")
Back to Journals » Vascular Health and Risk Management » Volume 18
Angiotensin Receptor Blockers in the Management of Hypertension: A Real-World Perspective and Current Recommendations
Authors Gallo G, Volpe M , Rubattu S
Received 20 May 2022
Accepted for publication 7 July 2022
Published 11 July 2022 Volume 2022:18 Pages 507—515
DOI https://doi.org/10.2147/VHRM.S337640
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Giovanna Gallo,1 Massimo Volpe,1 Speranza Rubattu1,2
1Department of Clinical and Molecular Medicine, Sapienza University of Rome, Sant’Andrea Hospital, Rome, Italy; 2IRCCS Neuromed, Pozzilli, IS, Italy
Correspondence: Speranza Rubattu, Department of Clinical and Molecular Medicine, Sapienza University of Rome, Sant’Andrea Hospital, Rome, Italy, Tel +390633775979, Email [email protected]
Abstract: Hypertension represents a major common cardiovascular risk factor. Optimal control of high blood pressure levels is recommended to reduce the global burden of hypertensive-mediated organ damage and cardiovascular (CV) events. Among the first-line drugs recommended in international guidelines, renin-angiotensin-aldosterone system antagonists [angiotensin converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARBs)] have long represented a rational, effective, and safe anti-hypertensive pharmacological strategy. In fact, current US and European guidelines recommend ACEi and ARBs as a suitable first choice for hypertension treatment together with calcium channel blockers (CCBs) and thiazide diuretics. Different studies have demonstrated that ARBs and ACEi exert a comparable effect in lowering blood pressure levels. However, ARBs are characterized by better pharmacological tolerability. Most importantly, the clinical evidence supports a relevant protective role of ARBs toward the CV and renal damage development, as well as the occurrence of major adverse CV events, in hypertensive patients. Moreover, a neutral metabolic effect has been reported upon ARBs administration, in contrast to other antihypertensive agents, such as beta-blockers and diuretics. These properties highlight the use of ARBs as an excellent pharmacological strategy to manage hypertension and its dangerous consequences. The present review article summarizes the available evidence regarding the beneficial effects and current recommendations of ARBs in hypertension. The specific properties performed by these agents in various clinical subsets are discussed, also including an overview of their implications for the current COVID-19 pandemic.
Keywords: hypertension, renin-angiotensin-aldosterone system, ACEi, ARBs, HMOD, MACE
Introduction
Hypertension represents one of the most common and relevant cardiovascular (CV) risk factor (RF), accounting for more than 10 million deaths and 208 million Disability‐Adjusted Life Years.1
Indeed, subjects affected by hypertension have a significantly increased risk of major CV events (MACE). The relationship between blood pressure (BP) levels and vascular mortality shows a
remarkable continuous association, starting from a systolic BP (SBP) level of 115 mmHg and a diastolic BP (DBP) level of 75 mmHg for each decade of age.2,3
On the other hand, the benefits of antihypertensive treatment are well established. A 10 mmHg decrease in SBP reduces the risk of MACE by 20%, of coronary heart disease by 17%, of stroke by 27%, of heart failure (HF) by 28%, and of all‐cause mortality by 13%. These effects are independent of age, baseline BP levels, concomitant comorbidities, and previous CV disease (CVD).4
Moreover, an increasing body of evidence shows that a tighter control of BP can improve CV prevention. Therefore, the most recent European5 and US Guidelines6 recommend achieving a SBP target between 120 and 130 mmHg and a DBP target between 70 and 80 mmHg in the most hypertensive patients aged <65 years. This goal should be pursued by using combined pharmacological strategies of two or more medications with complementary activity, preferably contained in a single pill.
Due to the fundamental role of the renin-angiotensin-aldosterone system (RAAS) in the development and persistence of hypertension, angiotensin‐converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARBs) are recommended as a suitable first choice for initiation and maintenance of antihypertensive treatment, either as monotherapy or in combination.5–7
In this narrative review, we will discuss and summarize the available evidence on the benefits of the treatment with ARBs in the reduction of BP levels and in the development of hypertension mediated organ damage (HMOD) and MACE. We will also discuss their ancillary effects and pharmacological tolerability.
Efficacy of ARBs in Reducing BP Levels
Since the clinical development of ACEi in the Nineties, a large body of literature has shown that the blockade of the RAAS has a very favorable impact on morbidity and mortality in hypertension management.
ACEi and ARBs share common effects, though with significant differences in their mechanisms of action.8,9
ACEi inhibit the formation of angiotensin II and consequently the downstream effects through both the angiotensin II type 1 receptor (AT1R) and the angiotensin II type 2 receptor (AT2R). AT1R mediates detrimental effects, such as vasoconstriction, cell growth, sodium and water retention and sympathetic activation, whereas AT2R exerts vasodilation and antiproliferative effects.10,11 Moreover, the presence of non-ACE pathways, such as chymases, caspases and elastases, leads to a continued low-level production of angiotensin II in the CV system despite the inhibition of ACE.12 Finally, ACEi inhibit the breakdown of bradykinin, which releases nitric oxide and increases the synthesis of vasoactive prostaglandins, causing vasodilation.13
In contrast, ARBs specifically displace angiotensin II from the AT1R and increase the stimulation of AT2R. The class of ARBs includes several compounds that share similar effects, though presenting specific pharmacokinetic and pharmacodynamic characteristics and ancillary effects, such as the increased urinary uric acid excretion and the activation of peroxisome proliferator-activated receptor (PPAR)-γ.14 The latter effect has been described for telmisartan, irbesartan, candesartan and losartan and it may contribute to a favorable metabolic profile.
Candesartan, olmesartan, irbesartan, losartan, and valsartan have a common tetrazolo-biphenyl structure, candesartan and telmisartan have a common benzimidazole group, and eprosartan has a non-biphenyl, nontetrazole chemical structure.15 Apart from irbesartan, all active ARBs have a free carboxylic acid group. Eprosartan, irbesartan, telmisartan, and valsartan do not require metabolic activation. These structural characteristics contribute to the pharmacologic and pharmacokinetic differences among the members of the ARB class regarding oral bioavailability, rate of absorption, metabolism, rate, and route of elimination16 (Table 1).
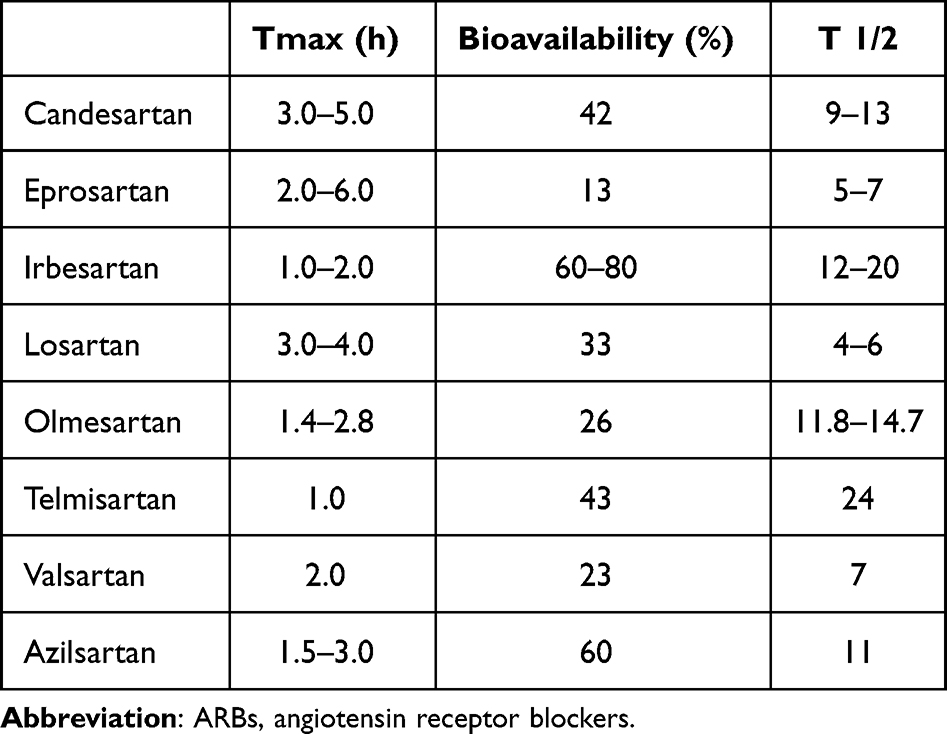 |
Table 1 Pharmacokinetic Properties of ARBs |
A large body of evidence has shown that ARBs have a comparable efficacy in reducing BP levels with respect to ACEi. However, some studies demonstrated a greater antihypertensive effect of ARBs. The treatment with azilsartan produced a 20.6 mmHg reduction of office SBP compared to 12.2 mmHg achieved with ramipril.17 Consistently, a greater reduction in central SBP was obtained with olmesartan compared to perindopril (13 mm Hg vs 10 mm Hg) when these drugs were used in combination with amlodipine in the SEVITENSION (Sevikar Compared to the Combination of Perindopril Plus Amlodipine on Central Arterial Blood Pressure in Patients With Moderate-to-Severe Hypertension) Study.18 A meta-analysis of 354 randomized trials showed that although a 10-mmHg decrease in office SBP was obtained with both ARBs and ACEi, these results were achieved with an ARB standard dose, whereas almost twice the standard ACEi dose was needed to achieve the same SBP decrease.19
In the ESPORT study (Efficacy and safety of olmesartan medoxomil and ramipril in elderly patients with mild-to-moderate essential hypertension) olmesartan produced a greater reduction of office SBP and DBP and of 24-hour average BP, particularly in the last 6 hours from the dosing interval compared to ramipril in a population of older hypertensives. BP normalization rate was also greater in patients treated with olmesartan.20
ARBs can be effectively combined with either diuretics, in particular thiazide-like diuretics, or dihydropyridine calcium-channel blockers (CCBs), in an attempt to enhance their ability to lower BP. These combinations show an excellent tolerability profile and a high adherence to the prescribed antihypertensive regimen. Compared to ARB-based monotherapies, the combination treatment based on ARBs and thiazides produced a greater reduction in both office SBP and DBP and in mean sitting BP values. Consistently, also mean daytime and mean 24-hr SBP and DBP were significantly lowered with the ARB/thiazide combination treatment compared to monotherapy.21–24 These results have also been confirmed in the elderly patients aged 65 years or older.
In addition, the ARB/CCB combination has the advantage of combining the optimal pharmacodynamic properties of the two pharmacological classes, thus providing a relevant antihypertensive efficacy and a satisfactory safety profile. Different trials demonstrated that the combination of ARB and CCB was significantly more effective than each single component of either monotherapy in reducing both seated SBP and DBP levels and 24-hr BP. Furthermore, combination therapies were well tolerated and associated with a lower incidence of oedema compared to the monotherapy with a full dose of CCB.25–27
In those patients with difficult-to-treat hypertension or in those with treated uncontrolled hypertension under dual therapy, triple combination therapies should be adopted to achieve the recommended BP treatment targets. In fact, they are associated with greater reductions in both SBP and DBP levels as compared with dual-combination therapies.28
In such a context, combination therapies with long-lasting ARBs may be preferred to favor adherence to treatment and to improve BP control.
The Role of ARBs in Preventing HMOD and MACE
Over the last twenty years, several randomized clinical trials have shown the beneficial role of ARBs in the prevention of HMOD and MACE, beyond their BP-lowering effect, revealing non-inferiority to ACEi and often superiority to other drug comparators (Table 2).
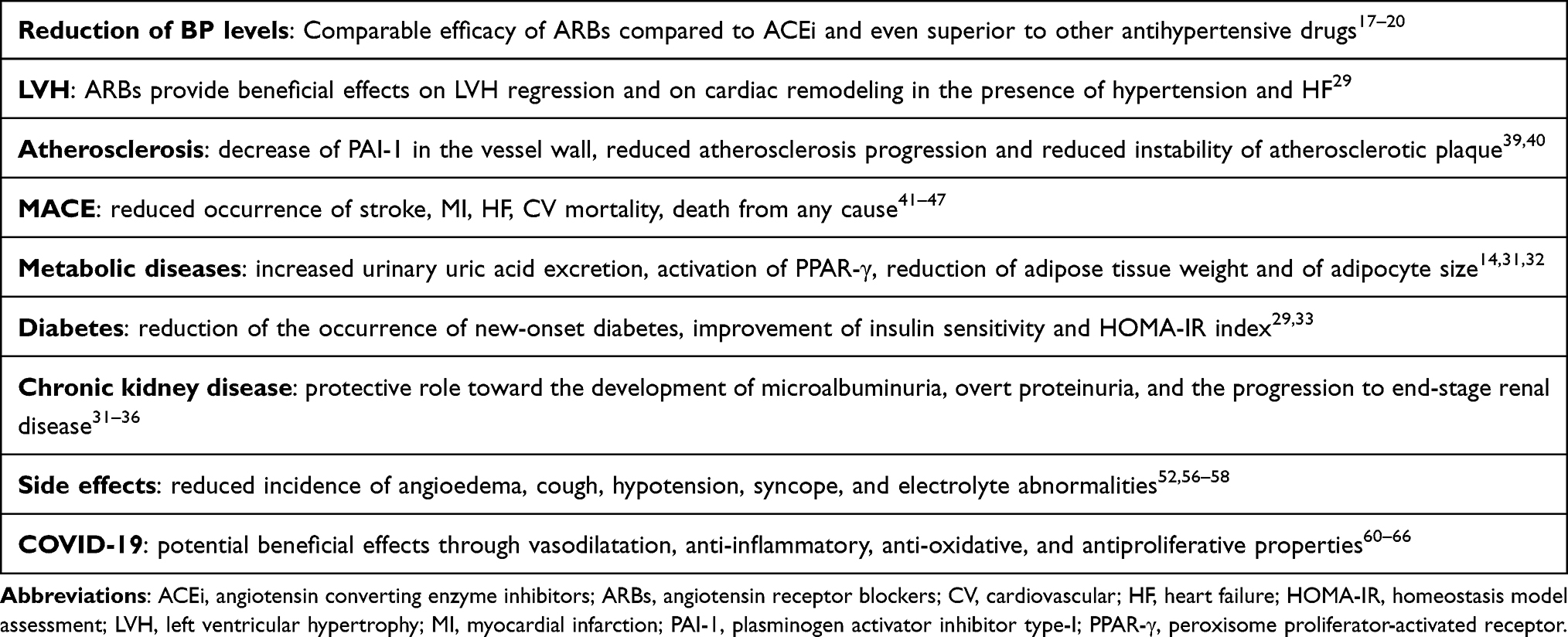 |
Table 2 Benefits of ARBs in Different Clinical Subsets |
The LIFE (Losartan Intervention For Endpoint Reduction) trial was the first study to demonstrate the superiority of the ARB losartan in reducing the degree of left ventricular hypertrophy compared to the beta-blocker atenolol in over 9000 patients with moderate-to-severe hypertension. The incidence of the primary composite endpoint of CV mortality, stroke and myocardial infarction (MI) was also lower in patients who received losartan. Moreover, losartan treatment was associated with a 25% lower incidence of new-onset diabetes.29
In the MOSES (MOrbidity and mortality after Stroke Eprosartan compared with nitrendipine for Secondary prevention) trial conducted in hypertensive patients with a history of a cerebral event within the previous 24 months, the ARB eprosartan showed superiority to the CCB nitrendipine for the secondary prevention of morbidity and mortality after stroke.30
Notably, ARBs reduce the occurrence of new-onset diabetes. Thus, they should be preferred in subjects with metabolic syndrome or other clinical conditions which may predispose to the incidence of this syndrome (5–7) (Table 2). Different studies have shown that ARBs are able to improve insulin sensitivity both in experimental models and in humans, suggesting a potential involvement of the excess of angiotensin II in the development of insulin resistance.
ARBs have also been shown to decrease the adipose tissue weight and the adipocyte size and to increase the adipose expression of PPAR-γ and of its target gene adiponectin, independently of their effects on BP and plasma insulin concentration.31 Moreover, both azilsartan and valsartan enhanced adipogenesis, induced the expression of adipokines, including leptin, adipsin, and adiponectin, and enhanced the expression of PPAR-α and -δ in cultured preadipocytes.32
In the animal model of obese Koletsky rats, treatment with azilsartan decreased hyperinsulinemia, improved the homeostasis model assessment (HOMA-IR) index, suppressed the over-increase in plasma glucose and insulin concentrations during the oral glucose tolerance test, and reduced the basal plasma concentrations of glucose, triglyceride, and non-esterified fatty acids.33
Several studies have demonstrated a protective role of ARBs toward the development of microalbuminuria or overt proteinuria, which represent relevant RF for chronic kidney disease development and for the progression to end-stage renal disease, particularly in diabetic patients (Table 2).
Although the exact mechanisms are unknown, the normalization of glomerular capillary pressure, the inhibition of podocyte injury, as well as of the proliferation of mesangial cells and of the epithelial–mesenchymal transition of tubular cells have been proposed.34
Olmesartan was associated with a delayed onset of microalbuminuria in the ROADMAP (Randomised Olmesartan And Diabetes Microalbuminuria Prevention) study.35
Irbesartan was shown to delay the progression from microalbuminuria to overt proteinuria and to restore normo-albuminuria in a significant proportion of patients with hypertension and type 2 diabetes. Moreover, irbesartan reduced the risk of advanced nephropathy in hypertensive patients with type 2 diabetes, independently of BP control.36
In the RENAAL (Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan),37 IDNT (Irbesartan Diabetic Nephropathy Trial)38 and IRMA (IRbesartan in patients with type 2 diabetes and Microalbuminuria)36 studies, the treatment with ARBs reduced the risk of chronic kidney disease compared to the conventional optimal therapy.
Losartan has been also associated to a reduction in serum uric acid levels compared with placebo in patients with type 2 diabetes and nephropathy.39
Of interest, ARBs reduced the expression of plasminogen activator inhibitor type-I (PAI-1) in the vessel wall, which is involved in the atherosclerosis progression, as well as in the instability of atherosclerotic plaque and in the process of fibrosis associated with negative left-ventricular remodeling40 (Table 2).
Indeed, studies performed in patients with hypertension, stable angina or type 2 diabetes mellitus, the long-term treatment with ARBs showed a reduction in the levels of markers of vascular inflammation [high-sensitive C-reactive protein (CRP), alpha tumor necrosis factor, interleukin-6, and macrophage chemotactic protein-1], a regression of the atheromatous plaque volume at the carotid and coronary arteries and a regression of vascular hypertrophy.41
In patients with high CV risk, ARBs have shown comparable protective effects with respect to ACEi.
The ONTARGET (Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial) study, which included 25,000 patients with coronary, peripheral or cerebrovascular disease and diabetes with end organ damage, demonstrated that telmisartan had similar effects compared to ramipril on the primary composite endpoint of CV death, MI, stroke or hospitalization for HF and death from any cause.42
In a large meta-analysis, conducted by Bangalore and colleagues on 37 randomized clinical trials including 147,020 participants, ARBs were not associated with an increase in the risk of MI, death, or angina pectoris. Compared with controls, ARBs were associated with a reduction in the risk of stroke, HF and new onset diabetes with similar results when compared with placebo or with active treatment.43
ARBs performed equally to ACEi in HF [ELITE and ELITE II—Evaluation of Losartan in the Elderly44,45 Val‐HefT—Valsartan Heart Failure Trial46 and CHARM—Candesartan in Heart failure Assessment of mortality and Morbidity]47, and following MI [OPTIMAAL—OPtimal Trial In Myocardial infarction with Angiotensin II Antagonist Losartan,48 VALIANT—VALsartan In Acute myocardial iNfarcTion].49 This evidence achieved with different compounds supports the beneficial impact on CV outcomes as a class effect of ARBs.
In addition, several meta-analyses have been performed to compare the effects of ARBs vs ACEi in terms of CV benefits. In a meta-analysis including 80 trials with 146 active treatment arms and 17 placebo arms, ARBs reduced the left ventricular mass by 13% and ACEi by 10%, although the difference was not statistically significant.50 Urinary protein excretion was similarly reduced by ACEi and ARBs in another meta-analysis of 17 randomized controlled trials including 17,951 patients.51
In a meta-analysis including 26 randomized trials of 100,000 high CV risk patients, Savarese et al showed that both ACEi and ARBs reduced the risk of the composite endpoints of MI, stroke, and CV mortality without significant difference.52
A Cochrane meta-analysis of 9 randomized trials with a prespecified follow-up period of at least one year including about 11,000 participants demonstrated no significant differences in total mortality, CV events and CV death between patients treated with ACEi or ARBs. In addition, ARBs were slightly more tolerable than ACEi with an absolute risk reduction for withdrawals due to adverse events.53
In the propensity score–adjusted REACH (Reduction of Atherothrombosis for Continued Health) cohort of 40,625 patients the incidence of the primary composite outcome of CV mortality, non-fatal MI, non-fatal stroke, or hospitalization for CV reasons was lower in patients taking ARBs compared to those receiving ACEi (29.2% vs 33.4%; adjusted hazard HR, 0.90; 95% CI, 0.86–0.95; p < 0.001) during the 4-year follow-up period.54 Similar results were observed for CV mortality (6.9% vs 8.2%; HR, 0.83; 95% CI, 0.75–0.93; p < 0.001) and all-cause mortality (11.6% vs 12.6%; HR: 0.89, 95% CI, 0.82–0.97; p = 0.005).54
Moreover, a meta-analysis of 106 randomized trials including 254,301 patients without HF showed that ARBs were as efficacious and safe as ACEi.55 Similarly, in a network meta-analysis of randomized trials of patients at high CV risk, ARBs and ACEI prevented the composite endpoint of CV death, MI, and stroke in a comparable manner.56
The recently published LEGEND-HTN (Large-scale Evidence Generation and Evaluation across a Network of Databases for Hypertension) study compared the real-world effectiveness and safety of ACEi (n = 2,297,881) and ARBs (n = 673,938) for the first-line treatment of hypertension across a global network of 8 large observational databases.57 Of these patients, over 123,000 patients on ACEi and 44,000 on ARBs had >500 days of follow-up. The 4 primary effectiveness outcomes consisted of acute MI, hospitalization for HF, ischemic or hemorrhagic stroke and a composite outcome which included the previous outcomes and sudden cardiac death. The study also analyzed safety outcomes or adverse effects including angioedema, cough, hypotension, syncope, and electrolyte abnormalities. No statistically significant differences were found between patients on ACEi and on ARBs regarding acute MI (hazard ratio [HR], 1.11; 95% confidence interval [CI], 0.95–1.32), HF (HR, 1.03; 95% CI, 0.87–1.24), stroke (HR, 1.07; 95% CI, 0.91–1.27) and the composite outcome of CV events (HR, 1.06; 95% CI, 0.90–1.25). Across secondary and safety outcomes, ACEi showed a significantly increased risk of acute pancreatitis (HR, 1.32; 95% CI, 1.04–1.70, P = 0.02), angioedema (HR, 3.31; 95% CI, 2.55–4.51, P < 0.01), cough (HR, 1.32, 95% CI, 1.11–1.59, P < 0.01), gastrointestinal bleed (HR, 1.18, 95% CI, 1.01–1.41, P = 0.04), and abnormal weight loss (HR, 1.18, 95% CI, 1.01–1.41, P = 0.04) as compared with ARBs. There was no statistically significant difference across any of the safety outcomes, including deterioration of renal function and electrolyte abnormalities.57
Other analyses have reported that ACEi have several-fold higher incidence of side effects at most
doses compared to ARBs (Table 2). In addition, the pooled estimate of withdrawal rates resulting from adverse events (WDAEs) for all doses was significantly lower with ARBs compared to ACEi.53
Thomopoulos et al found that, compared with placebo, ACEi and not ARBs significantly increased discontinuation rates for adverse events (RR, 2.78; 95% CI, 1.37 to 5.47).58
In other head-to-head comparisons, withdrawal rates with ARBs were 22% lower than with ACEi.
With regard to angioedema, which is a rare but sometimes life-threatening condition, the risk of developing it was two-fold lower in patients receiving ARBs when compared with those treated with ACEi.59
In the last few years, the risk of cancer from antihypertensive drugs has generated a large debate. A meta-analysis of 70 randomized controlled trials with 324,168 participants has shown no difference in the risk of cancer and cancer-related mortality with ARBs, ACEI, beta-blockers, CCBs and diuretics compared to placebo.60
It should be also underlined that medical costs are lower in patients treated with ARBs compared to those who receive ACEi ($2780 annually compared with $3163, respectively).61
ARBs and COVID-19
In the early phases of the COVID-19 pandemic, a concern was raised that RAAS inhibitors might increase the risk of infection, severe disease, or death due to their capacity to upregulate the expression of ACE2, which represents the binding site of SARS-CoV-2 as the gateway for entry into cells.62 Further studies, however, proposed that treatment with ACEi or ARBs might even reduce the risk of severe COVID-19 or death. Indeed, the ACE2 counteracts the ACE pathway by cleaving angiotensin-II to angiotensin-(1-7), thereby reducing angiotensin-II availability to the AT1R.63 Of interest, angiotensin-(1-7), through its MAS-receptor, plays vasodilatation, anti-inflammatory, anti-oxidative, and antiproliferative actions which may contribute to reduce the severity of COVID-19 disease and to improve prognosis64–68 (Table 2).
In the randomized BRACE-CORONA trial, 659 hospitalized patients with COVID-19 were assigned to continuation of ACEi/ARB treatment or temporary suspension of the therapy for 30 days. There were no significant differences between the two groups in the primary outcome of the number of days alive and out of hospital at 30 days.69 In a cohort of hospitalized COVID-19 patients the ARB telmisartan significantly reduced CRP levels and COVID-19 related outcomes, including intensive care unit admission, time to discharge and death, compared to usual care.70 The results of these studies provide further scientific evidence that earlier concerns about the use of RAAS-inhibitors in patients with COVID-19 were unwarranted and may even result in benefits.71
Of note, previous studies have shown that ACEi reduce the risk of pneumonia, including aspiration pneumonia in elderly patients with stroke.72–74
Conclusions
The available evidence supports the effectiveness of ARBs in reducing the incidence of HMOD and MACE in hypertensive patients, with a better safety profile compared to ACEi. Current US and European guidelines equally recommend ACEi and ARBs as first-line therapies both as monotherapies and in combination with other pharmacological classes (Table 2). Due to the more tolerable profile of ARBs, with a lower risk of withdrawals due to adverse events, these agents may be preferred to increase the percentage of treated hypertensive patients who achieve the recommended BP targets. Moreover, a large body of evidence supports the safety profile and even the protective role of the RAS blockers during COVID-19. As a result, international guidelines and expert consensus have repeatedly recommended to not discontinue the treatment with ACEi/ARBs in case of SARS-CoV-2 infection.
Acknowledgments
This work was supported by a grant from the Italian Ministry of Health, by a University Sapienza grant (project number RM1181641BF8C865), by Progetto PRIN 2017 (from the Italian Ministry of Instruction, University and Research, n. 2017PZY5K7).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Forouzanfar MH, Alexander L, Anderson HR, et al.; GBD 2013 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990‐2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2015;386(10010):
2. Ettehad D, Emdin CA, Kiran A, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387(10022):957–967. doi:10.1016/S0140-6736(15)01225-8
3. Rahimi K, Bidel Z, Nazarzadeh M, et al.; Blood Pressure Lowering Treatment Trialists’ Collaboration. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: an individual participant-level data meta-analysis. Lancet. 2021;397(10285):1625–1636. doi:10.1016/S0140-6736(21)00590-0.
4. Katsanos AH, Filippatou A, Manios E, et al. Blood pressure reduction and secondary stroke prevention: a systematic review and metaregression analysis of randomized clinical trials. Hypertension. 2017;69(1):
5. Williams B, Mancia G, Spiering W, et al. ESC scientific document group. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021–3104. doi:10.1093/eurheartj/ehy339
6. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/ AHA/ AAPA/ ABC/ ACPM/ AGS/ APhA/ ASH/ ASPC/ NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2018;71(19):e127–e248. doi:10.1016/j.jacc.2017.11.006
7. Volpe M, Gallo G, Battistoni A, Tocci G. Implications of guidelines for hypertension management in Europe. Circ Res. 2019;124(7):972–974. doi:10.1161/CIRCRESAHA.119.314724
8. Burnier M. Angiotensin II type 1 receptor blockers. Circulation. 2001;103:904–912. doi:10.1161/01.CIR.103.6.904
9. Burnier M, Vuignier Y, Wuerzner G. State-of-the-art treatment of hypertension: established and new drugs. Eur Heart J. 2014;35(9):557–562. doi:10.1093/eurheartj/eht465
10. Schmieder RE. Mechanisms for the clinical benefits of angiotensin II receptor blockers. Am J Hypertens. 2005;18(5 Pt 1):720–730. doi:10.1016/j.amjhyper.2004.11.032
11. Messerli FH, Bangalore S, Bavishi C, Rimoldi SF. Angiotensin-converting enzyme inhibitors in hypertension: to use or not to use? J Am Coll Cardiol. 2018;71(13):1474–1482. doi:10.1016/j.jacc.2018.01.058
12. Boehm M, Nabel EG. Angiotensin-converting enzyme 2 – a new cardiac regulator. N Engl J Med. 2002;347(22):1795–1797. doi:10.1056/NEJMcibr022472
13. Taddei S, Bortolotto L. Unraveling the pivotal role of bradykinin in ACE inhibitor activity. Am J Cardiovasc Drugs. 2016;16(5):309–321. doi:10.1007/s40256-016-0173-4
14. Iwai M, Chen R, Imura Y, Horiuchi M. TAK-536, a new AT1 receptor blocker, improves glucose intolerance and adipocyte differentiation. Am J Hypertens. 2007;20:579–586. doi:10.1016/j.amjhyper.2006.12.010
15. Oparil S. Newly emerging pharmacologic differences in angiotensin II receptor blockers. Am J Hypertens. 2000;13(1 Pt 2):18S–24S. doi:10.1016/S0895-7061(99)00250-2
16. Abraham HM, White CM, White WB. The comparative efficacy and safety of the angiotensin receptor blockers in the management of hypertension and other cardiovascular diseases. Drug Saf. 2015;38(1):33–54. doi:10.1007/s40264-014-0239-7
17. Gitt AK, Bramlage P, Potthoff SA, et al.; EARLY Registry Group. Azilsartan compared to ACE inhibitors in anti-hypertensive therapy: one-year outcomes of the observational EARLY registry. BMC Cardiovasc Disord. 2016;8(16):56. doi:10.1186/s12872-016-0222-6.
18. Ruilope L, Schaefer A. The fixed-dose combination of olmesartan/amlodipine was superior in central aortic blood pressure reduction compared with perindopril/amlodipine: a randomized, double-blind trial in patients with hypertension. Adv Ther. 2013;30(12):1086–1099. doi:10.1007/s12325-013-0076-6
19. Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials. BMJ. 2003;326(7404):1427. doi:10.1136/bmj.326.7404.1427
20. Malacco E, Omboni S, Volpe M, Auteri A, Zanchetti A; ESPORT Study Group. Antihypertensive efficacy and safety of olmesartan medoxomil and ramipril in elderly patients with mild to moderate essential hypertension: the ESPORT study. J Hypertens. 2010;28(11):2342–2350. doi:10.1097/HJH.0b013e32833e116b
21. Chrysant SG, Weber MA, Wang AC, Hinman DJ. Evaluation of antihypertensive therapy with the combination of olmesartan medoxomil and hydrochlorothiazide. Am J Hypertens. 2004;17(3):252–259. doi:10.1016/j.amjhyper.2003.11.003
22. Kereiakes DJ, Maa JF, Shojaee A, Dubiel R. Effect of an olmesartan medoxomil-based treatment algorithm on systolic blood pressure in patients with stage 1 or 2 hypertension: a randomized, double-blind, placebo-controlled study. Am J Cardiovasc Drugs. 2010;10(4):239–246. doi:10.2165/11538630-000000000-00000
23. Kereiakes DJ, Neutel J, Stoakes KA, et al. The effects of an olmesartan medoxomil-based treatment algorithm on 24-h blood pressure levels in elderly patients aged 65 and older. J Clin Hypertens. 2009;11(8):411–421. doi:10.1111/j.1751-7176.2009.00147.x
24. Sellin L, Stegbauer J, Laeis P, Rump LC. Adding hydrochlorothiazide to olmesartan dose dependently improves 24-h blood pressure and response rates in mild-to-moderate hypertension. J Hypertens. 2005;23(11):2083–2092. doi:10.1097/01.hjh.0000186022.74245.01
25. Punzi H, Neutel JM, Kereiakes DJ, et al. Efficacy of amlodipine and olmesartan medoxomil in patients with hypertension: the AZOR trial evaluating blood pressure reductions and control (AZTEC) study. Ther Adv Cardiovasc Dis. 2010;4(4):209–221.
26. Chrysant SG, Melino M, Karki S, Lee J, Heyrman R. The combination of olmesartan medoxomil and amlodipine besylate in controlling high blood pressure: COACH, a randomized, double blind, placebo-controlled, 8-week factorial efficacy and safety study. Clin Ther. 2008;30(4):587–604. doi:10.1016/j.clinthera.2008.04.002
27. Volpe M, Brommer P, Haag U, Miele C. Efficacy and tolerability of olmesartan medoxomil combined with amlodipine in patients with moderate to severe hypertension after amlodipine monotherapy: a randomized, double-blind, parallel-group, multicentre study. Clin Drug Investig. 2009;29(1):11–25. doi:10.2165/0044011-200929010-00002
28. Volpe M, Gallo G, Tocci G. New approach to blood pressure control: triple combination pill. Trends Cardiovasc Med. 2020;30(2):72–77. doi:10.1016/j.tcm.2019.03.002
29. Lindholm LH, Ibsen H, Dahlöf B, et al.; LIFE Study Group. Cardiovascular morbidity and mortality in patients with diabetes in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet. 2002;359(9311):1004–1010. doi:10.1016/S0140-6736(02)08090-X
30. Schrader J, Lüders S, Kulschewski A, et al.; MOSES Study Group. Morbidity and mortality after stroke, eprosartan compared with nitrendipine for secondary prevention: principal results of a prospective randomized controlled study (MOSES). Stroke. 2005;36(6):1218–1226. doi:10.1161/01.STR.0000166048.35740.a9.
31. Volpe M, Savoia C. New treatment options in the management of hypertension: appraising the potential role of azilsartan medoxomil. Integr Blood Press Control. 2012;5:19–25. doi:10.2147/IBPC.S13784
32. Kajiya T, Ho C, Wang J, Vilardi R, Kurtz W. Molecular and cellular effects of azilsartan: a new generation angiotensin II receptor blocker. J Hypertens. 2011;29:2476–2483. doi:10.1097/HJH.0b013e32834c46fd
33. Zhao M, Li Y, Wang J, et al. Azilsartan treatment improves insulin sensitivity in obese spontaneously hypertensive Koletsky rats. Diabetes Obes Metab. 2011;13(12):1123–1129. doi:10.1111/j.1463-1326.2011.01471.x
34. Kusumoto K, Igata H, Ojima M, et al. Antihypertensive, insulin sensitizing and renoprotective effects of a novel, potent and long-acting angiotensin II type 1 receptor blocker, azilsartan medoxomil, in rat and dog models. Eur J Pharmacol. 2011;669:84–93.
35. Haller H, Ito S, Izzo JL Jr, et al. ROADMAP Trial Investigators. Olmesartan for the delay or prevention of microalbuminuria in type 2 diabetes. N Engl J Med. 2011;364(10):907–917. doi:10.1056/NEJMoa1007994
36. Parving HH, Lehnert H, Bröchner-Mortensen J, Gomis R, Andersen S, Arner P; Irbesartan in patients with type 2 diabetes and microalbuminuria study group. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med. 2001;345(12):870–878. doi:10.1056/NEJMoa011489
37. Brenner BM, Cooper ME, de Zeeuw D, et al.; RENAAL Study Investigators. The losartan renal protection study–rationale, study design and baseline characteristics of RENAAL (reduction of endpoints in NIDDM with the angiotensin II antagonist losartan). J Renin Angiotensin Aldosterone Syst. 2000;1(4):328–335. doi:10.3317/jraas.2000.062.
38. Lewis EJ, Hunsicker LG, Clarke WR, et al.; Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345(12):851–860. doi:10.1056/NEJMoa011303.
39. Miao Y, Ottenbros SA, Laverman GD, et al. Effect of a reduction in uric acid on renal outcomes during losartan treatment: a post hoc analysis of the reduction of endpoints in non-insulin-dependent diabetes mellitus with the angiotensin II antagonist losartan trial. Hypertension. 2011;58(1):2–7. doi:10.1161/HYPERTENSIONAHA.111.171488
40. Koh KK, Chung WJ, Ahn JY, et al. Angiotensin II type 1 receptor blockers reduce tissue factor activity and plasminogen activator inhibitor type-1 antigen in hypertensive patients: a randomized, double-blind, placebo-controlled study. Atherosclerosis. 2004;177(1):155–160. doi:10.1016/j.atherosclerosis.2004.07.008
41. Bryniarski P, Nazimek K, Marcinkiewicz J. Immunomodulatory activity of the most commonly used antihypertensive drugs-angiotensin converting enzyme inhibitors and angiotensin ii receptor blockers. Int J Mol Sci. 2022;23(3):1772. doi:10.3390/ijms23031772
42. Verdecchia P, Sleight P, Mancia G, et al.; ONTARGET/TRANSCEND Investigators. Effects of telmisartan, ramipril, and their combination on left ventricular hypertrophy in individuals at high vascular risk in the ongoing telmisartan alone and in combination with ramipril global end point trial and the telmisartan randomized assessment study in ACE intolerant subjects with cardiovascular disease. Circulation. 2009;120(14):1380–1389. doi:10.1161/CIRCULATIONAHA.109.865774.
43. Bangalore S, Kumar S, Wetterslev J, Messerli FH. Angiotensin receptor blockers and risk of myocardial infarction: meta-analyses and trial sequential analyses of 147 020 patients from randomised trials. BMJ. 2011;342:d2234. doi:10.1136/bmj.d2234
44. Pitt B, Segal R, Martinez FA, et al. Randomised trial of losartan versus captopril in patients over 65 with heart failure (evaluation of losartan in the elderly study, ELITE). Lancet. 1997;349(9054):747–752. doi:10.1016/S0140-6736(97)01187-2
45. Pitt S, Poole-Wilson PA, Segal R, et al. Randomised trial of losartan versus captopril on mortality in patients with symptomatic heart failure: the losartan heart failure survival study – ELITE II. Lancet. 2000;355:1582–1587. doi:10.1016/S0140-6736(00)02213-3
46. Cohn JN, Tognoni G, Glazer RD, Spormann D, Hester A. Rationale and design of the valsartan heart failure trial: a large multinational trial to assess the effects of valsartan, an angiotensin-receptor blocker, on morbidity and mortality in chronic congestive heart failure. J Card Fail. 1999;5(2):155–160. doi:10.1016/S1071-9164(99)90038-6
47. Young JB, Dunlap ME, Pfeffer MA, et al.; Candesartan in heart failure assessment of reduction in mortality and morbidity (CHARM) investigators and committees. Mortality and morbidity reduction with Candesartan in patients with chronic heart failure and left ventricular systolic dysfunction: results of the CHARM low-left ventricular ejection fraction trials. Circulation. 2004;110(17):2618–2626. doi:10.1161/01.CIR.0000146819.43235.A9
48. Dickstein K, Kjekshus J; OPTIMAAL Steering, Committee of the OPTIMAAL study group. Effects of losartan and captopril on mortality and morbidity in high-risk patients after acute myocardial infarction: the OPTIMAAL randomised trial. Optimal trial in myocardial infarction with angiotensin ii antagonist losartan. Lancet. 2002;360(9335):752–760. doi:10.1016/s0140-6736(02)09895-1
49. Pfeffer MA, McMurray JJ, Velazquez EJ, et al.; Valsartan in Acute Myocardial Infarction Trial Investigators. Valsartan, captopril, or both in myocardial infarction complicated by heart failure, left ventricular dysfunction, or both. N Engl J Med. 2003;349(20):1893–1906. doi:10.1056/NEJMoa032292.
50. Klingbeil AU, Schneider M, Martus P, Messerli FH, Schmieder RE. A meta-analysis of the effects of treatment on left ventricular mass in essential hypertension. Am J Med. 2003;115(1):41–46. doi:10.1016/S0002-9343(03)00158-X
51. Xu R, Sun S, Huo Y, et al. Effects of ACEIs versus ARBs on proteinuria or albuminuria in primary hypertension: a meta-analysis of randomized trials. Medicine. 2015;94(39):e1560. doi:10.1097/MD.0000000000001560
52. Savarese G, Costanzo P, Cleland JG, et al. A meta-analysis reporting effects of angiotensin-converting enzyme inhibitors and angiotensin receptor blockers in patients without heart failure. J Am Coll Cardiol. 2013;61:131–142. doi:10.1016/j.jacc.2012.10.011
53. Li EC, Heran BS, Wright JM. Angiotensin converting enzyme (ACE) inhibitors versus angiotensin receptor blockers for primary hypertension. Cochrane Database Syst Rev. 2014;2014(8):CD009096.
54. Potier L, Roussel R, Elbez Y, et al.; REACH Registry Investigators*. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers in high vascular risk. Heart. 2017;103(17):1339–1346. doi:10.1136/heartjnl-2016-310705.
55. Bangalore S, Fakheri R, Toklu B, Ogedegbe G, Weintraub H, Messerli FH. Angiotensin-converting enzyme inhibitors or angiotensin receptor blockers in patients without heart failure? Insights from 254,301 patients from randomized trials. Mayo Clin Proc. 2016;91(1):51–60. doi:10.1016/j.mayocp.2015.10.019
56. Ricci F, Di Castelnuovo A, Savarese G, Perrone Filardi P, De Caterina R. ACE-inhibitors versus angiotensin receptor blockers for prevention of events in cardiovascular patients without heart failure - A network meta-analysis. Int J Cardiol. 2016;15(217):128–134. doi:10.1016/j.ijcard.2016.04.132
57. Chen R, Suchard MA, Krumholz HM, et al. Comparative first-line effectiveness and safety of ACE (angiotensin-converting enzyme) inhibitors and angiotensin receptor blockers: a multinational cohort study. Hypertension. 2021;78(3):591–603. doi:10.1161/HYPERTENSIONAHA.120.16667
58. Thomopoulos C, Parati G, Zanchetti A. Effects of blood-pressure-lowering treatment in hypertension: discontinuations for adverse events attributed to different classes of antihypertensive drugs: meta-analyses of randomized trials. J Hypertens. 2016;34:1921–1932. doi:10.1097/HJH.0000000000001052
59. Toh S, Reichman ME, Houstoun M, et al. Comparative risk for angioedema associated with the use of drugs that target the renin-angiotensin-aldosterone system. Arch Intern Med. 2012;172(20):1582–1589. doi:10.1001/2013.jamainternmed.34
60. Bangalore S, Kumar S, Kjeldsen SE, et al. Antihypertensive drugs and risk of cancer: network meta-analyses and trial sequential analyses of 324,168 participants from randomised trials. Lancet Oncol. 2011;12(1):65–82. doi:10.1016/S1470-2045(10)70260-6
61. Angiotensin receptor blockers: impact on costs of care. Am J Manag Care. 2005;11(13 Suppl):S400–S403.
62. Hofmann M, Kleine-Weber H, Schroeder S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181:
63. Savoia C, Arrabito E, Parente R, et al. Mas receptor activation contributes to the improvement of nitric oxide bioavailability and vascular remodeling during chronic AT1R (angiotensin type-1 receptor) blockade in experimental hypertension. Hypertension. 2020;76:1753–1761. doi:10.1161/HYPERTENSIONAHA.120.15527
64. Gallo G, Calvez V, Savoia C. Hypertension and COVID-19: current evidence and perspectives. High Blood Press Cardiovasc Prev. 2022;29(2):115–123. doi:10.1007/s40292-022-00506-9
65. Sattar Y, Mukuntharaj P, Zghouzi M, et al. Safety and efficacy of renin-angiotensin-aldosterone system inhibitors in COVID-19 population. High Blood Press Cardiovasc Prev. 2021;28(4):405–416. doi:10.1007/s40292-021-00462-w
66. Mancusi C, Grassi G, Borghi C, et al.; SARS-RAS Investigator Group. Clinical characteristics and outcomes of patients with COVID-19 infection: the results of the SARS-RAS study of the Italian society of hypertension. High Blood Press Cardiovasc Prev. 2021;28(1):5–11. doi:10.1007/s40292-020-00429-3.
67. Rubattu S, Gallo G, Volpe M. A contemporary view of natriuretic peptides in the SARS-CoV-2 era. Front Physiol. 2021;16(12):643721. doi:10.3389/fphys.2021.643721
68. Rubattu S, Gallo G, Volpe M. Sacubitril/valsartan: potential impact of ARNi “Beyond the Wall” of ACE2 on treatment and prognosis of heart failure patients with coronavirus disease-19. Front Cardiovasc Med. 2020;27(7):616564. doi:10.3389/fcvm.2020.616564
69. Lopes RD, Macedo AVS, de Barros E Silva PGM, et al.; BRACE CORONA Investigators. Effect of discontinuing vs continuing angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on days alive and out of the hospital in patients admitted with COVID-19: a randomized clinical trial. JAMA. 2021;325(3):254–264. doi:10.1001/jama.2020.25864.
70. Duarte M, Pelorosso F, Nicolosi LN, et al. Telmisartan for treatment of Covid-19 patients: an open multicenter randomized clinical trial. EClinicalMedicine. 2021;37:100962. doi:10.1016/j.eclinm.2021.100962
71. The Task Force for the management of COVID-19 of the European Society of Cardiology. ESC guidance for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic: part 2—care pathways, treatment, and follow-up. Eur Heart J. 2021. doi:10.1093/eurheartj/ehab697
72. Arai T, Yasuda Y, Takaya T, et al. Angiotensin-converting enzyme inhibitors, angiotensin-II receptor antagonists, and pneumonia in elderly hypertensive patients with stroke. Chest. 2001;119:660–661. doi:10.1378/chest.119.2.660
73. Harada J, Sekizawa K. Angiotensin-converting enzyme inhibitors and pneumonia in elderly patients with intracerebral hemorrhage. J Am Geriatr Soc. 2006;54:175–176. doi:10.1111/j.1532-5415.2005.00575_8.x
74. Liu CL, Shau WY, Wu CS, Lai MS. Angiotensin-converting enzyme inhibitor/angiotensin II receptor blockers and pneumonia risk among stroke patients. J Hypertens. 2012;30:2223–2229. doi:10.1097/HJH.0b013e328357a87a
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.