")
Back to Journals » International Journal of Nanomedicine » Volume 17
Antimicrobial Coating: Tracheal Tube Application
Authors Chen X , Ling X, Liu G, Xiao J
Received 21 December 2021
Accepted for publication 21 March 2022
Published 29 March 2022 Volume 2022:17 Pages 1483—1494
DOI https://doi.org/10.2147/IJN.S353071
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ebrahim Mostafavi
Xuemeng Chen,1 Xiaomei Ling,2 Gaowang Liu,1 Jinfang Xiao1
1Department of Anesthesiology, Nanfang Hospital, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Anesthesiology, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangzhou, Guangdong, People’s Republic of China
Correspondence: Jinfang Xiao, Department of Anaesthesiology, Nanfang Hospital, Southern Medical University, Jingxi Street, Guangzhou, 510515, Guangdong, People’s Republic of China, Tel +86 198 6518 2069, Email [email protected]
Abstract: Ventilator-associated pneumonia (VAP) is a common and serious nosocomial infection in mechanically ventilated patients, increasing mortality, prolonging the patient length of stay, and increasing costs. In recent years, extensive studies on ventilator-associated pneumonia have shown that tracheal intubation plays an essential role in the pathogenesis of VAP, with the primary mechanism being the rapid colonization of the tracheal intubation surface by microbiota. Antibiotics do not combat microbial airway colonization, and antimicrobial coating materials offer new ideas to solve this problem. This paper reviews the current research progress on the role of endotracheal tube (ET) biofilms in the pathogenesis of VAP and antimicrobial coating materials.
Keywords: antibacterial, biofilm, materials, ventilator-associated pneumonia
Introduction
Tracheal intubation is an important measure to establish an artificial airway and ensure the unobstructed airway, the body’s oxygen demand, and carbon dioxide excretion. It is a necessary technique for endotracheal anesthesia cardiopulmonary resuscitation or respiratory therapy. Tracheal tubes have become an essential and crucial medical device in clinical medical practice. VAP is defined as in-hospital pneumonia that occurs 48 hours after a patient is mechanically ventilated through an ET or tracheostomy tube. VAP occurs in 25–56% of all mechanically ventilated patients and has a 25–45% morbidity and mortality rate.1 Clinical data show that mechanically ventilated patients for more than 48h have a 16–60% probability of developing VAP, significantly increased morbidity and mortality.2 Also, VAP may cause multi-drug resistant bacterial infections in Intensive Care Unit (ICU) patients, which aggravates the healthcare costs for patients and hospitals.3 The formation of ET biofilm is a significant cause of VAP. Current studies have shown that antimicrobial materials for tracheal tubes have potent antimicrobial effects. This paper reviews the current research progress of the mechanisms of ET biofilm formation, drug resistance, and antimicrobial coating materials.
Biofilm Formation
Eighty percent of human bacterial infections are associated with biofilms. Tracheal tubes provide an ideal opportunity for bacterial adhesion and biofilm formation. In 1967, microbial colonization on ET was the first discovered.4 In 1986, microbial films on the surface of ET were observed for the first time under a microscope.5
Studies have confirmed that microbial film formation includes five stages: adhesion, aggregation, growth and maturation, and dispersion (Figure 1).6 Microorganisms form biofilms by adhering to biological surfaces (endothelial damage, necrotic tissue, mucosa) or non-biological surfaces (intravenous catheters, catheters, tracheal tubes).7 After microorganisms adhere to specific locations, they can directly induce tissue necrosis, further promoting adhesion. At the same time, the surface on which microorganisms colonize The physicochemical properties of the microbial colonization surface can also affect microbial adhesion, the negatively charged hydrophobic particles carried by bacteria will change as biofilm formation progresses.8
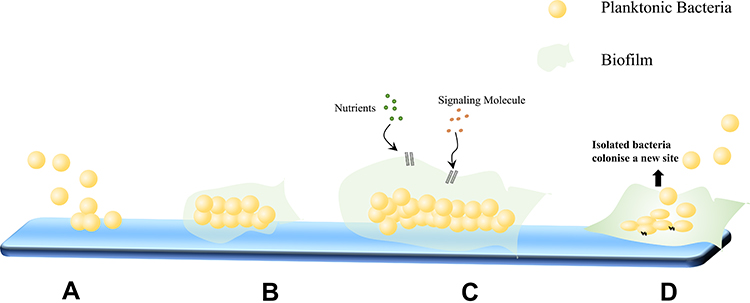 |
Figure 1 Biofilm formation. (A) Adherence: Planktonic bacteria adhere to the surface of tracheal ducts. (B) Aggregation: Microorganisms undergo multilayer aggregation to form microcolonies. (C) Maturation: Channels form in the biofilm structure, allowing for the gradient transfer of nutrients and signaling molecules and facilitating the organized aggregation and differentiation of cells based on their metabolic state. (D) Dispersion: After maturation, the biofilm thickens and the interior forms an anaerobic environment, while the outer layer may begin to separate. |
Biofilms typically contain a variety of interacting species and their environments. Biofilms are specialized microbial aggregates that depend on solid surfaces and extracellular products such as extracellular polymers (EPS). EPS matrices consist of a mixture of biopolymers.7 However, the mixture varies depending on the environment, broth cultures produce different matrices than microbial colonization of microsurfaces, and biofilms differ in vivo and in vitro conditions. In addition, microorganisms can also produce EPS to enhance microbial colony colonization adhesion.9 Subsequently, microorganisms undergo multilayer aggregation, and microcolonies are formed as a result of bacterial aggregation. In the process of biofilm maturation, some channels that allow nutrients and signal molecules to pass are formed, which promotes the orderly aggregation and differentiation of cells according to their metabolic state.10 Studies have confirmed that the biofilm comprises multiple layers of cells, and the cells in the outer biofilm exhibit active metabolism. On the contrary, the cells of the deep biofilm can enter a dormant and persistent state, slowing down the metabolism and making the maturation and shedding of the biofilm a cycle.11 In the late stages of biofilm maturation, the biofilm thickens, the interior gradually develops an anaerobic environment, and the exterior begins to separate and enter the dispersion phase. Notably, biofilms may also disperse when there is a nutrient imbalance.12 Isolated bacteria or groups of bacteria can spread as septic plugs and may colonize new sites, producing new biofilms and leading to infection.12
Biofilm-Mediated Mechanisms of Antimicrobial Drug Resistance
Polysaccharide-Protein Complexes
The polysaccharide-protein complex can be found in both Gram-positive and Gram-negative bacteria and is an integral part of the biofilm. Electrostatic and hydrogen bonds are established between this complex and the abiotic surface, which may contribute to the formation of mature biofilms. With the development of the biofilm, the composition of glycoproteins and polysaccharides varies. Moreover, the biofilm supports the survival of the pathogen under unfavorable conditions. The polysaccharide-protein complexes support antibiotic resistance and different units of antimicrobial drugs. It is both an attachment for exoenzymes and an outer layer structure to obtain antimicrobial compounds, which can provide substrates to attenuate the antimicrobial effect after the degradation of fungicides.13
Enzymes
β-lactamases in the biofilm matrix degrade antibacterial drugs and reduce their bactericidal effect. A study investigated that mature Pseudomonas aeruginosa biofilms were more resistant to ceftazidime and meropenem than non-maturing biofilms, probably due to the gradual increase in β-lactamase levels biofilm maturation.13 In addition, enzymes with drug resistance are present in the microbiota of biofilms. Glucosyltransferase (ndvB) is a Pseudomonas aeruginosa biofilm-specific antibiotic resistance gene that functions in forming biofilms without defects and in altering microbial susceptibility by screening for random transposon mutants.14 Clinical reports have shown that ndvB-derived glucan can be detected in the blood of patients with Pseudomonas aeruginosa infection.15 In the case of the biofilm-based model of infection with slow-killing nematodes, cyclic glucans are vital for biofilm persistence.16
Physiological Heterogeneity, Hypoxia, and Reduced Growth Rate
Physiological heterogeneity is characterized by differences in gene expression, metabolic activity, and phenotype (including antimicrobial drug tolerance) of cells located in different regions of the biofilm. Heterogeneity arises due to a gradient of oxygen and other nutrients within the biofilm. Studies have shown an oxygen gradient between the various cell layers of the biofilm of each species. This oxygen gradient arises because most nutrients have been consumed when they penetrate the deep biofilm, leaving the deep biofilm in a hypoxic environment where the cells in this zone have little metabolic activity and are in a quiescent state. At the same time, antibiotics are usually effective against fast-growing cells, and the slow growth rate of the biofilm enhances resistance to antibiotics.17
Population Induction and the Efflux Pump
Population sensing affects the heterogeneous structure of cells. In a convenient nutrient supply and suitable environment, population sensing plays a crucial role in cell migration, thereby influencing the resistance of biofilms to antimicrobial drugs. A study found that the quorum-sensing regulatory molecule 2-heptyl-4-hydroxyquinoline-N-oxide (HQNO) inhibits the cytochrome BC1 complex in the electron transport chain, leading to Reactive Oxygen Species (ROS) accumulation and a decrease in membrane potential, ultimately leading to cellular autolysis, which helps to explain the population-sensing function in Pseudomonas aeruginosa biofilms.18 Autolysis leads to the release of eDNA and promotes antibiotic tolerance in the biofilm. Thus, the Pseudomonas aeruginosa population sensing contributes eDNA to the matrix through autolysis, thereby enhancing biofilm tolerance.
Bacterial efflux pumps can be divided into several superfamilies. Members of the Resistance-Nodulation-Division (RND) family have been most studied for bacterial biofilm resistance or biofilm formation, consisting of inner membrane proteins, periplasmic membrane fusion proteins, and outer membrane proteins.19 This complex spans the Gram-negative cell envelope and allows efficient translocation of a wide range of molecules. Bacteria use specific membrane-associated proteins to excrete large amounts of compounds from the cytoplasm. In combination with the reduced influx or enzymatic degradation of these compounds, the efflux pump is responsible for keeping the cytoplasmic concentration of certain antimicrobial compounds below a critical threshold.20
Genetic Profile
Bacteria can extract eDNA from the biofilm matrix and may also achieve horizontal gene transfer through intercellular transfer plasmids bound in the biofilm. Increased transcription of antibiotic resistance genes loaded with plasmids contributes to increased copy number in biofilms, indicating that resistance genes have a protective effect on biofilms.21
Integrons consist of genetic elements consisting of integration sites, promoters, and genes encoding integrases, where the role of integrases is to facilitate gene excision and integration. The current study found that integrons are present that frequently encode antibiotic resistance determinants clusters and are involved in transmitting resistance genes between bacteria in the clinical setting.22 In addition, integrase expression is upregulated in biofilms through a strict response, and the frequency of excision of antibiotic resistance genes is increased.23
Previously, resistance in biofilms was thought to be phenotypic and not due to genetic changes. However, it has been shown that microbial cells in biofilms mutate at a higher rate than scattered microbial cells and that these high-intensity mutations result in increased biofilm resistance to antibiotics. For example, highly mutated Pseudomonas aeruginosa with defective methyl mismatch repair or oxidative DNA repair systems are typically more resistant to antibiotics than strains with intact DNA repair mechanisms.24 Similarly, the frequency of mucin and rifampicin resistance mutations is higher in biofilms compared to planktonic cells.25
Progress in Research on Antimicrobial Materials for Tracheal Tubes
Active Antimicrobial Coatings
The most common antimicrobial coating method is to add antimicrobial materials directly. The polymer forms a matrix on the coating surface through covalent or ionic bonding to achieve the antimicrobial effect.26 The most common antimicrobial materials are phages, enzymes, nitric oxide (NO), antimicrobial peptides (AMPs), photoactivators, liposomes.27 Free fatty acids or natural lipophilic components from human tissues can be formulated into solid lipid nanoparticles.28 They produced them as coatings containing the non-toxic chemicals lauric and oleic acids, which acted on bacteria through various mechanisms at the nanoscale, including damaging bacteria leading to DNA release and reducing the adhesion of dead bacteria down to approximately 1%. In addition, the research found that incorporated the NO donor S-nitroso-N-acetyl penicillamine (SNAP) into endotracheal tubes by solvent swelling, and the impregnation of SNAP provided seven days of NO release without altering the mechanical properties of the ETs.29 At the same time, NORel-ETs successfully reduced bacterial infection by Pseudomonas aeruginosa, a common pathogen in VAP. In addition, researchers observed a significant reduction of biofilms by phages, especially for multi-drug resistant strains.30 In the study, two phages were selected as cocktail components considering anti-biofilm screening, and the ability of the cocktail to prevent settlement on the surface of tracheal tubes was tested in a dynamic biofilm model.30
However, simple antimicrobial coatings may be prone to delamination during use, thus compromising the antimicrobial effect, and the development of new active antimicrobial coatings has received extensive attention. In terms of surface modification of ET catheters, In terms of surface modification of ET catheters, observed the antimicrobial effect of the Nantong ET topology combined with sugar metabolites. After 24 hours, the presence of fructose on the surface of the nano-lenses reduced the number of planktonic Staphylococcus aureus in solution and biofilm formation on the surface.31 In addition, it was found that a Polyvinyl chloride (PVC) (HEMA: MAA) copolymer consisting of an 80:20 or 70:30 hydroxyethyl methacrylate (HEMA): methacrylic acid (MAA) ratio could be used as a tracheal tube coating in combination with clinical nebulization with gentamicin for the prevention of ventilator-associated pneumonia.32 A study developed poly (lauryl acrylate) nanocapsules containing eugenol (4-allyl-2-methoxy phenol) nanocapsules mediated by the slow release of natural antimicrobial agents to enhance the performance of the repellent polymer coating and entrap it in an interpenetrating network designed to repel bacteria.33 When applied to catheters and tracheal tubes, this hemocompatible system allowed for the slow release of eugenol, resulting in a significant reduction in surface-bound Klebsiella pneumoniae and methicillin-resistant Staphylococcus aureus (MRSA). Furthermore, When blended a conventional biomedical grade polyurethane, Tecoflex, with 10wt% UP-C12-50-T to alter the surface properties of the polyurethane fundamentally and with biocompatibility, the model coating with a certain level of P-C12-50 combines a high antimicrobial effect with low toxicity to human cells.34 While developing new antimicrobial materials, sphingosine and phytosphingosine coatings be stable in vivo and non-toxic to airway epithelial cells without inducing an inflammatory response, and such antimicrobial coatings are effective against Staphylococcus aureus, Acinetobacter baumannii, and Pseudomonas aeruginosa.35 A novel styrene-based antimicrobial agent (BCP3) also showed significant growth inhibition against Staphylococcus aureus and Pseudomonas aeruginosa, with a more substantial effect on Staphylococcus aureus.36 BCP3 showed no cytotoxicity against mammalian (L929) fibroblasts.36 In addition, a covalent construction of polyhexamethylene biguanide (PHMB) as an efficient bactericidal coating on silicone rubber (SR) could kill 100% of Staphylococcus aureus cells within one hour with an initial density of less than 1.18×105 CFU/cm2 without affecting the cytocompatibility of the substrate.37 At the same time, the coating dramatically increases the mechanical properties of the SR substrate due to the additional cross-linking introduced by the coating.37 The synergistic anti-biofilm activity of citral and thymol was recently demonstrated, and without altering the growth and metabolic viability of methicillin-resistant Staphylococcus aureus, the anti-biofilm activity of the coating was unaffected by plasma modulation. In addition, the anti-biofilm coating was non-hemolytic and non-toxic to peripheral blood mononuclear cells.38
Silver and Silver Nanoparticles
Silver ions alter fundamental processes by interacting strongly with bacterial cellular components. It is capable of causing effects including disruption of cellular proteins, disruption of cell signaling, increased cell membrane permeability, generation of free radicals, and ultimately bacterial cell death.39 In an animal model of mechanical ventilation, tracheal cannulae coated with antimicrobial silver showed delayed and reduced bacterial colonisation.40 New antimicrobial tracheal cannulae coated with nanosilver/polyurethane had more potent antimicrobial and anti-biofilm proliferation properties.41 In a prospective randomized clinical trial using silver sulfadiazine (SSD)-coated ET, it was demonstrated that SSD-ET could be safely used to prevent bacterial colonization of the ET surface in patients intubated for up to 24 hours.42 A multicentre prospective study found a 36% reduction in the relative risk of VAP in patients intubated with a silver-plated tube but did not show a reduction in mechanical ventilation time, ICU length of stays, or mortality.43 However, a meta-analysis showed that silver-coated ETs effectively reduced VAP risk and in-hospital mortality in patients requiring mechanical ventilation for 24 hours or longer, particularly during the first ten days of mechanical ventilation, compared with standard uncoated ETs.44
Although much research has been conducted on silver antibacterial materials, the biocompatibility and mechanical properties need to be further investigated. We know that silver ions are usually deposited on the surface or mesopores by physical adsorption or ion exchange. It was found that Pseudomonas aeruginosa adhered less to nanorough PVC than conventional PVC using a vortex method to remove biofilms and bacteria.45 Whereas, by modifying the PVC surface using a combination of solvents (tetrahydrofuran) and non-solvents (ethanol and methanol), the superhydrophobic PVC surface prepared, the initial attachment time of Pseudomonas aeruginosa PAO1 was delayed to 18 and 24 h, respectively.46 In addition, silver nanolayers of different thicknesses were sputtered on polyimide PI and sputtered with Gram-negative and Gram-positive bacterial strains. The antibacterial properties of the sputtered and annealed samples were investigated, and the inhibition of bacterial strains increased significantly after annealing.47 Prepared silica-based Ag+ coatings usable on ET by combining the composites SiO2/c-KH-570 and SiO2/KH-570/MTES with polyethylene (PE) through a sol-gel process. Antimicrobial tests showed that the composite antimicrobial coatings inhibited Escherichia coli by 93.5%, with no significant increase in antimicrobial activity when the Ag concentration was higher than 2.6%.48 Recently, a study found that a novel polyamide with a good hydrophilic/hydrophobic molecular balance was used to embed green reduced silver nanoparticles (AgNPs) in composite coated ETs.49 Compared with the uncoated ET, the coating inhibited the adhesion and growth of bacterial flora on the ET surface, providing a rapid bactericidal effect, especially for Pseudomonas aeruginosa and Staphylococcus aureus.
Currently, silver nanoparticles are increasingly favored for the preparation of ET. Therefore, the cytotoxicity and deposition of silver nanomaterials in vital organs are of significant concern. Researchers believe that an essential mechanism for the cytotoxicity of AgNP is the release of metal ions upon entry of metal nanomaterials into the organism, which dissolves in the cells, causing metal overload and ultimately activating reactive oxygen species.50–52 AgNP has significant size-dependent toxicity, and the intensity of toxicity correlates with the rate of intracellular Ag release.53 Therefore, the bio-mediated synthesis of NPs may be a better option. Synthesized Ag NPs using hydrogel beads based on k-Carrageenan as antimicrobial agents found to be effective against Staphylococcus aureus, methicillin-resistant Staphylococcus aureus, Pseudomonas aeruginosa, and Escherichia coli.54 Recently, researchers formed swollen polyelectrolytes by in situ reductions of AgNPs by deposition on aqueous LbL Antimicrobial and biofilm-protected ETs were prepared in pre-coated layers of the matrix.55 The whole fabrication process was from the green chemistry perspective and included all fabrication using an aqueous medium, a natural reducing agent of lemon eucalyptus leaf extract, and a biocompatible polyelectrolyte material for the encapsulation of AgNPs. The coating was uniformly distributed over the surface of the bend, the surface of the film, and the interior of the catheter. The encapsulated ET inhibited the adhesion of Staphylococcus aureus and Gram-negative Pseudomonas aeruginosa by 99.9% and 99.99%, respectively (p<0.05). In addition, a new ETT coated with a sub-micron layer of noble metal alloy (NMA) of gold, silver, and palladium does not significantly release metals into the body, causing Bactiguard infection protection (BIP). Clinical studies have found a delayed onset of VAP and a trend toward decreased antibiotic use in the group of patients coated with NMA compared to controls.56
Notably, the accumulation of mucus can reduce the antimicrobial activity of silver-coated ETs by isolating bacterial colonization from the silver surface. One study wanted to enhance the antimicrobial performance of silver-coated ETs by regular removal of airway secretions. Still, the regular removal of airway secretions did not reduce bacterial colonization of ETs compared to standard aspiration, nor did it reduce airway colonization.57
Antimicrobial Metal and Composite ET Coatings
In addition to silver, selenium, and zinc and their oxides, among others, are incorporated into or coated on polymer surfaces. Selenium (Se) acts as an antimicrobial agent because, unlike silver, it is a trace element (55–70 mg per day) and is necessary for the production of the endogenous antioxidant selenoprotein. The antimicrobial activity of selenium is attributed to the catalytic oxidation of intracellular sulfhydryl groups, which induces apoptosis.58 Selenium nanoparticles (SeNP) deposited in large amounts on PVC and that SeNP coatings had better antimicrobial activity against Staphylococcus aureus compared to silver-plated PVC-ETs.59 ZnO nanoparticles also could further enhance their antimicrobial properties.60 While developing the antibacterial properties of metal nanomaterials, the cytotoxicity of the materials cannot be ignored. It is currently believed that metal oxide nanoparticle-induced toxicity is related to the nanoparticles’ nature (size, surface area, shape, crystallinity) and their corresponding ability to induce ROS. SeNPs promote intracellular ROS production, and the amount of intracellular ROS production is highly correlated with the diameter of SeNPs.61 Cytotoxicity of silicon dioxide is related to ROS, and the intensity of toxicity is related to its size.62 ZnO nanoparticles are less toxic than other metal oxides and are also associated with ROS induction.63,64 Therefore, the search for new green materials is more applicable to biomedicine. Recently, in a study, an environmentally friendly and harmless ZnO nanoparticle biosynthesized by Escherichia coli was identified. The biosynthetic ZnO NPs showed antibacterial and anti-biofilm activity in combination with antibiotics. They can be used against multidrug-resistant bacteria and coated on medical materials.65 Attempts have been made to develop composite ET coatings combining metals with other biomaterials, A hybrid coating based on dextran grafted to a substrate and embedded with AgNPs was present.66 In terms of its antimicrobial activity, DEX-Ag2 is more resistant to bacterial adhesion than DEX-Ag5, which in turn is better than dextran and silicon. D-tyrosine has been found to penetrate bacterial cell membranes to exchange with D-alanine within the membrane, thereby reducing the affinity between the bacteria and the biofilm matrix, and can be achieved by adding 1–15 wt% Ag to PVC ET, zeolite, and antifouling D-tyrosine coatings to achieve the antibacterial effect.67 In addition, it was found that used the precursor methyltrimethoxysilane (MTMS) to form a superhydrophobic surface on the samples by preparing different silica sols through alkali hydrolysis, which significantly reduced the adhesion of bacteria.68 For clinical studies, compared the grade of biofilm formation on ETs made of uncoated PVC, silica-coated PVC, and metal-coated PVC after > 24 hours of mechanical ventilation in critically ill patients. The study demonstrated that the formation of high-grade biofilm on ETs was associated with VAP development. Silica-coated and precious metal-coated PVC ETs were independently associated with a reduction in high-grade biofilm formation compared to uncoated PVC ETs.69
Photocatalytic Antibacterial Materials
Methylene blue (MB) is a photosensitizer that can effectively destroy microorganisms. Microorganisms can absorb methylene blue under excitation of 664 nm, proton transfer produces reactive radicals, as well as molecular oxygen and single linear state oxygen formed by MB, and these oxidized radicals cause cell damage. The study demonstrated that in the Clinical tracheal intubation model, sprayed MB solutions were tested in the trachea, and photoactivation was induced using optical fibers passing. The results showed a 1-log reduction in bacterial colonization of MB-ETs in the absence of light and a 3-log reduction in bacterial colonization of MB-ETs after light exposure.70
Activation of TiO2 as a photoactivated compound for photocatalysts at approximately 385 nm leads to the production of electron holes that are detrimental to bacterial ROS.71 Researchers found that both silver-containing sol-gel TiO2 and silver-containing Degussa TiO2 weakened the growth of Pseudomonas aeruginosa but had no effect on Staphylococcus aureus colonization showed no effect.72 Subsequently, it was confirmed that the silver-mounted titanium dioxide (TiO2) antimicrobial-coated endotracheal tube had good antimicrobial properties and correlated with the concentration of the antimicrobial agent, showing a strong antimicrobial effect when the antimicrobial concentration was above 1.0% and bacteria were almost completely killed in the soaking solution.73 Also, in mechanical ventilation animal studies, the Ag-TiO2 antimicrobial-coated endotracheal tube oral mucosa irritation test was confirmed to be negative, which met the national standard for the biological evaluation of medical devices.74 In further studies, the activation wavelength of iodine-modified TiO2 (I-TiO2) was shifted to visible light to observe its photocatalytic antibacterial properties.75 Also, I-TiO2 PVC was designed to resist Escherichia coli attack in an in vitro antimicrobial test. Ultimately, the study confirmed that the iodine-modified titanium dioxide (I-TiO2) PVC-ETs antimicrobial coating prevents bacterial growth and bacterial damage to tissues. Furthermore, comparing TiO2 tracheal catheters with nitrogen-modified TiO2, both inhibited bacterial growth under visible fluorescence.76 However, compared to TiO2, N-TiO2 showed higher antibacterial activity against Staphylococcus aureus and did not significantly improve the sensitivity of Pseudomonas aeruginosa, but the photocatalytic efficiency was species-dependent, and N-doping could improve its broad-spectrum application.77 In addition, TiO2 also has certain antibacterial properties against fungi. The study confirmed that the Ag-TiO2 antibacterial coated tracheal catheter showed a gradual decrease in the number of fungal colonies on the Schachter plate as the concentration of Ag-TiO2 continued to increase, while the inhibition rate gradually increased, indicating that the test catheter had a significant inhibitory effect on fungal growth in a concentration-dependent manner. 0.8% was the Ag-TiO2 0.8% is the critical concentration of Ag-TiO2, and the inhibition effect is not obvious below this concentration. The test results show that the test catheter has a similar inhibitory ability to sensitive and resistant fungi, which may be related to the mechanism of Ag-TiO2 and fungal inhibition, through the photocatalytic generation of free radicals can destroy the cell wall, and then enter the inner cell to destroy the inner membrane and various components leading to cell death.78
Photodynamic therapy is a non-invasive alternative to microbial inactivation, which combines light with photosensitive molecules to produce reactive oxygen species, which in turn causes bacterial death. Researchers used the photosensitizer (PS) curcumin, a light source of 450 nm LED, to determine its bactericidal effect on ET biofilms. The highest microbial inactivation was observed at 1.25 mg/mL curcumin, 2 h of PS incubation, and 50 J/cm2, with a 70% reduction in biofilm.79 Furthermore, under blue light activation (450 nm), curcumin-functionalized tracheids (ETT-curc) exhibited substantial photodynamic inactivation against Escherichia coli, Staphylococcus aureus, and Pseudomonas aeruginosa, and no degradation or leaching of ETT-curc occurred over a range of pH values.80 Then a study combined molecular oxygen, a non-toxic PS, and light at the appropriate wavelength, resulting in the formation of cytotoxic reactive oxygen species.81 The prevention of secondary infections achieved during the use of photosensitizer-enabled tracheal catheters provides the basis for what may become a greater clinical approach to the treatment of respiratory infections.
Antimicrobial Peptides
AMPs, as endogenous polyamines, can display nonspecific spectral antimicrobial activity by interacting with negatively charged microbial cell membranes. Researchers achieved their antimicrobial effects by synthesizing a class of small molecules, nonpeptides (ceragenins), that mimic the properties of AMPs.82 Ceragenins exhibit broad-spectrum antibacterial and antifungal properties that can inhibit endotoxins from reducing inflammation and exhibit good antidegradation properties, all of which are suitable for studying antimicrobial coatings on ET. Next, incorporated ceragenin CSA-131 into polyurethane hydrogels dip-coated on PVC ET and studied CSA-131 using Pseudomonas aeruginosa, MRSA, Klebsiella pneumoniae, Candida albicans, and Staphylococcus aureus. The antimicrobial properties of PVC ETs with CSA-131 applied as an antimicrobial coating on ETs showed a significant reduction in biofilm formation and inflammation.82 Another study compared ceragenin CSA-131-coated ETs and uncoated ETs. This study showed that biofilm formation was significantly reduced in coated ETs. Notably, the difference in Staphylococcus aureus was not statistically significant.83 Therefore, a more in-depth study of ceragenins and other AMPs to prevent and reduce VAP and other intubation-related complications is warranted (Table 1).
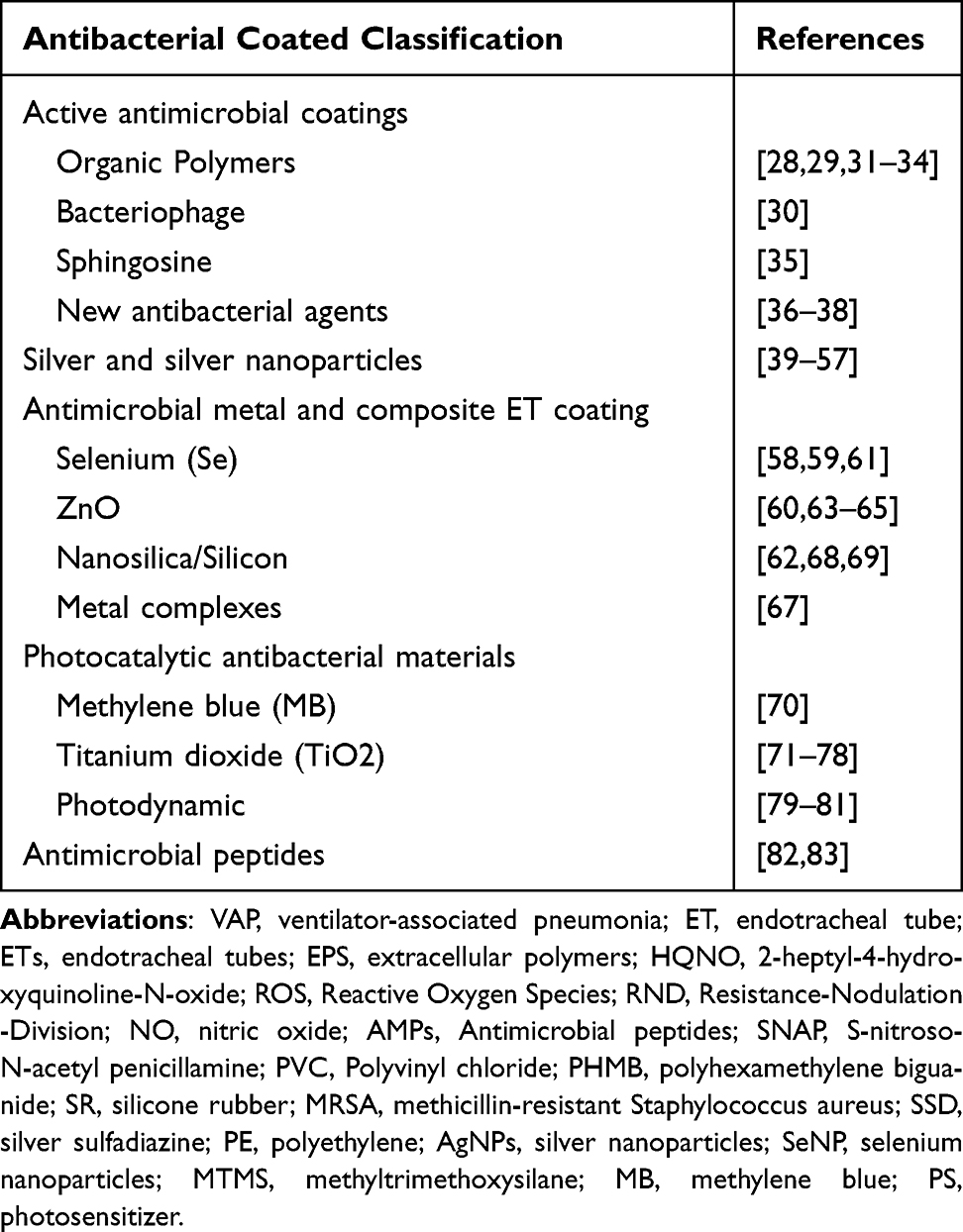 |
Table 1 Antibacterial Coated Tracheal Tubes: Progress |
Prospects and Challenges
VAP is a common hospital-acquired infection in mechanically ventilated patients. Microbial colonization of the ET surface is one of the leading causes of VAP. Biofilm-based infections are difficult to eradicate, and bacterial biofilms significantly increase morbidity and mortality in patients with VAP. This paper discusses the many mechanisms of biofilm resistance, such as biofilm heterogeneity and nutrient limitation, that have been shown to contribute to enhanced biofilm resistance and resistance to antibiotics. At the same time, studies have confirmed that the underlying mechanisms of antibiotic resistance and tolerance in biofilms have a genetic basis in many cases. However, many questions about biofilm resistance remain to be answered. Ideally, different pathogens have different biofilm-specific antibiotic resistance mechanisms, which will facilitate the development of therapeutic approaches that are targeted to disrupt these pathogen-specific mechanisms.
The fact that systemic antibiotic use has little effect on airway colonization has led to a growing number of researchers exploring antimicrobial coated tracheal catheters as a method of preventing VAP. As discussed in this paper, numerous antimicrobial materials are now widely studied, such as silver nanoparticles, antimicrobial metal, composite ET coatings, and photocatalytic antimicrobial materials, showing excellent antimicrobial properties. The high cost of moving from in vitro and animal studies to clinical trials has led most studies to stay in the preclinical stage. Recently, however, researchers have begun to conduct relevant prospective trials to test the clinical use of antimicrobial materials. Clinically, numerous factors influence the development and persistence of ET biofilm, the duration of treatment of the patient’s disease, catheter contamination during tracheal intubation, the depth of tracheal intubation depending on age and gender, the effect of physiological contact between the tracheal tube and the lower airway on airflow, and the movement of tissue secretions caused by the adjustment of air sac inflation and deflation. However, we believe that considering these relevant factors and developing refined experimental protocols will help overcome these challenges. Furthermore, achieving the leap from observing the antimicrobial properties of antimicrobial polymers against a single species forming biofilms to developing antimicrobial ETs against complex VAP infections and designing more refined representatives of VAP pathogens in test models is a subsequent direction for researchers. Therefore, the development and optimization of standard assessment methods regarding biofilm antimicrobial properties and cytotoxicity are key to comparing materials already researched and developed with new materials under development, which will help facilitate subsequent experiments.
In conclusion, further research on larger populations is needed to better characterize the microorganisms associated with biofilms. A more in-depth exploration of the complex factors affecting antibiotic resistance in biofilms will provide us with new ideas to reduce VAP incidence. Antimicrobial surface coatings or modified antimicrobial coatings have been applied to ET and will continue to be researched and developed to develop a broader market prospect. Antimicrobial materials are mainly divided into passive and active materials. Passive approaches can reduce bacterial adhesion, and reduce the likelihood of biofilm formation, which is more beneficial than the potential problems of dosing or leaching of some active antimicrobial materials. Ideally, either combination of passive and active materials approaches is superior, providing limitation of bacterial adhesion and simultaneous provision of biocidal activity. Once successful materials have been developed, their application in a clinical setting could help reduce the microbial load on ET surfaces and the resulting potential complications and mortality caused by VAP.
Acknowledgments
This study was supported by Science and Technology Planning Project of Guangdong Province, China (No. 2017B020235001).
Disclosure
The authors have no financial or non-financial conflicts of interest for this work.
References
1. Mehta A, Bhagat R. Preventing ventilator-associated infections. Clin Chest Med. 2016;37(4):683–692. doi:10.1016/j.ccm.2016.07.008
2. Zhao Q, Yang LP. Effect observation of airway management optimization to prevent (P<0.05) in patients undergoing mechanical ventilation. Nurs Pract Res. 2018;15(13):29–31.
3. Hawe CS, Ellis KS, Cairns CJS, Longmate A. Reduction of ventilator-associated pneumonia: active versus passive guideline implementation. Intensive Care Med. 2009;35(7):1180–1186. doi:10.1007/s00134-009-1461-0
4. Redman LR, Lockey E. Colonisation of the upper respiratory tract with Gram-negative bacilli after operation, endotracheal intubation and prophylactic antibiotic therapy. Anaesthesia. 1967;22(2):220–227. doi:10.1111/j.1365-2044.1967.tb02722.x
5. Sottile FD, Marrie TJ, Prough DS, et al. Nosocomial pulmonary infection: possible etiologic significance of bacterial adhesion to endotracheal tubes. Crit Care Med. 1986;14(4):265–270. doi:10.1097/00003246-198604000-00001
6. Carvalho I, Henriques M, Carvalho S. New Strategies to Fight Bacterial Adhesion. Microbial Pathogens and Strategies for Combating Them: Science, Technology and Education. Formatex Research Center. 2013:170–178.
7. Săndulescu O. Managing sticky situations - anti-biofilm agents. Germs. 2016;6(2):49. doi:10.11599/germs.2016.1088
8. Boulané-Petermann L. Processes of bioadhesion on stainless steel surfaces and cleanability: a review with special reference to the food industry. Biofouling. 1996;10(4):275–300. doi:10.1080/08927019609386287
9. Chmielewski RAN, Frank JF. Biofilm formation and control in food processing facilities. Compr Rev Food Sci Food Saf. 2003;2(1):22–32. doi:10.1111/j.1541-4337.2003.tb00012.x
10. Otto M. Staphylococcus epidermidis pathogenesis. Methods Mol Biol. 2014;1106:17–31. doi:10.1007/978-1-62703-736-5_2
11. Wimpenny J, Manz W, Szewzyk U. Heterogeneity in biofilms. FEMS Microbiol Rev. 2000;24(5):661–671. doi:10.1111/j.1574-6976.2000.tb00565.x
12. Kim KY, Frank JF. Effect of nutrients on biofilm formation by Listeria monocytogenes on stainless steel. J Food Prot. 1995;58(1):24–28. doi:10.4315/0362-028X-58.1.24
13. Sugano M, Morisaki H, Negishi Y, et al. Potential effect of cationic liposomes on interactions with oral bacterial cells and biofilms. J Liposome Res. 2016;26(2):156–162. doi:10.3109/08982104.2015.1063648
14. Mah TF, Pitts B, Pellock B, Walker GC, Stewart PS, O’Toole GA. A genetic basis for Pseudomonas aeruginosa biofilm antibiotic resistance. Nature. 2003;426(6964):306–310. doi:10.1038/nature02122
15. Koya J, Nannya Y, Kobayashi H, Okugawa S, Moriya K, Kurokawa M. Simultaneous increase in 1,3-β-D-glucan and procalcitonin levels in Pseudomonas aeruginosa infection. J Infect. 2013;67(2):164–166. doi:10.1016/j.jinf.2013.03.017
16. Zhang L, Fritsch M, Hammond L, et al. Identification of genes involved in Pseudomonas aeruginosa biofilm-specific resistance to antibiotics. PLoS One. 2013;8(4):e61625. doi:10.1371/journal.pone.0061625
17. Stewart P, Zhang T, Xu R, et al. Reaction-diffusion theory explains hypoxia and heterogeneous growth within microbial biofilms associated with chronic infections. NPJ Biofilms Microbiomes. 2016;2. doi:10.1038/npjbiofilms.2016.12
18. Hazan R, Que YA, Maura D, et al. Auto poisoning of the respiratory chain by a quorum-sensing-regulated molecule favors biofilm formation and antibiotic tolerance. Curr Biol. 2016;26(2):195–206. doi:10.1016/j.cub.2015.11.056
19. Nikaido H. Structure and mechanism of RND-type multidrug efflux pumps. Adv Enzymol Relat Areas Mol Biol. 2011;77:1–60. doi:10.1002/9780470920541.ch1
20. Soto SM. Role of efflux pumps in the antibiotic resistance of bacteria embedded in a biofilm. Virulence. 2013;4(3):223–229. doi:10.4161/viru.23724
21. Cook LC, Dunny GM. Effects of biofilm growth on plasmid copy number and expression of antibiotic resistance genes in Enterococcus faecalis. Antimicrob Agents Chemother. 2013;57(4):1850–1856. doi:10.1128/AAC.02010-12
22. Gillings MR. Integrons: past, present, and future. Microbiol Mol Biol Rev. 2014;78(2):257–277. doi:10.1128/MMBR.00056-13
23. Strugeon E, Tilloy V, Ploy MC, Da Re S. The stringent response promotes antibiotic resistance dissemination by regulating integron integrase expression in biofilms. mBio. 2016;7(4). doi:10.1128/mBio.00868-16
24. Mandsberg LF, Ciofu O, Kirkby N, Christiansen LE, Poulsen HE, Høiby N. Antibiotic resistance in Pseudomonas aeruginosa strains with increased mutation frequency due to inactivation of the DNA oxidative repair system. Antimicrob Agents Chemother. 2009;53(6):2483–2491. doi:10.1128/AAC.00428-08
25. Ryder VJ, Chopra I, O’Neill AJ. Increased mutability of Staphylococci in biofilms as a consequence of oxidative stress. PLoS One. 2012;7(10):e47695. doi:10.1371/journal.pone.0047695
26. Polívková M, Hubáček T, Staszek M, Švorčík V, Siegel J. Antimicrobial treatment of polymeric medical devices by silver nanomaterials and related technology. Int J Mol Sci. 2017;18(2):419. doi:10.3390/ijms18020419
27. Dizaj SM, Lotfipour F, Barzegar-Jalali M, Zarrintan MH, Adibkia K. Antimicrobial activity of the metals and metal oxide nanoparticles. Mater Sci Eng C Mater Biol Appl. 2014;44:278–284. doi:10.1016/j.msec.2014.08.031
28. Taylor EN, Kummer KM, Dyondi D, Webster TJ, Banerjee R. Multi-scale strategy to eradicate Pseudomonas aeruginosa on surfaces using solid lipid nanoparticles loaded with free fatty acids. Nanoscale. 2014;6(2):825–832. doi:10.1039/c3nr04270g
29. Homeyer KH, Singha P, Goudie MJ, Handa H. S ‐Nitroso‐ N‐ acetylpenicillamine impregnated endotracheal tubes for prevention of ventilator‐associated pneumonia. Biotechnol Bioeng. 2020;117(7):2237–2246. doi:10.1002/bit.27341
30. Oliveira VC, Macedo AP, Melo LDR, et al. Bacteriophage cocktail-mediated inhibition of Pseudomonas aeruginosa biofilm on endotracheal tube surface. Antibiotics. 2021;10(1):78. doi:10.3390/antibiotics10010078
31. Durmus NG, Taylor EN, Inci F, Kummer KM, Tarquinio KM, Webster TJ. Fructose-enhanced reduction of bacterial growth on nanorough surfaces. Int J Nanomedicine. 2012;7:537–545. doi:10.2147/IJN.S27957
32. Jones DS, McCoy CP, Andrews GP, McCrory RM, Gorman SP. Hydrogel antimicrobial capture coatings for endotracheal tubes: a pharmaceutical strategy designed to prevent ventilator-associated pneumonia. Mol Pharm. 2015;12(8):2928–2936. doi:10.1021/acs.molpharmaceut.5b00208
33. Venkateswaran S, Henrique Dos Santos OD, Scholefield E, et al. Fortified interpenetrating polymers - bacteria resistant coatings for medical devices. J Mater Chem B. 2016;4(32):5405–5411. doi:10.1039/c6tb01110a
34. Wang C, Zolotarskaya O, Ashraf KM, Wen X, Ohman DE, Wynne KJ. Surface characterization, antimicrobial effectiveness, and human cell response for a biomedical grade polyurethane blended with a mixed soft block PTMO-quat/PEG copolyoxetane polyurethane. ACS Appl Mater Interfaces. 2019;11(23):20699–20714. doi:10.1021/acsami.9b04697
35. Seitz AP, Schumacher F, Baker J, et al. Sphingosine-coating of plastic surfaces prevents ventilator-associated pneumonia. J Mol Med. 2019;97(8):1195–1211. doi:10.1007/s00109-019-01800-1
36. Ozcelik B, Pasic P, Sangwan P, et al. Evaluation of the novel antimicrobial BCP3 in a coating for endotracheal tubes. ACS Omega. 2020;5(18):10288–10296. doi:10.1021/acsomega.9b04178
37. Peng W, Yin H, Liu P, et al. Covalently construction of poly (hexamethylene biguanide) as high-efficiency antibacterial coating for silicone rubber. Chem Eng J. 2021;412:128707. doi:10.1016/j.cej.2021.128707
38. Valliammai A, Selvaraj A, Mathumitha P, Aravindraja C, Pandian SK. Polymeric antibiofilm coating comprising synergistic combination of citral and thymol prevents methicillin-resistant Staphylococcus aureus biofilm formation on titanium. Mater Sci Eng. 2021;121:111863. doi:10.1016/j.msec.2021.111863
39. Hemeg HA. Nanomaterials for alternative antibacterial therapy. Int J Nanomedicine. 2017;12:8211–8225. doi:10.2147/IJN.S132163
40. Olson ME, Harmon BG, Kollef MH. Silver-coated endotracheal tubes associated with reduced bacterial burden in the lungs of mechanically ventilated dogs. Chest. 2002;121(3):863–870. doi:10.1378/chest.121.3.863
41. Hu Y, Ji X, Wei D, Deng J. Antibacterial properties and application of nanosilver material in the tracheal tube. J Nanosci Nanotechnol. 2020;20(10):6542–6546. doi:10.1166/jnn.2020.18520
42. Berra L, Kolobow T, Laquerriere P, et al. Internally coated endotracheal tubes with silver sulfadiazine in polyurethane to prevent bacterial colonization: a clinical trial. Intensive Care Med. 2008;34(6):1030–1037. doi:10.1007/s00134-008-1100-1
43. Kollef MH, Afessa B, Anzueto A, et al. Silver-coated endotracheal tubes and incidence of ventilator-associated pneumonia: the NASCENT randomized trial. JAMA. 2008;300(7):805–813. doi:10.1001/jama.300.7.805
44. Tokmaji G, Vermeulen H, Müller MCA, Kwakman PHS, Schultz MJ, Zaat SAJ. Silver-coated endotracheal tubes for prevention of ventilator-associated pneumonia in critically ill patients. Cochrane Database Syst Rev. 2015;(8):CD009201. doi:10.1002/14651858.CD009201.pub2
45. Seil JT, Rubien NM, Webster TJ, Tarquinio KM. Comparison of quantification methods illustrates reduced Pseudomonas aeruginosa activity on nanorough polyvinyl chloride. J Biomed Mater Res B Appl Biomater. 2011;98(1):1–7. doi:10.1002/jbm.b.31821
46. Loo CY, Young PM, Lee WH, Cavaliere R, Whitchurch CB, Rohanizadeh R. Superhydrophobic, nanotextured polyvinyl chloride films for delaying Pseudomonas aeruginosa attachment to intubation tubes and medical plastics. Acta Biomaterialia. 2012;8(5):1881–1890. doi:10.1016/j.actbio.2012.01.015
47. Polivkova M, Siegel J, Kolarova K, Rimpelova S, Svorcik V. Silver nanostructures sputtered on polyimide: surface characterization and antibacterial properties. Chem Listy. 2016;110(2):139–143.
48. Jiang X, Lv B, Shen Q, Wang X. Preparation of silicon-modified antimicrobial polyethylene endotracheal tubes. J Biomed Mater Res B Appl Biomater. 2017;105(1):91–98. doi:10.1002/jbm.b.33530
49. Lethongkam S, Daengngam C, Tansakul C, et al. Prolonged inhibitory effects against planktonic growth, adherence, and biofilm formation of pathogens causing ventilator-associated pneumonia using a novel polyamide/silver nanoparticle composite-coated endotracheal tube. Biofouling. 2020;36(3):292–307. doi:10.1080/08927014.2020.1759041
50. Setyawati MI, Yuan X, Xie J, Leong DT. The influence of lysosomal stability of silver nanomaterials on their toxicity to human cells. Biomaterials. 2014;35(25):6707–6715. doi:10.1016/j.biomaterials.2014.05.007
51. Strauch BM, Hubele W, Hartwig A. Impact of endocytosis and lysosomal acidification on the toxicity of copper oxide nano- and microsized particles: uptake and gene expression related to oxidative stress and the DNA damage response. Nanomaterials. 2020;10(4):E679. doi:10.3390/nano10040679
52. Delaval M, Wohlleben W, Landsiedel R, Baeza-Squiban A, Boland S. Assessment of the oxidative potential of nanoparticles by the cytochrome c assay: assay improvement and development of a high-throughput method to predict the toxicity of nanoparticles. Arch Toxicol. 2017;91(1):163–177. doi:10.1007/s00204-016-1701-3
53. Gliga AR, Skoglund S, Wallinder IO, Fadeel B, Karlsson HL. Size-dependent cytotoxicity of silver nanoparticles in human lung cells: the role of cellular uptake, agglomeration and Ag release. Part Fibre Toxicol. 2014;11:11. doi:10.1186/1743-8977-11-11
54. Azizi S, Mohamad R, Abdul Rahim R, Mohammadinejad R, Bin Ariff A. Hydrogel beads bio-nanocomposite based on Kappa-Carrageenan and green synthesized silver nanoparticles for biomedical applications. Int J Biol Macromol. 2017;104(Pt A):423–431. doi:10.1016/j.ijbiomac.2017.06.010
55. Daengngam C, Lethongkam S, Srisamran P, et al. Green fabrication of anti-bacterial biofilm layer on endotracheal tubing using silver nanoparticles embedded in polyelectrolyte multilayered film. Mater Sci Eng C Mater Biol Appl. 2019;101:53–63. doi:10.1016/j.msec.2019.03.061
56. Damas P, Legrain C, Lambermont B, et al. Prevention of ventilator-associated pneumonia by noble metal coating of endotracheal tubes: a multi-center, randomized, double-blind study. Ann Intensive Care. 2022;12:1. doi:10.1186/s13613-021-00961-y
57. Pirrone M, Imber DA, Marrazzo F, et al. Silver-coated endotracheal tubes cleaned with a mechanism for secretion removal. Respir Care. 2019;64(1):1–9. doi:10.4187/respcare.06222
58. Ramos JF, Webster TJ. Cytotoxicity of selenium nanoparticles in rat dermal fibroblasts. Int J Nanomedicine. 2012;7:3907–3914. doi:10.2147/IJN.S33767
59. Tran PA, Webster TJ. Antimicrobial selenium nanoparticle coatings on polymeric medical devices. Nanotechnology. 2013;24(15):155101. doi:10.1088/0957-4484/24/15/155101
60. Seil JT, Webster TJ. Reduced Staphylococcus aureus proliferation and biofilm formation on zinc oxide nanoparticle PVC composite surfaces. Acta Biomater. 2011;7(6):2579–2584. doi:10.1016/j.actbio.2011.03.018
61. Huang T, Holden JA, Heath DE, O’Brien-Simpson NM, O’Connor AJ. Engineering highly effective antimicrobial selenium nanoparticles through control of particle size. Nanoscale. 2019;11(31):14937–14951. doi:10.1039/c9nr04424h
62. Inoue M, Sakamoto K, Suzuki A, et al. Size and surface modification of silica nanoparticles affect the severity of lung toxicity by modulating endosomal ROS generation in macrophages. Part Fibre Toxicol. 2021;18(1):21. doi:10.1186/s12989-021-00415-0
63. Huang YW, Wu CH, Aronstam RS. Toxicity of transition metal oxide nanoparticles: recent insights from in vitro studies. Materials. 2010;3(10):4842–4859. doi:10.3390/ma3104842
64. Pati R, Das I, Mehta RK, Sahu R, Sonawane A. Zinc-oxide nanoparticles exhibit genotoxic, clastogenic, cytotoxic and actin depolymerization effects by inducing oxidative stress responses in macrophages and adult mice. Toxicol Sci. 2016;150(2):454–472. doi:10.1093/toxsci/kfw010
65. Suhad H, Neihaya HZ, Raghad AL. Synergic effect of biosynthesized ZnO- nanoparticles with some antibiotic on multi-drug resistance bacteria. Ann RSCB. 2021;25:2293–2305.
66. Ferrer MCC, Hickok NJ, Eckmann DM, Composto RJ. Antibacterial biomimetic hybrid films. Soft Matter. 2012;8(8):2423–2431. doi:10.1039/c2sm06969e
67. Milenkovic J, Hrenovic J, Goic-Barisic I, Tomic M, Djonlagic J, Rajic N. Synergistic anti-biofouling effect of Ag-exchanged zeolite and D-Tyrosine on PVC composite against the clinical isolate of Acinetobacter baumannii. Biofouling. 2014;30(8):965–973. doi:10.1080/08927014.2014.959941
68. Mishra A, Loganathan H, Bhatt N. Preparation and characterization of nanosilica based superhydrophobic antimicrobial coatings and evaluation of bacterial adhesion on coated surface. Trends Biomater Artif Organs. 2019;33(3):64–68.
69. Thorarinsdottir HR. Biofilm formation on three different endotracheal tubes: a prospective clinical trial. Critical Care. 2020;24:12.
70. Biel MA, Sievert C, Usacheva M, et al. Reduction of endotracheal tube biofilms using antimicrobial photodynamic therapy. Lasers Surg Med. 2011;43(7):586–590. doi:10.1002/lsm.21103
71. Foster HA, Ditta IB, Varghese S, Steele A. Photocatalytic disinfection using titanium dioxide: spectrum and mechanism of antimicrobial activity. Appl Microbiol Biotechnol. 2011;90(6):1847–1868. doi:10.1007/s00253-011-3213-7
72. Tarquinio KM, Kothurkar NK, Goswami DY, Sanders RC, Zaritsky AL, LeVine AM. Bactericidal effects of silver plus titanium dioxide-coated endotracheal tubes on Pseudomonas aeruginosa and Staphylococcus aureus. Int J Nanomedicine. 2010;5:177–183. doi:10.2147/IJN.S8746
73. Jiang X, Wang Y, Hua J, Lyu B. [Study on antibacterial property of silver loaded titanium dioxide antibacterial coated endotracheal intubation tube]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2014;26(5):343–346. Chinese. doi:10.3760/cma.j.issn.2095-4352.2014.05.012
74. Xu J, Cao J, Wang Y, Jiang X. [Study on oral mucsa irritation due to silver loaded titanium dioxide antibacterial coating endotracheal intubation tube]. Zhonghua Wei Zhong Bing Ji Jiu Yi xue. 2014;26(12):920–922. Chinese. doi:10.3760/cma.j.issn.2095-4352.2014.12.016
75. Deng W, Ning S, Lin Q, et al. I-TiO2/PVC film with highly photocatalytic antibacterial activity under visible light. Colloids Surf B Biointerfaces. 2016;144:196–202. doi:10.1016/j.colsurfb.2016.03.085
76. Gentile MA, Siobal MS. Are specialized endotracheal tubes and heat-and-moisture exchangers cost-effective in preventing ventilator associated pneumonia? Respir Care. 2010;55(2):
77. Caratto V, Ball L, Sanguineti E, et al. Antibacterial activity of standard and N-doped titanium dioxide-coated endotracheal tubes: an in vitro study. Rev Bras Ter Intensiva. 2017;29(1):55–62. doi:10.5935/0103-507X.20170009
78. Zhou H, Wang Y, Jiang XH. Study on antifungal property of antimicrobial coated endotracheal tube with silver loaded titanium dioxide. Chin J Health Lab Technol. 2017;27(5):
79. Zangirolami AC, Inada NM, Bagnato VS, Blanco KC. Biofilm destruction on endotracheal tubes by photodynamic inactivation. Infect Disord Drug Targets. 2018;18(3):218–223. doi:10.2174/1871526518666180523085754
80. Zangirolami AC, Dias LD, Blanco KC, et al. Avoiding ventilator-associated pneumonia: curcumin-functionalized endotracheal tube and photodynamic action. PNAS. 2020;117(37):22967–22973. doi:10.1073/pnas.2006759117
81. Inada NM, Dias LD, Blanco KC, Kassab G, Buzzá HH, Bagnato VS. Antimicrobial photodynamic therapy of the respiratory tract: from the proof of principles to clinical application. Photodyn Ther. 2021. doi:10.5772/intechopen.95602
82. Hashemi MM, Rovig J, Bateman J, et al. Preclinical testing of a broad-spectrum antimicrobial endotracheal tube coated with an innate immune synthetic mimic. J Antimicrob Chemother. 2018;73(1):143–150. doi:10.1093/jac/dkx347
83. Latorre MC, Pérez-Granda MJ, Savage PB, et al. Endotracheal tubes coated with a broad-spectrum antibacterial ceragenin reduce bacterial biofilm in an in vitro bench top model. J Antimicrob Chemother. 2021;76:1168–1173. doi:10.1093/jac/dkab019
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.