")
Back to Journals » Infection and Drug Resistance » Volume 15
Antibiotic Resistance, Molecular Characteristics and Risk Factors of Carbapenem-Resistant Klebsiella pneumoniae in Clinical Isolates
Received 12 August 2022
Accepted for publication 20 October 2022
Published 15 November 2022 Volume 2022:15 Pages 6671—6680
DOI https://doi.org/10.2147/IDR.S383010
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Jingxuan Zhu, Ye Chen, Xuejing Yang
The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Traditional Chinese Medicine), Hangzhou, Zhejiang, 310006, People’s Republic of China
Correspondence: Xuejing Yang, Department of Clinical Laboratory, The First Affiliated Hospital of Zhejiang Chinese Medical University, 54 Youdian Road, Hangzhou, Zhejiang, 310006, People’s Republic of China, Email [email protected]
Background: The global epidemic of carbapenem-resistant Klebsiella pneumonia (CRKP) has become a significant public health challenge. This study aimed to investigate the antibiotic resistance and molecular characteristics of CRKP and the clinical characteristics of infected patients.
Methods: Sixty-two clinically isolated CRKP strains were collected for the first time from the First Affiliated Hospital of Zhejiang Chinese Medical University in Zhejiang Province. The carbapenemase gene, virulence-associated gene, capsular serotype gene and fenestra protein gene were detected by PCR. Univariate logistic regression and multivariate logistic regression analyses were performed to predict the risk factors for the prognosis of CRKP infection.
Results: All CRKP isolates were resistant to meropenem, piperacillin-tazobactam, and ceftazidime (100%, 62/62), and all but one CRKP isolate was resistant to imipenem and cefepime (96.8%, 61/62). The rate of colistin resistance was the lowest (11.9%, 8/62). For CRKP in the ICU, the rates of resistance to various antibiotics were significantly higher than those in general ward patients. Fifty strains carried the carbapenemase gene blaKPC, and 3 strains carried both the blaKPC and blaNDM genes. The virulence genes uge, wabG, ycf, entB, ureA and fimH were detected in more than 90% of the 62 CRKP strains. Two strains had Ompk35, Ompk36 and Hcp gene deletions. The blaKPC, rmpA and rmpA2 genes had the highest positive rate in blood samples, and blaNDM had the highest positive rate in stool samples. Multivariate analysis showed that pulmonary disease affected the prognosis of CRKP infection.
Conclusion: The prevalence and molecular characteristics of CRKP clinical isolates in Zhengjiang Province in China were described, and the antibiotic resistance rate was higher. Additionally, relevant genes of CRKP strains and clinical characteristics of patients are related to the progression and prognosis of CRKP infection.
Keywords: Klebsiella pneumoniae, carbapenem-resistant, antibiotic resistance, carbapenemase, virulence gene, risk factor
Introduction
Klebsiella pneumoniae (KP) is an Enterobacteriaceae pathogen associated with hospital and community-acquired infections, such as pneumonia, blood infection, and urinary tract infection.1 Carbapenem antibiotics are widely used to treat patients with KP infection due to their stable effects on β-lactamase.2 Antibiotic resistance and widespread dissemination of CRKP have become some of the most difficult challenges in clinical infection therapy. However, carbapenem-resistant Klebsiella pneumonia (CRKP) has become a severe threat in both hospitals and communities due to the widespread use of antibiotics. According to previous reports, the production of carbapenemase is the most common mechanism of carbapenem resistance among KP isolates.3 Molecular methods have detected that the majority of CRKP isolates contain a carbapenemase gene, such as the K. pneumoniae carbapenemase (blaKPC) or New-Delhi-metallo-b-lactamase (blaNDM) genes.4 CRKP has been reported in almost all regions of China and is traditionally believed to not be highly virulent.5 However, the recent emergence of highly virulent Klebsiella pneumoniae (hvKP) in mainland China has attracted much attention because it can cause highly invasive infections, such as severe pneumonia, liver abscesses, meningitis and dophthalmitis.6,7 hvKP tends to exhibit high viscosity, probably associated with specific virulence genes and capsular polysaccharides.8,9 The string test is commonly used to identify hyperviscosity phenotypes. Genetic determinants of high virulence usually reside in mobile genetic elements, such as the high virulence plasmid-related genes rmpA, rmpA2, and iutAetc.10
In recent years, the detection rate of CRKP with high virulence and high drug resistance has continued to increase, and the horizontal movement of its drug resistance genes can cause the proliferation of drug-resistant strains. Therefore, early detection and monitoring of CRKP colonization or infection and research on the occurrence and development of its drug resistance mechanism are essential to control the occurrence and spread of bacterial drug resistance.11 Furthermore, an epidemiological analysis of CRKP is imperative. Effective monitoring of these isolates can limit the spread of antibiotic resistance. In hospital treatment, multiple risk factors can affect the prognosis of CRKP infection, and analysis of risk factors for CRKP infection is necessary to help clinicians take effective preventive measures in the early stage.12 This study investigated the clinical characteristics, drug resistance and molecular characteristics of CRKP clinical strains and the risk factors for CRKP infection. The goal of this study was to provide a reference for the diagnosis and treatment of clinical infection and rational drug use and to provide information to help reduce the possibility of strain outbreaks.
Materials and Methods
Clinical Data Collection
All infected patient (the clinical source of 62 CRKP isolates) characteristics were extracted and are presented in Table 1. The survey items included demographic data, such as age, sex and basic medical history; hospitalization characteristics, including sample type and separation department; and treatment with invasive surgery, including tracheal intubation or tracheotomy, arteriovenous catheterization, indwelling catheter, etc. The prognosis of the patient was based on the patient’s condition at discharge: those who died of irreversible organ failure and did not improve at discharge were considered to have a poor prognosis. The consent was waived by the Ethics Committee of the First Affiliated Hospital of Zhejiang Chinese Medical University (2019-KL-090-01). The clinical samples were part of the routine hospital laboratory procedure, and noninfected patients were removed. The study was performed in accordance with the guidance of the Declaration of Helsinki and relevant regulations.
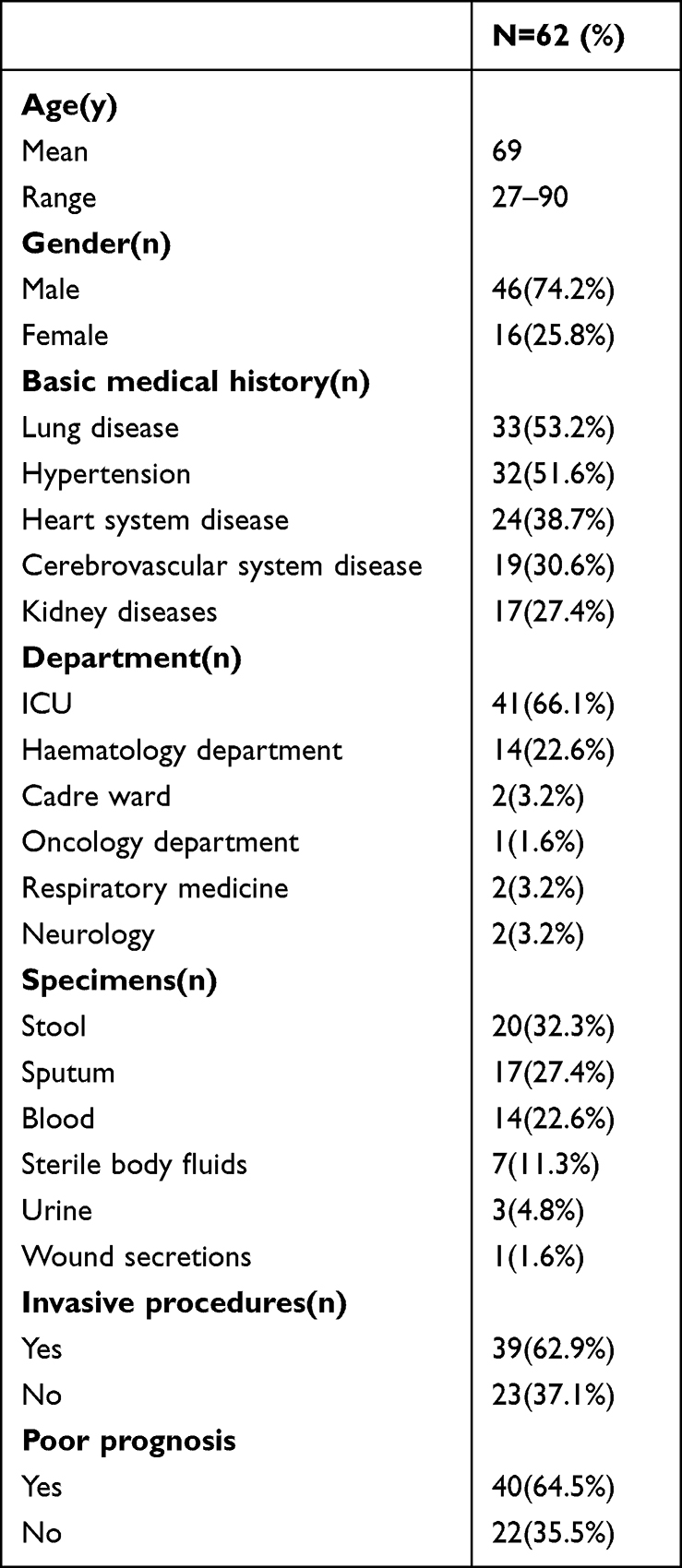 |
Table 1 Clinical Patient Data |
Sample Collection and Antibiotic Susceptibility Test
Sixty-two CRKP strains were isolated for the first time from The First Affiliated Hospital of Zhejiang Chinese Medical University from August 2019 to May 2020, and the specimens of noninfected patients were removed. The antibiotics commonly used clinically were tested for antimicrobial susceptibility through the micro broth dilution method and the Vitek 2 Compact system (Biomerieux, Marcy L’Etoile, France). Antibiotic susceptibility results refer to the unified standards of the Clinical and Laboratory Standards Institute (https://clsi.org/standards/products/microbiology/documents/, Published in 2022). Tigecycline MICs were interpreted using EUCAST (http://www.eucast.org) MIC breakpoint standards, and CRKP was defined as resistance to meropenem, imipenem or ertapenem (minimum inhibitory concentration ≥ 4 µg/mL). All CRKP strains were reconfirmed by the paper diffusion method to avoid Vitek system errors13 (according to CLSI: the diameter of the meropenem and imipenem inhibition zone is ≤ 19 mm, and the diameter of the ertapenem inhibition zone is ≤ 18 mm (antibiotics from Oxoid UK). Escherichia coli (ATCC 25922) and Pseudomonas aeruginosa (ATCC 27853) were used as quality control strains for the antibiotic susceptibility test.
String Test
The isolates of Klebsiella pneumoniae on the agar plate were stretched through the inoculation ring. A viscous silk with a length of >5 mm was produced in all three experiments, the drawing test was considered positive, and the strain belonged to the hyperviscosity phenotype.14
DNA Extraction and Application of Genes
Chromosomal DNA was extracted using a TIANamp Bacteria Genomic DNA Kit (Tiangen Biotech Co. Ltd, Beijing, China). PCR amplifications were performed for carbapenemase genes (blaKPC, blaNDM, blaOXA-48, blaVIM, blaGIM, blaSIM, and blaIMP), virulence genes (magA, uge, aerobactin, wcaG, mrkD, wabG, fimH, rmpA, ycf, urea, ybtA, kfuB, iorN, iutA, rntB, and alls), capsular serotype-specific genes (K1, K2, K5, K20, K54, and K57), fenestra protein genes (ompk35 and ompk36) and a bacterial pathogenicity-associated gene (hcp) that encodes a haemolysin-coregulated protein, and the primers are listed in Table S1.9,11,15–18 The PCR conditions were as follows: 95 °C predenaturation for 5 minutes; 95 °C denaturation for 10 seconds, 50–62°C annealing for 20 seconds, 72 °C extension for 20 seconds, a total of 35 cycles; 72°C end extension for 40s and storage at 4 °C. The amplified products were electrophoresed in a 1% agarose gel, and the PCR-positive products were sent to Shanghai Shenggong Company for sequencing. The sequencing results were performed in GenBank for BLAST comparison to confirm the genotype.
Statistical Analysis
The continuous data are described as the mean and standard deviation, and classification data are expressed in quantity and percentage. The resistance rate between ICU and general ward patients was compared using the χ2 test. The positive rate of genes among different strains was compared by the χ2 test for categorical variables. A univariate logistic regression model was analysed by the χ2 test, and multivariate analysis was performed by logistic regression analysis. P<0.05 (two-sided) was considered statistically significant. All statistical analyses were performed using SPSS 25.0 software (IBM, Armonk, NK, USA).
Results
Clinical Characteristics
The 62 patients infected with CPKP were mainly males (74.2%, 46/62), with a median age of 69 years. In the basic medical history, the incidence of pulmonary disease and hypertension were 53.2% (33/62) and 51.6% (32/62), respectively. The incidences of heart system, cerebrovascular system and kidney diseases were 38.7% (24/62), 30.6% (19/62) and 27.4% (17/62), respectively. For the distribution of departments, the ICU had the highest detection rate (66.1%, 41/62), followed by the haematology department (22.6%, 14/62), cadre ward (3.2%, 2/62), respiratory medicine and neurology departments (3.2%, 2/62), and oncology department (1.6%, 1/62). For sample type, the stool detection rate was the highest (32.3%, 20/62), followed by sputum (27.4%, 17/62), blood (22.6%, 14/62), sterile body fluids (11.3%, 7/62), urine (4.8%, 3/62) and wound secretions (1.6%, 1/62). Among the 62 CRKP-infected patients, 39 underwent invasive procedures, and 40 patients had a poor prognosis (Table 1).
Antibiotic Sensitivity Results
The detailed antibiotic resistance results of the 62 CRKP clinical isolates are shown in Table 2. All strains were resistant to meropenem (100%, 62/62), piperacillin-tazobactam (100%, 62/62), and ceftazidime (100%, 62/62), and all but one strain was resistant to imipenem (96.8%, 61/62) and cefepime (96.8%, 61/62). Meanwhile, as shown in Figure 1, the antibiotic resistance rates of CRKP in ICU patients for ciprofloxacin, levofloxacin, amikacin, aztreonam and tigecycline were significantly higher than those in general ward patients (P=0.004, P=0.002, P < 0.001, P = 0.001, and P = 0.002, respectively).
 |
Table 2 Antibiotic Sensitivity Results of CRKP Isolates |
 |
Figure 1 Antibiotic resistance rate of CRKP in ICU and general ward patients. *P<0.05, **P<0.01. |
String Test of Carbapenemase Genes, Virulence Genes, and Capsular Serotype Specific Genes
The gene results are shown in Table 3. Among the 62 CRKP isolates, 57 isolates carried carbapenemase genes (91.9%, 57/62). The positive rate of blaKPC was the highest (80.6%, 50/62), followed by those of blaNDM (12.9%, 8/62) and blaIMP (4.8%, 3/57). Among the virulence genes, the positive rates of ycf, entB, and ureA were the highest (96.8%, 60/62), followed by those of WabG (93.5%, 58/62), Uge (91.9%, 57/62), and fimH (90.3%, 56/62). Among the 62 CRKP isolates, 1 isolate was the K5 serotype. The other 61 strains did not have the common capsular serotypes (K2, K5, K20, K54, and K57). Among the 62 CRKP isolates, 2 isolates had a hypermucoid phenotype (3.2%, 2/62).
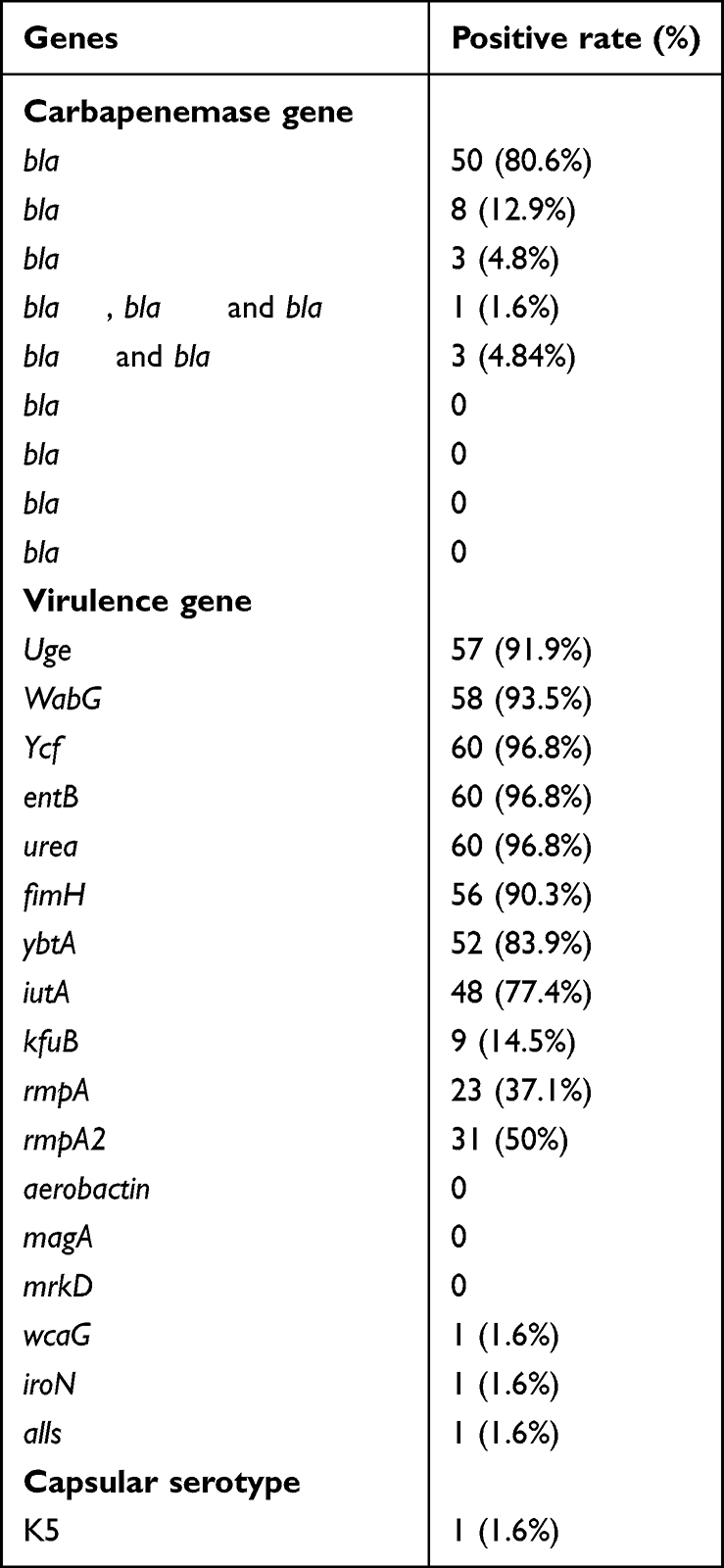 |
Table 3 The Positive Rate of Genes in 62 CRKP Isolates |
HCP and Fenestra Protein Gene Test
In this study, 2 of 62 CRKP isolates lost the bacterial pathogenicity-associated gene Hcp (3.2%, 2/62). Seven of the 62 CRKP isolates lost the fenestra gene, Ompk35 or Ompk36 (11.29%, 7/62), and 2 isolates lost both the Ompk35 and Ompk36 genes.
Comparison of Molecular Types in Different Specimen Types
We compared the positive rate of carbapenemase genes (blaKPC and blaNDM) and virulence genes (rmpA and rmpA2) in the specimen types. The positive rate of blaKPC in blood samples was higher than that in stool and sputum samples, although statistical analysis showed no significant difference. In stool samples, the positive rate of blaNDM was highest (25%). Moreover, the positive rates of the virulence genes rmpA and rmpA2 in blood were both higher than those in stool and sputum samples (Table 4).
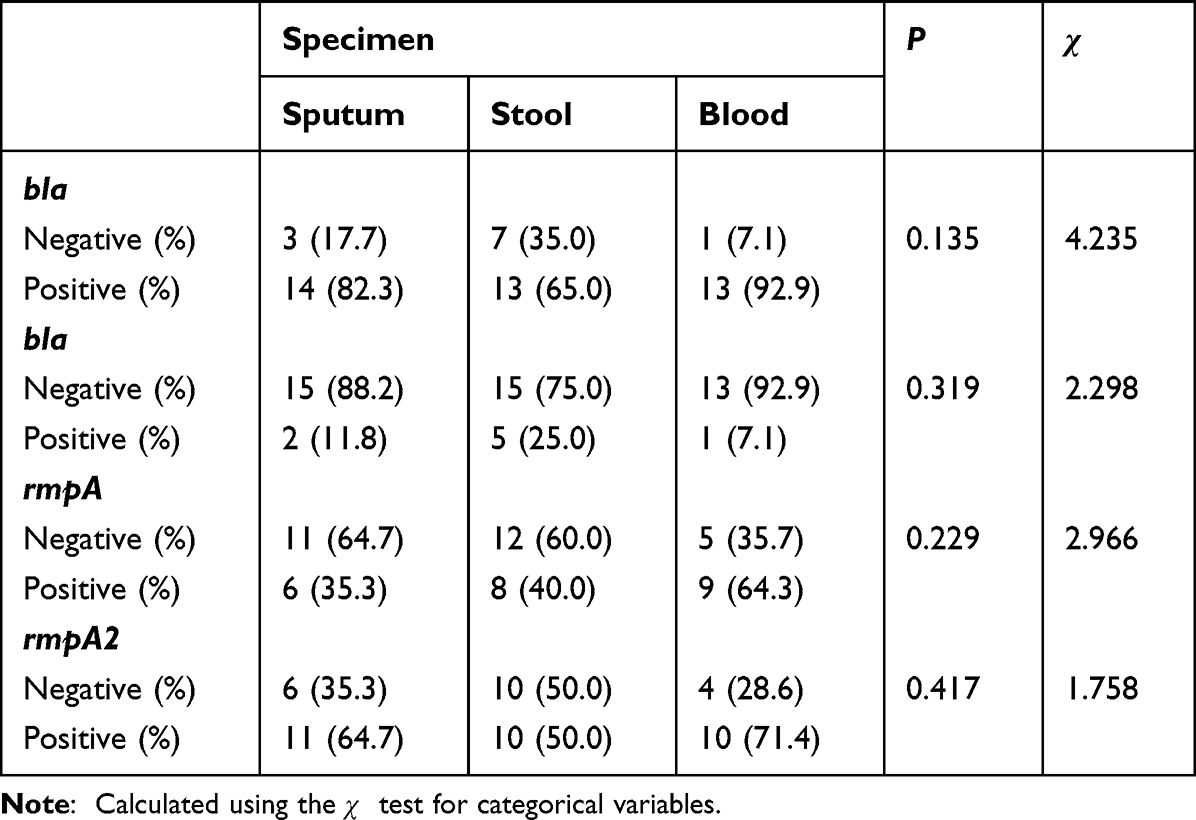 |
Table 4 Comparison of Molecular Types in Different Specimen Types |
Risk Factors for Poor Prognosis in CRKP-Infected Patients
The relevant characteristics of 62 CRKP-infected patients were analysed to predict the risk factors for poor prognosis. The univariate analysis showed that male sex, ICU admission, lung disease (primary or secondary diagnosis of lung disease recorded in the medical record), and infection with isolates carrying the blaKPC gene were significantly different between the prognosis groups (Table S2). Furthermore, logistic regression models were performed to predict the correlations of these factors with poor prognosis, and the results showed that pulmonary disease was a potential factor (Table 5).
 |
Table 5 Multivariate Analysis for Prognosis in CRKP-Infected Patients |
Discussion
In recent years, carbapenem-resistant Klebsiella pneumonia has become a severe threat in both hospitals and communities due to the widespread use of antibiotics. Moreover, the emergence of hypervirulent Klebsiella pneumoniae is causing an increasing challenge in China.19 Previous reports have indicated that a majority of CRKP isolates carry resistance genes, and hvKP tends to exhibit high viscosity, probably associated with specific virulence genes and capsular polysaccharides.26,27 However, studies on the prevalence of CRKP strains in Zhejiang Province in China are limited. In this study, 62 clinically isolated CRKP strains were collected to investigate the drug resistance, molecular characteristics and clinical characteristics of infected patients.
Among the 62 CRKP-infected patients, 41% were distributed in the ICU, and 14% were distributed in the haematology department. This is probably related to the severe basic diseases that present in those departments and the more invasive treatments administered there. Similarly, Li et al found that ICU admission was a risk factor for CRKP infection.12 The median age of the CRKP-infected patients was 69 years, and the infections were mainly distributed in the digestive tract, respiratory tract and blood, which indicated that elderly patients and other immunocompromised people are more prone to invasive infections. In this study, the resistance rates of CRKP strains to ceftazidime, cefepime, aztreonam, meropenem, imipenem, cefoperazone and sulbactam were high, and the resistance rate to colistin was the lowest. Moreover, the resistance rate was higher than that in a previous report,20 probably due to the severe condition of patients and the clinical treatment of multiple types of antibiotics. Therefore, antibiotics should be used appropriately to avoid unnecessary new drug resistance in the clinical treatment of CRKP infection. In this study, the antibiotic resistance rates of CRKP in ICU patients to ciprofloxacin, levofloxacin, amikacin, aztreonam and tigecycline were significantly higher than those in general ward patients, which was probably related to the severe basic diseases of ICU patients and the clinical treatment of multiple antibiotics.
The production of carbapenemase is the most common mechanism of carbapenem resistance among KP isolates. Common carbapenemase genes include blaKPC, blaNDM, blaOXA-48, blaVIM, blaGIM, blaSIM, blaIMP, etc.21 In our study, 57 strains carried carbapenemase genes, and the most common carbapenemase genes were blaKPC (80.6%) and blaNDM (14.0%). A previous study showed that KP carries both blaKPC and blaNDM and is resistant to almost all antibiotics.22 Our research detected three strains carrying both blaKPC and blaNDM and one strain carrying both blaKPC, blaNDM and blaIMP. In addition, carbapenemase genes can be spread horizontally between strains through plasmids.23 This suggests that our test results have value for clinical application in regards to taking effective measures to avoid the outbreak of drug-resistant strains in hospitals through accurate diagnosis of microorganisms, rational use of antibiotics and reduction of invasive procedures. In this study, common carbapenemase genes were not detected in five CRKP strains, which was probably because those strains had other uncommon carbapenemase genes or other resistance mechanisms. In this study, the positive rates of the virulence genes uge, wabG, ycf, entB, ureA, fimH and ybt were all above 90%, which suggests that these genes may be the main pathogenic factors of CRKP. At present, there is no uniform standard for the hvKP test, but studies have shown that the presence of the iro, rmpA and rmpA2 genes located on the mobile virulence plasmid can highly predict hvkp.24 rmpA can activate capsule production, resulting in the hypermucoviscosity phenotype, and increase in virulence.25 In this study, the positive rates of rmpA and rmpA2 were 37.1% and 50%, indicating that these strains are super bacteria (with high virulence and high drug resistance) and need more clinical attention.
The hypermucoviscous phenotype of KP strains is more likely to cause some special invasive infections, which is usually related to the increased production of capsular polysaccharides and the presence of specific virulence genes. The capsular serotypes of KP can be divided into 82 serotypes.26 In this study, only one K5 strain was detected among the 62 CRKP strains, and a large number of rmpA gene-positive strains did not show a hypermucoid phenotype. This may be due to the reduced expression of the capsule by resistant strains or the presence of other undetected capsule serotypes and regulatory mechanisms. Some studies have shown that the lack of hypermucoviscosity in some rmpA-positive K. pneumoniae strains was associated with a concurrent mutation of rmpA genes.27 Therefore, more studies in other strains are needed to clarify the mechanisms. The type IV secretion system (T6SS) of gram-negative bacteria participates in the formation of bacterial biofilms, resists phagocytosis by macrophages, and induces biological functions, such as apoptosis.28 As the core component of the T6SS, Hcp plays an important role in bacterial pathogenicity.29 There is increasing evidence that the T6SS is related to the pathogenesis of KP.30 In this study, 2 of 62 CRKP isolates did not have Hcp, which may be related to the mechanism of resistance. Seven isolates among the 62 CRKP isolates did not have the fenestra gene, Ompk35 or Ompk36. In addition, we found that 2 isolates without carbapenemase genes also had deletion of Ompk35/Ompk36, suggesting that the loss of outer membrane protein may be related to the mechanism of resistance. This is in line with Sugawa E and Zhang Yong, who found that the existence of Ompk35 and Ompk36 promoted the diffusion of β-lactam drugs in cells.31,32 However, whether that is accompanied by efflux pump expression, ESBL/AmpC, and high-affinity binding sites requires further study.33
A previous study revealed a strong association between the rmpA gene and hypervirulence,25 and the carbapenemase genes blaKPC and blaNDM were the most common resistance genes in KP isolates. However, the association of carbapenemase and virulence genes with CRKP sources has not been reported. We investigated the potential association between the gene distribution of CRKP among the specimens, and the results showed that the positive rates of blaKPC, rmpA, and rmpA2 in blood samples were the highest, suggesting that highly resistant and virulent strains are more likely to cause blood invasive infections. Bacteraemia is an extreme complication of CRKP infection that commonly occurs with severe invasive injury. Therefore, more samples and further studies on the molecular mechanism of CRKP infection in blood invasion should be performed.
However, a limitation of this study was the lack of in-depth research on the mechanism of drug resistance and virulence. Statistical investigation of risk factors can help clinicians take effective preventive measures in the early stage of infection.34 In this study, the univariate analysis showed that sex, ICU admission, pulmonary disease, and infection with strains carrying the blaKPC gene were statistically significant for the prognosis of CRKP infection. However, multiple regression analysis showed that only pulmonary disease was a potential risk factor for the prognosis of CRKP infection. Notably, there have been few reports about pulmonary diseases as a risk factor for CRKP infection in published studies; thus, this is a clinically significant finding. Klebsiella pneumoniae is part of the normal commensal flora of the respiratory tract and can cause pulmonary infection, including lobar pneumonia, empyema, and lung abscess, when immunocompromised or external infection occurs.7 Patients with a poor prognosis usually have severe infections, long medical treatment times, and even irreversible organ failure. Therefore, patients with such risk factors should receive more attention and effective clinical treatment. However, an in-depth study to explore the possible resistance mechanism is necessary.
Conclusion
The prevalence and molecular characteristics of CRKP clinical isolates in Zhengjiang Province in China were described, and the antibiotic resistance rate was higher than that in a previous report, suggesting that antibiotics should be used appropriately to avoid unnecessary new drug resistance in the clinical treatment of CRKP infection. In addition, blaKPC and blaNDM are the most prevalent carbapenemase genes of K. pneumoniae. The CRKP isolates carrying the virulence genes rmpA and rmpA2 are more likely to cause invasive blood infection, and the deletion of the ompk35 and ompk36 genes may increase drug resistance. Also, lung disease is a potential factor for poor prognosis.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
Compliance with ethical standards: This study was approved by the Medical Ethics Committee of the Hospital (No. 2019-KL-090-01) and was conducted in compliance with ethical, legal, and regulatory norms. The consent was waived by the Ethics Committee of the First Affiliated Hospital of Zhejiang Chinese Medical University due to the retrospective nature of the review. Privacy of the participants was protected and the data was anonymized or maintained with confidentiality.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by research grants from Zhejiang Provincial Traditional Chinese Medical Technology Project (no. 2023ZL380).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mil-Homens D, Martins M, Barbosa J, et al. Carbapenem-resistant Klebsiella pneumoniae clinical isolates: in vivo virulence assessment in galleria mellonella and potential therapeutics by polycationic oligoethyleneimine. Antibiotics. 2021;10(1):56. doi:10.3390/antibiotics10010056
2. Wang G, Zhao G, Chao X, Xie L, Wang H. The characteristic of virulence, biofilm and antibiotic resistance of Klebsiella pneumoniae. Int J Environ Res Public Health. 2020;17(17):6278.
3. Lin D, Chen J, Yang Y, Cheng J, Sun C. Epidemiological study of carbapenem-resistant Klebsiella Pneumoniae. Open Med. 2018;13:460–466. doi:10.1515/med-2018-0070
4. Logan LK, Weinstein RA. The epidemiology of carbapenem-resistant enterobacteriaceae: the impact and evolution of a global menace. J Infect Dis. 2017;215(suppl_1):S28–S36. doi:10.1093/infdis/jiw282
5. Hua YU, Xuesong XU, Min LI. Expert consensus statement on laboratory detection and clinical report of carbapenemase among Enterobacterales (second edition). Chin J Infect Chemother. 2022;22(4):463–474. doi:10.16718/j.1009-7708.2022.04.014
6. Zhou C, Wu Q, He L, et al. Clinical and molecular characteristics of carbapenem-resistant hypervirulent Klebsiella pneumoniae isolates in a Tertiary Hospital in Shanghai, China. Infect Drug Resist. 2021;14:2697–2706. doi:10.2147/IDR.S321704
7. Ding Y, Wang Y, Hsia Y, Sharland M, Heath PT. Systematic review of carbapenem-resistant Enterobacteriaceae causing neonatal sepsis in China. Ann Clin Microbiol Antimicrob. 2019;18(1):36. doi:10.1186/s12941-019-0334-9
8. Hasani A, Soltani E, Ahangarzadeh RM, et al. Klebsiella pneumoniaeSerotyping of and its relation with capsule-associated virulence genes, antimicrobial resistance pattern, and clinical infections: a descriptive study in medical practice. Infect Drug Resist. 2020;13:1971–1980. doi:10.2147/IDR.S243984
9. Russo TA, Olson R, Fang CT, et al. Identification of biomarkers for differentiation of hypervirulent Klebsiella pneumoniae from classical K. pneumoniae. J Clin Microbiol. 2018;56:e00776–18. doi:10.1128/JCM.00776-18
10. Russo TA, Marr CM. Hypervirulent Klebsiella pneumoniae. Clin Microbiol Rev. 2019;32(3). doi:10.1128/CMR.00001-19
11. Candan ED, Aksöz N. Klebsiella pneumoniae: characteristics of carbapenem resistance and virulence factors. Acta Biochim Pol. 2015;62(4):867–874. doi:10.18388/abp.2015_1148
12. Li J, Li Y, Song N, Chen Y. Risk factors for carbapenem-resistant Klebsiella pneumoniae infection: a meta-analysis. J Glob Antimicrob Resist. 2020;21:306–313. doi:10.1016/j.jgar.2019.09.006
13. Liu YL, Xu HP, Xiao M, et al. Evaluation of the capabilities of disc diffusion and Vitek2-compact GN13 methods for testing antimicrobial susceptibility and screening of ESBLs Enterobacteriaceae clinical isolates. Chin J Microbiol Immunol. 2015;35(2):139–145. doi:10.3760/cma.j.issn.0254-5101.2015.02.011
14. Nadasy KA, Domiati-Saad R, Tribble MA. Invasive Klebsiella pneumonia syndrome in North America. Clin Infect Dis. 2007;45(3):e25–e28. doi:10.1086/519424
15. Poirel L, Walsh TR, Cuvillier V, et al. Multiplex PCR for detection of acquired carbapenemase genes. Diagn Microbiol Infect Dis. 2011;70(1):119–123. doi:10.1016/j.diagmicrobio.2010.12.002
16. Li Y, Ding YF, Wu SY, et al. Genetic elements of drug-resistance in a strain of multidrug-resistant Klebsiella pneumoniae isolated from bronchoalveolar lavage fluid. Chin J Clin Infect Dis. 2014;7(2):150–156.
17. Turton JF, Perry C, Elgohari S, et al. PCR characterization and typing of Klebsiella pneumoniae using capsular type-specific, variable number tandem repeat and virulence gene targets. J Med Microbiol. 2010;59(5):541–547. doi:10.1099/jmm.0.015198-0
18. Yu WL, Ko WC, Cheng KC, et al. Comparison of prevalence of virulence factors for Klebsiella pneumoniae liver abscesses between isolates with capsular K1/K2 and non-K1/K2 serotypes. Diagn Microbiol Infect Dis. 2008;62(1):1–6. doi:10.1016/j.diagmicrobio.2008.04.007
19. Zhang Y, Zeng J, Liu W, et al. Emergence of a hypervirulent carbapenem-resistant Klebsiella pneumoniae isolate from clinical infections in China. J Infect. 2015;71(5):553–560. doi:10.1016/j.jinf.2015.07.010
20. Hu Y, Liu C, Shen Z, et al. Prevalence, risk factors and molecular epidemiology of carbapenem-resistant Klebsiella pneumoniae in patients from Zhejiang, China, 2008–2018. Emerg Microbes Infect. 2020;9(1):1771–1779. doi:10.1080/22221751.2020.1799721
21. Micozzi A, Gentile G, Minotti C, et al. Carbapenem-resistant Klebsiella pneumoniae in high-risk haematological patients: factors favouring spread, risk factors and outcome of carbapenem-resistant Klebsiella pneumoniae bacteremias. BMC Infect Dis. 2017;17(1):203. doi:10.1186/s12879-017-2297-9
22. Liu X, Zhang J, Li Y, et al. Diversity and frequency of resistance and virulence genes in bla KPC and bla NDM co-producing Klebsiella pneumoniae strains from China. Infect Drug Resist. 2019;12:2819–2826. doi:10.2147/IDR.S214960
23. Lu MC, Chen YT, Chiang MK, et al. Colibactin contributes to the hypervirulence of pks+ K1 CC23 Klebsiella pneumoniae in mouse meningitis infections. Front Cell Infect Microbiol. 2017;7:103. doi:10.3389/fcimb.2017.00103
24. Choby JE, Howard-Anderson J, Weiss DS. Hypervirulent Klebsiella pneumoniae - clinical and molecular perspectives. J Intern Med. 2020;287(3):283–300. doi:10.1111/joim.13007
25. Struve C, Roe CC, Stegger M, et al. Mapping the evolution of hypervirulent Klebsiella pneumoniae. mBio. 2015;6(4):e00630. doi:10.1128/mBio.00630-15
26. Lee CR, Lee JH, Park KS, et al. Antimicrobial resistance of hypervirulent Klebsiella pneumoniae: epidemiology, hypervirulence-associated determinants, and resistance mechanisms. Front Cell Infect Microbiol. 2017;7:483. doi:10.3389/fcimb.2017.00483
27. Lin ZW, Zheng JX, Bai B, et al. Characteristics of hypervirulent Klebsiella pneumoniae: does low expression of rmpA contribute to the absence of hypervirulence? Front Microbiol. 2020;11:436. doi:10.3389/fmicb.2020.00436
28. Chen Y, Wong J, Sun GW, Liu Y, Tan GY, Gan YH. Regulation of type VI secretion system during Burkholderia pseudomallei infection. Infect Immun. 2011;79(8):3064–3073. doi:10.1128/IAI.05148-11
29. Gallique M, Bouteiller M, Merieau A. The type VI secretion system: a dynamic system for bacterial communication? Front Microbiol. 2017;8:1454. doi:10.3389/fmicb.2017.01454
30. Barbosa VAA, Lery LMS. Insights into Klebsiella pneumoniae type VI secretion system transcriptional regulation. BMC Genom. 2019;20(1):506. doi:10.1186/s12864-019-5885-9
31. Sugawara E, Kojima S, Nikaido H, DiRita VJ. Klebsiella pneumoniae major porins OmpK35 and OmpK36 allow more efficient diffusion of beta-lactams than their Escherichia coli homologs OmpF and OmpC. J Bacteriol. 2016;198(23):3200–3208. doi:10.1128/JB.00590-16
32. Zhang Y, Jiang X, Wang Y, et al. Contribution of beta-lactamases and porin proteins OmpK35 and OmpK36 to carbapenem resistance in clinical isolates of KPC-2-producing Klebsiella pneumoniae. Antimicrob Agents Chemother. 2014;58(2):1214–1217. doi:10.1128/AAC.02045-12
33. Chiu SK, Chan MC, Huang LY, et al. Tigecycline resistance among carbapenem-resistant Klebsiella Pneumoniae: clinical characteristics and expression levels of efflux pump genes. PLoS One. 2017;12(4):e0175140. doi:10.1371/journal.pone.0175140
34. Jiao Y, Qin Y, Liu J, et al. Risk factors for carbapenem-resistant Klebsiella pneumoniae infection/colonization and predictors of mortality: a retrospective study. Pathog Glob Health. 2015;109(2):68–74. doi:10.1179/2047773215Y.0000000004
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.