")
Back to Journals » Local and Regional Anesthesia » Volume 13
Anesthetic Techniques: Focus on Lumbar Erector Spinae Plane Block
Authors Tulgar S , Aydin ME , Ahiskalioglu A , De Cassai A , Gurkan Y
Received 16 July 2020
Accepted for publication 16 September 2020
Published 25 September 2020 Volume 2020:13 Pages 121—133
DOI https://doi.org/10.2147/LRA.S233274
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Stefan Wirz
Serkan Tulgar,1 Muhammed Enes Aydin,2,3 Ali Ahiskalioglu,2,3 Alessandro De Cassai,4 Yavuz Gurkan5
1Maltepe University Faculty of Medicine, Department of Anesthesiology and Reanimation, Istanbul, Turkey; 2Ataturk University School of Medicine, Department of Anaesthesiology and Reanimation, Erzurum, Turkey; 3Clinical Research, Development and Design Application and Research Center, Ataturk University School of Medicine, Erzurum, Turkey; 4Anaesthesiology and Intensive Care, University Hospital of Padua, Padua, Italy; 5Koc University, Faculty of Medicine Department of Anesthesiology and Reanimation, Istanbul, Turkey
Correspondence: Serkan Tulgar
Maltepe University Hospital, Maltepe, Istanbul, Turkey
Tel +905055423985
Email [email protected]
Abstract: Defined in the last decade, erector spinae plane block (ESPB) is one of the more frequently used interfacial plans, and it has been the most discussed block among the recently defined techniques. Lumbar ESPB administered at lumbar levels is relatively novel and is a new horizon for regional anesthesia and pain practice. In this article, we aim to explain and introduce different approaches and explain the possible mechanism of action of lumbar ESPB. The objective of this review is to analyze the case reports, clinical and cadaveric studies about lumbar ESPB that have been published to date. We performed a search in “Pubmed” and “Google Scholar” database. After a selection of the relevant studies, 59 articles were found eligible and were included in this review. While we believe that lumbar ESPB is reliable and easy, we suggest that its efficacy and indications should be verified with anatomical and clinical studies, and its safety should be confirmed with pharmacokinetic studies. Moreover, the possibility of complications must be considered.
Keywords: lumbar erector spinae block, regional anesthesia, interfascial plane blocks
Introduction
With the introduction of ultrasound technology into regional anesthesia and pain management routines, the popularity of interfascial plane blocks has increased. Although primarily limited to abdominal wall blocks such as transversus abdominis plane block, ilioinguinal-iliohypogastric blocks and rectus sheath blocks, the range of blocks has increased to also include anterior and lateral thoracic wall blocks (such as pectoral blocks and serratus blocks), posterior thoracoabdominal blocks (quadratus lumborum blocks – QLB) and more recently peri-paravertebral blocks.1–4
Despite being a recently defined block,5 erector spinae plane block has quickly gained popularity due to its ease of application and safety profile.6,7 ESPB was first reported for use in chronic pain of the thoracic area. Its range of indications then gradually increased to include acute and chronic pain, reported sequentially in the lumbar,8 cervical9 and sacral10 areas. Although several studies and reviews summarize the efficacy and limitations of thoracic ESPB, none have been conducted for lumbar ESPB. The goal of this study is to review the literature on the efficacy of lumbar ESPB in several surgeries, pain management, and its potential opioid-sparing effects.
In this review, we will discuss the mechanism of action and applications of ESPB performed from the lumbar level in the light of the current literature.
Anatomic Considerations in ESPB
Although anatomical similarities exist for ESPB performed at different levels, sonoanatomic and application-specific differences are significant at different levels. The erector spinae muscles are back muscles that aid in keeping the body upright and are also known as Autochthonous back muscles.11 The ESM extends from the cervical to sacral levels. In the thoracic area, they exist as the spinalis, longissimus, and iliocostalis muscles from medial to lateral. In the lumbosacral region, the anatomy differs. The multifidus muscle, which also exists in the cervical and thoracic region, thickens as it descends to the lumbosacral region and becomes prominent towards the medial of the spinous processes and adheres to the dorsal side of the sacrum. While some authors accept the multifidus muscle as part of the ESM in the lumbosacral region,11 some accept it as a separate muscle, based on Terminologiaanatomica.12 Similar to most figures in published literature, we consider the multifidus muscle as part of ESM and likewise accept this for our current paper.
The anatomy of the thoracic nerves also differs between the two areas. Spinal nerves continue as the dorsal ramus and ventral ramus (intercostal nerves) after leaving the epidural foramen. However, in the lumbosacral region, the ventral ramus merges to form the lumbar and sacral plexuses. While the dorsal ramus split into the lateral and medial branches in the thoracic area, in the lumbosacral area they separate into the medial, intermediate, and lateral branches (Figure 1). The dorsal ramus of the lumbosacral nerves merges within themselves to form the cluneal nerves which are responsible for the sensory innervation of the waist and buttocks. Therefore, the sensorial anatomy of the lower abdomen and lower extremity is more complicated than the thoracoabdominal region. Consequently, craniocaudal spread of ESPB is more limited in the lumbar region when compared to the thoracic region.13 Craniocaudal spreading is related to the spreading in the fascial plane, but due to the size of the vertebra, the area of the fascial plane where the LA will spread (in proportion to the muscle size), the differences observed in the structure of the fascia between the thoracic and lumbar regions, and the differences in the anatomical barriers that may be effective in the transition to the anterior region. In a review in the literature where anatomical investigations are evaluated, it is stated that; a median of 3.3 mL of local anesthetic was needed to cover one vertebral level when considering the whole vertebral column, whereas 2.5 mL was needed for thoracic and 5 mL were needed for the lumbar area.13
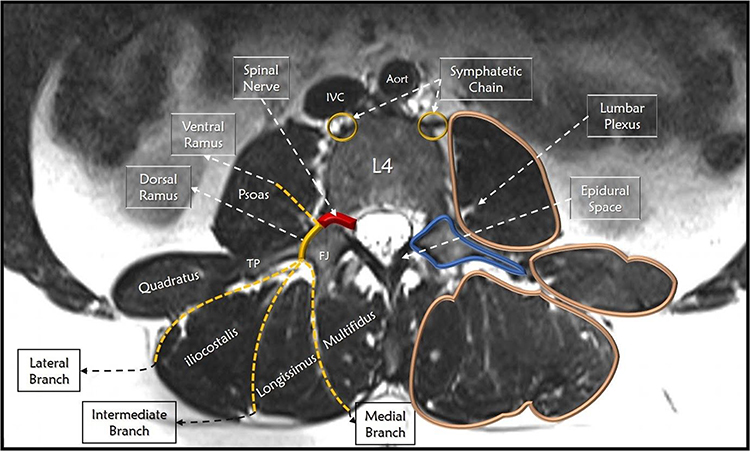 |
Figure 1 Illustration of anatomical structures of axial MR section from L4 level. |
It should be kept in mind that as the application point is deeper and more latera, lumbar ESPB is more challenging to perform and to more difficult to sonographicallyvisualize when compared to thoracic applications.14
Literature Review
A literature review was performed by searching Pubmed (http://pubmed.ncbi.nlm.nih.gov) and Google Scholar (http://scholar.google.com) using the keywords “Erector spinae block” and “Erector Block” on 21/06/2020. Some published articles were observed to include the strings “Erector spine” and “Erector Spinal” so we suggest that any future review includes these strings too. Results were analyzed and 59 articles – mostly case reports and correspondences, were included in the review. Article types, content, block features, and anatomic evaluations were included as points of evaluation for this review.
Lumbar ESPB Technical Features
Approaches and Sonography
Lumbar ESPB was first defined using the parasagittal approach (Figure 2).8 As the parasagittal approach allows for in-plane and out of plane techniques to be used, it is the choice of many clinicians.
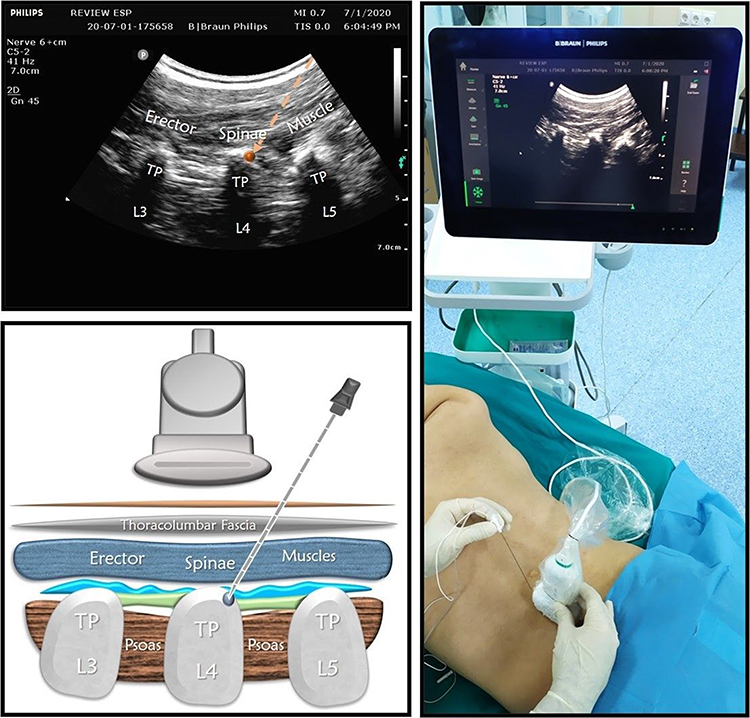 |
Figure 2 Illustration, local anesthetic spreading, position, and orientation of the ultrasound transducer during a parasagittal scan of the lumbar region with the subject in the prone position. Ultrasound images indicated a parasagittal approach for the lumbar erector spinae plane block. |
In this level, ESP can be performed on the transverse plane (Figure 3). The transverse plane allows the dorsals structures of the vertebra to be sonographically visualized simultaneously. A convex probe can be used to distinguish the different anatomic structures from each other. This approach can be performed easily using both the in-plane and the out of plane technique.
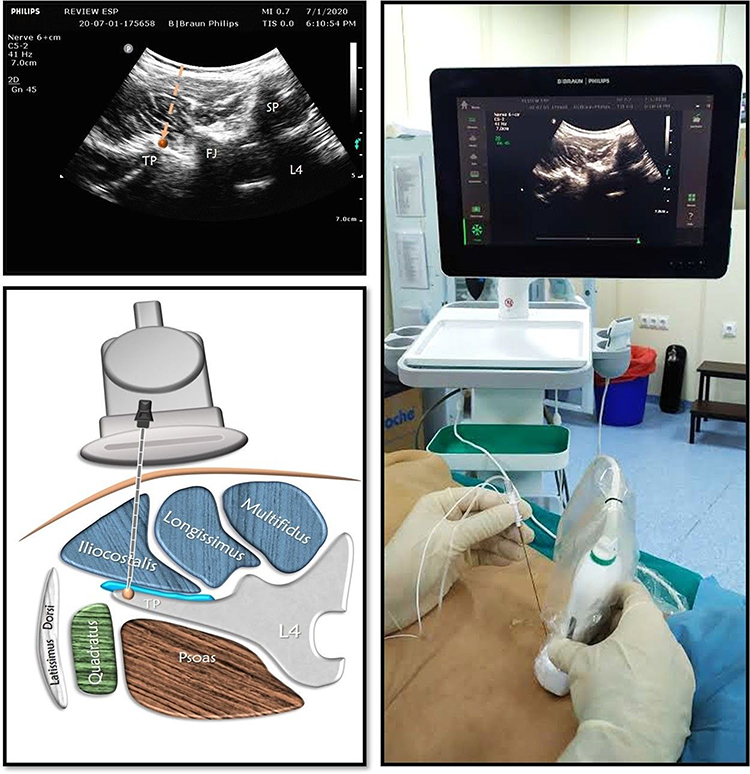 |
Figure 3 Illustration, local anesthetic spreading, position, and orientation of the ultrasound transducer during a transverse scan of the lumbar region with the subject in the prone position. Ultrasound images indicated a transverse approach for the lumbar erector spinae plane block. |
The transverse subcostal approach – also named as the Aksu approach – was later defined (Figure 4).15 This approach leads to improved visualization, especially at L3-4-5 levels, but has also been used for upper lumbar areas. This approach allows for the application of ESPB in the lateral position under general anesthesia. This approach can easily be applied as it uses the “Shamrock” technique – in which clinicians generally have a better command of sonoanatomicstructures. The major disadvantage of this technique is accepted as worse sono-visualization of LA spread. It appears that this technique is easily applied mainly in pediatric patients.16
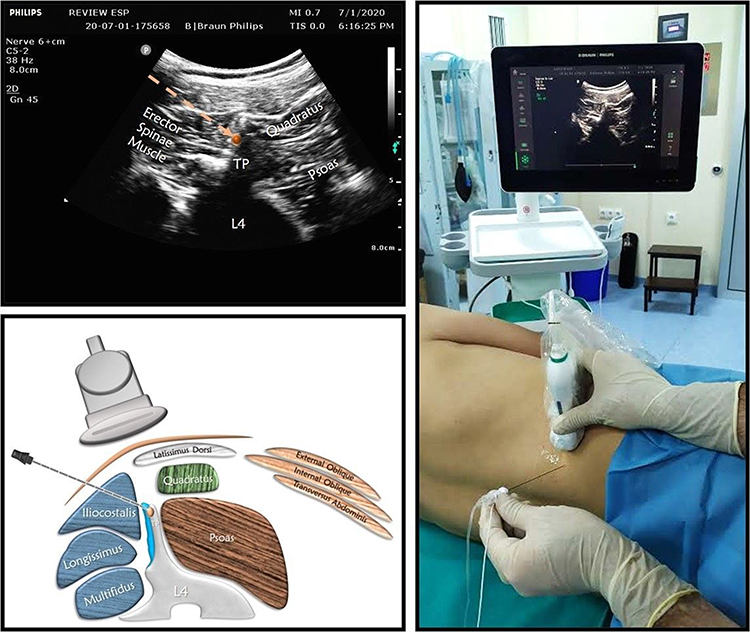 |
Figure 4 Illustration, local anesthetic spreading, position, and orientation of the ultrasound transducer during a lateral scan of the lumbar region with the subject in the lateral decubitus position. Ultrasound images indicated an “Aksu” approach for the lumbar erector spinae plane block. |
In the Tulgar modification, in addition to classical ESPB, a second injection of LA is performed between the transverse process and the psoas major muscle (Figure 5). This modification aims to block the lumbar plexus, which is close to the psoas major muscle.17,18
 |
Figure 5 Illustration, local anesthetic spreading, position, and orientation of the ultrasound transducer during a parasagittal scan of the lumbar region with the subject in the prone position. Ultrasound images indicated a “Tulgar” approach for the lumbar erector spinae plane block. |
In cases in which ultrasonography is unavailable, the landmark guided ESPB can be an alternative option.19,20 In landmark guided ESPB, the procedure can be performed by targeting the transverse process 3 cm lateral to the spinous process for the thoracic and approximately 5–6 cm for the lumbar area.
The Darling modification also exists and will be mentioned later in the catheterization section of this paper.
ESPB can be performed in any position. Generally, the choice of position for hip and knee surgeries is the lateral position and for lumbar surgery or pain medicine, the prone position is preferred.21,22 Although it can also be performed in a sitting position, it may be less comfortable for both the practitioner and the patient.
When compared to thoracic ESPB, lumbar ESPB is a deeper block.14 A convex probe will, therefore, give better anatomic visualization compared to a linear probe. However, the convex and linear probes appear to be equally utilized in the literature. Most clinicians have reported the use of the in-plane technique, but it can also be applied practically via the out-of-plane method. Transducers can be placed in parasagittal and transverse planes.
Only two reports of catheter use – both in knee surgery – have been reported with successful results.23,24 In a lumbar ESPB performed using a thoracic approach, Darling et al25,26 placed a catheter at the T11-12 level and advanced the catheter caudally to the lumbar area with excellent results. Lumbar ESPB (L4) using the landmark technique has also been reported with adequate analgesia obtained in hip surgery.24 While no consensus exists on the regiment of bolus vs continuous infusion or the rate for catheter application, it should be kept in mind that personalized plans should be made per patient with calculations on maximum daily doses kept in mind. After low concentration and high volume boluses, 5–10 mL/h continuous injections maybe suitable for interfascial plane blocks.
Choice of Local Anesthetic and Additives
Ropivacaine and bupivacaine are the most common choice of LA in lumbar ESPB and are generally used in a concentration of 0.375% or 0.25%. When a rapid onset of the block is sought, the combination of 0.5% bupivacaine to 2% lidocaine with other local anesthetics is recommended. Higher volume mixtures generally include 1/200.000 ratio of adrenaline to avoid local anesthetic toxicity.27 Long-acting corticosteroids may also be added to the mixture when used for the management of chronic pain, neuropathic pain, low back pain, or myofascial pain.28
The Spread of Injectate; Anatomical Studies and Radiological Imaging
Although many cadaveric studies and radiological imaging studies investigating the spread of LA in thoracic ESPB have been published, an accepted predictable spread cannot be suggested.7 Unfortunately, this is similar to the lumbar ESPB. In a minireview, the relationship between injectate volume and anatomical distribution and differences were revealed separately in thoracic and lumbar ESPB.13 In this article, a 5 mL local anesthetic application is recommended for each lumbar nerve blockade in lumbar ESPB. The anatomic spread of LA in lumbar ESPB has been reported in only a few clinical/cadaveric studies and case reports.29–34 Lumbar ESPBs have been performed from the L4 vertebra transverse process level in all reports. All papers, including anatomic evaluation, have been demonstrated in Figure 6.
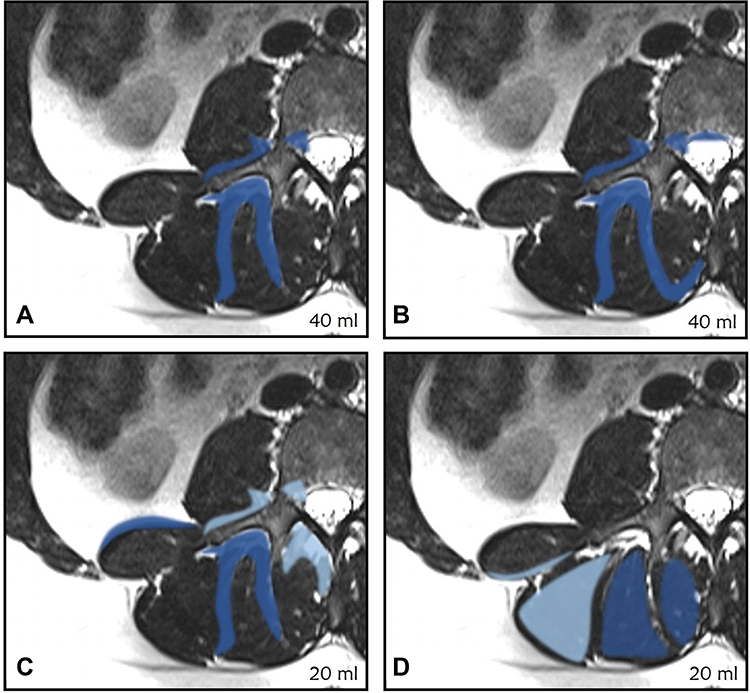 |
Figure 6 Demonstration of the spread of injectate related to lumbar ESPB. (A) Tulgar et al (B) Celik et al (C) S.J. De Lara González et al (D) Monica W Harbell. In Figures (C and D), Dark blue, the spread of mixture with all injections, Light blue, the spread of mixture with some injections. |
In the first article with radiographic evaluation of lumbar ESPB, it was reported that the contrast agent spreads craniocaudally between T12 and S1 on the posterior of the transverse process. And also reported that LA significantly passed to the anterior of the transverse process and spread to lumbar neural foramina, around the psoas muscle and lumbar plexus.29
Chung et al administered ESPB using a 20 mL mixture for pain management in lower extremity complex regional pain syndrome.30,31 Balaban et al performed ESPB with 30 mL mixture for postoperative analgesia in total knee arthroplasty.30,31 Fluoroscopic imaging demonstrated spread to L2-S1 levels in both lumbar ESBP cases.
In a study reporting the high volume used in a single injection (40mL), MRI was used to demonstrate the spread of LA between L1-S4.32 Contrast was observed in the facial spinal muscle and the surrounding fascia, as well as in the erector spinae muscle. On the side of application, there were extensions to the L1/L2 to L4/L5 neural foramina, and to the anterior and posterior epidural space. The contrast agent had the following borders: facet joints and erector spinae muscles. When performed in high volumes, the mixture can show a wide range of distribution.
De Lara González et al33 reported their findings in 6 cadavers where bilateral lumbar ESPB (totaling 12 blocks) was performed using a 20 mL LA mixture. In all applications, the spread of the LA mixture was observed between L2-4 in the craniocaudal plane. In nine applications, the spread included L5 caudally and in one application L1 cranially. The first question regarding lumbar ESPB is whether LA spreads to the anterior of the transverse process. In nine injections this anterior spread was observed, with spread to the medial border of the psoas muscle in seven and spread to the L3 and L4 spinal nerves in two injections.
Harbell et al34 performed nine lumbar ESPB on five cadavers using 20mL at the L4 transverse process level and reported staining of the multifidus and longissimus muscles following six injections. In only one injection the spread was reported to have been observed posterior to the lumborum muscle. No spread to the anterior of the transverse process was reported.
Reports from cadaveric anatomic studies are essential for understanding the mechanism of action of plane blocks. However, due to their nature, cadaveric studies have a significant limitation. Even when fresh cadavers are used, tissue tension decreases due to the loss of vitality. Therefore, the spread of injectate in cadavers most probably does not accurately represent the spread that would occur under normal conditions.
Evaluation of Sensorial Block
To the best of our knowledge, there exists no study which systematically evaluated the sensorial effects of lumbar ESPB. Only a few case reports have reported sensorial findings after lumbar ESPB.8,17,23,25,28,30,35–47 Spread of LA between T12 and S1 dermatomes were reported when 30–40 mL of LA was used,28 with similar findings for the lower volume of 20 mL also reported.30,38 Low volume injections have generally been utilized in back pain and spinal surgeries.
In the only study that evaluated the sensorial effect of ESPB in the thoracic area, 20mL of LA was administered from the mid-thoracic region with spread reported in nine dermatomal areas.48 However, there is no such study for lumbar ESPB. Dose/effect studies for lumbar ESPB are required to determine the sensorial block and analgesic effect that lumbar ESPB leads to.
Dermatomes of the lower abdomen and lower extremities differ from the thoracoabdominal region in their distribution and course. While the dermatomes of the thoracic nerves follow a slightly oblique and parallel route, dermatomes of the lumbosacral nerves follow a more angled, intersectioned and complicated course.
In order to evaluate the sensorial blockage of lumbosacral ESPB, it is necessary to know the innervation field of the lateral and anterior branches of the posterior cutaneous branches of the spinal nerves. However, no paper has reported any details of the spinal nerve rami when evaluating lumbar ESPB’s sensorial blockage. It may be preferable to evaluate lumbar ESPB using cutaneous areas/percentages as the innervation areas of the lumbosacral nerve roots can be irregular and overlap with each other.49
Reported Indications
The first indication of thoracic ESPB was neuropathic pain but it has since been used for many indications from cervical to sacral areas. The first application of lumbar ESPB was for the postoperative analgesia of hip arthroplasty.8 As with thoracal ESPB, lumbar ESPB has been used for many indications of acute and chronic pain. Original studies involving Lumbar ESPB application are also presented in Table 1.
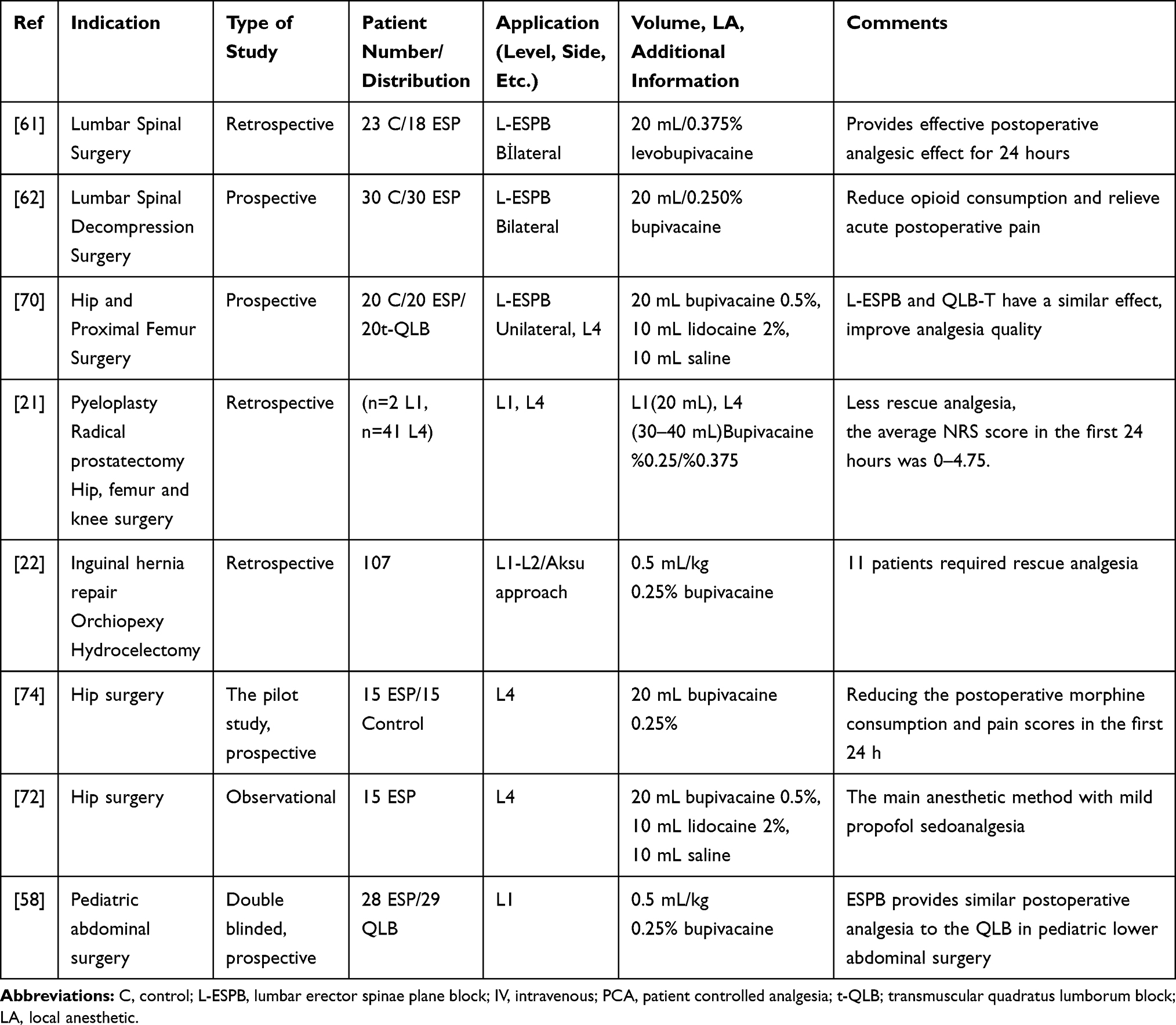 |
Table 1 Studies About Lumbar Erector Spinae Plane Block |
Pain Management
ESPB has been reported for use in complex regional pain syndromes,30,50 radiculopathy and myofascial pain of the back,32,36,51,52 chronic cancer pain,47 relief of zona spreading to the lower extremity,28,46 chronic pain after herniorrhaphy (L2)43 and similar indications. All papers are case reports and to our knowledge, no randomized controlled trial exists. Many cases have been reported regarding the effectiveness of ESPB for myofascial pain syndrome, especially in the thoracic region.53 However, ESPB can be an alternative approach for relieving myofascial pain in the lumbar region also.54,55 Steroids have been frequently added in applications related to pain medicine. The clinical and radiological similarities of epidural injection and high volume lumbar ESPB has been reported as similar.32 Lumbar ESPB is a promising procedure where failure or difficulty in completing fluoroscopy assisted pain management applications such as medial branch blockage, facet joint injection and epidural injections occur. The level of injection can be the same as the pathology leading to clinical findings or at an adjacent level. This leads to the safe and effective application of lumbar ESPB in conditions such as postherpetic neuralgia where the procedure can be performed from a non-infective level.
Postoperative Analgesia
Abdominal surgeries: unilateral or bilateral application for many indications such as inguinal hernia and other abdominal area surgeries (L1),56 iliac crest autograft (L1-2),26,57 nephrectomy (L2)41 and Pfannenstiel incisions (L-2)42 have been reported. The stated levels indicate the authors’ preferences. It should be noted that the level of application can be modified according to the dermatome that is going to be targeted. There are only two original studies on the indications mentioned above, although there are many case reports. Aksu et al retrospectively reviewed their thoracic/lumbar and sacral ESPB applications and offered their proposals for different indications.22 We recommend that those especially interested in pediatric anesthesia read this review. The same authors reported that ESPB performed at L1 level using 0.5 mL/kg 0.25% bupivacaine (max 20 mL) and QLB with the same volume has similar analgesic effects.58 There are case reports and clinical studies on ESPB performed from lower thoracic levels for lower abdominal surgeries – although we have chosen not to include these in this paper.
Spinal Surgeries
There are several case reports of lumbar ESPB used in lumbosacral spinal surgeries, one of which combined ESPB with thoracolumbar interfascial plane (TLIP) block, and another that reported modified lumbar ESPB dual injection.38,40,59,60 In a retrospective study evaluating the effectiveness of classical lumbar ESPB in microendoscopic lumbar surgery, lumbar ESPB added to multimodal analgesia (20mL of 0.25% bupivacaine per side, totaling 40mL) decreased first 24-hour opioid requirement and increase analgesia quality when compared to a control group.61 In a recently published randomized controlled study, the above-mentioned volume and concentrations were used to perform bilateral ESPB in lumbar decompression surgery with similar results.62 While ESPB can be performed from the same level as surgery, it can also be applied from adjacent levels. While there are studies of ESPB used for spinal surgeries of the lower thoracic area,63 we did not include them as they are out of the scope of this paper.
Orthopedic Procedures
Lumbar ESPB was first described for hip surgery8 and later for use in hip and femur surgery.17,24,25,29,39,64–68 Radiological evaluation and clinical results have shown that high volume lumbar ESPB results in similar analgesia as lumbar plexus block.29,32 It has also been reported for the postoperative analgesia of knee surgery.31,69 In a feasibility study, lumbar ESPB was found to decrease postoperative analgesia when compared to a control group.70 The same study found that transmuscular QLB and lumbar ESPB had similar analgesic effects.
Main Anesthetic Method
The use of ESPB and other interfascial blocks as the main anesthetic method are being increasingly reported.71 However, some time was required for the hypothetical principles of lumbar ESPB as the main anesthetic method to be formed. The basis of the hypothesis was formed following the use of lumbar ESPB for the postoperative analgesia of hip surgery and studies that radiologically demonstrated the spread of LA to the lumbar plexus and lumbar spinal nerves.8,29 The first use of lumbar ESPB and transmuscular QLB as the main anesthetic method was reported in a high-risk patient undergoing surgery for femur neck fracture.37 In this case report, 40 mL LA and 20 mL of LA were used for ESBP and QLB, respectively. Surgery was completed successfully with minimal dose opioids and ketamine without the need for general anesthesia.
In another case series of 15 high-risk geriatric patients, 40 mL LA was used for lumbar ESPB in hemiarthroplasty and intramedullary nailing surgery. All surgeries were completed under mild propofol sedation.72 It has been shown that in areas with complex innervation such as the hip and proximal femur, lumbar ESPB can be used as the main anesthetic method as it provides adequate anesthesia. The mechanism of action can be explained by the spread of LA given in lumbar EPSB to the paravertebral, epidural, and lumbar plexus.
In two separate case reports of two high-risk patients, bilevel ESPB performed from T12 and L1 with 15 mL of LA in each level, as the main anesthetic method in inguinal hernia surgery.45,73
Lumbar ESPB in Special Cases
Radicular pain can especially be observed during pregnancy and its treatment is challenging. Although medical treatment options are available, the uteroplacental transition is problematic and the use of drugs during pregnancy may not be preferred. A 13-week pregnant woman was relieved of cervical radiculopathy pain following ESPB at T3 level.75 Although lumbar ESPB is extensively used for lumbar radiculopathies, it should be kept in mind that acute radicular symptoms can be alternatively managed by lumber ESPB in pregnant women. Details on lumbar ESPB in pediatrics patients have previously been given in the indications section. Caution should be taken when determining the LA concentration and dosage of a single application or cumulative daily dosage. There are differing reports of lumbar ESPB used in patients of advanced age. Age groups, special patient populations, and those with different anatomical features (sportsperson, spinal anomalies, previous spinal surgery, etc.) should be evaluated for the use of lumbar ESPB.
Complications and Block Failure
ESPB is a relatively safe regional anesthesia technique with a low complication rate. However, pneumothorax and Harlequin syndrome has been reported following thoracic ESPB.76,77 Priapism following lumbar ESPB, lower extremity motor weakness following lower thoracic ESPB, and total motor block after lumbar procedures have been reported.35,50,78 Local anesthetic toxicity is a probable and feared complication of all regional anesthesia applications. Karaca et al52 reported a patient with a history of lumbar discopathy with subsequent chronic pain. Following high volume lumbar ESPB, the patient became unconscious at the 3rd minute with seizures lasting 25 minutes. Epidural spread may be common in patients with a history of spinal surgery, leading to exaggerated response at low volumes. Also, revascularisation and anatomic changes may increase the risk of intravascular injection.
Defining block failure in lumbar ESPB is as difficult as it is for thoracal ESPB7 as the success of interfascial plane blocks depends on the volume of LA. For example, while 15–20 mL applied for lumbar spinal surgeries may lead to adequate analgesia, the same volume would be inadequate for lower abdominal and hip surgeries. As with all other interfascial plane blocks, it is also possible that adequate volume at the correct anatomical location may not lead to the expected result. In a series of 12 patients undergoing lumbar ESPB for hip and femur surgery, one patient was reported to have block failure confirmed with clinical findings.29
Sacral ESPB: A New Paradigm
Following the description of the thoracic and lumbar erector spinae plane block, sacral ESPB was defined owing to the course of ESM from the cervical area to the sacrum.10,79 Sacral ESPB was first defined as the application of LA between the multifidus and the intermediate crest that lies immediately medial to the sacral foramina in the interfascial plane. Soon after, it was described using the longitudinal midline approach.79 Both the midline approach and the original description were quickly adopted in many indications including blockage of the posterior branches of the sacral nerves,10 lumbosacral radicular pain,80 postoperative analgesia for sacral fracture81 and inferior cluneal nerve entrapment82 for the original description and anoplasty,83 gender reassignment surgery84 and possibly every indication of the caudal block for the modified longitudinal midline approach. The nomenclature of the sacral area and the anatomy of sacral ESPB is still debated. While the original describing authors state that “sonographic image was synonymous with the retrolaminar area rather than the transverse process”, sacral retrolaminar block is also used in accordance with Hamilton’s suggestion.12
Although cadaveric and radiological demonstration of LA spread has not yet been demonstrated, it is obvious that the midline approach can be an alternative to caudal block and that the original technique may play an important role in pain management.
Concerns and Further Debate
The effectiveness of lumbar ESPB for pain management and postoperative pain has been shown in clinical studies. Anatomic studies evaluating the spread of LA generally used 20 mL volumes and did not spread anterior to the transverse process. However, clinicians’ observations are that lumbar ESPB is similar to lumbar plexus block and that LA spreads to the epidural space through the transforaminal route. Even in studies of thoracic ESPB the spread of LA, its pathway and volume-spread relationship have yet to be put forward. These points must also be topics for further research.
In lumbar ESPB, although the transverse process may appear to be an anatomic barrier to the point of LA application, it minimizes the risk of damaging vascular and/or neural structures, although this minimum risk does not completely rule out safety issues. Although rare, motor weakness, motor block, and local anesthesia toxicity are serious complications that have been reported. The LA volume-spread relationship, differing spread at differing levels, and blood concentration/time relationship of LA are some features of lumbar ESPB that need further evaluation.
Conclusion
Lumbar ESPB has taken its place in literature not only as an effective method for pain management but for postoperative pain management, especially improving analgesia quality when added to multimodal analgesia. Lumbar ESPB is a safe, effective, and easy to apply method that is sure to be the subject of many randomized controlled trials, comparative studies, cadaveric and anatomic studies.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chin KJ, McDonnell JG, Carvalho B, et al. Essentials of our current understanding: abdominal wall blocks. Reg Anesth Pain Med. 2017;42:133–183. doi:10.1097/AAP.0000000000000545
2. FitzGerald S, Odor PM, Barron A, Pawa A. Breast surgery and regional anaesthesia. Best Pract Res Clin Anaesthesiol. 2019;33:95–110. doi:10.1016/j.bpa.2019.03.003
3. El-Boghdadly K, Elsharkawy H, Short A, Chin KJ. Quadratus lumborum block nomenclature and anatomical considerations. Reg Anesth Pain Med. 2016;41:548–549. doi:10.1097/AAP.0000000000000411
4. Chin KJ, Adhikary SD, Forero M. Erector Spinae Plane (ESP) block: a new paradigm in regional anesthesia and analgesia. Curr Anesthesiol Rep. 2019;1–10.
5. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41:621–627. doi:10.1097/AAP.0000000000000451
6. Huang W, Wang W, Xie W, Chen Z, Liu Y. Erector spinae plane block for postoperative analgesia in breast and thoracic surgery: a systematic review and meta-analysis. J Clin Anesth. 2020;66:109900. doi:10.1016/j.jclinane.2020.109900
7. Tulgar S, Ahiskalioglu A, De Cassai A, Gurkan Y. Efficacy of bilateral erector spinae plane block in the management of pain: current insights. J Pain Res. 2019;12:2597–2613. doi:10.2147/JPR.S182128
8. Tulgar S, Senturk O. Ultrasound guided Erector Spinae Plane block at L-4 transverse process level provides effective postoperative analgesia for total hip arthroplasty. J Clin Anesth. 2018;44:68. doi:10.1016/j.jclinane.2017.11.006
9. Hamadnalla H, Elsharkawy H, Shimada T, et al. Cervical erector spinae plane block catheter for shoulder disarticulation surgery. Can J Anaesth. 2019;66:1129–1131. doi:10.1007/s12630-019-01421-9
10. Tulgar S, Senturk O, Thomas DT, Deveci U, Ozer Z. A new technique for sensory blockage of posterior branches of sacral nerves: ultrasound guided sacral erector spinae plane block. J Clin Anesth. 2019;57:129–130.
11. Paulsen F, Böckers TM, Waschke J. Sobotta Anatomy Textbook: English Edition with Latin Nomenclature. Elsevier Health Sciences; 2018.
12. Hamilton DL. The erector spinae plane block: time for clarity over anatomical nomenclature. J Clin Anesth. 2020;62:109699. doi:10.1016/j.jclinane.2020.109699
13. De Cassai A, Andreatta G, Bonvicini D, et al. Injectate spread in ESP block: a review of anatomical investigations. J Clin Anesth. 2020;61:109669. doi:10.1016/j.jclinane.2019.109669
14. Kose HC, Kose SG, Thomas DT. Lumbar versus thoracic erector spinae plane block: similar nomenclature, different mechanism of action. J Clin Anesth. 2018;48:1. doi:10.1016/j.jclinane.2018.03.026
15. Aksu C, Gürkan Y. Aksu approach for lumbar erector spinae plane block for pediatric surgeries. J Clin Anesth. 2018;54:74–75.
16. Cesur S, Yayik AM, Öztürk F, Ahiskalioğlu A. Does ‘Aksu approach’ make erector spinae plane block technique easier? J Clin Anesth. 2019;55:142–143. doi:10.1016/j.jclinane.2019.01.010
17. Tulgar S, Unal OK, Thomas DT, Ozer Z. A novel modification to ultrasound guided lumbar erector spinae plane block: Tulgar approach. J Clin Anesth. 2019;56:30–31. doi:10.1016/j.jclinane.2019.01.016
18. Ip VHY, Sondekoppam RV, Özelsel TJP. Evaluating the success of Erector Spinae Plane block: believing is seeing? J Clin Anesth. 2019;57:5–6. doi:10.1016/j.jclinane.2019.02.021
19. Elkoundi A, Chouikh C, Baite A, et al. Successful erector spinae plane block without ultrasound guidance in a severely cardiovascular compromised patient. J Clin Anesth. 2019;53:50. doi:10.1016/j.jclinane.2018.10.002
20. Vadera HK, Mistry T. Erector spinae plane block: anatomical landmark-guided technique. Saudi J Anaesth. 2019;13:268–269. doi:10.4103/sja.SJA_780_18
21. Tulgar S, Selvi O, Senturk O, Serifsoy TE, Thomas DT. Ultrasound-guided Erector Spinae Plane block: indications, complications, and effects on acute and chronic pain based on a single-center experience. Cureus. 2019;11:e3815.
22. Aksu C, Gurkan Y. Defining the indications and levels of Erector Spinae Plane block in pediatric patients: a retrospective study of our current experience. Cureus. 2019. doi:10.7759/cureus.5348
23. Kinjo S, Schultz A. Continuous lumbar erector spinae plane block for postoperative pain management in revision hip surgery: a case report. Rev Bras Anestesiol. 2019;69:420–422. doi:10.1016/j.bjane.2019.02.002
24. Dey S, Mistry T, Mittapalli J, Neema PK. Landmark guided continuous erector spinae plane block: an adjunct for perioperative analgesia in a patient with difficult back operated for total hip arthroplasty. Saudi J Anaesth. 2020;14:276–277.
25. Darling CE, Pun SY, Caruso TJ, Tsui BCH. Successful directional thoracic erector spinae plane block after failed lumbar plexus block in hip joint and proximal femur surgery. J Clin Anesth. 2018;49:1–2. doi:10.1016/j.jclinane.2018.05.002
26. Darling CE, Lin C, Caruso TJ, Tsui BCH. Lumbar erector spinae plane catheter via a thoracic approach for iliac crest autograft in a pediatric patient. J Clin Anesth. 2019;54:164–165. doi:10.1016/j.jclinane.2018.12.008
27. Neal JM, Barrington MJ, Fettiplace MR, et al. The Third American Society of Regional Anesthesia and pain medicine practice advisory on local anesthetic systemic toxicity. Reg Anesth Pain Med. 2018;43:113–123. doi:10.1097/AAP.0000000000000720
28. Alici HA, Ahiskalioglu A, Aydin ME, Ahiskalioglu EO, Celik M. High volume single injection lumbar erector spinae plane block provides effective analgesia for lower extremity herpes zoster. J Clin Anesth. 2019;54:136–137. doi:10.1016/j.jclinane.2018.11.009
29. Tulgar S, Selvi O, Senturk O, et al. Clinical experiences of ultrasound-guided lumbar erector spinae plane block for hip joint and proximal femur surgeries. J Clin Anesth. 2018;47:5–6. doi:10.1016/j.jclinane.2018.02.014
30. Chung K, Kim ED. Continuous erector spinae plane block at the lower lumbar level in a lower extremity complex regional pain syndrome patient. J Clin Anesth. 2018;48:30–31. doi:10.1016/j.jclinane.2018.04.012
31. Balaban O, Aydın T. Lumbar erector spinae plane catheterization for continuous postoperative analgesia in total knee arthroplasty: a case report. J Clin Anesth. 2019;55:138–139. doi:10.1016/j.jclinane.2018.12.017
32. Celik M, Tulgar S, Ahiskalioglu A, Alper F. Is high volume lumbar erector spinae plane block an alternative to transforaminal epidural injection? Evaluation with MRI. Reg Anesth Pain Med. 2019;44(9):906–907. doi:10.1136/rapm-2019-100514
33. De Lara González SJ, Pomés J, Prats-Galino A, et al. Anatomical description of anaesthetic spread after deep erector spinae block at L-4. Rev Esp Anestesiol Reanim. 2019;66:409–416. doi:10.1016/j.redar.2019.07.001
34. Harbell MW, Seamans DP, Koyyalamudi V, Kraus MB, Craner RC, Langley NR. Evaluating the extent of lumbar erector spinae plane block: an anatomical study. Reg Anesth Pain Med. 2020. doi:10.1136/rapm-2020-101523
35. Selvi O, Tulgar S. Ultrasound guided erector spinae plane block as a cause of unintended motor block. Rev Esp Anestesiol Reanim. 2018. doi:10.1016/j.redar.2018.05.009
36. Takahashi H, Suzuki T. Erector spinae plane block for low back pain in failed back surgery syndrome: a case report. JA Clin Rep. 2018;4:60. doi:10.1186/s40981-018-0198-6
37. Tulgar S, Ermis MN, Ozer Z. Combination of lumbar erector spinae plane block and transmuscular quadratus lumborum block for surgical anaesthesia in hemiarthroplasty for femoral neck fracture. Indian J Anaesth. 2018;62:802–805. doi:10.4103/ija.IJA_230_18
38. Brandão J, Graça R, Sá M, Cardoso JM, Caramelo S, Correia C. Lumbar erector spinae plane block: successful control of acute pain after lumbar spine surgery - A clinical report. Rev Esp Anestesiol Reanim. 2018. doi:10.1016/j.redar.2018.10.005
39. Santonastaso DP, De Chiara A, Kraus E, et al. Ultrasound guided erector spinae plane block: an alternative technique for providing analgesia after total hip arthroplasty surgery? Minerva Anestesiol. 2019;85:801–802. doi:10.23736/S0375-9393.19.13459-1
40. Canturk M. Ultrasound-guided bilateral lumbar erector spinae plane block for postoperative analgesia after spondylolisthesis correction surgery. J Clin Anesth. 2019;57:77–78. doi:10.1016/j.jclinane.2019.03.015
41. Canturk M. Lumbar erector spinae plane block for postoperative analgesia after nephrectomy followed by emergent complication surgery. Minerva Anestesiol. 2019;85:1032–1033. doi:10.23736/S0375-9393.19.13663-2
42. Canturk M, Canturk FK. Ultrasound-guided bilateral lumbar erector spinae plane block for postoperative analgesia after myomectomy with Pfannenstiel incision. J Clin Anesth. 2020;59:40–41.
43. Canturk M. Ultrasound-guided lumbar erector spinae plane block: a new alternative for the treatment of post-herniorrhaphy neuralgia. J Clin Anesth. 2019;58:128–129. doi:10.1016/j.jclinane.2019.07.009
44. Wu X, Yang L. Quadratus lumborum and modified Erector Spinae Plane (QLESP) block: a single-puncture technique for total hip arthroplasty. J Clin Anesth. 2020;61:109643. doi:10.1016/j.jclinane.2019.109643
45. Canturk M. Ultrasound-guided lumbar erector spinae plane block: the sole anesthetic method for emergent strangulated inguinal herniorrhaphy for a patient on anticoagulant treatment. J Clin Anesth. 2020;61:109685. doi:10.1016/j.jclinane.2019.109685
46. Kumar A, Mistry T, Gupta N, Kumar V, Bhatnagar S. Lumbar Erector Spine plane block for pain management in postherpetic neuralgia in a patient with chronic lymphocytic leukemia. Indian J Palliat Care. 2020;26:134–136. doi:10.4103/IJPC.IJPC_134_19
47. Sirohiya P, Yadav P, Bharati SJ, Sushma B. Unfolding role of Erector Spinae Plane block for the management of chronic cancer pain in the palliative care unit. Indian J Palliat Care. 2020;26:142–144. doi:10.4103/IJPC.IJPC_188_19
48. Barrios A, Julio Camelo MD, Jorge Gómez MD, et al. Evaluation of sensory mapping of Erector Spinae Plane block. Pain Physician. 2020;23:E289–E296.
49. Nielsen TD, Moriggl B, Barckman J, et al. Cutaneous anaesthesia of hip surgery incisions with iliohypogastric and subcostal nerve blockade: a randomised trial. Acta Anaesthesiol Scand. 2019;63:101–110. doi:10.1111/aas.13221
50. Elkoundi A, Eloukkal Z, Bensghir M, Belyamani L. Priapism following erector spinae plane block for the treatment of a complex regional pain syndrome. Am J Emerg Med. 2019;37(4):
51. Schwartz RH, Urits I, Viswanath O, Kaye AD, Eskander J. Extended pain relief utilizing lumbar Erector Spinae Plane block in a patient with discogenic low back pain. Pain Physician. 2019;22:E519–E521.
52. Karaca O, Pinar HU. Is high dose lumbar erector spinae plane block safe? J Clin Anesth. 2020;62:109721. doi:10.1016/j.jclinane.2020.109721
53. Piraccini E, Corso RM, Maitan S. Ultrasound guided erector spinae plane block for myofascial pain syndrome. J Clin Anesth. 2019;57:121.
54. Fusco P, De Paolis V, De Sanctis F, et al. The association of erector spinae plane block and ultrasound guided dry needling could be a winning strategy for long-term relief of chronic musculoskeletal pain. Minerva Anestesiol. 2019;85:1138–1139. doi:10.23736/S0375-9393.19.13575-4
55. Piraccini E, Calli M, Taddei S, et al. Erector spinae plane block for myofascial pain syndrome: only a short-term relief? Minerva Anestesiol. 2020;86:888–890. doi:10.23736/S0375-9393.20.14523-1
56. Aksu C, Gürkan Y. Opioid sparing effect of Erector Spinae Plane block for pediatric bilateral inguinal hernia surgeries. J Clin Anesth. 2018;50:62–63. doi:10.1016/j.jclinane.2018.06.048
57. Gürkan Y, Aksu C. Iliac crest bone graft donor site analgesia: a new indication for erector spinae plane block. Can J Anaesth. 2019;66:338–339. doi:10.1007/s12630-018-01276-6
58. Aksu C, Şen MC, Akay MA, Baydemir C, Gürkan Y. Erector Spinae Plane Block vs Quadratus Lumborum Block for pediatric lower abdominal surgery: a double blinded, prospective, and randomized trial. J Clin Anesth. 2019;57:24–28. doi:10.1016/j.jclinane.2019.03.006
59. Kline J, Chin KJ. Modified dual-injection lumbar erector spine plane (ESP) block for opioid-free anesthesia in multilevel lumbar laminectomy. Korean J Anesthesiol. 2019;72:188–190. doi:10.4097/kja.d.18.00289
60. Schwartz RH, Urits I, Viswanath O, et al. Successful combination of thoracodorsal interfascial plane block and erector spinae pain block for peri-operative pain control after lumbar laminectomy. J Clin Anesth. 2020;62:109705. doi:10.1016/j.jclinane.2020.109705
61. Ueshima H, Inagaki M, Toyone T, Otake H. Efficacy of the Erector Spinae Plane block for lumbar spinal surgery: a retrospective study. Asian Spine J. 2018. doi:10.31616/asj.2018.0114
62. Yayik AM, Cesur S, Ozturk F, et al. Postoperative analgesic efficacy of the ultrasound-guided Erector Spinae Plane block in patients undergoing lumbar spinal decompression surgery: a randomized controlled study. World Neurosurg. 2019;126:e779–e785. doi:10.1016/j.wneu.2019.02.149
63. Cesur S, Yayik AM, Ozturk F, Ahiskalioglu A. Ultrasound-guided low thoracic Erector Spinae Plane block for effective postoperative analgesia after lumbar surgery: report of five cases. Cureus. 2018;10:e3603.
64. Elkoundi A, Bentalha A, Kettani SE-CE, Mosadik A, Koraichi AE. Erector spinae plane block for pediatric hip surgery -a case report. Korean J Anesthesiol. 2019;72:68–71. doi:10.4097/kja.d.18.00149
65. Bugada D, Zarcone AG, Manini M, Lorini LF. Continuous Erector Spinae Block at lumbar level (L4) for prolonged postoperative analgesia after hip surgery. J Clin Anesth. 2019;52:24–25. doi:10.1016/j.jclinane.2018.08.023
66. Munshey F, Caruso TJ, Wang EY, Tsui BCH. Programmed intermittent bolus regimen for Erector Spinae Plane blocks in children: a retrospective review of a single-institution experience. Anesth Analg. 2018. doi:10.1213/ANE.0000000000003817
67. Tulgar S, Selvi O, Şentürk Ö, Özer Z, Ünal ÖK, Thomas DT. The Maltepe combination: novel parasacral interfascial plane block and lumbar erector spinae plane block for surgical anesthesia in transfemoral knee amputation. J Clin Anesth. 2019;57:95–96.
68. Singh S, Ranjan R, Lalin D. A new indication of erector spinae plane block for perioperative analgesia is total hip replacement surgery - A case report. Indian J Anaesth. 2019;63:310–311. doi:10.4103/ija.IJA_25_19
69. Ayub A, Talawar P, Gupta SK, Kumar R, Alam A. Erector spinae plane block: a safe, simple and effective alternative for knee surgery. Anaesth Intensive Care. 2019;47:469–471. doi:10.1177/0310057X19877655
70. Tulgar S, Selvi O, Şentürk Ö, Özer Z, Ünal ÖK, Thomas DT. Comparison of ultrasound-guided lumbar Erector Spinae Plane block and transmuscular quadratus lumborum block for postoperative analgesia in hip and proximal femur surgery: a prospective randomized feasibility study. Anesth Essays Res. 2018;12:825–831.
71. Cesur S, Ay AN, Yayık AM, Naldan ME, Gürkan Y. Ultrasound-guided erector spinae plane block provides effective perioperative analgesia and anaesthesia for thoracic mass excision: a report of two cases. Anaesth Crit Care Pain Med. 2018. doi:10.1016/j.accpm.2018.01.002
72. Ahiskalioglu A, Tulgar S, Celik M, et al. Lumbar Erector Spinae Plane block as a main anesthetic method for hip surgery in high risk elderly patients: initial experience with a magnetic resonance imaging. Eur J Med. 2020;52:16–20. doi:10.5152/eurasianjmed.2020.19224
73. Aydin T, Turgut M, Balaban O. Ultrasound guided bi-level thoracic and lumbar erector spinae plane block as surgical anaesthesia method for inguinal hernia repair in a high-risk patient: case report. Indian J Anaesth. 2019;63:957–959. doi:10.4103/ija.IJA_440_19
74. Abdelnasser A, Zoheir H, Rady A, Ramzy M, Abdelhamid BM. Effectiveness of ultrasound-guided erector spinae plane block for postoperative pain control in hip replacement surgeries; A pilot study. J Clin Anesth. 2020;62:109732. doi:10.1016/j.jclinane.2020.109732
75. Restrepo-Garces CE, Urrego J, Mejia-Loaiza C, Giraldo L. The erector spinae plane block for radicular pain during pregnancy. Int J Obstet Anesth. 2019;39:143–144. doi:10.1016/j.ijoa.2019.02.009
76. Ueshima H. Pneumothorax after the erector spinae plane block. J Clin Anesth. 2018;48:12. doi:10.1016/j.jclinane.2018.04.009
77. Sullivan TR, Kanda P, Gagne S, Costache I. Harlequin syndrome associated with Erector Spinae Plane block. Anesthesiology. 2019;131:665. doi:10.1097/ALN.0000000000002733
78. De Cassai A, Fasolo A, Geraldini F, Munari M. Motor block following bilateral ESP block. J Clin Anesth. 2020;60:23.
79. Aksu C, Gürkan Y. Sacral Erector Spinae Plane Block with longitudinal midline approach: could it be the new era for pediatric postoperative analgesia? J Clin Anesth. 2019;59:38–39. doi:10.1016/j.jclinane.2019.06.007
80. Piraccini E, Antioco M, Maitan S. Ultrasound guided sacral erector spinae plane block: a useful tool for radicular pain treatment. J Clin Anesth. 2019;59:11–12. doi:10.1016/j.jclinane.2019.06.011
81. Kilicaslan A, Aydin A, Kekec AF, Ahiskalioglu A. Sacral erector spinae plane block provides effective postoperative analgesia for pelvic and sacral fracture surgery. J Clin Anesth. 2020;61:109674. doi:10.1016/j.jclinane.2019.109674
82. Tulgar S, Selvi O, Thomas DT, Ozer Z. ESRA19-0505 New indication for novel block: sacral erector spinae plane block for inferior cluneal/sacral nerve entrapment syndrome. E-Poster Viewing Abstracts. 2019. doi:10.1136/rapm-2019-esraabs2019.408
83. Öksüz G, Arslan M, Bilal B, Gişi G, Yavuz C. Ultrasound guided sacral erector spinae block for postoperative analgesia in pediatric anoplasty surgeries. J Clin Anesth. 2020;60:88. doi:10.1016/j.jclinane.2019.08.006
84. Kukreja P, Deichmann P, Selph JP, Hebbard J, Kalagara H. Sacral Erector Spinae Plane Block for gender reassignment surgery. Cureus. 2020;12:e7665.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.