")
Back to Journals » Psychology Research and Behavior Management » Volume 15
Anxiety Among Healthcare Workers During COVID-19 Pandemic in Lebanon: The Importance of the Work Environment and Personal Resilience
Authors Sakr CJ , Rahme D, Fakih L, Assaf SA , Redlich CA, Slade MD, Fakhreddine M, Usta J, Musharrafieh U, Maalouf G, Khater B
Received 1 December 2021
Accepted for publication 12 March 2022
Published 5 April 2022 Volume 2022:15 Pages 811—821
DOI https://doi.org/10.2147/PRBM.S350125
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Carine J Sakr,1,* Diana Rahme,1,* Lina Fakih,1 Sara A Assaf,1 Carrie A Redlich,2 Martin D Slade,2 Mohammad Fakhreddine,3 Jinan Usta,4 Umayya Musharrafieh,4 Grace Maalouf,4 Beatrice Khater4
1Employee Health Unit, American University of Beirut Medical Center, Beirut, Lebanon; 2Yale Occupational and Environmental Medicine Program,Yale University School of Medicine, New Haven, CT, USA; 3Faculty of Medicine, American University of Beirut, Beirut, Lebanon; 4Department of Family Medicine, American University of Beirut Medical Center, Beirut, Lebanon
*These authors contributed equally to this work
Correspondence: Beatrice Khater, Department of Family Medicine, AUBMC, Cairo Street, Hamra, Beirut, Lebanon, Email [email protected]
Background: Healthcare workers (HCWs) have been severely impacted by the COVID-19 pandemic. In addition to their risk of direct exposure to the virus, they were subjected to long working hours, scarcity of PPE, and additional stressors that impacted their psychological wellbeing. The purpose of this study was to assess anxiety and its predictors among a sample of HCWs at the American University of Beirut Medical Center (AUBMC) and to evaluate the association between resilience and anxiety.
Methods: This cross-sectional study was conducted using an online survey between March and June 2021 among HCWs at AUBMC. The psychosocial scale section included the 7-item generalized anxiety disorder (GAD-7) scale and a 25-item resilience scale, validated tools used to assess anxiety and resilience respectively. Data were analyzed on SPSS version 27, and descriptive statistics were applied. Predictors were evaluated using bivariate and multivariate linear regression.
Results: From a total of 92 participants, 75% were involved in direct patient care, and of those, 95% worked directly with suspected or confirmed COVID-19 patients. The majority (83%) had minimal to mild anxiety, whereas the rest had moderate to high anxiety levels. Around 41% reported moderately high to high resilience, 47% were found to be between the low end and moderate resilience scale and only 12% had very low or low resilience. More than 80% of the participants received PPE training, reported always working with adequate preventive infection control measures, and were vaccinated. Further, more than 70% of participants reported trusting the management and agreed that the safety of the workers is considered a high priority. No significant association between sociodemographic and COVID-19 work exposure factors with anxiety was found. Multivariate analysis results showed that a lower anxiety score was associated with higher resilience (p = 0.011).
Conclusion: This study has shown a strong association between low anxiety levels and high resilience scores in this group of mostly vaccinated HCWs caring for COVID-19 patients. The high percentage of vaccination along with PPE availability could explain the low anxiety levels reported among the participants.
Keywords: COVID-19, healthcare workers, anxiety, resilience, Lebanon
Introduction
Coronavirus disease 19 (COVID-19), which was first identified in Wuhan, China in early December 2019 rapidly spread to almost every country across the world posing a public health emergency of international concern. On March 11, 2020, the World Health Organization (WHO) declared COVID-19 a global pandemic.1 Lebanon, a 3rd world country currently facing harsh economical and political crises, has been hit hard by this ongoing pandemic where more than 600,000 confirmed COVID-19 cases and 8000 deaths have been reported since the epidemic began, according to the World Health Organization (WHO).2
Healthcare workers (HCWs) have been at the frontline in the fight against this pandemic and face a substantial risk of infection during the COVID-19 outbreak. Beyond the risk of infection, pandemics and outbreaks have a psychological impact on HCWs as they might become vectors in infection transmission. In addition, HCW worked for long hours, suffered from the scarcity of personal protective equipment (PPEs), and had to face difficult situations such as deciding which patients to treat after resources became limited.3 These difficulties result in adverse mental health outcomes that are not only detrimental to HCWs’ well-being, but may reduce their ability to address effectively the health emergency.4 Moreover, psychological distress among HCWs has been shown to be associated with a range of psychopathology including serious life-threatening behaviors as suicidal ideation.5 A cross-sectional survey investigating the psychological levels of HCWs in multiple centers in China reported that 54.2% and 58% of 958 HCWs had symptoms of anxiety and depression, respectively.6 Another meta-analysis study assessing the severity of mental problems during the COVID-19 pandemic and comparing the pooled incidence between COVID-19 and SARS and MERS, showed a higher overall prevalence of depression (27%) and a lower pooled incidence of post traumatic stress disorder (PTSD) during COVID-19 (16.4%) compared with SARS and MERS outbreaks.7
In Lebanon, the waves of COVID-19 patients that saturated the health care system, the subsequent overwhelming workload, the fake news portrayed by the media, along with the lack of needed drugs given the economic crisis and devaluation of the currency, are all factors that may contribute to the mental burden of HCWs. Previous studies carried out in Lebanese hospitals in 2020 showed a prevalence of 24% and 23% of anxiety and depression among HCWs respectively, emphasizing the need to assess factors associated with anxiety in this population.8,9
Resilience is the ability to withstand adversity and bounce back from difficult life events. In dealing with long-term pandemics, resilience or the ability to positively cope with challenging difficulties is an important asset. Several studies have highlighted the importance of resilience and coping behaviors in mitigating the psychological stress and mental breakdowns among HCWs during infectious disease outbreaks such as SARS, Ebola, and MERS-CoV.10,11 Further, evidence suggests that individuals who lack sufficient resilience and adaptive capacities are more likely to suffer negative mental repercussions during stressful situations like disasters and pandemics.12
To our knowledge, studies assessing risk and protective factors associated with anxiety among HCWs during the COVID-19 pandemic are limited, as is data on resilience among HCWs and the effect of resilience on their anxiety levels. Therefore, the current study aims to assess anxiety and its predictors among a sample of HCWs at the American University of Beirut Medical Center (AUBMC), and evaluate the association between resilience and anxiety.
Methods
Study Design
Healthcare workers at AUBMC, a tertiary care center affiliated with a university completed a survey assessing their exposure to COVID-19 as well as their anxiety and resilience levels. All healthcare workers (nurses, doctors, clerks, administrative officers, technicians, phlebotomists, and others) at AUBMC from any nationality were eligible for participation. The study was announced through flyers and posters that were distributed throughout the medical center. Convenience sampling was used where all participants who filled out the survey were enrolled. The study protocol was approved by the institutional review board (IRB) at the American University of Beirut.
Participants completed an online questionnaire which included the following sections: demographics, COVID-19 occupational and home exposure, work history, PPE training and use, self-reported past medical history, COVID-19 vaccination history, and psychosocial scales. The psychosocial section included the highly reliable and validated scales, 7-item generalized anxiety disorder (GAD-7) scale,13 and the 25-item resilience scale (Connor-Davidson Resilience scale (CD-RISC scale)).14 GAD-7 scale had 7 questions rated from 0 to 3 with 0 indicating not at all, 1 several days, 2 more than half of the days, and 3 almost every day. The resilience scale had 25 questions rated from 1 to 7 where 1 represents the lowest agreement with the statement and 7 the highest one. Anxiety and resilience scores were computed by adding the scores of all questions in each scale separately.
Following the GAD-7 guidelines, the anxiety score was divided into 4 categories: minimal (0–4), mild (5–9), moderate (10–14), and severe (15–21) anxiety. Resilience score was originally categorized in 6 categories: very low (25–100), low (101–115), on the low end (116–130), moderate (131–145), moderately high (146–160), and high (161–175). For analysis purposes, the score was further recoded into three categories: low (25–115), moderate (116–145), and high (146–175) resilience.
Data Collection
The questionnaire was developed as an online survey, a statistical survey web application used to collect data. The link to the survey was shared with the participants, and the questionnaire was completed online. Data were collected between March and June 2021. This study was conducted in accordance with the principles of the Declaration of Helsinki, and written informed consent was obtained from each participant before the completion of the questionnaire.
The responses of the survey were anonymous, and each participant was assigned a code. The study results were analyzed and reported in aggregate form.
Data Analysis
Data on 92 healthcare workers were entered, cleaned, and analyzed on SPSS version 27. Frequency and percentages were presented for categorical variables, whereas mean and standard deviation were presented for continuous variables.
The continuous outcome (anxiety score) was log-transformed as the dependent variable was found to be log-normally distributed. Linear regression was run for the log-transformed outcome with the following predictors: age, marital status, gender, occupation, COVID-19 vaccination status, and resilience. A p-value of <0.05 was considered statistically significant.
Results
As shown in Table 1, the majority of the participants were female (66.3%) and were less than 35 years old (56.5%). Most of the participants (96.6%) were Lebanese, and half of them were married. The vast majority (74%) reported no past medical history.
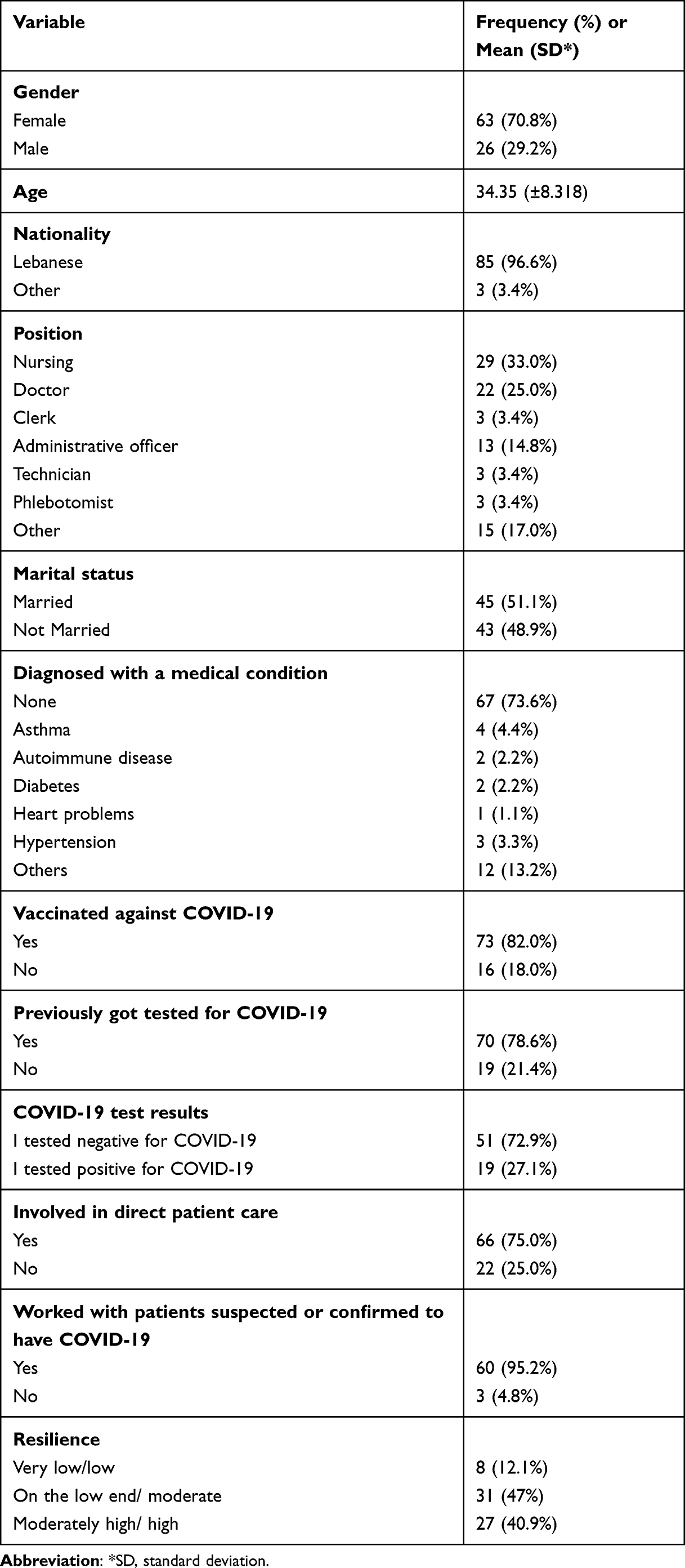 |
Table 1 Descriptive Statistics of the Study Population |
As for their occupation, 58% of the participants were nurses or medical doctors, and the remaining were distributed between clerks, administrative officers, technicians, phlebotomists, and others.
Nearly 80% of the participants were vaccinated against COVID-19 at the time of participation. Similarly, around 80% had previously been tested for COVID-19 in the context of a fever or upper respiratory tract infections (URTI) symptoms, and of those, 27% tested positive. Seventy-five percent or 66 participants were involved in direct patient care, and of those, 95% have worked directly with suspected or confirmed COVID-19 patients.
The resilience score shows that only 12.1% of the participants had very low or low resilience, and the remaining 87.9% had either moderate resilience (47%), or moderately high to high resilience scores (40.9%). The detailed descriptive data can be seen in Table 1 below.
The GAD-7 anxiety data are summarized in Table 2. The median anxiety score was 4, meaning that more than half of the participants reported minimal anxiety (score 0–4). When looking at the four categories of the GAD-7 scores, 82.7% of the participants had minimal to mild anxiety, whereas the rest had moderate to high anxiety levels.
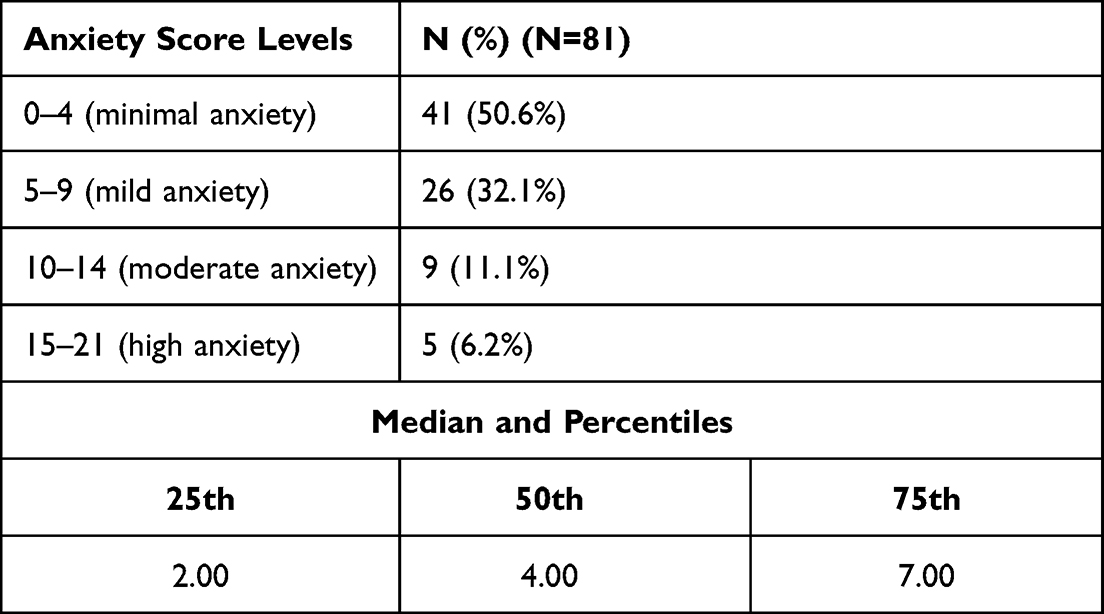 |
Table 2 Anxiety Score and Categories |
The detailed descriptive statistics of exposure variables can be found in Table 3 below. Most of the participants (75%) reported working with a COVID-19 positive colleague, and 49.1% declared working closely with COVID-19 patients (within 2 meters). Around 90% stated always working with a surgical mask on, and more than 95% reported receiving PPE training the past 3 years. Although more than two-thirds of the HCW reported having too much work to do everything well, the overwhelming majority reported that safety and health conditions at work were good, that safety is a high priority for management, and that they trust management.
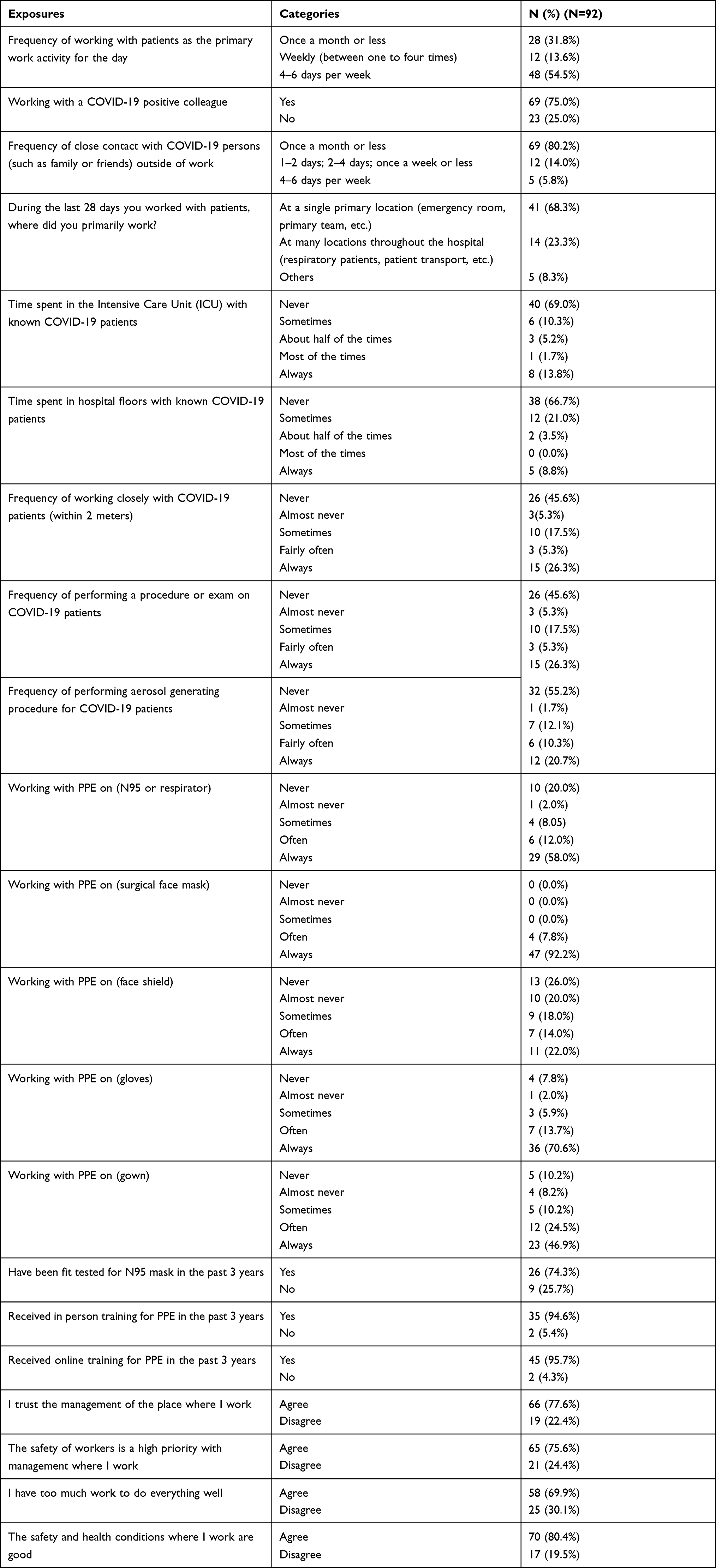 |
Table 3 Descriptive Statistics (Frequency and Percentages) of Exposure Variables, PPE Use, and Workplace Factors |
In the bivariate analysis, none of the independent variables in Tables 1 and 3 were found to be significantly associated with anxiety at a 95% level of significance.
The results of the multivariable regression analysis are presented in Table 4 below. Resilience was found to be a significant predictor of anxiety score (p=0.011*) controlling for gender, age, marital status, position, and COVID-19 vaccination. Particularly, high resilience had a negative association with the anxiety score, meaning that participants with high resilience had low anxiety scores.
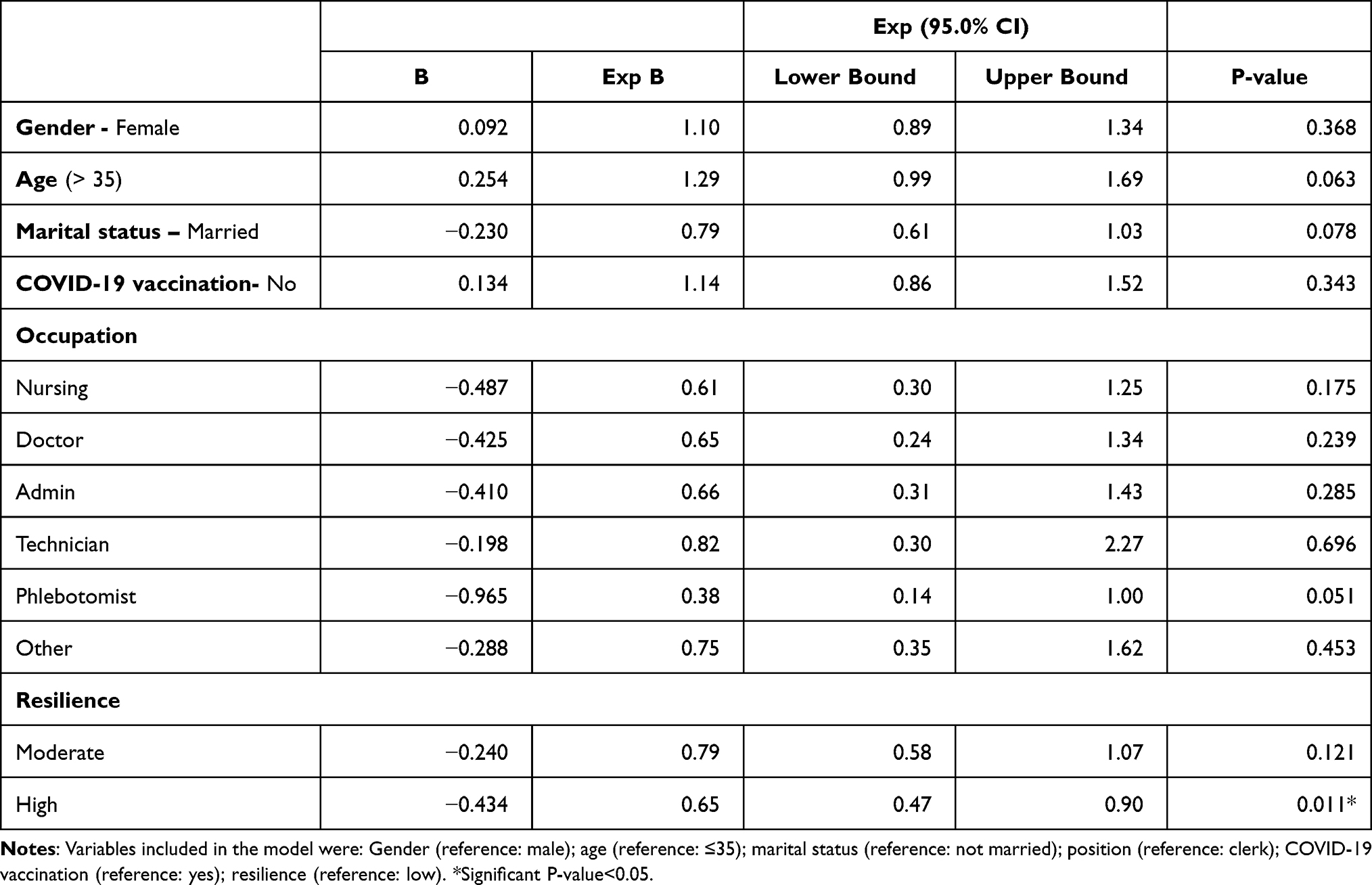 |
Table 4 Multivariate Linear Regression Model for Log (Anxiety) |
Discussion
In this study surveying 92 HCWS at AUBMC, high resilience was significantly associated with low anxiety. More than 80% of the participants received PPE training, reported following preventive infection control measures, and were vaccinated against COVID-19. More than three-quarters of participants had minimal to mild anxiety. No significant association between exposure to COVID-19 patients and anxiety was found.
The multivariate analysis showed that high resilience was found to be a significant predictor of anxiety score (p=0.011) with a negative association. This result is similar to findings of HCWs in other countries such as China, United States, Indonesia, and Turkey.15–18 Several studies reported the effectiveness of building resilience to improve employee well-being and reduce their burnout, especially in high-risk and demanding environments.19,20 Research on resilience has also pinpointed its role in improving quality of care and patient satisfaction.21 Interventions that aim to preserve and further increase resilience levels are highly recommended, including monitoring the health status of professionals, offering targeted support programs as stress management and coping techniques, and imposing policies to provide optimal working environments that prioritize the health and safety of HCWs.22
When assessing the resilience levels of the study participants using the 25-item Resilience Scale, 40.9% reported moderately high to high resilience, 47% were found to be between the low end and moderate resilience scale and only 12.1% had very low or low resilience. This finding is in agreement with studies assessing the resilience of nurses and HCWs in Lebanon,23 and other countries (China, Indonesia, and India).15,17,24 The high resilience levels among the participating HCWs may be attributable to the gratitude expressed by the public towards Lebanese masked heroes, which could have boosted their enthusiasm and raised their willingness to fight the pandemic. Furthermore, the high adaptability of the Lebanese population as a whole and caregivers particularly may be explained by the historical background of Lebanon, a country that has experienced several war episodes, civil disturbance, and economic crises over the past decades.25 Another possible factor, as suggested by an Indian study,26 could be coping strategies that HCWs have gained during the development of their professional careers, including competitive and vigorous training, long working hours, associated burnout, and routine exposure to a variety of infectious diseases. Paradoxically, exposure to such stressors greatly improves the attitude of health professionals in the face of the current crisis.
The low level of anxiety reported by study participants is in line with the results of a study assessing the mental health among Lebanese HCWs at the same medical center 6 months after the start of the COVID-19 pandemic, showing that only 23% of the participants had anxiety symptoms.8 However, several studies from different middle and high-income countries reported higher levels of anxiety among HCWs.27–30 The low prevalence of anxiety in our study compared to others may be explained by the good work environment, high trust in the management of the hospital, and adequate training and use of different PPE, where more than 70% of our participants trusted the management and agreed that the safety of the workers is considered a high priority. Moreover, more than half the participants reported always wearing different types of PPE (N95, surgical mask, gloves, and others) and having them readily available, while working. A multi-centered study evaluating the association between workplace factors and the mental health of HCWs during the pandemic in 41 countries supports these findings. A significant association between workplace factors and mental health of HCWs was reported: not being provided with appropriate PPE (p < 0.001), perceived poor workplace support within area/specialty (p < 0.001), and perceived poor mental health support (p < 0.001) negatively affected the psychological well-being of HCWs during COVID-19.31 In the current study, PPE use was not significantly correlated with anxiety, which might result from the fact that PPE use was extremely prevalent and such an association could not be elicited. In addition, the timing of the data collection occurred a year following the 1st COVID-19 case in Lebanon, which may have increased HCWs’ adaptability and preparedness in facing the pandemic with less anxiety. Another important explanation of the participants’ low anxiety levels may be the high percentage of vaccinated HCWs (82.0%) by the time this study took place. This is supported by the findings of a study carried out to evaluate the impact of COVID-19 vaccination on mental health, reporting that vaccinated individuals had higher life satisfaction scores and lower scores for depression, anxiety, and hopelessness.32
Concerning exposure factors, 58% of the sample participants were nurses or medical doctors, and around 80% had previously been tested for COVID-19 after presenting symptoms suggestive of COVID-19 infection. Nearly three-quarters of the participants were involved in direct patient care and of those, 95% have worked directly with suspected or confirmed COVID-19 patients. The bivariate analysis results showed no association between demographic or exposure factors with the anxiety levels of HCWs. This could have been different if the survey had been administered before vaccination. A study done in Turkey showed statistically significant differences in the participants’ anxiety levels with respect to their age, gender, unit of work, marital status, status of having children, and presence of a chronic disease (p < 0.05).33
This study is among the first to report the association between higher resilience levels and lower anxiety among health professionals directly caring for COVID-19 patients. However, it has a few limitations. First, the comparatively small number of participants (92 HCWs) who provided data can be considered a limitation in terms of generalizability of the results. Future studies may reveal more generalizable results by collecting data from a higher number of healthcare professionals. Moreover, the majority of the participants were nurses and medical doctors, thus creating some source of selection bias. Besides, the AUBMC is a private better-resourced healthcare institution in Lebanon and its characteristics likely differ significantly from those of other private and governmental hospitals in the country. Thus, the generalizability of the findings could be limited to hospitals with a similar context. Another limitation of the study is that self-reported answers to anxiety questions might include a degree of source and recall bias. To add, this study had a cross-sectional nature, and consequently, it cannot be used to assume causality. Finally, the study was performed via an online lime survey, in which we relied completely on information provided by the respondents, thus increasing the possibility of misunderstanding some of the questions in the survey questionnaire. These findings constitute an initial study that could help direct larger future research aimed at examining resilience and mental health in the setting of health crises and implementing resilience-based programs.
In summary, this study provides preliminary evidence about the significance of resilience in coping with stressors and mitigating anxiety in times of hard circumstances as health pandemics. Resilience development needs to be made a priority to prepare HCWs to deal with crises and reduce mental health problems in the future. Some ways that can help in acquiring resilience are experience, learning, and formal training.34,35 In addition, the findings of a study assessing the psychological resilience of HCWs during COVID-19 revealed that HCWs’ quality of sleep, positive emotions and life satisfaction need to be enhanced in order to raise their psychological resilience during the pandemic.36
Conclusion
Results have shown a strong association between the high resilience scores and low anxiety levels, highlighting the importance of high resilience as a protective factor for mental distress of frontline workers during the pandemic. This may be utilized by hospitals’ management to work on increasing HCWs’ resilience through providing education, training, psychiatric help, and modifications in workplace culture.
Funding
This study received funding from the Lebanese National Council for Scientific Research (CNRS) Grant.
Disclosure
Dr Carine Sakr reports grants from CNRS, Lebanon National Council for Scientific Research, during the conduct of the study; Ms Lina Fakih reports grants from Lebanese National Council for Scientific Research (CNRS), during the conduct of the study; Dr Sara Assaf reports grants from National Council for Scientific Research (CNRS). The authors report no other conflicts of interest in this work.
References
1. World Health Organization. WHO Coronavirus (COVID-19) dashboard; 2021. Available from: https://covid19.who.int/.
2. World Health Organization. Lebanon Coronavirus COVID-19 cases; 2021. Available from: https://covid19.who.int/region/emro/country/lb.
3. Sahebi A, Nejati-Zarnaqi B, Moayedi S, Yousefi K, Torres M, Golitaleb M. The prevalence of anxiety and depression among healthcare workers during the COVID-19 pandemic: an umbrella review of meta-analyses. Prog Neuropsychopharmacol Biol Psychiatry. 2021;107:110247. doi:10.1016/j.pnpbp.2021.110247
4. Preti E, Di Mattei V, Perego G, et al. The psychological impact of epidemic and pandemic outbreaks on healthcare workers: rapid review of the evidence. Curr Psychiatry Rep. 2020;22(8):43. doi:10.1007/s11920-020-01166-z
5. Amsalem D, Lazarov A, Markowitz JC, et al. Psychiatric symptoms and moral injury among US healthcare workers in the COVID-19 era. BMC Psychiatry. 2021;21(1):546. doi:10.1186/s12888-021-03565-9
6. Xiao X, Zhu X, Fu S, Hu Y, Li X, Xiao J. Psychological impact of healthcare workers in China during COVID-19 pneumonia epidemic: a multi-center cross-sectional survey investigation. J Affect Disord. 2020;274:405–410. doi:10.1016/j.jad.2020.05.081
7. Fan FC, Zhang SY, Cheng Y. Incidence of psychological illness after coronavirus outbreak: a meta-analysis study. J Epidemiol Community Health. 2021;75(9):836–842. doi:10.1136/jech-2020-215927
8. Msheik El Khoury F, Talih F, Khatib MFE, Abi Younes N, Siddik M, Siddik-Sayyid S. Factors associated with mental health outcomes: results from a tertiary referral hospital in Lebanon during the COVID-19 pandemic. Libyan J Med. 2021;16(1):1901438. doi:10.1080/19932820.2021.1901438
9. Abed AE, Razzak RA, Hashim HT. Mental health effects of COVID-19 within the socioeconomic crisis and after the Beirut blast among health care workers and medical students in Lebanon. Prim Care Companion CNS Disord. 2021;23(4). doi:10.4088/PCC.21m02977
10. Pincha Baduge MS, Morphet J, Moss C. Emergency nurses’ and Department preparedness for an ebola outbreak: a (narrative) literature review. Int Emerg Nurs. 2018;38:41–49. doi:10.1016/j.ienj.2017.12.002
11. De Brier N, Stroobants S, Vandekerckhove P, De Buck E. Factors affecting mental health of health care workers during coronavirus disease outbreaks (SARS, MERS & COVID-19): a rapid systematic review. PLoS One. 2020;15(12):e0244052. doi:10.1371/journal.pone.0244052
12. Labrague LJ, Hammad K, Gloe DS, et al. Disaster preparedness among nurses: a systematic review of literature. Int Nurs Rev. 2018;65(1):41–53. doi:10.1111/inr.12369
13. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
14. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
15. Huang L, Wang Y, Liu J, et al. Factors influencing anxiety of health care workers in the radiology department with high exposure risk to COVID-19. Med Sci Monit. 2020;26:e926008–1. doi:10.12659/MSM.926008
16. Huffman EM, Athanasiadis DI, Anton NE, et al. How resilient is your team? Exploring healthcare providers’ well-being during the COVID-19 pandemic. Am J Surg. 2021;221(2):277–284. doi:10.1016/j.amjsurg.2020.09.005
17. Setiawati Y, Wahyuhadi J, Joestandari F, Maramis MM, Atika A. Anxiety and resilience of healthcare workers during COVID-19 pandemic in Indonesia. J Multidiscip Healthc. 2021;14:1. doi:10.2147/JMDH.S276655
18. Yıldırım M, Arslan G, Özaslan A. Perceived risk and mental health problems among healthcare professionals during COVID-19 pandemic: exploring the mediating effects of resilience and coronavirus fear. Int J Ment Health Addict. 2020;1–11. doi:10.31234/osf.io/84xju
19. Heritage B, Rees CS, Osseiran‐Moisson R, et al. A re‐examination of the individual differences approach that explains occupational resilience and psychological adjustment among nurses. J Nurs Manag. 2019;27(7):1391–1399. doi:10.1111/jonm.12820
20. Ang S, Uthaman T, Ayre T, Mordiffi S, Ang E, Lopez V. Association between demographics and resilience–a cross‐sectional study among nurses in Singapore. Int Nurs Rev. 2018;65(3):459–466. doi:10.1111/inr.12441
21. Hart PL, Brannan JD, De Chesnay M. Resilience in nurses: an integrative review. J Nurs Manag. 2014;22(6):720–734. doi:10.1111/j.1365-2834.2012.01485.x
22. Selecting resilience and coping interventions. Available from: https://www.thriveatwork.org.au/resources/selecting-resilience-and-coping-interventions/.
23. Alameddine M, Bou-Karroum K, Ghalayini W, Abiad F. Resilience of nurses at the epicenter of the COVID-19 pandemic in Lebanon. Int J Nurs Sci. 2021;8:432–438. doi:10.1016/j.ijnss.2021.08.002
24. Jose S, Dhandapani M, Cyriac MC. Burnout and resilience among frontline nurses during COVID-19 pandemic: a cross-sectional study in the emergency department of a tertiary care center, North India. Indian J Crit Care Med. 2020;24(11):1081–1088. doi:10.5005/jp-journals-10071-23667
25. Ammar W, Kdouh O, Hammoud R, et al. Health system resilience: Lebanon and the Syrian refugee crisis. J Glob Health. 2016;6(2). doi:10.7189/jogh.06.020704
26. Wilson W, Raj JP, Rao S, et al. Prevalence and predictors of stress, anxiety, and depression among healthcare workers managing COVID-19 pandemic in India: a nationwide observational study. Indian J Psychol Med. 2020;42(4):353–358. doi:10.1177/0253717620933992
27. Maunder RG, Heeney ND, Kiss A, et al. Psychological impact of the COVID-19 pandemic on hospital workers over time: relationship to occupational role, living with children and elders, and modifiable factors. Gen Hosp Psychiatry. 2021;71:88–94. doi:10.1016/j.genhosppsych.2021.04.012
28. Aly HM, Nemr NA, Kishk RM, Elsaid NM. Stress, anxiety and depression among healthcare workers facing COVID-19 pandemic in Egypt: a cross-sectional online-based study. BMJ Open. 2021;11(4):e045281. doi:10.1136/bmjopen-2020-045281
29. Alenazi TH, BinDhim NF, Alenazi MH, et al. Prevalence and predictors of anxiety among healthcare workers in Saudi Arabia during the COVID-19 pandemic. J Infect Public Health. 2020;13(11):1645–1651. doi:10.1016/j.jiph.2020.09.001
30. Young KP, Kolcz DL, O’Sullivan DM, Ferrand J, Fried J, Robinson K. Health care workers’ mental health and quality of life during COVID-19: results from a mid-pandemic, national survey. Psychiatr Services. 2020;72(2):122–128. doi:10.1176/appi.ps.202000424
31. Khajuria A, Tomaszewski W, Liu Z, et al. Workplace factors associated with mental health of healthcare workers during the COVID-19 pandemic: an international cross-sectional study. BMC Health Serv Res. 2021;21(1):262. doi:10.1186/s12913-021-06279-6
32. Bilge Y, Keles E, Baydili KN. The impact of COVID-19 vaccination on mental health. J Loss Trauma. 2021;1–4. doi:10.1080/15325024.2021.1963558
33. Karasu F, Öztürk Çopur E, Ayar D. The impact of COVID-19 on healthcare workers’ anxiety levels. Zeitschrift fur Gesundheitswissenschaften. 2021;1–11. doi:10.1007/s10389-020-01466-x
34. Wu Z, McGoogan JM. Characteristics of and important lessons from the Coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72,314 cases from the Chinese center for disease control and prevention. JAMA. 2020;323(13):1239. doi:10.1001/jama.2020.2648
35. McAllister M, McKinnon J. The importance of teaching and learning resilience in the health disciplines: a critical review of the literature. Nurse Educ Today. 2009;29(4):371–379. doi:10.1016/j.nedt.2008.10.011
36. Bozdağ F, Ergün N. Psychological resilience of healthcare professionals during COVID-19 pandemic. Psychol Rep. 2021;124(6):2567–2586. doi:10.1177/0033294120965477
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.