")
Back to Journals » Infection and Drug Resistance » Volume 13
Antibiotic Resistance and mecA Gene Characterization of Coagulase-negative Staphylococci Isolated from Clinical Samples in Nepal
Authors Shrestha LB , Bhattarai NR, Rai K , Khanal B
Received 31 July 2020
Accepted for publication 25 August 2020
Published 14 September 2020 Volume 2020:13 Pages 3163—3169
DOI https://doi.org/10.2147/IDR.S274163
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Lok Bahadur Shrestha, Narayan Raj Bhattarai, Keshav Rai, Basudha Khanal
Microbiology & Infectious Diseases, B. P. Koirala Institute of Health Sciences, Dharan, Sunsari 56700, Nepal
Correspondence: Lok Bahadur Shrestha
Microbiology & Infectious Diseases, B. P. Koirala Institute of Health Sciences, Dharan 56700, Sunsari, Nepal
Email [email protected]
Background: Coagulase-negative Staphylococci (CoNS) are a significant cause of hospital-acquired and foreign-body-related infections. We conducted this research to assess methicillin susceptibility of CoNS by disc diffusion, agar dilution, and polymerase chain reaction (PCR) methods and to assess the antimicrobial susceptibility pattern.
Methods: We received 123 CoNS isolates from different specimens including blood, endotracheal tube, and central venous catheter. We performed sample processing, identification, and characterization following standard guidelines. Antimicrobial susceptibility was tested based on clinical and laboratory standards institute guidelines. We detected methicillin-resistant coagulase-negative staphylococci (MRCoNS) through mecA gene, disc diffusion method, and agar dilution method and compared the accuracy with PCR as reference.
Results: We detected eight species of CoNS with Staphylococcus epidermidis as the most common. Most of the samples were received from the intensive care unit and blood was the dominant specimen followed by endotracheal-tube aspirate. Seventy-one percentage of isolates were methicillin-resistant by PCR method; disc diffusion and agar dilution method detected methicillin resistance with an accuracy of 96.7% and 98.3%, respectively. Antimicrobial susceptibility revealed an association between the different origins of samples, and also among the types of sample. Similarly, a comparison of the degree of resistance of antimicrobial agents between mecA gene positive and negative isolates showed significant differences. Vancomycin, linezolid, and teicoplanin are still effective for treating MRCoNS.
Conclusion: CoNS are a crucial cause of human infections especially in an intensive care unit setup where the use of devices is common. Disc diffusion and agar dilution are reliable for the detection of MRCoNS. The degree of antimicrobial resistance is much higher in organisms obtained from intensive care unit and foreign-body-related infections.
Keywords: foreign-body-related infections, methicillin-resistant CoNS, mecA gene
Background
Coagulase-negative staphylococci (CoNS) are opportunistic bacteria that have emerged as a vital cause of hospital-acquired infections accounting for 30%.1,2 They frequently cause bloodstream and prostheses-related infections.3 A major surge in incidence of methicillin-resistant coagulase-negative staphylococci (MRCoNS) has occurred over the years. Currently, more than 70% of the CoNS worldwide are MRCoNS.1,3,4 The major mechanism of methicillin resistance is production of penicillin-binding protein (PBP 2a) encoded by the mecA gene.5 There are also some reports of mecC gene encoded methicillin resistance in Staphylococcus aureus and CoNS.6,7 The options for treatment of these infections are limited. Although novel antibiotics like telavancin, dalbavancin, oritavancin and linezolid have been found effective, vancomycin remains the gold standard drug.8 Due to the emergence of vancomycin-resistant staphylococci, the recommendation is to minimize use of this drug.2,9 Therefore, it is mandatory for laboratories to segregate methicillin-susceptible and resistant strains to mitigate inappropriate use of vancomycin.1,2,10
Although cefoxitin disk diffusion and agar dilution test are useful screening methods, detection of mecA gene by molecular method remains a reference method of detecting methicillin resistance among CoNS.2,11
This study aims to assess the methicillin susceptibilities of CoNS by correlating the outcome obtained by the disk diffusion and agar dilution methods with mecA gene detection.
Methods
We carried out this study at B. P. Koirala Insitute of Health Sciences, Dharan, Nepal from January 2018 to December 2018. We received 123 CoNS isolates from diverse samples including blood (n=43), urine (n=30), endotracheal tube (n=24), pus (n=14), and central venous catheter (n=12). We confirmed the isolate as CoNS based on their colony characteristics, gram staining, slide coagulase, and tube coagulase. We used the Kloos and Bannerman method to further characterize the isolates up to species level phenotypically. We employed a battery of biochemical tests like urease, acetoin production, sugars like mannitol, maltose, sucrose, xylose, and trehalose and discs like novobiocin and polymyxin B for characterization.12,13 All tests were performed twice following good clinical and laboratory practice guidelines.
Antimicrobial Susceptibility Testing14,15
We performed antimicrobial susceptibility test of the isolates by the Kirby–Bauer method adhering to clinical and laboratory standard institute (CLSI) guidelines against following antimicrobial discs: amikacin (10 µg), cefalexin (30 µg), ceftriaxone (30 µg), ofloxacin (5 µg), vancomycin (30 µg), linezolid (30 µg), and teicoplanin (30 µg) (HiMedia, India). We checked the quality of all the discs by testing them against Staphylococcus aureus ATCC 25923 before use.
Detection of mecA Gene by PCR16–19
For DNA extraction, we subcultured the isolates onto Mueller–Hinton agar. After growth, we suspended five colonies in 100 μL of Tris-EDTA buffer and heated at 100°C. We centrifuged the solution at 9000 xg for 30 seconds and used 2 μL of supernatant as template in a 50 μL reaction. We used primers (mecA-F: 5’-GTAGAAATGACTGAACGTCCGATGA and mecA-R: 5’- CCAATTCCACATTGTTTCGGTCTAA) based on methodology as described by Jaffe R et al.17 The master mix consist of reaction buffer, MgCl2, dNTPs, mecA primers, Taq polymerase and distilled water. We amplified DNA in a thermocycler (Eppendorf, Germany) and electrophoresed amplicons on a 1.5% agarose gel with 0.5 μg/mL ethidium bromide. We visualized gel under ultraviolet illumination. The positive tests showed PCR product of 310 bp. We used CoNS ATCC 25923 as negative control and CoNS ATCC 43300 as positive control.
Detection of MRCoNS by Disc Diffusion
We used cefoxitin (30 µg) disc along with other antimicrobial discs in the Mueller–Hinton agar plate to detect methicillin resistance.15
Detection of MRCoNS by Agar Dilution Method
We detected MRCoNS by estimating minimum inhibitory concentration (MIC) of oxacillin against the isolates as described by CLSI guidelines.20 We interpreted the results based on the breakpoints provided by the guideline.
Results
We obtained 123 CoNS isolates belonging to eight different species, including Staphylococcus epidermidis (n=51, 42%), S. saprophyticus (n=31, 25%), S. haemolyticus (n=11, 9%), S. lugdunensis (n=9, 7%), S. capitis (n=4, 3%), S. hominis (n=7, 6%) and S. warneri (n=5, 4%) and S. schleiferi (n=5, 4%). We collected majority of samples from intensive care units (n=58, 47%) followed by wards (n=46, 39%) [Table 1]. Regarding specimen type, we received most of the isolates from blood samples (n=43, 34%), followed by urine (n=30, 24%) and endotracheal tube aspirate (n=24,19.5%).
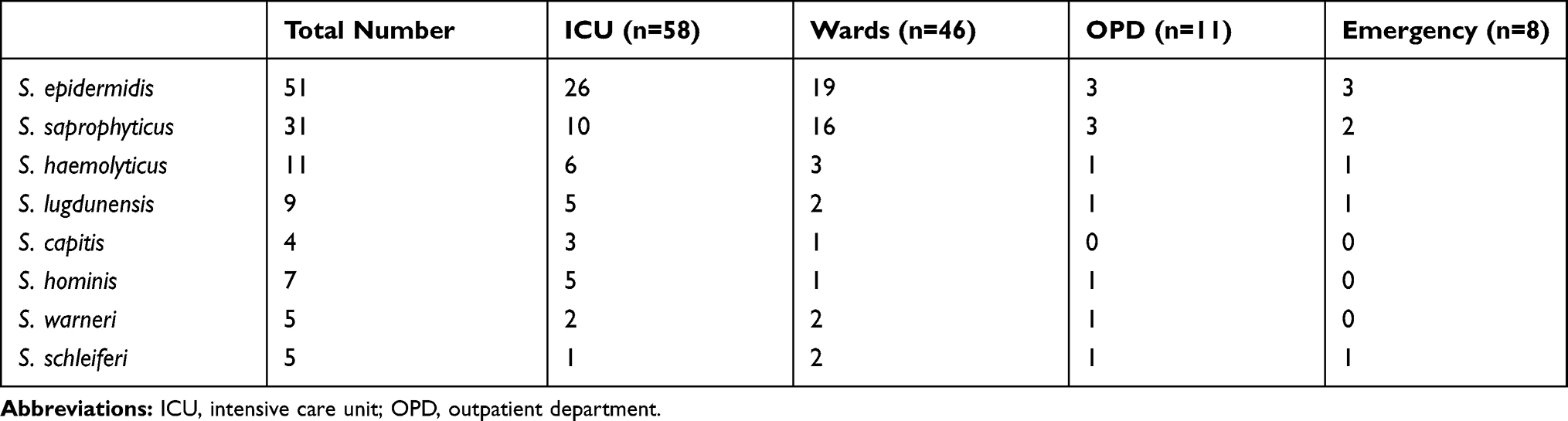 |
Table 1 Number of Organisms with Respect to the Origin of Sample |
We detected mecA gene in 70.7% (n=87) of the isolates. We observed that disc diffusion and agar dilution method detected methicillin resistance with 96.7% and 98.3% accuracy (Table 2).
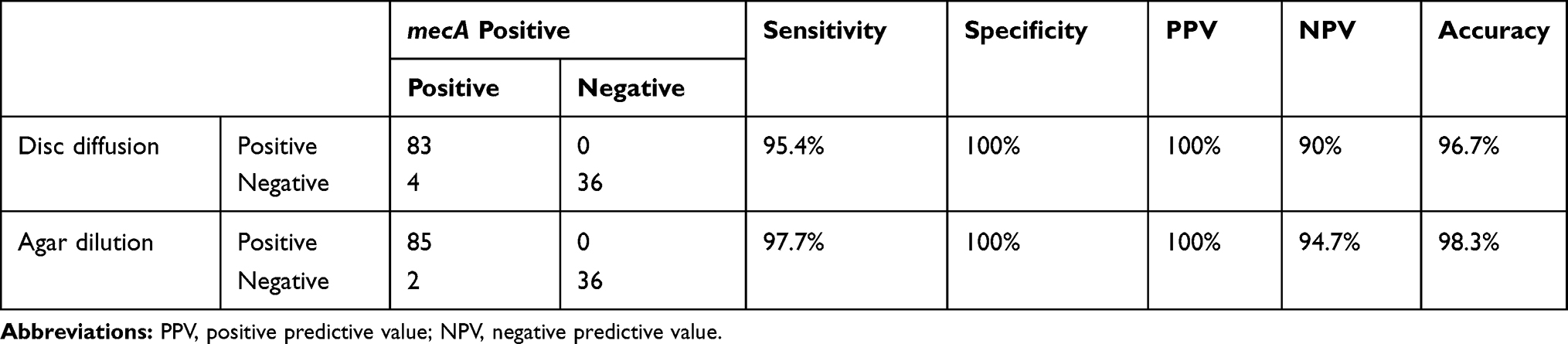 |
Table 2 Comparison of Disc Diffusion and Agar Dilution Method with mecA Gene |
We compared the mecA gene positivity with respect to origin of sample which was statistically significant (P-value 0.0001). The antimicrobial susceptibility was also compared between them, which turned out to be significant (Table 3).
 |
Table 3 Antimicrobial Resistance of Isolates with Respect to Origin |
Similarly, we also compared mecA gene output with the type of specimen. There was a significant difference (P-value <0.0001) between the samples with respect to mecA gene positivity (Table 4).
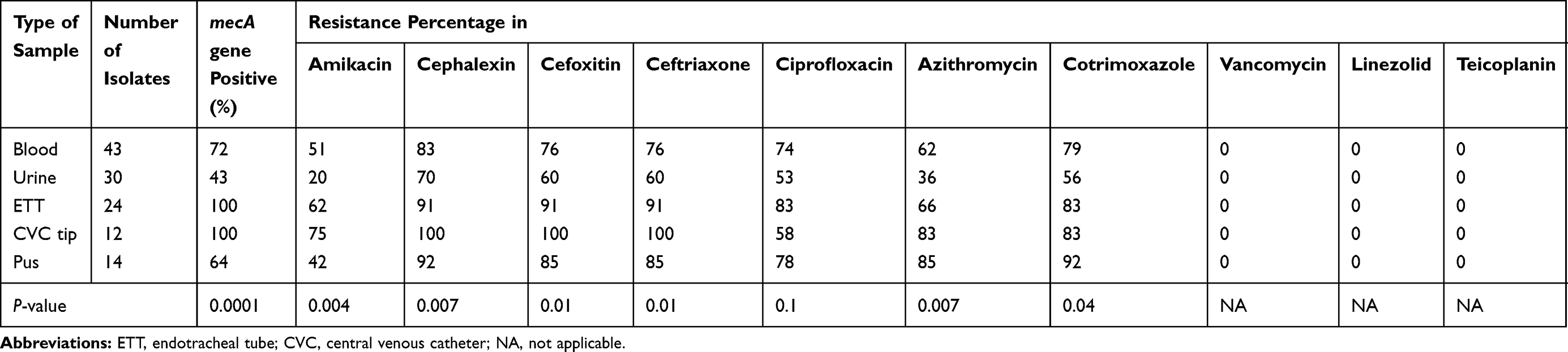 |
Table 4 Antimicrobial Susceptibility Pattern of Isolates with Respect to Type of Sample |
Finally, we observed the degree of antimicrobial resistance among mecA gene positive and negative isolates. We found a highly significant differences between the comparison groups (Table 5).
 |
Table 5 Comparison of Antimicrobial Resistance Between mecA Gene Positive and Negative |
Discussion
We obtained 123 clinically significant CoNS isolates, which were mostly from intensive care units and specimen was blood and device related (endotracheal tube and central venous catheter). Similar types of findings have been reported by many studies done in the past.21–23 CoNS are one of the most prevalent organisms affiliated with health-care-associated and device-associated infections.24 Increased use of medical devices in the ICU makes the patient vulnerable to colonization with CoNS.4,23
We isolated eight different species of CoNS, with S. epidermidis, as the most common. Several studies have identified S. epidermidis as the most commonly isolated CoNS.22,25–29 In contrast, some studies have suggested S. capitis30 and S. hemolyticus10,31,32 as the most common CoNS. S. epidermidis is the most common commensal of our skin and mucosa, and contamination through the devices during medical procedures are very common.4 In this study, S. saprophyticus was the second-most prevalent organism, which was found mostly in urine specimens. According to literature, S. saprophyticus is a frequently isolated CoNS and a common cause of urinary tract infection.4,21,31,33
In this study, we carried out detection of methicillin resistance by PCR method and the mecA gene was encountered in 70.7% of the isolates. The finding is similar to Secchi et al,34 Ferreira et al,11 and Hussain et al.35 Higher rate (87%) of MRCoNS has been reported by Hira et al.36 However, some studies reported a low occurrence of mecA gene positivity.37–39 The high prevalence of mecA gene positive isolates in our study might be due to the fact that most samples were received from intensive care units and almost all patients admitted in our hospitals are treated in primary care hospitals with several courses of antibiotics and referred here.
The prevalence of mecA gene positivity with respect to the origin of samples showed that 93% of patients from ICU were positive, while only 63% of patients from the ward and 6% of OPD were mecA gene positive (P-value <0.0001). Similar data were reported by Ehsan et al,40 Singh et al,32 and Avgald-Ohman et al.41 The higher occurrence of the mecA gene in ICU patients is due to long hospital stay, frequent invasive medical procedures, use of multiple antimicrobials, and chronic debilitated patients.4,42
Our study showed a sensitivity of 95.4% and 97.7% with disc diffusion and agar dilution methods, while specificity was 100% for both. Similar conclusions have been revealed by Secchi et al34 and Bhatt et al.37 Ferreira et al showed that although the sensitivity of both tests was high, specificity was lower (91% for disc diffusion and 73.5% for agar dilution).11 Contrary to our finding, Graham et al39 revealed that disc diffusion and dilution methods are inadequate to detect methicillin resistance. However, they have used oxacillin disc for disc diffusion and MIC was studied using E-test, which is different from our study. Other studies suggest that disc diffusion and agar dilution methods are reliable methods for the detection of methicillin resistance in CoNS.43,44
The comparison of antimicrobial susceptibility between mecA gene positive and negative isolates showed statistical difference. Amikacin resistance was exhibited in 55% of mecA positive isolates, while negative ones demonstrated 27% resistance (P-value 0.007) and a similar pattern was seen among other antimicrobials. The finding is similar to several studies.11,32,45–47 Origin-wise analysis of resistance pattern also showed a highly notable variation ie P-value <0.05 in amikacin, cephalexin, ceftriaxone, cotrimoxazole, azithromycin. The finding is coherent with other studies.32,42,48 Similarly, sample-wise analysis of resistance pattern reveals a significant difference in the degree of antimicrobial resistance between device-related samples and other samples (urine, pus). The finding is consistent with several other studies.23,49 Multiple hospital admissions, frequent instrumentations and the capacity to establish multilayered biofilms on the surfaces makes these organisms resistant to most antimicrobials.4,23,24
Our study also demonstrated no resistance against vancomycin, linezolid, and teicoplanin; hence, these drugs remain the mainstay of treatment for CoNS isolates. The finding is in concordance with several other studies.23,25,32,49 However, some studies suggest that there has been an increase in the number of cases with glycopeptide resistance.4,42,50 Although S. aureus receives more attention due to its virulence and methicillin-resistance, nevertheless, CoNS also deserves attention from clinicians due to its increasing significance and resistance.51
Conclusion
CoNS are crucial etiological agent of human infections especially in the ICU setup where the use of medical devices is common. Disc diffusion and agar dilution methods are simple and reliable methods for the detection of MRCoNS. The degree of antimicrobial resistance is much higher in isolates obtained from the intensive care unit and foreign-body-related infections. Resistance is much higher among mecA gene producer isolates as compared to negative ones.
Ethical Clearance
Obtained from Institutional Review Committee, BPKIHS (456/075/76-IRC).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kloos WE, Bannerman TL. Update on clinical significance of coagulase-negative staphylococci. Clin Microbiol Rev. 1994. doi:10.1128/CMR.7.1.117
2. Xu Z, Mkrtchyan HV, Cutler RR. Antibiotic resistance and mecA characterization of coagulase-negative staphylococci isolated from three hotels in London, UK. Front Microbiol. 2015;6:
3. Rupp ME, Archer GL. Coagulase-negative staphylococci: pathogens associated with medical progress. Clin Infect Dis. 1994;19(2):231–245. doi:10.1093/clinids/19.2.231
4. Becker K, Heilmann C, Peters G. Coagulase-negative staphylococci. Clin Microbiol Rev. 2014. doi:10.1128/CMR.00109-13
5. Chambers HF. Methicillin resistance in staphylococci: molecular and biochemical basis and clinical implications. Clin Microbiol Rev. 1997;10(4):781–791. doi:10.1128/cmr.10.4.781
6. Gajdács M, Urbán E. Epidemiology and resistance trends of staphylococcus aureus isolated from vaginal samples: A 10-year retrospective study in hungary. Acta Dermatovenerologica Alpina Pannonica Adriat. 2019;28(4):143–147. doi:10.15570/actaapa.2019.35
7. Venugopal N, Mitra S, Tewari R, et al. Molecular detection and typing of methicillin-resistant Staphylococcus aureus and methicillin-resistant coagulase-negative staphylococci isolated from cattle, animal handlers, and their environment from Karnataka, Southern Province of India. Vet World. 2019;12(11):1760–1768. doi:10.14202/vetworld.2019.1760-1768
8. Gajdács M. The continuing threat of methicillin-resistant Staphylococcus Aureus. Antibiotics. 2019;8(2):2. doi:10.3390/antibiotics8020052
9. Srinivasan A, Dick JD, Perl TM. Vancomycin resistance in Staphylococci. Clin Microbiol Rev. 2002;15(3):430–438. doi:10.1128/CMR.15.3.430-438.2002
10. Jain A, Agarwal J, Bansal S. Prevalence of methicillin-resistant, coagulase-negative staphylococci in neonatal intensive care units: findings from a tertiary care hospital in India. J Med Microbiol. 2004;53(9):941–944. doi:10.1099/jmm.0.45565-0
11. Ferreira RBR, Iorio NLP, Malvar KL, et al. Coagulase-negative staphylococci: comparison of phenotypic and genotypic oxacillin susceptibility tests and evaluation of the agar screening test by using different concentrations of oxacillin. J Clin Microbiol. 2004;42(8):3913. doi:10.1128/JCM.42.8.3913.2004
12. Winn W, Allen S, Janda W. Koneman’s Color Atlas and Textbook of Diagnostic Microbiology.
13. Kloos WE, Schleifer KH. Simplified scheme for routine identification of human Staphylococcus species. J Clin Microbiol. 1975. doi:10.1128/jcm.1.1.82-88.1975
14. Bauer AW, Kirby WM, Sherris JC, Turck M. Antibiotic susceptibility testing by a standardized single disk method. Am J Clin Pathol. 1966. doi:10.1093/ajcp/45.4_ts.493
15. CLSI. Clinical and Laboratory Standards Institute. Document No M100S. Performance Standards for Antimicrobial Susceptibility Testing.
16. Sambrookm J, Fritsch EF, Maniatis T. Molecular Cloning, a Laboratorry Manual. New York: Cold Spring Harbor Laboratory Press; 2001.
17. Jaffe RI, Lane JD, Albury SV, Niemeyer DM. Rapid extraction from and direct identification in clinical samples of methicillin-resistant staphylococci using the PCR. J Clin Microbiol. 2000;38(9):3407–3412. doi:10.1128/jcm.38.9.3407-3412.2000
18. Ryffel C, Kayser FH, Berger-Bachi B. Correlation between regulation of mecA transcription and expression of methicillin resistance in staphylococci. Antimicrob Agents Chemother. 1992;36(1):25–31. doi:10.1128/AAC.36.1.25
19. Goudarzi M, Tayebi Z, Fazeli M, Miri M, Nasiri MJ. Molecular characterization, drug resistance and virulence analysis of constitutive and inducible clindamycin resistance Staphylococcus aureus strains recovered from clinical samples, Tehran – iran. Infect Drug Resist. 2020;13:1155–1162. doi:10.2147/IDR.S251450
20. Clinical and Laboratory Standards Institute. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically, CLSI Document No M07-A9.
21. Shrestha LB, Baral R, Khanal B. Comparative study of antimicrobial resistance and biofilm formation among Gram-positive uropathogens isolated from community-acquired urinary tract infections and catheter-associated urinary tract infections. Infect Drug Resist. 2019;12:957–963. doi:10.2147/IDR.S200988
22. Oliveira A, Cunha MDLRS. Comparison of methods for the detection of biofilm production in coagulase-negative staphylococci. BMC Res Notes. 2010;3(1). doi:10.1186/1756-0500-3-260
23. Tayyar A, Al-Zoubi MS, Hussein E, Khudairat S, Sarosiekf K. Prevalence and antimicrobial susceptibility pattern of coagulase-negative staphylococci (CoNS) isolated from clinical specimens in northern of Jordan. Iran J Microbiol. 2015;7(6):294–301.
24. Von Eiff C, Jansen B, Kohnen W, Becker K. Infections associated with medical devices: pathogenesis, management and prophylaxis. Drugs. 2005. doi:10.2165/00003495-200565020-00003
25. Bora P, Datta P, Gupta V, Singhal L, Chander J. Characterization and antimicrobial susceptibility of coagulase-negative staphylococci isolated from clinical samples. J Lab Physicians. 2018. doi:10.4103/jlp.jlp_55_18
26. Lourtet-Hascoët J, Félicé MP, Bicart-See A, Bouige A, Giordano G, Bonnet E. Species and antimicrobial susceptibility testing of coagulase-negative staphylococci in periprosthetic joint infections. Epidemiol Infect. 2018;146(14):1771–1776. doi:10.1017/S0950268818001437
27. Shrestha LB, Bhattarai NR, Khanal B. Antibiotic resistance and biofilm formation among coagulase-negative staphylococci isolated from clinical samples at a tertiary care hospital of eastern Nepal. Antimicrob Resist Infect Control. 2017;6(1):1–7. doi:10.1186/s13756-017-0251-7
28. Shrestha L, Bhattarai NR, Khanal B. Comparative evaluation of methods for the detection of biofilm formation in coagulase-negative staphylococci and correlation with antibiogram. Infect Drug Resist. 2018;11:607–613. doi:10.2147/IDR.S159764
29. Khosravi AD, Roointan M, Montazeri EA, Aslani S, Hashemzadeh M, Soodejani MT. Application of tuf gene sequence analysis for the identification of species of coagulase-negative staphylococci in clinical samples and evaluation of their antimicrobial resistance pattern. Infect Drug Resist. 2018;11:1275–1282. doi:10.2147/IDR.S172144
30. De Vecchi E, George DA, Romanò CL, Pregliasco FE, Mattina R, Drago L. Antibiotic sensitivities of coagulase-negative staphylococci and staphylococcus aureus in hip and knee periprosthetic joint infections: does this differ if patients meet the international consensus meeting criteria? Infect Drug Resist. 2018;11:539–546. doi:10.2147/IDR.S151271
31. Singh L, Cariappa MP, Das NK. Drug sensitivity pattern of various staphylococcus species isolated at a tertiary care hospital. Med J Armed Forces India. 2016;72:S62–S66. doi:10.1016/j.mjafi.2016.07.009
32. Singh S, Dhawan B, Kapil A, et al. Coagulase-negative staphylococci causing blood stream infection at an Indian tertiary care hospital: prevalence, antimicrobial resistance and molecular characterisation. Indian J Med Microbiol. 2016;34(4):500–505. doi:10.4103/0255-0857.195374
33. Shrestha LB, Baral R, Poudel P, Khanal B. Clinical, etiological and antimicrobial susceptibility profile of pediatric urinary tract infections in a tertiary care hospital of Nepal. BMC Pediatr. 2019;19(1):1. doi:10.1186/s12887-019-1410-1
34. Secchi C, Souza Antunes AL, Rodrigues Perez LR, Cantarelli VV, d’Azevedo PA. Identification and detection of methicillin resistance in non-Epidermidis coagulase-negative staphylococci. Brazilian J Infect Dis. 2008;12(4):316–320. doi:10.1590/S1413-86702008000400012
35. Hussain Z, Stoakes L, Massey V, et al. Correlation of oxacillin MIC with mecA gene carriage in coagulase- negative staphylococci. J Clin Microbiol. 2000;38(2):752–754. doi:10.1128/jcm.38.2.752-754.2000
36. Hira V, Sluijter M, Estevão S, et al. Clinical and molecular epidemiologic characteristics of coagulase-negative staphylococcal bloodstream infections in intensive care neonates. Pediatr Infect Dis J. 2007;26(7):607–612. doi:10.1097/INF.0b013e318060cc03
37. Bhatt P, Tandel K, Singh A, Mugunthan M, Grover N, Sahni AK. Species distribution and antimicrobial resistance pattern of Coagulase-negative staphylococci at a tertiary care centre. Med J Armed Forces India. 2016;72(1):71–74. doi:10.1016/j.mjafi.2014.12.007
38. Pournajaf A, Ardebili A, Goudarzi L, Khodabandeh M, Narimani T, Abbaszadeh H. PCR-based identification of methicillin-resistant Staphylococcus aureus strains and their antibiotic resistance profiles. Asian Pac J Trop Biomed. 2014;4(1067):S293–S297. doi:10.12980/APJTB.4.2014C423
39. Graham JC, Murphy OM, Stewart D, Kearns AM, Galloway A, Freeman R. Comparison of PCR detection of mecA with methicillin and oxacillin disc susceptibility testing in coagulase-negative staphylococci. J Antimicrob Chemother. 2000;45(1):111–113. doi:10.1093/jac/45.1.111
40. Ehsan MM, Memon Z, Ismail MOFG. Identification and antibiotic susceptibility pattern of coagulase-negative staphylococci in various clinical specimens. Pakistan J Med Sci. 2013;29(6):1420–1424. doi:10.12669/pjms.296.4064
41. Agvald-Ohman C, Lund B, Hjelmqvist H, Hedin G, Struwe J, Edlund C. ICU stay promotes enrichment and dissemination of multiresistant coagulase-negative staphylococcal strains. Scand J Infect Dis. 2006;38(6–7):441–447. doi:10.1080/00365540600561751
42. Pereira VC, Romero LC, Pinheiro-Hubinger L, Oliveira A, Martins KB, Cunha MDLRDSD. Coagulase-negative staphylococci: a 20-year study on the antimicrobial resistance profile of blood culture isolates from a teaching hospital. Brazilian J Infect Dis. 2020;4(2):160–169. doi:10.1016/j.bjid.2020.01.003
43. Pereira VC, da Cunha M. Coagulase-negative staphylococci strains resistant to oxacillin isolated from neonatal blood cultures. Mem Inst Oswaldo Cruz. 2013;108(7):939–942. doi:10.1590/0074-0276130644
44. García A, Martínez C, Juárez RI, et al. Methicillin resistance and biofilm production in clinical isolates of Staphylococcus aureus and coagulase-negative Staphylococcus in México. Biomedica. 2019;39(3):513–523. doi:10.7705/biomedica.4131
45. Sharma V, Jindal N, Devi P. Prevalence of methicillin resistant coagulase negative staphylococci in a tertiary care hospital. Iran J Microbiol. 2010;2(4):185–188.
46. Nasaj M, Saeidi Z, Asghari B, Roshanaei G, Arabestani MR. Identification of hemolysin encoding genes and their association with antimicrobial resistance pattern among clinical isolates of coagulase-negative Staphylococci. BMC Res Notes. 2020;13(1):68. doi:10.1186/s13104-020-4938-0
47. Koksal F, Yasar H, Samasti M. Antibiotic resistance patterns of coagulase-negative staphylococcus strains isolated from blood cultures of septicemic patients in Turkey. Microbiol Res. 2009;164(4):404–410. doi:10.1016/j.micres.2007.03.004
48. Latif M, Usman J, Gilani M, Munir T, Mushtaq M, Anjum R. Coagulase negative staphylococci - a fast emerging threat. J Pak Med Assoc. 2015;65(3):283–286.
49. Jain A, Agarwal A, Verma RK, Awasthi S, Singh KP. Intravenous device associated blood stream staphylococcal infection in paediatric patients. Indian J Med Res. 2011;134(2):193–199.
50. Mashaly GES, El-Mahdy RH. Vancomycin heteroresistance in coagulase negative Staphylococcus blood stream infections from patients of intensive care units in Mansoura University Hospitals, Egypt. Ann Clin Microbiol Antimicrob. 2017;16(1):3–7. doi:10.1186/s12941-017-0238-5
51. Gajdács M. The concept of an ideal antibiotic: implications for drug design. Molecules. 2019;24(5):5. doi:10.3390/molecules24050892
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.