")
Back to Journals » Local and Regional Anesthesia » Volume 12
Anesthetic techniques: focus on transversus abdominis plane (TAP) blocks
Authors Mallan D, Sharan S, Saxena S , Singh TK, Faisal
Received 23 October 2018
Accepted for publication 12 April 2019
Published 5 September 2019 Volume 2019:12 Pages 81—88
DOI https://doi.org/10.2147/LRA.S138537
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Stefan Wirz

Deepanshu Mallan,1 Sandeep Sharan,2 Sumi Saxena,3 Tapas Kumar Singh,2 Faisal2
1Department of Anaesthesiology and Critical Care, Saraswati Medical College, Lucknow, India; 2Department of Anaesthesiology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, Uttar Pradesh, India; 3Department of Anaesthesiology and Critical Care, TSM Medical College, Lucknow, Uttar Pradesh, India
Correspondence: Tapas Kumar Singh
Department of Anaesthesiology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, Uttar Pradesh 226014, India
Email [email protected]
Abstract: Transverse abdominis plane (TAP) blocks, over the past decade, have emerged as a reliable tool in multimodal analgesia. Although they block only the somatic component of pain, studies have still revealed a consistent benefit in the first 24–48 hours after surgery in terms of pain scores and overall opioid consumption. The safety and dependability has increased with ultrasound usage. The aim of this review is to help the reader appreciate the applied anatomy required for a TAP block and its congeners, to standardize its nomenclature, and to help choose between variants of a TAP block and its complications and safety profile.
Keywords: tap block, ultrasound, regional anesthesia, truncal block
Introduction
Transversus abdominis plane (TAP) block has emerged as a reliable technique of postoperative multimodal analgesia over the past decade. Since its introduction by Rafi1 in 2001, due to increased usage of ultrasound and enhanced understanding of anatomy, the TAP block has evolved into various sub-blocks which target various dermatomes of the abdomen. The aim of this review is to help the reader appreciate the applied anatomy required for a TAP block and its congeners, to standardize its nomenclature, and to help choose between variants of TAP block and its complications and safety profile.
Applied anatomy
The key to abdominal surgery analgesia is understanding the dermatomes of the anterolateral) abdominal wall supplied by various spinal nerves and recognizing fascial planes of abdominal muscles within which these nerves lie after originating from transverse foramina of the vertebral column.2
Nerve supply
The skin and muscles of the abdominal wall are supplied by spinal nerves originating from T6 to L1 level. A typical spinal nerve originates and divides into anterior and posterior divisions, called anterior and primary rami. The anterior rami supplies the muscles and skin of the anterolateral abdominal wall. The spinal nerves can be clubbed into:
- Thoracoabdominal nerves: These are anterior rami of the spinal nerves of T6–T11.2 They divide into lateral and anterior cutaneous branches. Lateral cutaneous branches arise in the neurovascular plane between the internal oblique and transversus abdominis muscle, near the angle of the rib, and supply the skin after piercing the external oblique and internal oblique muscle. The anterior cutaneous branch arises similarly at the lateral border of the rectus sheath and it pierces the rectus abdominis muscle before supplying the skin. They supply the muscles and skin of the upper anterolateral abdominal wall, between the umbilicus and coastal margin.
- Subcostal nerve: This is the anterior rami of the T12 spinal nerve, which follows the course similar to thoracoabdominal nerves and terminates in similar lateral and cutaneous branches. It innervates muscles and skin of the lower anterolateral abdominal wall, between the umbilicus and inguinal ligament.
- Ilio-hypogastric and ilioinguinal nerves: Terminal branches of the anterior rami of the L1 spinal nerve.
The dermatomal distribution of the abdominal wall closely correlates with the pathway of spinal nerves and their branches because there is no plexus formation at paravertebral level.2
According to Rozen et al,3 branches further communicate at multiple locations, including large branch communications on the anterolateral abdominal wall (intercostal/upper TAP plexus) and plexuses that run with the deep circumflex iliac artery (DCIA) (lower TAP plexus) and the deep inferior epigastric artery (DIEA) (rectus sheath plexus). Since these segmental nerves communicate just above the transversus abdominis muscle, the subfascial spread of local anesthetic can provide anterolateral abdominal wall analgesia.
Muscles
The anterolateral abdominal wall is formed by bilaterally paired three flat muscles and two vertical muscles).4
- Flat muscles (from outside to inside): External oblique muscle, Internal oblique muscle, and Transversus abdominis muscle.
- Vertical muscles: Rectus abdominis and Pyramidalis muscle.
The function of these muscles is to flex and rotate the trunk. They also support and compress the abdominal viscera. The aponeuroses of flat abdominal muscles join together at the medial border to give rise to the rectus sheath. The rectus sheath envelops the rectus abdominis muscle. The anterior division of the rectus sheath completely covers the rectus abdominis muscle throughout its anterior surface, whereas the posterior division of the rectus sheath covers the posterior surface of the rectus abdominis to the arcuate line (midpoint between the umbilicus and pubis), below which it is lined by transversalis fascia.4 Transversalis fascia is a thin aponeurotic sheet between the inner surface of the transversus abdominis muscle and the parietal peritoneum. Linea Alba is a tendinous raphe in the midline of the abdomen, between two rectus abdominis muscles, which originates from the Xiphoid process and inserts at the pubic symphysis. It is formed by fusion of the anterior and posterior leaves of the rectus sheath.4
Nomenclature of TAP block
A TAP block basically involves deposition of local anesthetic in the plane between the internal oblique and transversus abdominis muscles to target the nerves passing through them. It is a field block, hence local anesthetic volumes required are high. Since the transversus abdominis plane is spread over a large area traversing dermatomes, it forms a huge bull’s eye for anesthesiologists to target. Hence, the TAP block has evolved considerably from the “Classical” TAP block introduced by Rafi, to other variants which try to approach the “Transabdominis Plane” via other sites.1 There is no standardized classification and nomenclature of TAP block.5,6 Tsai et al7 have classified the TAP block on the basis of the site of injection and the dermatomes targeted. These variants target various particular dermatomes and combinations of these blocks broaden the application of the TAP block in alleviating somatic pain compared to the classical TAP block technique.
Classical TAP block
The classical TAP block is the landmark based TAP approach which was first introduced by Rafi.1 The “triangle of petit” (Figure 1) is the landmark from where the TAP is approached. The triangle of petit is situated between the iliac crest and subcostal margin. The base of the triangle is formed by the iliac crest, and it is bounded anteriorly by the external oblique muscle and posteriorly by the lattissimus dorsi muscle. According to the technique described by McDonnell et al,8 the iliac crest is palpated in anterior to posterior direction, and insertion of the latissimus dorsi is identified.A 5 cm 25 gauge blunt tip needle is inserted just above iliac crest perpendicular to the skin, till a “double pop” sensation is felt. The first pop indicates that the needle has crossed the external oblique muscle. The second pop indicates that the needle has crossed internal oblique muscle and lies at a plane between internal oblique and transversus abdominis muscles, commonly known as the TAP plane. Since it is a field block, a large amount of local anesthetic is required. Usually 20 ml of local anesthetic is deposited on each side; the concentration is decided by the total safe dose of the local anesthetic used. We prefer to use Ropivacaine. According to a cadaveric and radiological study by McDonnell et al,9 the injectate via this approach spreads to T7 to L1. The problems with the classical landmark approach are apparent. It is difficult to ascertain the landmarks, especially in an obese individual, there are anatomical variations in the location of triangle of petit, and the pop sensation can be pretty subjective and prone to inter-individual variations with chances of peritoneal perforation.10 Thus, the landmark based TAP plane block is increasingly being abandoned in favor of ultrasound guided TAP blocks.11
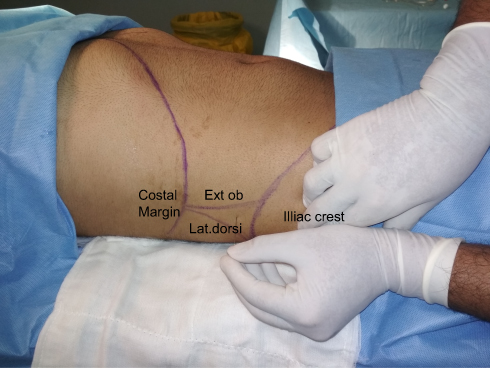 |
Figure 1 Triangle of Petit. |
Ultrasound guided TAP blocks
Ultrasound is now the established gold standard for peripheral nerve blocks.11 The key to ultrasound guided TAP blocks is identification of the transversus abdominis muscle and potential space above it, called the Transversus Abdominis Plane (TAP). We prefer to use high frequency linear probes. Figure 2 illustrates the probe position for various approaches. Low frequency curvilinear probes have been used for obese patients.12 The classification of an ultrasound guided TAP block proposed by Tsai et al7 is illustrated in Table 1. We use this classification as a template to explore various types of TAP block.
- Subcostal approach: Hebbard et al13 failed to replicate the spread of analgesia to supraumbilical areas when they performed a “mid-axillary line ultrasound guided TAP block”. The insertion point in this approach is in the mid axillary line, whereas in the classical landmark approach the insertion point is nearer the posterior axillary line, at the apex of the triangle of petit. A possible explanation is that, with the landmark approach, there is posterior spread of local anesthetic into the paravertebral space, thus achieving rostral spread of analgesia.14 Thus, Hebbard15 described a subcostal TAP block where local anesthetic is deposited between the rectus abdominis and transversus abdominis muscle, or alternatively between rectus abdominis muscle and posterior rectus sheath in cases where the transversus abdominis does not extend below the rectus abdominis. The scanning for a TAP block via any approach is similar. It is vital to identify the trans abdominis plane (TAP . Initially the probe is placed transversely in the midline of the anterior abdominal wall, just below the xiphoid process (Figure 2, position 1) with the patient in supine position. Linea Alba is easily identified in the center, in between two rectus abdominis muscles (Figure 3). The probe is moved laterally to identify the lateral border of the rectus abdominis muscle, Linea Semilunaris, external and internal oblique muscles, and transversus abdominis muscle (Figure 4). Once we have acquired this view, a 25 gauge needle is inserted in medial to lateral direction in the plane to the probe (Figure 5), till it reaches the TAP plane between the rectus abdominis and transversus abdominis muscles. The local anesthetic is deposited here after confirming the needle tip position with hydrodissection. The nerves blocked are T6–T9 supplying the upper abdomen just below the xiphoid and parallel to the costal margin, and this block is suitable for upper abdominal surgeries.7,16
- Lateral approach: Hebbard et al13 were among the first ones to attempt replication of the classical landmark technique with ultrasound guidance. In their study they found consistent analgesia over the infraumbilical area of the anterior abdominal wall between two midclavicular lines. The nerves blocked are anterior cutaneous branches of T10–T12. However, there is sparing of lateral cutaneous branches of T10 to T12 which supply the infraumbilical lateral abdominal wall. The probe is placed transversely on the lateral abdominal wall at mid-axillary line between costal margin and iliac crest (Figure 6). The three abdominal muscles are seen below subcutaneous fat, the plane between internal oblique and transversus abdominis muscle is identified (Figure 7). The needle is inserted in the plane in medial to lateral direction, local anesthetic injected in the TAP plane. Even if local anesthetic is deposited below the fascia, and above the transversus abdominis muscle, it may exert an analgesic effect as all nerves travel in the deep part of fascia according to studies done by Rozen et al3 and Gadsden et al17. It is always better to hydrodissect with saline to confirm the correct position of the needle tip before injecting local anesthetic.
- Posterior approach: The advantages of the posterior approach over lateral approach are better prolonged anesthesia and probable blockade of lateral cutaneous nerves providing better coverage.18 The prolonged analgesia is explained by posterior spread of local anesthetic to paravertebral space from T4 to L1 and partial blockade of the thoracolumbar sympathetic chain.19 Although definitive RCTs comparing lateral and posterior TAP blocks are lacking. The linear probe is placed in a lateral approach initially, then it is moved posteriorly till a scan reveals the transversus abdominis muscle tailing off into the aponeurosis, near the Quadratus lumborum muscle (Figures 8 and 9). Local anesthetic is deposited superficial to aponeurosis.
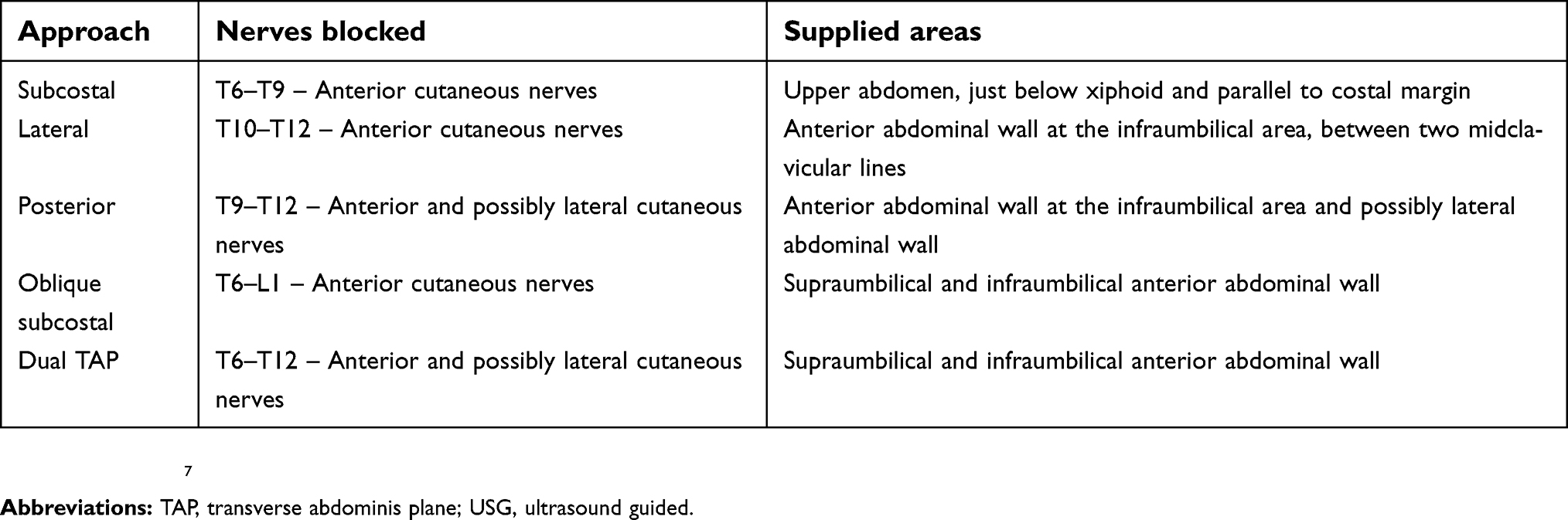 |
Table 1 Classification of USG guided TAP block |
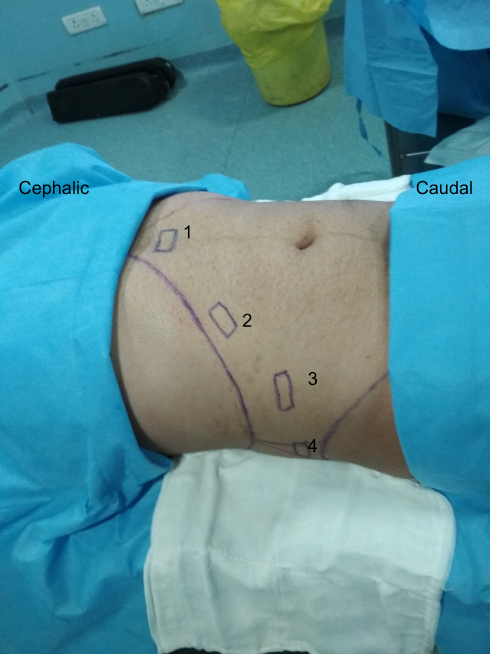 |
Figure 2 Suggested ultrasound probe positions for various approaches. (A) Initial scanning position for identification of linea alba and rectus abdominis, (B) probe position for subcostal approach, (C) probe position for lateral approach, (D) probe position for posterior approach. |
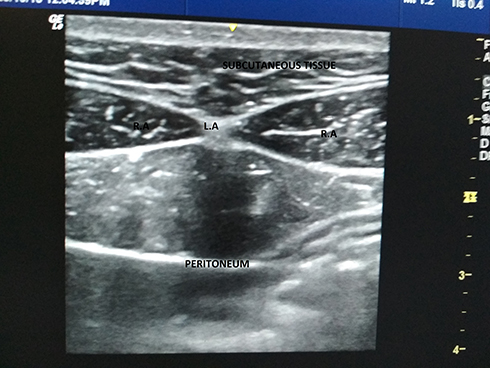 |
Figure 3 USG image at position 1 of Figure 2. Abbreviations: RA, rectus abdominis; LA, linea alba; USG, ultrasound guided. |
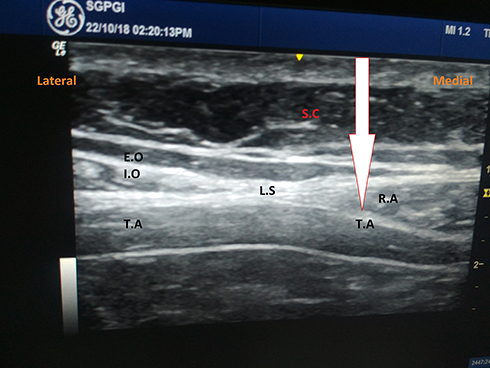 |
Figure 4 Subcostal TAP block. Arrow highlights the tap plane where the drug should be deposited. Abbreviations: RA, rectus abdominis; IO, internal oblique; EO, external oblique; LS, linea semilunaris; SC, subcutaneous tissue; P, peritoneum; TAP, transverse abdominis plane. |
 |
Figure 5 Subcostal TAP block: direction of needle and probe.Abbreviation: TAP, transverse abdominis plane. |
 |
Figure 6 Lateral TAP block. Direction of needle and probe. Abbreviation: TAP, transverse abdominis plane. |
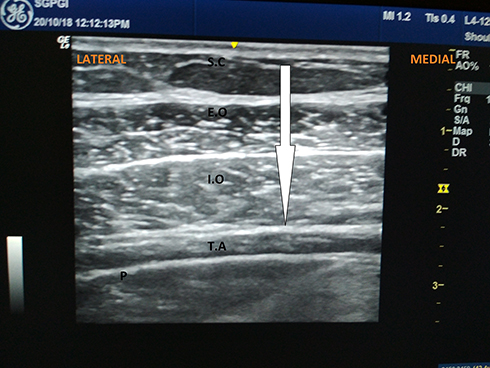 |
Figure 7 Lateral TAP block. Arrow highlights the tap plane where drug should be deposited. Abbreviations: RA, rectus abdominis; IO, internal oblique; EO, external oblique; SC, subcutaneous tissue; P, peritoneum; TAP, transverse abdominis plane. |
 |
Figure 8 Posterior TAP block. Direction of needle and probe.Abbreviation: TAP, transverse abdominis plane. |
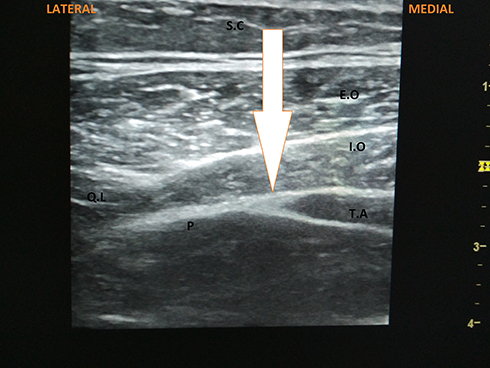 |
Figure 9 Posterior TAP block. Arrow highlights the TAP plane where drug should be deposited. Abbreviations: RA, rectus abdominis; IO, internal oblique; EO, external oblique; SC, subcutaneous tissue; P, peritoneum; QL, quadratus lumborum; TAP, transverse abdominis plane. |
Combined approaches
- Oblique Subcostal Block: This is a modified form of the subcostal TAP block, introduced by Hebbard et al20 in 2010. The initial steps are like the subcostal approach, a linear probe is positioned over the subcostal area and the TAP plane identified. A long needle of 15–20 cm is introduced in the plane in medial to lateral direction till it reaches between the transversus abdominis and rectus abdominis. The TAP plane is hydrodissected obliquely under ultrasound view along the line shown in Figure 10. This requires a large amount of local anesthetic (around 40–80 mL) and is technically difficult to perform compared to other TAP block approaches. The advantage it offers is a single site injection for both supraumbilical and infraumbilical analgesic coverage, while the obvious disadvantage is the risk of local anesthetic toxicity due to the large volumes of local anesthetic required. It is said to provide analgesia from T6–L1.20 According to Chen et al,21 an oblique subcostal block produced reliable analgesia over T7–T12 dermatomes consistently, but it blocked T6 and L1 dermatomes variably. However, other studies have illustrated analgesic effects in both supraumbilical and infraumbilical surgeries.22–24
- Dual TAP Block: This approach is a combination of subcostal block with posterior or lateral TAP block. The bilateral dual TAP block was first introduced by Borglum et al.25 Niraj et al26 did something similar and called it a four quadrant TAP block. This offers the same advantage as the oblique subcostal block, but is technically less challenging.
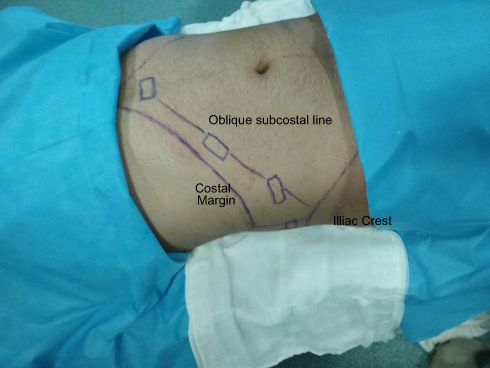 |
Figure 10 Direction of hydrodisscetion in oblique subcostal block. Initially subcostal TAP block is performed, then the needle moved along the oblique subcostal line.Abbreviation: TAP, transverse abdominis plane. |
Complications
The TAP block has remarkably low incidence of complications. Since a TAP block is a field block, where relatively large amounts of local anesthetic are used, especially when performed bilaterally, it is vital to ensure that the total toxic dose of local anesthetic is not exceeded.27 Like any other regional block, it is important to have lipid emulsion and other resuscitation equipment at hand. Liver injury has been reported due to blind and ultrasound guided TAP blocks.28,29 It is important to keep in mind the abdominal anatomy and to keep the needle tip in view in the ultrasound at all times. There is a case report of Transient Femoral palsy after a TAP block was induced by incorrect local anesthetic deposition between the transversus abdominis and the transversalis fascia.30 This complication is self-limiting and is due to seepage of local anesthetic through the transversalis fascia plane to the femoral triangle.
Conclusion
Over the past decade, the TAP block has emerged as a reliable tool of multimodal analgesia. Although it blocks only the somatic component of pain, still studies have revealed a consistent benefit in the first 24–48 hours after surgery in terms of pain scores and overall opioid consumption.18,31 Its safety and dependability have increased with ultrasound usage. However, due to multiple approaches and techniques, it is vital to have a lucid and recognized nomenclature system for TAP block. We found the classification by Tsai et al7 (Table 1) to be most comprehensive compared to another classification offered by Hebbard.6 Effective use of the TAP block requires sound knowledge of the dermatomes involved in surgical incision and optimum approach and dosage of local anesthetic to be used. A posterior TAP block offers a longer duration of analgesia than does a lateral TAP block for the infraumbilical abdominal wall.18 If analgesia over the supraumbilical wall is required, subcostal, oblique subcostal, or dual TAP blocks are recommended. Studies with catheters in the TAP plane for continuous local anesthetic infusion have also yielded encouraging results.16,20,24,26 Thus, based on accumulating evidence, the TAP block is going to be a cornerstone in postoperative multimodal analgesia, especially in situations where central neuraxial blocks are contraindicated or difficult to perform.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rafi AN. Abdominal field block: a new approach via the lumbar triangle. Anaesthesia. 2001;56(10):1024–1026. doi:10.1046/j.1365-2044.2001.02279-40.x
2. Moore KL, Dalley AF
3. Rozen WM, Tran TMN, Ashton MW, Barrington MJ, Ivanusic JJ, Taylor GI. Refining the course of the thoracolumbar nerves: a new understanding of the innervation of the anterior abdominal wall. Clin Anat. 2008;21(4):325–333. doi:10.1002/ca.20625
4. Standring S, Gray H, editors. Chapter 61. In: Gray‘s Anatomy: The Anatomical Basis of Clinical Practice.
5. Borglum J, Abdallah FW, McDonnell JG, Moriggl B, Bendtsen TF. TAP block terminology. Anaesthesia. 2014;69:1055–1056. doi:10.1111/anae.12812
6. Hebbard P. TAP block nomenclature. Anaesthesia. 2015;70:112–113. doi:10.1111/anae.12970
7. Tsai H-C, Yoshida T, Chuang T-Y, et al. Transversus abdominis plane block: an updated review of anatomy and techniques. Biomed Res Int. 2017;2017(8284363). doi:10.1155/2017/8284363
8. McDonnell JG, Curley G, Carney J, et al. The analgesic efficacy of transversus abdominis plane block after cesarean delivery: a randomized controlled trial. Anesth Analg. 2008;106:186–191. doi:10.1213/01.ane.0000290294.64090.f3
9. McDonnell JG, O‘Donnell BD, Farrell T, et al. Transversus abdominis plane block: a cadaveric and radiological evaluation. R eg Anesth Pain Med. 2007;32(5):399–404.
10. Zietek Z, Starczewski K, Sulikowski T, et al. Useful points of geometry and topography of the lumbar triangle for transversus abdominis plane block. Med Sci Monit. 2015;21:4096–4101. doi:10.12659/MSM.894620
11. Hopkins PM. Ultrasound guidance as a gold standard in regional anaesthesia. Br J Anaesth. 2007;98(3):299–301. doi:10.1093/bja/ael387
12. Ueshima H, Kubo K, Sakamoto S, et al. A case of the transversus abdominis plane block in a super obese patient using a convex probe. Masui (Jpn J Anesthesiol). 2013;62(4):439–441.
13. Hebbard P, Fujiwara Y, Shibata Y, Royse C. Ultrasound-guided transversus abdominis plane (TAP) block. Anaesth Intensive Care. 2007;35(4):616–617.
14. Carney J, Finnerty O, Rauf J, Bergin D, Laffey JG, Mc Donnell JG. Studies on the spread of local anaesthetic solution in transversus abdominis plane blocks. Anaesthesia. 2011;66(11):1023–1030. doi:10.1111/j.1365-2044.2011.06855.x
15. Hebbard P. Subcostal transversus abdominis plane block under ultrasound guidance. Anesth Analg. 2008;106(2):674–675. doi:10.1213/ane.0b013e318161a88f
16. Maeda A, Shibata SC, Wada H, et al. The efficacy of continuous subcostal transversus abdominis plane block for analgesia after living liver donation: a retrospective study. J Anesth. 2016;30(1):39–46. doi:10.1007/s00540-016-2183-4
17. Gadsden J, Ayad S, Gonzales JJ, Mehta J, Boublik J, Hutchins J. Evolution of transversus abdominis plane infiltration techniques for postsurgical analgesia following abdominal surgeries. Local Reg Anesth. 2015;8:113–117. doi:10.2147/LRA
18. Abdallah FW, Laffey JG, Halpern SH, Brull R. Duration of analgesic effectiveness after the posterior and lateral transversus abdominis plane block techniques for transverse lower abdominal incisions: a meta-analysis. Br J Anaesth. 2013;111(5):721–735. doi:10.1093/bja/aet214
19. Finnerty O, McDonnell JG. Transversus abdominis plane block. Curr Opin Anaesthesiol. 2012;25:610–614. doi:10.1097/ACO.0b013e328357b165
20. Hebbard PD, Barrington MJ, Vasey C. Ultrasound-guided continuous oblique subcostal transversus abdominis plane blockade: description of anatomy and clinical technique. Reg Anesth Pain Med. 2010;35(5):436–441. doi:10.1097/AAP.0b013e3181e66702
21. Chen Y, Shi K, Xia Y, et al. Sensory assessment and regression rate of bilateral oblique subcostal transversus abdominis plane block in volunteers. Reg Anesth Pain Med. 2018;43(2):174–179. doi:10.1097/AAP.0000000000000715
22. Chen CK, Tan PCS, Phui VE, Teo SC. A comparison of analgesic efficacy between oblique subcostal transversus abdominis plane block and intravenous morphine for laparascopic cholecystectomy. a prospective randomized controlled trial. Korean J Anesthesiol. 2013;64(6):511–516. doi:10.4097/kjae.2013.64.6.511
23. Mukherjee A, Guhabiswas R, Kshirsagar S, Rupert E. Ultrasound guided oblique subcostal transversus abdominis plane block: an observational study on a new and promising analgesic technique. Indian J Anaesth. 2016;60(4):284–286. doi:10.4103/0019-5049.179468
24. Yoshida T, Furutani K, Watanabe Y, Ohashi N, Baba H. Analgesic efficacy of bilateral continuous transversus abdominis plane blocks using an oblique subcostal approach in patients undergoing laparotomy for gynaecological cancer: a prospective, randomized, triple-blind, placebo-controlled study. Br J Anaesth. 2016;117(6):812–820. doi:10.1093/bja/aew339
25. Borglum J, Maschmann C, Belhage B, Jensen K. Ultrasound-guided bilateral dual transversus abdominis plane block: a new four-point approach. Acta Anaesthesiol Scand. 2011;55(6):658–663. doi:10.1111/j.1399-6576.2011.02454.x
26. Niraj G, Kelkar A, Hart E, Kaushik V, Fleet D, Jameson J. Four quadrant transversus abdominis plane block and continuous transversus abdominis plane analgesia: a 3-year prospective audit in 124 patients. J Clin Anesth. 2015;27(7):579–584. doi:10.1016/j.jclinane.2015.07.005
27. Scherrer V, Compere V, Loisel C, Dureuil B. Cardiac arrest from local anesthetic toxicity after a field block and transversus abdominis plane block: a consequence of miscommunication between the anesthesiologist and surgeon. A A Case Rep. 2013;1;1(5):75–76. doi:10.1097/ACC.0b013e3182973a3f
28. Farooq M, Carey M. A case of liver trauma with a blunt regional anesthesia needle while performing transversus abdominis plane block. Reg Anesth Pain Med. 2008;33(3):274–275. doi:10.1016/j.rapm.2007.11.009
29. Lancaster P, Chadwick M. Liver trauma secondary to ultrasound-guided transversus abdominis plane block. Br J Anaesth. 2010;104(4):509–510. doi:10.1093/bja/aeq046
30. Manatakis DK, Stamos N, Agalianos C, Karvelis MA, Gkiaourakis M, Davides D. Transient femoral nerve palsy complicating “blind” transversus abdominis plane block. Case Rep Anesthesiol. 2013;2013:3. Article ID 874215. doi:10.1155/2013/874215
31. Petersen PL, Mathiesen O, Torup H, Dahl JB. The transversus abdominis plane block: a valuable option for postoperative analgesia? Topical Rev Acta Anaesthesiol Scand. 2010;54:529–535. doi:10.1111/j.1399-6576.2010.02215.x
32. Obstetric anaesthesia. New York: Mount Sinai Hospital. Available from: http://pie.med.utoronto.ca/OBAnesthesia/OBAnesthesia_content/OBA_blocks_module.html. Accessed 1 September 2018.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.