")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 14
Anti-Ribosomal-P Antibody Association with Neuropsychiatric Lupus in Sudanese Patients Attending Rheumatology Clinic in Omdurman Military Hospital
Authors Taha ZI, Awad Ibrahim IA, Hamza SB , Abdalla YA , Elagib EM, Ali HAM, Joseph S, William J
Received 12 September 2022
Accepted for publication 16 November 2022
Published 21 November 2022 Volume 2022:14 Pages 281—289
DOI https://doi.org/10.2147/OARRR.S387650
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Ziryab Imad Taha,1– 4 Israa Abdelghani Awad Ibrahim,3,4 Salih Boushra Hamza,4,5 Yassin A Abdalla,4,5 Elnour M Elagib,3,4,6 Husam A M Ali,4,7 Sara Joseph,8 Jimmy William4,9
1Medical and Cancer Research Institute (MCRI), Department of Clinical Medicine, Nyala, Sudan; 2University of Bahri, Department of Internal Medicine, Khartoum, Sudan; 3Sudan Medical Specialization Board, Department of Internal Medicine, Khartoum, Sudan; 4Rheumatology Department, Ziryab Research Group, Khartoum, Sudan; 5Omdurman Islamic University, Department of Internal Medicine, Khartoum, Sudan; 6Omdurman Military Hospital, Department of Rheumatology, Omdurman, Sudan; 7Fedail Hospital, Department of Neurology, Khartoum, Sudan; 8University of Medical Sciences and Technology, Department of Pharmacy, Khartoum, Sudan; 9Sligo University Hospital, Department of Haematology, Sligo, Ireland
Correspondence: Jimmy William, Sligo University Hospital, The Mall, Rathquarter, Sligo, F91 H684, Ireland, Tel +353851173213, Email [email protected]
Purpose: To assess and establish the relationship between neuropsychiatric systemic lupus erythematosus (NPSLE) involvement and serological biomarkers like antiribosomal-P antibodies.
Patients and Methods: This is an analytical cross-sectional hospital-based study conducted on patients attending Omdurman Military Hospital from July 2019 to December 2019. A total of 90 patients were enrolled, 30 of whom had NPSLE compared with 60 SLE patients without NPSLE. SLE diagnosis was established based on the revised SLICC criteria (presence of at least 4 criteria) for SLE classification, with neuropsychiatric manifestations defined based on the ACR nomenclature. The immunological examination results have been performed by (ELISA immune-enzymatic method, immunofluorescence, and Western immunoblotting test). SPSS v 21.0 software was utilised for data analysis.
Results: NPSLE patients exhibited +ve ANA in 96.7% vs 75% in non-NPSLE (P-value = 0.008), antiribosomal-P antibodies (46.7% vs 20%; P-value = 0.0001), anti-nucleosome antibodies (26.7% vs 5%; P-value = 0.005), and anti-histones antibodies (40% vs 20%; P-value = 0.04). ANA antibodies were significantly associated with neurological manifestations as ANA antibodies were common in epilepsy (n = 9; 91%) and stroke (n = 8; 27.6%) (P-value < 0.001).
Conclusion: Neuropsychiatric manifestation of systemic lupus erythematosus exhibits variable clinical manifestations. Neuropsychiatric manifestations of SLE are strongly associated with the anti-ribosomal P antibody presence and can be employed as a powerful diagnostic tool.
Keywords: SLE, neuropsychiatric, ANA, anti-ribosomal-P antibodies, anti-histone antibodies
Introduction
One of the highest globally prevalent autoimmune diseases is systemic lupus erythematosus (SLE), which predominantly afflicts females of childbearing age, leading to significant morbidity burden and mortality. A primary concern regarding SLE is its fluctuating course and unpredictable flares leading to a relapse-remitting pattern. The principal aetiology behind SLE development is unknown; however, it is possibly multifactorial, including environmental factors, medications and hormonal and other factors collectively causing dysregulation of the immune system and consequently leading to autoantibodies production and precipitation in almost all body organs.1 The clinical presentation complexity of SLE makes its recognition and diagnosis challenging to define, mandating the utilisation of classification criteria to identify and differentiate relatively akin patients’ groups.2 Hence, the American College of Rheumatology (ACR) SLE classification criteria and its revised version in the late nineties were globally applied and consequently improved our insight about the disease.3 This improvement was evident in routine clinical practice by demonstrating several explicit skin manifestations and utilising immunological tests like complement levels (C3 &C4) and anti-B2Glycoprotein I (Anti-B2GPI) antibodies. Furthermore, mucocutaneous and several other organ involvements were better understood, warranting modifications to the classification criteria employed.4 Consequently, the Systemic Lupus International Collaborating Clinics (SLICC) classification criteria 2012 was launched, addressing several considerations.5 The newer criteria included mucocutaneous and neuropsychiatric manifestations, extra antiphospholipid antibody tests, hypocomplementemia, and refinement of criteria definitions. SLE diagnosis is established by the presence of at least one immunologic and clinical criteria or biopsy‐proven nephritis consistent with SLE and the presence of antinuclear antibodies (ANA) or anti-double-stranded DNA (dsDNA) antibodies. When comparing both criteria, the SLICC criteria had lower specificity but raised sensitivity than the ACR criteria.5,6
Furthermore, in 2019, the EULAR/ACR classification criteria for SLE were introduced. It included ten domains, each weighted 2 to 10; seven clinical (Cutaneous, Serosal, Haematologic, Renal Neuropsychiatric, Musculoskeletal, and Constitutional) as well as three immunologic (SLE‐specific antibodies, antiphospholipid antibodies, and complement proteins). A positive ANA is a requisite entry criterion and cumulative weighted criterion subsequently. Upon assessing the three criteria, the EULAR/ACR criteria achieved the highest specificity and sensitivity of 93.4% and 96.1% as compared to 93% and 82.8% and 83.7% and 96.7% by revised ACR and SLICC criteria, respectively.3
Furthermore, neuropsychiatric manifestations could be the presenting symptom of systemic lupus erythematosus.7 These manifestations range from mild to severe, requiring high clinical suspicion to recognise and diagnose early.7 The common presentations include anxiety, mood disorders, cognitive deterioration and others. However, the unpredictable patterns in the presentation of NPSLE and the frequent encounters with atypical or delayed characteristic laboratory findings make NPSLE very challenging even in a current era of enormous technological advancement.8 Thus, recognising a biomarker to aid early diagnosis is crucial as it will impact outcomes and reduce comorbidities associated with such a devastating disease.9 In 1985, anti-ribosomal P antibodies were recognised, with ongoing studies emphasising their prognostic value and implications. These autoantibodies occur exclusively in SLE.9 However, several studies have highlighted a potential direct association between anti-ribosomal P antibodies and NPSLE, although no clear-cut decision was concluded.8 In this current study, we emphasise the correlation between neuropsychiatric systemic lupus erythematosus (NPSLE) involvement and serological biomarkers like antiribosomal-P antibodies.
Materials and Methods
Participants
This is an analytical case–control hospital-based study conducted in the rheumatology clinic at Omdurman Military Hospital in Sudan from July 2019 to December 2019. We included all patients with systemic lupus erythematosus who demonstrated neuropsychiatric manifestations and fulfilled the ACR (NPSLE) criteria. In contrast, our control group included SLE patients with no NP manifestations fulfilling a minimum of 4 criteria of the revised ACR classification for SLE. Patients with neuropsychiatric disorders other than SLE and patients with other coexistent connective tissue diseases were excluded. Both case and control group patients were randomly selected and matched by age, sex, and level of education.
Ethical Consideration
Ethical approval was obtained from Sudan Medical Specialisation Board (SMSB) under approval no. QA-9176. Approval acceptance to the hospital authority was given. Patients were counselled about the purpose of the study. The study complied with the tenets of the Declaration of Helsinki. Written and verbal consent were obtained from patients. Data was used anonymously using identity numbers instead of names to protect the patient’s identity and kept securely and in a separate file. No reference to any individual participant was made in the study reports. Subject identities were known only by the study staff.
Data Collection Tools and Methods
We used an interview questionnaire as a data collection tool; data from files and records of patients were obtained, and a complete medical history and clinical examination were conducted on all patients. SLE diagnosis was established upon the presence of at least 4 of the 11 revised SLICC criteria.5 The nomenclature of ACR was used to define neuropsychiatric manifestations. Standard laboratory examinations were performed, and the immunological examination was performed by (ELISA immune-enzymatic method, immunofluorescence, and Western immunoblotting test).
Data Analysis
The collected data was entered and encoded in SPSS (SPSS v.21.0) datasheet. The data were analysed and presented in tables and figures. Chi-square test/Fisher exact test was used to assess the associations between continuous and categorical data, with a P-value considered significant if less than 0.05. Adjusted P-value (AdjP-value) was also calculated via the Chow–Denning test as required.
Results
Characteristics of the Patients
The overall recruitment in this study included 90 SLE patients, 30 patients with neuropsychiatric SLE (NPSLE) and 60 non-neuropsychiatric SLE (non-NPSLE). NPSLE patients’ mean age was 36.6 ± 12.3 years, and non-NPSLE was 37.3 ± 12.5 years. All the NPSLE patients (n = 30; 100%) and 55 (91.7%) of non-NPSLE were females (Table 1).
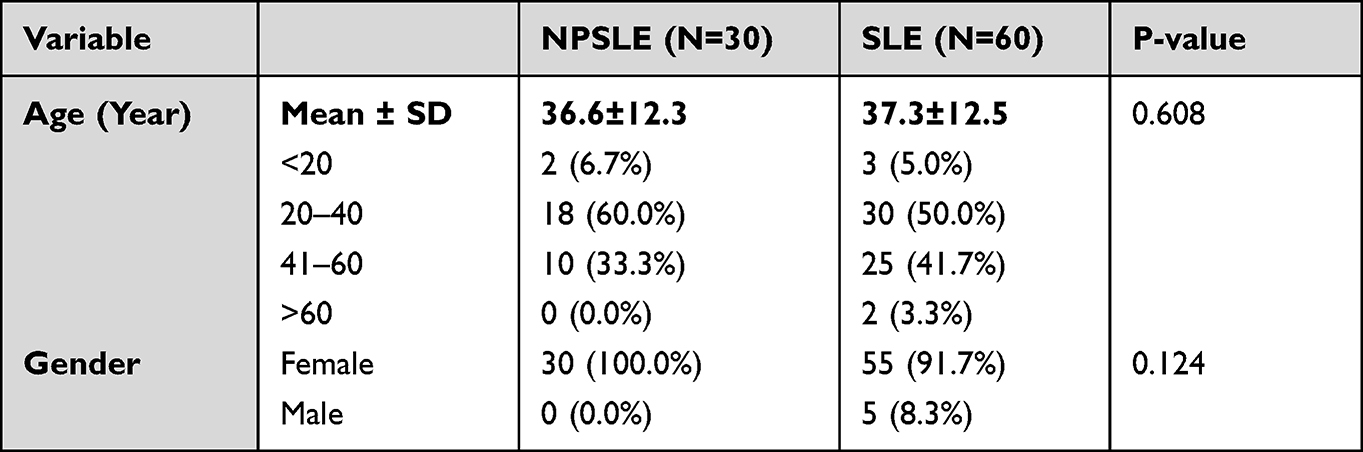 |
Table 1 The Sociodemographic Characteristics of NPSLE and Non-NPSLE Groups |
The mean SLE duration was 4.7 ± 3.3 years, and 19 (64%) had an SLE duration of fewer than five years. Also, the mean NPSLE duration was 3.4 ± 2.6 years; 22 (73.3%) patients had an NPSLE duration of fewer than five years, and the remaining 8 (27%) patients had a duration of 5–10 years.
Clinical Presentations
Cutaneous clinical presentations, hair loss (80% vs 56.7%; P-value = 0.024) and oral ulcer (73.3% vs 46.7%; P-value = 0.014) were significantly common among NPSLE patients more than non-NPSLE patients (Table 2).
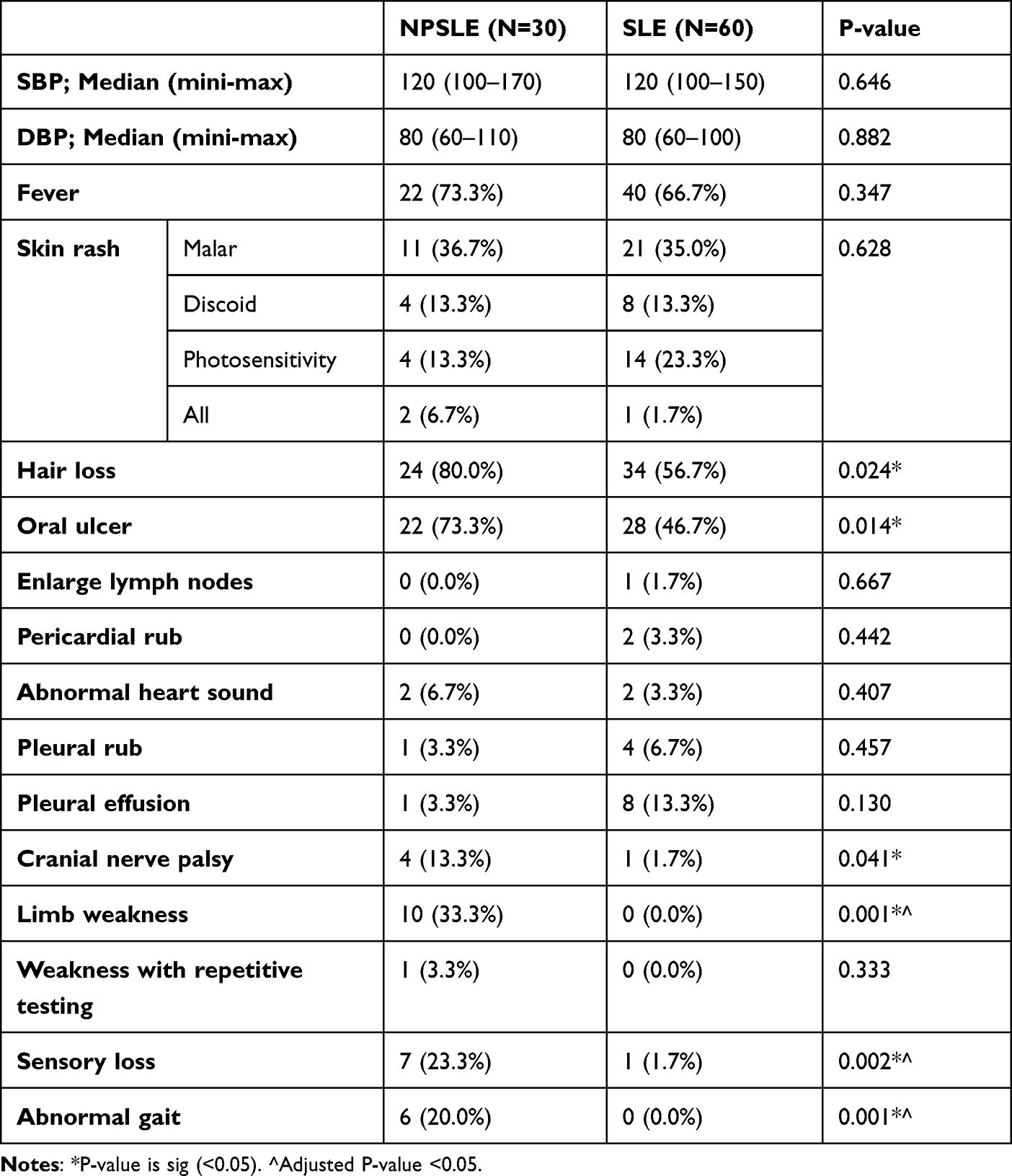 |
Table 2 The Clinical Presentations of NPSLE and Non-NPSLE Groups |
Neuropsychiatric Manifestations
Headache (n = 26; 86.7%) and confusion (n = 16; 53.3%) were the major CNS-related clinical presentations, and excessive anxiety was the main psychiatric-related presentation in 14 (46.7%) patients. The Mini-Mental State Examination scale (MMSE) was used to assess cognitive function; 18 (60%) patients were normal, while 12 (40%) were borderline. The clinical examinations showed that NPSLE patients more likely to have cranial nerve palsy (13.3% vs 1.7%; P-value = 0.041), limb weakness (33.3% vs 0%; P-value = 0.000), sensory loss (23.3% vs 1.7%; P-value = 0.002) and abnormal gait (20% vs 0%; P-value = 0.001) more than non-NPSLE patients (Table 3) patients had borderline findings and 12 (20%) patients were normal (Table 2).
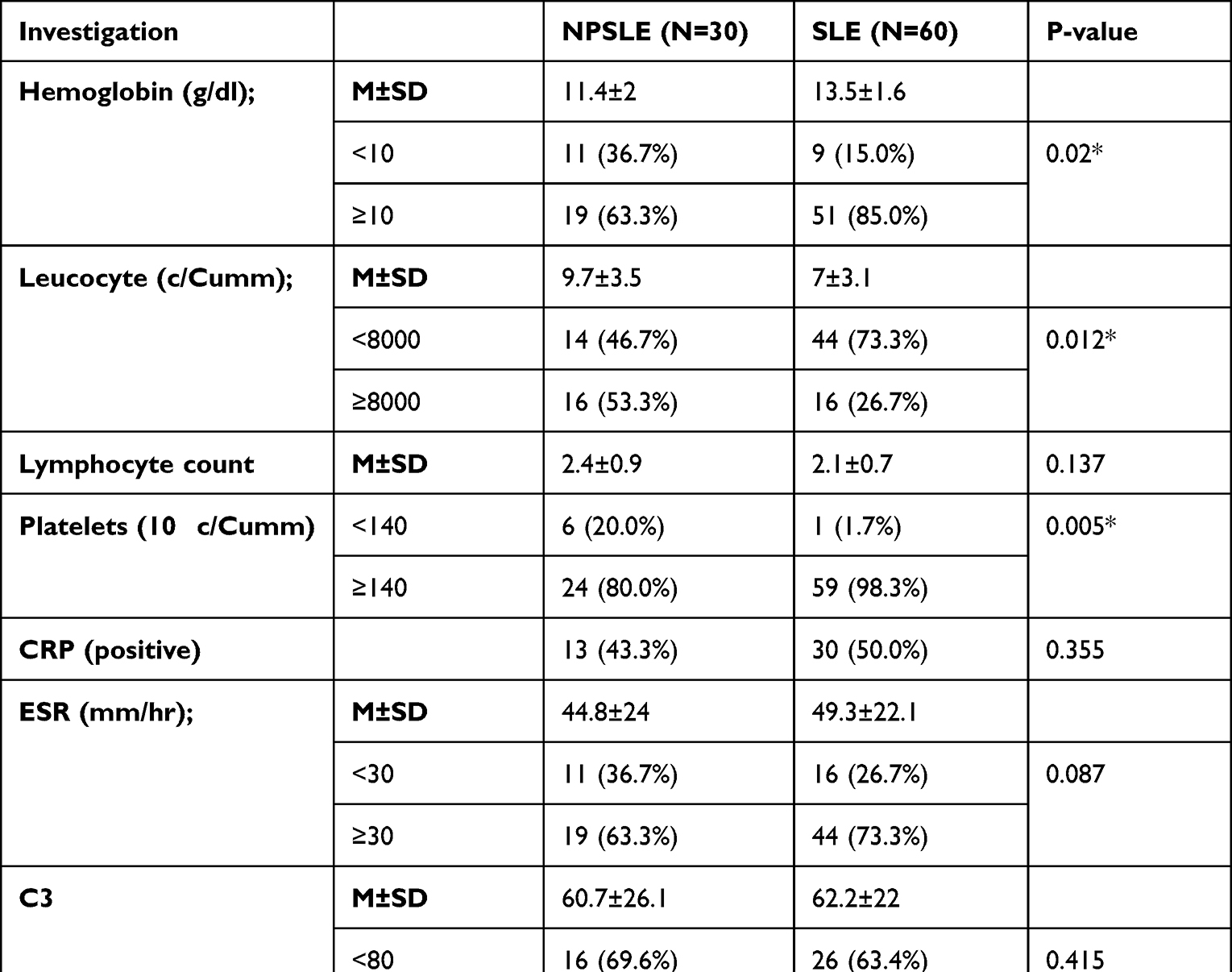 |
Table 3 The Laboratory Investigations of NPSLE and Non-NPSLE Groups |
Laboratory Investigations
Hematological laboratory investigations showed that NSPLE patients were more prone to anemia than non-NSPLE patients (hemoglobin <10 g/dl) (36.7% vs 15%; P-value = 0.02) with hemoglobin means (11.4 ± 2 g/dl vs 13.5 ± 1.6 g/dl). NSPLE patients were more predisposed to have leukocytosis than non-NSPLE patients (leucocytes <8000 cell/Cumm) (53.3% vs 26.7%; P-value = 0.012) with leucocytes count means (9.7 ± 3.5 cell/Cumm vs 7 ± 3.1 cell/Cumm). In addition, thrombocytopenias were observed more in NSPLE patients than non-NSPLE patients (platelets <148*103 cell/mm) (20% vs 1.7%; P-value = 0.005) with platelets count means (210*103 ± 79.5 cell/mm vs 279*103 ± 65 cell/mm). Inflammatory investigations included CRP (P-value = 0.335), ESR (P-value = 0.087), C3 complement levels (P-value = 0.415) and C4 complement levels (P-value = 0.528) were not significantly varying between both groups. Moreover, hypoalbuminemia was common among NPSLE than non-NPSLE patients (36.7% vs 11.6%; P-value = 0.008). Nevertheless, blood glucose levels (P-value = 0.078), urea levels (P-value = 0.407), creatinine levels (P-value = 0.204), proteinuria (P-value = 0.552) and urine cellular cast (P-value = 0.543); all showing no significant differences between the NPSLE and non-NPSLE groups (Table 3).
Furthermore, ANA titres were more positive among NPSLE patients than in the non-NPSLE group (96.7% vs 75%; P-value = 0.008). Similarly, anti-ribosomal-p antibodies, anti-histones antibodies and anti-nucleosome antibodies were more positive among NPSLE group than non-NPSLE group (46.7% vs 20%; P-value = 0.001), (26.7% vs 5%; P-value = 0.005), (40% vs 20%; P-value = 0.04), respectively. Other ANA profile antibodies were not significantly varying between NPSLE and the control groups (Table 4). Additionally, anti-lupus antibodies (26.7% vs 1.7%; P-value = 0.001), anticoagulant antibodies (30% vs 3.3%; P-value = 0.001), and anticardiolipin antibodies (26.7% vs 0%; P-value = 0.001) were significantly more observed in NPSLE group than the non-NPSLE group.
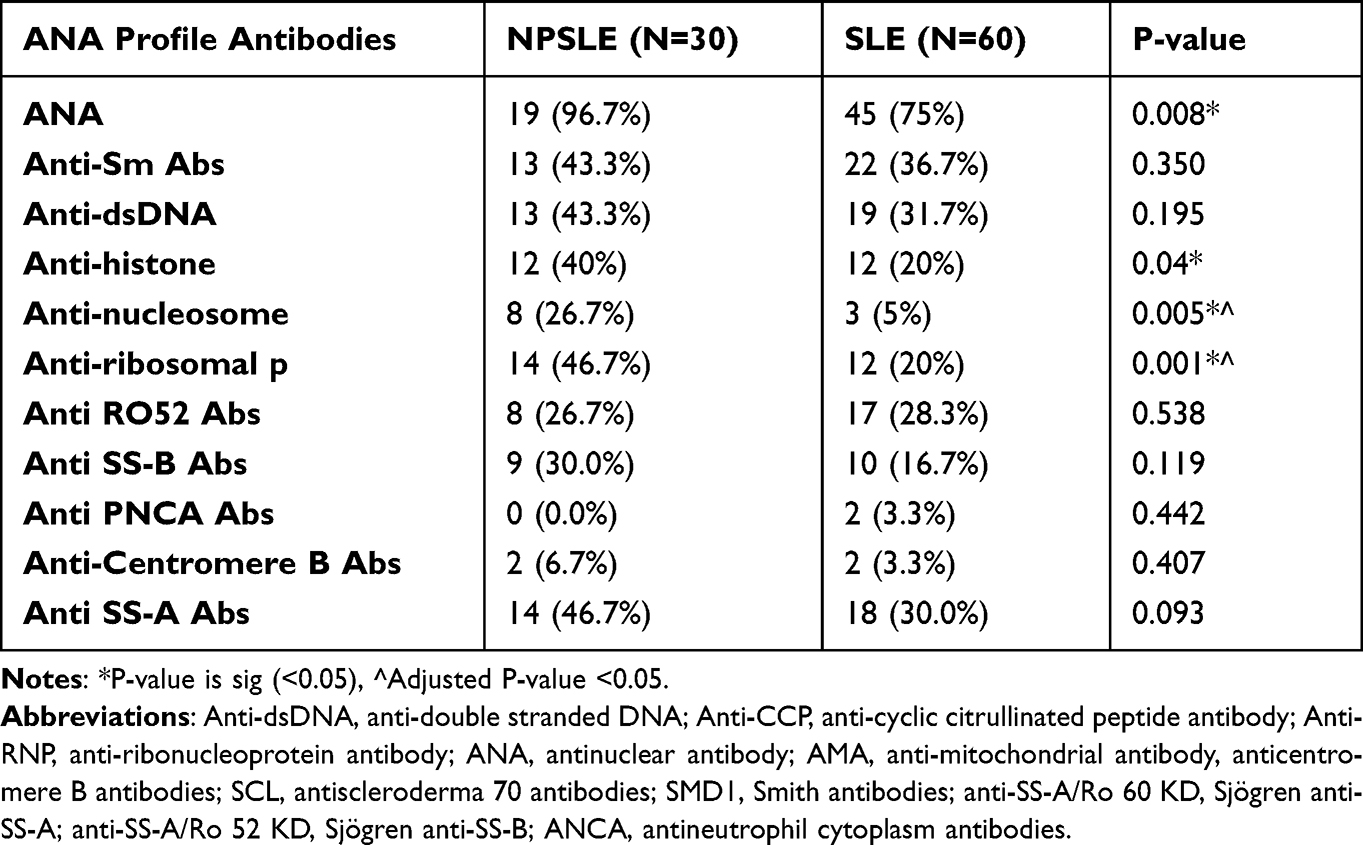 |
Table 4 The Other ANA Profile Antibodies among NPSLE and Non-NPSLE Groups |
ANA profile distribution regarding the neurological manifestations according to ACR criteria of NPSLE is shown in Table 5, in which ANA antibodies were significantly associated with neurological manifestations as ANA antibodies were common among epilepsy (n = 9; 91%) and stroke (n = 8; 27.6%) manifestations (P-value = 0.001). In addition, other antibodies in the ANA profile were not significantly differed between neurological manifestations (P-value >0.05).
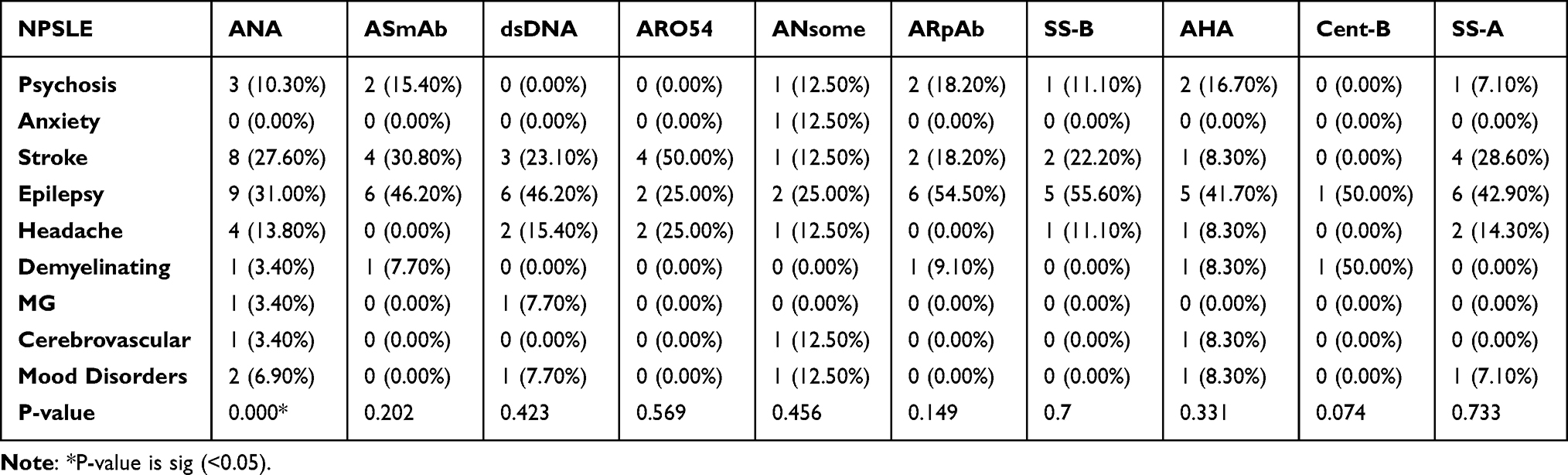 |
Table 5 Distribution of ANA Profile Regard to the Neuropsychiatric Manifestations According to ACR Criteria of NPSLE |
Discussion
Concomitant neuropsychiatric symptoms substantially impact the severity of SLE and the patient’s quality of life, and the prognosis is relatively poor. Neuropsychiatric systemic lupus erythematosus symptoms may range from mild diffuse ones to acute life-threatening events. While the chief mechanism behind NPSLE is still primarily unravelled, various hypotheses have been identified, for instance, neurotoxicity and vasculopathy caused by antibodies and cytokines.10 The current study is aimed to evaluate and correlate anti-ribosomal P antibodies among the Sudanese population demonstrating NPSLE manifestations.
The present study showed that all the patients with NPSLE were females (n = 30; 100), with a mean age of 36.6 ± 12.3 years. These findings are comparable to several previous studies; Mengdi et al found that 93% were females with a mean age of 33.11 Also, Wei et al reported females in 90% of NPSLE with a mean age of 35.2 ± 13.7.7 All these findings confirmed that NPSLE was common in young aged females.
In our study, 73.3% of the patients with NPSLE manifestations developed NP events as early as five years after SLE onset, similar to prior findings by Jönsen et al, Bertsias et al, and Bernatsky et al.12–14 This is presumably due to the insufficient control of the disease activity in the early stages of treatment. In our current study, 30 SLE patients demonstrated neuropsychiatric presentations, primarily epilepsy in 9 (30%) patients, stroke in 8 (26.7%) patients, and headache in 4 (13.3%) patients. Wei et al reported comparable outcomes, with epilepsy being the most common NP manifestation in 47% of NPSLE patients, followed by headache and psychosis.7 Similarly, Zhou et al illustrated that epilepsy was the most frequent presentation in NPSLE patients seen in 35%.15 Nevertheless, an Italian study by Antonella et al reported different manifestations in patients with NPSLE: cognitive impairment, mood disorders and stroke (52%, 27% and 24%), respectively.16 However, among the Sudanese NPSLE patients, epilepsy was the most frequent NP presentation.
Additionally, the current study demonstrated that patients with NPSLE significantly exhibited more severe cutaneous presentation (hair loss and oral ulceration), chest and cardiac presentations (breathing difficulty and rapid or irregular heartbeat), and central and peripheral nervous system-related clinical presentations, as well as psychiatric related clinical presentations. Nevertheless, on assessing adjusted P-value for clinical presentations, neurological symptoms were significantly (adjP-value <0.05) correlated with NPSLE. Although NPLSE diagnosis is not associated with a particular blood test, we observed that NPSLE patients tend to have anaemia, leucocytosis, thrombocytopenia, and hypoalbuminemia non-NPSLE patients (P < 0.05), with similar results reported by Maria et al.16
Our present study showed that ANA was more positive among NPSLE patients than non-NPSLE patients (96.7% vs 75%; P-value = 0.008). These results were in agreement with studies of Wei et al in China.7 Although anti-nucleosome antibodies are probably better for predicting flares in quiescent Lupus, we observed in this study that anti-nucleosome antibodies were present among the NPSLE more than in the non-NPSLE group (26.7% vs 5%; P-value = 0.005), and correspondingly adjP-value was <0.05. These findings were similar to Dina et al, which might be explained by the recognised significant direct relationship between lupus disease severity and the level of anti-nucleosome antibodies.17,18 Significantly, anti-histones antibodies were more positive among the NPSLE group than in the non-NPSLE group (40% vs 20%; P-value = 0.04). Likewise, Parodi et al reported that anti-histones antibodies correlated with Alzheimer’s, dementia and other neurological diseases.19 Also, Xiao‐Yun et al noticed that the anti‐histone antibodies are significantly present in approximately 50% of patients with NPSLE compared with SLE.20
Furthermore, excitingly anti-ribosomal-p antibodies were positive among patients with NPSLE than non-NPSLE patients (46.7% vs 20%; P-value = 0.001) in the current study, and significance level was further confirmed through adjP-value of <0.05. These results were consistent with several studies reporting a direct correlation between neuropsychiatric manifestations in SLE and anti-ribosomal-p antibodies.8,21,22
Regard to the antiphospholipid antibodies (APA) profile, anti-lupus antibodies (26.7% vs 1.7%; P-value = 0.001), anticoagulant antibodies (30% vs 3.3%; P-value = 0.001), and anticardiolipin antibodies (26.7% vs 0%; P-value = 0.000) were substantially noted in the NPSLE group than the non-NPSLE group. Comparably, Sciascia et al reported that antiphospholipid antibodies (Anti-Cardiolipin, Lupus anticoagulant, and anti-β2GP) were commonly seen in NPSLE patients.23 Furthermore, De Groot et al observed that concurrent prevalence of antiphospholipid syndrome (APS) and SLE is associated with a raised prothrombotic risk linked to anti-β2-glycoprotein presence.24 Additionally, some studies have pointed out that NPSLE is more prevalent among APS patients.25 Lastly, testing for APA in SLE patients is paramount since it is present in around 40% of these patients, and it has been linked with a raised likelihood of a future CNS manifestation.26
Conclusion
Neuropsychiatric manifestation of systemic lupus erythematosus exhibits variable clinical manifestations; epilepsy is the common neuropsychiatric manifestation. Anti-ribosomal P antibodies are strongly correlated to SLE neuropsychiatric manifestations; thus, it can be employed as a powerful diagnostic tool. In addition, anti-phospholipid, anti-histone, and anti-nucleosome antibodies are linked to a certain extent with neuropsychiatric manifestations. ANA antibodies were significantly associated with neurological manifestations, particularly epilepsy. Other antibodies in the ANA profile were not significantly differed between neurological manifestations.
Data Sharing Statement
The authors declare that all the data supporting the findings of this study are available within the article.
Acknowledgments
Omdurman Military Hospital medical staff and admission office.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Systemic Lupus FD. Erythematosus — basic, applied, and clinical aspects. J Rheumatol. 2016;43(11):2087. doi:10.3899/jrheum.160771
2. Johnson S. New ACR EULAR guidelines for systemic sclerosis classification. Curr Rheumatol Rep. 2015;17(5). doi:10.1007/s11926-015-0506-3
3. Cheng S, Ding H, Xue H, Cao L. Evaluation of the 2019 EULAR/ACR classification criteria for systemic lupus erythematosus in children and adults [published online ahead of print, 2022 Jul 19] [published correction appears in Clin Rheumatol. 2022 Aug 6]. Clin Rheumatol. 2022. doi:10.1007/s10067-022-06293-x
4. Albrecht J, Berlin JA, Braverman IM, et al. Dermatology position paper on the revision of the 1982 ACR criteria for systemic lupus erythematosus [published correction appears in Lupus. 2005;14(2):178. Connolly, MK [added]]. Lupus. 2004;13(11):839–849. doi:10.1191/0961203304lu2020oa
5. Petri M, Orbai AM, Alarcón GS, et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012;64(8):2677–2686. doi:10.1002/art.34473
6. Aringer M, Dörner T, Leuchten N, Johnson SR. Toward new criteria for systemic lupus erythematosus-a standpoint. Lupus. 2016;25(8):805–811. doi:10.1177/0961203316644338
7. Clinical FW. Manifestations of neuropsychiatric systemic lupus erythematosus in Chinese patients. Arch Rheumatol. 2014;29(2):88–93. doi:10.5606/archrheumatol.2014.4051
8. Bogdanovic G, Stojanovich L, Djokovic A, Stanisavljevic N. Physical activity program is helpful for improving quality of life in patients with systemic lupus erythematosus. Tohoku J Exp Med. 2015;237(3):193–199. doi:10.1620/tjem.237.193
9. Haddouk S, Marzouk S, Jallouli M, et al. Clinical and diagnostic value of ribosomal P autoantibodies in systemic lupus erythematosus. Rheumatology. 2009;48(8):953–957. doi:10.1093/rheumatology/kep142
10. Kivity S, Agmon-Levin N, Zandman-Goddard G, Chapman J, Shoenfeld Y. Neuropsychiatric lupus: a mosaic of clinical presentations. BMC Med. 2015;13:43. doi:10.1186/s12916-015-0269-8
11. Jiang M, Shi X, Gao X, et al. Clinical features of central nervous system infections and experience in differential diagnosis from neuropsychiatric lupus erythematosus in a cohort of 8491 patients with systemic lupus erythematosus. Arthritis Res Ther. 2019;21(1):189. doi:10.1186/s13075-019-1971-2
12. Jönsen A, Bengtsson AA, Nived O, Ryberg B, Sturfelt G. Outcome of neuropsychiatric systemic lupus erythematosus within a defined Swedish population: increased morbidity but low mortality. Rheumatology. 2002;41(11):1308–1312. doi:10.1093/rheumatology/41.11.1308
13. Bertsias GK, Ioannidis JP, Aringer M, et al. EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs. Ann Rheum Dis. 2010;69(12):2074–2082. doi:10.1136/ard.2010.130476
14. Bernatsky S, Clarke A, Gladman DD, et al. Mortality related to cerebrovascular disease in systemic lupus erythematosus. Lupus. 2006;15(12):835–839. doi:10.1177/0961203306073133
15. Zhou HQ, Zhang FC, Tian XP, et al. Clinical features and outcome of neuropsychiatric Lupus in Chinese: analysis of 240 hospitalised patients. Lupus. 2008;17(2):93–99. doi:10.1177/0961203307085671
16. Afeltra A, Garzia P, Mitterhofer A, et al. Neuropsychiatric lupus syndromes: relationship with antiphospholipid antibodies. Neurology. 2003;61(1):108–110. doi:10.1212/01.wnl.0000058904.94330.a7
17. Cozzani E, Drosera M, Gasparini G, Parodi A. Serology of Lupus Erythematosus: correlation between Immunopathological Features and Clinical Aspects. Autoimmune Dis. 2014;2014:321359. doi:10.1155/2014/321359
18. Doe K, Nozawa K, Hiruma K, et al. Antibody against chromatin assembly factor-1 is a novel autoantibody specifically recognised in systemic lupus erythematosus. Lupus. 2014;23(10):1031–1041. doi:10.1177/0961203314536245
19. Zardi EM, Taccone A, Marigliano B, Margiotta DP, Afeltra A. Neuropsychiatric systemic lupus erythematosus: tools for the diagnosis. Autoimmun Rev. 2014;13(8):831–839. doi:10.1016/j.autrev.2014.04.002
20. Sun XY, Shi J, Han L, Su Y, Li ZG. Anti-histones antibodies in systemic lupus erythematosus: prevalence and frequency in neuropsychiatric Lupus. J Clin Lab Anal. 2008;22(4):271–277. doi:10.1002/jcla.20248
21. Schroeder JO, Euler HH. Recognition and management of systemic lupus erythematosus. Drugs. 1997;54(3):422–434. doi:10.2165/00003495-199754030-00005
22. Tomietto P, D’Agostini S, Annese V, De Vita S, Ferraccioli G. Mycophenolate mofetil and intravenous dexamethasone in the treatment of persistent lupus myelitis. J Rheumatol. 2007;34(3):588–591.
23. McGlasson S, Wiseman S, Wardlaw J, Dhaun N, Hunt DPJ. Neurological disease in lupus: toward a personalised medicine approach. Front Immunol. 2018;9:1146. doi:10.3389/fimmu.2018.01146
24. De Groot PG, De Laat B. Mechanisms of thrombosis in systemic lupus erythematosus and antiphospholipid syndrome. Best Pract Res Clin Rheumatol. 2017;31(3):334–341. doi:10.1016/j.berh.2017.09.008
25. Pedroza Díaz N, Ortiz Reyes B, Vásquez Duque G. Biomarcadores proteicos en lupus neuropsiquiátrico. Revista Colombiana de Reumatología. 2012;19(3):158–171. doi:10.1016/s0121-8123(12)70023-3
26. González NL, Escobar M. Lupus eritematoso sistémico y embarazo. Revista Colombiana de Reumatología. 2011;18(3):175–186. doi:10.1016/s0121-8123(11)70052-4
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.