")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Antibiotic Treatment for Hidradenitis Suppurativa in France: A Practice Survey
Authors Fougerousse AC , Maccari F, Guillem P, Reguiai Z
Received 4 July 2022
Accepted for publication 13 October 2022
Published 8 December 2022 Volume 2022:15 Pages 2641—2645
DOI https://doi.org/10.2147/CCID.S374643
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jeffrey Weinberg
Anne-Claire Fougerousse,1 François Maccari,1,2 Philippe Guillem,3 Ziad Reguiai4 On behalf of the GEM ResoVerneuil
1Dermatology Department, Military Teaching Hospital Bégin, Saint Mandé, France; 2Dermatology, Private Practice, Saint-Maur-des-Fossés, France; 3Visceral Surgery department, Clinique du Val d’Ouest, Ecully, France; 4Dermatology Department, Polyclinique Courlancy-Bezannes, Reims, France
Correspondence: Anne-Claire Fougerousse, Dermatology department, Military Teaching Hospital Bégin, Saint Mandé, France, Tel +1 43 98 50 00, Email [email protected]
Purpose: Antibiotics are used for hidradenitis suppurativa’s management with limited evidence. Choice of antibiotics is based on small randomized controlled trial or open case-series.
Patients and Methods: We performed a practice survey in Resoverneuil, a French network of physicians treating hidradenitis suppurativa, to identify the antibiotic strategy according to the Hurley stage. Online questionnaire was sent to all members of ResoVerneuil between January and February 2021.
Results: In total, 108 physicians answered the survey: 37.6% were hospital based, 34.6% had a private practice and 27.8% a mixed practice, and 13.8% had a dedicated consultation for hidradenitis suppurativa. Sixty-three physicians reported seeing fewer than 5 patients with hidradenitis suppurativa per month; 29 seeing 5 to 15 patients per month; and 9 seeing more than 15 patients per month. More than 90% declared prescribing antibiotics for flares in Hurley 1 and 2 stages, and 83% in Hurley 3 stages, mostly amoxicillin-clavulanic acid and pristinamycin. Of these physicians, 29.7% declared prescribing a background antibiotic therapy for Hurley 1 stage with less than 4 flares per year, and more than 75% for Hurley 1 stage with more than 4 flares per year, Hurley 2 and Hurley 3 stages; mostly cyclins, combination of rifampicin and clindamycin and sulfamethoxazole-trimethoprim.
Conclusion: This survey underlines the heterogeneity in antibiotic prescription for hidradenitis suppurativa in France, particularly as background therapy.
Keywords: hidradenitis suppurativa, antibiotics, practice survey
Introduction
Although hidradenitis suppurativa is not primarily an infectious disease, antibiotics are widely used to treat this pathology based on limited evidence. The choice of type and length of antibiotics regimen is based on small randomized controlled trials for topical clindamycin1 and tetracyclin2 and on open case-series for other antibiotics as combinations of rifampicin-clindamycin,3–9 clindamycin as monotherapy,10 ofloxacin-clindamycin11 or rifampicin-moxifloxacin-metronidazole,12 dapsone.13 French guidelines for the management of hidradenitis suppurativa were published in 2019, comprising recommandations concerning antibiotherapy use.14 For Hurley stage I or II hidradenitis suppurativa, use of amoxicillin/clavulanic acid or pristinamycin for 7 days was recommended; for preventive treatment or post acute care, cotrimoxazole or cyclins. For Hurley stage II or III hidradenitis suppurativa, use of ceftriaxone/metronidazole or levofloxacin/clindamycin for 15–21 days was recommended, then cotrimoxazole or cyclins. We sought to describe the practice regarding antibiotic prescriptions for hidradenitis suppurativa in France, 18 months after the first communication of the French guidelines.
Patients and Methods
We performed a practice survey in the French physicians network “ResoVerneuil” to identify the antibiotic strategy used in daily life by these physicians for the treatment of hidradenitis suppurativa according to the Hurley stage. ResoVerneuil comprises 278 members (dermatologists, surgeons, gastroenterologists [excluding students in medicine]), objectives of which are to improve the knowledge of healthcare professionals and patients about hidradenitis suppurativa, to improve the patient’s journey and to promote research about hidradenitis suppurativa. A questionnaire was sent by e-mail (with two reminders) to all members of ResoVerneuil between 4th of January and 14th of February 2021 (see Figure 1).
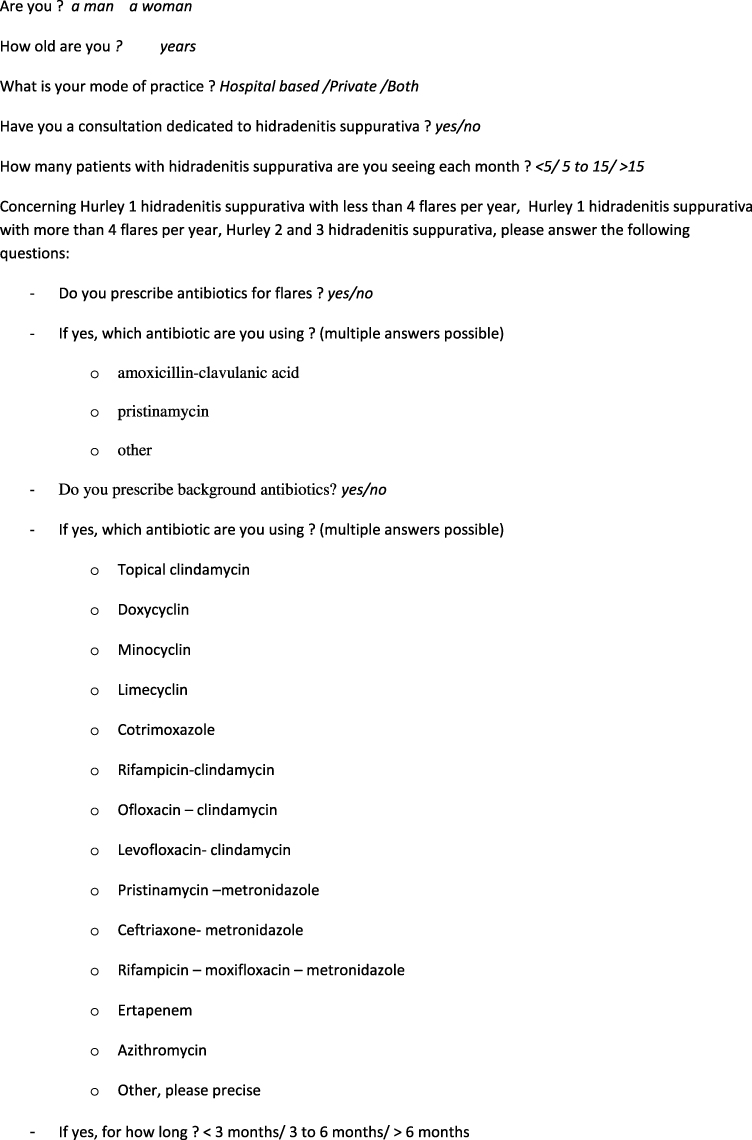 |
Figure 1 Questionnaire. |
The questionnaire collected the gender of the dermatologist, the mode of practice (hospital, private or mixed) and the prescription of antibiotics for hidradenitis suppurativa. For each Hurley stage, the physician was asked whether they use antibiotics to treat hidradenitis suppurativa’s flares and/or as background therapy and, when appropriate, which antibiotic (multiple answers were possible for each Hurley stage) and, for the background therapy, the length of the prescription. For this type of study, French regulations do not require submission to an ethics committee, as this study does not enter the field of the deliberation n°2018-154 of the 3rd of May 2018 (JORF n°0160 of the 13th of July 2018).
Results
One-hundred-eight physicians answered the survey, with 101 analyzable answers. Among those, 75.9% were women, 37.6% were hospital based, 34.6% had a private practice and 27.8% a mixed practice (hospital and private), and 13.8% had a dedicated consultation for hidradenitis suppurativa. Sixty-three physicians reported seeing fewer than 5 patients with hidradenitis suppurativa per month, 29 seeing 5 to 15 patients per month and 9 seeing more than 15 patients per month.
Antibiotics prescription according to Hurley stage is presented in Table 1 for flares and in Table 2 for background therapy.
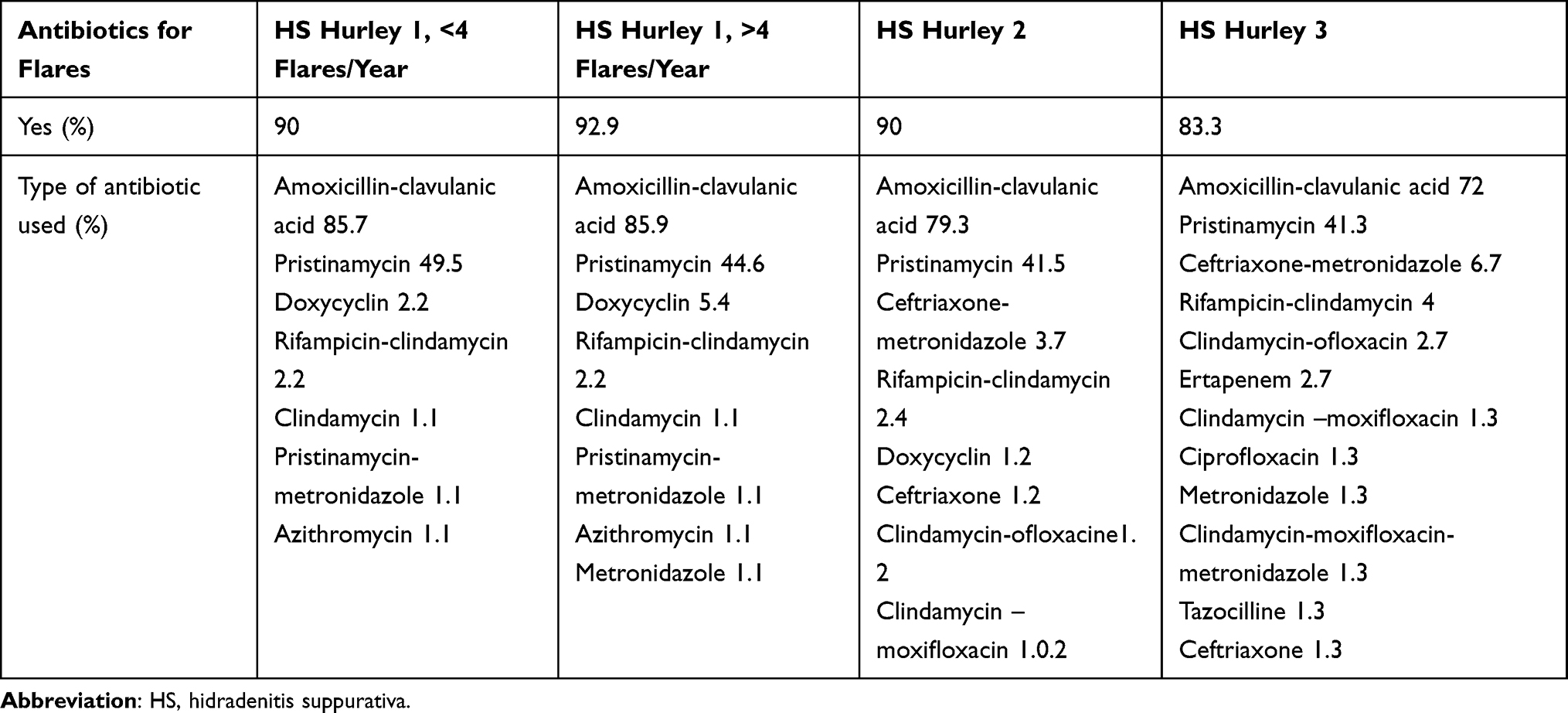 |
Table 1 Antibiotics for Flares |
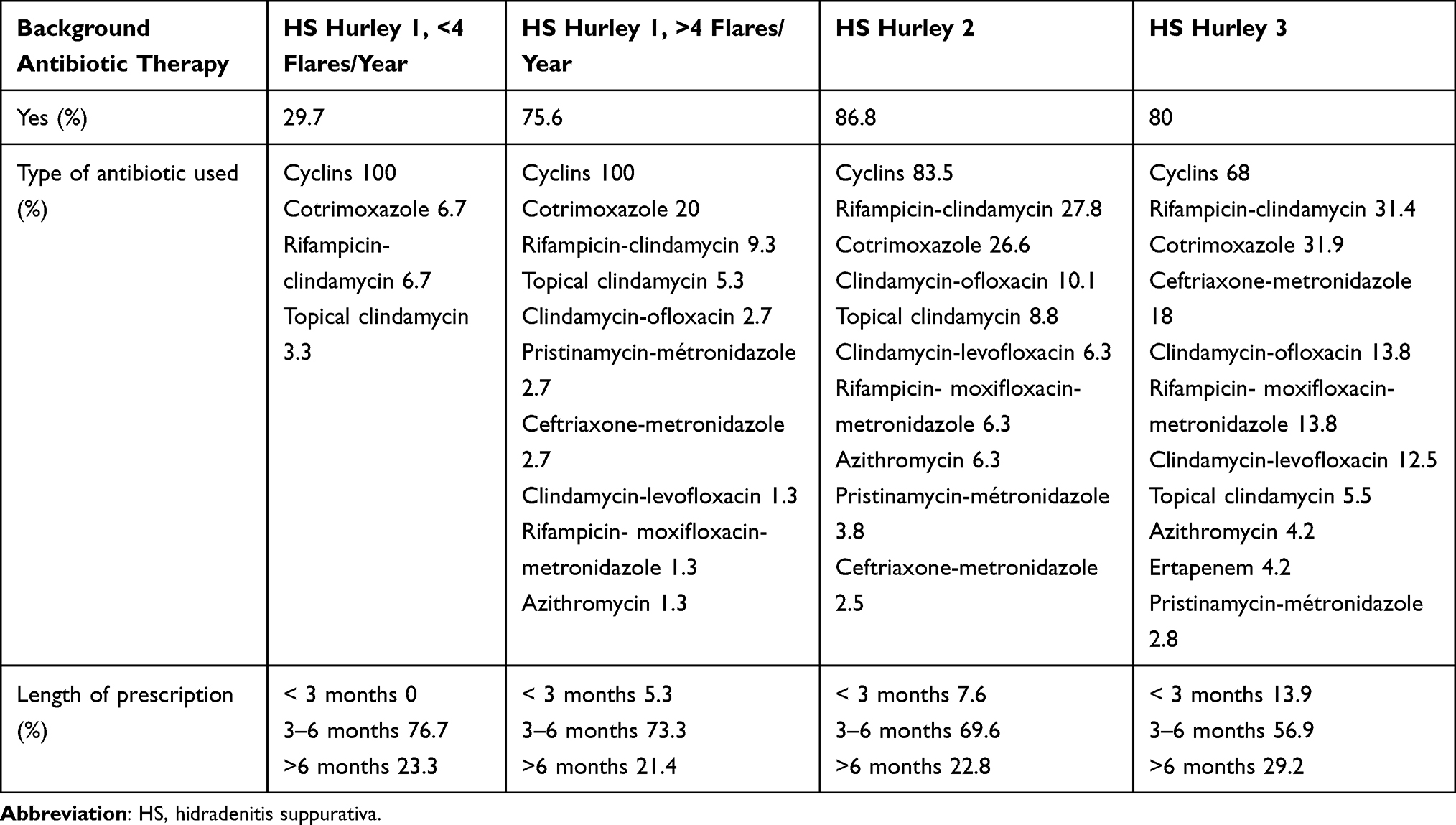 |
Table 2 Background Antibiotic Therapy |
Discussion
A vast majority of physicians prescribe antibiotics for flares whatever the Hurley stage is, mostly amoxicillin-clavulanic acid and pristinamycin, in accordance with the French recommendations.14 Background antibiotic therapy is prescribed by about 80% of physicians for patients with hidradenitis suppurativa Hurley 2 and 3 and for those with Hurley 1 with more than 4 flares per year. Thirty percent of physicians, however, prescribe background antibiotic therapy for patients with Hurley 1 hidradenitis suppurativa with less than 4 flares per year, which is not proposed in French recommendations. We can hypothesize that this situation concerns Hurley 1 patients experiencing few but severe flares, as abscesses requiring surgical management. Background antibiotics used are mostly cyclins, cotrimoxazole and combination of ceftriaxone and metronidazole (for Hurley 3 stage). Several other antibiotics are used as combinations of rifampicin and clindamycin (as proposed in European recommendations for the treatment of hidradenitis suppurativa)15 and clindamycin and quinolones, azithromycin, etc. The combination of clindamycin and levofloxacin proposed in French recommendations as attack treatment in Hurley 2 and 3 stages is very little used in practice. Length of combination of antibiotics exceeds 3 months in 80% of cases, contrary to the recommendations. This can been explained by the absence of therapeutic alternatives, as adalimumab was not reimbursed for hidradenitis suppurativa at this time in France.
Physicians seeing more than 15 patients with hidradenitis suppurativa per month were more likely to respect French recommendations, probably being more up to date about hidradenitis suppurativa’s management. There was no difference in antibiotic pattern prescription according to the existence of a dedicated consultation for hidradenitis suppurativa.
Limits of this study are the absence of a question about the impact of the French recommendations on the habits of antibiotic prescription, and the impossibility to determinate exactly the length of each type of background antibiotic when the physicians declared prescribing more than one type.
Conclusion
This survey underlines the heterogeneity in antibiotic prescription for hidradenitis suppurativa in France, particularly as background therapy, and the high rate of long prescription of antibiotic combinations. As long-term use of antibiotic combinations, in particular fluoroquinolones and rifampicin, can lead to serious adverse events and development of antibioresistance, their use should be limited. Cyclins or cotrimoxazole appear to be a safer long-term option. Since this survey was taken, adalimumab is now reimbursed for hidradenitis suppurativa, which may lead to a modification of antibiotic use. However, studies with a better level of evidence are needed in order to improve the use of antibiotics in hidradenitis suppurativa and to clarify their place in the management of hidradenitis suppurativa (monotherapy, combination with biologics or surgery, etc.).
Acknowledgments
To the members of the scientific committee of the GEM ResoVerneuil: Laurent Abramowitz, Pierre-André Bécherel, Anne-Cécile Ezanno, Charlotte Fite, Germaine Gabison, Aude Nassif, Laure Mery-Bossard and Domitille Thomas- Beaulieu. The abstract of this paper was presented at the 10th Conference of the European Hidradenitis Suppurativa Foundation (EHSF) 2021 and at the Journées Dermatologiques of Paris 2021.
Disclosure
Dr Philippe Guillem reports receiving personal fees from Abbvie, Novartis, UCB Pharma and Concatec, outside the submitted work. Dr Ziad Reguiai reports being an investigator in clinical trials and a consulting (board) speaker for Abbvie, Amgen, Leo Pharma, Pfizer, Janssen, Almirall, UCB and Novartis; and a speaker for Medac, an investigator in clinical trial consulting (board) for Celltrion and a consulting (board) speaker for Lilly, outside the submitted work. The authors have no other conflicts of interest to declare.
References
1. Clemmensen OJ. Topical treatment of hidradenitis suppurativa with clindamycin. Int J Dermatol. 1983;22(5):325–328. doi:10.1111/j.1365-4362.1983.tb02150.x
2. Jemec GB, Wendelboe P. Topical clindamycin versus systemic tetracycline in the treatment of hidradenitis suppurativa. J Am Acad Dermatol. 1998;39(6):971–974. doi:10.1016/S0190-9622(98)70272-5
3. Gener G, Canoui-Poitrine F, Revuz JE, et al. Combination therapy with clindamycin and rifampicin for hidradenitis suppurativa: a series of 116 consecutive patients. Dermatology. 2009;219(2):148–154. doi:10.1159/000228334
4. Iannone M, Janowska A, Bartolomei G, et al. Systemic antibiotics in hidradenitis suppurativa: efficacy and effects of body mass index and smoking pack-year on the response to therapy. Dermatol Ther. 2021;34(3):e14919. doi:10.1111/dth.14919
5. Mendonça CO, Griffiths CE. Clindamycin and rifampicin combination therapy for hidradenitis suppurativa. Br J Dermatol. 2006;154(5):977–978. doi:10.1111/j.1365-2133.2006.07155.x
6. van der Zee HH, Boer J, Prens EP, Jemec GB. The effect of combined treatment with oral clindamycin and oral rifampicin in patients with hidradenitis suppurativa. Dermatology. 2009;219(2):143–147. doi:10.1159/000228337
7. Bettoli V, Zauli S, Borghi A, et al. Oral clindamycin and rifampicin in the treatment of hidradenitis suppurativa-acne inversa: a prospective study on 23 patients. J Eur Acad Dermatol Venereol. 2014;28(1):125–126. doi:10.1111/jdv.12127
8. Dessinioti C, Zisimou C, Tzanetakou V, Stratigos A, Antoniou C. Oral clindamycin and rifampicin combination therapy for hidradenitis suppurativa: a prospective study and 1-year follow-up. Clin Exp Dermatol. 2016;41(8):852–857. doi:10.1111/ced.12933
9. Yao Y, Jørgensen AR, Ring HC, Thomsen SF. Effectiveness of clindamycin and rifampicin combination therapy in hidradenitis suppurativa: a 6-month prospective study. Br J Dermatol. 2021;184(3):552–553. doi:10.1111/bjd.19578
10. Rosi E, Pescitelli L, Ricceri F, et al. Clindamycin as unique antibiotic choice in Hidradenitis Suppurativa. Dermatol Ther. 2019;32(2):e12792. doi:10.1111/dth.12792
11. Delaunay J, Villani AP, Guillem P, Tristan A, Boibieux A, Jullien D. Oral ofloxacin and clindamycin as an alternative to the classic rifampicin-clindamycin in hidradenitis suppurativa: retrospective analysis of 65 patients. Br J Dermatol. 2018;178(1):e15–e16. doi:10.1111/bjd.15739
12. Delage M, Jais JP, Lam T, et al. Rifampin-moxifloxacin-metronidazole combination therapy for severe Hurley Stage 1 Hidradenitis Suppurativa: prospective short-term trial and one-year follow-up in 28 consecutive patients. J Am Acad Dermatol. 2020. doi:10.1016/j.jaad.2020.01.007
13. Yazdanyar S, Boer J, Ingvarsson G, Szepietowski JC, Jemec GB. Dapsone therapy for hidradenitis suppurativa: a series of 24 patients. Dermatology. 2011;222(4):342–346. doi:10.1159/000329023
14. Bertolotti A, Sbidian E, Join-Lambert O, et al. Guidelines for the management of hidradenitis suppurativa: recommendations supported by the Centre of Evidence of the French Society of Dermatology. Br J Dermatol. 2021;184(5):963–965. doi:10.1111/bjd.19710
15. Zouboulis CC, Desai N, Emtestam L, et al. European S1 guideline for the treatment of hidradenitis suppurativa/acne inversa. J Eur Acad Dermatol Venereol. 2015;29(4):619–644. doi:10.1111/jdv.12966
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.