")
Back to Journals » Journal of Pain Research » Volume 13
Anterior Cervical Surgery for the Treatment of Cervicogenic Headache Caused by Cervical Spondylosis
Received 19 August 2020
Accepted for publication 29 September 2020
Published 2 November 2020 Volume 2020:13 Pages 2783—2789
DOI https://doi.org/10.2147/JPR.S275680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Robert B. Raffa
Xiaodong Pang, Chunyu Liu, Baogan Peng
Department of Spinal Surgery, The Third Medical Center of Chinese PLA General Hospital, Beijing 100039, People’s Republic of China
Correspondence: Baogan Peng
Department of Spinal Surgery, The Third Medical Center of Chinese PLA General Hospital, 69 Yongding Road, Beijing 100039, People’s Republic of China
Tel +86-10-57976611
Fax +86-10-57976937
Email [email protected]
Study Design: Retrospective study.
Objective: To report the efficacy of anterior cervical surgery for the relief of cervicogenic headache (CEH) caused by cervical spondylosis.
Methods: From January 2014 to December 2016, a total of 166 cases of cervical radiculopathy and/or myelopathy received anterior cervical decompression and fusion (ACDF) in our institution, among which 50 cases (mean age 44.7 years) were accompanied by CEH and followed up at 3, 6, 12, and 24 months postoperatively, respectively. Neck pain and headache scores according to neck disability index (NDI) were documented for all patients at regular intervals. The results measured at different follow-up time point were compared statistically.
Results: All 50 patients reported neck pain and headache at the same time before surgery. The average NDIs for neck pain before and after surgery were 2.86 (95% CI: 2.7– 3.0) preoperatively, 0.98 (95% CI: 0.8– 1.1) at 3 months, 0.68 (95% CI: 0.5– 0.9) at 6 months, 0.62 (95% CI: 0.5– 0.8) at 12 months, and 0.60 (95% CI: 0.4– 0.8) at 24 months postoperatively, respectively. The average NDIs for CEH before and after surgery were 2.32 (95% CI: 2.2– 2.5) preoperatively, 0.62 (95% CI: 0.5– 0.8) at 3 months, 0.60 (95% CI: 0.4– 0.8) at 6 months, 0.56 (95% CI: 0.4– 0.7) at 12 months, and 0.50 (95% CI: 0.3– 0.7) at 24 months postoperatively, respectively. The neck pain and headache improved in all cases and the NDI score of neck pain or headache at each follow-up point after surgery was significantly different from that before surgery (P < 0.001). The simple correlation analysis between neck pain and headache was performed, and the Pearson coefficient r was 0.71, indicating a positive correlation between neck pain NDI and headache NDI. No serious surgical complications were found.
Conclusion: Our study suggests that patients with cervical spondylosis complicated with CEH are always accompanied by neck pain. ACDF can not only relieve neck pain but also improve the accompanying CEH.
Keywords: cervicogenic headache, neck pain, cervical spondylosis, anterior cervical decompression and fusion
Introduction
In 1925, Barre1 introduced the term “syndrome cervical sympathique posterieur”, linking headache to the presumed cause of “posterior” sympathetic deficiency. Since then, there have been many reports that headaches may originate in the neck.2–9 Sjaastad first coined the term “cervicogenic headache (CEH)” in 1983 to describe headache referred from the neck.3 Various types of headaches are usually accompanied by neck pain. Neck pain and neck muscle tenderness are common and prominent symptoms of primary headaches (including migraine and tension-type headache).10 Although the incidence of neck pain in patients with primary headaches is quite high (68%), neck pain is usually found in cervicogenic headache, which is considered as a secondary headache disorder (secondary to neck disorders).11 Accordingly, in order to standardize the diagnosis and treatment of CEH, the International Headache Society (IHS) first formulated the criteria of CEH in 1988 and updated the latest criteria in 2013 (International Classification of Headache Disorders, ICHD-3 beta, Table 1).7 An estimated 1–4% of the general population experiences CEH.4–6
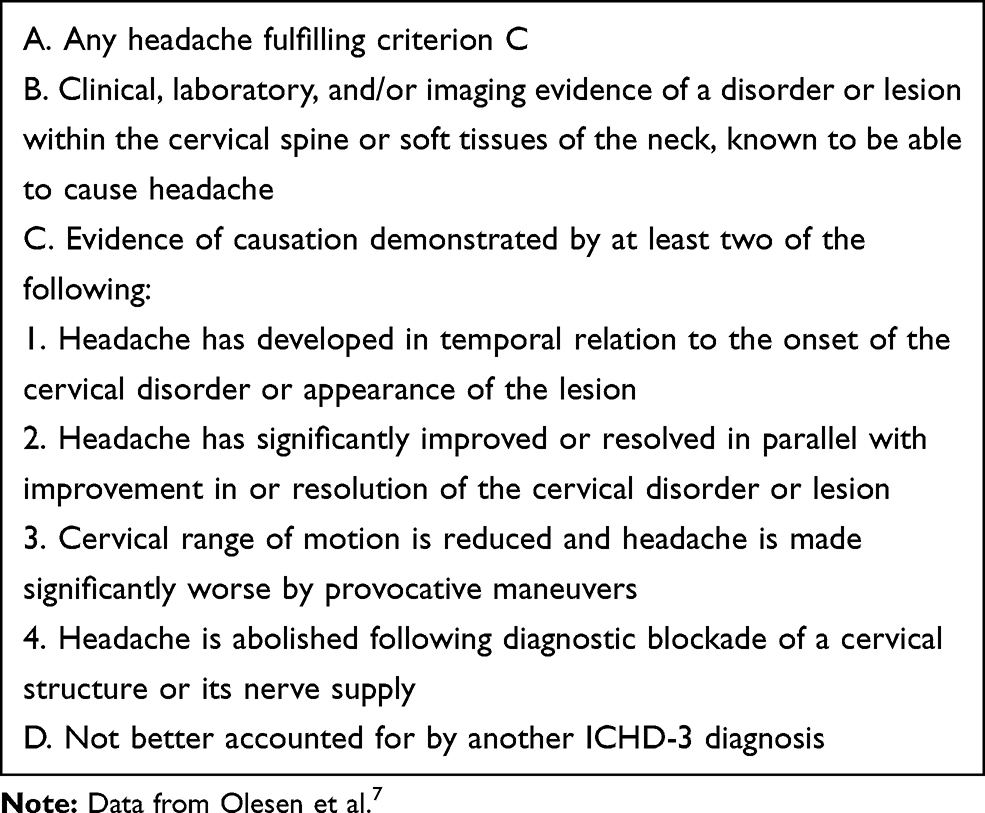 |
Table 1 Diagnostic Criteria of CEH (ICHD-3 Beta) |
The putative mechanism for cervicogenic headache involves the convergence of afferent sensory input from the upper cervical nerves (C1-C3) on the spinal trigeminal nucleus.4 However, it is well known that most of cervical spondylosis happens at lower cervical spine (C4-C7). Clinical studies have found that ACDF can not only relieve the clinical symptoms and signs about cervical spondylosis but also relieve accompanying headaches.8,9 CEH originating in the lower cervical spine was first described by Diener et al, who suggested that nociceptive afferents from the nerve roots of the lower cervical spine also converge on the cervical trigeminal nucleus.12 Persson et al13 analyzed headaches in patients with lower cervical radiculopathy and showed that selective nerve root blocks produced a headache reduction of 50% or more at the pathological level, with 69% of patients reporting complete headache relief. This study supports the theory that CEH can be relieved with lower cervical discectomy.
However, the exact mechanism by which anterior cervical surgery can relieve headache is unknown. As we all know, the most characteristic change of cervical spondylosis is cervical disc degeneration, and degenerative cervical disc disease is usually accompanied by neck pain. In this study, we retrospectively analyzed 2-year follow-up data from our clinical patients with cervical spondylosis and CEH to assess the incidence of CEH in patients with cervical spondylosis and the changes in postoperative neck pain and headache, so as to further analyze the relationship between neck pain and headache.
Methods
Patients
From January 2014 to December 2016, a total of 166 cases with cervical radiculopathy and/or myelopathy underwent ACDF in our institution. Of the 166 patients, 50 cases presented with CEH with an incidence of 30%. There were 26 males and 24 females. The age ranged from 23 to 72 years, with an average of 44.7 ± 12.5 years. The enrolled criteria included: 1) Except for the symptoms and signs of cervical myelopathy and/or radiculopathy, all patients with CEH are diagnosed according to the criteria of the International Classification of Headache Disorders (ICHD-3 beta).7 2) Significant compression of the cervical spinal cord or nerve roots showed on MRI. 3) Nonoperative treatment including non-steroid anti-inflammatory drugs, physiotherapy and trigger point injections failed for at least 6 months in all patients. The excluded criteria included: patients with a history of cervical trauma or surgery and patients with congenital or developmental abnormalities of the cervical spine. In addition, all patients were screened by neurologists, otolaryngologists, ophthalmologists or craniomaxillofacial surgeons to exclude the headaches related to each subject. Patients who had migraine or tension headaches at the same time were also excluded.
Surgical Techniques and Postoperative Management
The right-side dissection was performed in the anterior approach to the cervical spine. Subsequently, autologous bone particles (cervical posterior margin decompression) were filled in PEEK Cage using standard Smith-Robinson technique, and fixed with titanium plates and screws. Surgery ranged from C3-C4 to C6-C7. MRI was used to determine levels of spinal cord compression and involved nerve roots. Of the 50 patients who underwent ACDF, 35 underwent one segment operation, 10 underwent two segments operation, and 5 underwent three segments operation (Table 2). The patients usually wore neck collar for 1–3 months after surgery.
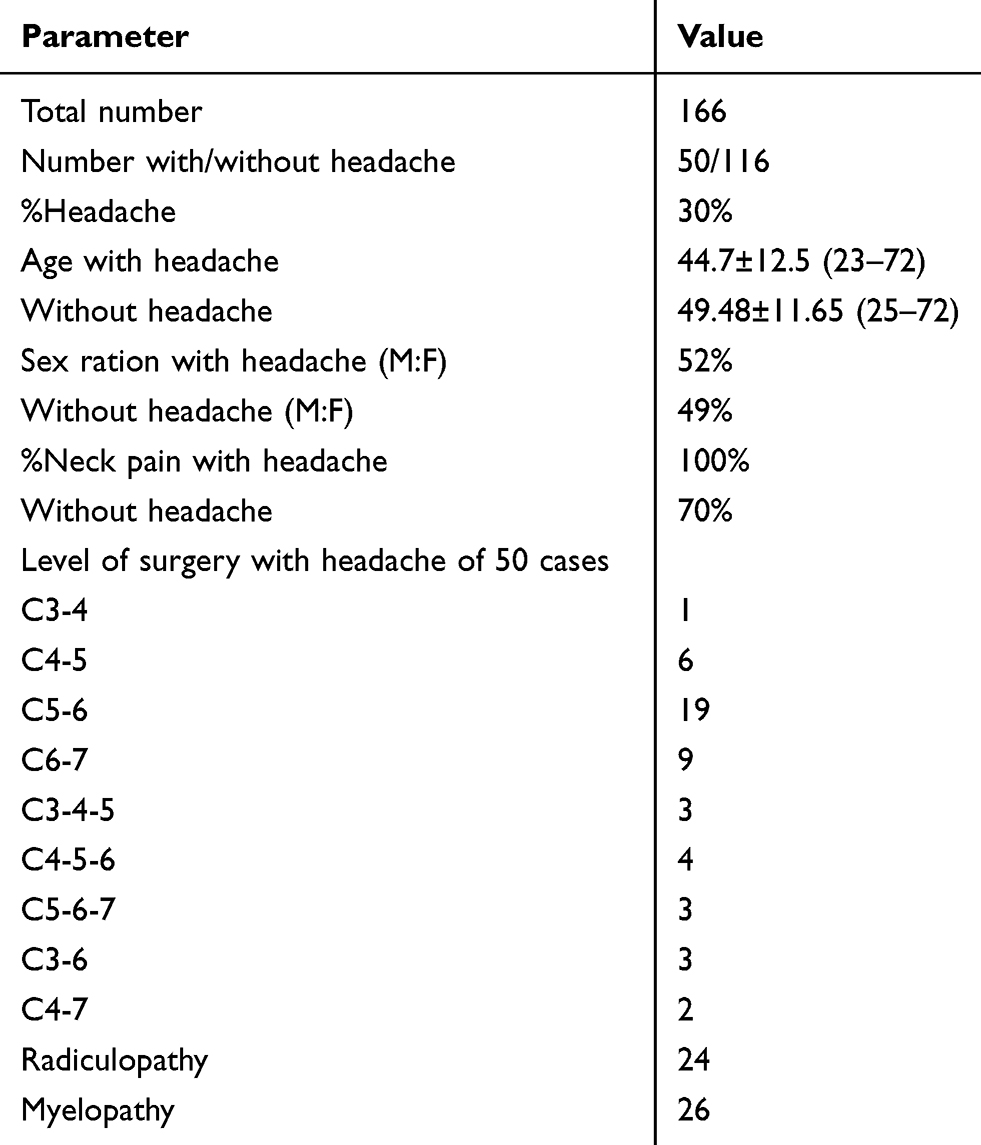 |
Table 2 Demographic Data of Patients |
Clinical Evaluation
Neck pain and headache were evaluated preoperatively and at 3, 6, 12 and 24 months after surgery, respectively. Severities of neck pain and headache were assessed with neck pain NDI and headache NDI.14,15 Originally, NDI was used widely as a tool to assess disability of cervical spine function due to neck pain. Now it was also used as an index to evaluate severity of headache. Severity is graded on a scale from 0 to 5: grade 0, no neck pain or headache; grade 1, infrequent slight neck pain or headache; grade 2, infrequent moderate neck pain or headache; grade 3, frequent moderate neck pain or headache; grade 4, frequent severe neck pain or headache; and grade 5, persistent extreme neck pain or headache.15
The study was approved by the ethical review committee from the General Hospital of Chinese Armed Police Forces and the study was in accordance with the Helsinki Declaration. All patients gave informed written consent.
Statistical Analysis
The statistical analysis was performed using Statistical Package for Social Sciences (SPSS) software, version 17.0 (IBM Corp., Armonk, NY). A repeated-measures analysis of variance was performed to compare neck pain or headache NDI at different follow-up time point. The simple correlation analysis between neck pain and headache was performed. Data are reported as mean (95% confidence interval). A p value of<0.05 was considered significant.
Results
The incidence of CEH in cervical spondylosis was 30% (50/166). The average NDIs for neck pain before and after surgery were 2.86 (95% CI: 2.7–3.0) preoperatively, 0.98 (95% CI: 0.8–1.1) at 3 months, 0.68 (95% CI: 0.5–0.9) at 6 months, 0.62 (95% CI: 0.5–0.8) at 12 months, and 0.60 (95% CI: 0.4–0.8) at 24 months postoperatively, respectively. The average NDIs for CEH before and after surgery were 2.32 (95% CI: 2.2–2.5) preoperatively, 0.62 (95% CI: 0.5–0.8) at 3 months, 0.60 (95% CI: 0.4–0.8) at 6 months, 0.56 (95% CI: 0.4–0.7) at 12 months, and 0.50 (95% CI: 0.3–0.7) at 24 months postoperatively, respectively. The neck pain and headache improved in all cases, and the NDI score of neck pain or headache at each follow-up point after surgery was significantly different from that before surgery (P <0.001) (Figures1–3). Pearson coefficient r was 0.71, which displayed that the neck pain NDI was positive correlation to the headache NDI.
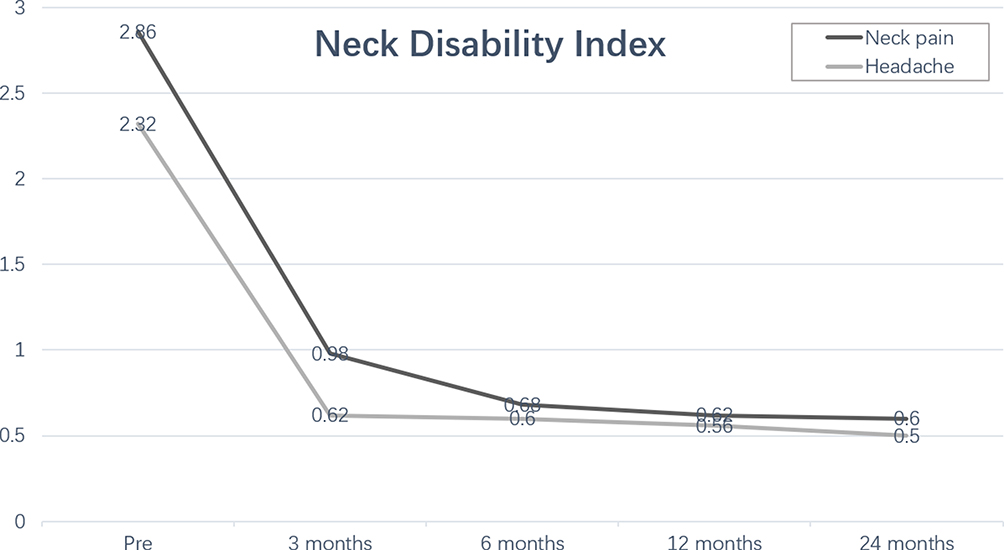 |
Figure 1 Preoperative and postoperative changes in neck pain and headache neck disability index scores. |
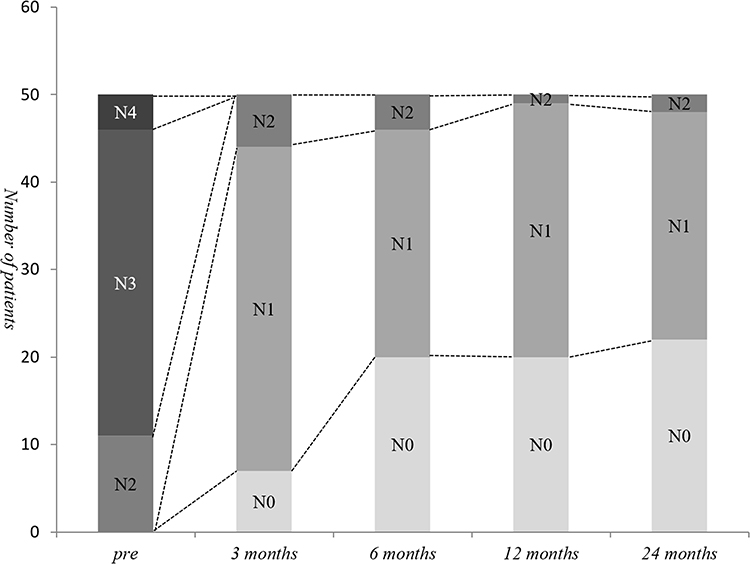 |
Figure 2 Detailed view of postoperative changes in neck pain neck disability index scores. N0–N5 indicated neck pain severity index graded on a scale from 0 to 5. Higher scores indicate greater degrees of self-related disability. |
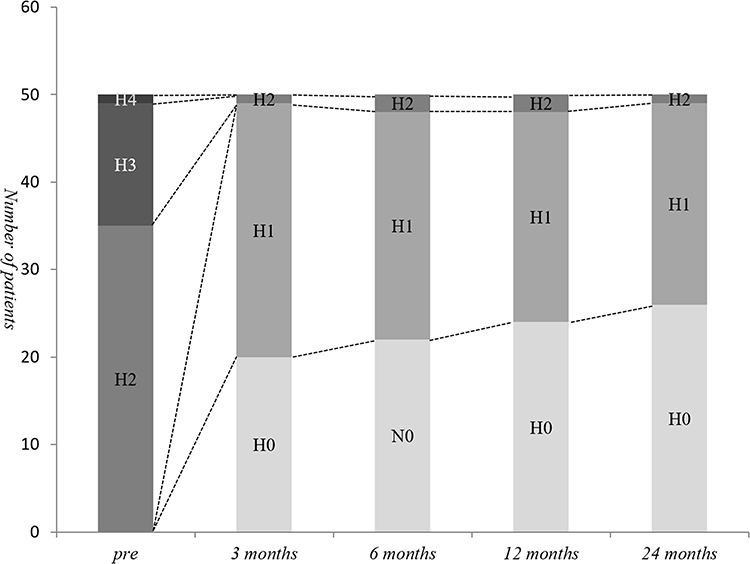 |
Figure 3 Detailed view of postoperative changes in headache neck disability index scores. H0–H5 indicated headache severity index graded on a scale from 0 to 5. Higher scores indicate greater degrees of self-related disability. |
Postoperative X-ray follow-up of the cervical spine showed that 47 cases had bone fusion within 6 months and 3 cases had bone fusion within 10 months.
Complications
Two patients had mild dysphagia, but the symptoms disappeared one month after operation. One patient developed subcutaneous hematoma due to drainage obstruction, which was cleared 2 days after operation. There were no surgical complications such as infection, implant looseness and falling out, and aggravation of neurological symptoms.
Discussion
CEH is a pain in the head, but the pain occurs in the neck.16,17 CEH was a controversial topic due to lack of recognition on its pathogenesis.18,19 Some studies have suggested that damage to any innervated structures around the neck such as facet joints, nerve roots, vertebral arteries, uncovertebral joints, cervical muscles, and intervertebral discs20–25 can cause CEH. The C2-3 zygapophysial joints were thought to be the most common source of cervicogenic headache, accounting for about 70% of cases. The greater and lesser occipital nerves, and the third occipital nerve, branches of C2 and C3 roots, were reported to be responsible for CEH as well.24
A special feature of this group of patients with CEH is also accompanied by neck pain. The purpose of our original study was to observe the efficacy of ACDF on CEH. We did not deliberately choose patients with neck pain. Our current study has found that ACDF can not only relieve neck pain in patients with cervical spondylosis but also relieve headaches which is consistent with previous studies.21,23,25,26 Further statistical analysis found that CEH score is positively related to neck pain score. This is an exciting new finding. According to our knowledge of the literature, this is the first report. The NDI is a reliable, effective and sensitive self-report measurement tool.27 Included in the NDI is the headache severity index, using an ordinal scale. This headache measurement was originally used by Riina et al,28 and later by Schrot et al,8 and Shimohata et al.15 Headaches are rated as none (0), mild (1 or 2), or severe (3, 4, or 5).28 Shimohata et al15 also compared VAS and NDI scores for headache in patients with cervical spondylosis, which were highly correlated. Mean headache scores were calculated throughout the 2-year follow-up period in our current study. Our study found that this headache scoring method in the patients was highly consistent with clinical efficacy after surgery.
According to the IHS definition for CEH in 2013,7 CEH is defined as any headache due to abnormalities in the cervical spine or its components (such as bone, disc and/or soft tissue), usually but not always accompanied by neck pain. This definition is slightly inconsistent with our current results. It is possible that previous studies misdiagnosed other headaches as CEH.
The pathophysiology of CEH is unknown, but it is thought to originate from the pathological changes of the upper cervical innervation (C1-C3). The three cervical nerves form the basis of referred pain from the upper neck to the head, including radiation to the frontal and periorbital areas. The trigeminocervical nucleus not only receives C1-C3 afferents but also receives the first branch of the trigeminal nerve sensory afferents, which indicates that it receives second-order neuronal afferents from the trigeminal nerve and the upper three cervical nerves. This mechanism does not explain why ACDF relieves headache at lower cervical spondylosis.4
It is well known that cervical spine is innervated richly by sympathetic nerve fibers. Yamada et al29 reported different sympathetic nerve distribution patterns in the cervical dura and posterior longitudinal ligament. Kiray et al30 and Saylam et al31 found that the cervical sympathetic trunk consists of a main trunk and 2–4 ganglia located in front of the transverse processes. Cervical sympathetic ganglia include upper ganglion, middle ganglion, lower ganglion and vertebral ganglion. Therefore, we hypothesized that compression of the dura mater and the posterior longitudinal ligament of the cervical spine might cause sympathetic reflex. This activity travels through the ganglia and sympathetic trunk to the cervical complex of the caudal nucleus of the trigeminal nerve and subsequently causes headache. For patients with cervical spondylosis without compression of dura mater and posterior longitudinal ligament, cervical disc degeneration may be an important factor causing neck pain, and its pathophysiology may be similar to that of lumbar discogenic pain. Fujimoto et al32 found that the C5-C6 disc at rat was innervated multi-segmentally from neurons of the C2-C8 dorsal root ganglions, stellate ganglion (sympathetic ganglion), and nodose ganglion (parasympathetic ganglion). This animal research may explain the wide-ranging and chronic discogenic neck pain that occurs via the somatosensory and autonomic nervous systems in human.
The results of this study may lead to the emergence of a new theory of “cervical discogenic headache”. Biomechanical data suggest that disc injury induce pain.26 Anterior cervical discectomy with fusion or with arthroplasty can improve discogenic headache.8 It is not clear whether the lower cervical roots also project into the trigeminal cervical complex. However, the improvement of cervicogenic headache after lower cervical disc surgery (C4-C7) has been specifically reported as unilateral or bilateral headaches.33,34 In particular, our current study found that ACDF can eliminate the neck pain associated with cervical spondylosis, but also eliminate headache. Previous studies have shown that cervical disc degeneration is an important source of neck pain.35–39 Therefore, we believe that inflammation caused by cervical disc degeneration stimulates pain receptors in cervical disc, leading to neck pain; compression due to herniated disc or osteophyte stimulates sympathetic nerves in dura mater and posterior longitudinal ligament, inducing sympathetic reflexes. These nociceptive and sympathetic nerve excitabilities are projected into the trigeminal cervical complex, resulting in CEH. Thus, we consider that ACDF can improve CEH likely through two mechanisms: removal of the degenerated cervical disc and the presence of nociceptors within it, thereby improving neck pain; Release the compression of the dura mater and posterior longitudinal ligament, thereby eliminating the sympathetic reflex.
Conclusion
Our study found that in patients with severe cervical spondylosis who require ACDF, the incidence of CEH is 30%. Cervical spondylosis patients with CEH are always accompanied by neck pain. ACDF can not only relieve neck pain but also improve the accompanying CEH.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Fredriksen TA, Hovdal H, Sjaastad O. “Cervicogenic headache”: clinical manifestation. Cephalalgia. 1987;7(2):147–160. doi:10.1046/j.1468-2982.1987.0702147.x
2. Antonaci F, Bono G, Mauri M, Drottning M, Buscone S. Concepts leading to the definition of the term cervicogenic headache: a historical overview. J Headache Pain. 2005;6(6):462–466. doi:10.1007/s10194-005-0250-6
3. Sjaastad O, Saunte C, Hovdahl H, Breivik H, Gronbak E. “Cervicogenic” headache. An hypothesis. Cephalalgia. 1983;3(4):249–256. doi:10.1046/j.1468-2982.1983.0304249.x
4. Bogduk N, Govind J. Cervicogenic headache: an assessment of the evidence on clinical diagnosis, invasive tests, and treatment. Lancet Neurol. 2009;8(10):959–968. doi:10.1016/S1474-4422(09)70209-1
5. Evers S. Comparison of cervicogenic headache with migraine. Cephalalgia. 2008;28(1 Suppl 1):16–17. doi:10.1111/j.1468-2982.2008.01609.x
6. Sjaastad O. Cervicogenic headache: comparison with migraine without aura; Vågå study. Cephalalgia. 2008;28(Suppl 1):18–20. doi:10.1111/j.1468-2982.2008.01610.x
7. Olesen J, Bes A, Kunkel R, et al. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia. 2013;33:629–808. doi:10.1177/0333102413485658
8. Schrot RJ, Mathew JS, Li Y, Beckett L, Bae HW, Kim KD. Headache relief after anterior cervical discectomy: post hoc analysis of a randomized investigational device exemption trial: clinical article. J Neurosurg Spine. 2014;21(2):217–222. doi:10.3171/2014.4.SPINE13669
9. Liu JJ, Cadena G, Panchal RR, Schrot RJ, Kim KD. Relief of cervicogenic headaches after single-level and multilevel anterior cervical diskectomy: a 5-year post hoc analysis. Global Spine J. 2016;6(6):563–570. doi:10.1055/s-0035-1570086
10. Biondi DM. Cervicogenic headache: a review of diagnostic and treatment strategies. JAOA. 2005;105(4 Suppl 2):S16–S22.
11. Blumenfeld A, Siavoshi S. The challenges of cervicogenic headache. Curr Pain Headache Rep. 2018;22(7):47. doi:10.1007/s11916-018-0699-z
12. Diener HC, Kaminski M, Stappert G, Stolke D, Schoch B. Lower cervical disc prolapse may cause cervicogenic headache: prospective study in patients undergoing surgery. Cephalalgia. 2007;27(9):1050–1054. doi:10.1111/j.1468-2982.2007.01385.x
13. Persson LC, Carlsson JY, Anderberg L. Headache in patients with cervical radiculopathy: a prospective study with selective nerve root blocks in 275 patients. Eur Spine J. 2007;16(7):953–959. doi:10.1007/s00586-006-0268-8
14. MacDermid JC, Walton DM, Avery S, et al. Measurement properties of the neck disability index: a systematic review. J Orthop Sports Phys Ther. 2009;39(5):400–417. doi:10.2519/jospt.2009.2930
15. Shimohata K, Hasegawa K, Onodera O, et al. The clinical features, risk factors, and surgical treatment of cervicogenic headache in patients with cervical spine disorders requiring surgery. Headache. 2017;57(7):1109–1117. doi:10.1111/head.13123
16. Chua NH, Wilder-Smith O, Vissers K. The neck: a pain generator for the head. Pain Manage. 2012;2(3):191–194. doi:10.2217/pmt.12.10
17. Becker WJ. Cervicogenic headache: evidence that the neck is a pain generator. Headache. 2010;50(4):699–705.
18. Leone M, D’Amico D, Grazzi L, Attanasio A, Bussone G. Cervicogenic headache: a critical review of the current diagnostic criteria. Pain. 1998;78(1):1–5. doi:10.1016/S0304-3959(98)00116-X
19. Haldeman S, Dagenais S. Cervicogenic headaches: a critical review. Spine J. 2001;1(1):31–46. doi:10.1016/S1529-9430(01)00024-9
20. Jull G, Barrett C, Magee R, Ho P. Further clinical clarification of the muscle dysfunction in cervical headache. Cephalalgia. 1999;19(3):179–185. doi:10.1046/j.1468-2982.1999.1903179.x
21. Geissler K, Guntinas-Lichius O. Differenzial diagnostik des Kopfschmerzes [Differential diagnosis of headaches]. Laryngorhinootologie. 2014;93(6):405–421.
22. Peled ZM, Pietramaggiori G, Scherer S. Anatomic and compression topography of the lesser occipital nerve. Plast Reconstr Surg Glob Open. 2016;4(3):e639. doi:10.1097/GOX.0000000000000654
23. Fredriksen TA, Fougner R, Tangerud A, Sjaastad O. Cervicogenic headache. Radiological investigations concerning head/neck. Cephalalgia. 1989;9(2):139–146.
24. Pöllmann W, Keidel M, Pfaffenrath V. Headache and the cervical spine: a critical review. Cephalalgia. 1997;17(8):801–816. doi:10.1046/j.1468-2982.1997.1708801.x
25. Freund BJ, Schwartz M. Treatment of chronic cervical-associated headache with botulinum toxin A: a pilot study. Headache. 2000;40(3):231–236. doi:10.1046/j.1526-4610.2000.00033.x
26. Jansen J. Surgical treatment of cervicogenic headache. Cephalalgia. 2008;28(Suppl. 1):41–44. doi:10.1111/j.1468-2982.2008.01620.x
27. Vernon H. The neck disability index: state-of-the-art, 1991-2008. J Manipulative Physiol Ther. 2008;31(7):491–502. doi:10.1016/j.jmpt.2008.08.006
28. Riina J, Anderson PA, Holly LT, et al. The effect of an anterior cervical operation for cervical radiculopathy or myelopathy on associated headaches. J Bone Joint Surg Am. 2009;91(8):1919–1923. doi:10.2106/JBJS.H.00500
29. Yamada H, Honda T, Yaginuma H, Kikuchi S, Sugiura Y. Comparison of sensory and sympathetic innervation of the dura mater and posterior longitudinal ligament in the cervical spine after removal of the stellate ganglion. J Comp Neurol. 2001;434(1):86–100. doi:10.1002/cne.1166
30. Kiray A, Arman C, Naderi S, Güvencer M, Korman E. Surgical anatomy of the cervical sympathetic trunk. Clin Anat. 2005;18(3):179–185. doi:10.1002/ca.20055
31. Saylam CY, Ozgiray E, Orhan M, Cagli S, Zileli M. Neuroanatomy of cervical sympathetic trunk: a cadaveric study. Clin Anat. 2009;22(3):324–330. doi:10.1002/ca.20764
32. Fujimoto K, Miyagi M, Ishikawa T, et al. Sensory and autonomic innervation of the cervical intervertebral disc in rats: the pathomechanics of chronic discogenic neck pain. Spine (Phila Pa 1976). 2012;37(16):1357–1362. doi:10.1097/BRS.0b013e31824ba710
33. Liu H, Ploumis A, Wang S, Li C, Li H. Treatment of cervicogenic headache concurrent with cervical stenosis by anterior cervical decompression and fusion. Clin Spine Surg. 2017;30(8):E1093–E1097. doi:10.1097/BSD.0000000000000291
34. Vincent MB. Cervicogenic headache: the neck is a generator: con. Headache. 2010;50(4):706–709. doi:10.1111/j.1526-4610.2010.01643.x
35. Peng B, DePalma MJ. The cervical disc degeneration and neck pain. J Pain Res. 2018;11:2853–2857. doi:10.2147/JPR.S180018
36. Risbud MV, Shapiro IM. Role of cytokines in intervertebral disc degeneration: pain and disc content. Nat Rev Rheumatol. 2014;10(1):44–56. doi:10.1038/nrrheum.2013.160
37. García-Cosamalón J, Del Valle ME, Calavia MG, et al. Intervertebral disc, sensory nerves and neurotrophins: who is who in discogenic pain? J Anat. 2010;217(1):1–15. doi:10.1111/j.1469-7580.2010.01227.x
38. Yang L, Chen J, Yang C, et al. Cervical intervertebral disc degeneration contributes to dizziness: a clinical and immunohistochemical study. World Neurosurg. 2018;119:e686–e93.
39. Wu B, Yang L, Peng B. Ingrowth of nociceptive receptors into diseased cervical intervertebral disc is associated with discogenic neck pain. Pain Med. 2019;20(6):1072–1077. doi:10.1093/pm/pnz013
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.