")
Back to Archived Journals » International Journal of Clinical Transfusion Medicine » Volume 8
Anemia in Pediatric Critical Care
Authors Jutras C, Charlier J , François T , Du Pont-Thibodeau G
Received 3 July 2020
Accepted for publication 25 September 2020
Published 30 October 2020 Volume 2020:8 Pages 23—33
DOI https://doi.org/10.2147/IJCTM.S229764
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Cees Th. Smit Sibinga
Camille Jutras, Julien Charlier, Tine François, Geneviève Du Pont-Thibodeau
Department of Pediatrics, Division of Pediatric Critical Care Medicine, CHU Sainte-Justine, Montréal, Québec, Canada
Correspondence: Geneviève Du Pont-Thibodeau; Julien Charlier
Department of Pediatrics, Division of Pediatric Critical Care Medicine, CHU Sainte-Justine, Montréal, Québec, Canada
Tel +1 514-345-4931 ext. 5553
Email [email protected]; [email protected]
Abstract: Anemia is a common complication of pediatric critical illness; close to 75% of children that are admitted to the pediatric intensive care unit (PICU) are anemic at some point during their stay. The causes of anemia of critical illness are multifactorial and are most often attributable to inflammation and/or blood losses (iatrogenic or disease-related). The impact of anemia in critically ill children is unclear but given that hemoglobin is an important factor in the body’s oxygen-carrying capacity, low hemoglobin can result in insufficient oxygen delivery to vital organs and tissues especially in the context of an acute illness. The management of anemia of critical illness is yet to be developed. Transfusions of red blood cells are the fastest way to increase hemoglobin; however, they are associated with adverse events. Current recommendations suggest limiting transfusions to hemoglobin levels below 7g/dL in hemodynamically stabilized children. Iron and erythropoietin have been investigated to manage and/or prevent anemia; yet studies on these two therapeutic options have been either negative or inconclusive. Another approach to reduce or prevent anemia is to reduce blood testing and iatrogenic blood losses. Multiples strategies have shown promising results, such as small-volume phlebotomy, in-line blood testing and modifying physician behavior with regard to blood testing orders. Further studies are required to determine how efficient these interventions are to reduce the prevalence of anemia at PICU discharge. Anemia is a significant complication of critical illness and 50% of children are discharged from the PICU anemic. The long-term impact of this complication on these children is unknown, in particular the impact on their long-term neurocognitive development. Structured follow-up is required to understand the trajectory and consequences of anemia in this particular population.
Keywords: anemia, pediatric, critical care, management
Epidemiology and Pathophysiology
Definition
Anemia is a medical condition during which the number of red blood cells (RBCs) and consequently, the body’s oxygen-carrying capacity is insufficient to meet the body’s physiologic needs. Most of the definitions of anemia currently available are based on a hemoglobin cut-off level which varies with age. However, there is no universal definition for anemia and the cut-off values vary a lot depending on the reference. Furthermore, these definitions are not adapted to the characteristics of specific populations (for example, patients with cyanotic congenital heart disease) and they do not incorporate physiological component in the diagnosis (tachycardia, fatigue, etc.). This lack of a standardized definition has been a problem for clinicians and researchers. One definition that is commonly used is the World Health Organization (WHO) criteria for anemia is presented in Table 1.1 Still, this definition does not include cut-off values for diagnosis of anemia in infants less than 6 months old.
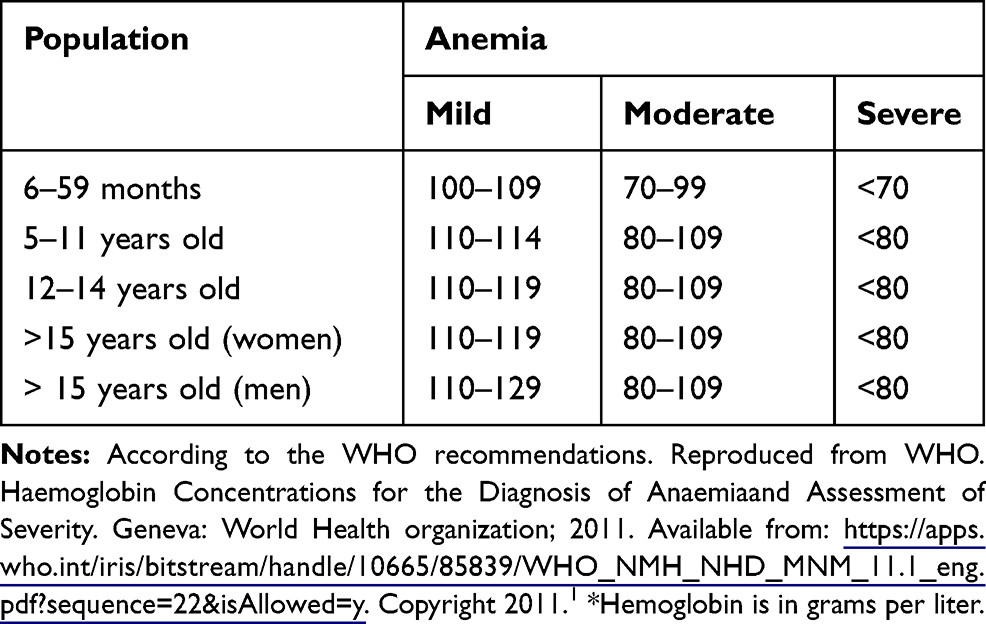 |
Table 1 Diagnosis of Anemia According to the Hemoglobin Level* |
Epidemiology
Anemia is common in critically ill children; indeed, close to 33% of children admitted to the pediatric intensive care (PICU) are anemic on admission and an additional 41% will become anemic during their PICU stay. Overall, close to 75% of children are anemic at some point during their critical illness.2 Children most at risk of developing anemia in the PICU are newborns (<28 days of age), those admitted with shock or with severity disease defined by a baseline Pediatric Logistic Organ Dysfunction score (PELOD)3 of ≥11, a respiratory comorbid condition and children who do not receive a RBC transfusion during their first two days in the PICU.2
Pathophysiology
Anemia of critical illness is multifactorial in origin. It can be caused by inflammation and insufficient erythropoiesis, blood loss, reduced lifespan of RBC (and cytolysis), and/or hemodilution; inflammation and blood losses being important contributors.4
Inflammation
Inflammation is an important component of pediatric critical illness. It causes a mild to moderate normocytic, normochromic anemia. It is characterized by decreased erythropoiesis, an abnormal iron metabolism and a decreased production and response to erythropoietin (EPO).5 Anemia of inflammation is intrinsically associated with iron metabolism which is greatly disturbed during systemic inflammation.6 Under normal circumstances, the major regulators of iron absorption are: 1) body iron stores, 2) bone marrow erythropoietic activity, 3) hemoglobin level, 4) hypoxia, and 5) inflammation.7 Most of the body’s iron is stored in the reticuloendothelial system, RBCs, macrophages and hepatocytes. Normally, iron is transported by transferrin, then binds to receptors on the surface of erythroblasts and is used for hemoglobin synthesis. In excess, iron can also bind to apoferritin to form ferritin; an iron-storing protein. Hepcidin is a regulator of iron absorption: it is a circulating polypeptide that inhibits the iron exporter ferroportin. Activation of hepcidin results in the retention of iron within enterocytes, macrophages and hepatocytes leading to a decrease in serum iron levels, even if there is no depletion of body iron store.8 During inflammation, interleukin-6 (IL-6) stimulates the synthesis of hepcidin which decreases iron absorption and iron availability.4 Interleukin-1 (IL-1) and Tumor Necrosis Factor (TNF) alpha also stimulate the synthesis of ferritin, the major protein associated with iron storage further reducing iron availability. Inflammation thus reduces erythropoiesis by limiting available iron for hemoglobin synthesis.8 TNF-alpha and IL-1 also reduce erythropoiesis and response to EPO by inducing the apoptosis of medullar erythrocyte progenitors, inhibiting the production of EPO by the kidney and downregulating EPO receptors.4,9
Blood Loss
Blood loss in critically ill patients can be secondary to the primary illness (surgery, acute bleeding from trauma, or digestive bleeding) or it can be the result of iatrogenic procedures and/or blood sampling. Excessive blood testing in the ICU has become a recognized contributor to anemia of critical illness.2,10 ICU patients require close monitoring, and this can include repetitive and sometimes excessive blood testing. In 1986, Burnum first reported the problem of “medical vampires”, describing the urge of medical teams to perform excessive blood testing on ICU patients to ensure adequate monitoring.11 Despite a growing concern for excessive blood testing, practices have not changed much over the past 30 years.11–13 Average daily blood volume sampled per ICU patient ranges from 13.5 to 88 mL.14,15 In PICU, daily blood volume sample ranges from 2.3 to 7.1 mLper patient.16–19 The amount of daily blood volume removed for testing is especially concerning in small children given their size and their blood volume. The estimated total blood volume of infants is about 80–85mL/kg. For a 3-kg baby, a 5mL daily blood loss for 5 days represents about 10% of his blood volume. Excessive blood testing is costly, can cause or worsen iatrogenic anemia and increases the need for RBC transfusions.20,21
The acute impact of anemia on critically ill children is unclear. Hemoglobin is an important factor in the body’s oxygen-carrying capacity. In the acute setting, low hemoglobin can result in insufficient oxygen delivery to vital organs and tissues. If oxygen delivery falls below a certain critical hemoglobin level, it can cause cells to enter in anaerobic metabolism which leads to lactic acid production and ultimately to end-organ failure and death. Increased cardiac output can counterbalance for lower oxygen delivery to a certain extent but this compensatory mechanism can be compromised in the context of an ongoing critical illness.22 The level of anemia at which oxygen delivery is impaired is thus dependent on each patient’s intrinsic physiological condition and risk factors. Consequently, it is unclear whether the WHO hemoglobin criteria can be safely applied to the PICU population given the complexity of PICU children’s underlying conditions. The development of guidelines for management of anemia in these children is therefore more challenging.
Management of Anemia
Many therapeutic options have been investigated to help prevent and/or treat anemia of critical illness. These include RBC transfusions, iron and EPO.
Transfusion
The theoretical goal of administering a RBC transfusion to PICU patients is to rapidly restore the body’s oxygen-carrying capacity, respond to physiologic needs, end anaerobic metabolism and improve organ function. In clinical settings, physicians usually prescribe RBC transfusions to patients with low hemoglobin, acute blood loss and/or cardiac insufficiency.2 Although it is compelling to believe that RBC transfusion improves the homeostasis and outcomes of acutely ill patients, the literature suggests that RBC transfusions can, on the contrary, be associated with worst outcomes in certain clinical scenarios.
First, in the adult population, numerous studies have demonstrated that transfusing RBCs may not be risk-free. In 1997, Hebert et al published in a retrospective manner, a study looking at the association between transfusion practices and mortality rate. Compared to survivors, patients who died were transfused RBC more frequently (42.6 vs 28.0% p <0.001).21–23 The number of RBC transfusions administered was also associated with worse outcomes; adjusted odd ratio predicting survival was 0.61 after having received 1 to 3 units of blood and 0.49 after having received 4 to 6 units of blood when compared to non-transfused anemic patients.24 The CRIT (Anemia and Blood Transfusion in the Critically Ill) study, by Corwin et al in 2004, demonstrated that the number of RBC transfusions received by ICU adults was directly associated with longer ICU stay and an increased mortality.25 RBC transfusions are also associated with more nosocomial infections. The risk of nosocomial infection increases with each additional RBC transfusion.26 A systematic review of 45 studies investigating the efficacy of RBC transfusion in 272,596 critically ill adults demonstrated that in 42 of the 45 studies, the risks of RBC transfusion exceeded their benefits.27 This review also highlighted that RBC transfusions were an independent risk factor for mortality, infection, multi-organ dysfunction syndrome and acute respiratory distress syndrome.27 Pediatric data show similar results; RBC transfusions are associated with higher mortality, higher rates of nosocomial infections and more cardiac and respiratory dysfunction. RBC transfusions are also associated with longer PICU stay and longer duration of mechanical ventilation.2 Furthermore, children have twice the rate of transfusion reactions than adults (278 vs 577 per 100,000, p< 0.001).28 Transfusion reactions are significant and can include infections, allergic transfusion reactions, fluid overload and transfusion-related acute lung injury.29,30
Adverse outcomes associated with RBC transfusions have forced clinicians to reevaluate indications for transfusion. The safety of lowering hemoglobin thresholds to avoid transfusions has since then been thoroughly investigated. The randomized controlled trial (RCT) TRICC (A Multicenter, RCT of Transfusion Requirements in Critical Care) by Hebert et al, randomized ICU adults to receive a RBC transfusion at a hemoglobin threshold of 7g/dL (restrictive strategy) versus 9g/dL (liberal strategy). The restrictive strategy allowed a reduction in RBC transfusions of 54% which was not associated with worst outcomes. There was even a trend towards reduction of mortality (18.7% in the restrictive group vs 23.3% in the liberal group p.011).23 Villanueva et al demonstrated a reduction in mortality in adults with upper GI bleed using a restrictive approach (Hb <7g/dL).31 The TRISS (Transfusion Requirements in Septic Shock) trial showed that there was no difference in mortality using a restrictive approach for patients in septic shock (Hb <7g/dL).32
In 2007, the TRIPICU (Transfusion Requirements in Pediatric Intensive Care) trial by Lacroix et al was conducted in PICU patients. Children were randomized to a restrictive hemoglobin threshold of 7g/dL vs standard of care. Only hemodynamically stabilized children were included. The results demonstrated a 44% reduction in RBC transfusion in the restrictive group; 54% of patients in this group did not receive any RBC transfusion during their PICU stay. On the opposite, 98% of patients in the liberal or standard of care group received a RBC transfusion. This restrictive strategy was not associated with new or progressive multiple organ dysfunction syndrome (MODS).33 This pediatric landmark study demonstrated the safety of tolerating lower hemoglobin thresholds and has since then created a significant shift in the way PICU physicians prescribe transfusions. They are now much more cautious when deciding to transfuse patients.34
In 2019, RBC transfusion recommendations for critically ill children were developed by the Transfusion and Anemia Expertise Initiative.35 Some of the key points of these recommendations are the following:
- Consider not only the hemoglobin level but also the global clinical status (signs and symptoms, laboratory results, physiologic values …) of the patient when deciding to transfuse RBC.
- RBC transfusion is recommended for critically ill children if the hemoglobin level is <5g/dL.
- For most patients who are hemodynamically stable and who have a hemoglobin level >7g/dL, the experts recommend no administration of RBC transfusion.
Iron
Iron-deficiency appears to contribute in part to the pathophysiology of anemia of critical illness.36 Administering iron to critically ill patients has been proposed as a promising treatment option. Yet, concerns were raised about the added risk of infection associated with iron therapy. In in vivo and in vitro studies, intravenous (IV) iron was associated with increased levels of circulating free iron, which impairs T cell and neutrophil function and promotes the growth of pathogens. The blunted erythropoietic response due to co-existing inflammation in these patients can also exacerbate iron overload and lead to an increased risk of infection.37 Moreover, IV iron is not without risk; allergic and anaphylactic reactions, oxidative damage and iron overload have been reported.38
Numerous ICU studies have investigated the role of iron supplementation to treat anemia of critical illness. The IRONMAN randomized controlled trial (RCT) randomized ICU adults with a hemoglobin concentration below 10g/dL to receive IV iron or placebo. IV iron or placebo was administered to a maximum of 4 doses depending on the hemoglobin concentration and the iron and transferrin levels.39 There was no significant difference between the number of RBC transfusions administered in each group during the ICU stay. However, hemoglobin at discharge was significantly higher in the IV iron group compared to placebo (10.7 vs 10.0 g/dL p= 0.02). There was no difference in the rate of infections in both groups. The authors concluded that IV iron therapy was not effective to avoid RBC transfusions in critically ill patients likely because of their underlying severe inflammation and blunted erythropoietic response preventing iron to be used for hemoglobin synthesis.39 Similar results were also obtained by Pierraci et al in the trauma population. In this trial, iron (or placebo) was given for 2 weeks to trauma patients with hemoglobin level <12g/dL. While iron supplementation led to an increase in the serum ferritin concentration, it did not change the requirements for RBC transfusions.40 Recently, Shah et al published a systematic review with meta-analysis on iron therapy in ICU. It included 6 RCTs for a total of 805 patients. They found no evidence of an effect of iron supplementation on the number of participants requiring a transfusion. There was also no difference between IV or oral iron. Iron therapy did, however, increase mean hemoglobin concentration. There was no difference in the rate of infections in patients who received iron vs placebo.37
The contribution of iron deficiency to the pathogenesis of anemia of critical illness needs to be better understood. Hepcidin and the soluble transferrin receptor (sTfR) are novel biomarkers that could help identify anemic patients with true absolute underlying iron deficiency from those with sole inflammation (i.e. functional iron deficiency). As mentioned above, hepcidin is a circulating polypeptide that inhibits the iron exporter ferroportin. Its activation results in the retention of iron within enterocytes, macrophages and hepatocytes leading to a decrease in serum iron levels even if there is no depletion of body iron store. Hepcidin expression is increased in the context of inflammation but reduced during iron deficiency. Soluble transferrin receptor (sTfR) is a soluble form of the membrane receptor derived from its proteolysis that is expressed on the cell surfaces. Its concentration is inversely correlated with intracellular iron levels and is less affected by inflammation and more affected by erythropoiesis.41,42 These markers may also help identify those patients that could positively respond to iron therapy.9,36,43 A nested study from the IRONMAN trial was performed to answer this question. In patients with low hepcidin (<53), iron was associated with a reduction of the risk of receiving a RBC transfusion (RR 0.48, CI 0.26–0.85). In patients with a high hepcidin level, there was no association between IV iron therapy and the risk of RBC transfusion.44 These results support the use of hepcidin as a biomarker to guide our therapy for ICU patients, but further studies are needed to consolidate this new knowledge.
Currently, it is not recommended to administer iron to PICU children to treat or prevent anemia. This recommendation may change as we learn more about the role of hepcidin in the pathogenesis of anemia of critical illness.
EPO
Another potential treatment option for anemia of critical illness is EPO. Anemia of critical illness is characterized by a blunted EPO production and abnormalities in iron metabolism. Critically ill patients have lower circulating EPO and a blunted response to endogenous EPO, likely as a result of the inhibition of the EPO gene by inflammatory mediators.4 Anemia of critical illness is mainly one of underproduction.45,46 EPO supplementation has already been proven effective in treatment of anemia secondary to renal failure or in patients with cancer.47,48 Given that the pathophysiology of anemia of critical illness shares similar origins with the anemia of chronic illness, EPO supplementation during critical illness could appear as a promising therapeutic option. However, current data do not support this theory. Results of studies on EPO treatment during critical illness are very difficult to interpret and generalize. For instance, the EPO protocols developed in these projects were very different; some studies administering EPO IV, others subcutaneously, or in combination with oral or IV iron.46 This makes it almost impossible to develop a solid meta-analysis and draw conclusions. Furthermore, concerns were raised about the possible severe adverse events associated to EPO administration such as thrombosis, blood hyperviscosity, hypertension, convulsions and red-cell aplasia.46
Corwin et al published a RCT looking at the effects of EPO on transfusion requirements in the ICU. Participants received EPO (or placebo) weekly for a maximum of four doses. Patients in the EPO group were less likely to receive RBC transfusions (50.5% vs 60.4% p=0.01). There was a 19% reduction in RBC transfusion in the EPO group and hemoglobin concentration at the end of the study was significantly higher in the EPO group (13.2 vs 9.4 g/dL, p< 0.01). There was no difference in mortality or adverse clinical events.49 These results were encouraging so further studies were designed to better evaluate the safety of this therapeutic option. In 2007, Corwin et al did a similar study looking at the efficacy and safety of an EPO treatment versus placebo on the need for RBC transfusion in a double-blind placebo-controlled RCT. A total of 1460 patients were randomized, and they found no statistical difference between both groups regarding the need for RBC transfusion. This could be explained, according to the authors, by changes in practice since the last studies (restrictive transfusion strategy). An interesting finding of this study is that mortality at 29 and 140 days tended to be lower in the EPO group. One hypothesis mentioned by the authors is that EPO’s effect on mortality can be related to the non-hematopoietic effect of EPO (anti-apoptotic activity, protection of cells from hypoxemia and ischemia). Adverse events were similar in the two groups except that thrombotic vascular events were more frequent in the EPO group (15.5 vs 11.5% p=0.008).50 A recent Cochrane review investigated the possible harms of EPO in ICU. Thirty-nine trials were included for a total of 945,240 participants. Results were inconclusive when looking at risk of adverse events with EPO (RR 1.05, CI 0.93–1.21) or venous thromboembolisms (RR 1.04, CI 0.7 to 1.41), but EPO seemed to decrease mortality (RR 0.76, CI 0.61 to 0.92).51
Pediatric data on EPO are scarce. One study looked at EPO therapy in children with bronchiolitis and anemia. Patients were randomized to EPO therapy with iron versus placebo with iron. They found that, in the EPO group, there was a trend towards a higher hematocrit (32 vs 34%) but there was no decrease in the number of transfusions needed. No adverse events were reported.52
EPO is probably beneficial in reducing the number of transfusions administered in the ICU but overall, benefits of EPO therapy seem marginal when a restrictive transfusion therapy is applied. As a consequence, its use is not recommended for treatment or prevention of anemia of critical illness. The impact of EPO on mortality by other mechanisms remains under investigation.
Patient Blood Management and Blood Conservation Strategies
In reaction to the emerging evidence on the risks associated with RBC transfusions and anemia, the WHO developed in 2011 the concept of a patient blood management strategy program (PBM) which is defined as a patient-focused, evidence-based and systematic approach to optimize the management of patient and transfusion of blood products for quality and effective patient care.53 This includes the development of blood conservation techniques to reduce the frequency of diagnostic blood sampling, the amount of blood removed and discarded. Restrictive transfusion strategies, early detection and management of anemia, optimizing hemostasis and coagulopathy as well as patient-centered care, are other important aspects of a PBM program.54
Over the last decade, several reviews have been published describing the best available strategies to minimize diagnostic blood loss. Strategies identified include the use of small-volume tubes or microtainers, point-of-care testing, minimizing the blood volume discarded by using closed blood sampling systems, streamlining lab orders, non-invasive monitoring, implementing blood sampling protocols, education and timely removal of unnecessary indwelling catheters.13,55–57
Small-Volume Phlebotomy
The use of small-volume phlebotomy tubes can significantly reduce the blood volume used for diagnostic blood sampling. This strategy has been shown to reduce blood losses by 30% to 45% in ICU patients. However, a difference in discharge hemoglobin using this technique failed to be demonstrated.12,20,21,58
In-Line Blood Sampling
ICU patients often have indwelling lines such as central venous catheters to administer fluids and medications, arterial lines to continuously monitor blood pressure, and sometimes dialysis catheters, all of them with the advantage of offering an easy access for blood sampling.12,59 Because of the mixing with other perfusions and the possibility of laboratory errors, a certain amount of blood volume needs to be discarded before taking a diagnostic blood sample. The discarded blood needs to be at least twice the dead space of the lumen60 and can thus represent an important percentage of the total blood volume sampled. For that reason, closed or in-line blood sampling has been shown to be an effective measure to reduce diagnostic blood loss. In 4 RCTs in ICU patients, arterial catheter conservation devices were compared to standard practice (open sampling) and all four reported a significant reduction in mean blood volume sampled per patient per day; ranging from an 18% to 80% reduction.61–64 Yet improvement in hemoglobin levels and transfusion rates with this technique failed to be demonstrated.65,66 In premature infants, in-line point-of-care (POC) monitoring system allowed for a relative reduction of 27% and 24% of total blood loss in the first and second weeks of admission67 as well as a decrease in transfusion rates.68 In children undergoing congenital heart surgery, transfusion rates were also lower using this technique (5 versus 3 units; p<0.001).69
Physician Behavior
Another strategy to spare blood volume is to modify physician behaviors in regard to blood sampling. Strategies reviewed in the literature are 1) auditing and giving feedback to the medical team about their prescription habits, 2) displaying the costs per laboratory test, 3) eliminating standing and repetitive orders.57 According to Sedrak et al, 67% to 88% of inpatient laboratory orders are unnecessary.70 Implementing educational strategies can reduce unnecessary laboratory orders;71–74 for example, removing routine postoperative complete blood count testing can reduce blood sampling by 50% within 7 days post-surgery.75 Clinical practice guidelines for blood culture use in PICU children reduces by 46% the rate of blood culture collection.76 Using blood volume discarded for blood cultures can also be considered and does not increase contamination rates.77
Finally, the timely removal of unnecessary indwelling lines can also help in reducing blood testing. In fact, the presence of indwelling central venous and arterial lines may encourage more blood sampling.59 Children with arterial or central venous lines are sampled 2.3 to 4 times more frequently in the first 2 weeks of their PICU stay than children with peripheral venous lines.2
Non-Invasive Hemoglobin Monitors
Non-invasive monitoring, such as non-invasive hemoglobin monitors, can provide valuable clinical data and help reduce the need for blood testing. This type of non-invasive measurement can also help to obtain faster results since they are not subjected to laboratory, analysis and validation delays.78 They can also be cost-effective and help avoid stressful situations for children.79,80
Non-invasive hemoglobin measurement devices such as the Radical-7 Pulse CO-Oximeter (Masimo) were developed based on the principle of spectrophotometry.78 Light is transmitted through or reflected from tissues and blood differentially depending on their biochemical variables. The difference in the degree of reflection allows for calculation of hemoglobin and hematocrit using a mathematical model.78 These measures are performed using a fingertip probe similar to a pulse oximeter sensor. These monitors also use a perfusion index (PI) to evaluate the strength of the peripheral signal. Circumstances that decrease peripheral perfusion can cause a drop in the perfusion index and reduce the quality and reliability of the signal.78
Data on the reliability of these non-invasive measurements and the extent to which they can safely replace blood testing are quite conflicting. A study performed in 53 PICU children compared non-invasive hemoglobin (SpHb) measures to laboratory measures.79 Non-invasive monitoring provided adequate agreement for the trending of hemoglobin levels with 95% of non-invasive hemoglobin readings ranging within 2.6g/dL of the corresponding laboratory hemoglobin. Nevertheless, this accuracy is insufficient to be used as the only parameter for transfusion decision or to avoid laboratory testing.79 A study in patients undergoing neurosurgery and volume expansion demonstrated that although the correlation between SpHb and laboratory hemoglobin (LabHb) was unsatisfactory (0.53; p<0.001), yet the correlation between the change in SpHb and the change in LabHb was better (0.75; p< 0.001).81 The authors of this study concluded that this monitor could be useful as a trend monitor but that it would be advisable to confirm a baseline hemoglobin level. This device also appears unreliable in cyanotic children with congenital heart disease.80
Further data are required to define the potential use of these monitors in clinical practice. The newer generation of pulse oximeter probes will need to be further investigated but may prove to be interesting solutions to decrease blood testing.80 At present, this technology is not sufficiently accurate to replace invasive measurement of hemoglobin.
Anemia at PICU Discharge and Its Long-Term Consequences
Despite all the strategies discussed above to decrease the prevalence of anemia, close to 60% of all PICU children leave the PICU anemic and the consequences of this complication have yet to be determined.82,83 Large RCTs have clearly demonstrated the safety of tolerating anemia in the short term,33,84,85 yet little is known about its effect on the long-term well-being of these children and in particular on their neurocognitive development. Anemia, in particular iron-deficiency anemia, may be associated with significant long-term abnormal neurocognitive function in children. Large studies, in otherwise healthy pre-school children, have shown the detrimental effect of anemia on their cognitive development and intelligence quotient.86,87 Deficiency in iron can impact the function of several iron-dependent enzymes that are active in the brain, which are responsible for the synthesis, transformation and degradation of important neurotransmitters.88 This can lead to behavioral, attention and developmental deficits.89–91 Whether this condition is reversible with iron therapy is unclear.92,93 Anemia can also contribute to many other health problems in PICU survivors; cardiovascular responses can be blunted and exercise tolerance is lower mainly because of depleted cardiac reserve.94 Anemia has also been associated with poorer quality of life, fatigue and muscular weakness in ICU survivors.95,96
It is uncertain whether the anemia of PICU survivors is only caused by iron deficiency and/or chronic systemic inflammation. Data in children are lacking. However, we do know that adult ICU survivors remain in a persistent state of systemic inflammation even up to six months after ICU discharge as demonstrated by elevated C-reactive protein and ferritin blood levels, increased cytokine production, suppressed bone marrow activity, iron-restricted erythropoiesis and functional iron-deficiency anemia.9,36,97,98 “Functional iron deficiency” refers to a state in which iron stores are not depleted, but the body is unable to access and use iron appropriately. However, chronic inflammation might not be the only cause of anemia in adult ICU survivors: 30–40% of these patients also have low hepcidin levels, which suggests that they also have underlying true iron deficiency.96
Currently, there are no guidelines for the management of anemia in critically ill children at and after PICU discharge. The Canadian Pediatric Society and the Canadian Task Force on Preventive Health Care recommend screening for anemia in all high-risk groups.99 Critically ill children certainly qualify as a high-risk group; yet no standardized screening has been established for them in Canada.
It is imperative that we ascertain whether permissive anemia is also safe for children in the long term and if not, that we rapidly determine strategies for prevention and/or treatment. The lack of standardized follow-up of PICU survivors is one of the main challenges obstructing the development of research in this field. The need for PICU follow-up clinics is becoming increasingly recognized.100
Conclusion and Futures Perspectives
In summary, anemia is a common complication in critically ill children. It is caused by multiple factors including blood losses, iatrogenic sampling and inflammation. Transfusions have been the cornerstone treatment to rapidly correct anemia, but multiple studies have shown their detrimental effects. Large RCTs have demonstrated the safety of tolerating some degree of anemia while patients are critically ill thereby avoiding unnecessary exposure to RBC transfusions. Other treatment options investigated to treat anemia have included EPO and iron; yet none have shown positive results in the acute setting. Patient blood management is a new program supported by the WHO to help physicians determine strategies to reduce blood sampling and improve blood conservation strategies. This could help in decreasing the contribution of iatrogenic anemia. Non-invasive monitoring devices, although promising, need further improvement before being able to replace blood measurements.
Although anemia appears safe in the acute setting, little is known about the long-term consequences. Anemia can impact neurocognitive function in particular in young children and also affect energy levels, quality of life and physical endurance. This is a major concern given that more than 50% of children are anemic at PICU discharge. PICU follow-up studies are required to better understand the epidemiology and long-term adverse consequences of anemia after a pediatric critical illness.
Disclosure
The authors report no conflicts of interest for this work.
References
1. WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Geneva: World Health organization; 2011. Available from: https://apps.who.int/iris/bitstream/handle/10665/85839/WHO_NMH_NHD_MNM_11.1_eng.pdf?sequence=22&isAllowed=y.
2. Bateman ST, Lacroix J, Boven K, et al. Anemia, blood loss, and blood transfusions in North American children in the intensive care unit. Am J Respir Crit Care Med. 2008;178(1):26–33. doi:10.1164/rccm.200711-1637OC
3. Leteurtre S, Martinot A, Duhamel A, et al. Validation of the paediatric logistic organ dysfunction (PELOD) score: prospective, observational, multicentre study. Lancet. 2003;362(9379):192–197. doi:10.1016/S0140-6736(03)13908-6
4. Sloniewsky D. Anemia and transfusion in critically ill pediatric patients: a review of etiology, management, and outcomes. Crit Care Clin. 2013;29(2):301–317. doi:10.1016/j.ccc.2012.11.005
5. Ozier Y, Aubron C, Nguyen BV. [Hospital-acquired anemia: facts, consequences and prevention]. Transfus Clin Biol. 2016;23(4):185–191. French. doi:10.1016/j.tracli.2016.07.005
6. Prakash D. Anemia in the ICU: anemia of chronic disease versus anemia of acute illness. Crit Care Clin. 2012;28(3):333–343. doi:10.1016/j.ccc.2012.04.012
7. Behera B, Singh RI, Xess I, Mathur P, Hasan F, Misra MC. Candida rugosa: a possible emerging cause of candidaemia in trauma patients. Infection. 2010;38(5):387–393. doi:10.1007/s15010-010-0044-x
8. Darveau M, Denault AY, Blais N, Notebaert E. Bench-to-bedside review: iron metabolism in critically ill patients. Crit Care. 2004;8(5):356–362. doi:10.1186/cc2862
9. Lasocki S, Baron G, Driss F, et al. Diagnostic accuracy of serum hepcidin for iron deficiency in critically ill patients with anemia. Intensive Care Med. 2010;36(6):1044–1048. doi:10.1007/s00134-010-1794-8
10. Demaret P, Loeckx I, Mulder A, Devos P, Lebrun F. [Anemia in the critically ill child and adult: a narrative review]. Rev Med Liege. 2014;69(1):26–34. French.
11. Burnum JF. Medical vampires. N Engl J Med. 1986;314(19):1250–1251. doi:10.1056/NEJM198605083141910
12. Smoller BR, Kruskall MS. Phlebotomy for diagnostic laboratory tests in adults. Pattern of use and effect on transfusion requirements. N Engl J Med. 1986;314(19):1233–1235. doi:10.1056/NEJM198605083141906
13. Whitehead NS, Williams LO, Meleth S, et al. Interventions to prevent iatrogenic anemia: a Laboratory Medicine Best Practices systematic review. Critical Care. 2019;23(1):278. doi:10.1186/s13054-019-2511-9
14. Packer ME, Thorne CJ, Arora N. Blood sampling on the intensive care unit. Intensive Care Med. 2014;40(1):S262–S3.
15. Liniewska G, Melvin JR, Becker B, Mosher BD, Morrison CA, Kepros JP. Iatrogenic blood loss in the ICU. Chest Conference: CHEST. 2010;138:4.
16. Johnson A, Hoch A, Bateman S, Valentine S. Reducing phlebotomy-induced blood loss in the PICU: a quality improvement study. Critical Care Med. 2015;43(12):200. doi:10.1097/01.ccm.0000474624.94468.91
17. Valentine SL, Bateman ST. Identifying factors to minimize phlebotomy-induced blood loss in the pediatric intensive care unit. Pediatr Crit Care Med. 2012;13(1):22–27. doi:10.1097/PCC.0b013e318219681d
18. Nexo E, Christensen NC, Olesen H. Volume of blood removed for analytical purposes during hospitalization of low-birthweight infants. Clin Chem. 1981;27(5):759–761. doi:10.1093/clinchem/27.5.759
19. Bushell LC, Hewson M. Phlebotomy practice at wellington NICU-a retrospective audit. J Paediatrics Child Health. 2014;50:73.
20. Foulke GE, Harlow DJ. Effective measures for reducing blood loss from diagnostic laboratory tests in intensive care unit patients. Crit Care Med. 1989;17(11):1143–1145. doi:10.1097/00003246-198911000-00008
21. Dolman HS, Evans K, Zimmerman LH, et al. Impact of minimizing diagnostic blood loss in the critically ill. Surgery. 2015;158(4):
22. Vallet B, Robin E, Lebuffe G. Venous oxygen saturation as a physiologic transfusion trigger. Crit Care. 2010;14(2):213. doi:10.1186/cc8854
23. Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med. 1999;340(6):409–417. doi:10.1056/NEJM199902113400601
24. Hebert PC, Wells G, Tweeddale M, et al. Does transfusion practice affect mortality in critically ill patients? Transfusion Requirements in Critical Care (TRICC) Investigators and the Canadian Critical Care Trials Group. Am J Respir Crit Care Med. 1997;155(5):1618–1623. doi:10.1164/ajrccm.155.5.9154866
25. Corwin HL, Gettinger A, Pearl RG, et al. The CRIT Study: anemia and blood transfusion in the critically ill–current clinical practice in the United States. Crit Care Med. 2004;32(1):39–52. doi:10.1097/01.CCM.0000104112.34142.79
26. Taylor RW, Manganaro L, O’Brien J, Trottier SJ, Parkar N, Veremakis C. Impact of allogenic packed red blood cell transfusion on nosocomial infection rates in the critically ill patient. Crit Care Med. 2002;30(10):2249–2254. doi:10.1097/00003246-200210000-00012
27. Marik PE, Corwin HL. Efficacy of red blood cell transfusion in the critically ill: a systematic review of the literature. Crit Care Med. 2008;36(9):2667–2674. doi:10.1097/CCM.0b013e3181844677
28. Vossoughi S, Perez G, Whitaker BI, Fung MK, Stotler B. Analysis of pediatric adverse reactions to transfusions. Transfusion. 2018;58(1):60–69. doi:10.1111/trf.14359
29. Tyrrell CT, Bateman ST. Critically ill children: to transfuse or not to transfuse packed red blood cells, that is the question. Pediatr Crit Care Med. 2012;13(2):204–209. doi:10.1097/PCC.0b013e318219291c
30. Francois T, Emeriaud G, Karam O, Tucci M. Transfusion in children with acute respiratory distress syndrome. Ann Transl Med. 2019;7(19):511. doi:10.21037/atm.2019.08.28
31. Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med. 2013;368(1):11–21. doi:10.1056/NEJMoa1211801
32. Holst LB, Haase N, Wetterslev J, et al. Lower versus higher hemoglobin threshold for transfusion in septic shock. N Engl J Med. 2014;371(15):1381–1391. doi:10.1056/NEJMoa1406617
33. Lacroix J, Hebert PC, Hutchison JS, et al. Transfusion strategies for patients in pediatric intensive care units. N Engl J Med. 2007;356(16):1609–1619.
34. Du Pont-Thibodeau G, Tucci M, Ducruet T, Lacroix J. Survey on stated transfusion practices in PICUs*. Pediatr Crit Care Med. 2014;15(5):409–416. doi:10.1097/PCC.0000000000000121
35. Valentine SL, Bembea MM, Muszynski JA, et al. Consensus recommendations for RBC transfusion practice in critically ill children from the pediatric critical care transfusion and anemia expertise initiative. Pediatr Crit Care Med. 2018;19(9):884–898. doi:10.1097/PCC.0000000000001613
36. Shah A, Wray K, James T, et al. Serum hepcidin potentially identifies iron deficiency in survivors of critical illness at the time of hospital discharge. Br J Haematol. 2018.
37. Shah A, Fisher SA, Wong H, et al. Safety and efficacy of iron therapy on reducing red blood cell transfusion requirements and treating anaemia in critically ill adults: a systematic review with meta-analysis and trial sequential analysis. J Crit Care. 2019;49:162–171. doi:10.1016/j.jcrc.2018.11.005
38. Muñoz M, Breymann C, García-Erce JA, Gómez-Ramírez S, Comin J, Bisbe E. Efficacy and safety of intravenous iron therapy as an alternative/adjunct to allogeneic blood transfusion. Vox Sang. 2008;94(3):172–183. doi:10.1111/j.1423-0410.2007.01014.x
39. Litton E, Baker S, Erber WN, et al. Intravenous iron or placebo for anaemia in intensive care: the IRONMAN multicentre randomized blinded trial: a randomized trial of IV iron in critical illness. Intensive Care Med. 2016;42(11):1715–1722. doi:10.1007/s00134-016-4465-6
40. Pieracci FM, Stovall RT, Jaouen B, et al. A multicenter, randomized clinical trial of IV iron supplementation for anemia of traumatic critical illness*. Crit Care Med. 2014;42(9):2048–2057. doi:10.1097/CCM.0000000000000408
41. Uijterschout L, Swinkels DW, Akkermans MD, et al. The value of soluble transferrin receptor and hepcidin in the assessment of iron status in children with cystic fibrosis. J Cyst Fibros. 2014;13(6):639–644. doi:10.1016/j.jcf.2014.03.007
42. Lee EJ, Oh EJ, Park YJ, Lee HK, Kim BK. Soluble transferrin receptor (sTfR), ferritin, and sTfR/log ferritin index in anemic patients with nonhematologic malignancy and chronic inflammation. Clin Chem. 2002;48(7):1118–1121.
43. Girelli D, Nemeth E, Swinkels DW. Hepcidin in the diagnosis of iron disorders. Blood. 2016;127(23):2809–2813. doi:10.1182/blood-2015-12-639112
44. Litton E, Baker S, Erber W, et al. Hepcidin predicts response to IV iron therapy in patients admitted to the intensive care unit: a nested cohort study. J Intensive Care. 2018;6:60. doi:10.1186/s40560-018-0328-2
45. Corwin HL. The role of erythropoietin therapy in the critically ill. Transfus Med Rev. 2006;20(1):27–33. doi:10.1016/j.tmrv.2005.08.002
46. Lacroix J, Toledano B. Erythropoietin for critically ill children. Pediatr Crit Care Med. 2003;4(1):123–124. doi:10.1097/00130478-200301000-00029
47. Cody JD, Hodson EM. Recombinant human erythropoietin versus placebo or no treatment for the anaemia of chronic kidney disease in people not requiring dialysis. Cochrane Database Syst Rev. 2016;1.
48. Tonia T, Mettler A, Robert N, et al. Erythropoietin or darbepoetin for patients with cancer. Cochrane Database Syst Rev. 2012;12:Cd003407.
49. Corwin HL, Gettinger A, Pearl RG, et al. Efficacy of recombinant human erythropoietin in critically ill patients: a randomized controlled trial. JAMA. 2002;288(22):2827–2835. doi:10.1001/jama.288.22.2827
50. Corwin HL, Gettinger A, Fabian TC, et al. Efficacy and safety of epoetin alfa in critically ill patients. N Engl J Med. 2007;357(10):965–976. doi:10.1056/NEJMoa071533
51. Mesgarpour B, Heidinger BH, Roth D, Schmitz S, Walsh CD, Herkner H. Harms of off-label erythropoiesis-stimulating agents for critically ill people. Cochrane Database Syst Rev. 2017;8(8):Cd010969.
52. Jacobs BR, Lyons K, Brilli RJ. Erythropoietin therapy in children with bronchiolitis and anemia. Pediatr Crit Care Med. 2003;4(1):44–48. doi:10.1097/00130478-200301000-00008
53. World Health Organization. Global Forum for Blood Safety: Patient Blood Management Dubai 2011 [Available from: https://www.who.int/bloodsafety/events/gfbs_01_pbm_concept_paper.pdf?ua=1.
54. Sullivan HC, Roback JD. The pillars of patient blood management: key to successful implementation (Article, p2840). Transfusion 2019;59(9):2763–2767. doi:10.1111/trf.15464
55. Hayden SJ, Albert TJ, Watkins TR, Swenson ER. Anemia in critical illness: insights into etiology, consequences, and management. Am J Respir Crit Care Med. 2012;185(10):1049–1057. doi:10.1164/rccm.201110-1915CI
56. Siegal DM, Manning N, Jackson CNL, Hillis CM, Heddle NM. Devices to reduce the volume of blood taken for laboratory testing in ICU patients: a systematic review. J Intensive Care Med. 2018;885066618810374.
57. Eaton KP, Levy K, Soong C, et al. Evidence-based guidelines to eliminate repetitive laboratory testing. JAMA Intern Med. 2017;177(12):1833–1839. doi:10.1001/jamainternmed.2017.5152
58. Kurniali PC, Curry S, Brennan KW, et al. A retrospective study investigating the incidence and predisposing factors of hospital-acquired anemia. Anemia. 2014;2014:634582. doi:10.1155/2014/634582
59. Low LL, Harrington GR, Stoltzfus DP. The effect of arterial lines on blood-drawing practices and costs in intensive care units. Chest. 1995;108(1):216–219. doi:10.1378/chest.108.1.216
60. Rickard CM, Couchman BA, Schmidt SJ, Dank A, Purdie DM. A discard volume of twice the dead space ensures clinically accurate arterial blood gases and electrolytes and prevents unnecessary blood loss. Crit Care Med. 2003;31(6):1654–1658. doi:10.1097/01.CCM.0000063448.98777.EF
61. Gleason E, Grossman S, Campbell C. Minimizing diagnostic blood loss in critically ill patients. Am J Crit Care. 1992;1(1):85–90. doi:10.4037/ajcc1992.1.1.85
62. Peruzzi WT, Parker MA, Lichtenthal PR, Cochran-Zull C, Toth B, Blake M. A clinical evaluation of a blood conservation device in medical intensive care unit patients. Crit Care Med. 1993;21(4):501–506. doi:10.1097/00003246-199304000-00007
63. Harber CR, Sosnowski KJ, Hegde RM. Highly conservative phlebotomy in adult intensive care–a prospective randomized controlled trial. Anaesth Intensive Care. 2006;34(4):434–437. doi:10.1177/0310057X0603400414
64. MacIsaac CM, Presneill JJ, Boyce CA, Byron KL, Cade JF. The influence of a blood conserving device on anaemia in intensive care patients. Anaesth Intensive Care. 2003;31(6):653–657. doi:10.1177/0310057X0303100607
65. Thorpe S, Thomas AN. The use of a blood conservation pressure transducer system in critically ill patients. Anaesthesia. 2000;55(1):27–31. doi:10.1046/j.1365-2044.2000.01129.x
66. Mukhopadhyay A, See KC, Chan YH, Yip HS, Phua J. Effect of a blood conservation device in patients with preserved admission haemoglobin in the intensive care unit. Anaesth Intensive Care. 2011;39(3):426–430. doi:10.1177/0310057X1103900313
67. Widness JA, Kulhavy JC, Johnson KJ, et al. Clinical performance of an in-line point-of-care monitor in neonates. Pediatrics. 2000;106(3):497–504. doi:10.1542/peds.106.3.497
68. Mahieu L, Marien A, De Dooy J, Mahieu M, Mahieu H, Van Hoof V. Implementation of a multi-parameter Point-of-Care-blood test analyzer reduces central laboratory testing and need for blood transfusions in very low birth weight infants. Clin Chim Acta. 2012;413(1–2):325–330.
69. Weber CF, Gorlinger K, Meininger D, et al. Point-of-care testing: a prospective, randomized clinical trial of efficacy in coagulopathic cardiac surgery patients. Anesthesiology. 2012;117(3):531–547. doi:10.1097/ALN.0b013e318264c644
70. Sedrak MS, Patel MS, Ziemba JB, et al. Residents’ self-report on why they order perceived unnecessary inpatient laboratory tests. J Hosp Med. 2016;11(12):869–872. doi:10.1002/jhm.2645
71. Sadowski BW, Lane AB, Wood SM, Robinson SL, Kim CH. High-value, cost-conscious care: iterative systems-based interventions to reduce unnecessary laboratory testing. Am J Med. 2017;130(9):1112e1- e7. doi:10.1016/j.amjmed.2017.02.029
72. Vidyarthi AR, Hamill T, Green AL, Rosenbluth G, Baron RB. Changing resident test ordering behavior: a multilevel intervention to decrease laboratory utilization at an academic medical center. Am J Med Qual. 2015;30(1):81–87. doi:10.1177/1062860613517502
73. Newman DB, Siontis KC, Chandrasekaran K, Jaffe AS, Kashiwagi DT. Intervention to reduce inappropriate ionized calcium ordering practices: a quality-improvement project. Perm J. 2015;19(1):49–51. doi:10.7812/TPP/14-108
74. Calderon-Margalit R, Mor-Yosef S, Mayer M, Adler B, Shapira SC. An administrative intervention to improve the utilization of laboratory tests within a university hospital. Int J Qual Health Care. 2005;17(3):243–248.
75. Dewan M, Galvez J, Polsky T, et al. Reducing unnecessary postoperative complete blood count testing in the pediatric intensive care unit. Perm J. 2017;21:16–051.
76. Woods-Hill CZ, Fackler J, Nelson McMillan K, et al. Association of a clinical practice guideline with blood culture use in critically ill children. JAMA Pediatr. 2017;171(2):157–164.
77. Dwivedi S, Bhalla R, Hoover DR, Weinstein MP. Discarding the initial aliquot of blood does not reduce contamination rates in intravenous-catheter-drawn blood cultures. J Clin Microbiol. 2009;47(9):2950–2951. doi:10.1128/JCM.00292-09
78. Joseph B, Haider A, Rhee P. Non-invasive hemoglobin monitoring. Int J Surg. 2016;33(Pt B):254–257. doi:10.1016/j.ijsu.2015.11.048
79. Phillips MR, Khoury AL, Bortsov AV, et al. A noninvasive hemoglobin monitor in the pediatric intensive care unit. J Surg Res. 2015;195(1):257–262. doi:10.1016/j.jss.2014.12.051
80. Kamel MM, Hasanin A, Nawar B, et al. Evaluation of noninvasive hemoglobin monitoring in children with congenital heart diseases. Paediatr Anaesth. 2020;30(5):571–576. doi:10.1111/pan.13851
81. Park YH, Lee JH, Song HG, Byon HJ, Kim HS, Kim JT. The accuracy of noninvasive hemoglobin monitoring using the radical-7 pulse CO-Oximeter in children undergoing neurosurgery. Anesth Analg. 2012;115(6):1302–1307. doi:10.1213/ANE.0b013e31826b7e38
82. Demaret P, Karam O, Tucci M, et al. Anemia at pediatric intensive care unit discharge: prevalence and risk markers. Ann Intensive Care. 2017;7(1):107. doi:10.1186/s13613-017-0328-8
83. Demaret P, Valla FV, Behal H, et al. Anemia at discharge from the PICU: a bicenter descriptive study. Pediatr Crit Care Med. 2019;20(9):e400–e9. doi:10.1097/PCC.0000000000002015
84. Doctor A, Cholette JM, Remy KE, et al. Recommendations on RBC transfusion in general critically ill children based on hemoglobin and/or physiologic thresholds from the pediatric critical care transfusion and anemia expertise initiative. Pediatr Crit Care Med. 2018;19(9S Suppl 1):S98–S113. doi:10.1097/PCC.0000000000001590
85. Cholette JM, Swartz MF, Rubenstein J, et al. Outcomes using a conservative versus liberal red blood cell transfusion strategy in infants requiring cardiac operation. Ann Thorac Surg. 2017;103(1):206–214. doi:10.1016/j.athoracsur.2016.05.049
86. Ai Y, Zhao SR, Zhou G, Ma X, Liu J. Hemoglobin status associated with performance IQ but not verbal IQ in Chinese preschool children. Pediatr Int. 2012;54(5):669–675. doi:10.1111/j.1442-200X.2012.03648.x
87. Yang L, Liu JM, Ye RW, Hong SX, Zheng JC, Ren AG. [Correlation on hemoglobin concentration and the development of cognition among pre-school children]. Zhonghua Liu Xing Bing Xue Za Zhi. 2010;31(4):389–393. Chinese.
88. Dallman PR. Biochemical basis for the manifestations of iron deficiency. Annu Rev Nutr. 1986;6:13–40. doi:10.1146/annurev.nu.06.070186.000305
89. Yager JY, Hartfield DS. Neurologic manifestations of iron deficiency in childhood. Pediatr Neurol. 2002;27(2):85–92. doi:10.1016/S0887-8994(02)00417-4
90. Dallman PR. Manifestations of iron deficiency. Semin Hematol. 1982;19(1):19–30.
91. Patel R, Sabat S, Kanekar S. Imaging manifestations of neurologic complications in anemia. Hematol Oncol Clin North Am. 2016;30(4):733–756. doi:10.1016/j.hoc.2016.03.002
92. Logan S, Martins S, Gilbert R. Iron therapy for improving psychomotor development and cognitive function in children under the age of three with iron deficiency anaemia. Cochrane Database Syst Rev. 2001;(2):CD001444.
93. Wang B, Zhan S, Gong T, Lee L. Iron therapy for improving psychomotor development and cognitive function in children under the age of three with iron deficiency anaemia. Cochrane Database Syst Rev. 2013;(6):CD001444.
94. Kapoor RK, Kumar A, Chandra M, Misra PK, Sharma B, Awasthi S. Cardiovascular responses to treadmill exercise testing in anemia. Indian Pediatr. 1997;34(7):607–612.
95. Walsh TS, Wyncoll DL, Stanworth SJ. Managing anaemia in critically ill adults. BMJ. 2010;341:c4408. doi:10.1136/bmj.c4408
96. Lasocki S, Chudeau N, Papet T, et al. Prevalence of iron deficiency on ICU discharge and its relation with fatigue: a multicenter prospective study. Crit Care. 2014;18(5):542. doi:10.1186/s13054-014-0542-9
97. Bateman AP, McArdle F, Walsh TS. Time course of anemia during six months follow up following intensive care discharge and factors associated with impaired recovery of erythropoiesis. Crit Care Med. 2009;37(6):1906–1912. doi:10.1097/CCM.0b013e3181a000cf
98. Walsh TS, Salisbury LG, Merriweather JL, et al. Increased hospital-based physical rehabilitation and information provision after intensive care unit discharge: the RECOVER randomized clinical trial. JAMA Intern Med. 2015;175(6):901–910.
99. Abdullah K, Zlotkin S, Parkin P, et al. Iron-deficiency anemia in children. Canadian Paediatric Surveillance Program. 2011. Available from: https://www.cpsp.cps.ca/uploads/publications/RA-iron-deficiency-anemia.pdf. Accessed September 1st 2020.
100. Needham DM, Davidson J, Cohen H, et al. Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders’ conference. Crit Care Med. 2012;40(2):502–509. doi:10.1097/CCM.0b013e318232da75
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.