")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Anemia and Associated Factors Among Adults with Human Immune Deficiency Virus on Antiretroviral Therapy in Public Health Facilities of Kembata Tembaro Zone, Southern Ethiopia: A Cross-Sectional Study
Authors Mengistu A , Egata G, Hawulte B , Markos M , Lolaso T
Received 21 April 2020
Accepted for publication 3 July 2020
Published 13 August 2020 Volume 2020:12 Pages 341—349
DOI https://doi.org/10.2147/HIV.S259259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Abrham Mengistu,1 Gudina Egata,2 Behailu Hawulte,3 Melese Markos,4 Tsegaye Lolaso5
1Department of Public Health, College of Medicine and Health Science, Wachemo University, Hosaena, Ethiopia; 2School of Public Health, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 3School of Public Health, College of Health and Medical Science, Haramaya University, Harar, Ethiopia; 4Department of Public Health, College of Health Science, Dire Dawa University, Dire Dawa, Ethiopia; 5School of Public Health, College of Health Science and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Correspondence: Abrham Mengistu Tel +251-913-356-995
Email [email protected]
Background: Anemia is an independent prognostic marker of HIV/AIDS disease progression. It causes impaired physical functioning, psychological distress, poor quality-of-life, and reduces life expectancy in HIV patients. However, there is limited information in Ethiopia. Therefore, the aim of this study was to assess the magnitude of anemia and associated factors among adult HIV patients on antiretroviral therapy in public health facilities of Kembata Tembaro Zone, southern Ethiopia.
Methods: We conducted a facility-based cross-sectional study. A total of 401 HIV patients attending antiretroviral therapy nested in five health facilities were included in the analysis. Simple random sampling was employed using medical record number to select study units. Data were collected using pretested and structured questionnaire, anthropometric measurements were taken, and a drop of capillary blood was collected to determine hemoglobin level by HemoCue 301 analyzer. Clinical related data were collected from patient medical records by using a structured checklist. The collected data were coded and entered into EpiData version 3.1 and exported to SPSS version 20 for analysis. Logistic regression analysis was carried out to identify factors associated with anemia and statistical tests were declared significant at a P-value< 0.05.
Results: The magnitude of anemia among adults HIV patients attending ART was 26.2%, 95% CI=21.7– 30.4. Being female (AOR=2.06, 95% CI=1.02– 4.16), body mass index < 18.5 Kg/m2 (AOR=2.28, 95% CI=1.09– 4.78), Zidovudine use (AOR=3.71, 95% CI=1.9– 7.26), having had an opportunistic infection (AOR=5.46, 95% CI=1.67– 17.7), and WHO stage III or IV (AOR=5.71, 95% C=2.68– 12.14) were significantly associated with the occurrence of anemia.
Conclusion: Anemia was found to be a moderate public health problem among ART attendants in the current study area. Thus, early detection and intervention targeting Zidovudine users, females, patients having body mass index < 18.5 Kg/m2, patients having opportunistic infections, and patients having clinical WHO stage III or IV disease is vital to reduce the magnitude of anemia and its consequences.
Keywords: anemia, BMI, HIV, ART, Zidovudine, Kembata Tembaro, adults
Introduction
Anemia is a condition in which the number of red blood cells and consequently their oxygen-carrying capacity are insufficient to meet the body’s physiologic needs.1 It remains a significant public health challenge, affecting 1.93 billion people worldwide, or 27% of the world’s population, in 2013.2 This disorder is particularly common among infants, preschool-aged children, young women, and older people, but it can occur at any age and in any region.3 It is also one of the most commonly observed hematological abnormalities among HIV patients and is a strong prognostic marker of disease progression.4,7
Multiple factors cause anemia, including nutritional deficiencies, infections, blood loss, and inherited or acquired disorders that affect hemoglobin synthesis.1,8,10 Among HIV patients on antiretroviral therapy (ART), anemia is mostly due to impaired hematopoiesis, opportunistic infections or malignancies, therapeutic agents, autoimmune phenomena, or malabsorption of vitamins and other nutrients, which may contribute independently or synergistically to impaired erythropoiesis and altered coagulation mechanisms. These abnormalities are severe in late-stage AIDS patients with high viremia but can be corrected by highly active antiretroviral therapy.6,8,10,12
Hematological complications like anemia, leukopenia, thrombocytopenia, and sometimes pancytopenia, including bone marrow dysplasia, have been documented to be the second-most-common causes of life-threatening conditions and strong independent predictors of morbidity, poor clinical outcomes, and mortality in HIV-infected individuals.10 Untreated anemia may lead to impaired physical functioning, psychological distress, poor quality-of-life, and accelerated disease progression, and is a strong prognostic marker for death.5,7,11
Previous studies conducted in Ethiopia reported the magnitude of anemia among adult HIV patients on ART ranges from 23–43.5%.13,20 Being female, illiterate, or ART naïve; having a history of taking anti-TB treatment; taking a Zidovudine (ZDV)-containing ART regimen; CD4+ T-lymphocyte count; nutritional status; body mass index (BMI); and WHO clinical stage of HIV/AIDS are important factors associated with the occurrence of anemia among adults HIV patients on ART.13,18
Despite the widely divergent socioeconomic factors that characterize HIV worldwide, the degree of clinical anemia remains an independent risk factor for predicting mortality from HIV, even upon initiation of therapy. So far, the majority of studies conducted on the magnitude of anemia targeted infants, children, and pregnant women. Very few studies have been conducted on the magnitude of anemia and its associated factors among HIV patients on ART, and none explicitly identified in Kembata Tembaro Zone. Therefore, this study assessed the magnitude of anemia and associated factors among HIV patients on ART attending public health facilities of Kembata Tembaro Zone, southern Ethiopia.
Materials and Methods
Study Design and Setting
An institution-based cross-sectional study design was conducted in the Kembata Tembaro Zone, southern Ethiopia from March 1 to April 1, 2019. The Kembata Tembaro Zone is among the central zone in South People Nation and Nationalities Region (SNNPR). Durame is the capital of the Zone, which is 119 km from Hawassa, the capital of SNNPR and 306 km from Addis Ababa, the capital of Ethiopia. There are 136 health posts, 35 health centers, three primary hospitals, and one general hospital in the zone. There are about six public health centers and four public hospitals providing ART services in the zone. In the zone a total of 994 people living with HIV were receiving ART in public health facilities.
Inclusion and Exclusion Criteria
All adult HIV patients attending an ART clinic for care and treatment at selected public health facilities of Kembata Tembaro Zone were considered for the study. Those patients who were on treatment for anemia currently or in the last 3 months (identified through history and record review), patients having ART follow-up for less than 6 months, patients on a therapeutic feeding program taking Plumpy-Nut, recent surgical procedure or bleeding due to any reason, females on mensuration, and patients with incomplete clinical records were excluded from the study.
Sample Size Determination and Sampling Procedure
The sample size was estimated using the formula for a single population proportion, n=(zα/2)2P(1-P)/(d)2, considering the following parameters: 52.3% prevalence of anemia among HIV patients based on a similar study conducted in Arba Minch, Ethiopia,12 95% confidence level, 5% margin of error (α), 0.05 degree of precision (d), and 10% non-response rate. Hence, the total sample size was 422.
From the total of ten public health facilities providing ART service in the zone, five public health facilities were selected randomly by lottery method. Then the sample was proportionally allocated to all selected public health facilities based on the total number of client’s there. The study participants were selected from a sampling frame prepared with the list of participant’s satisfying the inclusion criteria, from patients having appointment during data collection period, and finally by using a simple random sampling technique based on a random number generated by a computer using the medical record number (MRN) used for antiretroviral therapy in each health facility.
Data Collection Methods
Data were collected by:
Interview-Administered Questionnaire
Data were collected by interview-administered methods using a structured and pre-tested questionnaire developed through extensive review of the literature.4,6,12,14 The questionnaire consists of an inquiry regarding the socio-demographic characteristics, and 24 hour recall of dietary practice.
Record Review
Data were collected by reviewing the patient’s medical record using a structured checklist developed through extensive review of the literature. The checklist consists of nutritional, clinical, and immunologic characteristics of the study participants.
Blood Collection and Hemoglobin Measurement
A capillary blood sample was collected by cleaning the ring finger with 70% ethanol, air dried and puncturing using a sterile lancet following standard operating procedures after participants had the purpose and procedure of the study expalined to them and provided consent.21,22 HemoCue® HB 301 was used to measure the level of hemoglobin by experienced medical laboratory professionals at respective health facilities following standard procedures.22
Anthropometric Measurement
Anthropometric data were collected using a calibrated weight scale and height was measured by using a portable height measuring board. To determine the BMI of study participants, weight was measured by using calibrated weight scale measurement to the nearest of 0.1 Kg and height was measured by portable height measuring board to the nearest of 0.1 cm after checking the five contact points contacted with the measuring board. Each participant was weighed with light clothes and barefoot. All anthropometric measurements were collected twice and the average value was used for analysis.23
Data Quality Control
Data were collected by trained and experienced field staff (data collectors and supervisors). The interview was conducted by experienced trained diploma Nurses. Hemoglobin and anthropometric measurement were done by trained medical laboratory professionals who were bachelor degree graduates. Data collection instruments were pre-tested on 21 (5%) participants in one of the neighboring zonal health facilities, Halaba General Hospital before actual data collection, and few modifications were made. Laboratory procedures were conducted following the standard operating procedures.
Variables and Measurements
Anemia status was determined based on the new WHO classification after the hemoglobin level was adjusted for the altitudes of each campus, sex, and smoking status. The hemoglobin levels were adjusted for altitudes accordingly. For smokers, a further hemoglobin adjustment was made by −0.03 g/dL.24 WHO cut-off levels were used for interpretations of the measured hemoglobin. Accordingly, anemia is defined as hemoglobin; <12.0 g/dL for females and <13.0 g/dL for males.24
Severity of anemia was categorized as; hemoglobin level between 11–12.9 g/dL was considered as mild anemia, 8–10.9 g/dL moderate anemia, and <8 g/dL severe anemia for males; and hemoglobin level between 11–11.9 g/dL was considered as mild anemia, 8–10.9 g/dL moderate anemia, and <8 mg/dL severe anemia for females.24
Public health significance was categorized based on the magnitude of anemia which was classified as no public health problem (<5%); mild public health problem (5–19.9%); moderate public health problem (20–39.9%); and severe public health problem (≥40%).25
Body mass index (BMI) was defined as the weight of the individual divided by the square of the same individual height in meters and classified as BMI <18.5 kg/m2 (undernutrition), BMI ≥18.5 kg/m2 (normal weight).23
Good drug adherence was when they miss less than 10% of doses, whereas poor drug adherence was when they miss greater than 10% of doses during the last 30 days.26
CD4+ T-cell count was taken from patient records and classified as <200 cells/µL and ≥200 cells/µL.
Opportunistic infections (OIs) are infections which occur or are more severe in people with weakened immune systems, which were caused by a variety of germs (bacteria, viruses, fungi, and parasites). The common OIs in HIV patients were pneumonia, salmonella infections, toxoplasmosis, and tuberculosis.26
The other independent variables include socio-demographic factors (sex, age, residence, religion, ethnicity, educational status, marital status, occupation, family size, and monthly income), clinical and nutritional factors (WHO clinical stage, ART regimens, ART type, duration of ART, history of OIs, history of malaria infection, history of parasitic infections, daily meal pattern, and dietary diversity), and behavioral factors (cigarette smoking, alcohol drinking, tea/coffee intake after meal).
Data Processing and Analysis
All filled questionnaires were checked for completeness and consistency and entered to EpiData statistical software version 3.1, then exported to the SPSS version 20 for further analysis. Descriptive statistics were used to present the frequencies, proportion, and summary statistics. Bivariate analysis was carried out to see the association of each independent variable with the anemia. Those variables with a P-value less than 0.25 were included in multivariable logistic regression analysis. Multivariable logistic regression analysis was carried out to control possible confounders and identify factors independently associated with client satisfaction with family planning service. Finally, variables with a P-value less than 0.05 in multivariable logistic regression analysis were considered as a significant association with anemia. The odds ratio was used to identify the strength of association with anemia.
Ethical Statement
Ethical clearance was obtained from Haramaya University, Institutional Health Research Ethics Review Committee (IHRERC) with reference number IHRERC/034/2019. A permission letter was obtained from Southern Nations Nationalities and Peoples Regional Health office, Kembata Tembaro Zone Health Department and studied health facilities prior to the study. Voluntary written and signed consent was obtained from each study participant after informing the objective, confidentiality, right to withdrawal, benefit, and risks of the study and that this study was conducted in accordance with the Declaration of Helsinki. Anemic and underweight patients were linked to respective health facilities for further investigation and possible intervention.
Result
Socio-Demographic Characteristics
Out of 422 study samples, 401 participants have consented and participated in the study making a response rate of 95%. More than half (59.4%) of the study participants were females and three-quarters (73.8%) were from Kambata ethnicity. The mean±SD age of the study participants were 36.1±7.6 years. More than half of the participants (58.6%) were married and 65.3% were urban residents. The mean±SD of the family size of the participants were 3.6±2. Regarding their occupation and educational level, a quarter of the participants (25.9%) were housewives and 31.4% were attending secondary level education, respectively (Table 1).
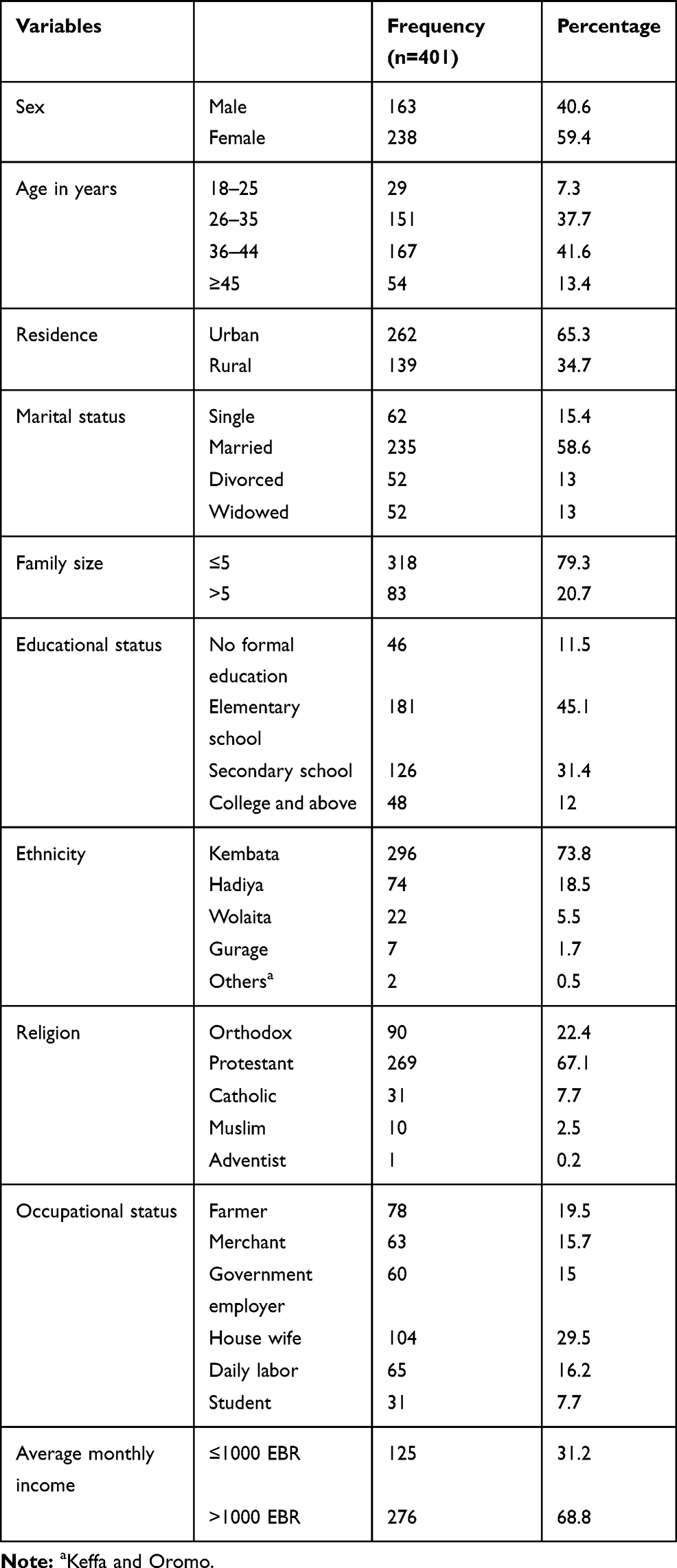 |
Table 1 Socio-Demographic Characteristics of Adult People Living with HIV on ART in Public Health Facilities of Kembata Tembaro Zone, Southern Ethiopia 2019 (n=401) |
Behavioral and Nutritional Characteristics
Concerning behavioral characteristics, 15% of the participants were currently cigarette smokers and 20% of the participants reported that they used alcohol in the past 30 days prior to the survey. One fifth of participants (19.7%) have a habit of drinking coffee or tea immediately within 30 minutes after a meal and three quarters of the respondents take all their medicines during the last 30 days.
Almost half of the respondents (50.1%) have an actual daily meal pattern of less than three times, which was below the daily recommended meal frequency for PLHIV on ART. According to a dietary diversity score assessed using nine food items on a dietary diversity scale, 59.4% of the study participants had an inadequate dietary diversity score. The majority (90.8%) of the study participants ate food items other than vitamin A rich fruits and vegetables and the least consumed food item was organ meat. One fifth (19.2%) of the study participants were underweight and 4% of the study participants were found to be overweight.
Clinical and Immunologic Characteristics
The mean±SD of CD4 T-Lymphocyte cell count of the participants was 559±239 cells/µL. The majority (94%) of the study participants had a CD4 count ≥200 cells/µL. The large proportion of the study participants (77.1%) were in a WHO clinical stage of I or II. About 93.3% of the participants were on the first line drug regimen. Regarding the ART drug adherence, 80% of the participants had good adherence or missed less than 10% of doses during the last 30 days and 91.3% had a working functional status. About 7.7% of the participants were identified with some type of opportunistic infection. The most commonly reported opportunistic infection was Pneumonia (Table 2).
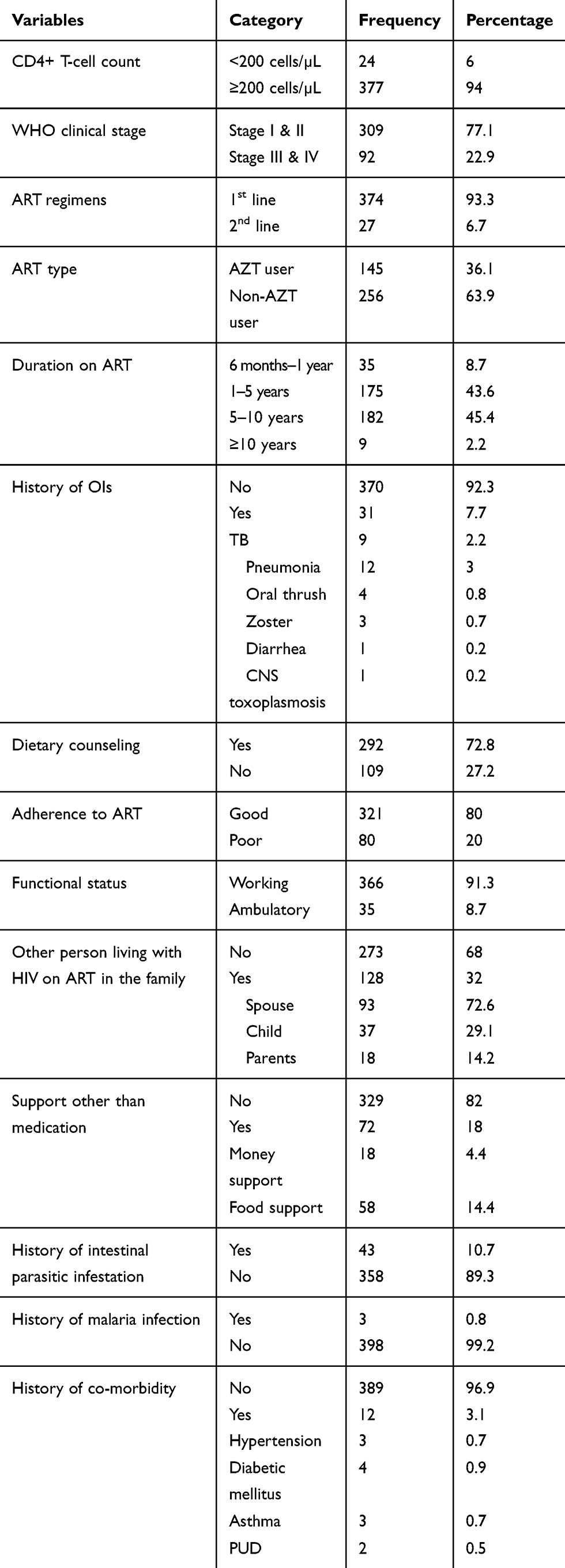 |
Table 2 Clinical and Immunologic Characteristics of Adult People Living with HIV on Antiretroviral Therapy in Public Health Facilities of Kembata Tembaro Zone, Southern Ethiopia, 2019 |
Magnitude of Anemia
The overall prevalence of anemia among HIV patients on ART was 26% (95% CI=21.7–30.4) of patients have a hemoglobin level below the normal range. The mean±SD of hemoglobin level among adult HIV patients on ART was 13.0±2.0 g/dL. The magnitude of anemia was significantly higher among females than males; 35.7% (95% CI= 29.8–42.1) among females vs 12.3% (95% CI=8.0–18.3) among males (chi-square (df)=27.61 (1), P<0.0001). The mean level of hemoglobin was 13.8±1.6 in males vs 12.45±2 in females and the difference was statistically significant (t=7.35 and P<0.001). The mean level of hemoglobin was significantly higher among WHO stage I patients (13.72±1.54) than participants on WHO stage four (10.10±1.77) (F=58.26 and P<0.0001).
Factors Associated with Anemia Among Adult People Living with HIV on ART
A total of 21 variables were considered for bivariate logistic regression and 14 variables were included in the multivariable logistic regression model. Accordingly, participants having opportunistic infection were 5-times more likely to develop anemia as compared to those with their counterpart (AOR=5.46, 95% CI=1.7–17.7). Those participants using Zidovudine containing ART drug were 4-times more likely to become anemic than users of non-Zidovudine containing ART drug (AOR=3.7, 95% CI=1.9–7.3). Females were 2-times more likely to develop anemia as compared to males (AOR=2.1, 95% CI= 1.02– 4.2). Those participants having a body mass index less than 18.5 kg/m2 were 2-times more likely to become anemic than patients having a body mass index greater than or equal to 18.5 kg/m2 (AOR=2.3, 95% CI=1.1– 4.8). Participants with advanced WHO clinical stage (III&IV) were 6-times more likely to be anemic than stage I & II (AOR=5.7, 95% CI=2.7–12.1) (Table 3).
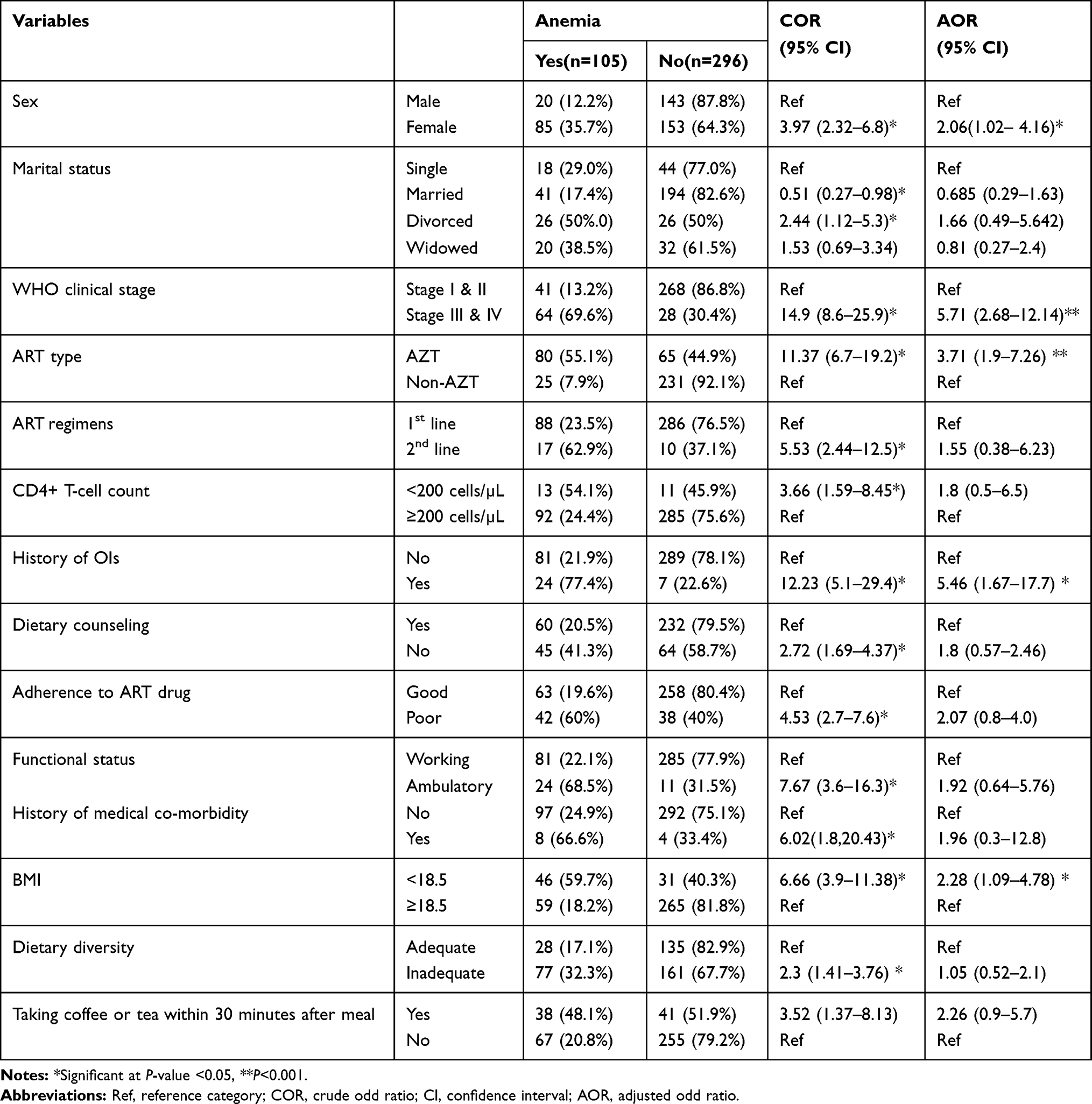 |
Table 3 Factors Associated with Anemia Among Adult People Living with HIV Taking Antiretroviral Therapy Drug in Public Health Facilities of Kembata Tembaro Zone, Southern Ethiopia, 2019 |
Discussion
In this study, the overall magnitude of anemia was found to be 26.2% (95% CI=21.7–30.4%). This indicates that anemia is a moderate public health problem in the study area. Moreover, being female, having WHO clinical stage III or IV, having a BMI less than 18.5 kg/m2, having had an opportunistic infection, and taking AZT-containing ART drugs have significant associations with anemia.
The magnitude of anemia found in this study is consistent with the findings of a systemic review of Ethiopia, which found the magnitude to be 31.0%;27 a study conducted in Gondar, North West Ethiopia (22.4%);28 and a study conducted in South Africa (25.8%).5 This study’s findings were lower than those of studies conducted in different health facilities in Ethiopia: Arba Minch (52.3%);13 Dire Dawa (41.2%);6 and Tikur Anbessa Specialized Hospital (34.6%).29 It was also lower than the findings of studies conducted in other sub-Saharan countries: Nigeria (67%),30 Benin City, Nigeria (60.16%),31 and Tanzania (70.7%).32 However, the magnitude found in the current study was higher than in studies conducted at Hawassa Referral Hospital (12.0%),7 Jimma University Hospital (16.2%),33 and Ras Desta Damtew Memorial Hospital (2.85%)34 and in Malawi (16.2%).35 The differences in the magnitude of anemia may be explained by differences in the study time, study area, and the health intervention measurement used. In addition, the differences may be due to the definition of anemia, adjustments made to hemoglobin levels for altitude and smoking, and the differences in the guidelines used for highly active ART in different settings.1
Consistent with the majority of previous studies,5,29,36 being female was strongly associated with anemia in the current study. This may be due to obstetric and gynecological factors like menses, pregnancy, and lactation. For example, during menses, the loss of iron in the menstrual blood ranges from 12.5–15.0 mg per month.37 Moreover, males are capable of storing more iron (approximately 1000 mg) than females (300–500 mg),11 leaving females at a higher risk of developing anemia than their male counterparts.
Using AZT-containing ART drugs was another factor significantly associated with the occurrence of anemia in this study. This finding was supported by studies done in South Africa,5 Tanzania,32 and Dire Dawa, Ethiopia.6 This is due to AZT’s side-effect of suppressing the erythropoiesis process in the bone marrow by inhibiting erythroid stem cells and consequently decreasing the production of reticulocyte and hemoglobin levels without hemolysis or blood loss.38
In line with the studies conducted in South Africa,5 Tanzania,32 and Dire Dawa, Ethiopia,6 this study also found that being at WHO clinical stage III or IV significantly contributed to the occurrence of anemia. This is a result of the high viral replication during the advanced stage of HIV and associated hematological abnormalities. That is, the high viral load during the late stage of the HIV leads to impaired hematopoiesis and altered coagulation mechanisms, resulting in a decline in the level of hemoglobin during this period and the development of anemia.6
In this study, having opportunistic infections also increased the risk of developing anemia. This finding was supported by study reports from South Africa5 and Arba Minch, Ethiopia.13 This is due to the immune system response to opportunistic infections which results in the release of cytokines that interfere with the body’s ability to use stored iron and absorb iron from the diet and affect the production and normal activity of the hormone erythropoietin.39
In the current study, participants with BMI less than 18.5 kg/m2 were found to be at an increased risk of developing anemia. This finding is in line with study reports from Malawi,35 South Africa,5 and Ethiopia.6,27 Lower BMI reflect undernutrition as a result of low calorie intake, poor absorption, or poor utilization of nutrients, which leads to insufficient levels of iron, folate, and vitamin B-12 for erythrocyte production. In addition, having a lower BMI increases the risk of infections, which can contribute to the occurrence of anemia.
Limitations of the Study
In this study, types of anemia, the effects of family history, menstrual disorder, cereal-based monotonous diet, and diet consumption habit was not assessed. In addition, stool examination to identify parasitic infections and blood film was not done. Furthermore, the current study did not consider acute and chronic illnesses, hereditary disorders, or infections other than opportunistic infections which may cause anemia.
Conclusion and Recommendation
The magnitude of anemia in the current study was found to be a moderate public health problem. Being female, having advanced WHO clinical stage disease III & IV, having BMI <18.5 kg/m2, developing OIs, and taking AZT containing ART drug were predictors of anemia among adults attending ART. Therefore, it is recommended that preventive strategies like nutritional education, nutritional screening, and iron supplementation should be considered targeting females, AZT containing ART drug users, advanced disease stage, and under-nourished patients. In addition, routine screening, early detection, and treatment of OI’s infection should be strengthened.
Abbreviations
ART, antiretroviral therapy; AZT, zidovudine; BMI, body mass index; IHRERC, Institutional Health Research Ethics Review Committee; MRN, medical record number; SNNPR, Southern Nations Nationalities and People Region; WHO, World Health Organization.
Data Sharing Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgment
We are thankful to the authorities of Kembata Tembaro Zonal Health Department, Kedida Gamela Health Office, Kedida Gamela Finance and Economic Development Office for supporting our project by stationary materials. Our gratitude also goes to Durame General Hospital, Shinshicho Primary Hospital, Hadaro Health Center, Damboya Health Center, Angacha Health Center. Lastly, our gratitude goes to the data collectors and supervisors.
Author Contributions
AM, GE, BH, MM, and TL: Conceived and designed the study; AM, GE, and BH: adopted data collection instrument and acquisition of data; AM, GE, BH, MM, and TL: Cleaned the data, analyzed the data, and interpreted findings; AM and BH: drafted the manuscript; AM, GE, BH, MM, and TL: critical revision and approval of the final manuscript. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. WHO, Worldwide prevalence of anaemia 1993–2005 in WHO Global Database on Anaemia. Geneva, switzerland; 2008. Available from: https://apps.who.int/iris/bitstream/handle/10665/43894/9789241596657_eng.pdf.
2. Kassebaum NJ. The Global burden of anemia. Hematol Oncol Clin North Am. 2016;30(2):247–308. doi:10.1016/j.hoc.2015.11.002
3. Sachin Pandey AS. A cross sectional study of nutritional anemia among medical students in a medical college, at bilaspur, chhattisgarh. Natl J Med Res. 2013;3(2):143–146.
4. Kumar MB, Thippeswamy T, Shankar R, Prathima C. Hematological abnormalities in early and advanced HIV infection patients. Int J Sci Study. 2016;3(11):1–5.
5. SimbarasheTakuva M, Brennan AT, IanSanne A. Anemia among HIV-infected patients initiating antiretroviral therapy in South Africa: improvement in hemoglobin regardless of degree of immunosuppression and the initiating ART regimen. J Trop Med. 2013;26(19):1–6.
6. Geleta D, Gudina E, Demissie B, Birhanu S. Prevalence of anemia and associated factors among phivs attendants antiretroviral therapy clinics in public health institutions in Dire Dawa Town, East Ethiopia. J Med Physiol Biophys. 2016;22.
7. Daka D, Lelissa D, Amsalu A. Prevalence of anaemia before and after the initiation of antiretroviral therapy at ART centre of Hawassa University Referral Hospital, Hawassa. South Ethiopia Schol J Med. 2013;3(1).
8. WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity in Vitamin and Mineral Nutrition Information System. Switzerland Geneva; 2011. Available from https://apps.who.int/iris/bitstream/handle/10665/85839/WHO_NMH_NHD_MNM_11.1_eng.pdf?ua=1.
9. Alli N, Vaughan J, Patel M. Anaemia: approach to diagnosis. Creat Commons Licence. 2017;107(1):23–27.
10. Phillips KD, Groer M. Differentiation and Treatment of Anemia in HIV Diseas. Knoxville: University of Tennessee; 2018:47–72. Available from http://trace.tennessee.edu/utk_nurspubs.
11. Sudhir ME, Jutur S, Gautam D. Hematologic Manifestations of HIV/AIDS. 2011.
12. Andamlak G, Fiseha T, Tesfay A, Kote M, Zemedu M, Tilahun T. Anemia and its associated risk factors at the time of antiretroviral therapy initiation in public health facilities of Arba Minch Town. South Ethiopia Sci Res Publishing. 2015;7:1657–1664.
13. Melese H, Mesele M, Tadesse A. Anemia among adult HIV patients in Ethiopia: a hospital-based cross-sectional study. DovePress. 2016;2017(9):25–30.
14. Ferede G, Wondimeneh Y. Prevalence and related factors of anemia in HAART-naive HIV positive patients at Gondar University Hospital, Northwest Ethiopia. BMC Blood Disord. 2013;13(1):8. doi:10.1186/2052-1839-13-8
15. Meidani M, Rezaei F, Maracy MR, Avijgan M, Tayeri K. Prevalence, severity, and related factors of anemia in HIV/AIDS patients. J Res Med Sci. 2012;17(2):138–142.
16. Zerihun KW, Bikis GA, Muhammad EA. Prevalence and associated factors of anemia among adult human immune deficiency virus positive patients on anti-retroviral therapy at Debre tabor Hospital, Northwest Ethiopia. BMC Res Notes. 2019;12(1):168. doi:10.1186/s13104-019-4214-3
17. Woldeamanuel GG, Wondimu DH. Prevalence of anemia before and after initiation of antiretroviral therapy among HIV infected patients at Black Lion Specialized Hospital, Addis Ababa, Ethiopia: a cross sectional study. BMC Hematol. 2018;18(1):7. doi:10.1186/s12878-018-0099-y
18. Gebremedhin KB, Haye TB. Factors associated with anemia among people living with HIV/AIDS taking ART in Ethiopia. J Advan Hematol. 2019;2019:8.
19. Omoregie R, Omokaro EU, Palmer O, et al. Prevalence of anaemia among HIV-infected patients in Benin City, Nigeria. Tanzan J Health Res. 2009;11:1–4. doi:10.4314/thrb.v11i1.43242
20. Tamir Z, Seid A, Haileslassie H. Magnitude and associated factors of cytopenias among antiretroviral therapy naïve human immunodeficiency virus infected adults in Dessie, Northeast Ethiopia. PLoS One. 2019;14(2):e0211708. doi:10.1371/journal.pone.0211708
21. Cheesbrough M. District Laboratory Practice in Tropical Countries Part 2.
22. Cheesbrough M. District Laboratory Practice in Tropical Countries. Part 1.
23. CDC. National Health and Nutrition Examination Survey: Anthropometry Procedures Manual, in Examination Protocol. Center for Disease Control;2009:32. Available from: https://www.cdc.gov/nchs/data/nhanes/nhanes_09_10/lab.pdf.
24. WHO, Hemoglobin concentrations for the diagnosis of anemia and assessment of severity, Vitamin and Mineral Nutrition Information System. WHO/NMH/NHD/MNM/11.1. 2011 Available from: http://www.who.int/vmnis/indicators/haemoglobin.
25. WHO. The Global Prevalence of Anaemia in 2011. Geneva, Switzerland: World Health Organization; 2015. Available from: https://apps.who.int/iris/bitstream/handle/10665/177094/9789241564960_eng.pdf?sequence=1.
26. FMOH. National Consolidated Guidelines for Comprehensive HIV Prevention, Care and Treatment. Addis Abeba; Fedral Minstry of Health; 2018:1–238. Availabe from: https://www.afro.who.int/sites/default/files/2019-04/National%20Comprehensive%20HIV%20Care%20%20Guideline%202018.pdf.
27. Negesse A, Getaneh T, Temesgen H, Taddege T, Jara D, Abebaw Z. Prevalence of anemia and its associated factors in human immuno deficiency virus infected adult individuals in Ethiopia. A systematic review and meta-analysis. BMC Hematol. 2018;18(32):1–10. doi:10.1186/s12878-018-0127-y
28. Alem M, Kena T, Baye N, Ahmed R, Tilahun S. Prevalence of anemia and associated risk factors among adult HIV patients at the anti-retroviral therapy clinic at the University of Gondar Hospital, Gondar, Northwest Ethiopia. Open Access Sci Rep. 2013;2(3). doi:10.4172/scientificreports.662
29. Bizuwork K, Bedada T. Factors associated with anemia among people living with HIV/AIDS taking ART in Ethiopia. Hindawi. 2019;1–8.
30. Pennap GR, Abubakar K. Prevalence of anemia among human immunodeficiency virus infected patients accessing healthcare in federal medical center Keffi. Nigeria Int J Trop Dis Health. 2015;10(3):1–7. doi:10.9734/IJTDH/2015/19657
31. Omregie R, Omokaro EU, Palmer O, et al. Prevalence of anaemia among HIV-infected patients in Benin City, Nigeria. Tanzan J Health Res. 2009;11(1):1–4. doi:10.4314/thrb.v11i1.43242
32. Daniel W, Kilonzo SB, Mpondo BC. Magnitude and correlates of moderate to severe anemia among adult HIV patients receiving first line HAART in Northwestern Tanzania: a cross sectional clinic based study. Pan Afr Med J. 2016;23:26. doi:10.11604/pamj.2016.23.26.8268
33. Gedefaw L, Yemane T, Sahlemariam Z, Yilma D. Anemia and risk factors in HAART Naı ¨ve and HAART experienced HIV positive persons in Jimma, South West Ethiopia. Plose One. 2013;8(8):1–6.
34. Kenenisa C, Tsegaye A, Desta K, et al. Prevalence of anemia before and after initiation of antiretroviral therapy on HIV infected patients at Ras Desta Damtew Memorial Hospital, Addis Ababa, Ethiopia. J Med Health Sci. 2018;7(4):22–30.
35. Adamu AL, Crampin A, Kayuni N, et al. Prevalence and risk factors for anemia severity and type in Malawian men and women: urban and rural differences. Bio Med Central. 2017;15(12).
36. Mohsen M, Rezaei F, Maracy MR, Avijgan M, Tayeri K. Prevalence, severity, and related factors of anemia in HIV/AIDS patients. J Res Med Sci. 2012;17(2):138–142.
37. Sheila C, Vir N, Arun S, Nigam K, Jain R. Weekly ion and folic acid supplementation with counseling reduces anemia in adolescent girls: a large scale effectiveness study in Uttar Pradesh, India. Food Nutri Bull. 2008;5(1):95–98.
38. Prashant J, Amit S, Mumtaz S, Ashok S. Zidovudine-Induced Anemia in HIV/AIDS. J Ped Assoc India. 2015;5(1):47–49.
39. NIDDK. National Institute of diabetes and digestive and kidney diseases. Anemia Inflam Chron Dis. 2013;122(2):103–108.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.