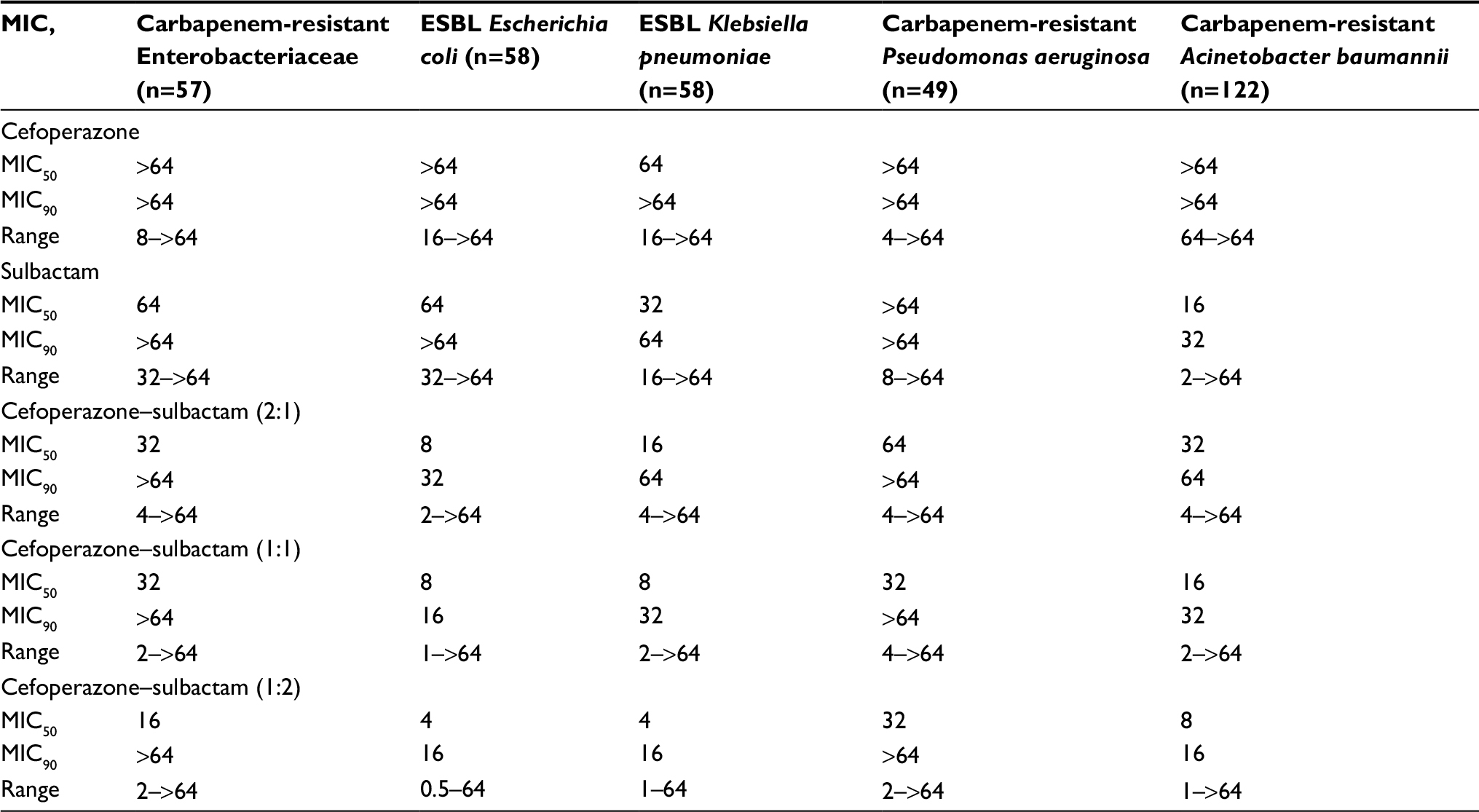 | Table 1 MIC range, MIC50 and MIC90 of cefoperazone alone, cefoperazone–sulbactam (2:1), cefoperazone–sulbactam (1:1) and cefoperazone–sulbactam (1:2) against different drug-resistant organisms Abbreviations: ESBL, extended-spectrum β-lactamase; MIC, minimum inhibitory concentration. |
Table 2 shows the antibiotic susceptibility rate of cefoperazone alone and in combination with different ratios of sulbactam against MDROs. The susceptibility rates of cefoperazone alone against all MDROs were much lower than cefoperazone–sulbactam combinations (all P<0.05), excluding carbapenem-resistant P. aeruginosa. For the different ratios of cefoperazone–sulbactam combinations, the susceptibility rate gradually increased as the ratio of cefoperazone–sulbactam was changed from 2:1 to 1:1 and to1:2 for carbapenem-resistant Enterobacteriaceae, ESBL-producing K. pneumoniae and carbapenem-resistant A. baumannii. For these three MDROs, cefoperazone–sulbactam at a 1:2 ratio had a higher susceptibility rate than at a 2:1 ratio (P<0.05). For carbapenem-resistant Enterobacteriaceae and carbapenem-resistant A. baumannii, cefoperazone–sulbactam at a 1:2 ratio had a higher susceptibility rate than at a 1:1 ratio (P<0.05). For ESBL-producing E. coli, the susceptibility rates were the same for cefoperazone–sulbactam at 1:1 and 1:2 ratios, but both were higher than the susceptibility at a 2:1 ratio. For carbapenem-resistant P. aeruginosa, no significant changes in susceptibility rates were observed across different ratios of cefoperazone–sulbactam.
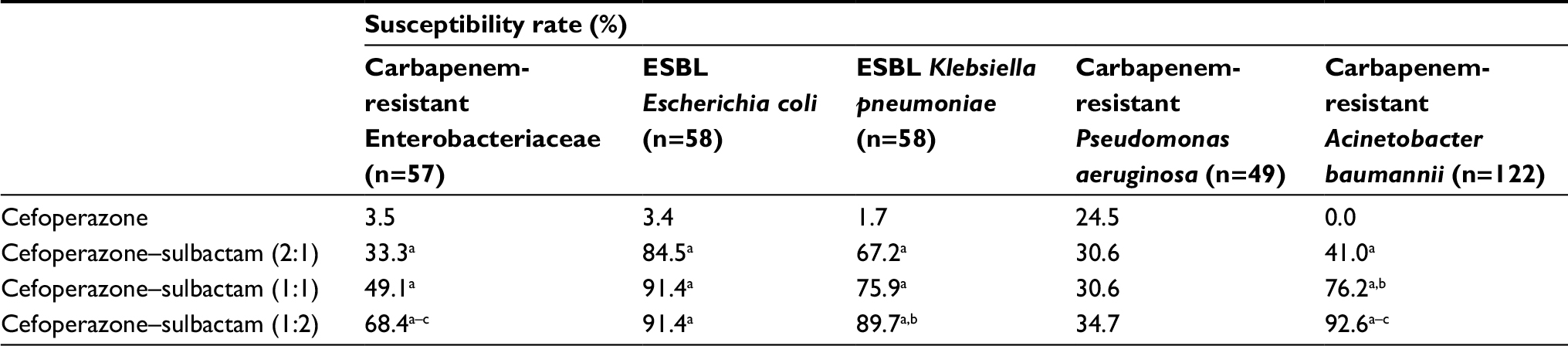 | Table 2 Antibiotic susceptibility rates of cefoperazone alone, cefoperazone–sulbactam (2:1), cefoperazone–sulbactam (1:1) and cefoperazone–sulbactam (1:2) against different drug-resistant organisms Notes: Susceptibilities of cefoperazone alone and cefoperazone–sulbactam at 2:1, 1:1 and 1:2 ratios were classified according to the MIC of cefoperazone ≤16 mg/L. aP-value <0.05 compared to cefoperazone. bP-value <0.05 compared to cefoperazone–sulbactam (2:1). cP-value <0.05 compared to cefoperazone–sulbactam (1:1). Abbreviations: ESBL, extended-spectrum β-lactamase; MIC, minimum inhibitory concentration. |
Discussion
This study investigated the in vitro activity of different ratios of cefoperazone–sulbactam and of cefoperazone alone against various MDROs and identified several significant findings. First, both MIC and antibiotic susceptibility tests show that the in vitro activity of cefoperazone against MDROs, even carbapenem-resistant A. baumannii, can be enhanced after adding sulbactam, with carbapenem-resistant P. aeruginosa being the only exception. This is consistent with a previous study by Kuo et al,13 which demonstrated that the addition of sulbactam to cefoperazone can significantly enhance the antimicrobial activities against Serratia marcescens, Enterobacter cloacae, ESBL-K. pneumoniae and A. baumannii. In addition to Kuo et al’s finding,13 our study showed this combination can also enhance the antibiotic activity against carbapenem-resistant Enterobacteriaceae and ESBL-E. coli. Overall, our study and several other in vitro studies9,13,14 indicated that the addition of sulbactam can improve cefoperazone’s activity against MDR-Enterobacteriaceae and A. baumannii. However, further study will be needed to see if the result on planktonic bacteria also applies to biofilm-embedded bacteria, which is more likely to correspond to clinical antibiotic failure.
Second, the impact of sulbactam on the activity of cefoperazone–sulbactam against MDROs varies according to the ratio of sulbactam and the type of MDRO. For most MDRO isolates, we observed that the inhibitory activity of the cefoperazone–sulbactam combination would increase with increased ratios of sulbactam (1:2>1:1>2:1). These findings expand upon the previous knowledge9 that cefoperazone–sulbactam at a 1:1 ratio has a higher susceptibility rate against ESBL-producing E. coli, carbapenem-resistant E. coli and carbapenem-resistant A. baumannii than cefoperazone–sulbactam at a 2:1 ratio (all P<0.05). In contrast, this additional effect of sulbactam was not observed for carbapenem-resistant P. aeruginosa. Current commercial products containing cefoperazone–sulbactam are made using the fixed ratio of 1:1. Our findings indicate that adding more sulbactam to the current cefoperazone–sulbactam formulations could enhance their in vitro activity against some MDROs, including carbapenem-resistant Enterobacteriaceae, ESBL-producing E. coli, ESBL-producing K. pneumoniae and carbapenem-resistant A. baumannii. Similar findings report that piperacillin–sulbactam at a 2:1 ratio has improved activity against most Gram-negative bacteria, compared to piperacillin–sulbactam at a 4:1 ratio.15 Even for Mycobacterium tuberculosis, a 1:1 ratio of ampicillin to β-lactamase inhibitor was more active than a 2:1 ratio.16 However, in vitro activity may not translate into clinical efficacy, and further studies are required to confirm this effect.
Third, we found that the in vitro activity of sulbactam alone against MDROs was poor. While 17 carbapenem-resistant A. baumannii isolates had MIC ≤4 mg/L, all other organisms had MIC ≥8 mg/L. Temocin et al17 showed that 2 (6.7%) out of 30 MDR-A. baumannii were susceptible to sulbactam. Fass et al18 showed that among 28,000 isolates of the family Enterobacteriaceae, sulbactam alone was inactive against 99.6% of the isolates with the exception of Acinetobacter calcoaceticus and Pseudomonas cepacia. These data suggest that sulbactam alone may not be a good choice for treating MDROs, except in the case of A. baumannii.
In conclusion, the addition of sulbactam can enhance cefoperazone’s activity against most MDROs, except carbapenem-resistant P. aeruginosa, and the activity of cefoperazone–sulbactam against these MDROs is greatest at a 1: two ratio, followed by 1:1 and 2:1 ratios.
Disclosure
The authors report no conflicts of interest in this work.
References
Thomson JM, Bonomo RA. The threat of antibiotic resistance in Gram-negative pathogenic bacteria: beta-lactams in peril! Curr Opin Microbiol. 2005;8(5):518–524. | ||
Drawz SM, Bonomo RA. Three decades of beta-lactamase inhibitors. Clin Microbiol Rev. 2010;23(1):160–201. | ||
Ambrose PG, Lomovskaya O, Griffith DC, Dudley MN, Vanscoy B. β-Lactamase inhibitors: what you really need to know. Curr Opin Pharmacol. 2017;36:86–93. | ||
Docquier JD, Mangani S. An update on β-lactamase inhibitor discovery and development. Drug Resist Updat. 2018;36:13–29. | ||
Wong D, van Duin D. Novel beta-lactamase inhibitors: unlocking their potential in therapy. Drugs. 2017;77(6):615–628. | ||
van Duin D, Bonomo RA. Ceftazidime/avibactam and ceftolozane/tazobactam: second-generation β-lactam/β-lactamase inhibitor combinations. Clin Infect Dis. 2016;63(2):234–241. | ||
Jorgensen SCJ, Rybak MJ. Meropenem and vaborbactam: stepping up the battle against carbapenem-resistant Enterobacteriaceae. Pharmacotherapy. 2018;38(4):444–461. | ||
Zhanel GG, Lawrence CK, Adam H, et al. Imipenem–relebactam and meropenem–vaborbactam: two novel carbapenem-β-lactamase inhibitor combinations. Drugs. 2018;78(1):65–98. | ||
Chang PC, Chen CC, Lu YC, et al. The impact of inoculum size on the activity of cefoperazone–sulbactam against multidrug resistant organisms. J Microbiol Immunol Infect. 2018;51(2):207–213. | ||
National Committee for Clinical Laboratory Standards. Performance Standards for Antimicrobial Susceptibility Testing, 9th Informational Supplement. M100-S24. Wayne, PA: National Committee for Clinical Laboratory Standards; 2014. | ||
Lai CC, Chen CC, Huang HL, Chuang YC, Tang HJ. The role of doxycycline in the therapy of multidrug-resistant E. coli – an in vitro study. Sci Rep. 2016;6:31964. | ||
National Committee for Clinical Laboratory Standards. Methods for Dilution Antimicrobial Susceptibility Testing of Bacteria That Grow Aerobically. Approved Standard. 8th ed. Wayne, PA: CLSI; 2012. | ||
Kuo HY, Wang FD, Yen YF, Lin ML, Liu CY. In vitro activities of piperacillin or cefoperazone alone and in combination with beta-lactamase inhibitors against gram-negative bacilli. New Microbiol. 2009;32(1):49–55. | ||
Williams JD. Beta-lactamase inhibition and in vitro activity of sulbactam and sulbactam/cefoperazone. Clin Infect Dis. 1997;24(3):494–497. | ||
Hung MN, Hsueh PR, Chang HT, et al. In vitro activities of various piperacillin and sulbactam combinations against bacterial pathogens isolated from Intensive Care Units in Taiwan: SMART 2004 programme data. Int J Antimicrob Agents. 2007;29(2):145–152. | ||
Sorg TB, Cynamon MH. Comparison of four beta-lactamase inhibitors in combination with ampicillin against Mycobacterium tuberculosis. J Antimicrob Chemother. 1987;19(1):59–64. | ||
Temocin F, Erdinc FS, Tulek N, et al. Synergistic effects of sulbactam in multi-drug-resistant Acinetobacter baumannii. Braz J Microbiol. 2015;46(4):1119–1124. | ||
Fass RJ, Gregory WW, D’Amato RF, et al. In vitro activities of cefoperazone and sulbactam singly and in combination against cefoperazone-resistant members of the family Enterobacteriaceae and nonfermenters. Antimicrob Agents Chemother. 1990;34(11):2256–2259. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.